")
Back to Journals » Clinical Ophthalmology » Volume 19
Distribution of Angle Alpha in a Large Population in Eastern China: An Analysis of the 30705 Eyes Using the Ray Tracing Aberrometer
Authors Hua Z, Zeng Q, Zhang L, Shen J, Yang J
Received 9 October 2024
Accepted for publication 12 February 2025
Published 4 March 2025 Volume 2025:19 Pages 753—762
DOI https://doi.org/10.2147/OPTH.S492933
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Zhixiang Hua,1– 5,* Qiulin Zeng,6,* Limei Zhang,7 Jiying Shen,7,* Jin Yang1– 5,*
1Department of Ophthalmology and the Eye Institute, Eye and Ear, Nose, and Throat Hospital, Fudan University, Shanghai, People’s Republic of China; 2The Key Laboratory of Myopia, Ministry of Health, Shanghai, People’s Republic of China; 3Shanghai Key Laboratory of Visual Impairment and Restoration, Shanghai, People’s Republic of China; 4Key National Health Committee of the Key Laboratory of Myopia, Fudan University, Shanghai, People’s Republic of China; 5The Key Laboratory of Myopia, Chinese Academy of Medical Sciences, Shanghai, People’s Republic of China; 6Department of Ophthalmology, Shanghai Xinshijie Dongqu Eye Hospital, Shanghai, People’s Republic of China; 7Department of Ophthalmology, Shanghai Heping Eye Hospital, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jin Yang, Department of Ophthalmology, Eye, Ear, Nose, and Throat Hospital of Fudan University, Shanghai, People’s Republic of China, Tel +008613671632525, Email [email protected] Jiying Shen, Department of Ophthalmology, Shanghai Heping Eye Hospital, Shanghai, People’s Republic of China, Tel +008613817505149, Email [email protected]
Purpose: To describe the distribution of angle alpha orientation and magnitude in a large population and to analyze the impact of eye laterality, gender, and age on angle alpha.
Setting: EENT Hospital of Fudan University and Shanghai Heping Eye Hospital, 2017– 2023.
Design: A retrospective analysis utilizing the iTrace system to examine preoperative angle alpha in patients undergoing cataract surgery.
Methods: Angle alpha orientation and magnitude were collected from 30,705 individuals. The distribution of angle alpha direction and the value of its magnitude were analyzed. In addition, the influence of eye laterality, gender, and age on angle alpha was analyzed in different subgroups.
Results: The analysis revealed that the binocular angle alpha orientation was predominantly located in the temporal region, followed by the nasal region, while the upper and lower regions had a smaller proportion. The average magnitude of angle alpha in the right eye was 0.32 ± 0.19 mm, larger than that of the left eye, and this result was consistent in all subsequent subgroup studies. In a subgroup analysis categorized by gender, females exhibited significantly larger angle alpha than males. Furthermore, in an age-grouped subgroup analysis, a clear tendency was observed that the angle alpha value was increasing with age.
Conclusion: This study analyzed the distribution of angle alpha in a large population and is the first to report the effects of eye laterality, gender, and age on angle alpha. These findings enhance ophthalmologists’ understanding of angle alpha and provide a deeper perspective for cataract surgical planning.
Keywords: angle alpha, iTrace, cataract
Introduction
- Angle alpha, defined as the intersection between the visual and optical axes, is of critical importance in ophthalmology, especially in the context of cataract and refractive surgery. Historically, the clinical application of angle alpha was constrained due to challenges associated with accurately measuring the optical axis. With the advent of high-precision measurement instruments employing Ray-tracing technology, such as iTrace, accurate measurement of angle alpha became feasible, leading to its increasing recognition and utilization by clinicians.1 Although the angle alpha in iTrace actually represents the linear distance between the center of the visual axis and the central vertex of the cornea, which might be different from what other instruments are measured.
- Recently, it has been reported that angle alpha is an essential parameter in the decision-making process for the multifocal intraocular lens (IOL) implantation. This is due to its predictive capacity for postoperative IOL centrality, as well as the direction and distance from the optical axis, factors that are crucial for understanding postoperative higher-order aberrations and visual quality in cataract patients.2–6 Consequently, the magnitude and orientation of angle alpha are not only influential in surgical planning and outcomes but are also critical in determining postoperative visual quality and photic phenomena.
- Previous research delving into the range and variations of angle alpha was constrained by a limited sample size.7 A larger scale can furnish more comprehensive, nuanced data, and aid in a deeper understanding. Therefore, in this retrospective study, a large sample of the Asian population, encompassing various ages and genders, was collected to investigate the direction and magnitude of angle alpha. This was achieved by utilizing iTrace measurements, with the aim of providing deeper insights into the distribution and characteristics of angle alpha, and contributing to the improvement of surgical planning and postoperative outcomes.
Materials and Methods
Subjects
All participants scheduled for conventional cataract surgery and who underwent iTrace examinations were included between 2017 and 2023 at two investigating sites: the Eye and ENT Hospital of Fudan University and Shanghai Heping Eye Hospital in Shanghai. The exclusion criteria were as follows: iTrace reports with over 10 machine-defined failed data points for biometric parameters, a history of ocular surgery or trauma, presence of corneal opacity or disease, strabismus, nystagmus, or any other ocular pathology, and inability to cooperate with the examination.
Ethical approval for this retrospective study was obtained from the Ethics Committees of both the Eye and ENT Hospital of Fudan University and Shanghai Heping Eye Hospital. As this was a retrospective study using de-identified patient data, the Ethics Committees waived the requirement for informed consent, in accordance with local regulations and the Declaration of Helsinki.
Biometric Measurements
The iTrace aberrometer (Tracey Technologies, Houston, TX, USA) was conducted by experienced technicians in a dimly lit room, with the scan area of maximum non-pharmacologically dilated pupil size. To minimize the potential impact of the tear film on angle alpha measurements, subjects were instructed to blink vigorously immediately before the measurements were taken. The aberrometer captures an iris image through an infrared camera to display the center of the pupil, the center of the visual axis, and the center of the limbus (Supplementary Figure 1), Angle alpha is defined by the radial distance between the center of the limbus and the visual axis. The mean of three taken measurements per eye is reported.
Statistical Analysis
The patient data were directly exported from the iTrace software. The angle alpha magnitude represents the linear distance from the visual axis center to the central vertex of the cornea. The angle alpha direction was calculated as a vector angle based on the measured visual axis. The temporal, nasal, superior, and inferior quadrants were defined based on the angle alpha direction in each eye along the meridians of 45°, 135°, 225°, and 315°, respectively. In the present study, the data were processed, analyzed, and visualized using the R Studio software (Version 4.3.3, R Studio, Inc. Boston). Quantitative variables were presented as mean ± standard deviation (SD), while qualitative variables were analyzed in terms of absolute number (n) and frequency (%).
Normality was assessed using the Shapiro–Wilk test. For data that did not follow a normal distribution, the Mann–Whitney U-test was employed for comparisons of the difference of the mean Angle alpha magnitude between left and right eyes in different distribution (superior, nasal, inferior and temporal), while the Wilcoxon Signed-Rank Test was to compare the difference of the mean Angle alpha magnitude between left and right eyes in other subgroups. The relationships between continuous variables were evaluated using Spearman correlation analysis. A p-value of less than 0.05 was considered to indicate statistical significance.
Results
Characteristics
Ultimately, the study comprised a total of 33,634 participants, out of which 32,360 individuals met the inclusion criteria. A total of 30,705 patients’ bilateral iTrace examination data were included, which comprised the data from 31,530 right eyes and 31,535 left eyes after taking the intersection. Out of the 30,705 patients, 12,358 were male and 18,347 were female (accounting for 59.75%). The average age was 47.39, with a range from 10 to 99 years (Figure 1).
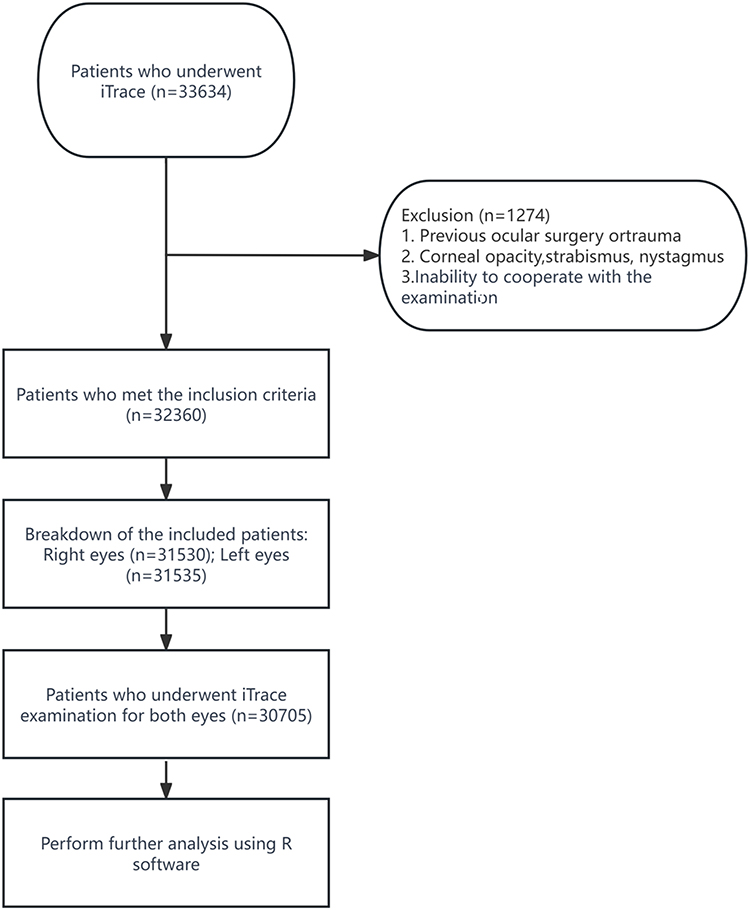 |
Figure 1 Flowchart of Participant Selection. |
Angle Alpha Orientation
In this study, the orientation of angle alpha in each eye was examined. In the right eye, the distribution of angle alpha orientation was as follows: superior (130 cases, 0.42%), nasal (3,020 cases, 9.84%), inferior (268 cases, 0.87%), and temporal (27,287 cases, 88.87%), with the temporal orientation being predominant. A similar pattern was observed in the left eye, with the orientations being superior (118 cases, 0.38%), nasal (4,414 cases, 14.38%), inferior (423 cases, 1.38%), and temporal (25,750 cases, 83.86%). The analysis revealed that in both eyes, the majority of angle alpha orientations were located in the temporal region, followed by the nasal area, whereas the superior and inferior regions had fewer occurrences (Table 1). The orientations and magnitudes of angle alpha were depicted in a polar scatterplot (Figure 2).
 |
Table 1 The Angle Alpha Magnitude in Different Eye and Orientation Groups |
 |
Figure 2 Polar scatterplot of angle alpha in both eyes. Locations of angle alpha were clustered around the horizontal line on both sides of corneal light reflection. |
Angle Alpha Magnitude
The angle alpha magnitudes in both right and left eyes displayed notable positive skewness, evidenced by skewness values of 0.32 and 0.50, respectively. For the right eye, the mean angle alpha magnitude was 0.31 ± 0.19 mm with a median of 0.29 mm. The 25th and 75th percentiles were 0.16 mm and 0.44 mm, respectively (Figure 3a). In contrast, the left eye showed a mean magnitude of 0.27 ± 0.18 mm and a median of 0.24 mm, with the 25th and 75th percentiles at 0.12 mm and 0.38 mm, respectively (Figure 3b).
 |
Figure 3 Comparative Analysis of Angle Alpha Magnitudes and Orientations in Right and Left Eyes.(A) The distribution of angle alpha magnitudes in the right eye.(B) The distribution of angle alpha magnitudes in the left eye.(C) The orientational analysis of angle alpha magnitudes in various anatomical regions (superior, nasal, inferior, temporal) of both eyes, comparing the differences in mean magnitudes between these regions. In this figure, “ns” indicates no significance (p > 0.05), and *** indicates p < 0.001. |
Normality was assessed using the Shapiro–Wilk test, which indicated that the distribution of Angle Alpha magnitude between the left and right eyes did not follow a normal distribution (p < 0.05). A statistically significant correlation was observed in the mean Angle Alpha magnitudes between the left and right eyes (Spearman correlation analysis, p < 0.001). Additionally, a statistically significant difference was found in the mean Angle Alpha magnitudes between the left and right eyes (p < 0.001).
Orientational analysis revealed that in the right eye, the angle alpha magnitudes were 0.64 ± 0.11 mm (superior), 0.14 ± 0.15 mm (nasal), 0.60 ± 0.06 mm (inferior), and 0.33 ± 0.19 mm (temporal). In the left eye, the magnitudes were 0.63 ± 0.12 mm (superior), 0.14 ± 0.14 mm (nasal), 0.59 ± 0.05 mm (inferior), and 0.28 ± 0.18 mm (temporal), as depicted in Figure 3c. Notably, the mean angle alpha magnitudes in the temporal and inferior regions were larger in the right eye than in the left eye (p < 0.001).
Angle Alpha Magnitude in Gender Subgroup
In the gender-based subgroup analysis, the relationship between gender and angle alpha magnitude of both eyes was explored. For females, the mean angle alpha magnitude of the right eye was 0.320 ± 0.195 mm, which was 0.275 ± 0.185 mm of the left eye. The mean magnitude of angle alpha in right eyes were larger than that in left eyes (P < 0.001). For males, the mean angle alpha magnitude was 0.303 ± 0.193 mm for the right eye and 0.262 ± 0.179 mm for the left eye, showing a significantly larger angle alpha magnitude in the right eye as well (P < 0.001). Furthermore, the angle alpha magnitude of both eyes was significantly greater in females than in males, with statistical significance (P < 0.001) (Table 2 and Figure 4).
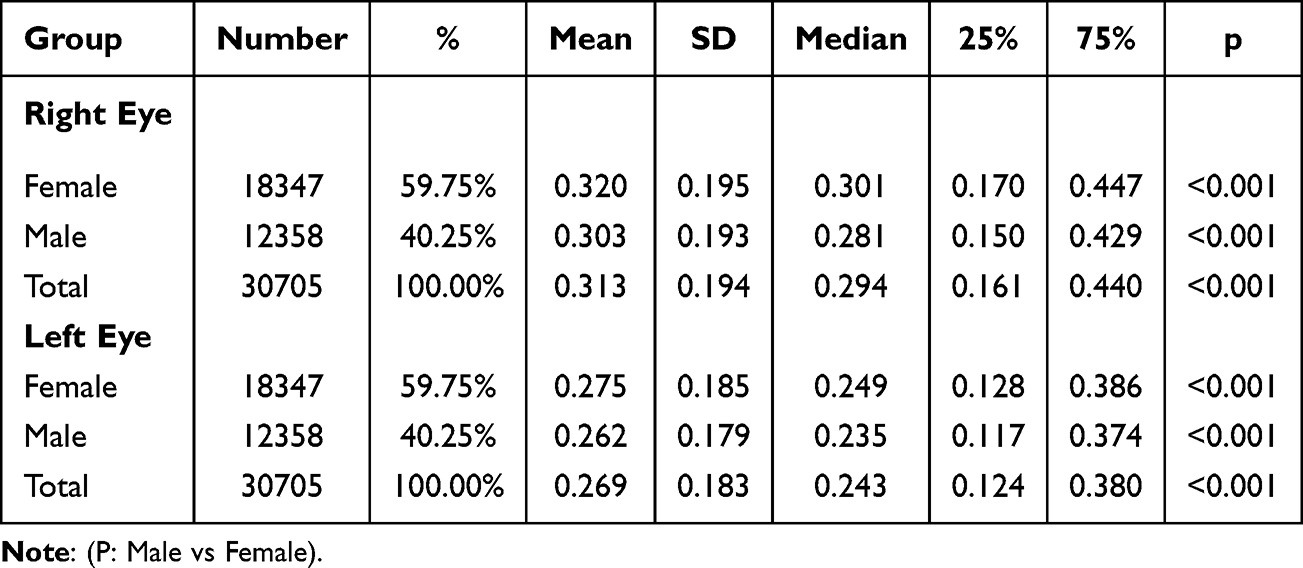 |
Table 2 Angle Alpha Magnitude in Gender Subgroup |
 |
Figure 4 Gender-Based Comparison of Angle Alpha Magnitudes in Right and Left Eyes. In this figure, *** indicates p < 0.001. |
Angle Alpha Magnitude In Age Subgroup
In the age-based subgroup analysis, the mean values and standard deviations of the angle alpha magnitude across eight distinct age groups were displayed in Figure 5. A noticeable trend was observed that the angle alpha magnitude in both eyes gradually increasing with age. Furthermore, within each age subgroup, the angle alpha magnitude of the right eye remains significantly higher than that of the left eye (Table 3 and Figure 5).
 |
Table 3 Angle Alpha Magnitude in Age Subgroup |
 |
Figure 5 Age-Based Comparison of Angle Alpha Magnitudes in Right and Left Eyes. In this figure, *** indicates p < 0.001. |
Discussion
Reflecting the current state of knowledge, this study represented the most comprehensive investigation into angle alpha globally to date. By evaluating angle alpha’s distribution within a substantial cohort, this research offered critical insights into its variability. Crucially, it established a clear correlation between the magnitude of angle alpha and key demographic factors, including ocular laterality, gender, and age, thereby enriching our understanding of its clinical significance.
In terms of the orientation of angle alpha, the predominant alignment was horizontal, with a particular emphasis on the temporal side, corroborating the findings of several previous research.7,8 However, discrepancies emerged in comparing of the magnitude with prior studies, in which the average magnitude of angle alpha was estimated to be around 0.44 and 0.45 mm.7,8
In our study, the overall sample’s results showed an average angle alpha magnitude of about 0.30 mm, which is smaller than those observed in other studies. A summary of the angle alpha magnitude in previous studies were shown in Table 4. Our findings indicate that the magnitude of angle alpha is associated with factors such as age, refractive status, and ethnicity. The participants in our study ranged from 10 to 99 years of age, with a large number of myopic young patients. Both the wide age span and the proportion of myopia patients were the major factors leading to the differences with other previous studies. Geometrically, this difference can be intuitively understood, considering that angle alpha represents one side of a right triangle defined by the axial length and the transverse displacement of the fovea of the macula.8,9 Consequently, patients with high myopia frequently exhibit a smaller angle alpha.
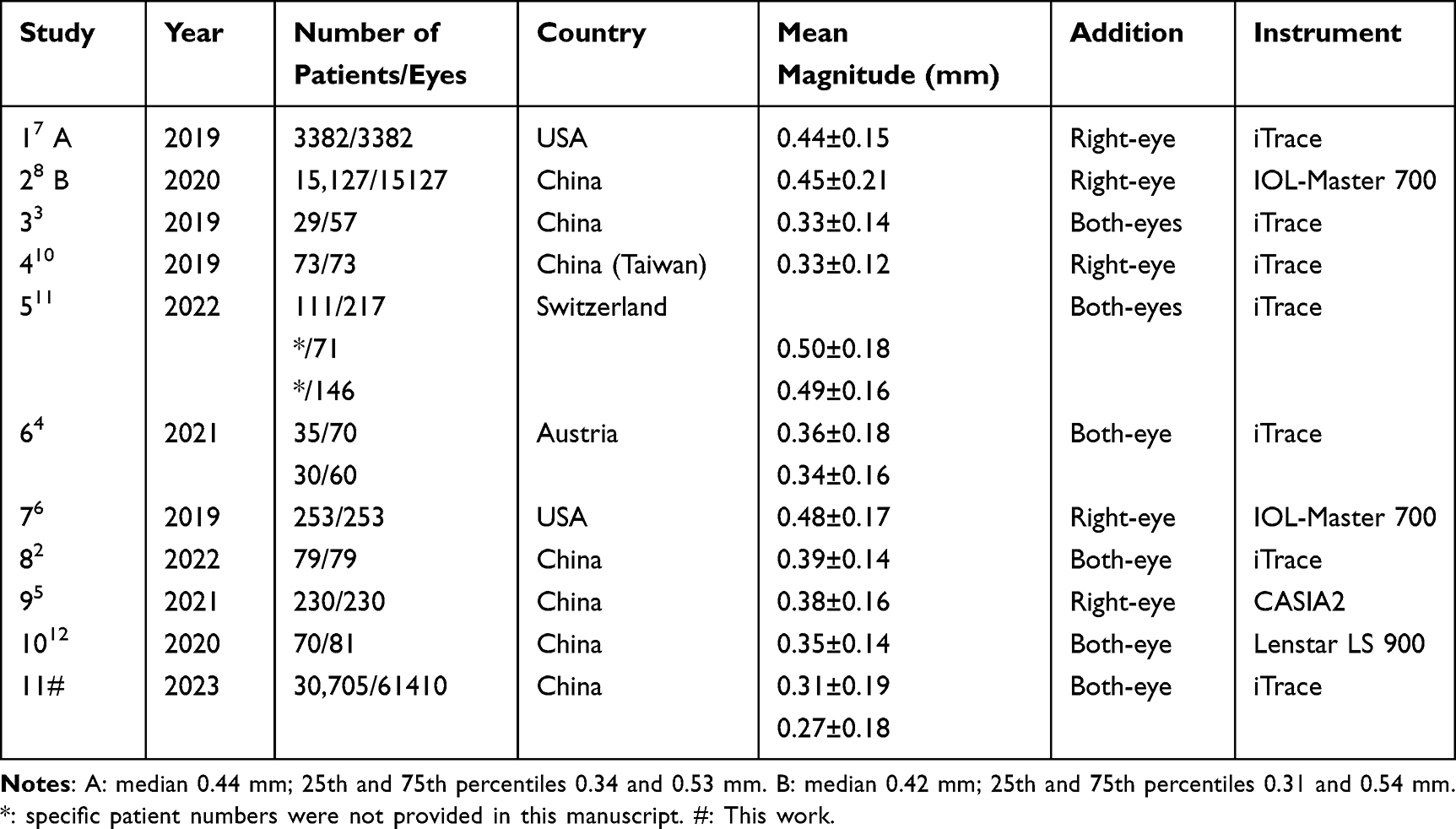 |
Table 4 A Summary of Previous Study of the Angle Alpha Magnitude |
Thus, it can be inferred that ethnic variations might stem from the prevalence of high myopia among different populations. Consistent with reports from Chinese research teams, the magnitude of angle alpha measured using iTrace in our study was also about 0.30 mm. Conversely, the results from studies of western countries seemed to be noticeable larger. Moreover, our results further confirm the impact of gender on angle alpha, indicating that females tend to have a larger angle alpha.
As mentioned above, angle alpha changed with age. The values of angle alpha in the older groups are obviously bigger than that in the younger group, which is in line with the results reported in previous studies. The observed increase of angle alpha in elderly individuals may be associated with several typical ocular changes of aging, such as the prevalent presbyopic refractive status, which is often accompanied by esotropia;13 the flattening of corneal curvature, which could be a factor potentially linked to the natural reduction in eyelid tension;14 and the increase in lens thickness, which might also contribute to this variation in angle alpha.15
In addition, our research firstly reported the influence of ocular laterality on the magnitude of angle alpha. Significant disparities were observed between the right and left eyes. The underlying cause of this observation remains ambiguous; however, based on scant references, it is conjectured that differences in anatomical structures or biological processes may underlie this distinction. For example, nuanced differences pertaining to facial symmetry might be contributing factors.16 Besides, considering the predominance of right-handed individuals, it is plausible that the right eye is predominantly employed for primary visual tasks, potentially impacting specific ocular parameters.14,17
Previous studies have shown that angle alpha seems to be able to predict the tilt of the IOL relative to the visual axis, and thus the angle of incidence of the light onto the IOL, which makes it becoming a important predictor of light phenomena and patient satisfaction after multifocal IOL implantation.10,12 Therefore, it is crucial to consider the individual variability of angle alpha in cataract surgery planning, especially for refractive multifocal IOL implantation. Factors such as ethnicity, examination instruments, age, gender and ocular laterality play a key role in this variability. Surgeons should conduct a comprehensive examination and evaluation of their patients prior to surgical procedures. The variation in angle alpha between the left and right eyes within the same patient underscores the necessity of tailored treatment approaches.
Our results revealed that the binocular angle alpha orientation was predominantly located in the temporal region, followed by the nasal region, with smaller proportions in the upper and lower regions. Meanwhile, it is crucial to position the optic axis within the distal optic zone when implanting a refractive multifocal IOL to ensure optimal distant vision and favorable postoperative outcomes. Therefore, based on our results, in the absence of specific measurements for angle alpha and optic axis position, medical institutions can refer to the typical visual axis location in the general population to minimize potential negative effects caused by misplacement.
Our study still has several limitations. Firstly, as a retrospective study, there is a degree of selection bias in the inclusion of samples. Despite the relatively large sample size, the ocular biometric data drawn from the patients may not fully represent the entire population of China. Secondly, this study is based on preoperative measurements taken from patients using the iTrace device, without conducting cross-device comparisons. Lastly, this study did not include additional ocular biometric parameters beyond angle alpha and analyze their potential associations.
In future research, we aim to investigate angle alpha in a larger sample using different devices and conduct in-depth analyses regarding the effects of eye laterality and gender on angle alpha.
In conclusion, after examining a large population in eastern China, the orientation of angle alpha is primarily distributed in the horizontal direction, both nasally and temporally. A larger magnitude of angle alpha is associated with the right eye, older age, and female gender.
Acknowledgments
We gratefully acknowledge statistical expert Zi-Ang Li for his invaluable assistance in the statistical analysis of this study. Additionally, we thank Aijun Wang for her assistance during the revision process. We would also like to extend our appreciation to Bing Wang and Yvchen Zhang for their helpful guidance on the usage of iTrace equipment. Zhixiang Hua and Qiulin Zeng contributed equally to this work and share first authorship. Jin Yang and Jiying Shen contributed equally to this work and share corresponding authorship.
Funding
This work was funded by the Chinese National Nature Science Foundation (82171039).
Disclosure
All authors declare that they have no conflicts of interest in this work.
References
1. Montrimas A, Žemaitienė R, Yao K, Grzybowski A. Chord mu and chord alpha as postoperative predictors in multifocal intraocular lens implantation. Graefes Arch Clin Exp Ophthalmol. 2023;262(2):367–380. doi:10.1007/s00417-023-06098-x
2. Qin M, Ji M, Zhou T, et al. Influence of angle alpha on visual quality after implantation of extended depth of focus intraocular lenses. BMC Ophthalmol. 2022;22:82. doi:10.1186/s12886-022-02302-4
3. Fu Y, Kou J, Chen D, et al. Influence of angle kappa and angle alpha on visual quality after implantation of multifocal intraocular lenses. J Cataract Refract Surg. 2019;45:1258–1264. doi:10.1016/j.jcrs.2019.04.003
4. Miháltz K, Vécsei-Marlovits PV. The impact of visual axis position on the optical quality after implantation of multifocal intraocular lenses with different asphericity values. Graefes Arch Clin Exp Ophthalmol. 2021;259:673–683. doi:10.1007/s00417-020-05052-5
5. Li Z, Zhu Z, Li X, Meng Z, Qu W, Zhao Y. Age-related changes in crystalline lens tilt and decentration: swept-source OCT study. J Cataract Refract Surg. 2021;47:1290–1295. doi:10.1097/j.jcrs.0000000000000632
6. Wang L, Guimaraes de Souza R, Weikert MP, Koch DD. Evaluation of crystalline lens and intraocular lens tilt using a swept-source optical coherence tomography biometer. J Cataract Refract Surg. 2019;45:35–40. doi:10.1016/j.jcrs.2018.08.025
7. Mahr MA, Simpson MJ, Erie JC. Angle alpha orientation and magnitude distribution in a cataract surgery population. J Cataract Refract Surg. 2020;46:372–377. doi:10.1097/j.jcrs.0000000000000066
8. Meng J, Du Y, Wei L, et al. Distribution of angle α and angle κ in a population with cataract in Shanghai. J Cataract Refract Surg. 2021;47:579–584. doi:10.1097/j.jcrs.0000000000000490
9. Grzybowski A, Eppig T. Angle alpha as predictor for improving patient satisfaction with multifocal intraocular lenses? Graefes Arch Clin Exp Ophthalmol. 2021;259:563–565. doi:10.1007/s00417-020-05053-4
10. Lee CY, Huang JY, Sun CC, Yang SF, Chen HC, Lin HY. Correlation and predictability of ocular aberrations and the visual outcome after quadrifocal intraocular lens implantation: a retrospective longitudinal study. BMC Ophthalmol. 2019;19:188. doi:10.1186/s12886-019-1195-x
11. Baenninger PB, Rinert J, Bachmann LM, et al. Distribution of preoperative angle alpha and angle kappa values in patients undergoing multifocal refractive lens surgery based on a positive contact lens test. Graefes Arch Clin Exp Ophthalmol. 2022;260:621–628. doi:10.1007/s00417-021-05403-w
12. Wang R, Long T, Gu X, Ma T. Changes in angle kappa and angle alpha before and after cataract surgery. J Cataract Refract Surg. 2020;46:365–371. doi:10.1097/j.jcrs.0000000000000063
13. Wright WW, Gotzler KC, Guyton DL. Esotropia associated with early presbyopia caused by inappropriate muscle length adaptation. J AAPOS. 2005;9:563–566. doi:10.1016/j.jaapos.2005.06.008
14. Carey DP. Vision research: losing sight of eye dominance. Curr Biol. 2001;11:R828–R830. doi:10.1016/S0960-9822(01)00496-1
15. Jonas JB, Nangia V, Gupta R, Sinha A, Bhate K. Lens thickness and associated factors. Clin Exp Ophthalmol. 2012;40:583–590. doi:10.1111/j.1442-9071.2012.02760.x
16. Lira J, Langelier N, Lepsch A, Cypen SG, Ranjit-Reeves R, Woodward J. Facial and orbital asymmetry in oculofacial surgery patients. Cutis. 2018;101:E22–e23.
17. Carey DP, Hutchinson CV. Looking at eye dominance from a different angle: is sighting strength related to hand preference? Cortex. 2013;49:2542–2552. doi:10.1016/j.cortex.2012.11.011
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.