")
Back to Journals » Journal of Inflammation Research » Volume 18
Dynamic Trends of Albumin-to-C-Reactive Protein Ratio: A Prognostic Indicator in Elderly Patients with Community-Acquired Pneumonia
Authors Miao L, Gong C, Liao J , Xie C, Shen X, Cheng Y
Received 11 January 2025
Accepted for publication 14 March 2025
Published 19 March 2025 Volume 2025:18 Pages 4195—4211
DOI https://doi.org/10.2147/JIR.S512632
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Tara Strutt
Lei Miao,1,* Chen Gong,2,* Jingxian Liao,2 Chunhui Xie,2 Xiaozhu Shen,2 Yajuan Cheng1
1Department of Critical Care Medicine, The second People’s Hospital of Lianyungang, Lianyungang, 222000, People’s Republic of China; 2Department of Geriatrics, The second People’s Hospital of Lianyungang, Lianyungang, 222000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jingxian Liao, Email [email protected] Yajuan Cheng, Email [email protected]
Background: The prognostic significance of dynamic changes in the albumin-to-C-reactive protein ratio (ACR) in elderly patients with community-acquired pneumonia (CAP) has not been fully elucidated. This study aims to evaluate the utility of ACR as a dynamic biomarker for predicting 28-day mortality and enhancing risk stratification in this high-risk population.
Methods: A retrospective cohort study was conducted on 437 elderly CAP patients (≥ 65 years). Serum albumin and C-reactive protein (CRP) levels were measured at admission (T0), 24 hours (T1), and 3 days (T2) post-admission. ACR was calculated for each time point, and its prognostic value was assessed using advanced statistical methods.
Results: The 28-day mortality rate was 16.7%. ACR levels were consistently lower in non-survivors across all time points (P < 0.001). RCS analysis revealed a nonlinear relationship between ACR and mortality risk. Time-varying ROC analysis demonstrated that ACR consistently outperformed CRP in predicting mortality, with superior area under the curve (AUC) values at all time points. Random-effects modeling indicated minimal inter-individual variability in ACR (random effects variance: 0.030; standard deviation: 0.175). Time-varying Cox regression confirmed a strong negative association between dynamic ACR changes and mortality risk, with a C-statistic of 0.833 (P < 0.001).
Conclusion: Dynamic monitoring of ACR is a robust and clinically applicable tool for predicting short-term mortality in elderly CAP patients. By integrating markers of inflammation and nutritional status, ACR facilitates early identification of high-risk patients and supports personalized treatment strategies. These findings highlight the potential of ACR as a novel biomarker for improving clinical outcomes in this vulnerable population.
Keywords: elderly, community-acquired pneumonia, albumin-to-C-reactive protein ratio, dynamic monitoring, prognosis
Introduction
Community-acquired pneumonia (CAP) is a significant cause of morbidity and mortality in the elderly population, posing substantial clinical and public health challenges.1 While CAP affects individuals across all age groups, its impact on elderly patients is disproportionately severe due to age-related immune decline, underlying comorbidities, and differences in causative pathogens.2 The pathophysiology of CAP in older adults is particularly complex, involving microbial infections, dysregulated inflammatory responses, and immune dysfunction.3 Immunosenescence, or the age-related decline in immune function, coupled with a high prevalence of chronic conditions such as diabetes, chronic obstructive pulmonary disease (COPD), and cardiovascular diseases, renders older adults highly vulnerable to severe disease and poor outcomes.4 Furthermore, the clinical presentation of CAP in the elderly is often atypical, such as the absence of fever or cough, leading to delayed diagnosis and treatment, which further exacerbates mortality risks.5 Early identification of high-risk patients and timely interventions are therefore critical for improving outcomes in this vulnerable population.
Inflammation and nutritional status are increasingly recognized as key factors influencing CAP prognosis.6 Excessive immune activation in response to pathogens, often manifesting as a “cytokine storm”, plays a central role in disease progression, particularly in elderly patients.7 C-reactive protein (CRP), a well-established acute-phase inflammatory biomarker, has been widely utilized for diagnosing and predicting outcomes in infectious diseases.8 However, CRP alone has limited prognostic value in elderly CAP patients, as it does not adequately capture their nutritional status or chronic inflammatory burden.9 Malnutrition, particularly hypoalbuminemia, has been identified as a critical risk factor for poor outcomes in this population.10 Albumin, a key marker of nutritional status, also exhibits antioxidant, anti-inflammatory, and immune-modulating properties, with lower levels consistently associated with higher mortality risk.11
To address the limitations of single biomarkers, the albumin-to-CRP ratio (ACR) has recently been proposed as a composite indicator that integrates information on both inflammation and nutritional status.12,13 ACR offers a more comprehensive assessment of a patient’s pathophysiological state. Previous studies have demonstrated the prognostic significance of ACR in various conditions, including cardiovascular diseases, cancer, and infectious diseases.14,15 For instance, recent evidence indicates that lower ACR levels are strongly associated with higher mortality in critically ill CAP patients, suggesting its potential as a sensitive prognostic tool.16 Specifically, little is known about the dynamic changes in ACR during the early stages of treatment and their association with mortality risk. This knowledge gap is particularly relevant in elderly CAP patients, where the interplay between inflammation and malnutrition is complex and dynamic.
This study aims to address these gaps by investigating the dynamic changes in ACR during the early treatment stages of elderly CAP patients and their association with 28-day mortality. Unlike previous studies that relied on single-point measurements, this research focuses on ACR trends at multiple time points—admission (T0), 24 hours post-admission (T1), and 3 days post-admission (T2)—to provide a more nuanced understanding of its prognostic value. By integrating dynamic inflammation and nutritional markers, this study seeks to clarify the role of ACR as a sensitive and practical biomarker for risk stratification in elderly CAP patients. The findings offer a novel perspective on how dynamic ACR monitoring can inform clinical decision-making and guide individualized treatment strategies. Early recognition of high-risk patients through ACR monitoring may enable timely interventions, ultimately improving outcomes in this vulnerable population.
Methods
Study Design and Patients
This single-center, retrospective cohort study was conducted at the Second People’s Hospital of Lianyungang from June 2019 to June 2024. We included patients aged 65 years or older who were hospitalized with CAP and followed up for 28 days after admission. Clinical data were extracted from the hospital’s electronic medical record system and included demographic information, clinical characteristics, laboratory findings, microbiological results, comorbidities, and clinical outcomes.
Definition of CAP
The diagnosis of CAP was based on the criteria outlined in the guidelines of the American Thoracic Society (ATS) and Infectious Diseases Society of America (IDSA).17 Specifically, CAP was defined as the presence of newly acquired respiratory symptoms (eg, cough, sputum production, dyspnea, or chest pain), accompanied by at least one systemic symptom (eg, fever, chills, or leukocytosis), and supported by chest radiographic confirmation of new infiltrates consistent with pneumonia. These criteria excluded patients with hospital-acquired pneumonia, ventilator-associated pneumonia, or other noninfectious causes of pulmonary infiltrates.
Inclusion Criteria
1. Age ≥65 years.
2. Diagnosis of CAP according to the ATS/IDSA CAP guidelines.17
3. Availability of comprehensive laboratory data, including serum albumin and CRP measurements.
4. Hospital stay of ≥ 3 days to ensure the collection of dynamic data.
Exclusion Criteria
1. Diagnosis of hospital-acquired pneumonia.
2. Liver dysfunction classified as Child-Pugh Grade C.
3. End-stage renal disease requiring long-term dialysis.
4. Immunosuppressed state, including patients with HIV infection, those on long-term immunosuppressive therapy, or corticosteroid treatment (≥ 20 mg/day for ≥ 2 weeks).
5. Terminal-stage malignant tumors.
6. Missing critical data, such as serum albumin and CRP at key time points.
Ethics Approval
The study was approved by the Ethics Committee of the Second People’s Hospital of Lianyungang (Approval No. 2022K040) and adhered to the ethical principles outlined in the Declaration of Helsinki. As this was a retrospective study utilizing pre-existing clinical data without direct patient intervention, the requirement for informed consent was waived by the Ethics Committee.
Data Collection
Trained researchers extracted clinical data from the hospital’s electronic medical record system. The collected data included:
Demographic Information: Gender and age.
Clinical Characteristics: Body mass index (BMI),18 Charlson Comorbidity Index (CCI)19 to assess comorbidities, and pathogen information.
Vital Signs: Heart rate (HR), systolic blood pressure (SBP), and diastolic blood pressure (DBP).
Nutritional Assessment: Mini Nutritional Assessment-Short Form (MNA-SF) score to evaluate nutritional status.
Laboratory Data: Serum albumin and CRP levels measured on the day of admission (T0), 24 hours after admission (T1), and three days after admission (T2). Additional laboratory parameters included white blood cell count (WBC), platelet count (PLT), hemoglobin (HB), aspartate aminotransferase (AST), alanine aminotransferase (ALT), blood urea nitrogen (BUN), and blood glucose (Glu).
Clinical Outcomes: Survival or death within the 28-day follow-up period.
Underlying Diseases and Microbiological Data
Patient data regarding underlying diseases were extracted from the hospital electronic medical record system and admission notes. The following comorbidities were evaluated: diabetes mellitus, chronic obstructive pulmonary disease (COPD), cardiovascular diseases (eg, hypertension, coronary artery disease), chronic kidney disease, cerebrovascular disease, and others.
The microbiological data for this study were retrospectively collected from the electronic medical record system of the hospital. Data included results from routine microbiological tests performed during hospitalization, recorded as part of standard clinical care. These tests aimed to identify potential pathogens associated with CAP and included bacterial, fungal, and viral pathogens. Microbiological results were obtained from respiratory samples (eg, sputum, bronchoalveolar lavage fluid), blood cultures, and urinary antigen tests. Additionally, for viral pathogens, nasopharyngeal or throat swab samples collected during admission were tested for respiratory viruses including: COVID-19 (SARS-CoV-2), identified using reverse transcription polymerase chain reaction (RT-PCR) in line with standard clinical protocols, and Influenza viruses (A and B), identified by either RT-PCR or rapid antigen detection tests.
Only microbiological test results obtained within the first 48 hours of admission were included in this study to ensure that the data represented pathogens associated with community-acquired infections rather than hospital-acquired infections.
Nutritional Assessment
Nutritional status was assessed using the Mini Nutritional Assessment-Short Form (MNA-SF), a validated screening tool specifically designed for elderly patients.20 The MNA-SF consists of six items evaluating key aspects of nutritional health, with a total score ranging from 0 to 14. Based on the total score, patients were classified into three categories: (1) 12–14 points: Normal nutritional status; (2) 8–11 points: At risk of malnutrition; (3) 0–7 points: Malnutrition. All assessments were conducted by trained healthcare professionals upon patient admission.
Albumin/CRP Ratio Calculation
The ACR was calculated for each patient at each time point using the formula:ACR = serum albumin (g/L) / serum CRP (mg/L).21 All laboratory measurements were performed in the hospital’s clinical laboratory department following standardized operating procedures and quality control protocols.
Missing Data Handling
In this study, the proportion of missing data was low (<5%) and primarily classified as missing completely at random (MCAR). To address this, multiple imputation was employed to handle random missing values. Variables included in the imputation process were demographic information (eg, age, gender), clinical characteristics (eg, BMI, Charlson Comorbidity Index), laboratory parameters (eg, serum albumin, CRP), and 28-day survival status. The imputation was performed using a multivariate regression model, generating five imputed datasets, and the results were pooled for subsequent analyses. For systematic missingness, such as data loss at later time points due to early death, a competing risks model was utilized to minimize bias.
Statistical Analysis
All statistical analyses were conducted using SPSS Statistics version 21.0 and R software version 4.4.1. The normality of continuous variables was assessed using the Shapiro–Wilk test. Variables with a normal distribution were expressed as mean ± standard deviation (SD), while non-normally distributed variables were presented as median and interquartile range (IQR). Categorical variables were summarized as counts and percentages. Comparisons of continuous variables with a normal distribution were performed using the independent samples t-test, while the Mann–Whitney U-test was used for non-normally distributed data. Categorical variables were analyzed using the chi-square test or Fisher’s exact test, as appropriate.
To investigate the nonlinear relationship between the ACR and mortality risk, restricted cubic spline (RCS) regression analysis was employed. The dynamic trends of CRP and ACR over time were evaluated using linear mixed-effects models, which included fixed effects (time points and survival status), random effects (individual variability), and interaction terms between time and survival status to assess differences in trajectories between groups.
The prognostic performance of CRP and ACR at various time points was assessed using receiver operating characteristic (ROC) curve analysis. The area under the ROC curve (AUC) was calculated for each biomarker, with higher AUC values indicating superior discriminatory ability. Differences between AUCs were statistically compared using the DeLong test. To further evaluate the predictive accuracy of CRP and ACR over time, time-dependent ROC curve analyses were conducted at days 10, 15, and 25, employing a cumulative/dynamic approach to account for data censoring and changes in follow-up duration.
The relationship between dynamic ACR changes and 28-day mortality was assessed using Cox proportional hazards regression. Hazard ratios (HRs) with 95% confidence intervals (CIs) were calculated for univariate and multivariate analyses. Subgroup analyses explored the effects of dynamic ACR changes across patient categories. The goodness-of-fit of the Cox regression model was assessed using Harrell’s concordance index (C-statistic). All statistical tests were two-sided, and a P-value < 0.05 was considered statistically significant.
Results
Clinical Characteristics Across Groups
A total of 437 elderly patients diagnosed with CAP were included in the study based on the predefined inclusion and exclusion criteria, as illustrated in Figure 1. The overall 28-day mortality rate was 16.7%. The clinical characteristics of the survival and deceased groups are summarized in Table 1. No significant differences were observed in gender distribution between the two groups. However, the mean age of the deceased group (81.10 ± 5.44 years) was significantly higher than that of the survival group (76.99 ± 6.52 years, P < 0.001). Although body mass index (BMI) did not differ significantly between the groups, nutritional status assessments revealed notable differences. The Mini Nutritional Assessment-Short Form (MNA-SF) score in the deceased group was significantly lower than that in the survival group (P < 0.001), with a higher proportion of malnourished patients (MNA-SF ≤ 7) in the deceased group (64.4%) compared to the survival group (21.4%, P < 0.001). The Charlson Comorbidity Index (CCI), which reflects the burden of comorbidities, was significantly higher in the deceased group than in the survival group (P < 0.001).
 |
Table 1 Clinical Characteristics Across Groups |
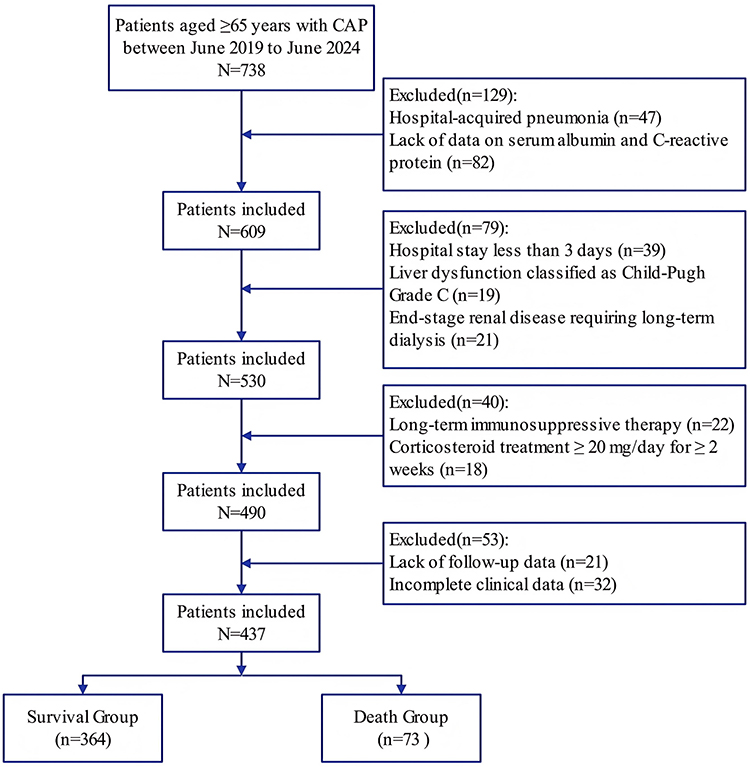 |
Figure 1 Flow diagram displaying the progress of all participants through the study. |
The levels of CRP were significantly higher in the deceased group compared to the survival group at all three time points: T0, T1, and T2 (P < 0.001). Conversely, serum albumin levels were significantly lower in the deceased group than in the survival group at the same time points (P < 0.001). The ACR, a composite indicator of nutritional and inflammatory status, was markedly lower in the deceased group compared to the survival group at T0, T1, and T2 (P < 0.001). Figure 2 illustrates the differences in CRP levels (Figure 2A) and ACR levels (Figure 2B) between the survival and deceased groups at three time points: T0 (admission), T1 (24 hours post-admission), and T2 (3 days post-admission). CRP levels were consistently higher in the deceased group across all time points, indicating a stronger inflammatory response. Conversely, ACR levels were significantly lower in the deceased group, reflecting poorer nutritional and inflammatory status.
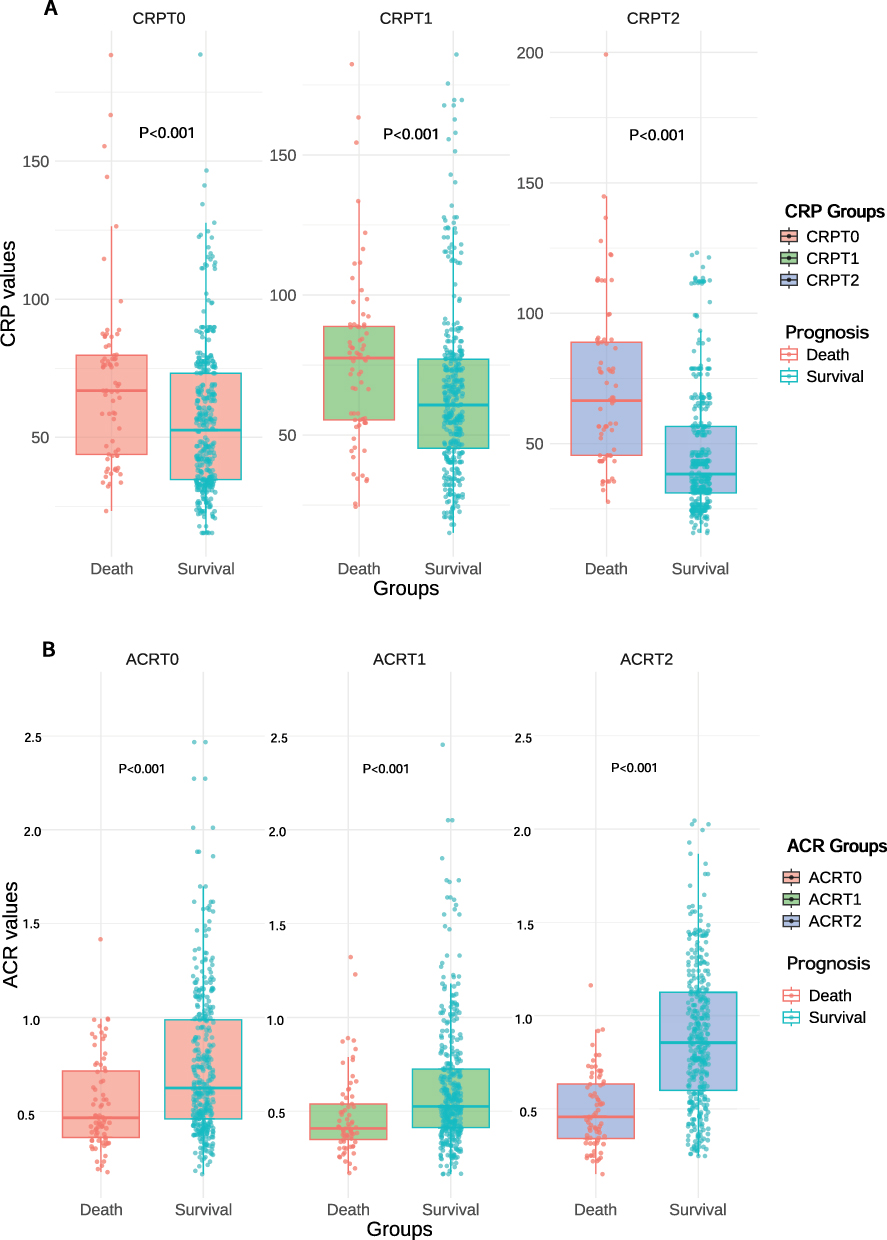 |
Figure 2 Comparison of CRP (A) and ACR (B) between different prognostic groups. Abbreviations: CRP, C-reactive protein; ACR, Albumin-to-C-reactive protein ratio; T0, On the day of admission; T1, 24 hours after admission; T2, 3 days after admission. Notes: (A) shows the median CRP levels at T0, T1, and T2 for the survival and deceased groups. CRP levels were consistently higher in the deceased group across all time points (P < 0.001). (B) illustrates the median ACR levels at T0, T1, and T2 for the survival and deceased groups. Statistical significance was determined using the Mann–Whitney U-test. |
Non-Linear Association Between Dynamic Changes in ACR and Mortality Risk
Using restricted cubic spline (RCS) analysis, we evaluated the relationship between the ACR and mortality risk (expressed as Odds Ratio, OR) while density curves illustrated the distribution of ACR values. At admission (T0), a significant nonlinear relationship was observed between ACR values and mortality risk. As ACR values increased, OR values declined markedly, indicating that higher ACR values were associated with a reduced mortality risk. Specifically, when ACR increased from 0.5 to 1.5, OR values decreased from approximately 1 to 0.5, demonstrating a protective effect (Figure 3A). The density curve revealed that ACR values at T0 were relatively concentrated, primarily ranging between 0.5 and 1.5. At 24 hours after admission (T1), the nonlinear relationship between ACR and mortality risk persisted, but the trend exhibited a notable change. As ACR values increased, OR values initially decreased, followed by an upward trend, suggesting that excessively high ACR values might be associated with increased mortality risk (Figure 3B). The density curve showed a more dispersed distribution of ACR values at T1 compared to T0, extending from 0.5 to 2.5. At 3 days after admission (T2), the relationship between ACR and mortality risk became more complex. OR values significantly decreased when ACR values were low (<1.0) but tended to stabilize when ACR values exceeded 1.5 (Figure 3C). This suggests that in the early stages of treatment, increases in ACR values were associated with a significant reduction in mortality risk, though the impact diminished at later stages. The density curve at T2 indicated a more uniform distribution of ACR values, primarily ranging from 0.5 to 2.0.
 |
Figure 3 The relationship between ACR and mortality risk across the three time points. Abbreviations: CRP, C-reactive protein; ACR, Albumin-to-C-reactive protein ratio; T0, On the day of admission; T1, 24 hours after admission; T2, 3 days after admission. Notes: (A) ACR at T0 and its association with OR. (B) ACR at T1 and its association with OR. (C) ACR at T2 and its association with OR. The blue line represents the estimated OR for mortality associated with different ACR values, and the shaded area indicates the 95% CI. The red dashed line denotes the ACR threshold, which serves as the cutoff point for comparing the association between ACR levels and mortality risk. The gray curve represents the density distribution of ACR values in the population. |
Dynamic Trends of Predicted CRP Values
This study analyzed the trends in predicted CRP values, stratified by survival status into the survival and death groups, and assessed them at three time points (T0, T1, T2). The linear mixed-effects model revealed significant differences in CRP values across time points and between prognostic groups. Specifically, CRP values significantly increased at T1, rising by 9.15 compared to baseline (T0, P < 0.001), and then significantly decreased at T2, dropping by 9.33 compared to T1 (P < 0.001). Additionally, CRP values in the death group were significantly higher than those in the survival group, with an increase of 13.70 (P < 0.001). Interaction effects revealed that at T2, CRP values in the death group were significantly higher than in the survival group, with an increase of 12.04 (P = 0.004). These findings suggest that dynamic changes in CRP values are closely associated with patient prognosis (Figure 4A).
 |
Figure 4 Dynamic trends of predicted values for CRP (A) and ACR (B). Abbreviations: CRP, C-reactive protein; ACR, Albumin-to-C-reactive protein ratio; T0, On the day of admission; T1, 24 hours after admission; T2, 3 days after admission. |
Dynamic Trends of Predicted ACR Values
The trends in predicted ACR values were also analyzed using a linear mixed-effects model, which identified significant differences across time points and prognostic groups. ACR values significantly decreased at T1, dropping by 0.12 compared to T0 (P < 0.001), and then rebounded significantly at T2, increasing by 0.14 (P < 0.001). ACR values in the death group were consistently lower than those in the survival group, with a reduction of 0.21 (P < 0.001). Interaction effects showed that at T2, the ACR in the death group was significantly lower than in the survival group, with a decrease of 0.19 (P = 0.001). Random effects analysis indicated minimal variability in ACR values among individuals, with a random effects variance of 0.030 (standard deviation: 0.175), suggesting consistent changes across patients (Figure 4B).
ROC Curves for CRP and ACR in Prognostic Prediction
The prognostic predictive capabilities of CRP and ACR were evaluated at different time points in elderly patients with CAP. As shown in Figure 5, at T0, the area under the curve (AUC) for CRP was 0.650 (95% CI: 0.584–0.715). At T1, the AUC was 0.638 (95% CI: 0.569–0.708), and by T2, the AUC increased to 0.775 (95% CI: 0.723–0.826), indicating significantly improved predictive ability (P < 0.001). In contrast, the AUC for ACR at T0 was 0.664 (95% CI: 0.599–0.730), which slightly increased to 0.665 (95% CI: 0.599–0.731) at T1. By T2, the AUC for ACR rose significantly to 0.821 (95% CI: 0.776–0.865, P < 0.001), outperforming CRP in prognostic prediction (P < 0.001).
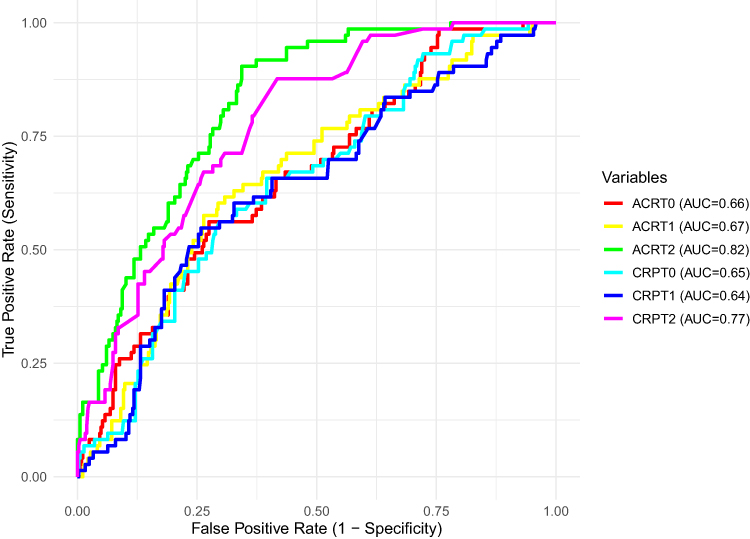 |
Figure 5 ROC curves for CRP and ACR at T0, T1, and T2. Abbreviations: CRP, C-reactive protein; ACR, Albumin-to-C-reactive protein ratio; ACU, Area under the curve; T0, On the day of admission; T1, 24 hours after admission; T2, 3 days after admission. |
Time-Dependent ROC Curve Analysis and AUC Values
In this study, the CRP levels and ACR on days 10, 15, and 25 were not directly measured values but rather predicted values generated based on a statistical model. The calculation of these predicted values aims to explore the dynamic changes of biomarkers and their potential prognostic significance. For the CRP model, the time-dependent AUC values were 0.528, 0.603, and 0.641 at D10, D15, and D25, respectively. In comparison, the time-dependent AUC values for the ACR model were 0.575, 0.631, and 0.655 at the corresponding time points (Figure 6).
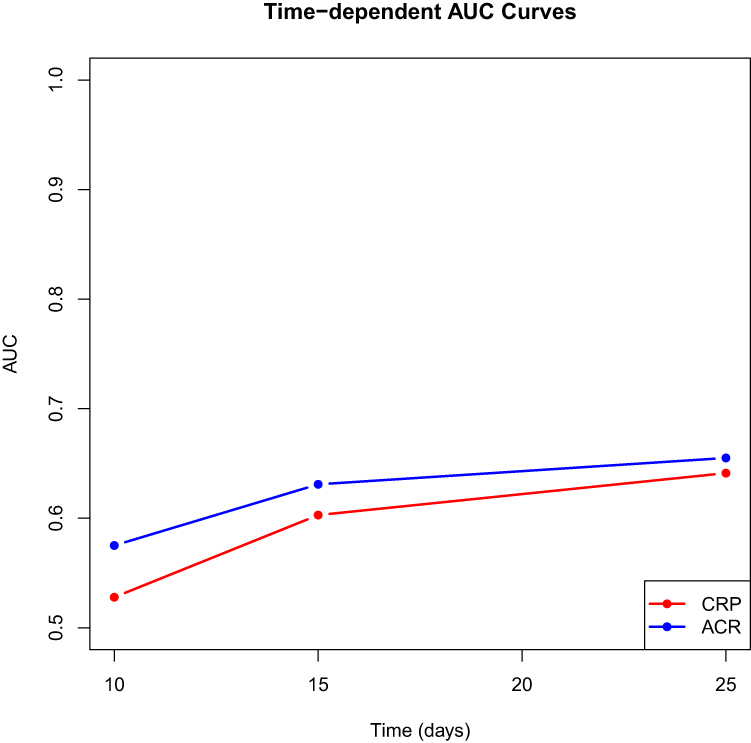 |
Figure 6 Time-dependent AUC values for CRP and ACR models at different time points. Abbreviations: CRP, C-reactive protein; ACR, Albumin-to-C-reactive protein ratio; ACU, Area under the curve. |
As shown in the time-varying ROC curve analysis (Figure 7), the predictive performance of the ACR model was consistently superior to that of the CRP model over time. At all key time points, the AUC for ACR exceeded that of CRP, highlighting the stronger prognostic predictive capability of ACR for monitoring dynamic disease progression.
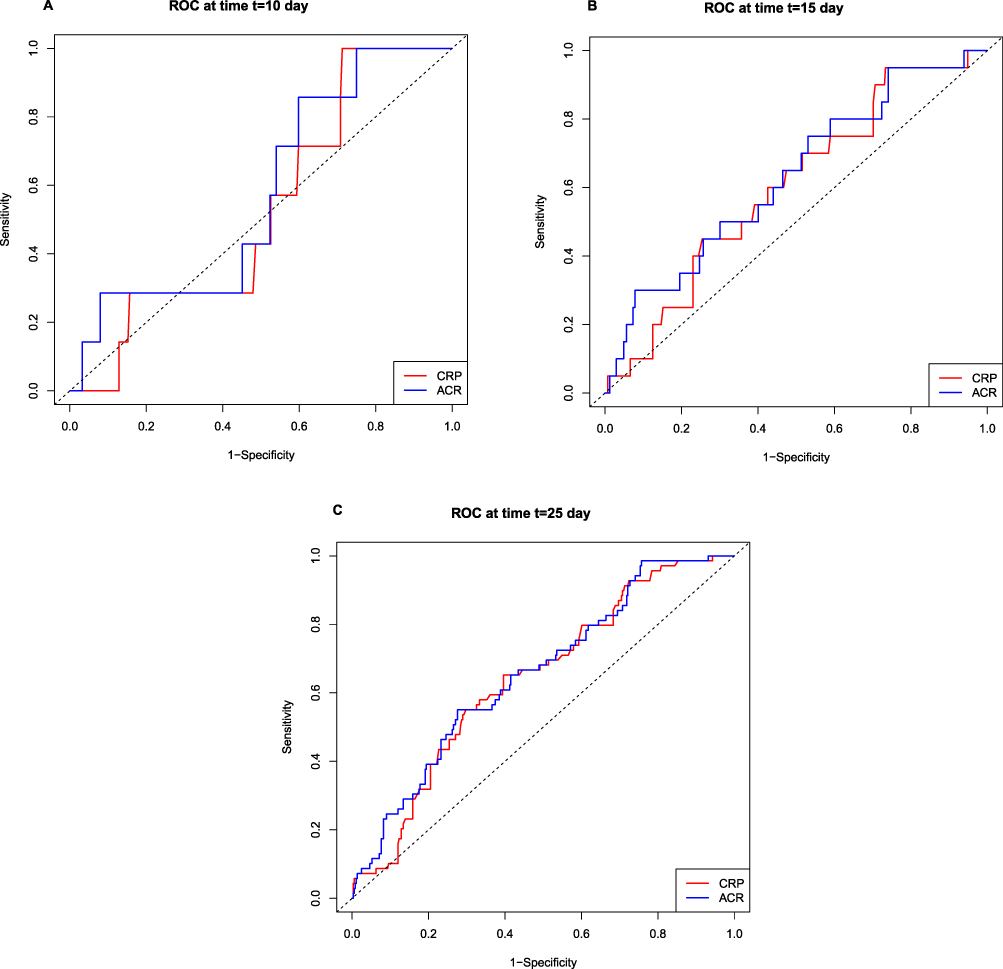 |
Figure 7 Time-dependent ROC curves for Day 10 (A), Day 15 (B), and Day 25 (C). Abbreviations: CRP, C-reactive protein; ACR, Albumin-to-C-reactive protein ratio. |
Cox Regression Analysis Results of ACR Dynamics by Subgroup
The relationship between dynamic ACR values and survival outcomes was evaluated across multiple subgroups using Cox proportional hazards models, as presented in Table 2. Covariates such as age, sex, diabetes, hypertension, and malnutrition were included in the analysis. Overall, ACR dynamic values exhibited a significant association with survival, with p < 0.001 in the global model. The C-statistic for the Cox model was 0.833 (standard error = 0.017), indicating excellent discriminative ability in predicting 28-day mortality (p < 0.001).
 |
Table 2 Cox Regression Analysis Results of ACR Dynamics by Subgroup |
Dynamic ACR values demonstrated a robust negative correlation with mortality risk across all subgroups. Women and elderly patients (≥85 years) showed the strongest association with reduced event risk, emphasizing the predictive importance of ACR dynamics in these populations. Additionally, the consistent significance observed across conditions such as hypertension, diabetes, and malnutrition further supports the universal applicability of ACR as a prognostic marker.
Discussion
This study evaluated dynamic changes in the ACR as a prognostic indicator among elderly patients with community-acquired pneumonia. The findings suggest that ACR may serve as a marker for predicting short-term mortality, reflecting both inflammatory and nutritional responses to infection.
Inflammation, Nutrition, and Prognosis in Elderly CAP Patients
The findings of this study align with existing evidence that inflammation and nutritional status play critical roles in the progression and outcomes of CAP, particularly in elderly patients.3 Upon pathogen invasion, the host immune system activates rapidly, releasing cytokines and inflammatory mediators to combat the infection.22 However, excessive inflammation can lead to tissue damage and organ dysfunction, particularly in elderly patients who experience age-related immune decline and heightened chronic inflammation.23 The severity of CAP has been shown to correlate with the intensity of inflammation, with persistent or excessive responses often predicting poor outcomes.24
Role of CRP and Albumin in CAP Diagnosis and Prognosis
CRP, a classical marker of acute-phase inflammation, is widely used in the diagnosis and monitoring of CAP.25 Synthesized by the liver, CRP levels rise rapidly in response to infection or tissue injury, reflecting the inflammatory burden and immune response intensity.26 However, CRP alone has limitations, as it does not account for nutritional status or chronic inflammation, both of which are critical in elderly patients.27,28
Serum albumin, a key plasma protein, is a sensitive indicator of nutritional status and is closely associated with chronic inflammation.29,30 In CAP patients, low Alb levels often indicate malnutrition, heightened inflammation, and increased mortality risk.31 Research has linked low Alb levels to adverse outcomes, including prolonged hospitalization, complications, and higher mortality rates.32 In elderly CAP patients, low Alb levels may reflect the cumulative effects of chronic inflammation and malnutrition. Therefore, combining Alb with CRP provides a more comprehensive assessment of a patient’s pathophysiological state.33
While our study primarily focuses on ACR’s prognostic role, these findings also underscore the potential utility of ACR in identifying high-risk patients earlier in the disease course. However, this application requires further validation in larger, prospective studies.
Significance of the Albumin-to-CRP Ratio
The ACR integrates inflammatory (CRP) and nutritional (Alb) markers, offering a unique advantage in assessing disease severity and prognosis.34,35 Compared to using CRP or Alb alone, the ACR may provide a more accurate representation of a patient’s overall health. Previous studies have highlighted the association between low ACR levels and higher mortality in critically ill patients.36 However, research specifically focusing on elderly CAP patients and the dynamic relationship between ACR and prognosis remains limited.
Our study addresses this gap by assessing the dynamic relationship between ACR and prognosis in elderly CAP patients. Unlike prior studies that relied on single time-point measurements, we monitored changes in ACR over time to evaluate their association with short-term prognosis. This approach provides insights into how ACR reflects disease progression and therapeutic response during hospitalization.
Dynamic Monitoring of ACR in Prognosis
Unlike prior studies that relied on single time-point measurements, this study innovatively employed dynamic monitoring of ACR changes to assess their relationship with short-term prognosis in elderly CAP patients. The results revealed that ACR levels in the mortality group were significantly lower at T1 (24 hours after admission) and remained lower at T2 (3 days after admission), despite slight improvement following treatment. This suggests that dynamic ACR changes may reflect disease progression and therapeutic response. Notably, ACR at T2 demonstrated the strongest predictive ability for mortality risk, highlighting the potential value of early dynamic monitoring in identifying high-risk patients. The linear mixed-effects model further confirmed the close association between ACR dynamics and survival status, with minimal inter-individual variability, highlighting the stability and consistency of ACR as a clinical indicator.
Host Conditions and Pathogens
Host factors, such as chronic comorbidities, age-associated immune decline, and pre-existing nutritional status, significantly influence inflammation and prognosis in elderly CAP patients. Chronic conditions such as diabetes and chronic obstructive pulmonary disease (COPD) are associated with heightened inflammation and impaired anabolic recovery, which may contribute to lower ACR values. Hypoalbuminemia, often exacerbated by comorbidities, reflects both nutritional depletion and heightened catabolism during infection. These factors collectively underscore the need to assess host conditions alongside ACR dynamics to contextualize their prognostic significance.
Although pathogen-specific data were not available in this study, previous research has shown that certain bacterial pathogens, such as Streptococcus pneumoniae and Klebsiella pneumoniae, are associated with more severe inflammatory responses and worse outcomes in CAP. Viral pathogens (eg, influenza, COVID-19) further modulate inflammatory responses and nutritional metabolism, which could also impact ACR dynamics. Future studies should incorporate detailed pathogen identification to better understand these interactions.
Clinical Implications of ACR
The ACR combines CRP, an acute-phase inflammatory marker, and Alb, a nutritional marker, to provide a comprehensive reflection of both acute inflammation and the patient’s nutritional and immune status.37 Elderly patients with CAP are particularly susceptible to immune dysregulation and excessive inflammatory responses due to immunosenescence and malnutrition.38 A decline in ACR may signify the body’s inability to effectively control inflammation while maintaining adequate nutritional and immune function, ultimately leading to adverse outcomes.
The findings of this study suggest that ACR may have potential as a prognostic tool for elderly CAP patients. Subgroup analyses revealed that the relationship between dynamic changes in ACR and mortality risk was more pronounced in females, older patients, and those with chronic conditions such as hypertension and diabetes. These populations may be more sensitive to fluctuations in inflammatory and nutritional status, highlighting the potential value of ACR as a prognostic indicator in these high-risk groups.39,40
This study further demonstrates the utility of ACR in clinical decision-making for elderly CAP patients. Dynamic ACR monitoring may improve risk stratification and guide personalized treatment strategies. For example, patients with declining ACR levels may benefit from early nutritional support, anti-inflammatory therapies, or interventions aimed at modulating immune responses. Additionally, the application of advanced statistical methods, such as time-dependent ROC curves and linear mixed-effects models, underscores the robustness of ACR as a prognostic indicator and its potential for broader applications in clinical research and practice.
From a practical clinical perspective, monitoring ACR dynamics provides practical, bedside-relevant insights into disease progression. ACR offers the advantage of integrating two critical dimensions of CAP prognosis: inflammation (CRP) and nutritional status (albumin). Dynamic ACR monitoring may help identify patients at higher risk of mortality earlier, allowing clinicians to escalate care, tailor anti-inflammatory therapies, or provide nutritional support as needed. For example, a persistent decline in ACR during the initial hospitalization period could prompt clinicians to consider intensive monitoring or transfer to an intensive care unit.
Limitations and Future Directions
Despite its strengths, this study has several limitations. First, the retrospective, single-center design may limit the generalizability of the findings, and the potential for selection bias cannot be excluded. Future studies should adopt prospective, multicenter designs to validate these results in diverse populations. Second, the reliance on electronic medical records may have led to incomplete data, which could affect the accuracy of the findings. Improved data collection and standardization are essential for future research.
In this study, we systematically explored the clinical characteristics and prognostic factors of elderly patients with CAP. However, we acknowledge several limitations. First, although comorbidities such as diabetes were included in the analysis, specific information regarding glycemic control, such as HbA1c levels, was not systematically available for all patients due to retrospective data collection. As glycemic control is an important factor in disease outcomes, future studies with detailed diabetes staging data are needed to explore its prognostic significance in CAP patients.
Additionally, this study did not explore the biological mechanisms underlying changes in ACR or account for potential confounding factors influencing its association with prognosis. Future research should focus on elucidating the interplay between inflammation, nutrition, and immune status in CAP progression. Investigating the impact of specific interventions, such as targeted nutritional support or anti-inflammatory therapies, on ACR dynamics and patient outcomes could further enhance its clinical utility.
Finally, we acknowledge the significant age differences observed between the survived and non-survived groups in our analysis. Age is a well-established prognostic factor in CAP, and the variation in age between these groups could introduce a confounding effect that may skew the results. Our findings indicate that although ACR dynamics are associated with mortality risk, the age-related risks cannot be overlooked and must be considered when interpreting the data. To enhance the robustness of future studies, it is important to stratify patients based on age or employ advanced statistical methods such as propensity score matching. This approach may help mitigate the impact of age-related confounding and yield clearer insights into the prognostic value of ACR dynamics. Additionally, larger sample sizes would be beneficial to ensure sufficient power for subgroup analyses.
Conclusion
This study demonstrates that dynamic monitoring of the ACR is a clinically relevant tool for assessing short-term mortality risk in elderly patients with CAP. By integrating markers of inflammation (CRP) and nutritional status (albumin), ACR provides an additional perspective on patient prognosis, complementing existing prognostic tools. Its dynamic changes offer a method for tracking disease progression and treatment response, with potential value for identifying high-risk patients who may benefit from timely nutritional and anti-inflammatory support.
Our findings suggest that dynamic ACR monitoring may improve risk stratification, particularly in vulnerable populations such as older adults, females, and those with chronic conditions like hypertension and diabetes. However, we recognize that while this study highlights the potential utility of ACR, its application should be interpreted cautiously and in conjunction with other clinical factors to avoid over-reliance on a single biomarker.
Importantly, this study builds on existing research by emphasizing the value of analyzing ACR trends over multiple time points, rather than relying solely on single time-point measurements. Despite these contributions, further research is needed to validate these findings in larger, multicenter cohorts and to explore the causal relationships between ACR dynamics, therapeutic interventions, and patient outcomes. Future studies should also address potential limitations, such as the retrospective design and the absence of disease-specific pathogen data, to better contextualize the role of ACR in clinical practice.
Data Sharing Statement
The datasets generated during the current study are available from the corresponding author (Jingxian Liao) upon reasonable request.
Ethics Approval
This study was approved by the Ethics Committee of the Second People’s Hospital of Lianyungang (Approval No. 2022K040). The Ethics Committee of the Second People’s Hospital of Lianyungang waived the requirement for informed consent due to the retrospective nature of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Lianyungang Aging Health Research Project (L202308), Health and Family Planning Commission of Lianyungang City (QN202210), Lianyungang City Cancer Prevention and Treatment Science and Technology Project (MS202408).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Aliberti S, Dela Cruz CS, Amati F, Sotgiu G, Restrepo MI. Community-acquired pneumonia. Lancet. 2021;398(10303):906–919. doi:10.1016/S0140-6736(21)00630-9
2. Quinton LJ, Walkey AJ, Mizgerd JP. Integrative physiology of pneumonia. Physiol Rev. 2018;98(3):1417–1464. doi:10.1152/physrev.00032.2017
3. Cillóniz C, Dominedò C, Pericàs JM, Rodriguez-Hurtado D, Torres A. Community-acquired pneumonia in critically ill very old patients: a growing problem. Eur Respir Rev. 2020;29(155):190126. doi:10.1183/16000617.0126-2019
4. Pieralli F, Vannucchi V, De Marzi G, et al. Performance status and in-hospital mortality of elderly patients with community acquired pneumonia. Intern Emerg Med. 2018;13(4):501–507. doi:10.1007/s11739-018-1822-1
5. Rombauts A, Abelenda-Alonso G, Cuervo G, Gudiol C, Carratalà J. Role of the inflammatory response in community-acquired pneumonia: clinical implications. Expert Rev Anti Infect Ther. 2022;20(10):1261–1274. doi:10.1080/14787210.2021.1834848
6. Brands X, Haak BW, Klarenbeek AM, et al. Concurrent immune suppression and hyperinflammation in patients with community-acquired pneumonia. Front Immunol. 2020;11:796. doi:10.3389/fimmu.2020.00796
7. Jarczak D, Nierhaus A. Cytokine Storm-Definition, Causes, and Implications. Int J mol Sci. 2022;23(19):11740. doi:10.3390/ijms231911740
8. Zheng N, Zhu D, Han Y. Procalcitonin and C-reactive protein perform better than the neutrophil/lymphocyte count ratio in evaluating hospital acquired pneumonia. BMC Pulm Med. 2020;20(1):166. doi:10.1186/s12890-020-01207-6
9. Ito A, Ishida T. Diagnostic markers for community-acquired pneumonia. Ann Transl Med. 2020;8(9):609. doi:10.21037/atm.2020.02.182
10. Wiedermann CJ. Hypoalbuminemia as surrogate and culprit of infections. Int J mol Sci. 2021;22(9):4496. doi:10.3390/ijms22094496
11. Kim H, Jo S, Lee JB, et al. Diagnostic performance of initial serum albumin level for predicting in-hospital mortality among aspiration pneumonia patients. Am J Emerg Med. 2018;36(1):5–11. doi:10.1016/j.ajem.2017.06.039
12. Liu Y, Gao Y, Liang B, Liang Z. The prognostic value of C-reactive protein to albumin ratio in patients with sepsis: a systematic review and meta-analysis. Aging Male. 2023;26(1):2261540. doi:10.1080/13685538.2023.2261540
13. Huang L, Zhang R, Ji J, et al. Hypersensitive C-reactive protein-albumin ratio is associated with stroke-associated pneumonia and early clinical outcomes in patients with acute ischemic stroke. Brain Behav. 2022;12(7):e2675. doi:10.1002/brb3.2675
14. Çağdaş M, Rencüzoğullari I, Karakoyun S, et al. Assessment of relationship between C-reactive protein to albumin ratio and coronary artery disease severity in patients with acute coronary syndrome. Angiology. 2019;70(4):361–368. doi:10.1177/0003319717743325
15. Liao CK, Yu YL, Lin YC, et al. Prognostic value of the C-reactive protein to albumin ratio in colorectal cancer: an updated systematic review and meta-analysis. World J Surg Oncol. 2021;19(1):139. doi:10.1186/s12957-021-02253-y
16. Kunutsor SK, Laukkanen JA. Serum C-reactive protein-to-albumin ratio is a potential risk indicator for pneumonia: findings from a prospective cohort study. Respir Med. 2022;199:106894. doi:10.1016/j.rmed.2022.106894
17. Metlay JP, Waterer GW, Long AC, et al. Diagnosis and treatment of adults with community-acquired pneumonia: an official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care Med. 2019;200(7):e45–e67. doi:10.1164/rccm.201908-1581ST
18. Veronese N, Cereda E, Solmi M, et al. Inverse relationship between body mass index and mortality in older nursing home residents: a meta-analysis of 19,538 elderly subjects. Obes Rev. 2015;16(11):1001–1015. doi:10.1111/obr.12309
19. Roffman CE, Buchanan J, Allison GT. Charlson Comorbidities Index. J Physiother. 2016;62(3):171. doi:10.1016/j.jphys.2016.05.008
20. Kaiser MJ, Bauer JM, Ramsch C, et al. Validation of the mini nutritional assessment short-form (MNA-SF): a practical tool for identification of nutritional status. J Nutr Health Aging. 2009;13(9):782–788. doi:10.1007/s12603-009-0214-7
21. Rathore SS, Oberoi S, Iqbal K, et al. Prognostic value of novel serum biomarkers, including C-reactive protein to albumin ratio and fibrinogen to albumin ratio, in COVID-19 disease: a meta-analysis. Rev Med Virol. 2022;32(6):e2390. doi:10.1002/rmv.2390
22. Rea IM, Gibson DS, McGilligan V, McNerlan SE, Alexander HD, Ross OA. Age and Age-Related Diseases: role of Inflammation Triggers and Cytokines. Front Immunol. 2018;9:586. doi:10.3389/fimmu.2018.00586
23. Shive C, Pandiyan P. Inflammation, Immune Senescence, and Dysregulated Immune Regulation in the Elderly. Front Aging. 2022;3:840827. doi:10.3389/fragi.2022.840827
24. Rosolowski M, Oberle V, Ahnert P, et al. Dynamics of cytokines, immune cell counts and disease severity in patients with community-acquired pneumonia - Unravelling potential causal relationships. Cytokine. 2020;136:155263. doi:10.1016/j.cyto.2020.155263
25. Ticinesi A, Lauretani F, Nouvenne A, et al. C-reactive protein (CRP) measurement in geriatric patients hospitalized for acute infection. Eur J Intern Med. 2017;37:7–12. doi:10.1016/j.ejim.2016.08.026
26. Sproston NR, Ashworth JJ. Role of C-Reactive Protein at Sites of Inflammation and Infection. Front Immunol. 2018;9:754. doi:10.3389/fimmu.2018.00754
27. Thiem U, Niklaus D, Sehlhoff B, et al. C-reactive protein, severity of pneumonia and mortality in elderly, hospitalised patients with community-acquired pneumonia. Age Ageing. 2009;38(6):693–697. doi:10.1093/ageing/afp164
28. Liao J, Shen X, Du Z, Wang X, Miao L. Nutritional status and inflammation as mediators of physical performance and delirium in elderly community-acquired pneumonia patients: a retrospective cohort study. Clin Interv Aging. 2024;19:1641–1652. doi:10.2147/CIA.S483481
29. Gremese E, Bruno D, Varriano V, Perniola S, Petricca L, Ferraccioli G. Serum albumin levels: a biomarker to be repurposed in different disease settings in clinical practice. J Clin Med. 2023;12(18):6017. doi:10.3390/jcm12186017
30. Sheinenzon A, Shehadeh M, Michelis R, Shaoul E, Ronen O. Serum albumin levels and inflammation. Int J Biol Macromol. 2021;184:857–862. doi:10.1016/j.ijbiomac.2021.06.140
31. Zhao L, Bao J, Shang Y, et al. The prognostic value of serum albumin levels and respiratory rate for community-acquired pneumonia: a prospective, multi-center study. PLoS One. 2021;16(3):e0248002. doi:10.1371/journal.pone.0248002
32. Akirov A, Masri-Iraqi H, Atamna A, Shimon I. Low albumin levels are associated with mortality risk in hospitalized patients. Am J Med. 2017;130(12):
33. Tokgoz Akyil F, Yalcinsoy M, Hazar A, et al. Prognosis of hospitalized patients with community-acquired pneumonia. Pulmonology. 2018;24(3):164–169. doi:10.1016/j.rppnen.2017.07.010
34. Wang S, Xu S, Wang J, et al. Preoperative C-reactive protein to albumin ratio may be a good prognostic marker in patients undergoing hepatectomy for hepatocellular carcinoma: a meta-analysis. Front Nutr. 2024;11:1444352. doi:10.3389/fnut.2024.1444352
35. Li J, Zhu P, Li Y, et al. A novel inflammatory biomarker, high-sensitivity C-reactive protein-to-albumin ratio, is associated with 5-year outcomes in patients with type 2 diabetes who undergo percutaneous coronary intervention. Diabetol Metab Syndr. 2023;15(1):14. doi:10.1186/s13098-022-00977-9
36. Oh TK, Song IA, Lee JH. Clinical usefulness of C-reactive protein to albumin ratio in predicting 30-day mortality in critically ill patients: a retrospective analysis. Sci Rep. 2018;8(1):14977. doi:10.1038/s41598-018-33361-7
37. Llop-Talaveron J, Badia-Tahull MB, Leiva-Badosa E. An inflammation-based prognostic score, the C-reactive protein/albumin ratio predicts the morbidity and mortality of patients on parenteral nutrition. Clin Nutr. 2018;37(5):1575–1583. doi:10.1016/j.clnu.2017.08.013
38. Teissier T, Boulanger E, Cox LS. Interconnections between Inflammageing and Immunosenescence during Ageing. Cells. 2022;11(3):359. doi:10.3390/cells11030359
39. Li Y, Wang C, Peng M. Aging immune system and its correlation with liability to severe lung complications. Front Public Health. 2021;9:735151. doi:10.3389/fpubh.2021.735151
40. Schoevaerdts D, Sibille FX, Gavazzi G. Infections in the older population: what do we know? Aging Clin Exp Res. 2021;33(3):689–701. doi:10.1007/s40520-019-01375-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Prognostic Value of the Age-Adjusted Charlson Comorbidity Index Among the Elderly with Breast Cancer
Wang Z, Zhong Y, Zhou Y, Mao F, Zhang X, Wang C, Sun Q
Clinical Interventions in Aging 2023, 18:1163-1174
Published Date: 26 July 2023
Elevated High Sensitivity Cardiac Troponin T is Nonlinearly Associated with Poor Prognosis in Aging COVID-19 Patients: A Retrospective Study
Jin X, Yang H, Ma W, Yuan Y, Li T
Infection and Drug Resistance 2023, 16:5155-5163
Published Date: 9 August 2023
Prognosis of Older Adult Patients Suffering from Atrial Fibrillation and Hypokalemia
Wang XD, Wang Y, Liu J, Yao JW, Zhang J, Zhang YN
Clinical Interventions in Aging 2023, 18:1363-1371
Published Date: 17 August 2023
Associations of Serum Clara Cell Protein 16 with Severity and Prognosis in Adults with Community-Acquired Pneumonia
Li JF, Zou Q, Li X, Liu Y, He QY, Fu L, Zhao H
International Journal of General Medicine 2023, 16:4907-4917
Published Date: 31 October 2023
Frailty and Adverse Outcomes After SARS-CoV-2 Infection in Elderly Patients on Maintenance Hemodialysis: A Cohort Study
Yang Y, Yang H, Diao Z, Liu X, Yao L, Wang L, Shi X, Li X, Ma Q
Clinical Interventions in Aging 2023, 18:1937-1948
Published Date: 23 November 2023