")
Back to Journals » Clinical Ophthalmology » Volume 19
Effect of Capsular Tension Ring on Refractive and Morphological Outcomes in Pseudoexfoliative Eyes
Authors Cunha B , Gil P , Rodrigues Alves N, Hipólito-Fernandes D , Maduro V, Feijão J, Alves N
Received 24 December 2024
Accepted for publication 28 February 2025
Published 5 March 2025 Volume 2025:19 Pages 763—771
DOI https://doi.org/10.2147/OPTH.S514116
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Bruna Cunha, Pedro Gil, Nuno Rodrigues Alves, Diogo Hipólito-Fernandes, Vitor Maduro, João Feijão, Nuno Alves
Ophthalmology Department, ULS São José, Lisboa, Portugal
Correspondence: Bruna Cunha, Email [email protected]
Purpose: To evaluate the effect on anterior chamber depth (ACD) and postoperative refractive prediction error (PE) of capsular tension ring (CTR) implantation during phacoemulsification in pseudoexfoliative (PEX) eyes.
Methods: Prospective case-control study of eyes submitted to uneventful cataract surgery, divided into three study groups: Group 1 – controls; Group 2 – PEX eyes without CTR implantation; Group 3 – PEX eyes with CTR implantation. Biometric data including ACD were measured preoperatively and 1-month postoperatively, using swept-source anterior segment optical coherence tomography (ANTERION®, Heidelberg Engineering), and endothelial cell density (ECD) with specular microscopy. Postoperative refractive PE was calculated using an optimized A-constant and the Kane formula.
Results: A total of 25 eyes were included in each group. Anterior chamber increased significantly in all groups (p< 0.001), with the change being significantly greater in Group 2 compared to Group 1 (p=0.014). No significant differences in ACD changes were observed between Group 3 and the other groups (p> 0.05). In Group 2, a significant hyperopic shift (p=0.035) and 12% of eyes with a prediction error above 1D was observed, which were not seen in Groups 1 or 3. The percentage of eyes with a PE within ± 0.25D was significantly lower in Group 2 (p=0.013). IOP and ECD decreased similarly across all groups (p> 0.05).
Conclusion: Routine CTR implantation during uneventful phacoemulsification in PEX eyes appears to prevent the pseudoexfoliative hyperopic shift previously reported, likely due to more even zonular tension distribution. If CTR is not used, a slightly myopic target should be considered.
Keywords: pseudoexfoliation syndrome, phacoemulsification, anterior chamber, capsular tension ring
Introduction
Cataract surgery is the most commonly performed refractive procedure worldwide.1 Achieving the desired refractive outcome has become a primary concern for surgeons, as patients’ expectations regarding refractive precision have risen over the years. One of the main challenges in cataract surgery is accurately estimating the effective lens position (ELP), defined as the distance between the anterior surface of the intraocular lens (IOL) and the corneal endothelium. A shift of just 1 mm in the IOL position can result in a refractive change of approximately 1.25 diopters (D).2,3 According to Olsen et al, despite advancements in technology, errors in predicting postoperative anterior chamber depth (ACD) might account for 42% of the postoperative refractive error.4
Pseudoexfoliation (PEX) syndrome is a systemic, age-related condition characterized by the deposition of abnormal fibrillary extracellular material within the anterior segment of the eye, as well as in other organs. PEX is associated with premature cataract formation,5,6 poor pharmacologic mydriasis, zonular instability and fragility, and an increased risk of complications during and after surgery, such as posterior capsule rupture, anterior capsule tears, dropped nucleus, vitreous prolapse, in-the-bag IOL dislocation, anterior capsule phimosis, IOL subluxation, and cystoid macular edema.7–10
In eyes with PEX, the combination of zonular weakness and an unstable capsular bag may lead to significant changes in anterior chamber morphology postoperatively, potentially causing unexpected refractive outcomes. However, the limited studies available on this topic report inconsistent findings.11–15
Capsular tension rings (CTR) were introduced by Hara et al16 in the early 1990s to stabilize the lens capsule by maintaining the circular contour of the capsular bag equator during and after cataract surgery. Various CTR designs have since been developed, with a primary purpose to stretch and stabilize the capsular bag, balancing the tension on the zonular fibers. Studies have demonstrated the effectiveness of CTRs in managing eyes with zonular instability, significantly reducing the risks of vitreous prolapse, IOL decentration, and IOL dislocation.17–21 However, the potential refractive consequences of CTR implantation, particularly in PEX eyes, remain uncertain due to the scarcity of available literature.
This study aims to evaluate the impact of prophylactic CTR use in PEX eyes without apparent zonulopathy following uneventful phacoemulsification, focusing on changes in anterior chamber morphology and refractive outcomes.
Methods
Patients
This was a single-center prospective case-control study, including consecutive patients who underwent cataract surgery performed by a single experienced cataract surgeon. The surgeries were conducted at a tertiary hospital from January 2023 to August 2024. The study adhered to the principles of the Declaration of Helsinki and institutional (ULS São José) review board approval was obtained. Written informed consent was obtained from all patients.
Inclusion criteria included patients with visually significant cataracts who underwent surgery using topical anesthesia, horizontal chop technique, and the same phacoemulsification device (CENTURION® Vision System, Alcon Laboratories, Inc.) through a 2.4 mm clear corneal incision. The same monofocal IOL model (AU0T00 AcrySof IQ, Alcon Laboratories, Inc.) was implanted in the bag. Intracameral cefuroxime (1 mg/0.1 mL) was administered in all cases. Postoperative medication included topical ofloxacin 3 mg/mL 4id, dexamethasone phosphate 1 mg/mL 4id, and flurbiprofen 0.3 mg/mL 4id, all of which were gradually tapered.
Exclusion criteria encompassed the presence of corneal or other ocular conditions that could result in a visual acuity worse than 20/40, glaucoma, corneal astigmatism >2D, systemic medications influencing anterior chamber morphology (eg topiramate), fixation difficulties (eg nystagmus or strabismus), topical antiglaucomatous medication, previous ocular trauma or surgery, incomplete biometric data, evidence of phacodonesis or lens subluxation, any intra- or postoperative complications, and the use of iris stretching devices, iris hooks, or Malyugin rings. Only one eye per patient was included. In cases of bilateral phacoemulsification, the eye with the worst visual acuity was selected.
Patients were divided into three groups by consecutive inclusion: group 1 (control group): non-PEX eyes; group 2: PEX eyes (diagnosed by the presence of PEX material visible during anterior segment evaluation under pharmacologic mydriasis) without the implantation of a CTR; group 3: PEX eyes with implantation of a CTR. CTR implantation was performed using MORCHER® Eyejet® (Morcher GmbH, Stuttgart, Germany) device, selected based on axial length: Type 14 for an axial length < 24mm, Type 14C for an axial length between 24–28mm and Type 14A for an axial length > 28mm. The CTR was inserted after phacoemulsification using a CTR injector, before IOL implantation.
Preoperative Data
All patients underwent a comprehensive ophthalmologic examination, which included distance and near best-corrected visual acuity, manifest (non-cycloplegic) refraction, slit-lamp examination, intraocular pressure (IOP) measurement with a Goldmann Applanation Tonometer, and fundus examination following pharmacological mydriasis. Demographic data were recorded.
Swept-Source Anterior Segment Optical Coherence Tomography (SS-AS-OCT) using the Anterion® device (Heidelberg Engineering Inc.) was performed in all patients to collect ocular biometry data. The Anterion® employs a 1300 nm wavelength light source, offering a scan depth of 14.5 mm and a scan width of 16.5 mm. Imaging was conducted under mesopic light conditions with patients seated, without pupil dilation. Patients were instructed to fixate on the internal fixation target while ensuring that their eyelids remained open without assistance from the technician. All images were captured by trained technicians following a standardized imaging protocol. Using the CATARACT mode, the device measured axial length (AL), anterior chamber depth (ACD), central corneal thickness (CCT), flat keratometry (K1), steep keratometry (K2), mean keratometry (Km), lens thickness (LT), and white-to-white distance (WTW). The keratometric index used was 1.3375. Endothelial cell density (ECD) was assessed using specular microscopy (SP-1P, Topcon Corp). Intraocular lens (IOL) power was calculated using the Kane Formula (www.iolformula.com) with the A-constant recommended for the IOL model (118.93), as specified by IOLcon (www.iolcon.org).
Postoperative Data and Outcome Measures
Non-cycloplegic manifest refraction was measured at a distance of 6 meters by the same ophthalmologist, one month after surgery. IOP was measured using Goldmann applanation tonometry. The refractive prediction error was calculated as the difference between the spherical equivalent of the postoperative manifest refraction and the predicted value from the IOL calculation formula. A negative refractive prediction error indicated a myopic error, while a positive prediction error indicated a hyperopic error. Mean absolute errors (MAE) were calculated, along with the percentage of eyes with a prediction error within ±0.25, ±0.50, and ±1.00 diopters.
Anterion® imaging and specular microscopy were repeated one month postoperatively, capturing the same parameters as in the preoperative assessment. Numerical and percentile changes in ACD, IOP and ECD were calculated.
Statistical Analysis
Demographics, anterior chamber angle, IOP, biometric data and ECD were described using frequencies (percentages) and mean ± standard deviation (SD) or median ± interquartile range (IQR), depending on data normality. Normality was assessed using the Kolmogorov–Smirnov test. Independent samples t-test or Mann–Whitney-U was used to compare differences between groups. One-way ANOVA or Kruskal–Wallis test was used to assess changes between preoperative and postoperative measurements for each group, as appropriate. The parametric one-sample t-test or nonparametric Wilcoxon signed-rank test (1 sample) were used, as appropriate, to evaluate whether the mean refractive prediction error in each group was different from zero. Chi-square test was used to compare the percentages of prediction error between study groups. Pearson correlation test was used to evaluate the relationship between the refractive results and anatomical data. A p-value of less than 0.05 was considered statistically significant. Statistical analysis was performed using SPSS for Macintosh Software (version 24.0, SPSS, Inc).
Based on an expected postoperative MAE of 0.320 ± 0.273 D in the control group and 0.569 ± 0.431 D in the PEX eyes,12 a sample size calculation was performed using a significance level of 5% and a power of 80%. The minimum required sample size was 17 patients per group, totaling 51 patients across the three groups, ensuring adequate power to detect differences in refractive outcomes.
Results
A total of 75 eyes from 75 patients met the inclusion criteria, with a mean age of 78.15 ± 6.73 years. There were no statistically significant differences in demographic or baseline characteristics among the three groups (Table 1).
 |
Table 1 Demographics and Baseline Measurements (Biometric Data, IOP, ECD and IOL Power) in Both Groups. |
Postoperative ACD differed significantly between groups (p<0.001), being greater in Group 2 compared to Group 1 (p<0.001). No significant differences were observed between the two PEX groups (Group 2 and Group 3) (p=0.067). ACD increased significantly after surgery in all groups (p<0.001). The magnitude of this increase varied between groups (p=0.016), with Group 2 showing a greater increase compared to Group 1 (p=0.014). Postoperative intraocular pressure (IOP) and endothelial cell density (ECD) were significantly reduced in all groups (p<0.05 for all comparisons). The numerical and percentage changes in IOP and ECD were not significantly different among the groups. A summary of postoperative measurements and their changes is presented in Table 2.
 |
Table 2 Postoperative Measurements for ACD, IOP and ECD and their change cfter Phacoemulsification Surgery. |
In terms of refractive outcomes, the mean PE did not differ significantly between the groups (p=0.233). While the MAE was lowest in Group 1, followed by Group 3 and then Group 2, these differences were not statistically significant (p=0.186). The mean PE was not significantly different from zero in Group 1 and Group 3 (p=0.893 and p=0.532, respectively). However, Group 2 showed a statistically significant difference from zero (p=0.032), with a tendency towards hyperopic deviation (Figure 1).
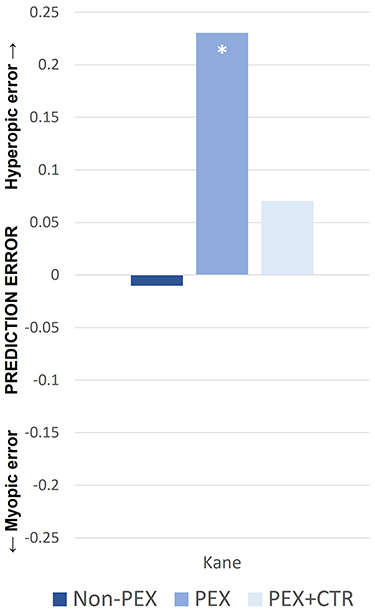 |
Figure 1 Mean Prediction Error (in diopters) in each group. *p<0.05 –one sample t-test. |
The percentage of eyes achieving a PE within ±0.25 D was significantly lower in Group 2 (p=0.013). In this group, 13.3% of eyes exhibited a PE greater than ±1.00 D, a finding not observed in Group 1 or Group 3 (Figure 2). A summary of refractive results is provided in Table 3.
 |
Table 3 Refractive Outcomes After Uneventful Cataract Surgery |
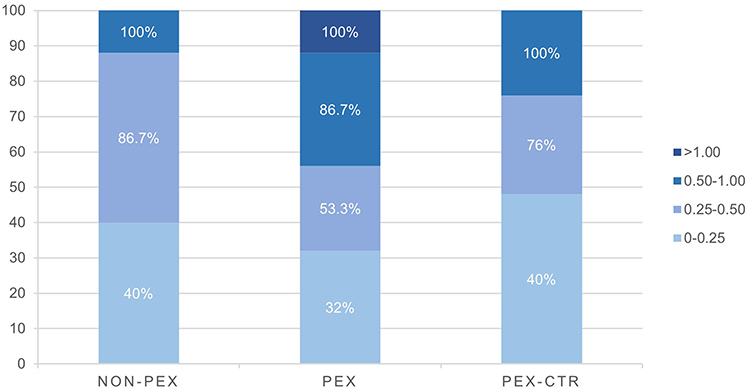 |
Figure 2 Stacked histogram comparing the percentages of eyes within ±0.25, ±0.50, ±1.00 and >±1.00 diopters of prediction error. |
A weakly positive correlation was identified between PE and ACD numerical change (r=0.408, p=0.002), percentile of change (r=0.331, p=0.014), and postoperative ACD depth (r=0.372, p=0.005).
Discussion
This study aimed to evaluate the effect of prophylactic CTR implantation on anterior chamber morphology and refractive outcomes in PEX eyes after uneventful phacoemulsification. Our findings indicate that postoperative ACD was significantly lower in PEX eyes with CTR implantation, resembling the ACD change observed in non-PEX controls. However, the magnitude of ACD change did not differ significantly between PEX eyes with or without CTR. Refractive outcomes were less precise in PEX eyes without CTR, showing a slight hyperopic shift and reduced percentage of eyes within ±0.25 D.
Regarding anterior chamber morphology, postoperative ACD and the magnitude of its numerical increase were higher in PEX eyes without CTR compared to controls, consistent with previous literature.14,15 For instance, Kassos et al14 reported a greater percentile increase in ACD in PEX eyes (39.51 ± 16.11%) compared to non-PEX eyes (31.50 ± 13.25%, p=0.017). Güngor et al15 using Scheimpflug imaging, showed greater ACD changes in PEX eyes (0.46 ± 0.3 mm vs 0.12 ± 0.1 mm, p=0.04). Zonular fragility in PEX eyes may contribute to a more posterior position of the IOL, which may explain the increased ACD after surgery. In contrast, the ACD in PEX eyes with CTR was comparable to controls, suggesting that CTR implantation provides a more stable and physiological IOL position by evenly distributing zonular tension, resembling the mechanics of normal eyes. To our knowledge, no prior studies have directly compared these two populations.
When analyzing the effects of CTR implantation in PEX eyes, postoperative ACD, its numerical magnitude, and percentage change were similar between PEX eyes with and without CTR, consistent with studies by Besek et al22 and Malekahmadi et al.23 The actual impact of CTR on ACD changes may vary across populations but does not appear to significantly influence depth changes when comparing similar groups. In normal eyes without pseudoexfoliation or zonulopathy, studies by Weber et al24 and Park et al25 found no differences in postoperative ACD between eyes with and without CTR implantation. Similarly, in other conditions associated with zonular laxity, such as high myopia or post-pars plana vitrectomy, CTR implantation did not significantly affect postoperative ACD.26–29
Estimating the ELP remains a critical challenge in IOL power calculation. Larger ACD changes complicate ELP prediction, potentially leading to poorer refractive outcomes, particularly in PEX patients. Despite no significant differences in arithmetic or absolute PE between groups, our study demonstrated less precise refractive outcomes in PEX eyes without CTR implantation. These included a hyperopic PE shift, a lower percentage of eyes within ±0.25 D, and over 10% of eyes with PE > ±1.00 D. These findings align with existing literature,11–15,30 which similarly reports hyperopic tendencies in PEX eyes.13,14,30
CTR was initially designed to stabilize the capsular bag by balancing zonular tension, improving IOL centration and reducing tilt. While some studies suggest that CTR improves refractive precision in high myopes,28,29 most reveal no significant differences in MAE between eyes with and without CTR, with no clear tendency toward hyperopic or myopic shifts.26–29,31 Nevertheless, CTR implantation is associated with better IOL centration, reduced tilt, larger anterior capsule openings, and more consistent posterior capsule adherence to the IOL surface.26,27
A recent meta-analysis indicated that CTR co-implantation is more likely to cause hyperopic shifts in non-myopic eyes; however, these conclusions were limited by the lack of studies.32 The scarcity of included PEX patients makes it insufficient to draw solid conclusions about this population. In our study, CTR use in PEX eyes resulted in more precise refractive outcomes, avoiding the significant hyperopic shift observed in PEX eyes without CTR, and achieving results comparable to non-PEX eyes. However, the other two published studies have reported conflicting results. Malekahmadi et al23 found no difference in postoperative refractive error between PEX eyes with and without CTR but did not provide details on absolute errors or the percentage of eyes with PE > ±1.00 D. Besek22 et al reported a hyperopic shift in PEX eyes with CTR but exhibited several methodological issues, including using a generalized target of −0.50 D instead of an individualized target for the IOL power, potentially introducing bias. Additionally, the reported “absolute error” likely reflect arithmetic errors based on negative signs, suggesting a misinterpretation. Notably, significant postoperative refractive cylinder reduction in their CTR group (−1.44 ± 1.24 D vs −0.50 ± 1.31 D) and lower endothelial cell counts suggest more traumatic surgeries, potentially leading to zonular damage and IOL tilt, which were not evaluated. The cylindrical change could be responsible for the hyperopic result, as the spherical refraction remained similar between the groups. Moreover, the study did not follow the recommended size optimization for CTR implantation, as the same CTR size was used for all eyes, potentially introducing further variability in outcomes.
We hypothesize that the prophylactic use of CTR in PEX eyes without evident zonulopathy facilitates even distribution of zonular tension, improving IOL centration and delivering refractive results comparable to non-PEX eyes. Further research is needed to confirm and expand upon these findings.
Our study has some limitations. Each group sample size was small, and the refractive outcomes were measured 1 month after surgery, not allowing us to take long-term conclusions. Moreover, we only included one IOL model and one CTR design, so we could not evaluate the influence of different IOL and CTR designs and materials and a cost-analysis was not performed, which may also be interesting. On the other hand, the study also has some strengths, including its prospective design, the use of up-to-date technology for pre and postoperative measurements, the inclusion of only one experienced surgeon performing all surgeries and the use of one of the most accurate modern IOL power calculation formulas, following the guidelines to present the refractive results.
Conclusions
Based on our findings, we conclude that PEX characteristics, particularly zonular fragility and capsular instability, may contribute to a more posterior IOL position, leading to poorer refractive outcomes and a significant hyperopic shift. CTR implantation appears to improve refractive precision by stabilizing the capsular bag and optimizing IOL position. In PEX patients where CTR implantation is not planned, it may be prudent to select a slightly myopic refractive target during IOL power selection.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author.
Ethics
The authors declare having followed the protocols of their work centre on the data publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. All the authors read and approved the final manuscript. All the authors had full access to all the data and took full responsibility for the integrity of the data and the accuracy of the data analysis; all were responsible for conceiving this research.
Disclosure
The authors report no financial or non-financial conflicts of interest in this work.
References
1. Ang M, Gatinel D, Reinstein DZ, Mertens E, Del Barrio JL A, Alió JL. Refractive surgery beyond 2020. Eye. 2021;35(2):362–382. doi:10.1038/s41433-020-1096-5
2. Sanders DR, Higginbotham RW, Opatowsky IE, Confino J. Hyperopic shift in refraction associated with implantation of the single-piece Collamer intraocular lens. J Cataract Refract Surg. 2006;32(12):2110–2112. doi:10.1016/J.JCRS.2006.07.030
3. Erickson P. Effects of intraocular lens position errors on postoperative refractive error. J Cataract Refract Surg. 1990;16(3):305–311. doi:10.1016/S0886-3350(13)80699-2
4. Olsen T. Calculation of intraocular lens power: a review. Acta Ophthalmologica Scandinavica. 2007;85(5):472–485. doi:10.1111/J.1600-0420.2007.00879.X
5. Puska P, Tarkkanen A. Exfoliation syndrome as a risk factor for cataract development: five-year follow-up of lens opacities in exfoliation syndrome. J Cataract Refract Surg. 2001;27(12):1992–1998. doi:10.1016/S0886-3350(01)00972-5
6. Anastasopoulos E, Founti P, Topouzis F. Update on pseudoexfoliation syndrome pathogenesis and associations with intraocular pressure, glaucoma and systemic diseases. Current Opinion Ophthalmol. 2015;26(2):82–89. doi:10.1097/ICU.0000000000000132
7. Drolsum L, Haaskjold E, Sandvig K. Phacoemulsification in eyes with pseudoexfoliation. J Cataract Refract Surg. 1998;24(6):787–792. doi:10.1016/S0886-3350(98)80132-6
8. Küchle M, Viestenz A, Martus P, Händel A, Jünemann A, Naumann GOH. Anterior chamber depth and complications during cataract surgery in eyes with pseudoexfoliation syndrome. Am J Ophthalmol. 2000;129(3):281–285. doi:10.1016/S0002-9394(99)00365-7
9. Moreno J, Duch S, Lajara J. Pseudoexfoliation syndrome: clinical factors related to capsular rupture in cataract surgery. Acta ophthalmologica. 1993;71(2):181–184. doi:10.1111/J.1755-3768.1993.TB04987.X
10. Shingleton BJ, Crandall AS, Ahmed IIK. Pseudoexfoliation and the cataract surgeon: preoperative, intraoperative, and postoperative issues related to intraocular pressure, cataract, and intraocular lenses. J Cataract Refract Surg. 2009;35(6):1101–1120. doi:10.1016/J.JCRS.2009.03.011
11. Tekcan H, Alpogan O, Imamoglu S. Pseudoexfoliation glaucoma as a predictor of refractive surprise after uneventful cataract surgery. J Glaucoma. 2023;32(4):272–279. doi:10.1097/IJG.0000000000002187
12. Wlaź A, Kustra A, Rozegnał-Madej A, Żarnowski T. Intraocular lens power calculations in eyes with pseudoexfoliation syndrome. Sci Rep. 2021;11(1):1–8. doi:10.1038/s41598-021-98675-5
13. Tafti M, Beiki H, Mohammadi S, Latifi G, Ashrafi E, Tafti Z. Anterior chamber depth change following cataract surgery in pseudoexfoliation syndrome; A preliminary study. J Ophthalmic Vis Res. 2017;12(2):165–169. doi:10.4103/jovr.jovr_81_15
14. Kassos I, Tzamalis A, Dermenoudi M, et al. Ocular parameter changes after phacoemulsification in pseudoexfoliative eyes: case-control study. J Cataract Refract Surg. 2022;48(8):894–899. doi:10.1097/j.jcrs.0000000000000885
15. Gür Güngör S, Akman A, Asena L, Aksoy M, Sezenöz A S. Changes in anterior chamber depth after phacoemulsification in pseudoexfoliative eyes and their effect on accuracy of intraocular lens power calculation. Turk Oftalmoloiji Dergisi. 2016;46(6):255–258. doi:10.4274/tjo.56659
16. Hara T, Hara T, Yamada Y. “Equator ring” for maintenance of the completely circular contour of the capsular bag equator after cataract removal. Ophthalmic Surg. 1991;22(6):358–359.
17. Georgopoulos GTH, Papaconstantinou D, Georgalas I, Koutsandrea CN, Margetis I, Moschos MM. Management of large traumatic zonular dialysis with phacoemulsification and IOL implantation using the capsular tension ring. Acta Ophthalmologica Scandinavica. 2007;85(6):653–657. doi:10.1111/j.1600-0420.2007.00901.x
18. Wang BZ, Chan E, Vajpayee RB. A retrospective study of the indications and outcomes of capsular tension ring insertion during cataract surgery at a tertiary teaching hospital. Clin Ophthalmol. 2013;7:567–572. doi:10.2147/OPTH.S38543
19. Jakobsson G, Zetterberg M, Lundström M, Stenevi U, Grenmark R, Sundelin K. Late dislocation of in-the-bag and out-of-the bag intraocular lenses: ocular and surgical characteristics and time to lens repositioning. J Cataract Refract Surg. 2010;36(10):1637–1644. doi:10.1016/j.jcrs.2010.04.042
20. Bayraktar S, Altan T, Küçüksümer Y, Yilmaz OF. Capsular tension ring implantation after capsulorhexis in phacoemulsification of cataracts associated with pseudoexfoliation syndrome. Intraoperative complications and early postoperative findings. J Cataract Refract Surg. 2001;27(10):1620–1628. doi:10.1016/s0886-3350(01)00965-8
21. Mayer-Xanthaki CF, Hirnschall N, Pregartner G, et al. Capsular tension ring as protective measure against in-the-bag dislocations after cataract surgery. J Cataract Refract Surg. 2023;49(2):154–158. doi:10.1097/j.jcrs.0000000000001060
22. Kandemir Besek N, Gumus G, Karabulut GO, et al. Effect of capsular tension ring on refractive results in cases with pseudoexfoliation syndrome. Eur J Ophthalmol. 2022;32(1):263–267. doi:10.1177/1120672120965469
23. Mohammad M, Sadegh K, Farideh S, Farshad O, Rad AM, Mirdehghan MS. Effect of capsular tension ring implantation on predicted refractive error after cataract surgery in patients with pseudoexfoliation syndrome. Int J Ophthalmol. 2020;13(4):587–590. doi:10.18240/ijo.2020.04.09
24. Weber M, Hirnschall N, Rigal K, Findl O. Effect of a capsular tension ring on axial intraocular lens position. J Cataract Refract Surg. 2015;41(1):122–125. doi:10.1016/j.jcrs.2014.04.035
25. Park HJ, Lee H, Kim DW, Kim EK, Seo KY, Kim TI. Effect of co-implantation of a capsular tension ring on clinical outcomes after cataract surgery with monofocal intraocular lens implantation. Yonsei Med J. 2016;57(5):1236–1242. doi:10.3349/ymj.2016.57.5.1236
26. Yang S, Jiang H, Nie K, Feng L, Fan W. Effect of capsular tension ring implantation on capsular stability after phacoemulsification in patients with weak zonules: a randomized controlled trial. CTR implantation in cataract patients with weak zonules. BMC Ophthalmol. 2021;21(1):1–11. doi:10.1186/s12886-020-01772-8
27. Hu X, Qi J, Cheng K, et al. Effectiveness of prophylactic capsular tension ring implantation during cataract surgery in highly myopic eyes. J Cataract Refract Surg. 2022;2022:1030–1036; doi:10.1097/j.jcrs.0000000000001495
28. Liang J, Yan H, Xie X, Zhang J, Zhang Y, Qu L. Effect of capsular tension ring implantation on intraocular lens calculation formula selection for long axial myopia. BMC Ophthalmol. 2024;24(1). doi:10.1186/s12886-024-03602-7
29. Zhao HY, Zhang JS, Li M, Chen DJ, Wan XH. Effect of capsular tension ring on the refractive outcomes of patients with extreme high axial myopia after phacoemulsification. Eur J Med Res. 2024;29(1):1–7. doi:10.1186/s40001-024-01726-6
30. Gazit I, Gershevich A, Einan-Lifshitz A, Pras E, Barrett GD, Or L. Accuracy of intra ocular lens calculation formulae in patients with pseudoexfoliation syndrome. Intl Ophthalmol. 2024;44(1). doi:10.1007/s10792-024-03195-6
31. Schild AM, Rosentreter A, Hellmich M, Lappas A, Dinslage S, Dietlein TS. Effect of a capsular tension ring on refractive outcomes in eyes with high myopia. J Cataract Refract Surg. 2010;36(12):2087–2093. doi:10.1016/j.jcrs.2010.06.065
32. Xu S, Zhang Y, Li X, et al. Effect of implanted capsular tension ring on postoperative refractive shift: a systematic review and meta-analysis. Seminars Ophthalmol. 2024; 1–7. doi:10.1080/08820538.2024.2381770.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.