")
Back to Journals » Clinical Ophthalmology » Volume 19
Double C-Loop Haptic Lenses Are Rotationally Stable – A Systematic Review
Authors Daya S , Chassain C, Pagnoulle C
Received 23 April 2025
Accepted for publication 4 July 2025
Published 12 July 2025 Volume 2025:19 Pages 2259—2269
DOI https://doi.org/10.2147/OPTH.S536114
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Sheraz Daya,1 Christophe Chassain,2 Christophe Pagnoulle3
1Centre for Sight, East Grinstead, West Sussex, UK; 2Clinique Beau Soleil, Montpellier, France; 3Research and Development Department, BVI, Liège, Belgium
Correspondence: Christophe Pagnoulle, Research and Development Department, BVI.All. des Noisetiers 4, Liège, 4031, Belgium, Email [email protected]
Abstract: The purpose of this review is to summarize the clinical rotational stability outcomes reported in patients following implantation of the POD platform with double C-loop haptics. A literature search in PubMed (US National Library of Medicine) was carried out to find publications, both prospective and retrospective, which report rotational stability outcomes in patients who were implanted with this platform after cataract or refractive lens exchange surgeries. This platform is used in different commercially available intraocular lenses (IOLs), both monofocal and trifocal, made of hydrophilic or hydrophobic material. 19 clinical peer-reviewed studies published between 2013 and 2024 were included in this review. The data reported in the clinical publications was analyzed in detail, focusing on rotational stability (mean rotation values and ranges, and percentage of eyes with some degrees of rotation), measurement methods and rotation follow-up period. Our review encompassed a total of 1428 eyes implanted with the POD platform analyzed at different follow-up periods, up to a maximum of 26 months. The mean rotation across all the studies was 2.61 °.The analysis carried out in this review leads us to conclude that the POD platform provides good rotational stability when used with different IOL models based on monofocal or trifocal designs and made using hydrophilic or hydrophobic material.
Keywords: rotational stability, haptic, double C-loop, intraocular lens, platform
Introduction
Stability of an intraocular lens (IOL) when implanted after cataract or refractive lens exchange (RLE) surgery is crucial for providing optimal refractive and visual outcomes. Minimizing postoperative rotation of the IOL is essential for reducing postoperative residual astigmatism. The degree of postoperative IOL rotation can be affected by an array of factors including capsulorhexis size, axial length, and the IOL design which in turn influences rotational stability.1,2 Given the wide range of factors that can contribute to a possible misalignment, maximizing the intrinsic rotational stability of the IOL is an important component in optimizing visual outcomes.3 Rotational stability of a toric IOL is dependent on a number of aspects, including lens material and design.4 A recent systematic review and single-arm meta-analysis of 51 published studies including 4863 eyes revealed that postoperative rotation is dependent on many aspects of lens material and design.3 The haptic design and material of an IOL may play an important role in its stability, since these may induce changes in the capsule.
One of the most widely used haptic designs worldwide is the POD platform (BVI Inc., Waltham, USA). This structure with a double C-loop, has a symmetrical quadripod design with two-by-two oppositely oriented haptics. This design provides four contact points for fixing the IOL in the capsular bag when implanted along with a large area. It has been used in monofocal and trifocal IOLs, both in toric and non-toric versions. In a biomechanical laboratory study, Bozukova et al5 found that hydrophobic acrylic C-loop, double C-loop, and closed quadripod haptics applied optimum compression forces to the capsular bag with negligible optic axial displacement and tilt compared with plate haptics and poly (methyl methacrylate) haptics. The axial displacement and tilt tests carried out in this experiment showed that whatever the test-well diameter, the optical part of the C-loop and double C-loop IOLs remained in a stable position. These authors argued that the moderate haptic compression force of the double C-loop IOLs contributes to their positional and refractive stability. In a later study, Bozukova et al6 undertook a detailed analysis of the behavior of the double C-loop platform using a computer simulation, in vitro, and in vivo (animal) conditions, demonstrating the benefit of the haptic design in ensuring axial and centration stability. Recent studies7,8 using finite element modeling have looked at the biomechanical stability of IOLs prior to their implantation. The computer simulation7 analyzed the POD F and POD FT IOLs showing that the axial displacement was the maximal with the FT model, and the tilt, rotation, and lateral decentration were substantially lower than the acceptable tolerance limits established by ISO.11979−2.9 This study revealed that, in terms of rotation, all the IOL models were rotationally stable Although the POD F IOL showed maximum magnitude of rotation at all compression diameters (varying from 0.375 ° to 0.256 °), this amount is not clinically relevant confirming excellent stability of this platform.
In addition to laboratory evaluation, clinical studies are necessary to fully understand the performance of this platform when implanted. While several publications have confirmed rotational stability of several types of POD based IOLs, to our knowledge there has been no meta-analysis performed. This paper reviews the metanalysis of internationally peer-reviewed publications evaluating the rotational stability outcomes of the different POD-platform-based IOL.
Methods
The POD double C-loop platform has a symmetrical quadripod design with two-by-two oppositely oriented haptics. This design provides four contact points for fixing the IOL in the capsular bag when implanted. The double C-loop design allows the IOL to be rotated both clockwise and counterclockwise during surgery. This haptic orientation also helps fix the IOL in the capsular bag, providing four contact points; a higher degree of haptic contact between the IOL and the capsular bag is associated with greater material-tissue friction, reducing the IOL rotation within the bag.6 This platform has been used with different IOL models, from monofocal to trifocal lenses, both with and without a toric design and using either hydrophilic or hydrophobic material. The main characteristics of the lenses (currently available) are illustrated in Table 1 and Figure 1 shows their respective images. All the lenses have an overall diameter of 11.40 mm and an optical diameter of 6.00 mm. In all models, monofocal, monofocal toric, trifocal or trifocal toric the optic design is biconvex aspheric. Trifocal models are diffractive lenses with two additional powers at the IOL plane of +1.75 D and +3.50 D. Toric models have cylinder values ranging from 1.00 D up to 6.00 D. The spherical power ranges from 0 D up to +35.00 D, with different steps, depending on the model. The materials used are 26% hydrophilic acrylic (refractive index of 1.46 and Abbe number of 58) or GFY hydrophobic acrylic (refractive index of 1.53 and Abbe number of 42). The POD AY 26P, is no longer available on the market, and was the first lens to use this platform. This model has a monofocal aspherical design and is made of 26% hydrophilic acrylic with an overall diameter of 11.4 mm.
 |
Table 1 Characteristics of Different Intraocular Lenses That Use the POD Platform |
 |
Figure 1 Images of the different intraocular lenses evaluated (courtesy of BVI Inc., Waltham, USA). |
To find published clinical studies that include IOLs with the POD platform we used the PubMed database (US National Library of Medicine). Both retrospective and prospective clinical studies based on cataract or RLE surgeries published in peer-reviewed journals written in English were considered for this analysis. The date of the latest electronic search was January 15th, 2025. To be included, the publications had to provide data on the rotational stability of the platform. Note that any studies evaluating IOL models with this platform but which did not report rotational stability were excluded from the analysis. The search included a combination of any of the following keywords: “IOL”, “ANKORIS”, “PODEYE”, “TORIC”, “FINEVISION”, “POD F”, “POD FT”, “HP”, “PODTAY26P”, “PADAGF”, “PODT49P”, “PODFY26P”, “PODFTY26P”, “PODFGF”, and “PODFT49P”. Moreover, for each article selected from this search, all of its references were also checked to ensure that any clinical publications including the POD platform would not be missed.
Results
The search identified 19 articles with publication dates from 2013 to 2024.7,10–27 These were reviewed and analyzed in detail. The first publication that reported on rotational stability outcomes of the POD platform was published in 201310 (the reported lens POD AY 26P lens is no longer available commercially). The principle features of each publication were extracted, including the name of the authors, publication year, number of eyes and patients recruited, type of study (prospective or retrospective), type of surgery (cataract or RLE), follow-up time, patient age, axial length, and IOL power (sphere, and cylinder for the toric models. These are tabulated (Table 2). Where available, the mean, standard deviation, and ranges were included. Where data was reported for multiple follow-up periods, outcomes used for analysis were from the longest postoperative from surgery. Two articles assessed the POD AY 26P IOL,10,14 3 articles looked at the ANKORIS IOL,11,15,19 2 articles evaluated the PODEYE IOL,14,16 3 articles reported on the PODEYE TORIC IOL,24,25,27 3 articles studied the FINEVISION IOL,7,13,17 8 articles were on the FINEVISON TORIC IOL,7,12,15,17,18,20–23 and 1 analyzed the FINEVISION HP TORIC IOL.26 8 articles were retrospective and 11 prospective in cataract patients, except for one including both cataract and RLE patients.26 The follow-up period varied from 1 to 26 months.
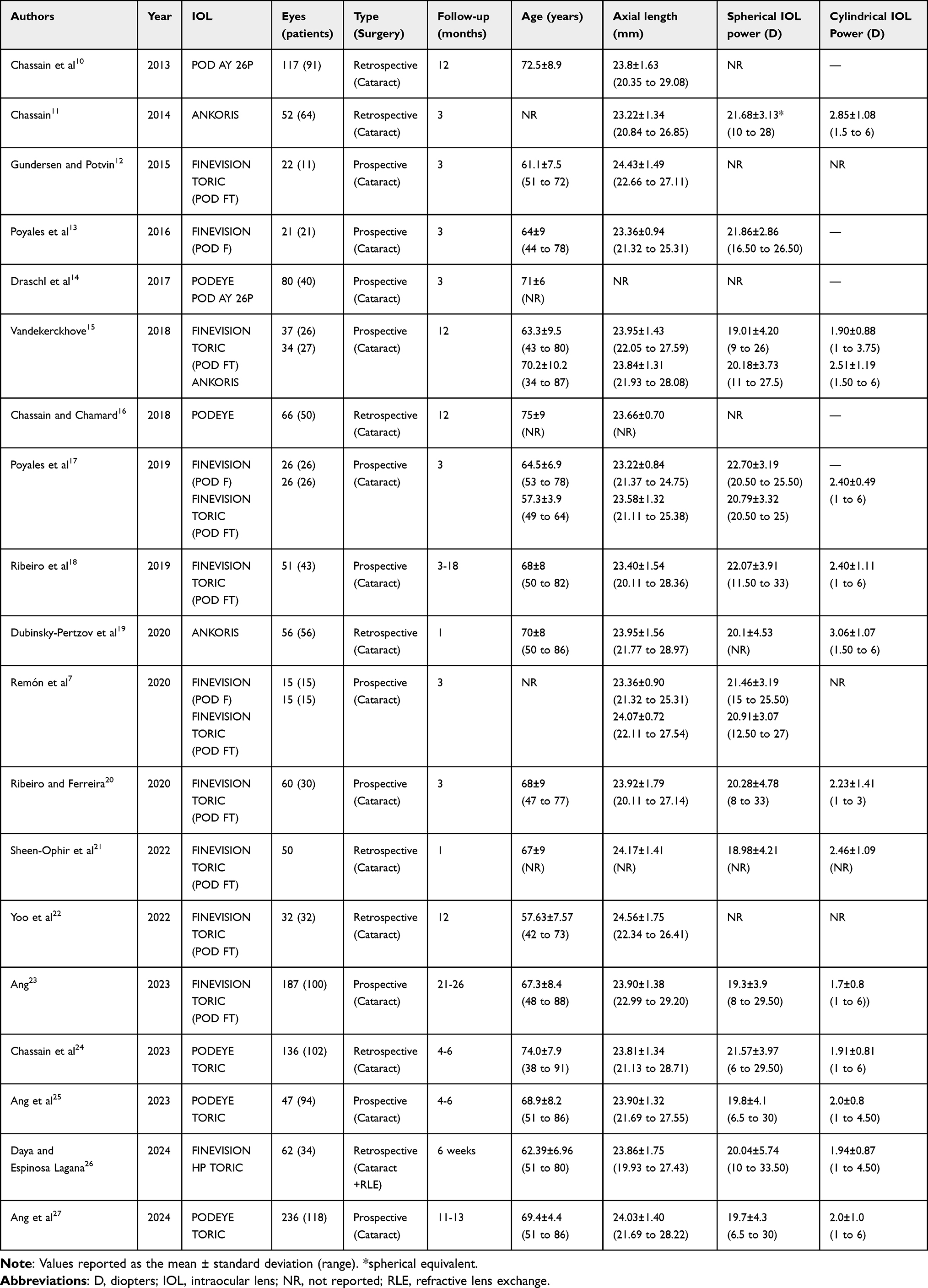 |
Table 2 Peer-Reviewed Clinical Publications Using the POD Platform Reporting Rotational Stability Outcomes |
Ang et al27 included the largest sample of eyes of all the 19 studies, with 236 eyes implanted with the PODEYE TORIC IOL. The study with the longest follow-up period, up to 21 to 26 months was also published by Ang,23 and reported on the FINEVISION TORIC IOL. It should be noted that four studies evaluated two models in the same publication: Draschl et al14 implanted the PODEYE IOL in one eye and the POD AY 26P IOL in the contralateral eye; Vandekerckhove15 evaluated the FINEVISION TORIC and the ANKORIS IOLs in different groups; and both Poyales et al17 and Remón et al7 assessed the FINEVISION and FINEVISION TORIC IOLs, also in different groups.
Collating data from all publications, a total of 1428 eyes were implanted with the POD platform (POD AY 26P IOL: 157 eyes; ANKORIS IOL: 142 eyes; PODEYE IOL: 106 eyes; PODEYE TORIC IOL: 419 eyes; FINEVISION IOL: 62 eyes; FINEVISON TORIC IOL: 480 eyes; and FINEVISION HP TORIC IOL: 62 eyes). The mean axial length across all the studies was 23.80±0.36 mm (range 23.22 mm11,17 to 24.56 mm).22 The average spherical IOL power across all the studies was 20.61±1.12 D, ranging from 18.98 D21 to 22.70 D.17 For toric lenses the mean astigmatic diopter power was 2.25±0.40 D, (ranging from 1.7 D23 to 3.06 D).19
The rotational stability outcomes for all the studies are tabulated (Table 3). In addition to the mean and ranges of rotation values, for each study, where available, the IOL used is indicated as well as the measurement method used to estimate the rotation of the IOL, and the period of time for which the rotation was calculated. There was a wide variety of measurement methods and examination periods. The mean rotation across all the studies was 2.61 °, but the individual rotation values ranged from 1.18 °17 to 5.84 °.26 Note that when two periods in the same study were evaluated the rotation of the lens was the summation of the two. Specifically, Table 4 shows the mean rotation for each IOL model from each individual study along with reference is illustrated in Table 4.
 |
Table 3 Rotational Stability Outcomes |
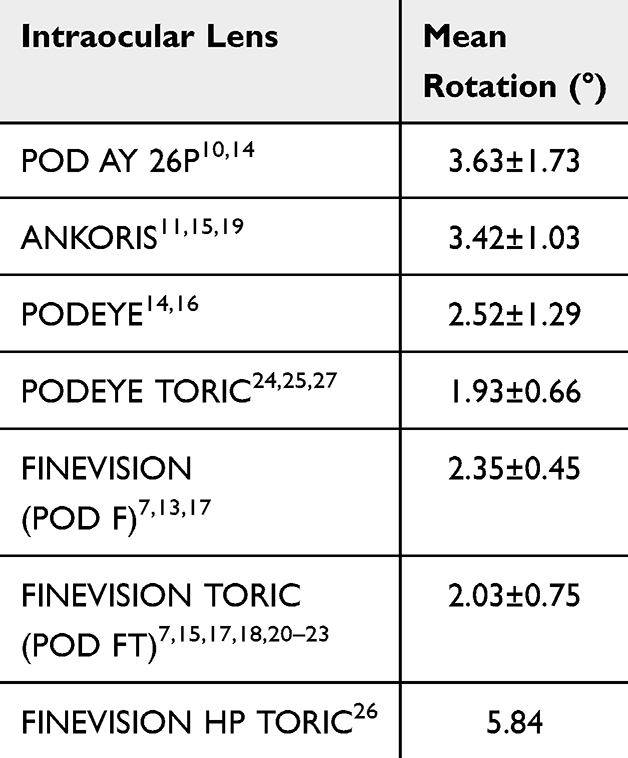 |
Table 4 Mean (± Standard Deviation) Rotational Stability Outcomes as a Function of the Intraocular Lens Model Computed From the Different Studies |
Discussion
As we have mentioned, the stability of an IOL once implanted is a key factor for the refractive success of the surgical procedure. This is especially relevant with toric lenses where minimal rotation if any is desired in order to ensure reliable astigmatic correction and in turn refractive and visual outcome. Increasing expectations of reliable astigmatic correction following use of toric lenses has influenced IOL design to ensure minimal if any rotation.
This review assesses the outcomes and rotational stability of the POD platform with four C loop haptics of a variety of lenses. This metanalysis revealed a mean rotation value 2.61 °. Individual mean rotation values ranged from 1.18 °, reported by Poyales et al17 for the FINEVISION TORIC IOL from the day of surgery to 3 months post-surgery, to 5.84 °, reported by Daya and Espinosa Lagana,26 for the FINEVISION HP TORIC IOL from the intended axis of implantation 6 weeks after the surgery. Note that all the other studies reported mean rotation values of less than 5 ° (see Table 3). The study by Daya and Espinosa Lagana26 was the only one that used internal aberrometry to measure rotation, and, as indicated by these authors, this method is not as accurate as directly observing the lens positioning with a dilated pupil; and highly dependent on the quality of the test performed and prone to error from lens tilt.26 A systematic review and single-arm meta-analysis on the rotational stability of toric IOLs, by Li et al3 found a pooled mean absolute rotation of 2.36 ° (95% CI, 2.08–2.64) for all studies with different lens designs, haptics and materials. The mean rotation for the POD platform is similar. Rotation of 5 ° is considered clinically relevant,28 <10 ° can lead to a minimal to moderate loss of cylindrical correction, with the largest cylindrical correction loss occurring between 10 ° and 20 °;29 ≥45 ° rotation leads to the total loss of cylindrical correction.30 Li et al3 reported that certain haptic designs and lens models exhibit exceptional rotational stability in comparison with others. After analyzing by haptic type, they indicated that loop haptics are more stable than plate-haptics, and double-loop haptics (quad-haptics) and plate loop haptics (closed-loop haptics) have even greater rotational stability than traditional loop haptics. They suggest that the exceptional rotational stability of double-loop haptics may be due to the increased number of contact points between the haptics and the capsular bag, effectively increasing the total friction. The study indicated that the FINEVISION TORIC lens exhibited exceptional rotational stability despite using hydrophilic lens material with its double-loop haptics. The pooled mean absolute rotation for this IOL reported by these authors was 1.53 ° (95% CI, 1.02–2.04). Specifically, in our review the mean value calculated was 2.03 ° (Table 4).
The sub-analysis performed as a function of the specific IOL model also reveals low mean values (see Table 4). Chassain et al10 were the first to assess the POD platform, with the POD AY 26P IOL. They found that the rotation was >5 ° in only one case (5%) and no rotation was >10 ° between 3 weeks and 3 months post-surgery. Furthermore, no rotation >5 ° was observed between 3 months and 1 year. Draschl et al14 analyzed the same lens up to 3 months post-surgery and found a rotation of <3 ° and <6 ° in 20 eyes (71.4%) and 27 eyes (96.4%), respectively. The direction of rotation was clockwise in 7 eyes (25.0%), counterclockwise in 9 eyes (32.1%), and essentially none (±1.5 °) in 12 eyes (42.9%). The mean rotation value for this lens based on these two studies was 3.63 °. Chassain11 was also the first to evaluate the ANKORIS IOL reporting that 96% of eyes had a rotation of <5 ° and 80.6% had ≤3 °; subsequently, in a 12-month follow-up period, Dubinsky-Pertzov et al19 found that the rotation was within 5 ° in 82% of eyes (46 eyes), between 6 and 10 ° in 10.8% of eyes (6 eyes), and between 11 and 13 ° in 7.2% of eyes (4 eyes). Vandekerckhove15 also examined this lens up to 12-months post-surgery, reporting 4 ° of rotation, using the Galilei 6 (Ziemer, Switzerland) to measure this rotation. Combining data from three studies, the mean rotation value for this lens was 3.42 °. The PODEYE lens was analyzed first by Draschl et al14 who found a rotation of <3 ° in 23 eyes (82.1%) and <6 ° in 27 eyes (96.4%). The direction of rotation was clockwise in 2 eyes (32.1%), counterclockwise in 6 eyes (21.4%), and none (±1.5 °) in 20 eyes (71.5%). Over a longer follow-up period, Chassain and Charmand16 found that no lenses case rotated >5 °. The mean rotation value for this lens was 2.52 °. The PODEYE TORIC lens was also assessed by Chassain et al24 who found that more than 85% of eyes rotated ≤3 °, with 58.0% of eyes rotating clockwise rotation and 42.0% of eyes rotated counterclockwise. Two other studies on the same lens supported these good outcomes, with 97.87%25 and 98.56%27 of eyes having a rotation of <10 °. Taking into account the three studies, the mean rotation value for this lens was 1.93 °.
The FINEVISION IOL (non-toric) was evaluated by both Remón et al7 and Poyales et al,13,17 up to 3-months post-surgery. These authors found similar mean values (see Table 3), with the mean rotation value for the three studies being 2.35 °. Specifically, Poyales et al17 observed that at the 24-h post-surgery evaluation, none of the lenses had rotated more than 5 °, whereas at the 3-month follow-up visit, only one lens had exceeded a 5 ° rotation, specifically 6.5 °. This is in line with the outcomes reported by different authors looking at the FINEVISION TORIC IOL (mean rotation value of 2.03 °). The rotation of this lens was analyzed in a number of studies. The first12 reported on only one lens, with a measured change in orientation of 5 ° between 1-day and 1-month post-surgery. In three of the cases, the 1-month postop orientation of the lens was noted to be about 10 ° from the intended axis. A chart review showed a similar but slightly lower alignment error 1-day after surgery, suggesting an alignment error rather than IOL rotation. With these exceptions, no change in lens orientation from 5 ° was measured between the 1- and 3-month visits. Vandekerckhove15 also examined this lens over a longer follow-up period (12-months), reporting about 2.5 ° of rotation measured using the Galilei 6 device. Poyales et al17 Ribeiro et al18,20 and Remón et al7 indicated lower values, 1.18 °, 1.33 °, 1.89 °, and 1.59 ° respectively, using retroilluminated slit-lamp photography. These values are in line with the pooled mean absolute rotation for this IOL reported by Li et al3 (1.53 °). Sheen-Ophir et al21 using the same method but for a short follow-up (1-month), reported a large value (3.52 °) with the following percentage distribution of eyes as a function of rotation: 18% <1 °, 54% 1.5 °, 22% 6–10 °, and 6% >10 °. Yoo et al22 and Ang,23 with longer follow-up periods (12 and 21–26 months), found low values: 2.14 ° and 2.00 °, respectively. Daya and Espinosa Lagana26 are, to date, the only authors to have published outcomes for the FINEVISION HP TORIC lens. The value reported is the highest for this platform (5.84 °) but, as indicated previously, they used internal aberrometry and the reported values were from the intended axis of implantation to 6 weeks after surgery. They found that in 61.3% of eyes the lens had rotated less than 5 °, 29% showed a rotation of between 6 and 10 °, and 9.7% presented a rotation of >10 °. The difference between this model and the FINEVISION TORIC lens is only the material: hydrophobic versus hydrophilic. This contrasts with the reported effect of the material on rotational stability, since greater rotational stability has been observed in hydrophobic acrylic lenses in comparison with hydrophilic acrylic lenses,1 maybe due to increased adhesive strength between the IOL and the capsular bag. Hydrophobic acrylic IOLs exhibit stronger adhesion owing to the charge effect and higher fibronectin content.31 This leads us to suspect that perhaps the high value obtained by these authors is more related to the measurement method than to the lens itself.
Different methodology of measurements by different investigators are a potential source of discrepancy between studies. Rotation can be measured subjectively directly using a slit-lamp, aligning the slit beam with the axis of the lens when the pupil is dilated. Some studies in this review used this method but certain errors are possible, including head tilt at the slit lamp and/or cyclotorsion effects. Notwithstanding, the majority of studies used digital image analysis, which is considered the best method for determining IOL orientation changes.32 Retroilluminated slit-lamp photography was the most common method used in these studies. Another factor that should be kept in mind when comparing studies is the rotation period. The timepoint from which the change in orientation is calculated is crucial. Some authors reported the change from the intended or planned axis,12,21,26 which may be significantly different to the actual implanted axis; some from the day of surgery;5,7,17,19,23–25,27 and others from days or weeks after the operation.10,11,13,16 It has been reported that lens rotation can occur within 1 hour of the surgery, with a large proportion of the rotation occurring within the first 10 days after implantation.33 As the diameter of the capsular bag gradually decreases after cataract surgery, IOL stability increases as the capsular bag contracts.34,35 The dimension of the capsular bag is another influencing factor in IOL rotation.34 However, the inability to readily measure the capsular bag makes it difficult to fully analyze this factor. Other parameters, such as white-to-white or lens thickness, have been used to indirectly estimate the dimension of the capsule to find a correlation with IOL rotation, but without a clear consensus.34 The same is true of axial length, which has traditionally been considered to be an important factor contributing to the early postoperative rotation of lenses after cataract surgery,33,36,37 but no significant correlation has been found between axial length and rotation in other studies.38–40 Note that the anterior segment length, which can be considered the sum of anterior chamber depth and lens thickness, may play a direct role instead directly the whole axial length. The mean values for axial length in the studies analyzed in our review (see Table 2) were about 23–24 mm. It should be noted, for example, that Chassain et al24 found good rotational stability for the PODEYE TORIC IOLs, even for the 25% of eyes with an axial length greater than 24.5 mm. Continuous curvilinear capsulorhexis (CCC) is also a factor, in this case related to the surgery, that has been analyzed.34 It has previously been reported that the size of the capsulorhexis could influence rotational stability, and a maximum of 5.8 mm was suggested to improve IOL stability.41 A recent study evaluating rotational stability with and without primary posterior CCC over a 1-year period in 112 eyes concluded that primary posterior CCC slightly reduced IOL rotation in the early postoperative period; this can be attributed to accelerated capsular fusion.42
Conclusions
This manuscript reviews the rotational stability outcomes of the POD platform. The clinical results reported in the peer-reviewed literature suggest that this platform model with double C-loop haptics provides good rotational stability when used with different IOL models based on monofocal and trifocal designs and made using hydrophilic or hydrophobic material. Future research on this platform should involve the hydrophobic toric trifocal lens as well as larger samples and longer follow-up periods and also to evaluate the role of different parameters such as axial length and anterior chamber depth (long and short eyes).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
Disclosure
Sheraz Daya reports grant support from Allotex and Johnson & Johnson Vision; consultant/advisor of, lecture fees, and grant support from Bausch + Lomb; consultant/advisor of and lecture fees from BVI–Physiol; consultant/advisor of Cristalens, Carl Zeiss Meditec, Nidek, Inc., Oyster Point, Tarsus, and Vialase; consultant/advisor of, stock options, grant support from Excellens; owner of company of Infinite Medical Ventures (EO); consultant/advisor for and stock options from PRN.
Christophe Chassain receives royalties by the company BVI–Physiol concerning PODEYE IOLs.
Christophe Pagnoulle has a proprietary interest in the GF material. Dr. Pagnoulle is an employee of BVI Medical.
Dr Christophe Pagnoulle has a patent US8636796B2 issued to Physiol SA, a patent BE1016383A3 issued to Physiol SA.
The authors report no other conflicts of interest in this work.
References
1. Kaur M, Shaikh F, Falera R, Titiyal JS. Optimizing outcomes with toric intraocular lenses. Indian J Ophthalmol. 2017;65:1301–1313. doi:10.4103/ijo.IJO_810_17
2. Patnaik JL, Kahook MY, Berdahl JP, et al. Association between axial length and toric intraocular lens rotation according to an online toric back-calculator. Int J Ophthalmol. 2022;15:420–425. doi:10.18240/ijo.2022.03.08
3. Li ES, Vanderford EK, Xu Y, Kang PC. Rotational stability of toric intraocular lenses by lens model and haptic design: systematic review and single-arm meta-analysis. J Cataract Refract Surg. 2024;50(9):976–984. doi:10.1097/j.jcrs.0000000000001486
4. Wu J, Yang C, Yin Y, Liu L, Wang H. Impact of material and lens design on repositioning surgery of toric intraocular lenses: a single-arm meta-analysis. J Ophthalmol. 2022;6699596. doi:10.1155/2022/6699596
5. Bozukova D, Pagnoulle C, Jérôme C. Biomechanical and optical properties of 2 new hydrophobic platforms for intraocular lenses. J Cataract Refract Surg. 2013;39(9):1404–1414. doi:10.1016/j.jcrs.2013.01.050
6. Bozukova D, Werner L, Mamalis N, et al. Double-C loop platform in combination with hydrophobic and hydrophilic acrylic intraocular lens materials. J Cataract Refract Surg. 2015;41(7):1490–1502. doi:10.1016/j.jcrs.2014.10.042
7. Remón L, Cabeza-Gil I, Calvo B, Poyales F, Garzón N. Biomechanical stability of three intraocular lenses with different haptic designs: in silico and in vivo evaluation. J Refract Surg. 2020;36(9):617–624. doi:10.3928/1081597X-20200713-02
8. Cabeza-Gil I, Frechilla J, Calvo B. Evaluation of the mechanical stability of intraocular lenses using digital image correlation. Sci Rep. 2023;13(1):9437. doi:10.1038/s41598-023-36694-0
9. International Organization for Standardization. 11979-2 IF. Ophthalmic implants-Intraocular lenses. Part 2: optical properties and test methods. 2014.
10. Chassain C, Pagnoulle C, Gobin L, Rozema J. Évaluation d’une nouvelle plateforme d’implant intraoculaire: centrage et stabilité rotatoire [Evaluation of a new intraocular lens platform: centration and rotational stability]. J Fr Ophtalmol. 2013;36(4):336–342. doi:10.1016/j.jfo.2012.04.012
11. Chassain C. Évaluation des performances visuelles après implantation d’une lentille intraoculaire torique à double anse en C [Evaluation of visual performance after implantation of a double C-Loop toric intraocular lens]. J Fr Ophtalmol. 2014;37(7):507–513. doi:10.1016/j.jfo.2014.02.007
12. Gundersen KG, Potvin R. Comparison of visual outcomes after implantation of diffractive trifocal toric intraocular lens and a diffractive apodized bifocal toric intraocular lens. Clin Ophthalmol. 2016;10:455–461. doi:10.2147/OPTH.S103375
13. Poyales F, Garzón N, Rozema JJ, Romero C, de Zárate BO. Stability of a novel intraocular lens design: comparison of two trifocal lenses. J Refract Surg. 2016;32(6):394–402. doi:10.3928/1081597X-20160428-04
14. Draschl P, Hirnschall N, Luft N, et al. Rotational stability of 2 intraocular lenses with an identical design and different materials. J Cataract Refract Surg. 2017;43(2):234–238. doi:10.1016/j.jcrs.2016.12.011
15. Vandekerckhove K. Rotational stability of monofocal and trifocal intraocular toric lenses with identical design and material but different surface treatment. J Refract Surg. 2018;34(2):84–91. doi:10.3928/1081597X-20171211-01
16. Chassain C, Chamard C. Performances visuelles, glistening et opacification capsulaire postérieure: 3 ans après l’implantation d’un nouvel implant hydrophobe [Posterior capsule opacification, glistenings and visual outcomes: 3 years after implantation of a new hydrophobic IOL]. J Fr Ophtalmol. 2018;41(6):513–520. doi:10.1016/j.jfo.2017.11.022
17. Poyales F, Garzón N, Pizarro D, Cobreces S, Hernández A. Stability and visual outcomes yielded by three intraocular trifocal lenses with same optical zone design but differing material or toricity. Eur J Ophthalmol. 2019;29(4):417–425. doi:10.1177/1120672118795065
18. Ribeiro FJ, Ferreira TB, Relha C, Esteves C, Gaspar S. Predictability of different calculators in the minimization of postoperative astigmatism after implantation of a toric intraocular lens. Clin Ophthalmol. 2019;13:1649–1656. doi:10.2147/OPTH.S213132
19. Dubinsky-Pertzov B, Hecht I, Gazit I, et al. Clinical outcomes of Ankoris toric intraocular lens implantation using a computer-assisted marker system. Int Ophthalmol. 2020;40(12):3259–3267. doi:10.1007/s10792-020-01511-4
20. Ribeiro FJ, Ferreira TB. Comparison of visual and refractive outcomes of 2 trifocal intraocular lenses. J Cataract Refract Surg. 2020;46(5):694–699. doi:10.1097/j.jcrs.0000000000000118
21. Sheen-Ophir S, Reitblat O, Levy A, Assia EI, Kleinmann G. Deviation from the planned axis of three toric intraocular lenses. Sci Rep. 2022;12(1):13760. doi:10.1038/s41598-022-17811-x
22. Yoo YS, Paik DW, Lim DH, Chung TY. One-year long-term clinical outcomes following diffractive trifocal toric intraocular lens implantation: retrospective observational case series study. Ann Transl Med. 2022;10(21):1159. doi:10.21037/atm-22-1007
23. Ang RET. Long-term trifocal toric intraocular lens outcomes in Asian eyes after cataract surgery. J Cataract Refract Surg. 2023;49(8):832–839. doi:10.1097/j.jcrs.0000000000001195
24. Chassain C, Hallak MK, Lesaffre M. Rotational stability and clinical outcomes after implantation of a new monofocal toric intraocular lens with double C-loop design. J Fr Ophtalmol. 2023;46(6):571–580. doi:10.1016/j.jfo.2022.07.005
25. Ang RET, Tañá-Rivero P, Pastor-Pascual F, Stodulka P, Tetz M, Fischinger I. Visual and refractive outcomes after bilateral implantation of a biconvex aspheric toric monofocal intraocular with a double c-loop haptic design. Clin Ophthalmol. 2023;17:2765–2776. doi:10.2147/OPTH.S432598
26. Daya S, Espinosa Lagana M. Visual and refractive outcomes of a new hydrophobic trifocal toric intraocular lens. Clin Ophthalmol. 2024;18:997–1007. doi:10.2147/OPTH.S453565
27. Ang RET, Tañá-Rivero P, Pastor-Pascual F, et al. One-year clinical outcomes following aspheric toric monofocal iol with a double c-loop haptic design implantation. Clin Ophthalmol. 2024;18:3515–3525. doi:10.2147/OPTH.S494313
28. Hahn U, Krummenauer F, Schmickler S, Koch J. Rotation of a toric intraocular lens with and without capsular tension ring: data from a multicenter non-inferiority randomized clinical trial (RCT). BMC Ophthalmol. 2019;19:143. doi:10.1186/s12886-019-1147-5
29. Németh G. One degree of misalignment does not lead to a 3.3% effect decrease after implantation of a toric intraocular lens. J Cataract Refract Surg. 2020;46:482. doi:10.1097/j.jcrs.0000000000000079
30. Tognetto D, Perrotta AA, Bauci F, et al. Quality of images with toric intraocular lenses. J Cataract Refract Surg. 2018;44:376–381. doi:10.1016/j.jcrs.2017.10.053
31. Sun J, Bai H, Cui W, et al. Comparison of clinical outcome after implantation of two toric intraocular lenses with different haptic type: a prospective randomized controlled trial. Graefes Arch Clin Exp Ophthalmol. 2024;262:847–855. doi:10.1007/s00417-023-06232-9
32. Sandoval HP, Lane S, Slade S, Donnenfeld ED, Potvin R, Solomon KD. Evaluating rotational stability of an extended depth of focus toric intraocular lens using a slit lamp and image-based analysis. Clin Ophthalmol. 2020;14:2405–2410. doi:10.2147/OPTH.S272240
33. Miyake T, Kamiya K, Amano R, Iida Y, Tsunehiro S, Shimizu K. Long-term clinical outcomes of toric intraocular lens implantation in cataract cases with preexisting astigmatism. J Cataract Refract Surg. 2014;40:1654–1660. doi:10.1016/j.jcrs.2014.01.044
34. Lin X, Ma D, Yang J. Insights into the rotational stability of toric intraocular lens implantation: diagnostic approaches, influencing factors and intervention strategies. Front Med. 2024;11:1349496. doi:10.3389/fmed.2024.1349496
35. Kim JH, Lee D, Cha YD, Oh SH, Mah KC, Lee MS. The analysis of predicted capsular bag diameter using modified model of capsule measuring ring in Asians. Clin Exp Ophthalmol. 2008;36(3):238–244. doi:10.1111/j.1442-9071.2008.01726.x
36. Shah GD, Praveen MR, Vasavada AR, Vasavada VA, Rampal G, Shastry LR. Rotational stability of a toric intraocular lens: influence of axial length and alignment in the capsular bag. J Cataract Refract Surg. 2012;38:54–59. doi:10.1016/j.jcrs.2011.08.028
37. Zhu X, He W, Zhang K, Lu Y. Factors influencing 1-year rotational stability of acrysof toric intraocular lenses. Br J Ophthalmol. 2016;100:263–268. doi:10.1136/bjophthalmol-2015-306656
38. Zhu X, Meng J, He W, Rong X, Lu Y. Comparison of the rotational stability between plate-haptic toric and c-loop haptic toric IOLs in myopic eyes. J Cataract Refract Surg. 2020;46:1353–1359. doi:10.1097/j.jcrs.0000000000000259
39. He S, Chen X, Wu X, Ma Y, Yu X, Xu W. Early-stage clinical outcomes and rotational stability of tecnis toric intraocular lens implantation in cataract cases with long axial length. BMC Ophthalmol. 2020;20:204. doi:10.1186/s12886-020-01465-2
40. Tataru CP, Dogaroiu AC, Tataru CI, Dogaroiu C. Enhancing rotational stability of toric intraocular lenses using a type 2l cionni capsular tension ring in patients with high myopia. J Cataract Refract Surg. 2019;45:1219–1221. doi:10.1016/j.jcrs.2019.05.045
41. Li S, Li X, He S, et al. Early postoperative rotational stability and its related factors of a single-piece acrylic toric intraocular lens. Eye. 2020;34:474–479. doi:10.1038/s41433-019-0521-0
42. Huang Y, Yu M, Liu X, Cai Y, Kang C, Wu W. Intraocular lens rotational stability after cataract surgery with and without primary posterior continuous curvilinear capsulorrhexis. J Cataract Refract Surg. doi:10.1097/j.jcrs.0000000000001579
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Visual and Refractive Outcomes After Bilateral Implantation of a Biconvex Aspheric Toric Monofocal Intraocular with a Double C-Loop Haptic Design
Ang RET, Tañá-Rivero P, Pastor-Pascual F, Stodulka P, Tetz M, Fischinger I
Clinical Ophthalmology 2023, 17:2765-2776
Published Date: 20 September 2023
Rotational Stability After Implantation of an Aspheric Toric Monofocal IOL with a Double C-Loop Haptic Design in Normal and High Axial Lengths
Ang RET, Tañá-Rivero P, Pastor-Pascual F, Stodulka P, Slovak M, Tetz M, Fischinger I, Cazal J, Gessa M, Ibarz-Barberá M, Holland D, Groneberg T
Clinical Ophthalmology 2025, 19:2393-2403
Published Date: 19 July 2025