")
Back to Journals » Journal of Inflammation Research » Volume 18
Dual Targeting of Inflammatory and Immune Checkpoint Pathways to Overcome Radiotherapy Resistance in Esophageal Squamous Cell Carcinoma
Authors Qu Z, Shi L, Wang P , Zhao A, Zheng X, Yin Q
Received 28 March 2025
Accepted for publication 8 July 2025
Published 12 July 2025 Volume 2025:18 Pages 9091—9106
DOI https://doi.org/10.2147/JIR.S531145
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Felix Marsh-Wakefield
Zhifeng Qu,1 Linlin Shi,2 Pei Wang,1 Anshun Zhao,2 Xuewei Zheng,3 Qinan Yin1,3
1Department of Radiation Oncology; Cancer Institute, The First Affiliated Hospital, and College of Clinical Medicine of Henan University of Science and Technology, Luoyang, People’s Republic of China; 2Henan Key Laboratory of Microbiome and Esophageal Cancer Prevention and Treatment; Henan Key Laboratory of Cancer Epigenetics; College of Basic Medicine and Forensic Medicine, Cancer Hospital, The First Affiliated Hospital, and College of Clinical Medicine of Henan University of Science and Technology, Luoyang, People’s Republic of China; 3Precision Medicine Laboratory, School of Medical Technology and Engineering, Henan University of Science and Technology, Luoyang, People’s Republic of China
Correspondence: Qinan Yin, Department of Radiation Oncology; Cancer Institute, The First Affiliated Hospital, and College of Clinical Medicine of Henan University of Science and Technology, No. 636, Guanlin Avenue, Luoyang, 471003, People’s Republic of China, Email [email protected] Xuewei Zheng Precision Medicine Laboratory, School of Medical Technology and Engineering, Henan University of Science and Technology, No. 263, Kaiyuan Avenue, Luoyang, 471000, People’s Republic of China, Email [email protected]
Abstract: Esophageal squamous cell carcinoma (ESCC) is characterized by chronic inflammation, immune evasion, and resistance to RT. Inflammatory pathways such as nuclear factor-kappa B (NF-κB) and signal transducer and activator of transcription 3 (STAT3), and cyclooxygenase 2 (COX-2) promote tumor progression and reduce radiosensitivity. RT activates pro-inflammatory cytokines and upregulates immune checkpoints including programmed death 1 (PD-1) and cytotoxic T-lymphocyte–associated antigen 4 (CTLA-4), which contribute to immune suppression and treatment failure. Dual targeting of inflammatory and immune checkpoint pathways has shown potential to reverse radio resistance and enhance therapeutic response. Inhibition of COX-2 can reduce inflammation and improve tumor control, while blockade of PD-1 can restore T cell function and promote antitumor immunity. Strategies that integrate anti-inflammatory components, immune checkpoint inhibitors (ICIs), and RT guided by molecular profiling may improve treatment outcomes in ESCC. This review focuses on the biological basis of inflammation-mediated radio resistance and presents dual targeting approaches as promising options to overcome current therapeutic limitations.
Keywords: esophageal squamous cell carcinoma, inflammation, radiotherapy (RT) resistance
Introduction
ESCC remains an aggressive malignancy with poor prognosis despite advances in early detection and multimodal treatments. Chronic inflammation, tumor microenvironment (TME), and resistance to RT contribute to its complexity, necessitating novel therapeutic strategies to improve patient outcomes.1
Inflammation is a key driver of ESCC progression, fueled by exposure to environmental carcinogens such as tobacco, alcohol, and dietary irritants. This results in oxidative stress, cytokine secretion, and immune cell infiltration, activating oncogenic pathways including NF-κB, STAT3, and COX-2/PGE2, which collectively promote tumor growth, immune evasion, and genomic instability.2 The inflammatory milieu fosters an immunosuppressive TME, further contributing to therapy resistance.3
RT influences the immune milieu through context-dependent pro-inflammatory and anti-inflammatory mechanisms that shape therapeutic outcomes in ESCC.4,5 Combining RT with immunotherapy offers a promising strategy to overcome resistance. RT induces ICD, enhancing antigen presentation and dendritic cell recruitment, thereby activating cytotoxic T cells.6,7 However, RT also upregulates immune checkpoint molecules such as PD-1 and programmed death ligand 1 (PD-L1), leading to T cell exhaustion and therapy resistance.8 Integrating RT with ICIs has demonstrated synergistic effects, restored T cell function, and improved tumor control.9 Targeting TME modulators such as transforming growth factor-beta (TGF-β) and VEGF further enhances RT response by counteracting immunosuppression and facilitating immune infiltration.10
Beyond ICIs, anti-inflammatory factors such as NSAIDs and COX-2 inhibitors are being explored as radiosensitizers in ESCC, as they attenuate RT-induced inflammation and suppress tumor-promoting pathways.11,12 Additionally, metabolic adaptations within the TME contribute to radio resistance, with alterations in glucose and lipid metabolism supporting tumor survival. Inhibiting glycolysis, glutaminolysis, or lipid biosynthesis represents a potential strategy to improve RT efficacy.13,14
Advancements in biomarker-driven and AI-assisted RT planning offer further opportunities to optimize ESCC treatment.15,16 Identifying predictive biomarkers, such as circulating inflammatory cytokines, immune cell profiles, and radio resistance signatures, will facilitate patient stratification and therapy selection.17 Integrating RT with novel therapies targeting inflammation, the TME, and metabolic pathways has the potential to improve clinical outcomes.18,19
ESCC remains a challenging malignancy due to its aggressive progression and resistance mechanisms driven by inflammation and RT. While RT remains fundamental, its efficacy is often limited by inflammatory responses and an immunosuppressive TME. Emerging approaches, including RT-ICI combinations, TME-targeting therapies, and metabolic inhibitors, offer promising avenues for enhancing therapeutic responses. A deeper understanding of these intricate interactions will be essential for developing personalized treatment strategies that improve survival and quality of life for ESCC patients.20–22 Inflammation-mediated radio resistance in ESCC is shaped by RT dose and fractionation. Hyperfractionation can reduce IL-6 and suppress pro-inflammatory signaling,23,24 while stereotactic RT may increase TGF-β and other immunosuppressive mediators,25 suggesting a dose-dependent inflammatory modulation relevant for treatment design. Stereotactic body radiation therapy (SBRT) has also been found to be associated with elevated TGF-β expression and an immunosuppressive TME.26–28 In Asian ESCC populations, IL-1β polymorphisms associated with betel quid exposure have been linked to chronic inflammation and elevated cancer risk,29 highlighting the need for population-adapted anti-inflammatory approaches. Concurrently, metabolic reprogramming in ESCC, including upregulation of fatty acid synthase (FASN), glucose transporter 1 (GLUT1), and sterol regulatory element-binding protein 1 (SREBP1), contributes to radio resistance and offers potential targets for radio sensitization.22,30,31 These mechanistic insights align with recent Phase II clinical trials investigating RT combined with ICIs in ESCC, which show promising clinical activity.32,33 These studies report improved response rates and progression-free survival, supporting the feasibility of dual targeting strategies.
Here, this review focuses on the ESCC-specific mechanisms by which inflammation drives radio resistance and highlights therapeutic strategies centered on dual targeting of inflammatory and immune checkpoint pathways as a promising approach to enhance RT efficacy and outcomes.
Inflammation in ESCC Development and Progression
Inflammation is a fundamental driver of ESCC initiation, progression, and resistance to therapy. Chronic inflammation, exacerbated by infections, environmental exposures, and dysregulated immune responses, establishes a tumor-promoting microenvironment that facilitates malignant transformation. Recent studies have provided deeper insights into the molecular mechanisms underlying inflammation in ESCC, highlighting novel therapeutic targets and biomarkers.
Inflammation as a Hallmark of Cancer
Chronic inflammation is a well-established hallmark of cancer, playing a critical role in ESCC pathogenesis. Persistent inflammatory stimuli induce DNA damage, genomic instability, and the activation of oncogenic pathways, collectively driving tumorigenesis. In ESCC, chronic inflammation is frequently triggered by infections, including human papillomavirus (HPV) and Helicobacter pylori, as well as environmental factors such as tobacco smoking, alcohol consumption, and dietary carcinogens.34 These factors generate a pro-inflammatory microenvironment that facilitates the transformation of normal esophageal epithelial cells into malignant counterparts.
HPV infection has been linked to ESCC.35 It has been demonstrated that HPV oncoproteins E6 and E7 disrupt key cellular regulatory mechanisms, notably the p53 and Rb pathways, leading to uncontrolled cell proliferation and immune evasion.36,37 Similarly, H. pylori, historically associated with gastric cancer.38 However, recent findings indicate HPV16E6 infection drives an inflammatory TME in ESCC by inducing M2 macrophage polarization, which enhances tumor invasion and metastasis through increased MMP-9 expression.39
Environmental carcinogens further exacerbate chronic inflammation and enhance ESCC progression.40 Tobacco smoke generates oxidative stress and DNA damage, thereby activating key inflammatory signaling pathways such as NF-κB, which support tumor cell survival, proliferation, and angiogenesis.41–45 Additionally, dietary carcinogens, including nitrosamines found in preserved foods, contribute to the inflammatory microenvironment that fosters ESCC development.46 These findings underscore the multifactorial nature of ESCC and the pivotal role of inflammation in its pathophysiology.
Key Inflammatory Pathways in ESCC
The NF-κB pathway is a critical regulator of inflammation and a major driver of ESCC progression. Activated by pro-inflammatory cytokines, infections, and environmental stressors, NF-κB orchestrates the transcription of genes that promote cell survival, proliferation, and immune evasion (Figure 1A).47
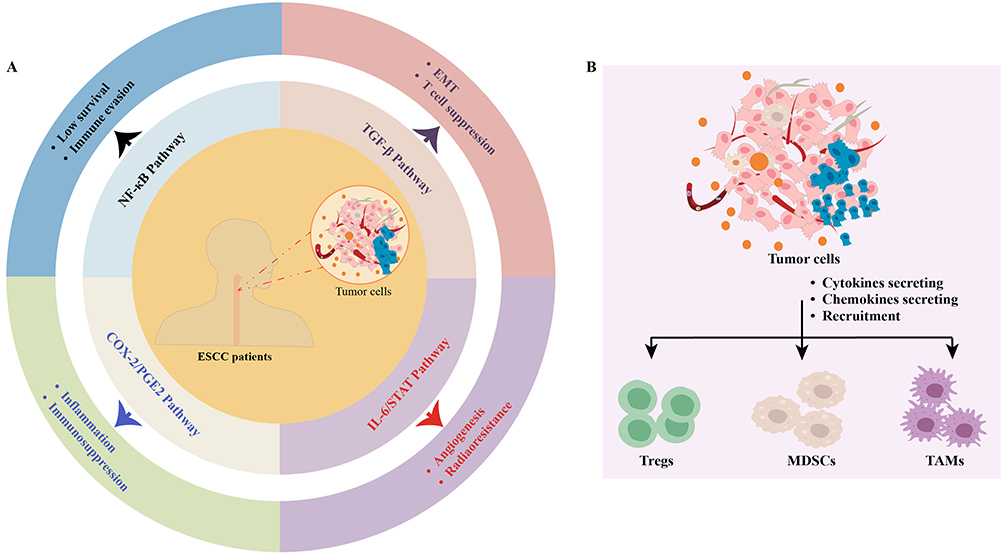 |
Figure 1 Key Inflammatory Pathways in ESCC. (A) Schematic illustration of key inflammation-related signaling pathways contributing to ESCC progression. Chronic inflammatory stimuli activate pathways such as NF-κB, IL-6/STAT3, COX-2/PGE2, and TGF-β, which promote tumor survival, immune evasion, angiogenesis, EMT, and resistance to therapy. These interconnected pathways establish a tumor-promoting and immunosuppressive microenvironment in ESCC; (B) Tumor cells secrete cytokines and chemokines that recruit TAMs, Tregs, and MDSCs, collectively enhancing tumor growth and facilitating immune evasion. |
Recent study revealed that NF-κB is constitutively activated in ESCC, upregulating cytokines such as TNF-α, which further sustain chronic inflammation.48 NF-κB also interacts with other oncogenic pathways, including STAT3 and COX-2, forming a pro-tumorigenic signaling network. The JAK/STAT3 pathway promotes ESCC progression by driving cancer-related inflammation through crosstalk with NF-κB and COX-2, highlighting STAT3 as a potential therapeutic target.49 PAR1 promotes ESCC progression through FAK/PI3K/AKT/STAT3/NF-κB signaling, while PAR4 inhibits tumor growth via nSMase2/MAPK/NF-κB, highlighting NF-κB and STAT3 as key regulators in ESCC pathogenesis.50
The STAT3 pathway is another key regulator of inflammation in ESCC, linking chronic inflammatory signals to tumor progression and immune suppression (Figure 1A). MEK inhibition in ESCC induces STAT3 activation through SOCS3 downregulation, linking inflammation to tumor progression and therapy resistance.51 High STAT3β expression in ESCC enhances sensitivity to platinum-based chemoradiotherapy (CRT) by upregulating the TNF signaling and necrotic cell death pathways, linking STAT3-mediated inflammation to treatment response.52 TGFβ-induced LAMC1 upregulation in ESCC activates Akt–NF-κB–MMP9/14 signaling to promote tumor progression while enhancing CXCL1 secretion, which drives inflammatory cancer-associated fibroblast (CAF) formation through CXCR2–pSTAT3 signaling.53 Additionally, extracellular vesicle-loaded IL-32 from ESCC cells is internalized by macrophages, inducing M2 polarization through the FAK-STAT3 pathway and promoting an inflammatory TME that drives metastasis.54 Given its pivotal role in linking chronic inflammation to tumor progression and therapeutic resistance, STAT3 represents a critical target for disrupting inflammatory pathways that sustain ESCC malignancy.
The COX-2/PGE2 pathway is another significant contributor to inflammation-driven carcinogenesis in ESCC (Figure 1A). COX-2 is frequently overexpressed in ESCC tissues and correlates with poor prognosis. PGE2, through its EP2 receptor, transactivates EGFR in ESCC cells, promoting inflammation-driven tumor progression by enhancing cell proliferation, invasion, and the secretion of pro-inflammatory cytokines via the COX-2/PGE2 axis.55 Negative COX-2 expression in ESCC is linked to reduced tumor-associated inflammation, enhanced radiosensitivity, and improved treatment response, underscoring the role of the COX-2/PGE2 axis in modulating inflammation-driven resistance to RT.56 Moreover, AHR promotes ESCC progression by activating the COX-2/PGE2/STAT3 axis, and its inhibition via genetic knockdown or DIM treatment suppresses tumor growth, migration, and inflammation-driven tumor progression.57
Cytokines such as IL-6 and IL-10 further reinforce the inflammatory microenvironment in ESCC. IL-6 promotes ESCC progression and inflammation through EGFR signaling, where MSA-mediated upregulation of miR-146a suppresses EGFR expression, subsequently reducing IL-6 secretion and disrupting the inflammatory TME in an IL-6-dependent manner.58 IL-6 also promotes ESCC progression and inflammation by activating STAT3 signaling (Figure 1A), which upregulates NANOG expression, thereby enhancing cancer cell proliferation, invasion, and stemness through the induction of downstream oncogenic targets.59 Likewise, IL-10 promotes inflammation and immune evasion in ESCC by upregulating PD-L1 and Met signaling, creating an immunosuppressive TME that enhances tumor progression, while targeting IL-10 in combination with PD-L1 blockade may offer a potential therapeutic strategy.60 In addition, IL-10 contributes to immune evasion in ESCC by interacting with the INPP5A/HLA-G1/MMP-21 regulatory network, promoting an immunosuppressive microenvironment that facilitates tumor progression and inflammation-mediated carcinogenesis.61
The dynamic interaction between immune cells and cancer cells within the ESCC microenvironment significantly influences tumor progression. Tumor cells have been shown to secrete cytokines and chemokines that recruit immunosuppressive immune cells, including TAMs, Tregs, and MDSCs (Figure 1B), collectively enhancing tumor growth and facilitating immune evasion.62 For instance, TAMs produce IL-10 and TGF-β, suppressing cytotoxic T cell activity and enhancing angiogenesis.63 Similarly, TAMs drive ESCC progression by secreting the chemokine CCL22, which activates CCR4-mediated FAK/AKT signaling, fostering an inflammatory TME that promotes malignancy and therapy resistance.64 Those pathways (Table 1) orchestrate inflammation-driven ESCC progression by promoting tumor proliferation, immune suppression, metastasis, and therapy resistance, making them critical targets for disrupting inflammation-mediated carcinogenesis. The major inflammation-related pathways involved in ESCC progression and radio resistance are illustrated in Figure 1.
 |
Table 1 Key Inflammatory Pathways in ESCC |
Inflammatory Biomarkers in ESCC
C-reactive protein (CRP) is a systemic inflammatory biomarker that has been correlated with poor prognosis in ESCC patients. Elevated CRP levels have been significantly correlated with advanced tumor stage, lymph node metastasis, and reduced overall survival in ESCC.65 CRP production is driven by IL-6, further emphasizing the impact of systemic inflammation on ESCC progression.66 IL-6 and IL8 not only activates oncogenic pathways such as STAT3 but also drives systemic inflammation and immune suppression, promoting tumor aggressiveness and metastasis.67,68 The neutrophil-to-lymphocyte ratio (NLR) serves as an indicator of immune dysregulation, predicting poor prognosis and resistance to therapy.69 Additionally, LAMC1 serves as a potential biomarker and therapeutic target in ESCC by promoting tumor proliferation and migration via Akt–NFκB–MMP9/14 signaling and inducing an inflammatory TME through CXCL1-mediated iCAF formation.53 Moreover, IL-1β-driven chronic inflammation promotes ESCC development in L2-IL-1β transgenic mice, characterized by increased inflammatory biomarkers, including T cell infiltration, iNOS, and pro-inflammatory cytokines, highlighting IL-1β as a key mediator in ESCC pathogenesis.70 IL-10 also modulates the immunosuppressive microenvironment in ESCC by downregulating PD-L1 expression via the Met signaling pathway, highlighting IL-10 as a key inflammation biomarker in ESCC pathogenesis.60 Hypomethylation-driven upregulation of PLCE1 activates the NF-κB signaling pathway in ESCC, promoting angiogenesis and tumor progression, highlighting PLCE1 as a key inflammation biomarker and potential therapeutic target.71 Peripheral blood VEGF and inflammation biomarkers (CLR and GPS) serve as key predictors of clinical response and prognosis in non-operative ESCC, providing a reliable inflammation-based biomarker model for patient evaluation.72 These biomarkers (Table 2) not only provide mechanistic insights into ESCC but also represent potential therapeutic targets and prognostic indicators, guiding personalized treatment strategies.
 |
Table 2 Inflammation-Related Biomarkers in ESCC |
RT in ESCC
RT is a cornerstone in the treatment of ESCC, utilized in neoadjuvant, definitive, and palliative settings. Despite its effectiveness, RT faces significant challenges, including tumor resistance and its impact on the TME. Advancements in the understanding of RT-induced tumor cell death, immunomodulation, and resistance have facilitated the development of optimized strategies to enhance therapeutic efficacy and improve patient outcomes.
RT as a Standard Treatment for ESCC
RT is employed across multiple treatment settings in ESCC. In the neoadjuvant setting, RT is frequently combined with chemotherapy to reduce tumor burden and enhance surgical resectability.73 Neoadjuvant CRT has been shown to significantly improve survival in locally advanced ESCC, leading to improved long-term outcomes.74 The definitive RT, often in combination with chemotherapy, serves as a primary treatment approach for patients who are ineligible for surgery. In advanced or metastatic ESCC, palliative RT is utilized to relieve symptoms such as dysphagia and pain.75
The efficacy and safety of RT are influenced by dose fractionation strategies. Conventional fractionation involves daily doses of 1.8–2.0 Gy, with a total dose of 50–60 Gy administered over 5–6 week.76 Hypofractionated radiotherapy (HFRT), delivering higher doses per fraction over a shorter treatment duration, has gained attention for its potential to improve tumor control while reducing treatment time.77 HFRT has been shown to enhance local tumor control in ESCC while maintaining an acceptable toxicity profile.78 Adaptive RT, which tailors treatment based on tumor response, has also emerged as a promising strategy to minimize radiation exposure to healthy tissues.79
RT-Induced Effects on Cancer and the TME
RT exerts its anti-tumor effects primarily by inducing DNA damage, leading to tumor cell death through apoptosis, necrosis, or mitotic catastrophe. Double-strand breaks (DSBs) represent the most lethal form of DNA damage, with repair mediated by pathways such as non-homologous end joining (NHEJ) and homologous recombination (HR).80 RT-induced double-strand breaks activate the ATM/ATR pathway, coordinating DNA repair and cell cycle arrest. However, cancer cells frequently exploit these repair mechanisms to evade RT-induced lethality, contributing to treatment resistance.81
Beyond direct cytotoxicity, RT influences the immune response, making it a potential ally in immunotherapy. Radiation-induced ICD plays a key role in stimulating anti-tumor immunity by releasing damage-associated molecular patterns (DAMPs) such as calreticulin and ATP, which activate dendritic cells (DCs) and enhance T cell-mediated tumor eradication.82 RT-induced immunogenic cell death has been associated with improved survival outcomes in ESCC patients receiving immunotherapy.83 RT also facilitates tumor antigen release, allowing DCs to present antigens to T cells and generate a systemic immune response.84 This phenomenon, known as the abscopal effect, has been observed in ESCC patients treated with RT in combination with ICIs.85 However, RT can also induce immune suppression by upregulating PD-L1 and CTLA-4 expression in the TME, thereby limiting its immunostimulatory effects.86,87
Limitations and Resistance Mechanisms
Hypoxia is a major factor contributing to RT resistance in ESCC. Tumor hypoxia reduces the generation of reactive oxygen species (ROS), which are essential for mediating RT-induced DNA damage.88 HIF-1α, a central regulator of hypoxic responses, enhances radio resistance by upregulating DNA repair pathways and promoting angiogenesis.4 Targeting HIF-1α with small-molecule inhibitors has been shown to enhance the efficacy of RT in hypoxic ESCC tumors.89
Cancer cells employ multiple mechanisms to evade RT-induced cell death, including activation of DNA repair pathways. The ATM/ATR pathway is critical for detecting and repairing DSBs, while PARP and Ku70/80 facilitate the repair of single-strand breaks (SSBs) and NHEJ, respectively.90 PARP inhibitor olaparib enhances the efficacy of proton beam therapy in platinum- and radiation-resistant ESCC by promoting DNA double-strand breaks and impairing homologous recombination repair.91 Similarly, targeting ATM/ATR with specific inhibitors has demonstrated potential in overcoming radioresistance.92
The TME further contributes to RT resistance through complex interactions between cancer cells and stromal components. CAFs secrete cytokines such as TGF-β and IL-6, which promote cancer cell survival and enhance stemness.93,94 CAF-secreted PAI-1 and TGF-β promote ESCC cell migration and invasion through the AKT and ERK1/2 pathways, and may enhance radio resistance via exosomal miR-3656 targeting the ACAP2/PI3K-AKT axis.95–97 TAMs, particularly those with an M2 phenotype, also contribute to radio resistance by secreting pro-survival factors and suppressing anti-tumor immunity.98 Targeting TAMs with CSF-1R inhibitors has been shown to enhance the efficacy of RT in ESCC.99
Inflammation and TME Modulation in Response to RT
RT exerts its therapeutic effects not only by directly eradicating cancer cells but also by reshaping the TME and modulating systemic immune responses. While RT can stimulate pro-inflammatory and immunogenic effects, it can also induce immunosuppressive mechanisms that contribute to resistance. Understanding the dual role of RT in inflammation and TME modulation is essential for optimizing its therapeutic efficacy in ESCC.
RT-Induced Inflammation
RT triggers a robust inflammatory response in the TME, characterized by the upregulation of pro-inflammatory cytokines such as IL-1β, IL-6, and TNF-α.100 These cytokines have complex roles in tumor progression and immune modulation. IL-6 promotes cancer cell survival and angiogenesis via STAT3 activation, while TNF-α, despite its apoptotic potential, can also contribute to tumor progression by activating NF-κB signaling.101–103 RT-induced IL-1β secretion has been shown to facilitate the recruitment of MDSCs into the TME, exacerbating immune suppression.104
The balance between pro-inflammatory and anti-inflammatory responses following RT significantly influences treatment outcomes. While RT initially induces a pro-inflammatory state, it can also activate immunosuppressive pathways, including the upregulation of TGF-β and IL-10, which inhibit anti-tumor immunity.105 The TGF-β pathway has been identified as a key mediator of RT-induced immune suppression, with its inhibition shown to enhance RT efficacy in ESCC. TGF-β signaling plays a central role in promoting radio resistance in ESCC by inducing epithelial-mesenchymal transition (EMT) through Smad2/3 phosphorylation and E-cadherin suppression,106 activating CAF-mediated expression of EMT markers such as Slug, Snail, and Zeb1,107 enhancing tumor progression via paracrine signaling from CAFs,96 and contributing to immune suppression by stimulating MDSC production through IL-6/exosomal miR-21 pathways.108 Notably, inhibition of TGF-β signaling using DNMT inhibitors sensitizes ESCC cells to RT by inducing G2/M cell cycle arrest and apoptosis.109
Additionally, RT can induce IL-10 expression in tumor-associated macrophages as part of a feedback mechanism involving HMGB1/TNF-α signaling, which activates downstream STAT3 pathways, thereby suppressing antigen presentation and T cell activation within the TME.110,111
Immune Modulation by RT
The abscopal effect describes a phenomenon in which RT elicits systemic anti-tumor immunity, leading to regression of tumors outside the irradiated field.112 This effect is mediated by the release of tumor antigens and DAMPs which activate DCs and promote T cell-mediated tumor clearance.113 RT-induced calreticulin exposure on cancer cells has been shown to enhance DC activation and antigen cross-presentation, facilitating a systemic immune response.114 However, the abscopal effect remains rare, likely due to the highly immunosuppressive TME in ESCC.
While RT can activate anti-tumor immunity, it also contributes to immune exhaustion by upregulating immune checkpoint molecules such as PD-L1 and CTLA-4. RT-induced PD-L1 expression on cancer cells and TAMs inhibits T cell activity, diminishing the effectiveness of RT.115 Similarly, upregulation of CTLA-4 on Tregs has been implicated in RT-induced immune suppression.116 Combining RT with ICIs has shown promise in overcoming these limitations and potentiating anti-tumor immunity.117 The bidirectional interactions between RT and immune response in ESCC are summarized in Figure 2.
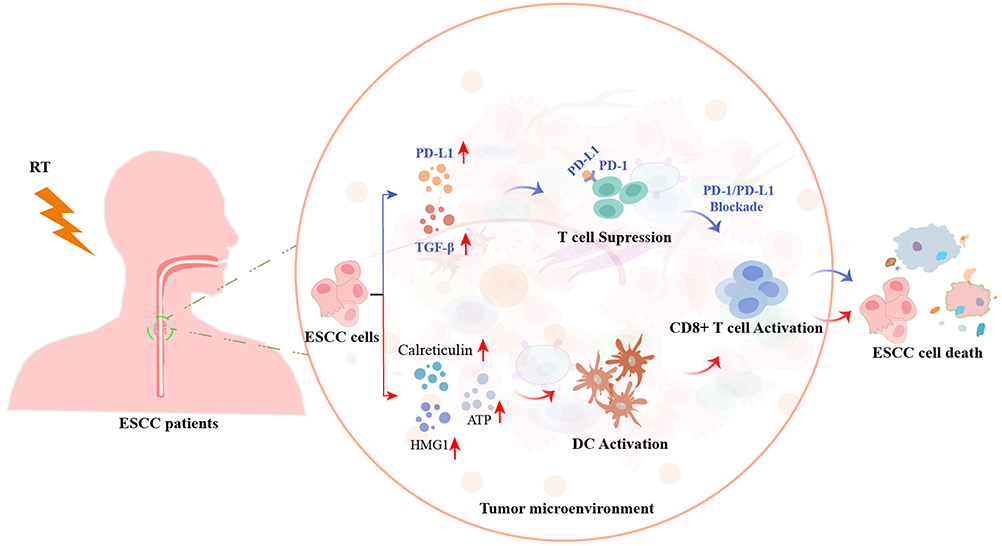 |
Figure 2 Interplay Between RT and Immunotherapy in ESCC. The dual role of RT and its synergy with ICIs in the ESCC TME. RT induces tumor cell death and ICD, releasing DAMPs such as calreticulin, HMGB1, and ATP, that activate DCs and initiate antitumor T cell responses. However, RT also upregulates immunosuppressive factors such as PD-L1 and TGF-β, contributing to T cell suppression. The addition of PD-1/PD-L1 blockade restores T cell function, enhancing CD8+ T cell activation and systemic immunity. |
Combination Approaches Targeting Inflammation and the TME
Targeting RT-induced inflammation with anti-inflammatory agents has emerged as a promising strategy to enhance RT efficacy. NSAIDs and COX-2 inhibitors reduce the production of pro-inflammatory cytokines and prostaglandins, mitigating RT-induced inflammation and tumor progression.118,119 COX-2 inhibitors enhance the efficacy of RT in ESCC by suppressing PGE2 production and inhibiting NF-κB signaling, thereby reducing inflammation, and improving tumor radiosensitivity.49 Although NSAIDs can reduce IL-6 levels and attenuate inflammation, their suppression of PGE2 may inadvertently elevate TNF-α production, highlighting the need to balance pro- and anti-inflammatory effects when combining NSAIDs with RT to optimize therapeutic outcomes.120
Modulating the TME to overcome RT resistance is another promising therapeutic strategy. TGF-β inhibitors counteract the immunosuppressive effects of TGF-β, enhancing T cell infiltration and activation within the TME.28 The combination of RT with TGF-β inhibition has been shown to improve tumor control and prolong survival in ESCC.11 VEGF blockade promotes vascular normalization and alleviates tumor hypoxia, thereby enhancing RT efficacy through improved oxygenation and modulation of the TME.121 Targeting VEGF enhances RT sensitivity in ESCC, as VEGF knockdown improves tumor cell responsiveness to RT and elevated serum VEGF levels correlate with poor clinical outcomes, supporting VEGF inhibition as a potential radio-sensitization strategy.122 Key strategies to improve RT outcomes in ESCC are summarized in Table 3.
 |
Table 3 Therapeutic Strategies to Enhance RT Efficacy in ESCC |
Therapeutic Implications and Future Directions
The intricate interplay between inflammation, TME, and RT in ESCC has paved the way for novel therapeutic strategies. Integrating immunotherapy with RT, targeting inflammatory pathways and the TME, and leveraging advanced technologies such as AI are transforming treatment approaches. These advancements hold the potential to improve therapeutic efficacy and personalize treatment for ESCC patients.
Integrating Immunotherapy with RT
The combination of ICIs with RT represents a promising strategy for enhancing anti-tumor immunity in ESCC. PD-1/PD-L1 inhibitors disrupt the interaction between PD-1 on T cells and PD-L1 on tumor cells, thereby restoring T cell function and promoting tumor elimination.123,124 RT has been shown to augment the efficacy of ICIs by inducing ICD and releasing tumor antigens, which facilitate DC activation and subsequent T cell priming.84,129 In ESCC, RT combined with anti-PD-1 therapy (camrelizumab) enhances peripheral CD8+T cell activation and more effectively reshapes memory T cell differentiation than CRT, contributing to improved prognosis in patients with locally advanced ESCC.125 Furthermore, Integrating PD-1/PD-L1 inhibitors with RT enhances antitumor immunity in ESCC by promoting tumor antigen release, increasing PD-L1 expression, and facilitating T cell activation through modulation of the TME and reversal of immune exhaustion.126,127
Personalized RT strategies, tailored to individual tumor biology and patient characteristics, are essential for optimizing outcomes. Advances in molecular profiling and imaging have facilitated the development of adaptive RT, which dynamically adjusts treatment plans based on tumor response and alterations in the TME.128 Hypofractionated RT delivers higher doses per fraction over a shorter treatment course and has been shown to improve tumor control while maintaining a favorable toxicity profile in ESCC.130 Additionally, radiogenomics integrates genomic data into RT planning and is emerging as a tool for identifying patients most likely to benefit from RT-ICI combination therapy.131
PD-1/PD-L1 inhibitors have demonstrated encouraging results in ESCC, particularly when combined with RT, by enhancing T cell-mediated antitumor responses and overcoming immune suppression.132 However, these agents represent only part of the evolving immunotherapeutic landscape. Newer checkpoint targets such as lymphocyte-activation gene 3 (LAG-3) and T cell immunoglobulin and mucin-domain containing-3 (TIM-3) are emerging as potential immunomodulatory regulators in ESCC, with early evidence suggesting they may mediate resistance to PD-1 blockade and contribute to immune escape.133,134 Thus, dual or sequential blockade strategies involving PD-1 and LAG-3 or TIM-3 warrant exploration in combination with RT. Additionally, while COX-2 inhibitors have been proposed to augment radiosensitivity by suppressing inflammation, recent findings from the CHECKRT trial reported no significant clinical benefit of COX-2 inhibition in radio sensitizing ESCC.12 This underscores the necessity of critically assessing the translational potential of inflammation-targeted therapies. Overall, while PD-1/PD-L1 inhibitors remain the most established class in immunoradiotherapy for ESCC, broadening the scope to include alternative checkpoints and negative findings is crucial for a balanced and comprehensive view of immunotherapeutic strategies. Table 4 summarizes selected phase II trials evaluating radiotherapy combined with ICIs in ESCC.
 |
Table 4 Selected Phase II Trials Evaluating Radiotherapy Combined with ICIs in ESCC |
Targeting Inflammatory Pathways and the TME in ESCC
Targeting the TME with emerging therapeutic agents offers new opportunities to overcome resistance and enhance RT efficacy. CXCR4 inhibitors disrupt the interaction between CXCR4 on tumor cells and CXCL12 within the TME, thereby limiting tumor cell migration and metastasis.135 CXCR4 blockade has been shown to enhance RT-induced tumor cell death and stimulate immune activation in ESCC.11 Similarly, inhibition of TGF-β, a key immunosuppressive cytokine in the TME, promotes T cell infiltration and enhances anti-tumor immunity.136 Combining RT with TGF-β blockade can be used to improve tumor control and prolong survival in ESCC models.11 Moreover, repositioning anti-inflammatory drugs such as NSAIDs and selective COX-2 inhibitors offers a cost-effective strategy to counteract RT-induced inflammation. They suppress the release of prostaglandins and cytokines like IL-6 and TNF-α, reduce PGE2 levels, and inhibit NF-κB signaling, collectively mitigating inflammation-driven resistance and improving RT outcomes in ESCC.49,118–120
Beyond classical cytokines such as IL-6 and TNF-α, recent studies have identified the NLRP3 inflammasome as a critical mediator of RT-induced inflammation in ESCC. German groups have demonstrated that NLRP3 activation contributes to immune suppression and treatment resistance in preclinical ESCC models, suggesting that NLRP3-targeted therapies may enhance RT efficacy.137
Translational Outlook
Advanced computational strategies, including AI-driven RT (AI-RT), are transforming precision oncology. While several models have emerged from East Asian institutions, notable innovations have also been developed in Western settings. For instance, researchers at Memorial Sloan Kettering Cancer Center (MSKCC) in the United States have proposed machine learning-based dose prediction models to optimize target coverage and minimize toxicity in ESCC.138 Additionally, global collaborations such as the NRG Oncology Phase III hypofractionation trials offer valuable insights into RT design and outcomes in multinational ESCC cohorts.139
Despite promising preclinical results, AI-based RT strategies face deployment challenges including image standardization, algorithm reproducibility, and integration into clinical workflows.138 These barriers highlight the need for rigorous validation and platform harmonization before widespread clinical implementation.
In parallel, recent findings on STING (stimulator of interferon genes) agonists suggest potential synergy with RT in reversing immune suppression and enhancing dendritic cell priming. Incorporating STING-RT combinations into ESCC treatment paradigms may potentiate antitumor immunity and deserves further investigation.99
RT elicits divergent effects on the TME, ranging from immune activation to profound immunosuppression. These opposing responses are shaped by cytokine release, immune cell infiltration, and the nature of RT delivery. To clarify these context-specific dynamics, Table 5 presents a comparative overview of pro-inflammatory versus immunosuppressive TME features after RT in ESCC. This table summarizes the distinct immunological profiles observed after RT in ESCC, comparing pro-inflammatory and immunosuppressive responses. These include key cytokines, immune cell subsets, molecular drivers, RT parameters, and associated biomarkers. The immunological outcome of RT is context-dependent and may influence sensitivity to immune checkpoint blockade or the need for combinatory interventions.This framework supports the rationale for tailoring combination therapies based on immune phenotype and radiation dose/fractionation strategies.
 |
Table 5 Contrasting Immune Networks in the TME Following RT in ESCC |
Statistical Considerations
To strengthen translational validity, future analyses of inflammatory biomarkers such as CRP and IL-6 should employ multivariate Cox proportional hazards models to adjust for potential confounding variables, including smoking history, human papillomavirus status, and tumor stage. Reliance on univariate analyses may lead to overestimation of effect sizes and misidentification of independent predictors of RT response.140 AI and machine learning applications in RT planning should adhere to established methodological frameworks, such as the TRIPOD reporting standards. Comprehensive reporting of model validation procedures, cross-validation strategies, and performance metrics, including area under the receiver operating characteristic curve with confidence intervals, is essential to ensure robustness and reproducibility in clinical implementation.141
In preclinical mechanistic studies, the use of underpowered statistical comparisons should be supplemented with appropriate corrections for multiple hypothesis testing, such as false discovery rate control or family-wise error rate adjustment, to mitigate the risk of spurious findings.140
Furthermore, claims regarding survival benefits from combined therapeutic regimens should be substantiated by quantitative measures, including hazard ratios, time-specific survival analyses, absolute risk reduction, and number needed to treat, to facilitate rigorous clinical extrapolation and inform future trial designs RT.142
As this is a narrative review, statistical metrics such as AUC with 95% confidence intervals and hazard ratios are discussed to highlight methodological recommendations for future studies. These metrics are not reported as original results.
Conclusion
This review highlights the central role of inflammation-driven mechanisms in shaping the TME and modulating RT responses in ESCC. Clinically validated strategies such as anti-PD-1 therapies combined with RT have demonstrated objective response rate (ORR) improvements of 20–30% in Phase II trials,33,143 supporting their near-term translational potential. In contrast, emerging modalities like STING agonists and NLRP3 inhibitors remain in early-stage evaluation and require further validation.144,145 Mechanistically, RT-induced cytokine release including IL-6 and TGF-β drives dynamic TME remodeling, promoting both immune activation and suppression depending on dose and fractionation. Targeting these bidirectional responses through dual checkpoint blockade, TME-modulatory agents, or radiosensitizers represents a rational path forward.
AI-driven tools, including RT planning algorithms and radiomic biomarkers, offer promising precision-guided approaches but currently face reproducibility and standardization challenges that limit clinical implementation.146,147 Furthermore, the cost-effectiveness and access to novel immuno-radiotherapeutics remain substantial barriers, particularly in low-resource settings. To accelerate clinical translation, future work must integrate robust biomarker-guided stratification, dose-adaptive immune profiling, and comparative trials distinguishing exploratory hypotheses from validated protocols. Such integration will be essential to move beyond generalized benefits toward durable, measurable, and equitable improvements in ESCC outcomes.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Henan Provincial Key Science and Technology Research Project (252102311044).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Morgan E, Soerjomataram I, Rumgay H, et al. The Global Landscape of Esophageal Squamous Cell Carcinoma and Esophageal Adenocarcinoma Incidence and Mortality in 2020 and Projections to 2040: new Estimates From GLOBOCAN 2020. Gastroenterology. 2022;163(3):649–658e2. doi:10.1053/j.gastro.2022.05.054
2. Lin EW, Karakasheva TA, Hicks PD, Bass AJ, Rustgi AK. The tumor microenvironment in esophageal cancer. Oncogene. 2016;35(41):5337–5349. doi:10.1038/onc.2016.34
3. Labani-Motlagh A, Ashja-Mahdavi M, Loskog A. The Tumor Microenvironment: a Milieu Hindering and Obstructing Antitumor Immune Responses. Front Immunol. 2020;11:940. doi:10.3389/fimmu.2020.00940
4. Kabakov AE, Yakimova AO. Hypoxia-Induced Cancer Cell Responses Driving Radioresistance of Hypoxic Tumors: approaches to Targeting and Radiosensitizing. Cancers. 2021;13(5):1102. doi:10.3390/cancers13051102
5. Oweida A, Paquette B. Reconciling two opposing effects of radiation therapy: stimulation of cancer cell invasion and activation of anti-cancer immunity. Int J Radiat Biol. 2023;99(6):951–963. doi:10.1080/09553002.2021.1956005
6. Yu S, Wang Y, He P, et al. Effective Combinations of Immunotherapy and Radiotherapy for Cancer Treatment. Front Oncol. 2022;12:809304. doi:10.3389/fonc.2022.809304
7. Li Z, Lai X, Fu S, et al. Immunogenic Cell Death Activates the Tumor Immune Microenvironment to Boost the Immunotherapy Efficiency. Adv Sci. 2022;9(22):e2201734. doi:10.1002/advs.202201734
8. Oweida A, Hararah MK, Phan A, et al. Resistance to Radiotherapy and PD-L1 Blockade Is Mediated by TIM-3 Upregulation and Regulatory T-Cell Infiltration. Clin Cancer Res. 2018;24(21):5368–5380. doi:10.1158/1078-0432.CCR-18-1038
9. Lee BM, Seong J. Radiotherapy as an immune checkpoint blockade combination strategy for hepatocellular carcinoma. World J Gastroenterol. 2021;27(10):919–927. doi:10.3748/wjg.v27.i10.919
10. Li L, Wen Q, Ding R. Therapeutic targeting of VEGF and/or TGF-β to enhance anti-PD-(L)1 therapy: the evidence from clinical trials. Front Oncol. 2022;12:905520. doi:10.3389/fonc.2022.905520
11. An L, Li M, Jia Q. Mechanisms of radiotherapy resistance and radiosensitization strategies for esophageal squamous cell carcinoma. Mol Cancer. 2023;22(1):140. doi:10.1186/s12943-023-01839-2
12. Yusup G, Akutsu Y, Mutallip M, et al. A COX-2 inhibitor enhances the antitumor effects of chemotherapy and radiotherapy for esophageal squamous cell carcinoma. Int J Oncol. 2014;44(4):1146–1152. doi:10.3892/ijo.2014.2300
13. Tufail M, Jiang CH, Li N. Altered metabolism in cancer: insights into energy pathways and therapeutic targets. Mol Cancer. 2024;23(1):203. doi:10.1186/s12943-024-02119-3
14. Akins NS, Nielson TC, Le HV. Inhibition of Glycolysis and Glutaminolysis: an Emerging Drug Discovery Approach to Combat Cancer. Curr Top Med Chem. 2018;18(6):494–504. doi:10.2174/1568026618666180523111351
15. Nakao E, Yoshio T, Kato Y, et al. Randomized controlled trial of an artificial intelligence diagnostic system for the detection of esophageal squamous cell carcinoma in clinical practice. Endoscopy. 2025;57(3):210–217. doi:10.1055/a-2421-3194
16. Chu LY, Peng YH, Weng XF, Xie JJ, Xu YW. Blood-based biomarkers for early detection of esophageal squamous cell carcinoma. World J Gastroenterol. 2020;26(15):1708–1725. doi:10.3748/wjg.v26.i15.1708
17. Feng Z, Qu J, Liu X, et al. Integrated bioinformatics analysis of differentially expressed genes and immune cell infiltration characteristics in Esophageal Squamous cell carcinoma. Sci Rep. 2021;11(1):16696. doi:10.1038/s41598-021-96274-y
18. Liu S, Wang W, Hu S, et al. Radiotherapy remodels the tumor microenvironment for enhancing immunotherapeutic sensitivity. Cell Death Dis. 2023;14(10):679. doi:10.1038/s41419-023-06211-2
19. Elbanna M, Chowdhury NN, Rhome R, Fishel ML. Clinical and Preclinical Outcomes of Combining Targeted Therapy With Radiotherapy. Front Oncol. 2021;11:749496. doi:10.3389/fonc.2021.749496
20. Jiang M, Hu Y, Lin G, Chen C, Li H. Radiotherapy combined with immune checkpoint inhibitors in locally advanced/metastatic esophageal squamous cell carcinoma: clinical trials, efficacy and future directions. Front Immunol. 2023;14:1177085. doi:10.3389/fimmu.2023.1177085
21. Zheng S, Liu B, Guan X. The Role of Tumor Microenvironment in Invasion and Metastasis of Esophageal Squamous Cell Carcinoma. Front Oncol. 2022;12:911285. doi:10.3389/fonc.2022.911285
22. Wang Z, Sun X, Li Z, Yu H, Li W, Xu Y. Metabolic reprogramming in esophageal squamous cell carcinoma. Front Pharmacol. 2024;15:1423629. doi:10.3389/fphar.2024.1423629
23. Chen MF, Chen PT, Lu MS, Lin PY, Chen W-C, Lee K-D. IL-6 expression predicts treatment response and outcome in squamous cell carcinoma of the esophagus. Mol Cancer. 2013;12(1):26. doi:10.1186/1476-4598-12-26
24. Zhao ZF, Li JX, Ye R, Wu X, Gao LL, Niu BL. Interleukin-6 as a potential molecular target in esophageal squamous cell carcinoma. Oncol Lett. 2016;11(2):925–932. doi:10.3892/ol.2015.3990
25. Liu Q, Zhu Z, Chen Y, et al. Phase 2 Study of Stereotactic Body Radiation Therapy for Patients with Oligometastatic Esophageal Squamous Cell Carcinoma. Int J Radiat Oncol Biol Phys. 2020;108(3):707–715. doi:10.1016/j.ijrobp.2020.05.003
26. Miljanic M, Montalvo S, Aliru M, et al. The Evolving Interplay of SBRT and the Immune System, along with Future Directions in the Field. Cancers. 2022;14(18). doi:10.3390/cancers14184530
27. Donlon NE, Power R, Hayes C, Reynolds JV, Lysaght J. Radiotherapy, immunotherapy, and the tumour microenvironment: turning an immunosuppressive milieu into a therapeutic opportunity. Cancer Lett. 2021;502:84–96. doi:10.1016/j.canlet.2020.12.045
28. Batlle E, Massagué J. Transforming Growth Factor-β Signaling in Immunity and Cancer. Immunity. 2019;50(4):924–940. doi:10.1016/j.immuni.2019.03.024
29. Sharan RN, Mehrotra R, Choudhury Y, Asotra K. Association of betel nut with carcinogenesis: revisit with a clinical perspective. PLoS One. 2012;7(8):e42759. doi:10.1371/journal.pone.0042759
30. Guo ZX, Ma JL, Zhang JQ, et al. Metabolic reprogramming and immunological changes in the microenvironment of esophageal cancer: future directions and prospects. Front Immunol. 2025;16:1524801. doi:10.3389/fimmu.2025.1524801
31. Sawayama H, Ogata Y, Ishimoto T, et al. Glucose transporter 1 regulates the proliferation and cisplatin sensitivity of esophageal cancer. Cancer Sci. 2019;110(5):1705–1714. doi:10.1111/cas.13995
32. Yuan Y, Luo S, Wang X, et al. Efficacy and safety of concurrent programmed cell death protein 1 inhibitor and definitive radiotherapy with immunonutrition support in esophageal squamous cell cancer: a phase II multicenter clinical trial. Radiat Oncol. 2025;20(1):58. doi:10.1186/s13014-025-02604-z
33. Zhao W, Ke S, Cai X, et al. Radiotherapy plus camrelizumab and irinotecan for oligometastatic esophageal squamous cell carcinoma patients after first-line immunotherapy plus chemotherapy failure: an open-label, single-arm, phase II trial. Radiother Oncol. 2023;184:109679. doi:10.1016/j.radonc.2023.109679
34. Cao F, Han H, Zhang F, et al. HPV infection in esophageal squamous cell carcinoma and its relationship to the prognosis of patients in northern China. ScientificWorldJournal. 2014;2014:804738. doi:10.1155/2014/804738
35. Syrjanen KJ. HPV infections and oesophageal cancer. J Clin Pathol. 2002;55(10):721–728. doi:10.1136/jcp.55.10.721
36. Zur Hausen H. Papillomaviruses and cancer: from basic studies to clinical application. Nat Rev Cancer. 2002;2(5):342–350. doi:10.1038/nrc798
37. Zhao H, Wei Y, Zhang J, et al. HPV16 infection promotes the malignant transformation of the esophagus and progression of esophageal squamous cell carcinoma. J Med Virol. 2023;95(10):e29132. doi:10.1002/jmv.29132
38. Gonzalez-Stegmaier R, Aguila-Torres P, Villarroel-Espindola F. Historical and Molecular Perspectives on the Presence of Helicobacter pylori in Latin America: a Niche to Improve Gastric Cancer Risk Assessment. Int J Mol Sci. 2024;25(3):1761. doi:10.3390/ijms25031761
39. Yuan X, Liu K, Li Y, et al. HPV16 infection promotes an M2 macrophage phenotype to promote the invasion and metastasis of esophageal squamous cell carcinoma. Clin Transl Oncol. 2021;23(11):2382–2393. doi:10.1007/s12094-021-02642-5
40. Prabhu A, Obi KO, Rubenstein JH. The synergistic effects of alcohol and tobacco consumption on the risk of esophageal squamous cell carcinoma: a meta-analysis. Am J Gastroenterol. 2014;109(6):822–827. doi:10.1038/ajg.2014.71
41. Walters MJ, Paul-Clark MJ, McMaster SK, Ito K, Adcock IM, Mitchell JA. Cigarette smoke activates human monocytes by an oxidant-AP-1 signaling pathway: implications for steroid resistance. Mol Pharmacol. 2005;68(5):1343–1353. doi:10.1124/mol.105.012591
42. Takahashi H, Ogata H, Nishigaki R, Broide DH, Karin M. Tobacco smoke promotes lung tumorigenesis by triggering IKKbeta- and JNK1-dependent inflammation. Cancer Cell. 2010;17(1):89–97. doi:10.1016/j.ccr.2009.12.008
43. Reynolds PR, Kasteler SD, Schmitt RE, Hoidal JR. Receptor for advanced glycation end-products signals through Ras during tobacco smoke-induced pulmonary inflammation. Am J Respir Cell Mol Biol. 2011;45(2):411–418. doi:10.1165/rcmb.2010-0231OC
44. Bos JL. ras oncogenes in human cancer: a review. Cancer Res. 1989;49(17):4682–4689.
45. Ma K, Cao B, Guo M. The detective, prognostic, and predictive value of DNA methylation in human esophageal squamous cell carcinoma. Clin Clin Epigenet. 2016;8:43. doi:10.1186/s13148-016-0210-9
46. Zhao C, Zhou J, Gu Y, et al. Urinary exposure of N-nitrosamines and associated risk of esophageal cancer in a high incidence area in China. Sci Total Environ. 2020;738:139713. doi:10.1016/j.scitotenv.2020.139713
47. Cao Y, Yi Y, Han C, Shi B. NF-kappaB signaling pathway in tumor microenvironment. Front Immunol. 2024;15:1476030. doi:10.3389/fimmu.2024.1476030
48. Zuo J, Zhao M, Liu B, et al. TNF‑alpha‑mediated upregulation of SOD‑2 contributes to cell proliferation and cisplatin resistance in esophageal squamous cell carcinoma. Oncol Rep. 2019;42(4):1497–1506. doi:10.3892/or.2019.7252
49. Fang J, Chu L, Li C, et al. JAK2 inhibitor blocks the inflammation and growth of esophageal squamous cell carcinoma in vitro through the JAK/STAT3 pathway. Oncol Rep. 2015;33(1):494–502. doi:10.3892/or.2014.3609
50. Zhao J, Jin G, Liu X, et al. PAR1 and PAR4 exert opposite effects on tumor growth and metastasis of esophageal squamous cell carcinoma via STAT3 and NF-kappaB signaling pathways. Cancer Cell Int. 2021;21(1):637. doi:10.1186/s12935-021-02354-4
51. Zheng ZY, Chu MY, Lin W, et al. Blocking STAT3 signaling augments MEK/ERK inhibitor efficacy in esophageal squamous cell carcinoma. Cell Death Dis. 2022;13(5):496. doi:10.1038/s41419-022-04941-3
52. Zheng ZY, Yang PL, Luo W, et al. STAT3beta Enhances Sensitivity to Concurrent Chemoradiotherapy by Inducing Cellular Necroptosis in Esophageal Squamous Cell Carcinoma. Cancers. 2021;13(4):901. doi:10.3390/cancers13040901
53. Fang L, Che Y, Zhang C, et al. LAMC1 upregulation via TGFbeta induces inflammatory cancer-associated fibroblasts in esophageal squamous cell carcinoma via NF-kappaB-CXCL1-STAT3. Mol Oncol. 2021;15(11):3125–3146. doi:10.1002/1878-0261.13053
54. Sun Y, Qian Y, Chen C, et al. Extracellular vesicle IL-32 promotes the M2 macrophage polarization and metastasis of esophageal squamous cell carcinoma via FAK/STAT3 pathway. J Exp Clin Cancer Res. 2022;41(1):145. doi:10.1186/s13046-022-02348-8
55. Cui FB, Huang DF, Zhang FL, et al. Investigation on the regulatory effect of PGE2 on ESCC cells through the trans-activation of EGFR by EP2 and the relevant mechanism. Eur Rev Med Pharmacol Sci. 2017;21(24):5668–5676. doi:10.26355/eurrev_201712_14011
56. Zhang Y, Dong S, Xu R, et al. Prognostic and predictive role of COX-2, XRCC1 and RASSF1 expression in patients with esophageal squamous cell carcinoma receiving radiotherapy. Oncol Lett. 2017;13(4):2549–2556. doi:10.3892/ol.2017.5780
57. Zhu P, Zhou K, Lu S, Bai Y, Qi R, Zhang S. Modulation of aryl hydrocarbon receptor inhibits esophageal squamous cell carcinoma progression by repressing COX2/PGE2/STAT3 axis. J Cell Commun Signal. 2020;14(2):175–192. doi:10.1007/s12079-019-00535-5
58. Wang Y, Liu X, Hu G, et al. EGFR-IL-6 Signaling Axis Mediated the Inhibitory Effect of Methylseleninic Acid on Esophageal Squamous Cell Carcinoma. Front Pharmacol. 2021;12:719785. doi:10.3389/fphar.2021.719785
59. Deng L, Zhang X, Xiang X, et al. NANOG Promotes Cell Proliferation, Invasion, and Stemness via IL-6/STAT3 Signaling in Esophageal Squamous Carcinoma. Technol Cancer Res Treat. 2021;20:15330338211038492. doi:10.1177/15330338211038492
60. Qian Q, Wu C, Chen J, Wang W. Relationship between IL-10 and PD-L1 in esophageal carcinoma tissues and IL-10 down-regulates PD-L1 expression via Met signaling pathway. J Gastrointest Oncol. 2020;11(2):337–355. doi:10.21037/jgo.2020.01.06
61. Ardalan Khales S, Aarabi A, Abbaszadegan MR, Forghanifard MM. INPP5A/HLA-G1/IL-10/MMP-21 Axis in Progression of Esophageal Squamous Cell Carcinoma. Iran Biomed J. 2022;26(6):440–453. doi:10.52547/ibj.3716
62. Huai Q, Guo W, Han L, et al. Identification of prognostic genes and tumor-infiltrating immune cells in the tumor microenvironment of esophageal squamous cell carcinoma and esophageal adenocarcinoma. Transl Cancer Res. 2021;10(4):1787–1803. doi:10.21037/tcr-20-3078
63. Cendrowicz E, Sas Z, Bremer E, Rygiel TP. The Role of Macrophages in Cancer Development and Therapy. Cancers. 2021;13(8):1946. doi:10.3390/cancers13081946
64. Chen J, Zhao D, Zhang L, et al. Tumor-associated macrophage (TAM)-derived CCL22 induces FAK addiction in esophageal squamous cell carcinoma (ESCC). Cell Mol Immunol. 2022;19(9):1054–1066. doi:10.1038/s41423-022-00903-z
65. Song ZB, Lin BC, Li B, et al. Preoperative elevation of serum C-reactive protein as an indicator of poor prognosis for early-stage esophageal squamous cell carcinoma. Kaohsiung J Med Sci. 2013;29(12):662–666. doi:10.1016/j.kjms.2013.01.016
66. Groblewska M, Mroczko B, Sosnowska D, Szmitkowski M. Interleukin 6 and C-reactive protein in esophageal cancer. Clin Chim Acta. 2012;413(19–20):1583–1590. doi:10.1016/j.cca.2012.05.009
67. Bhat AA, Nisar S, Maacha S, et al. Cytokine-chemokine network driven metastasis in esophageal cancer; promising avenue for targeted therapy. Mol Cancer. 2021;20(1):2. doi:10.1186/s12943-020-01294-3
68. Pastrez PRA, Barbosa AM, Mariano VS, et al. Interleukin-8 and Interleukin-6 Are Biomarkers of Poor Prognosis in Esophageal Squamous Cell Carcinoma. Cancers. 2023;15(7):1997. doi:10.3390/cancers15071997
69. Chen MF, Chen PT, Kuan FC, Chen WC. The Predictive Value of Pretreatment Neutrophil-To-Lymphocyte Ratio in Esophageal Squamous Cell Carcinoma. Ann Surg Oncol. 2019;26(1):190–199. doi:10.1245/s10434-018-6944-1
70. Muthupalani S, Annamalai D, Feng Y, et al. IL-1beta transgenic mouse model of inflammation driven esophageal and oral squamous cell carcinoma. Sci Rep. 2023;13(1):12732. doi:10.1038/s41598-023-39907-8
71. Chen Y, Wang D, Peng H, et al. Epigenetically upregulated oncoprotein PLCE1 drives esophageal carcinoma angiogenesis and proliferation via activating the PI-PLCepsilon-NF-kappaB signaling pathway and VEGF-C/ Bcl-2 expression. Mol Cancer. 2019;18(1):1. doi:10.1186/s12943-018-0930-x
72. Ma Y, Su X, Li X, et al. Combined detection of peripheral blood VEGF and inflammation biomarkers to evaluate the clinical response and prognostic prediction of non-operative ESCC. Sci Rep. 2021;11(1):15305. doi:10.1038/s41598-021-94329-8
73. Tang H, Wang H, Fang Y, et al. Neoadjuvant chemoradiotherapy versus neoadjuvant chemotherapy followed by minimally invasive esophagectomy for locally advanced esophageal squamous cell carcinoma: a prospective multicenter randomized clinical trial. Ann Oncol. 2023;34(2):163–172. doi:10.1016/j.annonc.2022.10.508
74. Jin Z, Chen D, Chen M, et al. (Neo)adjuvant Chemoradiotherapy is Beneficial to the Long-term Survival of Locally Advanced Esophageal Squamous Cell Carcinoma: a Network Meta-analysis. World J Surg. 2022;46(1):136–146. doi:10.1007/s00268-021-06301-2
75. Wu X, Li Y, Zhang K, et al. Immunotherapy with or without radiotherapy for metastatic or recurrent esophageal squamous cell carcinoma: a real-world study. Clin Transl Radiat Oncol. 2023;38:130–137. doi:10.1016/j.ctro.2022.10.011
76. Roohani S, Wiltink LM, Kaul D, Spalek MJ, Haas RL. Update on Dosing and Fractionation for Neoadjuvant Radiotherapy for Localized Soft Tissue Sarcoma. Curr Treat Options Oncol. 2024;25(4):543–555. doi:10.1007/s11864-024-01188-2
77. Akimoto T, Aoyama H, Chua MLK, et al. Challenges and Opportunities With the Use of Hypofractionated Radiation Therapy in Cancer Care: regional Perspectives From South Korea, Japan, Singapore, and Australia. Adv Radiat Oncol. 2023;8(6):101291. doi:10.1016/j.adro.2023.101291
78. Zhou R, Luo G, Guo S, et al. Moderately hypo-fractionated radiotherapy combined with S-1 in inoperable locally advanced esophageal squamous cell carcinoma: a prospective, single-arm phase II study (GASTO-1045). Front Oncol. 2023;13:1138304. doi:10.3389/fonc.2023.1138304
79. Dona Lemus OM, Cao M, Cai B, Cummings M, Zheng D. Adaptive Radiotherapy: next-Generation Radiotherapy. Cancers. 2024;16(6):1206. doi:10.3390/cancers16061206
80. Wu Y, Song Y, Wang R, Wang T. Molecular mechanisms of tumor resistance to radiotherapy. Mol Cancer. 2023;22(1):96. doi:10.1186/s12943-023-01801-2
81. Sia J, Szmyd R, Hau E, Gee HE. Molecular Mechanisms of Radiation-Induced Cancer Cell Death: a Primer. Front Cell Dev Biol. 2020;8:41. doi:10.3389/fcell.2020.00041
82. Zhu S, Wang Y, Tang J, Cao M. Radiotherapy induced immunogenic cell death by remodeling tumor immune microenvironment. Front Immunol. 2022;13:1074477. doi:10.3389/fimmu.2022.1074477
83. Guo S, Yao Y, Tang Y, et al. Radiation-induced tumor immune microenvironments and potential targets for combination therapy. Signal Transduct Target Ther. 2023;8(1):205. doi:10.1038/s41392-023-01462-z
84. Spiotto M, Fu YX, Weichselbaum RR. The intersection of radiotherapy and immunotherapy: mechanisms and clinical implications. Sci Immunol. 2016;1(3):1266. doi:10.1126/sciimmunol.aag1266
85. Cheng S, Li B, Yu J, Wang L. Update of latest data for combined therapy for esophageal cancer using radiotherapy and immunotherapy: a focus on efficacy, safety, and biomarkers. Chin J Cancer Res. 2023;35(5):483–500. doi:10.21147/j.issn.1000-9604.2023.05.06
86. Chen MF, Chen PT, Chen WC, Lu MS, Lin PY, Lee KD. The role of PD-L1 in the radiation response and prognosis for esophageal squamous cell carcinoma related to IL-6 and T-cell immunosuppression. Oncotarget. 2016;7(7):7913–7924. doi:10.18632/oncotarget.6861
87. Guo Z, Zhang K, Wei X, et al. Radiotherapy plus camrelizumab affects peripheral CD8 T-cell differentiation subsets expressing PD-1, TIGIT, and CTLA-4 in esophageal squamous cell carcinoma. J Leukoc Biol. 2023;113(1):11–17. doi:10.1093/jleuko/qiac018
88. Wang H, Jiang H, Van De Gucht M, De Ridder M. Hypoxic Radioresistance: can ROS Be the Key to Overcome It? Cancers. 2019;11(1):112. doi:10.3390/cancers11010112
89. Zhu Y, Zang Y, Zhao F, et al. Inhibition of HIF-1alpha by PX-478 suppresses tumor growth of esophageal squamous cell cancer in vitro and in vivo. Am J Cancer Res. 2017;7(5):1198–1212.
90. Wang M, Wu W, Wu W, et al. PARP-1 and Ku compete for repair of DNA double strand breaks by distinct NHEJ pathways. Nucleic Acids Res. 2006;34(21):6170–6182. doi:10.1093/nar/gkl840
91. Kageyama SI, Junyan D, Hojo H, et al. PARP inhibitor olaparib sensitizes esophageal carcinoma cells to fractionated proton irradiation. J Radiat Res. 2020;61(2):177–186. doi:10.1093/jrr/rrz088
92. Leszczynska KB, Dobrynin G, Leslie RE, et al. Preclinical testing of an Atr inhibitor demonstrates improved response to standard therapies for esophageal cancer. Radiother Oncol. 2016;121(2):232–238. doi:10.1016/j.radonc.2016.10.023
93. Yu Y, Xiao CH, Tan LD, Wang QS, Li XQ, Feng YM. Cancer-associated fibroblasts induce epithelial-mesenchymal transition of breast cancer cells through paracrine TGF-beta signalling. Br J Cancer. 2014;110(3):724–732. doi:10.1038/bjc.2013.768
94. Shintani Y, Fujiwara A, Kimura T, et al. IL-6 Secreted from Cancer-Associated Fibroblasts Mediates Chemoresistance in NSCLC by Increasing Epithelial-Mesenchymal Transition Signaling. J Thorac Oncol. 2016;11(9):1482–1492. doi:10.1016/j.jtho.2016.05.025
95. Sakamoto H, Koma YI, Higashino N, et al. PAI-1 derived from cancer-associated fibroblasts in esophageal squamous cell carcinoma promotes the invasion of cancer cells and the migration of macrophages. Lab Invest. 2021;101(3):353–368. doi:10.1038/s41374-020-00512-2
96. Okamoto M, Koma YI, Kodama T, Nishio M, Shigeoka M, Yokozaki H. Growth Differentiation Factor 15 Promotes Progression of Esophageal Squamous Cell Carcinoma via TGF-beta Type II Receptor Activation. Pathobiology. 2020;87(2):100–113. doi:10.1159/000504394
97. Jin Y, Meng Q, Zhang B, et al. Cancer-associated fibroblasts-derived exosomal miR-3656 promotes the development and progression of esophageal squamous cell carcinoma via the ACAP2/PI3K-AKT signaling pathway. Int J Biol Sci. 2021;17(14):3689–3701. doi:10.7150/ijbs.62571
98. Duan Z, Luo Y. Targeting macrophages in cancer immunotherapy. Signal Transduct Target Ther. 2021;6(1):127. doi:10.1038/s41392-021-00506-6
99. Nakajima S, Mimura K, Kaneta A, et al. Radiation-Induced Remodeling of the Tumor Microenvironment Through Tumor Cell-Intrinsic Expression of cGAS-STING in Esophageal Squamous Cell Carcinoma. Int J Radiat Oncol Biol Phys. 2023;115(4):957–971. doi:10.1016/j.ijrobp.2022.10.028
100. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454(7203):436–444. doi:10.1038/nature07205
101. Kumari N, Dwarakanath BS, Das A, Bhatt AN. Role of interleukin-6 in cancer progression and therapeutic resistance. Tumour Biol. 2016;37(9):11553–11572. doi:10.1007/s13277-016-5098-7
102. Laha D, Grant R, Mishra P, Nilubol N. The Role of Tumor Necrosis Factor in Manipulating the Immunological Response of Tumor Microenvironment. Front Immunol. 2021;12:656908. doi:10.3389/fimmu.2021.656908
103. Magne N, Toillon RA, Bottero V, et al. NF-kappaB modulation and ionizing radiation: mechanisms and future directions for cancer treatment. Cancer Lett. 2006;231(2):158–168. doi:10.1016/j.canlet.2005.01.022
104. Bergerud KMB, Berkseth M, Pardoll DM, et al. Radiation Therapy and Myeloid-Derived Suppressor Cells: breaking Down Their Cancerous Partnership. Int J Radiat Oncol Biol Phys. 2024;119(1):42–55. doi:10.1016/j.ijrobp.2023.11.050
105. Yi M, Li T, Niu M, et al. Targeting cytokine and chemokine signaling pathways for cancer therapy. Signal Transduct Target Ther. 2024;9(1):176. doi:10.1038/s41392-024-01868-3
106. Li H, Wang S, Li X, et al. CDCA7 promotes TGF-beta-induced epithelial-mesenchymal transition via transcriptionally regulating Smad4/Smad7 in ESCC. Cancer Sci. 2023;114(1):91–104. doi:10.1111/cas.15560
107. Ermakov MS, Nushtaeva AA, Richter VA, Koval OA. Cancer-associated fibroblasts and their role in tumor progression. Vavilovskii Zhurnal Genet Selektsii. 2022;26(1):14–21. doi:10.18699/VJGB-22-03
108. Zhao Q, Huang L, Qin G, et al. Cancer-associated fibroblasts induce monocytic myeloid-derived suppressor cell generation via IL-6/exosomal miR-21-activated STAT3 signaling to promote cisplatin resistance in esophageal squamous cell carcinoma. Cancer Lett. 2021;518:35–48. doi:10.1016/j.canlet.2021.06.009
109. Ou Y, Zhang Q, Tang Y, et al. DNA methylation enzyme inhibitor RG108 suppresses the radioresistance of esophageal cancer. Oncol Rep. 2018;39(3):993–1002. doi:10.3892/or.2018.6210
110. Klug F, Prakash H, Huber PE, et al. Low-dose irradiation programs macrophage differentiation to an iNOS(+)/M1 phenotype that orchestrates effective T cell immunotherapy. Cancer Cell. 2013;24(5):589–602. doi:10.1016/j.ccr.2013.09.014
111. Zhu L, Hu S, Chen Q, et al. Macrophage contributes to radiation-induced anti-tumor abscopal effect on transplanted breast cancer by HMGB1/TNF-alpha signaling factors. Int J Biol Sci. 2021;17(4):926–941. doi:10.7150/ijbs.57445
112. Nabrinsky E, Macklis J, Bitran J. A Review of the Abscopal Effect in the Era of Immunotherapy. Cureus. 2022;14(9):e29620. doi:10.7759/cureus.29620
113. Liu Y, Dong Y, Kong L, Shi F, Zhu H, Yu J. Abscopal effect of radiotherapy combined with immune checkpoint inhibitors. J Hematol Oncol. 2018;11(1):104. doi:10.1186/s13045-018-0647-8
114. Demaria S, Guha C, Schoenfeld J, et al. Radiation dose and fraction in immunotherapy: one-size regimen does not fit all settings, so how does one choose? J Immunother Cancer. 2021;9(4):1. doi:10.1136/jitc-2020-002038
115. Zhang H, Liu L, Liu J, et al. Roles of tumor-associated macrophages in anti-PD-1/PD-L1 immunotherapy for solid cancers. Mol Cancer. 2023;22(1):58. doi:10.1186/s12943-023-01725-x
116. Sobhani N, Tardiel-Cyril DR, Davtyan A, Generali D, Roudi R, Li Y. CTLA-4 in Regulatory T Cells for Cancer Immunotherapy. Cancers. 2021;13(6):1440. doi:10.3390/cancers13061440
117. Voronova V, Vislobokova A, Mutig K, et al. Combination of immune checkpoint inhibitors with radiation therapy in cancer: a hammer breaking the wall of resistance. Front Oncol. 2022;12:1035884. doi:10.3389/fonc.2022.1035884
118. Lai H, Liu Y, Wu J, et al. Targeting cancer-related inflammation with non-steroidal anti-inflammatory drugs: perspectives in pharmacogenomics. Front Pharmacol. 2022;13:1078766. doi:10.3389/fphar.2022.1078766
119. Maghsoudi H, Sheikhnia F, Sitarek P, et al. The Potential Preventive and Therapeutic Roles of NSAIDs in Prostate Cancer. Cancers. 2023;15(22):5435. doi:10.3390/cancers15225435
120. Page TH, Turner JJ, Brown AC, et al. Nonsteroidal anti-inflammatory drugs increase TNF production in rheumatoid synovial membrane cultures and whole blood. J Immunol. 2010;185(6):3694–3701. doi:10.4049/jimmunol.1000906
121. Cerniglia GJ, Pore N, Tsai JH, et al. Epidermal growth factor receptor inhibition modulates the microenvironment by vascular normalization to improve chemotherapy and radiotherapy efficacy. PLoS One. 2009;4(8):e6539. doi:10.1371/journal.pone.0006539
122. Li X, Su X, Yan C, et al. Role of vascular endothelial growth factor in radiotherapy resistance to esophageal squamous cell carcinoma. J Cancer Res Clin Oncol. 2023;149(6):2543–2550. doi:10.1007/s00432-022-04122-x
123. Tang Q, Chen Y, Li X, et al. The role of PD-1/PD-L1 and application of immune-checkpoint inhibitors in human cancers. Front Immunol. 2022;13:964442. doi:10.3389/fimmu.2022.964442
124. Budimir N, Thomas GD, Dolina JS, Salek-Ardakani S. Reversing T-cell Exhaustion in Cancer: lessons Learned from PD-1/PD-L1 Immune Checkpoint Blockade. Cancer Immunol Res. 2022;10(2):146–153. doi:10.1158/2326-6066.CIR-21-0515
125. Wei H, Li Y, Guo Z, et al. Comparison of dynamic changes in the peripheral CD8(+) T cells function and differentiation in ESCC patients treated with radiotherapy combined with anti-PD-1 antibody or concurrent chemoradiotherapy. Front Immunol. 2022;13:1060695. doi:10.3389/fimmu.2022.1060695
126. Yang Y, Ge H. Effective combinations of radiotherapy and immunotherapy in the treatment of esophageal squamous cell carcinoma. Future Oncol. 2020;16(31):2537–2549. doi:10.2217/fon-2020-0222
127. Zhang Y, Li Z, Huang Y, Xu Y, Zou B. Advancements in immunotherapy for advanced esophageal squamous cell carcinoma: a comprehensive review of current strategies and future directions. Expert Rev Clin Immunol. 2024;20(8):971–984. doi:10.1080/1744666X.2024.2368194
128. Chan HW, Kuo DY, Shueng PW, Chuang HY. Visualizing the Tumor Microenvironment: molecular Imaging Probes Target Extracellular Matrix, Vascular Networks, and Immunosuppressive Cells. Pharmaceuticals. 2024;17(12):1663. doi:10.3390/ph17121663
129. Gupta A, Probst HC, Vuong V, et al. Radiotherapy promotes tumor-specific effector CD8+ T cells via dendritic cell activation. J Immunol. 2012;189(2):558–566. doi:10.4049/jimmunol.1200563
130. Sanghera C, McClurg DP, Jones CM. Systematic Review of Hypofractionated Radiation Therapy for the Treatment of Oesophageal Squamous Cell Carcinoma and Oesophageal Adenocarcinoma. Clin Oncol. 2024;36(7):430–444. doi:10.1016/j.clon.2024.03.020
131. Chen M, Lu H, Copley SJ, et al. A Novel Radiogenomics Biomarker for Predicting Treatment Response and Pneumotoxicity From Programmed Cell Death Protein or Ligand-1 Inhibition Immunotherapy in NSCLC. J Thorac Oncol. 2023;18(6):718–730. doi:10.1016/j.jtho.2023.01.089
132. Yin Z, Zhang H, Zhang K, et al. Impacts of combining PD-L1 inhibitor and radiotherapy on the tumour immune microenvironment in a mouse model of esophageal squamous cell carcinoma. BMC Cancer. 2025;25(1):474. doi:10.1186/s12885-025-13801-0
133. Zhang Y, Y-d L, Y-l L, et al. Prognostic Value of Lymphocyte Activation Gene-3 (LAG-3) Expression in Esophageal Squamous Cell Carcinoma. J Cancer. 2018;9(22):4287–4293. doi:10.7150/jca.26949
134. Zhao Y, Chen D, Wang W, et al. Significance of TIM-3 Expression in Resected Esophageal Squamous Cell Carcinoma. Ann Thorac Surg. 2020;109(5):1551–1557. doi:10.1016/j.athoracsur.2019.12.017
135. Gupta N, Ochiai H, Hoshino Y, et al. Inhibition of CXCR4 Enhances the Efficacy of Radiotherapy in Metastatic Prostate Cancer Models. Cancers. 2023;15(4):1021. doi:10.3390/cancers15041021
136. Chen X, Wang L, Li P, et al. Dual TGF-beta and PD-1 blockade synergistically enhances MAGE-A3-specific CD8(+) T cell response in esophageal squamous cell carcinoma. Int, J, Cancer. 2018;143(10):2561–2574. doi:10.1002/ijc.31730
137. Yu S, Yin JJ, Miao JX, et al. Activation of NLRP3 inflammasome promotes the proliferation and migration of esophageal squamous cell carcinoma. Oncol Rep. 2020;43(4):1113–1124. doi:10.3892/or.2020.7493
138. Wu C, Zhang Y, Wang Y, Wang Q, Wang S. Multi-Modal Intermediate Feature Interaction Autoencoder for Overall Survival Prediction of Esophageal Squamous Cell Cancer. In: 2024 IEEE International Symposium on Biomedical Imaging. 2024:1–5.
139. Suntharalingam M, Winter K, Ilson D, et al. Effect of the Addition of Cetuximab to Paclitaxel, Cisplatin, and Radiation Therapy for Patients With Esophageal Cancer: the NRG Oncology RTOG 0436 Phase 3 Randomized Clinical Trial. JAMA Oncol. 2017;3(11):1520–1528. doi:10.1001/jamaoncol.2017.1598
140. Wei X-L, Wang F-H, Zhang D-S, et al. A novel inflammation-based prognostic score in esophageal squamous cell carcinoma: the C-reactive protein/albumin ratio. BMC Cancer. 2015;15(1):350. doi:10.1186/s12885-015-1379-6
141. Mela E, Tsapralis D, Papaconstantinou D, et al. Current Role of Artificial Intelligence in the Management of Esophageal Cancer. J Clin Med. 2025;14(6):1845. doi:10.3390/jcm14061845
142. Han Y, Zhu X, Hu Y, et al. Electronic Health Record–Based Absolute Risk Prediction Model for Esophageal Cancer in the Chinese Population: model Development and External Validation. JMIR Public Health Surveill. 2023;9:e43725. doi:10.2196/43725
143. Wu L, Li B, Wan G, et al. Toripalimab plus chemotherapy and radiotherapy for treatment-naive advanced esophageal squamous cell carcinoma: a single-arm phase 2 trial. Nat Commun. 2024;15(1):7116. doi:10.1038/s41467-024-51105-2
144. Lu Y, Wang W, Wang F. Clinical benefits of PD-1 inhibitors in specific subgroups of patients with advanced esophageal squamous cell carcinoma: a systematic review and meta-analysis of phase 3 randomized clinical trials. Front Immunol. 2023;14:1171671. doi:10.3389/fimmu.2023.1171671
145. Tengesdal IW, Dinarello CA, Marchetti C. NLRP3 and cancer: pathogenesis and therapeutic opportunities. Pharmacol Ther. 2023;251:108545. doi:10.1016/j.pharmthera.2023.108545
146. Xie Y, Liu Q, Ji C, et al. An artificial neural network-based radiomics model for predicting the radiotherapy response of advanced esophageal squamous cell carcinoma patients: a multicenter study. Sci Rep. 2023;13(1):8673. doi:10.1038/s41598-023-35556-z
147. Salari E, Wang J, Wynne JF, Chang CW, Wu Y, Yang X. Artificial intelligence-based motion tracking in cancer radiotherapy: a review. J Appl Clin Med Phys. 2024;25(11):e14500. doi:10.1002/acm2.14500
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Novel Predictor of Pathologic Complete Response for Neoadjuvant Immunochemotherapy in Resectable Locally Advanced Esophageal Squamous Cell Carcinoma
Yang Y, Xin D, Wang H, Guan L, Meng X, Lu T, Bai X, Wang F
Journal of Inflammation Research 2023, 16:1443-1455
Published Date: 5 April 2023