")
Back to Journals » Journal of Inflammation Research » Volume 18
Early Identification of Pediatric Inflammatory Bowel Disease Based on a Noninvasive Multivariable Predictive Model
Authors Wu H, Sun Y, Tang Z, Qin X, Wang Y, Huang Y
Received 9 April 2025
Accepted for publication 1 July 2025
Published 12 July 2025 Volume 2025:18 Pages 9107—9118
DOI https://doi.org/10.2147/JIR.S529537
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Nadia Andrea Andreani
Hailin Wu,1 Yinghua Sun,2 Zifei Tang,1 Xiaojiao Qin,2 Yuhuan Wang,1 Ying Huang1
1Department of Gastroenterology, Children’s Hospital of Fudan University, National Children’s Medical Center, Shanghai, People’s Republic of China; 2Department of Ultrasound, Children’s Hospital of Fudan University, National Children’s Medical Center, Shanghai, People’s Republic of China
Correspondence: Yuhuan Wang, Department of Gastroenterology, Children’s Hospital of Fudan University, National Children’s Medical Center, No. 399 Wanyuan Road, Minhang District, Shanghai, 201102, People’s Republic of China, Tel +8664932985, Email [email protected] Ying Huang, Department of Gastroenterology, Children’s Hospital of Fudan University, National Children’s Medical Center, No. 399 Wanyuan Road, Minhang District, Shanghai, 201102, People’s Republic of China, Tel +8664932985, Email [email protected]
Background: Early identification of pediatric inflammatory bowel disease (IBD) improves long-term outcomes; yet, significant diagnostic delays persist. This study aimed to establish and validate the optimal model of noninvasive evaluation tests to help clinicians with the early identification of pediatric IBD.
Methods: The study adopted a retrospective development and prospective temporal validation design within the same clinical center. A cohort of 314 pediatric patients (IBD, 103; non-IBD, 211) was used to develop a logistic regression model. The model based on noninvasive features, including IBD-related symptoms, routine laboratory tests, and transabdominal ultrasound findings. Ultrasound parameters included Limberg score > 1 (bowel wall thickening with blood flow), increased mesenteric fat, disrupted wall layering, and enlarged lymph nodes. The ultrasound operator was blinded to laboratory and endoscopic results. Feature selection was performed using logistic regression and random forest methods. Model performance was assessed via bootstrapped internal validation (1000 resamples), and temporally validated in a prospective cohort of 66 children (IBD, 19; non-IBD, 47).
Results: In the importance assessment, the ultrasound feature of Limberg level > 1 was identified as the most valuable feature, followed by the erythrocyte sedimentation rate, fecal calprotectin, C-reactive protein and hypoalbuminemia. The most valuable clinical symptom identified was active perianal abscess or fistula. The model, constructed from these features, demonstrated high accuracy and robustness in both internal validation (area under the curve, 0.97 [95% confidence interval: 0.95– 0.98]) and temporal external validation (area under the curve, 0.94 [95% confidence interval: 0.86– 1.00]). In the external validation set, the model showed good calibration, with a calibration slope of 0.86, and a Brier score of 0.08.
Conclusion: The nomogram, based on noninvasive factors, can identify children with IBD at early stages using accessible noninvasive testing.
Keywords: pediatric, inflammatory bowel disease, intestinal ultrasound, noninvasive, nomograms
Introduction
Inflammatory bowel disease (IBD) is a complex and common chronic digestive tract disease, with approximately 20% of the cases presenting during childhood or adolescence. The incidence of pediatric IBD has been steadily increasing worldwide over the past decades, highlighting the urgent need for effective early diagnostic strategies.1,2 Early diagnosis of pediatric IBD enables timely intervention, which can reduce disease complications, minimize growth and developmental delays, and improve long-term health outcomes.3–5 However, in a large cohort recruited in a previous study, more than one-tenth of the patients exhibited symptoms at least 5 years before receiving a definitive diagnosis.6
The high heterogeneity of symptoms, inaccessibility of diagnostic instruments, and lack of specialized gastroenterologists and pathologists pose substantial barriers to the early identification of pediatric IBD.7,8 Therefore, developing a reliable, time- and cost-effective diagnostic method to facilitate the early identification of children with IBD is urgently needed.
Although the Red Flag Index9 and IBD-REFER,10 developed based on clinical symptoms and routine laboratory test results, are currently available tools to help primary care physicians with early IBD detection, the former is not suitable for children and UC, and the latter has been widely validated internationally.
Intestinal ultrasonography is a noninvasive, radiation-free, and immediately available method for precise localization. Compared with the use of clinical symptoms and systemic inflammatory markers, the use of ultrasonography is more specific to the intestines and can localize lesions. Moreover, its value in the diagnosis and management of adults and children with IBD has been proven in many reports.11–13 The accuracy of intestinal ultrasonography is inferior to that of small-bowel computed tomography enterography or small-bowel magnetic resonance imaging enterography.14–16
Currently, few studies have assessed the combined use of ultrasonography with other noninvasive markers for the diagnosis of pediatric IBD. A systematic review published in 2019 reported that using endoscopy as the reference standard, the sensitivity of intestinal ultrasound, in whether detecting bowel wall thickening alone or in combination with other features (eg, vascularity, creeping fat, preserved wall stratification, and enlarged lymph nodes), in children ranged from 39% to 55%, with specificity ranging from 90% to 100%.17 In the study by DiLillo et al, the combination of bowel wall thickening and elevated fecal calprotectin (FC) improved specificity from 96.3% (88.5 to 99.1) to 100% (94.1 to 100), while maintaining a sensitivity of 69.6% (57.9 to 79.3), compared with bowel wall thickening alone.18
Following the Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis19 we aimed to establish and validate the optimal model of noninvasive evaluation tests to help clinicians with the early identification of pediatric IBD.
Materials and Methods
Data Collection
Data for the training set were retrospectively collected from December 2021 to September 2023. This study targeted individuals who were newly diagnosed and referred, aged 2–18 years, and presenting with symptoms of suspected IBD, including recurrent abdominal pain, changes in bowel habits, hematochezia, and perianal abscess. The data was collected from electronic health records of the Children’s Hospital. The exclusion criteria were children diagnosed with known organic diseases (eg, previously identified IBD or celiac disease), those who had commenced IBD induction therapy, and those who had no available endoscopic or ultrasonographic data, or whose endoscopy or ultrasonography was performed more than one week apart (Figure 1). For the validation set, children were prospectively enrolled from January to June 2024, using the same inclusion criteria.
 |
Figure 1 Flow diagram of the research participants. (a) Diagram of the flow of the training set. (b) Diagram of the flow of the validation set. (c) Diagnostic protocol for pediatric inflammatory bowel disease. Red-colored text indicates timing: (1) laboratory tests, endoscopy, and intestinal ultrasound were performed within one week; (2) the final reference standard diagnosis of IBD was made within one month following the completion of all assessments. Abbreviation: IBD, inflammatory bowel disease. |
Outcome and Predictors
Our primary outcome of interest was a diagnosis of pediatric IBD. On the basis of previous diagnostic scales and literature,9,10 as well as examinations conducted at our institution, we identified three sets of features. The first set included the following clinical symptoms: diarrhea lasting for at least 1 month, bloody stool lasting for at least 1 week, fever of an unknown cause, active perianal abscess, fistula or large inflamed skin tag, impaired growth, abdominal pain lasting for at least 1 month, weight loss (>10%), first-degree family history of IBD, rheumatological symptoms (ie, arthritis, uveitis, and erythema nodosum) not meeting a clear rheumatological diagnosis, and recurrent oral aphthous ulcerations. The second set included the following routine laboratory test results: elevated FC level, elevated C-reactive protein (CRP) level, elevated erythrocyte sedimentation rate (ESR), anemia, hypoalbuminemia, and positive antineutrophil cytoplasmic antibodies (ANCAs). The third set included the following intestinal ultrasonographic features: Limberg level >1 (bowel wall thickening with accompanying blood flow), mesenteric fat, disorganized or lost bowel wall layering, and enlarged lymph nodes.
Laboratory Evaluation
Laboratory tests included the complete blood count, albumin level, ESR, CRP level, and FC level. ANCA serotypes were assessed by indirect immunofluorescence with positive cytoplasmic ANCA or perinuclear ANCA and antigen-specific PR3 and MPO enzyme-linked immunosorbent assay. Blood count, ESR, and albumin values were determined using routine methods in the hospital laboratory. FC was measured using a quantitative immunochromatographic method, and the normal reference value is 0–50 μg/g. CRP was measured using the scattering turbidimetric method, and the normal reference value is less than 8 mg/L. Albumin was detected using the enzyme-linked immunosorbent assay, and the normal reference value was 39–54 g/L. ESR was detected using an ESR analyzer, and the normal reference value was 0–20 g/L. For ease of application, we converted the results for these markers into binary variables according to their normal cut-off values, similar to IBD-REFER.
Intestinal Ultrasound Examination
The same ultrasound expert performed all intestinal ultrasound examinations (>200 intestinal ultrasound examinations per year for 2 years). The ultrasound operator was aware of the patient’s symptoms and signs but was blinded to the endoscopic and laboratory findings. A Mindray R9 pro ultrasound system was used for the examination. A convex probe with a 1–7-MHz frequency was used for abdominal panoramic examination, followed by a high-frequency examination (3–12 MHz) using a linear probe for detailed intestinal evaluation. Color power Doppler imaging was applied, with the Doppler velocity range set to 3–5 cm/s. For each bowel segment, one image showing the maximal bowel wall thickness and one image capturing the area with the most prominent vascularity were saved as DICOM files. To assess inter-rater reliability, the primary operator and a second trained sonographer, who had completed institutional IUS training and had independently performed IUS in more than 50 pediatric IBD cases, independently scored the same set of saved images. Agreement was quantified using weighted kappa statistics.
To determine the maximum bowel wall thickening of each intestinal segment, we measured the longitudinal and transverse sections of the entire intestinal segment, excluding the rectum and duodenum. Mesenteric fat was characterized by the presence of hyperechoic areas extending from the serosa to the mesentery and effectively enveloping the outer bowel walls. Loss of echo-stratification was defined as when the multilayered bowel wall becomes prevalently hypoechogenic or hyperechogenic and is sometimes indiscernible.20 Enlarged lymph nodes were defined as those with a short axis >5 mm or >5 planar lymph nodes (Supplementary Figure 1).
We employed the Limberg scoring system in conjunction with the assessments of intestinal wall thickness and blood flow signals. The Limberg scores21,22 were categorized as follows: Limberg level 0 indicated no thickening of the intestinal wall; Limberg level 1 represented thickening of the intestinal wall without accompanying blood flow signals; Limberg level 2 denoted thickening of the intestinal wall (bowel wall thickening >3 mm) with punctate blood flow; Limberg level 3 indicated thickening of the intestinal wall with linear blood flow; and Limberg level 4 represented thickening of the intestinal wall with blood flow extending into the mesentery.
Definition of Inflammatory Bowel Disease
All enrolled participants had undergone endoscopy and had mucosal pathology examination data; some had capsule endoscopy data. A skilled pediatric gastroenterologist performed the endoscopy using Fuji devices. One month after follow-up, pediatric gastroenterologists determined whether the patients had IBD on the basis of the Porto criteria23 while considering each patient’s endoscopy and pathology results and their follow-up conditions.
Assessment of Disease Activity
In patients with CD, clinical disease activity is assessed using the Pediatric Crohn’s Disease Activity Index (PCDAI). Endoscopic activity in CD is evaluated using the Simple Endoscopic Score for Crohn’s Disease (SESCD). For patients with UC, the Pediatric Ulcerative Colitis Activity Index (PUCAI) assesses clinical disease activity. Endoscopic activity in UC is measured using the Mayo Endoscopic Subscore (MES). Histological disease activity in all patients is evaluated using the Nancy histological index.24
Development of the Model
Predictors were assessed by univariate logistic regression analysis, followed by an age-, sex- and disease duration-adjusted multivariate logistic regression analysis. To avoid false positives, a significance level of 1% was used as the threshold for confirming independent associated features. The effect sizes of significantly associated features were reported as odds ratios (OR) with their corresponding 95% confidence intervals (CI). Significant features were simultaneously subjected to LASSO regression and random forest analysis. LASSO regression, with an L1 penalty, was used to shrink the coefficients of less important variables to zero, thereby selecting key predictors while preventing overfitting. The optimal lambda value was determined through cross-validation. Meanwhile, random forest analysis was performed to rank features based on importance metrics for classification tasks, including accuracy decrease and Gini decrease. These importance metrics were calculated using the formulas provided in the “randomForest” and “randomForestExplainer” packages.25,26 Finally, the intersection of significant features identified by both LASSO regression and random forest analysis was selected for logistic regression modeling.
Model Evaluation
To assess the model’s quality of fit, we employed the Hosmer–Lemeshow test and coefficient of determination (R2). To evaluate predictive accuracy and model conformity, we used the receiver operating characteristic curve, area under the receiver operating characteristic curve (AUC), concordance index, and calibration curve. Additionally, a decision curve analysis demonstrated the net benefit of the model for patients. Both discrimination and calibration were assessed through bootstrapping in the training dataset, involving 1000 resamples, and validation dataset. We also validated the IBD-REFER using the training dataset for direct comparison.
Spearman correlation coefficients were used to examine the relationships between predictive probabilities and disease severity (clinical, endoscopic, and histological). PCDAI, SESCD, PUCAI, MES, and Nancy scores were converted into ordinal variables to evaluate their correlation with the probability of IBD classification across IBD populations.
Statistical Analysis
Statistical analyses were performed using R (version 4.4.1; R Core Team 2024). Data are reported as frequencies or mean±standard deviation. The statistical significance of comparisons between groups was defined as <0.05. Continuous variables were tested for normality using the Kolmogorov–Smirnov test. Normally distributed variables were evaluated using t-tests. Dichotomous variables were evaluated against mortality using the chi-square or Fisher exact test. We calculated the sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of the diagnostic methods using the formulas provided in the “caret” package.
Only the FC variable in the training dataset had 1% missing values, which were imputed using the mean of the FC values. The research location, inclusion and exclusion criteria, outcome measures, and predictive indicators of the validation and development datasets were similar.
Results
General Characteristics
In the final outcome assessment, 314 participants were included in the training dataset and 66 participants were included in the validation dataset. Table 1 shows the demographics of patients in the training dataset; the time from first symptoms to diagnosis in 74 (71.8%) children with IBD was >2 months. In the training dataset, 103 individuals were diagnosed with IBD, of which 89 had Crohn disease (CD), 13 had ulcerative colitis (UC), and one had IBD-Unclassified (Table 1). In the validation dataset, 19 individuals were diagnosed with IBD, of which 15 had CD and four had UC. The remaining 211 patients in the training dataset and 47 patients in the validation dataset were classified as non-IBD cases. The non-IBD group predominantly comprised individuals diagnosed with functional gastrointestinal disorders and allergic enteritis (Supplementary Table 1). For the same stored ultrasound images, the inter-rater agreement between two pediatric sonographers on Limberg grading was high, with a weighted kappa coefficient of 0.91, indicating excellent consistency.
 |
Table 1 Clinical, Laboratory, and Ultrasonographic Characteristics of Training Dataset |
Development of an Individualized Prediction Model Using the Training Dataset
Univariate analysis ruled out the following irrelevant factors: age, sex, abdominal pain, and first-degree family history (P>0.05). Fifteen factors remained significant after adjusting for age, sex and disease duration (P<0.01; Table 2). Figure 2a presents the results of the LASSO regression, identifying Limberg level >1, ESR, FC, CRP, hypoalbuminemia, and active perianal abscess or fistula as significant features. Similarly, Figure 2b shows the top features ranked by the random forest model based on Gini and accuracy decrease importance, which align with the LASSO results. Finally, these selected features were used to construct the logistic regression model. Diagnostic accuracy analysis was performed on these five features, with Limberg>1 demonstrating the highest accuracy (0.85). In the diagnostic interval subgroups, although the accuracy of ultrasound decreased slightly in the short diagnostic interval (<2 months) compared to the long diagnostic interval (≥2 months) (0.87 vs 0.83), it still maintained strong performance (Supplementary Figure 2). These features were then used to construct a logistic regression model. A personalized nomogram model was developed to categorize individuals according to their IBD risk scores (Figure 2b). By using the coefficients obtained from regression logistic analysis and applying the following formula, we calculated the estimated probability of children with IBD as 0.999:
 |
Table 2 Univariate and Multivariate Logistic Regression Models for Diagnosing Pediatric IBD |
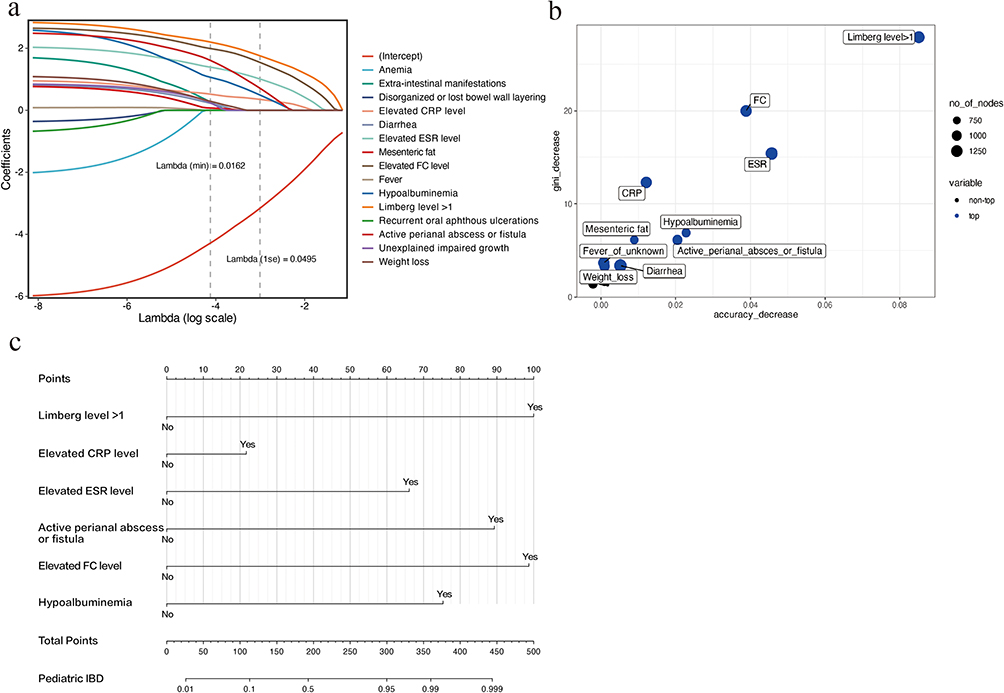 |
Figure 2 Visualization of the diagnostic prediction models. (a) Evolutionary selection in LASSO regression. (b) Feature importance for the random forest model based on datasets with ultrasound characteristics. (c) Nomogram for diagnosing pediatric IBD. Abbreviations: IBD, inflammatory bowel disease; CRP, C-reactive protein; FC, fecal calprotectin; ESR, erythrocyte sedimentation rate; AUC, area under the curve; CI, confidence interval. |
Logit (Probability)=−5.3092+2.7526×1 (Limberg level>1=Yes) +1.8198×1(elevated ESR = Yes) +2.7163×1 (elevated FC=Yes) +0.5974×1 (elevated CRP=Yes) +2.4585×1 (active perianal abscess or fistula=Yes) +2.0733×1 (hypoalbuminemia=Yes).
A free web-based calculator based on our model is available at: https://whlmt123456.github.io/PIBDcalculator.
Demonstrated Efficacy of the Nomogram in the Training and Validation Datasets
This nomogram of the training dataset exhibited a notable discriminative capability, achieving AUC of 0.97 (95% CI: 0.95–0.98) in the bootstrap resampling technique (n=1000) (Figure 3a). Supplementary Table 2 presents the general characteristics and distribution of included features in the test set patients. The model maintained its robust performance in the validation set with an AUC of 0.94 (95% CI: 0.86–1.00) (Figure 3b). The calibration plot demonstrated that the predictions closely matched the observed IBD probabilities, a finding further supported by the Hosmer–Lemeshow test results (P=0.19; Figure 3c). The model demonstrated good consistency in the external validation set, with the Hosmer–Lemeshow test results (P = 0.13) indicating a satisfactory fit, a well-calibrated curve, a calibration slope of 0.86, and a Brier score of 0.08 (Figure 3d). Decision curve analysis showed that the nomogram provided a higher net benefit than the IBD-REFER rule across a wide range of threshold probabilities (10–80%) in both the training and validation cohorts, indicating superior clinical utility for identifying children at risk of IBD (Supplementary Figure 3).
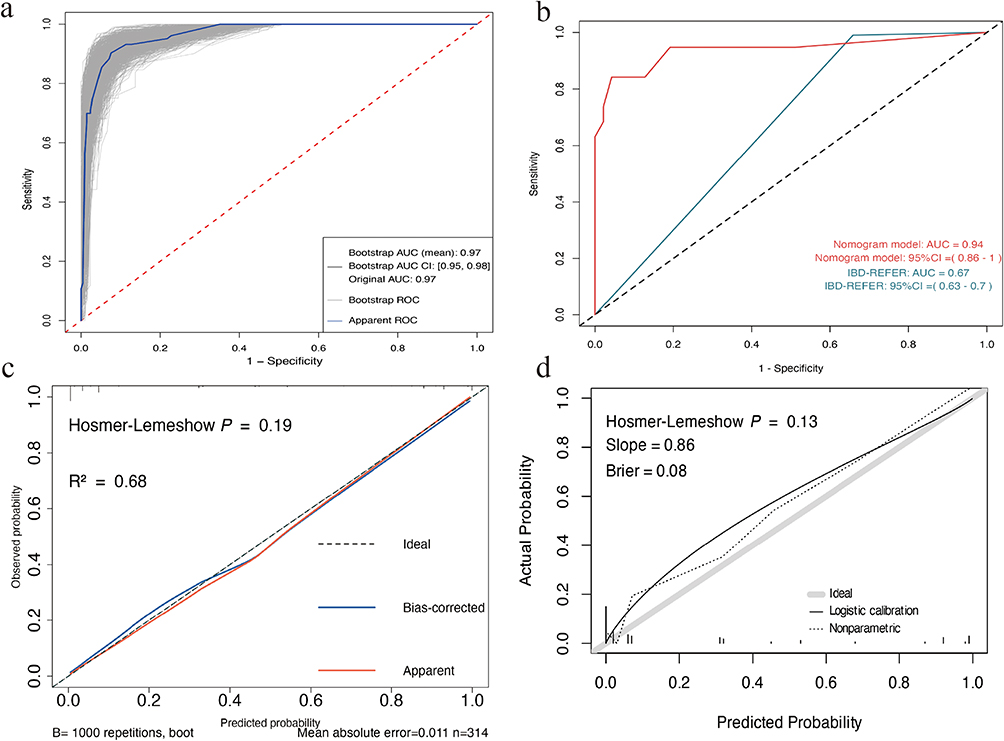 |
Figure 3 Evaluation of model stability and diagnostic performance in the training and validation datasets. (a) Receiver operating characteristic (ROC) curves of the nomogram model in the training dataset. (b) ROC curves of the nomogram model in the validation dataset. (c) Validation of the nomogram model for pediatric inflammatory bowel disease (IBD) in the training dataset. (d) Validation of the nomogram model for pediatric IBD in the validation dataset. Abbreviations: AUC, area under curve; CI, confidence interval. |
When the cut-off value was set at 0.32, the model attained the highest Youden index, with a sensitivity of 91% and a specificity of 91%, significantly exceeding the performance of the IBD-REFER criteria (sensitivity, 99%; specificity, 34%). In validation datasets, the AUC was significantly higher in our model than in the IBD-REFER (AUC=0.94 [95% CI: 0.86–1] versus 0.67 [95% CI: 0.63–0.7]; P<0.01; Figure 3b).
In the sensitivity analysis, we explored the utility of the simplified versions of the model without the ultrasound features (Limberg level >1). The performance of the simplified versions was inferior to that of the models that incorporated the ultrasound features (AUC=0.94 [95% CI: 0.91–0.97] versus 0.97 [95% CI: 0.95–0.98]).
The predicted probabilities of being classified as IBD were found to have a moderate to strong positive association with clinical (ρ =0.569 and 0.463, P<0.01), endoscopic (ρ =0.631 and 0.603, P<0.01), and histological (ρ =0.693 and 0.66, P<0.01) severity of IBD in both the training and test sets (Supplementary Figure 4).
To assess the impact of single imputation, a complete-case sensitivity analysis was performed (n = 311). The final logistic regression model based on complete cases retained the same six predictors as the main model and yielded similar coefficients and intercept values (Supplementary Table 3). Both models achieved the same AUC of 0.94 (95% CI: 0.86–1) in the validation cohort.
Discussion
This study constructed a time- and cost-efficient digital model for the early identification of children with pediatric IBD on the basis of noninvasive test results. The developed model achieved good classification accuracy and showed robust predictive capacity through internal and temporal external validations. Additionally, we explored the relationship between the regression model and IBD clinical, endoscopic, and histological severity. To our best of knowledge, our study enrolled the largest sample size of pediatric IBD cases. The unique advantage of this study is that primary healthcare personnel can identify IBD at an early stage through noninvasive examinations, facilitating patient referral and assisting accelerated endoscopic diagnosis.
Delayed diagnosis is associated with growth failure, more extensive disease, poorer response to medical treatment, increased need for surgery, and decreased health-related quality of life.27–29 Therefore, early identification and treatment of pediatric IBD are necessary. Unfortunately, the clinical manifestations of IBD are often nonspecific, and neither patient history nor physical examination can accurately distinguish IBD from functional or other gastrointestinal disorders.30 The diagnostic delay in our cohort underscores this issue, and the access of children at high risk of pediatric IBD to specialist resources may be limited. Furthermore, the increasing global incidence of IBD pressurize healthcare systems to accommodate the growing number of patients with IBD.31 Developing and implementing tools to assist clinicians in identifying patients at high risk of IBD is a strategy that ensures timely diagnosis and rational allocation of healthcare resources.
The initial index is a questionnaire developed by the International Organization for IBD based on symptoms and signs alone, but it showed poor sensitivity and specificity when it was validated across centers.10,32 Pediatricians also use noninvasive tools, including clinical disease activity indices and routine laboratory test results, such as CRP, ESR, and FC.33 Although these tools serve as nonspecific markers of inflammation, their utility in isolation for diagnosis is limited. IBD-REFER has provided methods for distinguishing IBD on the basis of clinical symptoms and biochemical markers, aiding in early referral.10 However, in the training dataset of this study, the specificity of the IBD-REFER diagnosis for children appeared low. Compared with clinical symptoms and inflammatory markers, ultrasonography can provide more direct visualization of intestinal inflammatory changes. Its accuracy in diagnosing intestinal inflammation is limited if the lesions are superficial or confined to areas in which ultrasound detection is poor, eg, the small intestine or rectum.34 Therefore, constructing a model with multiple levels of indicators is an appropriate option.
We included ultrasound indicators in the study model, and the importance ranking based on the random forest analysis indicated that bowel wall thickening with accompanying blood flow is the best diagnostic indicator for the classification models. Despite longer disease duration correlating with a higher probability of abnormalities in ultrasound, our study found that even in the early stages of disease (within 2 months), ultrasound can still achieve good diagnostic accuracy (Supplementary Figure 2). It is worth noting that, unlike clinical symptoms and biochemical markers, ultrasonography has weaknesses including operator dependency, which may also limit the generalizability of our model. However, a recent study35 reported that pediatric gastroenterologists can achieve good consistency with ultrasound experts in detecting bowel wall thickening after 1 month of short-term training about intestinal ultrasonography, which undoubtedly demonstrates the accessibility and convenience of the ultrasound method. The inclusion of Limberg level >1, a transabdominal intestinal ultrasound indicator, in this model ensures the scanning of the entire intestine length rather than focusing on a single segment. This indicator explores the qualitative assessment of intestinal wall thickening with blood flow. Compared with other indicators such as intestinal wall layering and specific segmental intestinal wall thickness, the Limberg level requires lower operational demands, making it advantageous for implementation in primary healthcare settings.
There are some limitations in the current study. First, this was a retrospective single-center study, and no geographical external validation was conducted. Our hospital is China’s largest IBD diagnosis and treatment center, with many newly diagnosed and referred patients. The high prevalence of IBD among our study population may be beneficial for the diagnostic performance of the model, which limits the external validity of our diagnostic tool to an extent. Second, although the sample size of this study is larger than that of existing IBD-referred studies, the number of IBD diagnoses was still small compared with that of non-IBD diagnoses. Future research should be conducted in a larger, multi-center setting to validate and refine the model. Third, children differ from adults as there are distinct developmental stages during childhood. Owing to the limited sample size, we combined younger and older children in our discussion. However, future research should systematically explore early noninvasive diagnostic models to accommodate different age groups. Fourth, the applicability of our model may be limited in centers without access to experienced pediatric IUS operators. The use of intestinal ultrasound in pediatric care remains restricted in many settings due to the lack of trained personnel and standardized protocols, which may affect reproducibility and real-world implementation. Finally, incorporation bias may have occurred because IUS operators were not blinded to the patients’ clinical information. Although this reflects routine clinical practice, where sonographers often interpret ultrasound findings based on available clinical data, it may lead to an overestimation of diagnostic performance, particularly concerning the contribution of IUS-related variables to the model. Future studies should adopt blinded IUS assessments to more rigorously evaluate the model’s robustness and minimize the risk of observer bias.
Conclusions
We developed a model based on rapid, simple, and cost-effective noninvasive tests and demonstrated its potential as a digital tool for the early identification of children with IBD. This is particularly important for IBD management, as the disease can progress rapidly and lead to serious complications if not diagnosed and treated promptly. Our findings suggest that a Limberg score >1 plays a key role in distinguishing between IBD and non-IBD cases. While promising, the model requires external validation in multicenter studies across diverse clinical settings before it can be recommended for routine implementation. Importantly, it is designed to complement, not replace, endoscopic evaluation.
Data Sharing Statement
Our data are available for review if required.
Ethics Approval Statement
This study was approved by the Ethics Review Committee of the Children’s Hospital of Fudan University (2023–30) and conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from the parents or legal guardians of all participants who were under the age of majority, in accordance with the approved ethical guidelines.
Consent for Publication
We hereby consent to the publication of the provided images, materials and confirm that we have reviewed the article content to be published.
Acknowledgments
We would like to thank all the patients and their families who participated in this study, as well as the staff of the gastroenterology department of Children’s Hospital of Fudan University who assisted with data collection. We would like to thank Weili Yan from the Children’s Hospital of Fudan University for providing valuable advice. We would like to thank Weili Yan from the Children’s Hospital of Fudan University for providing valuable advice. We are grateful to the Pathology Department of Sir Run Run Shaw Hospital for providing the pathology report and its interpretation.
Author Contributions
Wu and Sun collected and analyzed the data and drafted the manuscript. Qin performed intestinal ultrasound examinations and recorded the parameters. Tang and Wang performed the endoscopy examination. Wang and Huang developed the study design and revised the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Shanghai Municipal Health Commission (Project number; 202340216).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Agrawal MA-O, Jess T. Implications of the changing epidemiology of inflammatory bowel disease in a changing world. United Eur Gastroenterol J. 2022;10(10):1113–1120. doi:10.1002/ueg2.12317
2. Kuenzig ME, Fung SG, Marderfeld L, et al. Twenty-first century trends in the global epidemiology of pediatric-onset inflammatory bowel disease: systematic review. Gastroenterology. 2022;162(4):1147–1159e1144. doi:10.1053/j.gastro.2021.12.282
3. Krishna M, Britto S, Qian J, Ihekweazu F, Rodriguez JR, Kellermayer R. Diagnostic delay and colectomy risk in pediatric ulcerative colitis. J Pediatr Surg. 2020;55(3):403–405. doi:10.1016/j.jpedsurg.2019.03.012
4. Cantoro L, Monterubbianesi R, Falasco G, et al. The earlier you find, the better you treat: red flags for early diagnosis of inflammatory bowel disease. Diagnostics. 2023;13(20):3183. doi:10.3390/diagnostics13203183
5. Mählmann LA-O, Gerber M, Furlano RI, et al. Psychological wellbeing and physical activity in children and adolescents with inflammatory bowel disease compared to healthy controls. BMC Gastroenterol. 2017;17(1):160. doi:10.1186/s12876-017-0721-7
6. Blackwell J, Saxena S, Jayasooriya N, et al. Prevalence and duration of gastrointestinal symptoms before diagnosis of inflammatory bowel disease and predictors of timely specialist review: a population-based study. J Crohn's Colitis. 2020: jjaa146. 10.1093/ecco-jcc/jjaa146
7. Vardi I, Chermesh I, Werner L, et al. Monogenic inflammatory bowel disease: it’s never too late to make a diagnosis. Front Immunol. 2020;11:1775. doi:10.3389/fimmu.2020.01775
8. Sempere L, Bernabeu P, Cameo J, et al. Gender biases and diagnostic delay in inflammatory bowel disease: multicenter observational study. Inflamm Bowel Dis. 2023;29(12):1886–1894. doi:10.1093/ibd/izad001
9. Danese S, Fiorino G, Mary JY, et al. Development of red flags index for early referral of adults with symptoms and signs suggestive of crohn’s disease: an ioibd initiative. J Crohn's Colitis. 2015;9(8):601–606. doi:10.1093/ecco-jcc/jjv067
10. Atia O, Shosberger A, Focht G, et al. Development and validation of the ibd-refer criteria: early referral for suspected inflammatory bowel diseases in adults and children. Crohn's Colitis 360. 2020;2(2):otaa027. doi:10.1093/crocol/otaa027
11. Bots S, De Voogd F, De Jong M, et al. Point-of-care intestinal ultrasound in ibd patients: disease management and diagnostic yield in a real-world cohort and proposal of a point-of-care algorithm. J Crohn Colitis. 2022;16(4):606–615. doi:10.1093/ecco-jcc/jjab175
12. Calabrese E, Rispo A, Zorzi F, et al. Ultrasonography tight control and monitoring in crohn’s disease during different biological therapies: a multicenter study. Clin Gastroenterol Hepatol. 2022;20(4):e711–e722. doi:10.1016/j.cgh.2021.03.030
13. Kellar A, Dolinger M, Novak KL, Chavannes M, Dubinsky M, Huynh H. Intestinal ultrasound for the pediatric gastroenterologist: a guide for inflammatory bowel disease monitoring in children: expert consensus on behalf of the international bowel ultrasound group (IBUS) pediatric committee. J Pediatr Gastroenterol Nutr. 2023;76(2):142–148. doi:10.1097/MPG.0000000000003649
14. He L, Sun Y, Hu X, Yao Q. Diagnostic performance of magnetic resonance enterography and ultrasound in children with inflammatory bowel diseases: a diagnostic test accuracy meta-analysis. Eur Radiol. 2022;32(2):1330–1341. doi:10.1007/s00330-021-08172-6
15. Allocca M, Furfaro F, Fiorino G, Peyrin-Biroulet L, Danese S. Point-of-care ultrasound in inflammatory bowel disease. J Crohn's Colitis. 2021;15(1):143–151. doi:10.1093/ecco-jcc/jjaa151
16. Maconi G, Nylund K, Ripolles T, et al. EFSUMB recommendations and clinical guidelines for intestinal ultrasound (GIUS) in inflammatory bowel diseases. Ultraschall Med. 2018;39(3):304–317. doi:10.1055/s-0043-125329
17. van Wassenaer EA, de Voogd FAE, van Rijn RR, et al. Diagnostic accuracy of transabdominal ultrasound in detecting intestinal inflammation in paediatric IBD patients-a systematic review. J Crohn's Colitis. 2019;13:1501–1509. doi:10.1093/ecco-jcc/jjz085
18. Dilillo D, Zuccotti GV, Galli E, et al. Noninvasive testing in the management of children with suspected inflammatory bowel disease. Scand J Gastroenterol. 2019;54(5):586–591. doi:10.1080/00365521.2019.1604799
19. Collins GS, Reitsma JB, Altman DG, Moons KG. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): the TRIPOD statement. BMJ. 2015;350:g7594. doi:10.1136/bmj.g7594
20. van Wassenaer EA-OX, Benninga MA, van Limbergen JL, D’Haens GR, Griffiths AM, Koot BGP. Intestinal ultrasound in pediatric inflammatory bowel disease: promising, but work in progress. Inflamm Bowel Dis. 2022;28(5):783–787. doi:10.1093/ibd/izab125
21. Marin AM, Calapod OP, Moldoveanu AC, Tribus LC, Fierbințeanu-Braticevici C. Non-invasive ultrasonographic score for assessment of the severity of inflammatory bowel disease. Ultrasound Med Biol. 2021;47(4):932–940. doi:10.1016/j.ultrasmedbio.2020.11.026
22. Kucharzik T, Wittig BM, Helwig U, et al. Use of intestinal ultrasound to monitor crohn’s disease activity. Clin Gastroenterol Hepatol. 2017;15(4):535–542.e2. doi:10.1016/j.cgh.2016.10.040
23. Levine A, Koletzko S, Turner D, et al. ESPGHAN revised porto criteria for the diagnosis of inflammatory bowel disease in children and adolescents. J Pediatr Gastroenterol Nutr. 2014;58(6):795–806. doi:10.1097/MPG.0000000000000239
24. Marchal-Bressenot A, Salleron J, Boulagnon-Rombi C, et al. Development and validation of the Nancy histological index for UC. Gut. 2017;66(1):43–49. doi:10.1136/gutjnl-2015-310187
25. Breiman L. Random forests. Machine Learning. 2001;45:5–32. doi:10.1023/A:1010933404324
26. Ishwaran H, Kogalur UB, Gorodeski EZ, Minn AJ, Lauer MS. High-dimensional variable selection for survival data. J Am Stat Assoc. 2010;105(489):205–217. doi:10.1198/jasa.2009.tm08622
27. Jiménez Treviño S, Pujol Muncunill G, Martín-Masot R, et al. Spanish pediatric inflammatory bowel disease diagnostic delay registry: SPIDER study from sociedad española de gastroenterología. Hepatología y Nutrición Pediátrica Front Pediatr. 2020;8:584278.
28. Ajbar A, Cross E, Matoi S, et al. Diagnostic delay in pediatric inflammatory bowel disease: a systematic review. Dig Dis Sci. 2022;67:5444–5454. doi:10.1007/s10620-022-07452-5
29. Jayasooriya N, Baillie S, Blackwell J, et al. Systematic review with meta-analysis: time to diagnosis and the impact of delayed diagnosis on clinical outcomes in inflammatory bowel disease. Aliment Pharmacol Ther. 2023;57(6):635–652. doi:10.1111/apt.17370
30. Sakurai T, Saruta M. Positioning and usefulness of biomarkers in inflammatory bowel disease. Digestion. 2023;104(1):30–41. doi:10.1159/000527846
31. Coppell KJ, Galts CP, Huizing FY, et al. Annual incidence and phenotypic presentation of ibd in southern New Zealand: an 18-year epidemiological analysis. Inflamm Intest Dis. 2018;3(1):32–39. doi:10.1159/000492615
32. Fiorino G, Bonovas S, Gilardi D, et al. Validation of the red flags index for early diagnosis of crohn’s disease: a prospective observational IG-IBD study among general practitioners. J Crohn's Colitis. 2020;14(12):1777–1779. doi:10.1093/ecco-jcc/jjaa111
33. Menees SB, Powell C, Kurlander J, Goel A, Chey WD. A meta-analysis of the utility of C-reactive protein, erythrocyte sedimentation rate, fecal calprotectin, and fecal lactoferrin to exclude inflammatory bowel disease in adults with IBS. Am J Gastroenterol. 2015;110(3):444–454. doi:10.1038/ajg.2015.6
34. Parente F, Greco S, Molteni M, et al. Role of early ultrasound in detecting inflammatory intestinal disorders and identifying their anatomical location within the bowel. Aliment Pharmacol Ther. 2003;18(10):1009–1016. doi:10.1046/j.1365-2036.2003.01796.x
35. van Wassenaer EA, van Rijn RR, de Voogd FAE, et al. A healthcare physician can be trained to perform intestinal ultrasound in children with inflammatory bowel disease. J Pediatr Gastroenterol Nutr. 2022;74(6):e143–e147. doi:10.1097/MPG.0000000000003442
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.