")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Economic Burden of Intravenous Decitabine Administration in Patients Affected by Acute Myeloid Leukemia Ineligible for Induction Chemotherapy and Impact of Oral Formulation Introduction: A Micro-Costing Study in Italy
Authors Di Costanzo A , Loreto L , Vassallo C , Fiorentino F
Received 9 September 2024
Accepted for publication 1 February 2025
Published 13 March 2025 Volume 2025:17 Pages 171—187
DOI https://doi.org/10.2147/CEOR.S495401
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Dean Smith
Alessandra Di Costanzo, Luca Loreto, Chiara Vassallo, Francesca Fiorentino
Real World Solutions, IQVIA Solutions Italy S.r.l., Milan, Italy
Correspondence: Chiara Vassallo, Real World Solutions, IQVIA Solutions Italy s.r.l., Via Fabio Filzi 29, Milan, 20124, Italy, Tel +39 333 9326974, Fax +39 02 30 35 09 088, Email [email protected]
Purpose: Intravenous (IV) decitabine is a therapeutic option for patients with newly diagnosed acute myeloid leukemia (AML) ineligible for induction chemotherapy. Recently, the oral formulation of decitabine-cedazuridine demonstrated comparable efficacy and safety to IV decitabine, and pharmacokinetic equivalence. This study estimates the direct non-drug healthcare costs of IV decitabine administration in Italy, including central venous catheter (CVC) and infection management, and assesses the economic impact of oral decitabine introduction.
Methods: A micro-costing analysis from the Italian National Health Service (NHS) perspective was developed in four steps: 1) identification of the phases of IV and oral decitabine administration process, including CVC and infection management; 2) estimation of resource consumption, frequencies and proportion of patients for each phase; 3) collection of unit costs; 4) development of a cost analysis model. Inputs were retrieved from literature, public sources, IQVIA proprietary databases and a panel composed of clinicians, nurses and hospital pharmacists working in oncology departments. Two scenarios were explored: the first applying the economic impact to the population of interest over three years, the second including the cost of blood transfusions.
Results: The analysis estimated a total non-drug administration cost per patient of € 3574.6 and € 781.4 for a treatment course with IV and oral decitabine, respectively, leading to a cost impact of oral drug introduction of - € 2793.2 (− 78.1%). The first scenario estimated a total saving for the Italian NHS of € 1.09 million over three years, the second scenario estimated a potential additional impact of - € 3418.6/patient due to transfusions.
Conclusion: The administration of oral versus IV decitabine is expected to generate cost savings for the Italian NHS in terms of drug administration, CVC and infection management, in patients with AML ineligible for induction chemotherapy.
Keywords: economic evaluation, cost analysis, intravenous therapy, oral therapy, administration route, infections
Introduction
Acute myeloid leukemia (AML) is a hematopoietic malignancy of bone marrow stem cells with abnormal differentiation and clonal accumulation of myeloid stem cells.1–3 In Italy, there is an estimated annual incidence of 3.5 cases per 100,000 individuals,4 typically found in older patients, with a median age at diagnosis of about 70 years.5 Similar to other blood tumors, AML may cause severe anemia, neutropenia and thrombocytopenia, often resulting in dependence on blood transfusions6 and in the associated risks of hemorrhagic and infectious complications.7
The increasing incidence of AML with advancing age5 may compound existing comorbidities and genetic alterations, further exacerbating this frail population and severely restricting its treatment options.8 Indeed, it is currently estimated that in Italy half of newly diagnosed adults with AML are ineligible for standard induction chemotherapy.5
For these patients, a possible therapeutic option is the administration of intravenous (IV) decitabine,9,10 a hypomethylating agent that inhibits DNA methyltransferase, with a direct cytotoxic effect on cellular differentiation and apoptosis.8 Despite decitabine showing good efficacy and safety8 in the outpatient setting,11 also for elderly and unfit patients,12 its IV mode of administration might pose several challenges for these patients and the National Health Service (NHS). Indeed, existing literature on IV drug administration in patients affected by oncological diseases highlights the negative impact on patients’ quality of life (QoL) due to prolonged infusion times and frequent hospital visits.6,13–18 Additionally, the use of a central venous catheter (CVC) in such immunocompromised and frail patients19,20 increases this burden, and implies potential infectious complications associated with both frequent hospital access and IV administrations.15,21 From the NHS perspective, IV administration leads to costs of consumables and healthcare professional (HCP) time.13,14,22,23
In this context, characterized by the absence of exclusively oral treatments for patients with newly diagnosed AML ineligible for induction chemotherapy and by the significant burden of IV infusions on both patient’s and caregiver’s QoL, the introduction of an oral drug may constitute an opportunity to shift the whole treatment paradigm and recalibrate patient management.15 This transition to oral treatments taken at home would reduce patients’ dependence on hospitals, thus contributing to optimize hospital resource utilization,9 and alleviate the burdens experienced by patients, their families and caregivers.24,25
In September 2023, the European Medicines Agency (EMA) granted the marketing authorization for an oral formulation of decitabine-cedazuridine (hereinafter referred to as “oral decitabine”) which, although being registered by EMA as a novel active substance,26 can be considered a pharmacokinetically equivalent oral version of IV decitabine and comparable in terms of both efficacy and safety.27–30 This equivalence is supported by the findings of the registrational, randomized, crossover, pharmacokinetic Phase 3 ASCERTAIN clinical trial,28–30 which compared the systemic exposure of decitabine when administered intravenously at a dose of 20 mg/m² for 5 days with that of orally administered decitabine 35 mg with cedazuridine 100 mg for 5 days. The results demonstrated equivalent systemic decitabine exposures between the two formulations, with demethylation rates showing a minimal difference of ≤1.1%.28–30 Furthermore, the median overall survival, clinical response, and safety profile observed with oral decitabine were consistent with those previously reported for IV decitabine,8,28 underscoring the therapeutic interchangeability of the two formulations and providing robust evidence that supports the use of oral decitabine in patients with newly diagnosed AML ineligible for induction chemotherapy.
The primary objective of this study is to estimate the direct non-drug healthcare costs associated with IV and oral administrations of decitabine in patients affected by newly diagnosed AML ineligible for induction chemotherapy in Italy. The analysis implements a micro-costing approach and considers costs associated with drug administration, including CVC-related processes and the management of infections. Given that in Italy during the study period, oral decitabine was not commercialized, price was undefined, and treatment costs were not estimated, and the study exclusively focused on administration costs.
In addition, the study aims to estimate the expected economic impact of the introduction of an oral formulation of decitabine.
Materials and Methods
The analysis uses a bottom-up micro-costing approach and considers the perspective of the Italian NHS, including the cost of process-related consumables, HCP time and hospital overhead for drug administration and CVC management. Recent literature shows that hospital overhead costs are derived as a percentage of the cost of consumables and HCP time.13,14 In alignment with this literature, our study applies a 25% overhead rate.14 To estimate costs of different types of infections,31–33 tariffs have been applied in order to absorb the wide variability in management procedures.34
The study was developed in four steps: 1) identification of the phases involved in the administration of IV and oral oncology treatment administration process, including the administration itself, CVC insertion, follow-up and removal, and infection management; 2) estimation of resource consumption, frequencies of consumption and proportion of patients associated with each phase; 3) collection of unit costs and 4) integration of the information through a cost analysis model.
Specifically, the cost associated with each identified process was calculated by multiplying the resources consumed in each phase by their unit cost. The overall cost per patient was then determined by multiplying this value by the frequency of procedures and the proportion of patients estimated to undergo each.
Results are reported per patient treated with IV administration of decitabine, with oral administration of decitabine, and the differences between the two, considering the first and subsequent treatment cycles (cycle 1 and cycle 2+, respectively), and the entire treatment duration. Costs are expressed in Euros (€) for the year 2023 (for costs which required an adjustment for inflation, the coefficient referred to 2023 was considered more robust because it was calculated over the whole year, while the inflation coefficient for 2024 was available only for the first months of the year).
Two scenario assessments were then developed: the first one applies the expected impact of the introduction of oral decitabine to the population of interest over a three-year time horizon, while the second one includes the cost of administering blood transfusions and hypothesizes a potential cost impact from oral formulation introduction.
Identification of Processes and Phases
The most recent national and international guidelines,31,32,35,36 hospital protocols,37–39 national reports40 and published literature11,13,22,33,41 were assessed and reviewed to identify the processes to administer an IV and oral treatment in the population of interest, to insert, manage and remove a CVC and to manage infections. The retrieved information was integrated and validated with data extracted from an expert panel collaborating with IQVIA. This panel consisted of 6 oncologists, 6 hospital pharmacists and 6 nurses working in oncology departments distributed across Italian regions and representing the national context. In case no information was available about oral decitabine, assumptions based on either similar oral anticancer drugs or IV decitabine were made.
To ensure representation from the Italian NHS perspective, we only considered those processes performed within hospitals.
Resource Consumption
Resources considered in the analysis for drug administration and CVC management include process-related consumables, HCP time and hospital overhead.
To estimate the cost per patient for the whole treatment duration, frequencies of procedure per cycle, the average number of treatment cycles and the proportion of patients going through each procedure were investigated, looking for differences between patients treated with IV and oral drugs.
Similarly to identification of processes, data on resource consumption, frequencies and treatment duration were retrieved from the synergism between protocols,37–39 guidelines,31,32,35,36 reports40 and published literature11,13,22,33,41 and validated with the expert panel.
Drug-specific resource consumptions such as decitabine IV infusion duration and number of treatment days per cycle were obtained from decitabine’s summary of product characteristics27,42 and validated with published literature.9,43
Unit Costs Collection
Unit costs of consumables were retrieved from the IQVIA Medical Devices Hospital Consumption audit (a proprietary database containing information on quantities and costs of medical devices purchased by hospitals participating in medical device hospital tracking from 2014 onwards),44 IQVIA sales data,45 published literature46 and national tariffs.47–49
Direct costs associated with HCP time were estimated through the human capital approach,34,50 considering the most recent (2021) HCP annual salaries reported from the Italian Ministry of Economy and Finance51 adjusted for inflation to 2023.52
For infection management, resource consumption was estimated directly using national tariffs47,48 and unit costs of pharmacological treatments.40,49
Sensitivity Analysis
To test the robustness of our results, a deterministic sensitivity analysis (DSA) was conducted by applying ±20% variations on the most uncertain inputs of the study such as HCP time, unit costs, CVC utilization and infection incidence. Moreover, an additional phase in the IV administration process, a different percentage of overhead costs and an alternative input for infection incidence were included in the sensitivity analysis due to uncertainty that emerged from the assessed sources.
Scenario Assessment 1: Impact on NHS Budget in a Three-year Time Horizon
To estimate the extent of the impact of the introduction of oral decitabine on the NHS budget in terms of drug administration, CVC and infection management cost, the model compares two scenarios in a three-year time horizon. The first scenario assumes that no oral drug introduction occurs; therefore, the totality of patients with newly diagnosed AML ineligible for induction chemotherapy and receiving decitabine in Italy is treated with IV decitabine. Conversely, the second scenario assumes a gradual introduction of the oral formulation, with a decreasing portion of eligible patients receiving the therapy intravenously.
To identify the number of newly diagnosed patients with AML, ineligible for induction chemotherapy and candidates for decitabine in Italy, the adult Italian population was initially considered.53 To this population, an annual AML incidence rate of 0.009% was applied,5 of which 46.5% was considered ineligible for induction chemotherapy.5 Subsequently, the proportion of patients eligible to receive decitabine in Italy was retrieved from IQVIA Oncoview database,54 a proprietary database collecting real-world data on cancer diseases in Italy through monthly structured interviews with 480 specialized clinicians, and estimated at 18.0%. Finally, a corrective factor equal to +0.18% was considered to account for the increasing adult population over years 1–3 of this study.53 Therefore, the number of newly diagnosed AML patients not eligible for induction chemotherapy and candidates to receive decitabine in Italy was estimated at 376, 377 and 378, respectively, for year 1, year 2 and year 3.
As for oral drug penetration, oral decitabine-cedazuridine market share in the second scenario was estimated to be 13%, 32% and 58%, respectively, for year 1, year 2 and year 3.55
Scenario Assessment 2: Inclusion of Blood Transfusion Cost
Both IV and oral decitabine have been proven to reduce patients’ dependence on transfusions of red blood cells and platelets.28–30,56 As some expert insights suggested that patients treated with oral oncology drugs may exhibit lower transfusion dependence compared to those receiving IV therapies, we estimated the cost associated with the transfusion of blood components in patients newly diagnosed with AML ineligible for induction chemotherapy in order to explore the possibility of additional cost savings per patient treated with the oral formulation.
In alignment with the methodology presented in previous sections, details on phases, activities, and resource consumption were retrieved from national reports,57 national institutional documents,58,59 published literature,60 national tariffs,48 IQVIA sales data45 and integrated with expert panel insights. Details are provided in supplementary materials (Tables S1-S3).
Specifically, considering the absence of published data comparing IV and oral decitabine in terms of transfusion needs, we assessed explorative scenarios by assuming that patients treated with the oral formulation would exhibit an average reduction in transfusion dependence by 10%, 20%, and 30% after the first cycle, compared to those receiving IV decitabine.
Results
Identification of Processes and Phases
Identified processes and their specifics are outlined in Table 1.
 |
Table 1 Phases, Activities and Consumables Consumption by Process |
Based on assessed sources, administration of IV decitabine includes a drug preparation phase in the hospital pharmacy and the infusion itself. In contrast, when using oral formulations of decitabine, the only phase is the dispensation by the hospital pharmacist.
The process for managing a CVC, due to IV infusion of decitabine or transfusion support, includes its insertion, periodic follow-up, and eventual removal.
The most frequent infections are catheter-related bloodstream infections (CRBSI) from use of CVCs, and hospital-acquired infections (HAI) associated with hospital-based IV administration and check-up visits. In both cases, the infection management process involves a preliminary diagnosis, a pharmacological treatment at home or in hospital with a subsequent follow-up.
All identified processes occur mostly in the outpatient setting (day-hospital or ambulatory care) and rarely require an inpatient stay.
CVC and infection-related processes are valid for both patients treated with IV and oral drugs, as no variations in phases or activities emerged between different treatment settings in all the considered processes.
Resource Consumption
The quantity of consumables and the amount of HCP time required in each process are reported in Tables 1 and 2 respectively. Possible economies of scale were accounted for by considering the number of consumables and professionals serving more than one patient simultaneously. In terms of consumables, no differences emerged among different treatment cycles, whereas some variations emerged for HCP times: in particular, nurse time for IV decitabine administration was higher in cycle 1 due to a longer post-infusion monitoring period, while the clinicians’ involvement in the initial prescription of therapy before the first drug administration resulted in longer times during the first therapy cycle.
 |
Table 2 HCP Involvement Time by Process and Phase |
Phase-related frequencies and proportion of patients going through each procedure are reported in Table 3.
 |
Table 3 Parameters for Cost Estimations per Cycle by Phase and by Treatment Type |
Specifically, IV decitabine is prepared and administered during the first 5 days of a 28-day cycle, while oral decitabine, despite being taken daily for the first 5 days of a 28-day cycle, is estimated to be dispensed once per treatment cycle, as generally happens for oral anticancer drugs. CVC follow-up occurs weekly, and it was assumed that (i) CVC insertion occurs in cycle 1, (ii) infectious complications and related CVC removals or re-insertions occur only in cycles 2+, and (iii) no CVC removal takes place at the conclusion of therapy as it is usually retained for transfusion support.
Throughout these processes, both patients receiving IV and oral decitabine undergo weekly check-up visits and examinations to monitor disease progression. These assessments often coincide with drug administration and CVC follow-up sessions. However, these activities are directly related to the disease process and are not influenced by the route of administration; hence, it does not result in a cost differential between different routes of administration. Consequently, resource consumption associated with check-up visits and examinations has not been considered in the present analysis.
Lastly, regarding treatment duration, panel data indicated an average of 6 cycles for patients treated with IV decitabine, and the same duration was assumed for patients treated with oral decitabine.
In terms of proportions, it emerged from the panel that patients treated with an IV drug need access to catheter more frequently than patients treated with an oral drug (69% and 38%, respectively) since the latter requires it exclusively for transfusion support and not for drug administration. Given that the utilization of catheter is associated with the increased risk of CRBSIs and frequent access to the hospital for drug administration, a lower CVC use in patients treated with oral decitabine means reduced exposure to both CRBSIs and HAIs. Indeed, along the whole treatment duration with IV decitabine, infections are estimated to occur in 57% of cases, 22% of which are CRBSIs and 10% are HAIs. These estimates are well aligned with real-world data in the European context. Various studies on AML report overall infection rates ranging from 45% to 73%,61,62 averaging around 59%, which closely matches our estimate of 57%. Additionally, CRBSIs account for approximately 25% of total infections,63 consistent with our figure of 22%. For HAIs, incidence rates have been reported up to 9%,64 further validating our estimate of 10%. As for oral decitabine, while CRBSIs incidence is applied to fewer patients with a CVC, HAIs percentage reduces to 5% due to fewer visits to the hospital.
In addition to infectious complications, it was estimated that due to the invasive nature of both catheter insertion and IV drug administration, patients treated with IV decitabine are more often hospitalized for the drug administration when compared to those receiving oral decitabine (7% vs 4% of hospitalized patients per cycle, respectively). As no differences appeared between inpatient and outpatient administration-related processes, additional costs for hospitalized patients (eg, hospital bed, meals, routine visits, etc.) were estimated and applied to the incremental percentage of patients (about 3% per cycle) who would require hospitalization for receiving intravenous decitabine rather than the oral form.
Total Costs
Costs per patient per treatment cycle are detailed in Table 4. Consistent with different frequencies and different HCP time requirements, costs are usually higher in cycle 1.
 |
Table 4 Cost per Patient per Cycle by Treatment Type |
Including overhead, the cost per patient receiving IV decitabine amounts to € 687.4 and € 577.5, respectively, in cycle 1 and cycles 2+, and both are primarily driven by treatment administration costs; when considering oral decitabine, these values are reduced to € 176.3 and € 121.1, respectively, with CVC management being the largest cost component.
Considering the whole treatment duration (Figure 1), the total costs per patient treated with IV and oral decitabine were estimated to be € 3574.6 and € 781.4, respectively, with an overall cost reduction of € 2793.2 per patient (−78.1%).
 |
Figure 1 Cost per patient per whole treatment duration by treatment type and cost component. Abbreviations: CRBSI, catheter-related bloodstream infection; CVC, central venous catheter; HAI, hospital-acquired infection; IV, intravenous. |
Introduction of oral decitabine is estimated to generate cost savings in each of the processes included in the analysis. In particular, treatment administration costs are expected to be reduced by 93.1%, since no preparation and infusion are needed when taking an oral drug. CVC and CRBSI management costs are also expected to decrease by 45.0%, due to a lower percentage of patients requiring CVC insertion when treated with an oral drug. Ultimately, HAI management costs would be reduced by 50.3% because patients treated with oral decitabine are not expected to access hospitals as frequently, resulting in reduced exposure to HAIs.
In terms of HCP time allocation, Table 5 reports the overall working days spent by each HCP per treatment route with the relative cost. Results show that all HCPs would save time, but most of the savings are estimated to be achieved by nurses, for which the introduction of oral decitabine would spare 4.4 working days per patient throughout the whole treatment duration (4.8 vs 0.4 for patients treated with IV and oral decitabine, respectively), meaning that the time spent for each patient treated with IV decitabine may be re-allocated to treat 11 patients with oral decitabine.
 |
Table 5 HCP Working Days per Patient per Whole Treatment Duration by Treatment Type |
Sensitivity Analysis
Results of DSAs are presented in Figure 2.
 |
Figure 2 Tornado diagram presenting sensitivity analysis results. Abbreviations: HCP, healthcare professional; IV, intravenous. Notes: aIt refers to the administration of prophylactic treatments with cortisone and antihistamines suddenly before IV administration to prevent adverse events; bLower overhead cost means applying overhead costs as 20% of the cost of non-drug consumables and HCP time;13 cIV decitabine clinical trial65 reports the incidence of “Infections and infestations” of any grade during whole treatment duration, such value ranges from 45% (assuming more infections occurring concurrently) to 76% (assuming no infections occurring concurrently). |
Estimated difference in costs per patient of IV and oral decitabine administration is most sensitive to HCP time and unit cost variations (from - € 3127.9 to - € 2458.5 per patient, with respect to a baseline value of - € 2793.2); however, impact on cost savings does not exceed ±12%, confirming robustness of results. In all DSAs, the introduction of oral decitabine consistently emerges as a cost-saving alternative.
Scenario Assessment 1: Impact on NHS Budget in a Three-year Time Horizon
Results of the scenario assessment are reported in Figure 3. Considering costs of drug administration, CVC-related processes and infection management costs, the introduction of oral decitabine over a three-year time horizon is estimated to result in a potential cost saving for the Italian NHS equal to - € 1.09 million (−26.9%): from a total of € 4.04 million considering only IV decitabine to € 2.95 million considering the penetration of its oral formulation.
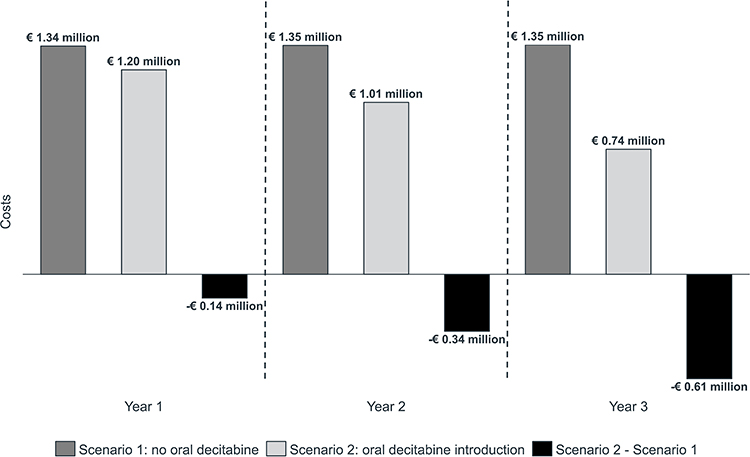 |
Figure 3 Cost impact of oral drug introduction by year. |
Scenario Assessment 2: Inclusion of Blood Transfusion Cost
Inclusive of blood donation, haemocomponent preparation, patient pre-medication and monitoring, the cost for a single blood transfusion was estimated at € 393.6, € 481.6 and € 805.0, respectively, for an infusion of red blood cells, platelets and both components.
Considering the whole treatment duration for a patient diagnosed with AML and ineligible for induction chemotherapy, the cost corresponds to a total of € 15505.1. Assuming an average reduction in transfusion dependence of 10%, 20% and 30% in subsequent cycles for patients treated with oral decitabine, the cost savings will increase at € 3932.8, € 5072.3 and € 6211.8, respectively, as presented in Figure 4.
 |
Figure 4 Cost impact per patient including blood transfusion cost. Abbreviation: IV, intravenous. |
Discussion
The administration of intravenous decitabine represents a possible therapeutic option for the treatment of patients with newly diagnosed AML who are ineligible for standard induction chemotherapy.9,10
In September 2023, the EMA approved the oral formulation of decitabine-cedazuridine for this population, based on the registrational, randomized, crossover, pharmacokinetic phase 3 ASCERTAIN clinical trial that demonstrated comparable efficacy and safety and pharmacokinetic equivalence to IV decitabine.27–30
The present analysis estimated, through a bottom-up micro-costing approach, the cost sustained by the Italian NHS to administer IV decitabine and the potential economic impact resulting from the introduction of the oral formulation, including costs related to CVC and infection management.
The cost per patient for a course of treatment with IV and oral decitabine was estimated to be € 3574.6 and € 781.4, respectively, leading to an overall cost impact of oral drug introduction of - € 2793.2 (−78.1%). In particular, the shorter time required for oral decitabine administration, reduced CVC catheter needs and reduced exposure to infections would all contribute to cost savings.
Far from being merely economic, savings also extend to HCP time: the introduction of oral decitabine is estimated to spare 4.4 working days for nurses throughout the whole treatment duration, potentially allowing nurses to treat 11 additional patients or re-invest time in other activities, making it possible for the Italian NHS to address shortages in HCP capacity.66
Being the study conducted from the NHS perspective, these results do not consider the implications for patients’ and caregivers’ quality of life and the associated indirect costs, both of which are expected to improve.13,22–24,67,68 Indeed, recent studies highlight the potential advantages of oral decitabine, evidencing how patients and caregivers can benefit from shorter infusion times and fewer hospital visits, thereby enhancing overall QoL. For instance, a survey conducted in US by Zeidan et al 202418 revealed that 85% of patients experienced improved QoL with oral decitabine compared to intravenous or subcutaneous hypomethylating agents, with 91% reporting less interference with daily life and fewer healthcare visits. Another US study by Zeidan et al 202217 underscored the burdens of injectable hypomethylating agents, noting significant interference with social life, daily activities and pain during administration in 74%, 70%, and 66% of cases, respectively.
At the national and international levels, published literature presents estimates of the cost associated with the administration of IV anticancer drugs in Europe,13,14,22,23 but to the best of our knowledge, there are no studies estimating administration costs in patients treated with either IV or oral decitabine. In addition, as far as we know, our study is the first one including the costs associated with both CVC process and infection management.
In this context, along with the collection of unit costs from relevant Italian tariffs47,49 and literature,46 our study is further enriched by the consultation of the constantly updated proprietary IQVIA Medical Devices Hospital Consumption audit44 representative of about half of national hospital sector and by the collaboration with different HCP professionals including experts in the drug preparation and dispensation processes, such as hospital pharmacists, in addition to clinician and nurses.
Furthermore, our results appear to be consistent with both national13,14 and international22,23 published literature. To enhance the comparability of results, elsewhere published studies were adjusted for inflation to the year 2023, by applying the general revaluation coefficients (excluded tobacco) provided by the Italian National Statistics Institute (ISTAT).52 Additionally, in the case of international studies, the results were also adjusted for purchasing power parity by applying currency conversion rates from the European Statistical Office (Eurostat) relevant to each study’s reference country and Italy.69 In particular, the study by Pradelli et al 202314 aimed at estimating, through a time-motion micro-costing analysis, the cost for the Italian NHS to administer daratumumab in patients diagnosed with multiple myeloma, including the cost of consumables, HCP time, overhead, and chair time. Their estimation was € 84.7, slightly higher than ours (€ 80.3, computed dividing cost for IV decitabine administrations in cycle 2+, equal to € 401.7, by 5 administrations throughout the cycle) due to both longer infusion times for daratumumab and higher unit costs retrieved from a hospital-specific cost center. A similar cost analysis was conducted by Bellone et al 202213 for the IV administration of obinutuzumab in patients with follicular lymphoma, with a higher estimation of € 97.8. In this case, the difference is also attributable to longer infusion times, higher unit costs retrieved exclusively from literature and a less conservative approach with no economies of scale considered. Internationally, Franken et al 201823 estimated a cost for IV administration of trastuzumab and rituximab to be € 51.5, basing their micro-costing estimations on real-world data coming from 6 hospitals in the Netherlands. Their value is lower than ours due to reduced HCP time, shorter infusion duration and lower overhead costs. Lastly, O’Brien et al 201922 conducted a cost analysis for IV administration of trastuzumab in patients with breast cancer in two Irish hospitals, leading to a cost estimation of € 90.6. The difference here is mainly associated with higher unit costs in Irish clinical practice.
Notwithstanding the accuracy of micro-costing estimations,34 we compared our results with Italian national tariffs to further assess the robustness of our analysis. In this regard, our estimations (excluding hospitalization and overhead costs to enhance comparability) are about 50.0% higher in the case of IV decitabine administration (10% of DRG 410)47,59,70 and up to 83.2% higher for CVC-related phases (outpatient national tariffs 38.97.2, 96.57, 89.01.1),48 highlighting how national tariffs adopted to reimburse hospital activities in Italy may be underestimated, in line with findings in other published literature.71–73
Despite its innovative features and contribution, our study also presents some limitations.
First of all, the size of the panel, composed of 18 experts, used to validate and retrieve some inputs may not reflect appropriately the entire national context. Nevertheless, the use of smaller expert panels seems to be a common and accepted practice in various fields of research, including micro-costing healthcare studies. Many recent studies adopting a micro-costing approach have relied on the external validation of limited expert panels ranging from 3 to 7 experts.60,74,75 In comparison, our panel is not only larger but also geographically diverse, encompassing professionals from the south, center, and north of Italy, ensuring a comprehensive representation of the national context and capturing regional variations in resource consumption and clinical practices. Additionally, at the time of its development, our panel was meticulously selected to include a diverse range of professionals with extensive experience, including clinicians, hospital pharmacists, and nurses. This diversity and depth of expertise, in conjunction with generally homogeneous insights suggested from the respondents, significantly enhance the reliability and robustness of our findings, even with a relatively small sample size. Hence, given the robustness demonstrated by the DSA results and the alignment of our estimations with those of studies pursuing similar objectives,13,14,22,23 we believe our findings to be solidly supported.
A second limitation is that no time-motion methodology was undertaken in our analysis. However, the micro-costing approach used for drug administration and CVC management is considered a “gold standard” for cost assessment34 and has been adopted in similar studies;13,60 a less granular approach was adopted only for management of infections, where their complexity would have led us to conduct an overly detailed analysis.34
A third limitation concerns the potential cost impact of oral decitabine related to lower transfusion requirements. It is necessary to emphasize that the results obtained in the second scenario assessment have a mere hypothetical and investigative nature. Although decitabine demonstrated to reduce patients’ dependence on transfusions, a major reduction with oral decitabine was exclusively extrapolated from panel insights, and the respective reduction rates were based solely on assumptions, without robust clinical evidence to support these claims. Therefore, should oral decitabine result in fewer blood transfusion requirements when compared to the IV formulation,76 this result could augment the economic impact observed in our analysis. However, until such evidence is available, the additional cost impact results of oral decitabine related to blood transfusions presented in this study should be interpreted with caution.
Despite these limitations, we believe that our study provides a relevant contribution to the existing published literature, estimating the non-drug healthcare costs associated with the administration of intravenous and oral decitabine in Italy, including costs related to CVC-related processes and to infection management, and we consider it to represent a starting point for further research. In particular, as oral decitabine becomes commercially available, more comprehensive investigations can be conducted, accounting for treatment costs in the analysis, incorporating real-world data on its market adoption and assessing differences in transfusion requirements and relative cost impact with the oral formulation more rigorously.
Conclusion
Our study has estimated the non-drug healthcare costs associated with the administration of IV and oral decitabine for patients with newly diagnosed AML ineligible for induction chemotherapy in Italy. From our results, we conclude that the introduction of the oral formulation of decitabine, with pharmacokinetic equivalence and a comparable efficacy and safety profile to the IV form, would result in cost savings for the Italian NHS in terms of drug administration, CVC-related processes and infection management.
Abbreviations
AML, Acute Myeloid Leukemia; CRBSI, Catheter-Related Bloodstream Infection; CVC, Central Venous Catheter; DRG, Diagnosis-Related Group; DSA, Deterministic Sensitivity Analysis; EMA, European Medicines Agency; HAI, Hospital-Acquired Infection; HCP, Healthcare Professional; IV, Intravenous; NHS, National Health Service; PICC, Peripherally Inserted Central Catheter; QoL, Quality of Life.
Ethics Approval and Informed Consent
This article does not stem from an interventional or retrospective study and does not include any sensitive or specific human data from confidential or public databases. Therefore, no response, approval, or informed consent was necessary. The analysis relied on previously conducted and published studies, as well as insights collected through an expert panel, and did not involve any patient-level data. Moreover, the study was performed according to the ISPOR CHEERS (Consolidated Health Economic Evaluation Reporting Standards) practices.50
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, writing, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted and agreed to account for all aspects of the work.
Funding
This study received financial support by Otsuka Pharmaceutical Italy s.r.l.
Disclosure
At the time of the start of the project and the drafting of the manuscript, ADC, LL, CV and FF were employees of IQVIA Solutions Italy s.r.l., a company that receives professional service commissions from a large number of sponsors for a variety of activities in the biopharmaceutical sector. The authors report no other conflicts of interest in this work.
References
1. Damiani D, Tiribelli M. Molecular landscape in adult acute myeloid leukemia: where we are where we going? J Lab Precis Med. 2019;4:17. doi:10.21037/jlpm.2018.09.08
2. Shallis RM, Wang R, Davidoff A, Ma X, Zeidan AM. Epidemiology of acute myeloid leukemia: recent progress and enduring challenges. Blood Rev. 2019;36:70–87. doi:10.1016/j.blre.2019.04.005
3. De Kouchkovsky I, Abdul-Hay M. Acute myeloid leukemia: a comprehensive review and 2016 update. Blood Cancer J. 2016;6(7):e441–e441. doi:10.1038/bcj.2016.50
4. AIRTUM. I numeri del cancro in Italia, 2023. (The numbers of cancer in Italy, 2023) Available from: https://www.registri-tumori.it/cms/pubblicazioni/i-numeri-del-cancro-italia-2023.
5. Calabria S, Ronconi G, Dondi L, et al. Acute myeloid leukemia: incidence, transplantation and survival through Italian administrative healthcare data. Tumori. 2023;109(5):496–503. doi:10.1177/03008916231153698
6. Cannas G, Fattoum J, Boukhit M, Thomas X. Economic analysis of blood product transfusions according to the treatment of acute myeloid leukemia in the elderly. Transfus Clin Biol. 2015;22(5–6):341–347. doi:10.1016/j.tracli.2015.06.249
7. Società Italiana di Ematologia. Linee guida leucemia mieloide acuta non promielocitica nel paziente ≥ 60 anni, 2023. (Guidelines for non-promyelocytic acute myeloid leukemia in patient ≥60 years old). Available from: https://www.iss.it/-/snlg-leucemia-acuta-non-promielocitica.
8. Kantarjian HM, Thomas XG, Dmoszynska A, et al. Multicenter, randomized, open-label, phase iii trial of decitabine versus patient choice, with physician advice, of either supportive care or low-dose cytarabine for the treatment of older patients with newly diagnosed acute myeloid leukemia. JCO. 2012;30(21):2670–2677. doi:10.1200/JCO.2011.38.9429
9. Briot T, Roger E, Lautram N, Verger A, Clavreul A, Lagarce F. Development and in vitro evaluations of new decitabine nanocarriers for the treatment of acute myeloid leukemia. IJN. 2017;Volume 12:8427–8442. doi:10.2147/IJN.S147659
10. Ministero della Salute. Regime di rimborsabilita’ e prezzo, a seguito di nuove indicazioni terapeutiche, del medicinale per uso umano «Dacogen». GU Serie Generale n.199 del 28-08-2018. (Reimbursement scheme and price, as a result of new therapeutic indications, of the medicinal product for human use «Dacogen». Official Journal, General Series No.199 of 28-08-2018).
11. Ali AM, Weisel D, Gao F, et al. Patterns of infectious complications in acute myeloid leukemia and myelodysplastic syndromes patients treated with 10‐day decitabine regimen. Cancer Med. 2017;6(12):2814–2821. doi:10.1002/cam4.1231
12. Urlu SM, Cengiz Seval G, Erdogan Yücel E, et al. Acute myeloid leukemia in elderly, unfit patients: analysis of Turkish AML prospective registry database, on behalf of acute leukemia working group of Turkish society of hematology. Blood. 2023;142(Supplement 1):5931. doi:10.1182/blood-2023-189714
13. Bellone M, Pradelli L, Tavarozzi R, et al. Economic consequences of administering obinutuzumab as a short duration infusion in Italian patients with advanced follicular lymphoma: a cost analysis. FE. 2022;23(1). doi:10.7175/fe.v23i1.1532
14. Pradelli L, Massaia M, Todisco E, et al. Improved efficiency of daratumumab treatment of multiple myeloma adopting the subcutaneous route: a micro‐costing analysis in three Italian hematology centers. Cancer Med. 2023;12(23):21480–21489. doi:10.1002/cam4.6699
15. Ponzetti C, Canciani M, Farina M, Era S, Walzer S. Potential resource and cost saving analysis of subcutaneous versus intravenous administration for rituximab in non-Hodgkin’s lymphoma and for trastuzumab in breast cancer in 17 Italian hospitals based on a systematic survey. CEOR. 2016;227. doi:10.2147/CEOR.S97319
16. Balducci L. Transfusion Independence in patients with myelodysplastic syndromes: impact on outcomes and quality of life. Cancer. 2006;106(10):2087–2094. doi:10.1002/cncr.21860
17. Zeidan AM, Jayade S, Schmier J, et al. Injectable hypomethylating agents for management of myelodysplastic syndromes: patients’ perspectives on treatment. Clin Lymphoma Myeloma Leukemia. 2022;22(3):e185–e198. doi:10.1016/j.clml.2021.09.009
18. Zeidan AM, Perepezko K, Salimi T, Washington T, Epstein RS. Patients’ perspectives on oral decitabine/cedazuridine for the treatment of myelodysplastic syndromes/neoplasms. Therapeutic Adv Hematol. 2024;15:20406207241257313. doi:10.1177/20406207241257313
19. Marchesi F, Salmanton-García J, Emarah Z, et al. COVID-19 in adult acute myeloid leukemia patients: a long-term follow-up study from the European hematology association survey (EPICOVIDEHA). haematol. 2022;108(1):22–33. doi:10.3324/haematol.2022.280847
20. Ivziku D, Gualandi R, Pesce F, De Benedictis A, Tartaglini D. Adult oncology patients’ experiences of living with a central venous catheter: a systematic review and meta-synthesis. Support Care Cancer. 2022;30(5):3773–3791. doi:10.1007/s00520-022-06819-8
21. McCloskey C, Ortega MT, Nair S, Garcia MJ, Manevy F. A systematic review of time and resource use costs of subcutaneous versus intravenous administration of oncology biologics in a hospital setting. PharmacoEconomics Open. 2023;7(1):3–36. doi:10.1007/s41669-022-00361-3
22. O’Brien GL, O’Mahony C, Cooke K, et al. Cost minimization analysis of intravenous or subcutaneous trastuzumab treatment in patients with HER2-positive breast cancer in Ireland. Clinical Breast Cancer. 2019;19(3):e440–e451. doi:10.1016/j.clbc.2019.01.011
23. Franken MG, Kanters TA, Coenen JL, et al. Potential cost savings owing to the route of administration of oncology drugs: a microcosting study of intravenous and subcutaneous administration of trastuzumab and rituximab in the Netherlands. Anti-Cancer Drugs. 2018;29(8):791–801. doi:10.1097/CAD.0000000000000648
24. Bordonaro S, Tralongo P, Romano F, et al. Effect of a structured, active, home-based cancer-treatment program for the management of patients on oral chemotherapy. PPA. 2014:917. doi:10.2147/PPA.S62666
25. O’Neill VJ, Twelves CJ. Oral cancer treatment: developments in chemotherapy and beyond. Br J Cancer. 2002;87(9):933–937. doi:10.1038/sj.bjc.6600591
26. European Medicines Agency. List of European public assessment reports. Available from: https://www.ema.europa.eu/en/medicines.
27. European Medicines Agency. Summary of product characteristics: decitabine/cedazuridine. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/inaqovi.
28. Geissler K, Koristek Z, Bernal Del Castillo T, et al. Oral decitabine/cedazuridine vs intravenous decitabine for acute myeloid leukemia: final results of a randomized, crossover, registration-enabling, pharmacokinetics study. Blood. 2023;142(Supplement 1):1538. doi:10.1182/blood-2023-173092
29. Geissler K, Koristek Z, Del Castillo TB, et al. Oral decitabine/cedazuridine versus intravenous decitabine for acute myeloid leukaemia: a randomised, crossover, registration, pharmacokinetics study. Br J Haematol. 2024;205(5):1734–1745. doi:10.1111/bjh.19741
30. Garcia-Manero G, McCloskey J, Griffiths EA, et al. Oral decitabine–cedazuridine versus intravenous decitabine for myelodysplastic syndromes and chronic myelomonocytic leukaemia (ASCERTAIN): a registrational, randomised, crossover, pharmacokinetics, phase 3 study. Lancet Haematol. 2024;11(1):e15–e26. doi:10.1016/S2352-3026(23)00338-1
31. Sousa B, Furlanetto J, Hutka M, et al. Central venous access in oncology: ESMO clinical practice guidelines. Ann Oncol. 2015;26:v152–v168. doi:10.1093/annonc/mdv296
32. Klastersky J, De Naurois J, Rolston K, et al. Management of febrile neutropaenia: ESMO clinical practice guidelines. Ann Oncol. 2016;27:v111–v118. doi:10.1093/annonc/mdw325
33. Aldea Mansilla C, Martínez-Alarcón J, Gracia Ahufinger I, Guembe Ramírez M. Microbiological diagnosis of catheter-related infections. Enfermedades Infecciosas y Microbiología Clínica. 2019;37(10):668–672. doi:10.1016/j.eimc.2018.07.009
34. Tarricone R. Cost-of-illness analysis. Health Policy. 2006;77(1):51–63. doi:10.1016/j.healthpol.2005.07.016
35. SIFO. La dispensazione del farmaco oncologico orale in farmacia ospedaliera, 2020. (Oral oncology drug dispensing in hospital pharmacy, 2020). Available from: https://www.sifoweb.it/images/pdf/attivita/attivita-scientifica/aree_scientifiche/area_oncologica/volume_terapie_orali.pdf.
36. Pittirutti M, Scoppettuolo G. Raccomandazioni gavecelt 2021 per la indicazione, l’impianto e la gestione dei dispositivi per accesso venoso, 2021. (Recommendations gavecelt 2021 for the indication, implantation and management of venous access devices, 2021).
37. Azienda Ospedaliera Universitaria Sassari. Procedura per la gestione dei chemioterapici antiblastici, 2014. (Procedure for the management of antiblastic chemotherapy drugs, 2014).
38. Commissione regionale dispositivi medici, direzione generale cura della persona, salute e welfare, settore assistenza ospedaliera - area governo del farmaco e dispositivi medici, protocollo di gestione degli accessi vascolari – giugno 2023. (regional medical devices commission, general directorate for personal care, health and welfare, hospital care sector - drug governance and medical devices area, vascular access management protocol - June 2023).
39. Azienda ospedaliera “Santa Maria” Terni. Protocollo per l’allestimento dei farmaci citotossici nella UFA, 2016. (Protocol for setting up cytotoxic drugs, 2016).
40. Osservatorio Nazionale sull’impiego dei Medicinali. L’uso degli antibiotici in Italia. Rapporto Nazionale 2021. Roma: agenzia Italiana del Farmaco, 2023. (The use of antibiotics in Italy. National Report 2021. Rome: agenzia Italiana del Farmaco, 2023).
41. Maki DG, Kluger DM, Crnich CJ. The risk of bloodstream infection in adults with different intravascular devices: a systematic review of 200 published prospective studies. Mayo Clin Proc. 2006;81(9):1159–1171. doi:10.4065/81.9.1159
42. European Medicines Agency. Summary of product characteristics: decitabine. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/dacogen. Accessed
43. Cashen AF, Schiller GJ, O’Donnell MR, DiPersio JF. Multicenter, Phase II study of decitabine for the first-line treatment of older patients with acute myeloid leukemia. JCO. 2010;28(4):556–561. doi:10.1200/JCO.2009.23.9178
44. IQVIA Italy medical devices hospital consumption audit, annual data MAT 09/2023.
45. IQVIA sales data, annual data MAT 09/2023.
46. Mandolfo S, Maggio M, Forneris G, Galli F. Analisi dei costi delle infezioni correlate al catetere venoso centrale per emodialisi attraverso il sistema dei DRG, “per conto del Gruppo di Progetto degli Accessi Vascolari della Società Italiana di Nefrologia”. G Ital Nefrol. ISSN 1724-5990. 2019;36(1).
47. Ministero della Salute. Tariffe delle prestazioni di assistenza ospedaliera per acuti, per tipo di ricovero (euro). GU Serie Generale n.23 del 28-01-2013 - Supplemento ordinario n. 8, allegato 1. (Tariffs of hospital acute care, by hospitalization type (euro). Official Journal, General Series No.23 of 28-01-2013 - Ordinary Supplement No. 8, Annex 1).
48. Ministero della Salute. Tariffe delle prestazioni di assistenza specialistica ambulatoriale. GU serie generale n.181 del 04-08-2023. (Tariffs for outpatient specialist care services. official journal, general series No.181 of 04-08-2023).
49. Ministero della Salute. Riclassificazione del medicinale per uso umano «Augmentin» (amoxicillina/acido clavulanico). GU serie generale n.136 del 14-06-2014. (Reclassification of the medicinal product for human use «Augmentin» (amoxicillin/clavulanic acid). official journal, general series no.136 of 14-06-2014).
50. Husereau D, Drummond M, Augustovski F, et al. Consolidated health economic evaluation reporting standards 2022 (CHEERS 2022) statement: updated reporting guidance for health economic evaluations. BMC Med. 2022;20(1):23. doi:10.1186/s12916-021-02204-0
51. Ministero dell’Economia e delle Finanze. (MEF). Retribuzioni medie pro-capite 2021. (Average wages per capita 2021). Available from: https://contoannuale.rgs.mef.gov.it/web/sicosito/spese-e-retribuzioni/retribuzione-media.
52. ISTAT. Rivalutazioni e documentazione su prezzi, costi e retribuzioni contrattuali. Consultato a maggio, 2024. (ISTAT. Revaluations and documentation on prices, costs, and contractual wages. Accessed May, 2024). Available from: https://rivaluta.istat.it/.
53. ISTAT. Popolazione residente in Italia al 1 Gennaio 2019-2023. (Resident population in Italy as of January 1, 2019-2023). Available from: www.istat.it.
54. IQVIA Oncoview database.
55. Otsuka estimation. Oral decitabine penetration by year, 2024.
56. He J, Xiu L, De Porre P, Dass R, Thomas X. Decitabine reduces transfusion dependence in older patients with acute myeloid leukemia: results from a post hoc analysis of a randomized phase III study. Leukemia Lymphoma. 2015;56(4):1033–1042. doi:10.3109/10428194.2014.951845
57. Catalano L, Piccinini V, Pati I, et al. Italian Blood System 2020: activity data, haemovigilance and epidemiological surveillance, 2021, iii, 103 p. Rapporti ISTISAN 21/14.
58. Ministero della Salute. Disposizioni relative ai requisiti di qualità e sicurezza del sangue e degli emocomponenti. GU Serie Generale n.300 del 28-12-2015. (Provisions on quality and safety requirements for blood and blood components. Official Journal, General Series No.300 of 28-12-2015).
59. Accordo Stato Regioni del 7 giugno 2023 (rep. Atti n°134/CSR) “Accordo interregionale per la compensazione della mobilità sanitaria aggiornato all’anno 2022 - Regole tecniche”. (Agreement State-Regions of 7 June 2023 - rep. Acts no. 134/CSR - “Interregional agreement for health mobility compensation updated to the year 2022”).
60. Mastrorilli G, Fiorentino F, Tucci C, Lombardi G, Aghemo A, Colombo GL. Cost analysis of platelet transfusion in Italy for patients with chronic liver disease and associated thrombocytopenia undergoing elective procedures. CEOR. 2022;Volume 14:205–220. doi:10.2147/CEOR.S354470
61. Zhu LX, Chen RR, Wang LL, et al. A real-world study of infectious complications of venetoclax combined with decitabine or azacitidine in adult acute myeloid leukemia. Support Care Cancer. 2022;30(8):7031–7038. doi:10.1007/s00520-022-07126-y
62. Bocchia M, Candoni A, Borlenghi E, et al. Real‐world experience with decitabine as a first‐line treatment in 306 elderly acute myeloid leukaemia patients unfit for intensive chemotherapy. Hematol Oncol. 2019;37(4):447–455. doi:10.1002/hon.2663
63. Badia-Cebada L, Peñafiel J, Saliba P, et al. Trends in the epidemiology of catheter-related bloodstream infections; towards a paradigm shift, Spain, 2007 to 2019. Eurosurveillance. 2022;27(19). doi:10.2807/1560-7917.ES.2022.27.19.2100610
64. Haque M, Sartelli M, McKimm J, Abu Bakar MB. Health care-associated infections – an overview. IDR. 2018;Volume 11:2321–2333. doi:10.2147/IDR.S177247
65. Eisai Inc. Trial of decitabine in patients with acute myeloid leukemia (DACO-016). Available from: https://clinicaltrials.gov/study/NCT00260832.
66. Il Sole 24 ore. Cittadinanzattiva: la carenza di personale attraversa tutta l’Italia, si rischia il deserto sanitario (Active Citizenship: staffing shortages run across Italy, health care desert at risk, 2023). Sanità24. 2023. Available from: http://s24ore.it/loD3SU.
67. Twelves C, Gollins S, Grieve R, Samuel L. A randomised cross-over trial comparing patient preference for oral capecitabine and 5-fluorouracil/leucovorin regimens in patients with advanced colorectal cancer. Ann Oncol. 2006;17(2):239–245. doi:10.1093/annonc/mdj023
68. Liu G, Franssen E, Fitch MI, Warner E. Patient preferences for oral versus intravenous palliative chemotherapy. JCO. 1997;15(1):110–115. doi:10.1200/JCO.1997.15.1.110
69. Eurostat. Purchasing power parities (PPP). Available from: https://ec.europa.eu/eurostat/en/.
70. Armeni P, Borsoi L, Fornaro G, Jommi C, Grossi F, Costa F. Cost-effectiveness and net monetary benefit of durvalumab consolidation therapy versus no consolidation therapy after chemoradiotherapy in stage III non–small cell lung cancer in the Italian national health service. Clin Ther. 2020;42(5):830–847. doi:10.1016/j.clinthera.2020.03.012
71. Filetti S, Ladenson PW, Biffoni M, D’Ambrosio MG, Giacomelli L, Lopatriello S. The true cost of thyroid surgery determined by a micro-costing approach. Endocrine. 2017;55(2):519–529. doi:10.1007/s12020-016-0980-z
72. Berto P, Lopatriello S, Aiello A, et al. Cost of laparoscopy and laparotomy in the surgical treatment of colorectal cancer. Surg Endosc. 2012;26(5):1444–1453. doi:10.1007/s00464-011-2053-y
73. Palmieri V, Baldi C, Di Blasi PE, et al. Impact of DRG billing system on health budget consumption in percutaneous treatment of mitral valve regurgitation in heart failure. J Med Economics. 2015;18(2):89–95. doi:10.3111/13696998.2014.980502
74. Gogas Yavuz D, Akhtar O, Low K, et al. The economic impact of obesity in Turkey: a micro-costing analysis. CEOR. 2024;Volume 16:123–132. doi:10.2147/CEOR.S446560
75. Rojas-Suarez J, Gutiérrez Clavijo J, Zakzuk J, et al. Cost analysis of thromboprophylaxis in patients at high thromboembolic risk with enoxaparin, dalteparin and nadroparin in Colombia: a systematic literature review-based study. CEOR. 2024;Volume 16:813–825. doi:10.2147/CEOR.S472192
76. Preliminary Otsuka data on file. Data on blood transfusion requirements, 2024.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cost Analysis of High-Flow Oxygen Therapy Compared with Conventional Oxygen Therapy in Severe COVID-19 in Colombia: Data from a Randomized Clinical Trial
Prada SI, Garcia-Garcia MP, Ospina-Tascón GA, Rosselli D
ClinicoEconomics and Outcomes Research 2023, 15:733-738
Published Date: 6 October 2023