")
Back to Journals » Advances in Medical Education and Practice » Volume 16
Does Health Education Through Videos and E-Leaflet Have a Good Influence on Improving Students’ Reproductive Health Knowledge, Attitudes, and Practices? an Intervention Study in Jatinangor, Indonesia
Authors Yuliasih ND, Sari P , Bestari AD, Martini N, Sujatmiko B
Received 29 July 2024
Accepted for publication 28 December 2024
Published 16 January 2025 Volume 2025:16 Pages 29—39
DOI https://doi.org/10.2147/AMEP.S487338
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Neneng Dewi Yuliasih,1 Puspa Sari,1,2 Astuti Dyah Bestari,1,2 Neneng Martini,1,2 Budi Sujatmiko2
1Midwifery Program, Faculty of Medicine, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Department of Public Health, Faculty of Medicine, Universitas Padjadjaran, Sumedang, West Java, Indonesia
Correspondence: Puspa Sari, Midwifery Program, Department of Public Health, Faculty of Medicine, Universitas Padjadjaran, Eyckman 38, Bandung, West Java, 40161, Indonesia, Tel +62 022 2032170, Email [email protected]
Background: Reproductive health issues remain a serious concern, especially for university students. The problem occurs due to a lack of knowledge about three primary threats to adolescent reproductive health, namely, sexuality, HIV / AIDS, and drug abuse, which will affect the attitudes and practices that university students will adopt related to reproductive health. This study aims to analyze the effect of reproductive health education through videos and e-leaflets on improving students’ reproductive health knowledge, attitudes, and practices. The hypothesis for this study was to explore the differences in knowledge, attitudes, and practices before and after the intervention.
Methods: This study used a quasi-experimental design. Purposive sampling was used to select participants from four universities in the Jatinangor District. 166 female first-year university students were divided into the study group through video (n = 83) and the control group through e-leaflet (n = 83). A structured questionnaire assessed reproductive health knowledge, attitude, and behavior before and after the intervention. SPSS version 27.0 was used to analyze the data.
Results: This study showed that university students’ knowledge, attitudes, and practice increased significantly after the intervention (p< 0.001). The comparison results between the intervention group and the control group did not show a significant difference in knowledge improvement (p> 0.001); however, they showed differences in attitude and behavior improvement (p< 0.001).
Conclusion: Reproductive health education through video and e-leaflets is equally effective in improving first-year students’ knowledge, attitude, and practice. University support is necessary for reproductive health education among students.
Keywords: health education, knowledge, attitude, practice, reproductive health
Introduction
Adolescence is a transitional period from childhood to adulthood characterized by physical, mental, emotional, and social growth and development.1–3 First-year students can be classified in the late adolescence category. The number of adolescents in Indonesia is quite large, around 17% of the total population of 275.7 million.4 This large number of adolescents has potential for the country’s development. However, reproductive health problems often occur because adolescents have great curiosity, try new things to find identity, and achieve personal maturity according to developmental tasks.5 A great sense of curiosity and high interest, as well as various physical and psychological changes, cause many problems that arise in the lives of adolescents.6 In addition, this is reinforced by the increasingly sophisticated flow of technology and information that allows adolescents to be at risk of being exposed to the Three primary threats to adolescent reproductive Health, which include sexuality, HIV / AIDS, and drugs if they get or access inappropriate information.7
Sexuality issues in adolescence are synonymous with premarital sexual behavior.8 The 2017 Indonesian demographic and health survey on adolescent reproductive health reported that 59% of women aged 15–19 years had their first sexual intercourse. In addition, 10% of adolescents stated that they had premarital sexual intercourse.9 The impact of this high incidence of sexual behavior among adolescents leads to reproductive health problems, such as sexually transmitted infections (STIs), unwanted pregnancy, and abortion.8 Women aged 15–19 years were among the groups with the highest prevalence of STIs or their symptoms at 21%.10 The incidence of unwanted pregnancy and abortion among adolescents in Indonesia in 2017 was 16% and 20%, respectively.9 In addition, unsafe sexual behavior, both premarital sexual intercourse and changing sexual partners, has the potential to cause HIV/AIDS.8
The incidence of HIV and AIDS cases that occurred in Indonesia in 2021 was 36,902 and 5750 cases, respectively. Meanwhile, HIV and AIDS cases in the age group of 15–19 years were 3.1% and 1.7%, respectively.11 The third problem in adolescents is involvement in the use of illegal drugs. The results of the national survey on drug abuse in 2021 stated that drug abuse has increased from year to year, including in adolescents aged 15–19 years. The incidence of drug abuse in adolescents in 2019 was 1.80%, while in 2021 it was 1.96%. The incidence of drug abuse by adolescent girls and boys in 2021 was 12.2% and 16.8%, respectively.12 Indonesian Demographic and Health Survey on Adolescent Reproductive Health 2017 states that the highest percentage of the starting age of women and men drinking alcohol is in the age group15–19 years.13 Several studies have shown that drinking alcohol increases the likelihood of risky sexual behavior.14–16
Risky sexual behavior is commonly found among university students.16,17 Many sexual activities can be classified as “unsafe” or “risky” including negative sexual behavior.18 Premarital sexual behavior is more common among university students, especially students who do not live with their parents and who lack parental or family supervision and dormitory regulations.19 The results of research by Abdissa et al reported that premarital sexual behavior in college students was significantly triggered by socio-demographic factors, including being separated from parents.20 In addition, lack of knowledge about reproductive health are factors that cause risky sexual behavior in late adolescents who are pursuing higher education.16,21
A study conducted by Mutiara in Jatinangor showed that out of 100 students living in Jatinangor District, they engaged in negative sexual behavior.17 The consequences of risky sexual behavior not only have an impact on reproductive health but also psychological and social.3 The government has made various programs to decrease reproductive problems that occur in adolescents. However, first-year university students have limited access to the available programs.21
The essential program to overcome the three primary threats of adolescent reproductive health problems needs to improve knowledge.7 This knowledge is obtained through various means, including health education.22 Health education is not only about communicating information but also about adopting motivation, skills, and confidence to take action to improve health.23 Health education media are one of the tools to convey health information. Adolescents prefer health education media that is technologically sophisticated, such as through an audio-visual approach in the form of video.23 Video can attract the target’s attention from various sources, save time, and be repeated anytime. Moreover, the audio volume can be adjusted when the presenter wants to explain something.24 Video displays moving images that can be seen and heard. Other than videos, e-leaflets can also be used to deliver messages. E-leaflets facilitate and accelerate students’ understanding of messages presented in short, concise, and easy-to-understand sentences with visuals. E-leaflets are effectively used by individuals, families, groups, and even communities.25,26
Edgar Dale’s cone of experience shows that humans can remember 10% of what is reading information, 20% of what is heard, and 30% of what is seen, but a person can remember 50% of what is seen and heard.27 Therefore, the study aimed to create a well-designed, easy-to-understand educational video and e-leaflet about reproductive health to enhance students’ knowledge, attitudes, and practices. The hypothesis for this study was that there were differences in knowledge, attitudes, and practices before and after the intervention.
Material and Methods
Study Design
A quasi-experiment design with a control group assessed first-year students’ knowledge, attitudes, and practices about reproductive health after intervention. This study was conducted in the Jatinangor district between October 2023 to January 2024. The study was conducted following the guidelines of the Declaration of Helsinki. The Ethical Committee of the Faculty of Medicine, Universitas Padjadjaran, approved the study, approval number 721/UN6.KEP/EC/2023. After being informed, participants were requested to provide written informed consent.
Sample Size and Sampling Procedure
Students from the four universities in the Jatinangor subdistrict participated in our study. The survey was conducted among first-year students with personal mobile phones. The total number of first-year students from four universities in Jatinangor is 12,364. Participants who resigned during the study were excluded, and those who completed the questionnaire were included. A purposive sampling technique was chosen to select study participants, with the criteria of female gender, first-year status, and willingness to participate at four universities in the Jatinangor sub-district. Female first-year students were selected based on the researcher’s area of competence. The sample size of 150 students was estimated using the paired numerical comparative formula.28

Where (Zα=1,96) for confidence level 95%, power test 20% (zβ=0,84), “s” is the magnitude obtained from the research of Qonitatum et al, which is s = 267.12.67,29 and x1-x2 The minimum mean difference set by the researcher is 10.


The minimum required sample size was 150 participants (75 respondents for each experimental and control group). The participants were selected by purposive sampling based on the inclusion criteria. If “n” is the sample size required (150 in this study) as per the formula and if d is the dropout rate (usually 10% to 20%), then the adjusted sample size N1 is obtained as N1 = n/(1–d).30 The researcher added the sample size to anticipate a 10% dropout; this means that 166 participants were needed to be enrolled in this study. The participants were divided into control (83) and intervention groups (83) based on their willingness.
Data Collection Tools
The study instrument was developed based on relevant studies to measure knowledge, attitudes, and practices toward reproductive health. The questionnaire consists of four parts: Part 1 consisted of eight questions about the demographic data of the students; Part 2 consisted of 15 questions with a Guttman scale related to students’ knowledge, which was divided into five items for sexuality, six items for HIV/AIDS, and four items for drug abuse. Responses were scored as 1 for correct responses or 0 for incorrect responses. Part 3 consisted of 14 questions with a Likert scale related to students’ attitudes, which were six items for sexuality, five items for HIV/AIDS, and three items for drug abuse. Part 4 consisted of 16 questions with a Likert scale related to students’ practice, which included six items for sexuality, eight items for HIV/AIDS, and two items for drug abuse. The scale attitude and practice rated as “strongly disagree” (1), “disagree”, (2), “agree”, (3), or “strongly disagree” (4). The total score ranges from 0 to 100, with higher scores indicating more positive attitudes and practices. Experts reviewed the questionnaires’ validity, reliability, and content. The data were entered into IBM SPSS version 27 statistical software to conduct an appropriate analysis test to measure the tool’s validity and reliability. Cronbach’s alpha was reported to be 0.738 for knowledge, 0.714 for attitude, and 0.855 for practice, indicating that the tool was reliable and valid.
Data Collection Procedure
The participants were divided into control and intervention groups based on their willingness. The researcher conducted a pre-test session to determine students’ knowledge, attitudes, and behavior related to reproductive health in the intervention and control groups. The questionnaire was distributed via Google Forms through the WhatsApp group that had been created. The post-test was conducted after 66 days of intervention with the same questionnaire as the pre-test.
The Intervention
Reproductive health education was provided to the intervention groups using a video with a duration of 10 minutes and to the control groups using an e-leaflet. E-leaflet, an abbreviation for electronic leaflet, is a digital health education tool that conveys specific messages to the audience. It can be embedded in soft file form in various media. The content of the e-leaflet is the same as that of the video media, without moving images or sounds. Researchers will send a reminder every week to ensure that participants undergo intervention. The video and e-leaflet used as reproductive health education media in this study have been feasibility tested by media experts. Some video screenshots are shown in Figures 1a–c, and the e-leaflet is shown in Figure 2a and b.
 |
Figure 1 (A) Reproductive health education through video. (B) Reproductive health education through video (sample case). (C) Reproductive health education through video (Reproductive health education by midwives). Notes: Individuals in Figure 1A-C provided consent for their images to be published. |
 |
Figure 2 Continued. |
 |
Figure 2 Reproductive health education through e-leaflet. |
Data Processing and Analysis
Data were checked, cleaned, coded, and tabulated using the IBM SPSS version 27 statistical software. Descriptive statistics were used to describe the characteristics of participants, presented by counting frequencies and percentages. The Wilcoxon test was used for a pretest and posttest comparison of the study variables within each group. The Mann–Whitney test compared the control and intervention groups’ main study variables. The p-value of less than 0.05 was considered significant.
Results
The sociodemographic characteristics of the participants are shown in Table 1. A total of 83 female first-year university students were included in the intervention group and the control group. It was found that most participants were from the non-health field, 61% of whom were in the intervention group and 70% in the control group. Participants who lived with both parents in the intervention group were 53%. In contrast, in the control group, most participants lived alone at 54%, with living status in the intervention group at 55% private houses and the control group at 47% cost/apartments. All participants stated that they had obtained reproductive health-related information from sources of information that came from healthcare workers, as little as 7% in the intervention group and 6% in the control group.
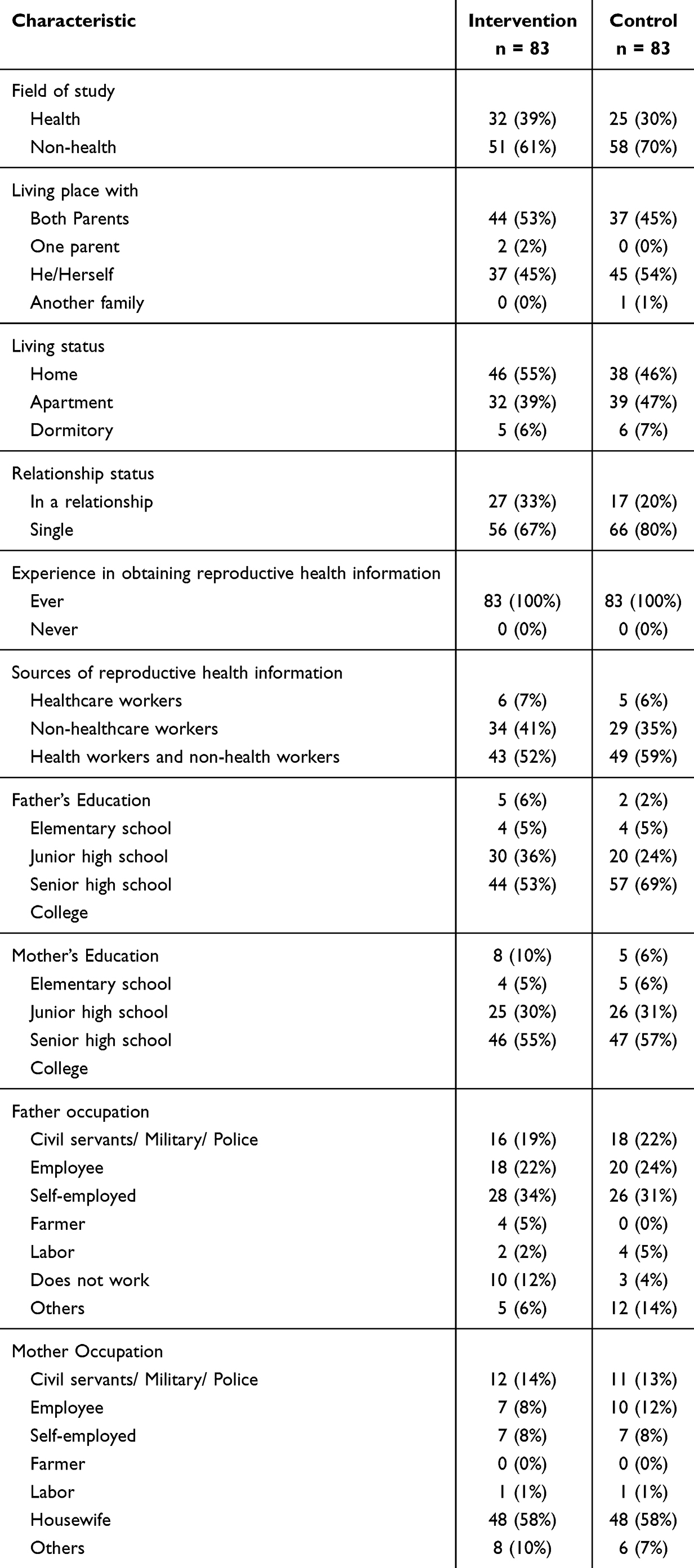 |
Table 1 Sociodemographic Characteristics of Respondents |
Parental data showed most of the last education of the participant’s parents was in college, with the father’s previous educational background at 53% in the intervention group and 69% in the control group, while the mother’s 55% in the intervention groups and 57% in the control groups. In addition, the parents’ data also showed that the father’s occupation, 34% in the intervention group and 31% in the control group stated that he worked as self-employed, while the mothers mainly were as housewives, namely 58% in the intervention group and 58% in the control group (Table 1).
The result showed that reproductive health education improved the group’s knowledge, behavior, and attitude through the video and e-leaflet summarized in Table 2. Following the intervention, the mean knowledge score increased to 91.80 ± 7.92 from the baseline mean of 83.65 ± 9.86. The mean attitude score was 85.30 ± 5.87 before the intervention and increased to 90.78 ± 4.14 following the intervention. Following the intervention, the average practice score increased from 75.78 ± 10.77 to 90.69 ± 5.32. Knowledge, attitudes, and practices also increased in the control group (e-leaflet). The same results in the control group revealed a significant increase in the total knowledge, attitude, and practice scores from the pretest to the posttest (Table 2).
 |
Table 2 Differences in Pretest and Posttest of Knowledge, Attitude, and Practice Scores Between Intervention and Control Group Based on Bivariate Analysis |
However, after health education, the intervention group recorded no significant difference between the total knowledge score (mean rank= 90.04) compared to the control group score (mean rank= 79.96) with p > 0.001. Furthermore, after health education, the intervention group had significantly higher total attitude and practices score (mean rank= 99.58 and 114.01) compared to the control group score (mean rank= 67.47 and 52.99), with p < 0.001 (Table 3).
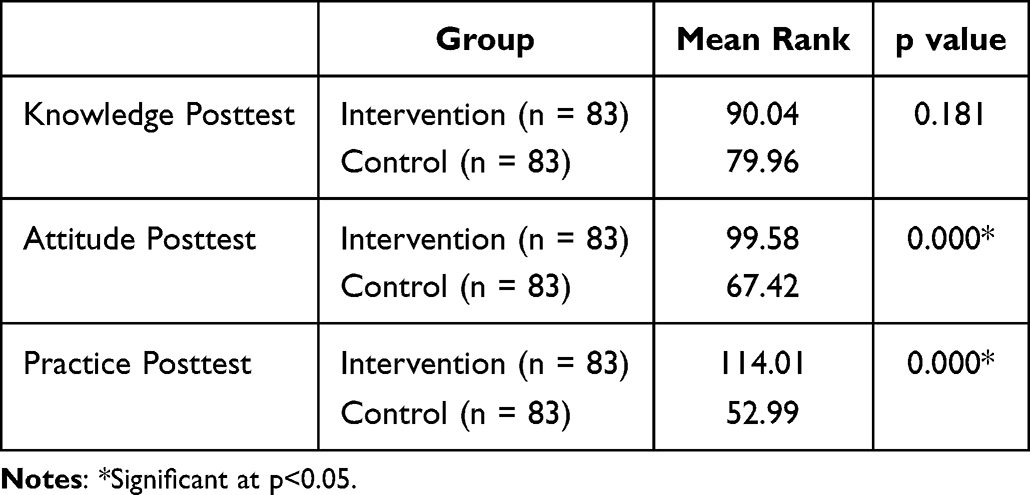 |
Table 3 Comparison of Knowledge, Attitude, and Practice Between Intervention and Control Group Based on the Mann–Whitney Test |
Discussion
The participants’ sociodemographic profile results showed that most first-year students in both the control and intervention groups lived alone. Previous studies showed that premarital sexual behavior is more common among university students, especially students who do not live with their parents and who lack parental or family supervision and dormitory regulations.19 Therefore, correct information is very necessary in preventing reproductive health problems. The results of research by Abdissa et al reported that premarital sexual behavior in college students was significantly triggered by socio-demographic factors, including being separated from parents.20
This study’s evidence showed that the reproductive health education provided by the video and e-leaflet improved the group’s knowledge, behavior, and attitude. This aligns with research conducted by A’isy et al, who also showed that audiovisual health education can significantly improve adolescents’ knowledge, attitudes, and practices about reproductive health.31 Providing health education is a beneficial experience that benefits knowledge in maintaining and improving their health.25,26 According to WHO, knowledge can be obtained from one’s own experience or the experience of others. Thus, cognitive skills are critical in shaping a person’s attitudes and practices.32 Rosenberg’s theory, known as affective cognitive consistency theory, also revealed that attitudes are centered on the relationship between cognitive and affective components.25
The use of media can help the success of the information delivery process. Hence, the media is one of the things that needs to be considered when delivering information.8 Information is one of the factors that can affect knowledge.32 Using video media in education makes it easier for students to understand and motivate them in learning activities.33 The ability of video to attract attention is an integral part of the process of persuading individuals to change attitudes. The attention-getting stimulus given by using video media causes communication and attention in the respondent. There is attention, and then there is an understanding of the stimulus given (correctly comprehended) so that there is good acceptance.24
Edgar Dale, in Dale’s Cone of Experience, suggests that humans can remember 30% of what they watch a video, in contrast to someone who only reads and can remember only 10% of what is read. This illustrates that the health education process, involving more senses, will be more readily accepted and remembered by the education target.27 This is in line with Lou’s observation that the messages presented in the media influence adolescents’ knowledge, attitudes, and behavior.34
Knowledge is essential to forming a person’s positive attitude and practice. A person who obtains reproductive health education has better knowledge about reproductive health and puts more effort into preventing reproductive health problems. The results of this study show that there is an increase in knowledge after being given reproductive health education with a video that can encourage students to seek and choose the correct information, communicate, and be open with parents to prevent reproductive health problems.
This study showed no significant difference between the intervention and control groups on knowledge. Meanwhile, attitudes and behavior significantly differ between the intervention and control groups. This is in line with Yuhandini et al’s research in 2021, which showed that the interventions carried out in the audio-visual and webtoon groups did not significantly differ in participants’ knowledge.35 The research conducted by A’isy et al showed that health education using audio-visual media is more effective than using leaflet media on adolescents’ knowledge, attitudes, and behavior about reproductive health.31
Health education with video and e-leaflets is equally effective in improving first-year university students’ reproductive health knowledge. This can occur because both media used for intervention have advantages and disadvantages. In this study, there were several possible factors. For example, when reading the e-leaflet, participants began to feel interested because the leaflet not only contained writing or text that was quite clear and easy to understand but also provided quite exciting images. The images did not move but could make the leaflet easily understood by participants. Furthermore, the video was exciting and easy to understand.31 It provided new insights about reproductive health, especially sexuality, HIV/AIDS, and drug abuse.
The limitation of this study was that each participant had a different ability to absorb information and intensity of attention when listening to videos. The extended video duration of more than 6 minutes also reduced the intensity of participants’ attention, causing no change in participants’ knowledge, even though they had participated in health education.36 These factors may have a minor impact on the variations between the intervention and control groups.
This study allowed for the transfer of information that provided new knowledge to the participants. The increase in knowledge in this study has a positive relationship with the rise in attitudes and practices, proving the truth of the theory that knowledge influences one’s decisions regarding attitudes and practices.32 After health education intervention in first-year students, knowledge, attitudes, and practices regarding reproductive health increased. In addition, universities need to intervene in efforts to reduce reproductive health problems.
Conclusion
Our study showed that reproductive health education through video and e-leaflets within 66 days can improve knowledge, attitude, and practices. Health education through appropriate media is essential to make interventions more effective in reducing reproductive health problems in first-year students. University support is necessary for reproductive health education for students.
Acknowledgments
The authors would like to thank the study participants for their contribution and Universitas Padjadjaran for the article processing charge (APC) if this article is published and also provides acceleration grants for senior lecturers (RPLK). We also express our gratitude to the expert assessors of videos and e-leaflets as health education media who have provided input and improvements to the media.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hanifah SD, Nurwati N, Santoso MB. Sexuality and Free Sex of Teenagers. J Res Community Serv. 2022;3(1):57.
2. Wirenviona R, AAIDC R. Adolescent Reproductive Health Education. Airlangga University Press; 2020.
3. Hapsari A. Reproductive Health Textbook Adolescent Reproductive Health Module. UPT UNDIP Press Semarang; 2019:143.
4. Central Bureau of Statistics. Total Population by Age Group and Sex</col> 2022 [Internet]. Central Bureau of Statistics. 2023
5. Aryani A, Widiyono Anitasari A. Overview of Adolescent Knowledge about HIV/AIDS. Indones J Nurs Sci. 2021;14(2):120.
6. Hidayah U, Sari P, Susanti AI. Overview of Adolescents’ Knowledge of Hiv/Aids After Participating in the Great Program at Junior High School Bandung City. J Heal Syst. 2018;3(3):111–115.
7. Handayani F. Improving Muhammadiyah High School Students’ Knowledge of the Three Basic Threats of Adolescent Reproductive Health. J Midwifery Community Serv. 2020;2(1):9.
8. Wilandika A, Kamila A. E-Module of Three Basic Threats of Adolescent Reproductive Health: impact on Student’s Knowledge. Malaysian J Public Heal Med. 2022;22(3):234–243. doi:10.37268/mjphm/vol.22/no.3/art.1419
9. BKBBN. Demographic and Health Survey: adolescent Reproductive Health 2017. 2018; Available from: http://www.dhsprogram.com.
10. Ministry of Health Republic Indonesia. Indonesia Demographic and Health Survey 2017.
11. Ministry of Health Republic Indonesia. Indonesia Health Profile Jakarta: Ministry of Health Republic Indonesia; 2022. Available from: https://www.kemkes.go.id/downloads/resources/download/pusdatin/profil-kesehatan-indonesia/Profil-Kesehatan-2021.pdf.
12. BNN. National Survey on Drug Abuse in 2021. 2022. Available from: http://www.jurnal.stan.ac.id/index.php/JL/article/view/557.
13. Badan Kependudukan dan Keluarga Berencana Nasional (BKKBN). Survei Demografi Dan Kesehatan Indonesia 2017: Kesehatan Reproduksi Remaja. Jakarta; 2018.
14. Agu CF, Oshi DC, Abel WD, et al. Alcohol consumption and sexual risk behaviour among Jamaican adolescents. Asian Pacific J Cancer Prev. 2018;19:1–6.
15. de Vlieg RA, van Empel E, Montana L, et al. Alcohol Consumption and Sexual Risk Behavior in an Aging Population in Rural South Africa. AIDS Behav. 2021;25(7):2023–2032. doi:10.1007/s10461-020-03132-5
16. Tekletsadik EA, Ayisa AA, Mekonen EG, Workneh BS, Ali MS. Determinants of risky sexual behaviour among undergraduate students at the University of Gondar, Northwest Ethiopia. Epidemiol Infect. 2022;150.
17. Mutiara W, Komariah M. Overview of Sexual Behavior with Heterosexual Orientation of Kos Students in Jatinangor District - Sumedang. J Unpad. 2018;10(18):14–27.
18. Marcus JL, Snowden JM. Words Matter: putting an End to “Unsafe” and “Risky. Sex Sex Transm Dis. 47(1):1–3.
19. Tooy GC, Wuaten GA, Umboh MJ, Tatangindatu MA. Relationship Knowledge And Motivation Of Boarding House Student With Premarital Sexual Actions In Manganitu District). Sesebanua Sci J. 2023;7(1):10–14. doi:10.54484/jis.v7i1.576
20. Abdissa B, Addisie M, Seifu W. Premarital Sexual Practices, Consequences and Associated Factors among Regular Undergraduate Female Students in Ambo University, Oromia Regional State, Central Ethiopia, 2015. Heal Sci J. 2017;11(1):1–7.
21. Aziz AR. Implementation of Generasi Berencana (GenRe) Program in Palembang City. J Public Adm Sci. 2021;19(1).
22. Ernawati D, Arini D, Hastuti P, et al. Health Education in Improving the Knowledge of Grade 10 Students about Adolescent Reproductive Health at Hang Tuah 1 Surabaya High School. Natl Semin Comm Serv. 2022;1(1):400–407.
23. Naufi B, Amanah S, Fatchiy A. Knowledge and Attitudes of Adolescent Information and Counseling Center Members Toward Three Basic Risks to Reproductive Health. Kommunity Online J. 2021;2(1):65–73. doi:10.15408/jko.v2i1.21893
24. Kurniawati DI, Andarmoyo S, Wahyuni NS, Muftiana E, Sari RM. The Effect of Health Counseling with Audio Visual Media on Smoking Behavior in Adolescents at Smpn 1 Sawoo. Heal Sci J. 6(1):45.
25. Pakpahan M, Siregar D, Susilawaty A, et al. Health Promotion and Health Behavior. Medan: Yayasan Kita Menulis; 2021.
26. Milah AS. Health Education and Health Promotion in Nursing. Tasikmalaya: Edu Publisher; 2022.
27. Khotimah H, Supena A, Hidayat N. Increasing Attention of Early Grade Students through Visual Media. J Child Educ. 2019;8(1):17–28.
28. Dahlan MS. Sample Size in Medical and Health Research. Jakarta: Indonesian Epidemiology; 2016.
29. Qonitatun A. The Effect Of Health Education Using Audiovisual Media About Reproductive Health Towards Increasing Knowledge Of Adolescent Girls At Akhul Muslim Islamic Boarding School Sragen. 2023.;
30. Gupta KK, Attri JP, Singh A, Kaur H, Kaur G. Basic concepts for sample size calculation: critical step for any clinical trials! Saudi J Anaesth. 2016;10(3):328–331. doi:10.4103/1658-354X.174918
31. Aisy HN, Betty Rahayuningsih F. Effectiveness of Audiovisual and Leaflet on Knowledge, Attitude, and Practice About Adolescent Reproductive Health at SMPN 1 Gemolong. Universitas Muhammadiyah; 2022.
32. Pratiwi AWE, Afriyani LD, Zulkarnain A. Differences in the Effectiveness of Health Education on Breast Self-Examination (SADARI) by Using Leaflet Media and Audio Visual Media on Adolescent Girls at SMK NU Ungaran. J Holistics Heal Sci. 2019;1(1):1–10.
33. Hadi Sofyan. TEP & PDs Proceedings: effectiveness of Using Video as Learning Media for Elementary School Students. Naut J Ilm Multidisiplin. 2017;97(1):15.
34. Lou C, Cheng Y, Gao E, Zuo X, Emerson MR, Zabin L. Media’s contribution to sexual knowledge, attitudes, and behaviors for adolescents and young adults in three Asian cities. J adoles health. 2008;42(2):157–162.
35. Yuhandini DS, Khulaidah N. the Effect of Audio Visual and Webtoon Explanation To Knowledge and Attitude About the Three Basic Threats of Adolescent Reproductive Health on Students of Sman 8 Cirebon City, 2021. Int Semin Gend Equity Matern Child Heal. 2021;1(1):80–91. doi:10.34305/gemic.v1i1.315
36. Andriani R. Development of Infants’ Anthropometric Measurements Video for Knowledge Improvement. J Pendidik Kedokt Indo J Med Educ. 2023;12(2):234.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Managing Pain in Low Resource Settings: Healthcare Professionals’ Knowledge, Attitude and Practice Regarding Pain Management in Western Nepal
Thapa P, KC B, Lee SWH, Dujaili JA, Gyawali S, Mohamed Ibrahim MI, Alrasheedy AA
Journal of Pain Research 2022, 15:1587-1599
Published Date: 2 June 2022
Knowledge, Attitudes, and Practices Regarding Ergonomic Hazards Among Healthcare Workers in a Saudi Government Hospital

ALHazim SS, Al-Otaibi ST, Herzallah NH
Journal of Multidisciplinary Healthcare 2022, 15:1771-1778
Published Date: 24 August 2022
Critical Care Nurses’ Knowledge, Attitudes, and Practices Regarding Pressure Injury Treatment: A Nationwide Cross-Sectional Survey
Li J, Zhu C, Liu Y, Song B, Jin J, Liu Y, Wen X, Cheng S, Wu X
Risk Management and Healthcare Policy 2022, 15:2125-2134
Published Date: 16 November 2022
Self-Medication Prevalence and Factors Associated with Knowledge and Attitude Towards Self-Medication Among Undergraduate Health Science Students at GAMBY Medical and Business College, Bahir Dar, Ethiopia
Siraj EA, Yayehrad AT, Kassaw AT, Kassahun D, Solomon E, Abdela H, Gizachew G, Awoke E
Patient Preference and Adherence 2022, 16:3157-3172
Published Date: 5 December 2022
Role of Community Pharmacist in Asthma Management: Knowledge, Attitudes and Practice
Jarab AS, Al-Qerem W, Alzoubi KH, Almomani N, Abu Heshmeh SR, Mukattash TL, Al Hamarneh YN, Al Momany EM
Journal of Multidisciplinary Healthcare 2024, 17:11-19
Published Date: 3 January 2024