")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Early Detection and Intervention Practices Provided by Physical and Occupational Therapists in Saudi Arabia for Children with or at Risk for Cerebral Palsy
Authors Gmmash A , Aljuhani T , Albesher RA
Received 1 April 2025
Accepted for publication 3 July 2025
Published 16 July 2025 Volume 2025:18 Pages 4045—4058
DOI https://doi.org/10.2147/JMDH.S526999
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Afnan Gmmash,1 Turki Aljuhani,2,3 Reem A Albesher4
1Department of Physical Therapy, Faculty of Medical Rehabilitation Sciences, King Abdulaziz University, Jeddah, 22252, Saudi Arabia; 2Department of Occupational Therapy, College of Applied Medical Sciences, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 3King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 4Department of Rehabilitation Sciences, College of Health and Rehabilitation Sciences, Princess Nourah Bint Abdulrahman University, Riyadh, 11671, Saudi Arabia
Correspondence: Afnan Gmmash, Department of Physical Therapy, Faculty of Medical Rehabilitation Sciences, King Abdulaziz University, Jeddah, Saudi Arabia, Tel +966 500310055, Email [email protected]
Purpose: Accurate cerebral Palsy (CP) diagnosis is possible before or at the age of 5 months. However, little is known about the practice of early detection guidelines in Saudi Arabia. The objective of this study was to explore the current physical therapy (PT) and occupational therapy (OT) early detection practices for children (0– 3 years) with or at risk for CP and knowledge and application of evidence-based practices (EBP) for these children.
Patients and Methods: A cross-sectional study using a purpose-developed electronic survey was distributed to physical and occupational therapists who work with young children with or at risk of CP. Descriptive statistics and cross-tabulations were employed to analyse the data.
Results: A total of 76 participants completed the survey questions and were included in the analysis. Less than half of the patients (46%) received a diagnosis of being at risk for CP between 0 and 5 months of age. Only 16% of the participants are certified in using the Prechtl Qualitative Assessment. Seventy-eight percent of the participants provide parents with prognostic information regarding their children’s diagnosis. Sixty-six percent of the providers always used goal-oriented therapy, 30% always used Neurodevelopmental Treatment, 22% always used passive intervention, and 84% always used caregiver education in their treatment. Application of constraint-induced movement therapy was significantly correlated with a number of demographic variables.
Conclusion: This study showed that the majority of therapists consider EBP in evaluating and treating young children with CP. However, more attention should be directed toward training therapists to utilize sensitive tools to detect CP early, enabling them to incorporate EBP in their management plan. Although therapists follow some of the recommended interventions, many therapists still use ineffective treatments with children with CP. A national guideline is required to unify practice and illustrate the role of PT and OT in the management of CP.
Keywords: pediatric, rehabilitation, infants, cerebral palsy, early diagnosis
Introduction
Cerebral palsy (CP) is one of the most frequently experienced disabilities affecting children worldwide. An estimated prevalence of CP in Saudi Arabia, according to a study done in Jeddah city, is 1.6 per 1000 births, which is similar to the worldwide prevalence.1 CP is a lifelong condition that commonly impacts various aspects of children’s development. The disability constrains the children’s as well as their family’s quality of life.2 In Saudi Arabia, CP was found to be one of the most common neurological disorders in children.3 Some of the most common risk factors that are correlated with the CP diagnosis in Saudi Arabia include preterm birth, multiple pregnancies, low neonatal birth weight, and family history.4 Children with CP face multiple challenges as they get older. Some of these difficulties include delayed school enrollment, the development of secondary complications, and limited social interactions later in life.5 Despite the availability of rehabilitation services, previous reports stated that limited use of these services was documented in Saudi Arabia.6 Early screening for CP is recommended to ensure prompt access to related services. Early detection of CP is integral to minimize any preventable long-term consequences. In addition, prompt recognition of CP facilitates early intervention.7 Systematic reviews, as well as published international practice guidelines, provide a detailed framework for early detection and outline the level of evidence for available interventions.8,9
Motor disabilities in young infants are not always identified until motor delays become noticeable, especially in the absence of known risk factors. Thus, CP diagnosis is often delayed, which in turn postpones intervention. Some of the recommended strategies that should be used for early detection of CP are surveillance of high-risk infants, use of early Magnetic Resonance Imaging (MRI), and application of highly sensitive well-established tools such as The General Movements Assessment (GMA).10
Systematic reviews illustrated that combining neuroimaging, which includes MRI, with the GMA exams increases the accuracy of diagnosing CP in infants prior to the onset of motor delays.8,11 Application of neuroimaging and GMA can be costly and requires a high level of skill and training. In addition, the GMA can only be used on infants under the age of 5 months. If such challenges arise, alternative objective assessment tools can be used.12,13 Some of these tools include the Ultrasounds, Hammersmith Infant Neurological Examination (HINE), Alberta Infant Motor Scale (AIMS), Bayley Scales of Infant and Toddler Development (BSID), and the Infant Motor Performance (TIMP) test. Knowledge of the most reliable and sensitive screening tools is vital to facilitate early diagnosis and early access to the available resources.13–15 In addition, other neurodevelopmental assessments such as the Specific Infant Motor Performance (STEP) showed excellent detection of neurodevelopmental delays, including developmental delays including CP before 3 months of age.16 Although CP can be detected before 12 months of age, diagnosis is usually delayed after the children’s first birthday.17 Some evidence suggests that the average age for CP diagnosis in Saudi Arabia is between 12 and 24 months.18 One source revealed that implementation of CP early diagnosis guidelines can reduce the age of diagnosis prior to the age of 12 months.19 Thus, more efforts should be directed toward the application of measures to encourage early diagnosis.
The American Academy for Cerebral Palsy and Developmental Medicine (AACPDM) provided a guideline in 2022 that illustrates recommendations to guide early intervention for children with CP. The AACPDM advised physical and occupational therapists to focus on self-initiated movements, mobility training, activity-based therapy, and parent education.20 Novak et al established a traffic light system to identify interventions that are supported by high-quality evidence. The guidelines support early intervention, parent education, home programs, strengthening exercises, task-specific training, bimanual training, CIMT, treadmill training, and environmental enrichment. On the other hand, motor interventions that are passive and the use of Neurodevelopmental Treatment (NDT) are not recommended and their effectiveness has not been strongly associated with enhanced functional outcomes for children with CP.9 Physical therapists and occupational therapists have a significant role in determining risk factors and conducting objective measures to assist in determining the diagnosis and prognosis of CP.8
In the past few years, the management of CP has gained increasing emphasis in research studies conducted in Saudi Arabia.21 Considering the significant advancements dedicated to healthcare infrastructure, more attention has been directed to early screenings, early intervention, and implementation of evidence-based practice (EBP). However, the current PT and OT knowledge and management of CP in Saudi Arabia have not been explored. Thus, this study assesses the current practices used in PT and OT related to early identification and intervention for children with CP to assist future researchers in providing the recommended practices and bridging the identified gap. This will aid in translating the best available EBP into clinical practice to improve services and decrease the uncertainty that the families may be experiencing.
Materials and Methods
Study Design
This is a quantitative cross-sectional study that was conducted based on a purpose-developed electronic self-administered online survey in English. The online survey was distributed to pediatric physical and occupational therapists in Saudi Arabia. Participants were included in the study if they met the following criteria: pediatric physical therapists, pediatric occupational therapists, treating or have treated infants and children from birth up to three years with or at risk for CP, and practicing or have practiced as a pediatric therapist in Saudi Arabia. In accordance with the Helsinki Declaration for Ethical Standards in Human Research, the Princess Nourah bint Abdulrahman University Ethics Committee approved the study (HAP-01-R-059) in Riyadh, Kingdom of Saudi Arabia. All methods were performed following relevant institutional review boards and regulations. The study protocol, procedures, and respondents’ rights were explained at the beginning of the study. Informed consent was obtained from all participants before completing the survey.
Survey Components
The purpose of the questionnaire is to explore the therapists’ perspectives and knowledge about early detection and intervention for children with or at risk of cerebral palsy. Prior to the start of data collection, two expert pediatric physical therapists and one occupational therapist revised the survey for clarity and functionality. Each user was allowed one attempt to fill out the survey. The reviewers had minor edits and comments, and the authors revised their comments and edited the survey accordingly. The survey was pilot tested on four physical therapy students to test for clarity and to resolve any potential technical issues.
The following sections were included in the survey: demographics, diagnosis, and treatment. First, the demographic section included questions related to their discipline, area of residence, age, gender, employment sector, experience, and the age of the children they usually treat. Second, the diagnosis section was developed based on the current recommendation guideline for detecting infants at risk for CP by Novak et al 2017. This section includes questions related to best practice and the therapist’s current practice. Questions include triggers for referral to PT and OT, the therapist’s role in early detection, the child’s age when starting therapy, tools used for early detection, and the provision of prognostic information. Third, the treatment section includes questions related to the type, dosage, and frequency of intervention therapists provide to children with CP. Where possible, participants were provided the option to mention other answers based on their situation, for example, other reasons for referral, role in diagnostic procedure, assessment tools, and intervention types.
Data Analysis
Statistical analysis was performed using SPSS version 30. Descriptive statistics using numbers and percentages were calculated to describe the demographic and the categorical data. Data were summarized as mean ± standard deviation, and the correlation between the variables were explored using chi-square. A p-value below 0.05 was considered to be statistically significant. The choice of the statistical methods was guided by the type of variables and the sample size to ensure appropriate interpretation of the data.
Results
Participants Demographics
A total of 77 participants completed the survey. One participant did not have experience in practicing in Saudi Arabia and was therefore, excluded from the study. Most of the participants were female (65%) and physical therapists (85.7%). The majority of the therapists were from the western region in Saudi Arabia (48.1%), working in hospital settings (40.3%), had five or fewer years of experience (46%), and mostly treated children from birth until three years of age. A detailed description of the demographic section is presented in (Table 1).
 |
Table 1 Participants Demographics |
Practices Related to Early Detection of CP
Therapists (81%) are aware that children with or at risk for CP should be referred to PT and OT based on the GMA scores or absent fidgety movements. However, only 44% percent of them reported that this reflects their actual practice. Therapy services start early for children at risk for CP and only (3.9%) of the participants stated that these children receive therapy after 24 months of age. More descriptions of the early detection practices are illustrated in Table 2.
 |
Table 2 Practices Related to Early Detection of CP |
Most of the participants are involved in the diagnosis process of CP (68.8%). Participants were asked about their involvement in the diagnosing process. Therapists described their role in the assessment process as follows: by using Prechtl’s assessment, assessment of the level of disability and how it is affecting the children’s community participation, classifying the children according to their GMFCS levels, conducting a muscle tone assessment, communicate our concerns with the primary care physician to make a diagnosis, and through a multidisciplinary collaboration.
Participants who were excluded from the diagnosing process stated that the children were usually diagnosed by the medical team, who then referred the patients to the rehabilitation facility as secondary care. Some also clarified that communication with the medical team is rarely accessible to the therapists. In addition, some stated that hospitals only accept children with confirmed diagnoses.
Practices Related to the Management of CP
In this section, participants were asked about the early intervention practices they provide for children with CP. Therapists reported that children with CP receive a high frequency of intervention, 53% reported providing interventions more than once a week. Most of the interventions that the therapists used were parent education and activity based interventions followed by goal oriented therapy as shown in (Table 3) and (Figure 1). Similar findings were evident in the frequency of providing interventions for children with CP, most of the therapists (84%) reported always using parent education, while passive interventions were the least type of intervention always used by the therapists in their treatment plan.
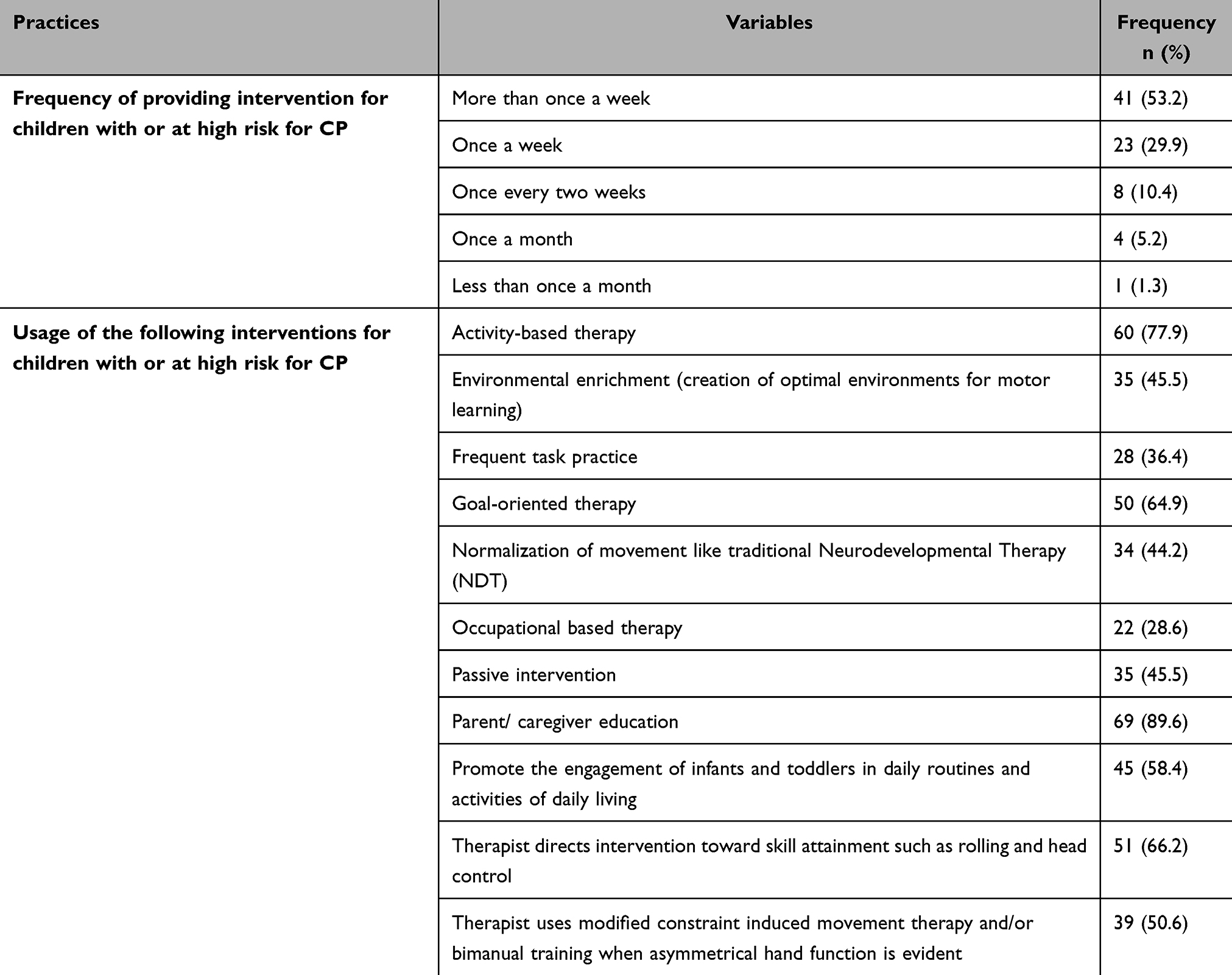 |
Table 3 Practices Related to Early Intervention for Children with CP |
 |
Figure 1 Frequencies of using different interventions for children with CP. |
Association Factors
A chi-square test was used to examine the association between the therapists’ demographic variables and early detection and intervention practices. The results of cross tabulation and chi-square test are presented in (Tables 4–6). A statistically significant relationship was found between the age of treating children and using observed developmental delays for early detection of CP. A significant relationship was also found between using modified constraint-induced movement therapy (mCIMT) and the therapists’ years of experience, the age of treated children and the region in which they practice.
 |
Table 4 Cross Tabulation Table Between Demographic Variables and Early Detection Practices Based on Best Available Evidence from Therapists’ Point of View |
 |
Table 5 Cross Tabulation Table Between Demographics Variables and Actual Early Detection Practices Followed in the therapists’ Work Setting |
 |
Table 6 Cross Tabulation Table Between Demographics Variables and Early Intervention Practices |
Discussion
This study aimed to explore the current physical therapists’ and occupational therapists’ knowledge and application of early identification and interventions for children with or at risk for CP in Saudi Arabia. Our results showed that the majority of therapists treat children between the ages of 0 and 3. Most of these therapists work in a hospital setting, which makes them more accessible to infants with severe risk factors. Many of the therapists also worked in universities, which made them more aware of the EBP. Most of the therapists in our sample stated that children with or at risk for CP are referred to them based on observed developmental delays, followed by prematurity, risk factors presented in the child’s medical history.
There is a clear lack of using early identification standardized assessments in identifying at-risk infants. Only 17% of the therapists are certified in using the most sensitive tool to diagnose CP. Yet, a good number of therapists reported knowledge of the assessments but not of implementing them. This is consistent with the findings of a study done in Brazil.22 One of the recommended tools to detect CP is GMA, which requires certification even after obtaining the costly basic training course, this could hinder the usage of this tool even in high income countries.23 Previous studies showed that lack of accessibility to structured training programs limit the number of certified therapists and the sustainable usage of this tool.24,25
EBP is essential in pediatric physical and occupational therapy. Nevertheless, diverse beliefs, attitudes, and barriers among pediatric physical and occupational therapists might influence the implementation of current evidence in clinical settings. A study investigating evidence-based practice in Saudi Arabia shows that most pediatric physical therapists believe that EBP is crucial in clinical practice to improve the quality of health services. This lack of applying EBP is shown in different areas as well. For example, two recent studies illustrated that therapists report using EBP as they are motivated to use EBP in general and with the pediatric population specifically. Yet both studies reported some difficulties implementing EBP in real practice due to difficulty obtaining full-text papers and lack of management support, motivation in research, and training.26,27 In general, therapists expressed an overall positive attitude toward EBP.28,29 As for occupational therapists, the same attitude toward EBP is evident with high motivation for the use of EBP and low and/or lack of implementation.30 Our results showed that pediatric therapists have a good understanding of the recommendations related to the early identification of infants with or at risk of CP. However, our results are unable to assess the real-world application of early identification protocol who are certificated or trained in using the recommended assessments due to the unavailability of their data in any registers. Organizations must keep records of individuals certified in using assessment tools for early detection and enable them to lead related workshops for other healthcare providers in the same field. The Prechtl GMA website, for example, provides a list of certified tutors.31 Similar websites could be generated to guide hospitals and rehabilitation centers to contact the intended population for early detection of certain conditions such as CP.
Current evidence shows that accurate and early detection of CP in infants can occur as early as 5 months of corrected age. The most commonly used motor assessment is GMA, in addition to MRI and clinical neurological assessment. HINE has been proven to detect CP accurately before 5 months of CA.8 Combining these assessments showed very high specificity and accuracy diagnosis of CP in children who are at risk. However, our results showed that these tests are not commonly used for the purpose of early identification. In addition to the limited use of motor and neurological assessments (GMA and HINE), the utilization of neuroimaging, specifically MRI, is very limited in the early detection of infants at risk of CP. Yet, studies demonstrate that specific patterns of brain injury shown in the MRI are associated with later diagnosis of CP.32 MRI should be incorporated into routine clinical practice and can increase the accuracy of early detection of CP or at risk of developmental delays.33
Correlation data showed that therapists’ years of experience was significantly correlated with the use of ultrasound and MRI data while, as the child gets older, the reliance on observation of developmental delays is correlated. The results are aligned with other studies reporting that more experienced therapists use multiple resources to help the children with older children even more.34,35 In addition, experienced therapists could be more proficient in knowing when neuroimaging data are indicated. Moreover, therapists’ years of experience, the age of the child, and gender were significantly associated with the use of CIMT. This could be expected as EBP is usually followed by more experienced therapists. Additionally, CIMT is typically used with older children because some researchers fear that the restriction associated with the CIMT modality might interfere with typical brain development in the first few years of life. However, some recent and limited evidence showed positive results from using CIMT in infants.35–37 Previous studies showed that although therapists support the use of pediatric CIMT, barriers related to cost and institutional restrictions limit their application.38
Even though most of the therapists stated that they were involved in the diagnosis process of CP, their involvement represented their assessment of the child’s functional disabilities rather than the actual diagnosis. Novak et al published a guideline that assists healthcare professionals in communicating diagnosis to parents.39 However, more studies should clearly state the role of PT and OT in the diagnosis process. For example, both AIMS and GMA can be conducted by physical and occupational therapists to predict CP,40 but only one therapist in our sample stated that using sensitive objective measures is how they are involved in the diagnosis. In addition, our study showed that most of the therapists provide the families with prognostic information. However, they are not using the appropriate tools to determine prognosis. Most of them stated using the gross motor functional classification system, which should not be used to determine prognosis before the age of two years. Instead, therapists should use the MRI results, HINE scores, gestational age, presence of comorbidities, presence or absence of primitive reflexes and sometimes gender to guide the prognosis.8,41,42
In terms of the implementation of early intervention methods, the most common methods used were activities of daily living (ADL), goal-oriented sessions, as well as parent education. However, passive intervention and NDT are still largely reported in early intervention as a choice method of intervention. The ongoing use of passive techniques is not surprising as it has been widely used by therapists and recommended in the literature before evidence emerged suggesting they are ineffective in providing long-term outcomes.9,43 Additionally, inconsistent use of EBP by physical and occupational therapists has been reported in other countries such as Brazil and the United States of America.22,44 This conflict of using EBP in early interventions stemmed from two main points: 1 – Lack of use of standardized assessments to track the child’s improvement and relying only on observation and objective measures, 2 – Absence of national clinical recommendations guiding early interventions with EBP guidelines. While ADL activities and goal oriented sessions are considered an effective EBP in early intervention, passive and NDT interventions are considered ineffective interventions and should be ceased by all therapists managing children with CP.45,46 More recent effects are shown in providing EBP clinical guidelines at the national level in Saudi Arabia. A recent study illustrates the availability of clinical guidelines for the management of children with autism spectrum disorder at a national level.47 Such clinical guidelines not only use the latest EBP and unify the practices among institutions but also take into account the differences in culture and resources if they exist and modify them based on the country’s requirements and needs. Similar findings were illustrated in a study by Baig et al in Ohio.48
This is the first study to explore the knowledge of therapists regarding early identification and interventions of children with or at risk for CP in Saudi Arabia. In addition, our study identified a gap and need in the current practice of early identification and early intervention of children with or at risk for CP. This study paves the path to the more specific application of early identification and intervention in the pediatric field and specifically for children with or at risk for CP. Lastly, the findings, while hard to generalize, highlight the need for more standardized clinical guidelines, specifically for early identification and interventions for children with or at risk for CP.
Limitations and Future Directions
There are several limitations in this study, the small sample size limited the generalizability of our findings to all practices within Saudi Arabia. Also, the use of a snowball sampling strategy may introduce a selection bias, which may limit the representation of our participants and restrict the diversity of our participants. These limitations are repeatedly noted in several similar surveys targeting medical professionals. The limited sample size could represent the limited number of pediatric physical and occupational therapists handling infants and young children with or at risk for CP in Saudi Arabia. This study targeted a sub-population of pediatric therapists in Saudi Arabia and yielded a similar sample size to that of previous study.27 More published data is needed to document the prevalence of physical and occupational therapists in Saudi Arabia. Future studies should focus on the implementation of early identification strategies and guidelines for children with or at risk of CP in Saudi Arabia. In addition, the studies should measure the effectiveness of the recommendations in Saudi Arabia and the ability to modify them if needed to fit the country’s culture and needs.12 Adaptation of global recommendations is needed, such as replacing the MRI or GMA with other more feasible assessment tools that could reduce cost and expedite identification and early intervention.
Conclusion
This study provides preliminary data showing that physical and occupational therapists have a substantial level of knowledge regarding early detection and intervention practices for young children with or at risk for CP. However, further implementation of EBP recommendations regarding early identification of CP and its prognosis should be encouraged. The role of PT and OT in the diagnosis process should be clearly identified to maximize their involvement in the diagnosis process and timely refer those at risk for CP to diagnosis-specific interventions. Publishing a national guideline could be beneficial to unify efforts and ensure effective implementation of EBP. In addition, future studies must report the actual application of EBP using objective measures in the work environments over an extended period of time to augment the results of this study and close any observed gaps. Researchers should also explore the parents’ and the therapists’ experiences and attitudes that are not easily quantifiable and could significantly interfere with the early detection of CP and the implementation of EBP.
Acknowledgement
Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2025R421), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Funding
Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2025R421), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Al-Jabri BA, Al-Amri AS, Jawhari AA, Sait RM, Talb RY. Prevalence, types, and outcomes of cerebral palsy at a tertiary center in Jeddah, Saudi Arabia. Cureus. 2022;14(8):e27716. doi:10.7759/cureus.27716
2. Vitrikas K, Dalton H, Breish D. Cerebral Palsy: an Overview. Am Fam Physician. 2020;101(4):213–220.
3. Al Salloum AA, El Mouzan MI, Al Omar AA, Al Herbish AS, Qurashi MM. The prevalence of neurological disorders in Saudi children: a community-based study. J Child Neurol. 2011;26(1):21–24. doi:10.1177/0883073810371510
4. Aa AS, Of B, Hm I, et al. Cerebral palsy in Saudi children. Neurosci Riyadh Saudi Arab. 2003;8(1):26–29.
5. Frisch D, Msall ME. Health, functioning, and participation of adolescents and adults with cerebral palsy: a review of outcomes research. Dev Disabil Res Rev. 2013;18(1):84–94. doi:10.1002/ddrr.1131
6. Saleh MN, Alharbi A, Albalwi A, et al. Characteristics of children with cerebral palsy and their utilization of services in Saudi Arabia. Healthc Basel Switz. 2023;11(19):2690. doi:10.3390/healthcare11192690
7. Hadders-Algra M, Boxum AG, Hielkema T, Hamer EG. Effect of early intervention in infants at very high risk of cerebral palsy: a systematic review. Dev Med Child Neurol. 2017;59(3):246–258. doi:10.1111/dmcn.13331
8. Novak I, Morgan C, Adde L, et al. Early, accurate diagnosis and early intervention in cerebral palsy: advances in diagnosis and treatment. JAMA Pediatr. 2017;171(9):897–907. doi:10.1001/jamapediatrics.2017.1689
9. Novak I, Morgan C, Fahey M, et al. State of the evidence traffic lights 2019: systematic review of interventions for preventing and treating children with cerebral palsy. Curr Neurol Neurosci Rep. 2020;20(2):3. doi:10.1007/s11910-020-1022-z
10. McIntyre S, Morgan C, Walker K, Novak I. Cerebral palsy--don’t delay. Dev Disabil Res Rev. 2011;17(2):114–129. doi:10.1002/ddrr.1106
11. Mcnamara LM, Scott KM, Boyd RN, Webb AE, Taifalos CJ, Novak IE. Effectiveness of early diagnosis of cerebral palsy guideline implementation: a systematic review. Minerva Pediatr. 2024;76(3):414–424. doi:10.23736/S2724-5276.22.07112-9
12. King AR, Al Imam MH, McIntyre S, et al. Early diagnosis of cerebral palsy in low- and middle-income countries. Brain Sci. 2022;12(5):539. doi:10.3390/brainsci12050539
13. Adde L, Helbostad JL, Jensenius AR, Taraldsen G, Grunewaldt KH, Støen R. Early prediction of cerebral palsy by computer-based video analysis of general movements: a feasibility study. Dev Med Child Neurol. 2010;52(8):773–778. doi:10.1111/j.1469-8749.2010.03629.x
14. Shen Y, Qu F, Wang C, et al. A TIMP-based assessment for early motor performance in cerebral palsy toddlers. J Army Med Univ. 2024;46(6):515–521. doi:10.16016/j.2097-0927.202309111
15. Eliks M, Gajewska E. The Alberta infant motor scale: a tool for the assessment of motor aspects of neurodevelopment in infancy and early childhood. Front Neurol. 2022;13:927502. doi:10.3389/fneur.2022.927502
16. Gower L, Jenkins D, Fraser JL, Ramakrishnan V, Coker-Bolt P. Early developmental assessment with a short screening test, the STEP, predicts one-year outcomes. J Perinatol off J Calif Perinat Assoc. 2019;39(2):184–192. doi:10.1038/s41372-018-0234-4
17. Module 13 • cerebral palsy for healthcare practitioners Early detection and diagnosis of cerebral palsy. the cerebral palsy alliance. Available from: https://iaacd.net/wp-content/uploads/2022/02/CP_Fact_Sheet13_IAACD_Early_detection_diagnosis-FA.pdf.
18. El-Halaby HAS, Sayed SKI, AlTurkestany IIM, et al. Characteristics and predisposing factors for cerebral palsy in children in Medina, Saudi Arabia. Int J Med Dev Ctries. 2020;4(12):2202. doi:10.24911/IJMDC.51-1603209568
19. Ches KB. How a network of hospitals reduced average age at cerebral palsy diagnosis to 9.5 months – pediatrics nationwide. 2020. Available from: https://pediatricsnationwide.org/2020/05/26/how-a-network-of-hospitals-reduced-average-age-at-cerebral-palsy-diagnosis-to-9-5-months/.
20. Noritz G, Davidson L, Steingass K, Council on Children with Disabilities, the American academy for cerebral palsy and developmental medicine, council on children with disabilities, the American academy for cerebral palsy and developmental medicine. Providing a primary care medical home for children and youth with cerebral palsy. Pediatrics. 2022;e2022060055. doi:10.1542/peds.2022-060055
21. Aleid MS, Alhamoud MA, Al Abbas LA, et al. Determining prevalence and identifying risk factors for cerebral palsy among Saudi Neonates: insights from a cross-sectional analysis. J Adv Trends Med Res. 2024;1(2):644. doi:10.4103/ATMR.ATMR_72_24
22. Souza RFA, Leite HR, Lucena R, Carvalho A. Early detection and intervention for children with high risk of cerebral palsy: a survey of physical therapists and occupational therapists in Brazil. Phys Occup Ther Pediatr. 2024;44(6):829–843. doi:10.1080/01942638.2024.2353124
23. General movements assessment: basic training course - 10/25/2018. Kaiser permanente rehabilitation services education. Available from: https://rehabilitationserviceseducation-ncal.kaiserpermanente.org/product/general-movements-assessment-10-25-2018/.
24. Maeda T, Kobayashi O, Ihara K, Bos AF. Fidgety movements assessment accuracy survey in Japan. Int J Environ Res Public Health. 2021;18(24):13428. doi:10.3390/ijerph182413428
25. Tomantschger I, Herrero D, Einspieler C, Hamamura C, Voos MC, Marschik PB. The general movement assessment in non-European low- and middle-income countries. Rev Saúde Pública. 2018;52:6. doi:10.11606/S1518-8787.2018052000332
26. Hasani F, MacDermid JC, Tang A, Kho M, Alghadir AH, Anwer S. Knowledge, attitude and implementation of evidence-based practice among physiotherapists working in the Kingdom of Saudi Arabia: a cross-sectional survey. Healthc Basel Switz. 2020;8(3):354. doi:10.3390/healthcare8030354
27. Alghadier M, Elnaggar RK, Alasraj MI, Khan N, Almeiman A, Albesher R. Evidence-based physiotherapy practice in paediatric subdiscipline: a cross-sectional study in Saudi Arabia. Healthcare. 2022;10(11):2302. doi:10.3390/healthcare10112302
28. Albishi AM. Knowledge, attitudes, and perceptions of physical therapists towards conventional physical therapy-across-sectional study. Ann Med Surg 2012. 2024;86(4):1942–1949. doi:10.1097/MS9.0000000000001883
29. Alhowimel AS, Alshahrani AA, Abulaban AA, et al. Saudi Arabian physical therapists’ knowledge, attitudes, and clinical practice in diabetes prevention and management. Diabetes Metab Syndr Obes Targets Ther. 2023;16:2967–2977. doi:10.2147/DMSO.S426949
30. Alshehri MA, Falemban R, Bukhari RA, Bakhsh HR. Occupational therapy practitioners’ decision-making preferences, attitudes, awareness and barriers in relation to evidence-based practice implementation in Saudi Arabia. Int J Evid Based Healthc. 2019;17(2):121–130. doi:10.1097/XEB.0000000000000162
31. General Movements Trust. The prechtl general movement assessment. Available from: https://general-movements-trust.info/48/licenced-tutors.
32. Badawi N, Novak I, Morgan C, Crowle C. Early detection of cerebral palsy using general movements assessment and MRIs - a sensible way forward. Pediatr Res. 2024;95(5):1191–1192. doi:10.1038/s41390-023-03008-z
33. Moss HG, Wolf LG, Coker-Bolt P, et al. Quantitative diffusion and spectroscopic neuroimaging combined with a novel early-developmental assessment improves models for 1-year developmental outcomes. AJNR Am J Neuroradiol. 2022;43(1):139–145. doi:10.3174/ajnr.A7370
34. Brookman-Frazee L, Haine RA, Baker-Ericzén M, Zoffness R, Garland AF. Factors associated with use of evidence-based practice strategies in usual care youth psychotherapy. Adm Policy Ment Health. 2010;37(3):254–269. doi:10.1007/s10488-009-0244-9
35. Yu SH, Brookman-Frazee L, Kim JJ, Barnett ML, Wright B, Lau AS. Therapist adaptations to evidence-based practices and associations with implementation outcomes in child therapy sessions. J Consult Clin Psychol. 2022;90(1):39–50. doi:10.1037/ccp0000667
36. Reidy TG, Carney J, Whiston N, Naber E. Infant constraint induced movement therapy: lessons learned from clinical implementation. J Pediatr Rehabil Med. 2017;10(1):61–67. doi:10.3233/PRM-170411
37. Eliasson AC, Nordstrand L, Ek L, et al. The effectiveness of Baby-CIMT in infants younger than 12 months with clinical signs of unilateral-cerebral palsy; an explorative study with randomized design. Res Dev Disabil. 2018;72:191–201. doi:10.1016/j.ridd.2017.11.006
38. Larson SC, Smith AE, Aravamuthan BR, et al. Pediatric Constraint-Induced Movement Therapy: current Practices and Implementation Barriers. OTJR Occup Particip Health. 2024;2024:15394492241300607. doi:10.1177/15394492241300607
39. Novak I, Morgan C, McNamara L, Te Velde A. Best practice guidelines for communicating to parents the diagnosis of disability. Early Hum Dev. 2019;139:104841. doi:10.1016/j.earlhumdev.2019.104841
40. Yildirim C, Asalioğlu A, Coşkun Y, Acar G, Akman İ. General movements assessment and Alberta infant motor scale in neurodevelopmental outcome of preterm infants. Pediatr Neonatol. 2022;63(5):535–541. doi:10.1016/j.pedneo.2022.06.002
41. Linsell L, Malouf R, Morris J, Kurinczuk JJ, Marlow N. Prognostic factors for cerebral palsy and motor impairment in children born very preterm or very low birthweight: a systematic review. Dev Med Child Neurol. 2016;58(6):554–569. doi:10.1111/dmcn.12972
42. Keeratisiroj O, Thawinchai N, Siritaratiwat W, Buntragulpoontawee M, Pratoomsoot C. Prognostic predictors for ambulation in children with cerebral palsy: a systematic review and meta-analysis of observational studies. Disabil Rehabil. 2018;40(2):135–143. doi:10.1080/09638288.2016.1250119
43. P T, D P, C M. The effectiveness of passive stretching in children with cerebral palsy. Dev Med Child Neurol. 2006;48(10). doi:10.1017/S0012162206001836
44. As G, Sk E. Early intervention therapy services for infants with or at risk for cerebral palsy. Pediatr Phys Ther off Publ Sect Pediatr Am Phys Ther Assoc. 2019;31(3). doi:10.1097/PEP.0000000000000619
45. Morgan C, Fetters L, Adde L, et al. Early intervention for children aged 0 to 2 years with or at high risk of cerebral palsy: international clinical practice guideline based on systematic reviews. JAMA Pediatr. 2021;175(8):846–858. doi:10.1001/jamapediatrics.2021.0878
46. Novak I, Honan I. Effectiveness of paediatric occupational therapy for children with disabilities: a systematic review. Aust Occup Ther J. 2019;66(3):258–273. doi:10.1111/1440-1630.12573
47. Alenezi S, Bashiri F, Alawami A, et al. Saudi Arabian evidence-based clinical practice guideline for the management of children with autism spectrum disorder: a national guideline adaptation using the KSU-modified-ADAPTE methodology. Clin Public Health Guidel. 2024;1(5):e70001. doi:10.1002/gin2.70001
48. Baig A, Morress C, Cecala E, Gallagher L, Gick E. OTs’ and physical therapists’ use of evidence-based practice for the treatment of motor function in infants with cerebral palsy. Am J Occup Ther. 2022;76(Supplement_1):7610510171p1–7610510171p1. doi:10.5014/ajot.2022.76S1-PO171
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.