")
Back to Journals » Clinical Ophthalmology » Volume 19
Effect of Direct Cyclopexy for Traumatic Cyclodialysis Cleft: A Retrospective Clinical Study
Authors Wang X , Jiang Z, Ma X
Received 30 August 2024
Accepted for publication 14 January 2025
Published 25 February 2025 Volume 2025:19 Pages 673—681
DOI https://doi.org/10.2147/OPTH.S484518
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Xiaoqiang Wang,1 Zhixin Jiang,1 Xiubin Ma2
1Tianjin Eye Hospital, Nankai University Affiliated Eye Hospital, Clinical College of Ophthalmology, Tianjin Medical University, Tianjin Eye Institute, Tianjin Key Laboratory of Ophthalmology and Visual Science, Tianjin, People’s Republic of China; 2Qingdao Eye Hospital, Shandong First Medical University, Qingdao, People’s Republic of China
Correspondence: Xiubin Ma, Shandong Eye Institute, Shandong First Medical University, Qingdao, 266071, People’s Republic of China, Tel +86-532-85876380, Email [email protected] Zhixin Jiang, Tianjin Eye Hospital, Nankai University Affiliated Eye Hospital, Clinical College of Ophthalmology, Tianjin Medical University, Tianjin Eye Institute, Tianjin Key Laboratory of Ophthalmology and Visual Science, Tianjin, 300020, People’s Republic of China, Email [email protected]
Purpose: To evaluate the clinical effects of direct cyclopexy in the treatment of traumatic cyclodialysis cleft.
Methods: This is a retrospective case study. Patients with traumatic cyclodialysis cleft, who were treated with direct cyclopexy and had complete medical records at Tianjin Eye Hospital between February 2021 and August 2022 were selected. The detailed characteristics of the 23 patients were analyzed. Preoperative and postoperative visual acuity, intraocular pressure (IOP), and the extent of ciliary detachment were recorded. All patients were followed up for six months.
Results: 19 of the 23 patients who underwent single direct cyclopexy, the other 4 patients with severe posterior segment damage underwent direct cyclopexy combined with vitrectomy, suprachoroidal drainage, etc. After surgery, 22 of the 23 patients successfully reset the ciliary body, including four patients who underwent combined operations, which showed a statistically significant difference (P < 0.01). The mean preoperative IOP was 6.48 ± 1.62 mmHg and it has a different degree of rebound in 21 cases reaching 13.29 ± 2.11 mmHg on 6 months after operation, including 6 cases of transient high intraocular pressure (> 21 mmHg) (P < 0.01). Best corrected visual acuity was increased from preoperatively 0.60 ± 0.21 logMAR to 0.38 ± 0.26 log MAR postoperatively, in which the vision > 0.3 logMAR reached 65.2% (P < 0.01).
Conclusion: Direct cyclopexy with or without vitrectomy is an effective method for treating traumatic ciliary body detachment.
Keywords: cyclodialysis cleft, trauma, direct cyclopexy, intraocular pressure
Introduction
Cyclodialysis cleft refers to the separation of ciliary muscle fibers from the scleral spur, creating an aberrant pathway for aqueous drainage into the suprachoroidal space.1,2 The most common cause of cyclodialysis cleft is blunt ocular trauma, which can induce disinsertion of the longitudinal ciliary muscle fibers from the sclera by stretching the ocular tissue owing to mechanical axial compression and rapid equatorial expansion.1,3 Traumatic cyclodialysis cleft occurs as a result of blunt trauma or open globe injuries to the eyeballs with an incidence of 1–11%,4 but it is not rare in some large ophthalmology departments in China. Traumatic cyclodialysis cleft frequently results in persisting ocular hypotony causing ocular complications such as cataract, hypotonic maculopathy, disc edema, choroidal detachment, and retinal damage.5
The principle of traumatic cyclodialysis cleft management is to restore the apposition of the detached ciliary body to the sclera and hence the IOP. Over 20 clinical methods are available for the treatment of ciliary body detachment,6–8 such as laser photocoagulation (argon laser, YAG laser, diode laser6), transconjunctival cryotherapy,3 transscleral diathermy, direct cyclopexy, intravitreous gas injection, gas endotamponade in conjunction with cryotherapy,7 vitrectomy, scleral buckling, and the use of intraocular lens haptics to compress the cleft against the sclera.8 However, the therapeutic effect of these methods for traumatic cyclodialysis cleft remains controversial. Few studies have systematically evaluated the safety and efficacy of these techniques, and there is no gold standard for the surgical treatments of traumatic cyclodialysis cleft.9
In this study, we reviewed a consecutive series of patients with traumatic cyclodialysis cleft treated with direct cyclopexy and evaluated the therapeutic effects by assessing the visual acuity, IOP, UBM examination.
Methods
Design and Population
This retrospective study was approved by the Ethics Committee of Tianjin Eye Hospital (KY2023087) and conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from all participants. The study recorded 23 eyes of 23 consecutive patients diagnosed with cyclodialysis cleft due to blunt ocular trauma during February 2021 to August 2022. All of the patients had additional anterior or posterior segment damage (including cataract, lens dislocation, vitreous hemorrhage, retinal detachment, subretinal hemorrhage, choroidal detachment, and suprachoroidal hemorrhage or choroidal avulsion). Patients with a history of intraocular surgery, such as glaucoma filtration surgery, cataract surgery, or vitrectomy, were excluded.
Clinical Evaluation
The patients’ preoperative information including age, sex, ocular history, uncorrected visual acuity (UCVA), best-corrected visual acuity (BCVA), IOP, gonioscopy, fundus photography, ultrasound biomicroscopy (UBM) (Model SW-3200L, Tianjin Suowei Electronic Technology Co., Ltd., Tianjin, China), and B-scan ultrasonography (Model MD-2300, Tianjin MEDA Co., Ltd. Tianjin, China) were collected. The IOP was measured three times using a Non-Contact Tonometer (Canon TX-20 tonometer; Canon Inc., Tokyo, Japan), and the mean value was calculated. The range of the cyclodialysis cleft was measured by two experienced doctors using UBM and gonioscopy when the anterior chamber angle could be clearly seen. All patients were followed up for at least six months postoperatively. The BCVA, IOP, and UBM were measured for the patients at each follow-up visit.
Surgical Management
Direct cyclopexy was performed as follows: a conjunctival flap was made at the site of the cyclodialysis cleft and the sclera was exposed. A partial-thickness scleral flap was then made 3 mm posterior to the limbus and the flap was a little larger than the cleft itself to ensure that no cleft was left without reapposition. After elevating the scleral flap, the sclera was incised at 1.5 mm posterior and parallel to the limbus. The aqueous humor was released and the cyclodialysis cleft was visualized. The detached ciliary body was directly fixed to the sclera with an interrupted loop suture through the anterior sclera, ciliary body, and posterior scleral lip using 10–0 nylon sutures. The scleral flap and conjunctiva were then closed by suturing (Figure 1). All patients received atropine and corticosteroid eye drops before surgery.
 |
Figure 1 Surgical procedure of direct cyclopexy for traumatic cyclodialysis cleft (A) A conjunctival flap was made and the sclera was exposed and incised for preparation of the scleral flap. (B) The scleral flap was being made. (C) The scleral flap has been created. (D) The sclera was incised 1.5 mm posterior and parallel to the limbus. The aqueous humor was released and the cyclodialysis cleft was visualized. (E) The detached ciliary body was directly fixed to the sclera with an interrupted loop suture through the anterior sclera, ciliary body, and again through the posterior scleral lip using 10–0 nylon sutures. (F) The full length of the cleft was closed. (G) The scleral flap was closed with interrupted sutures. (H) The conjunctiva was closed. |
Other surgical techniques were also performed during the cyclopexy surgery, such as coreoplasty, iridodialysis repair for anterior segment injury, vitrectomy, retinal reattachment, and scleral tapping for posterior segment injury based on the patients’ ocular conditions. Postoperative management included atropine eye drops to paralyze the ciliary muscle, corticosteroids eye drops for anti-inflammation, antibiotics to prevent infection, and IOP- lowering medications if needed.
Statistical Analysis
SPSS16.0 statistical software was used for data analysis. Fisher’s exact test was used to compare the conditions of cyclodialysis cleft reattachment before and after surgery, and paired t-test was used to compare IOP and visual acuity. Statistical significance was set at P<0.05.
Results
The 23 patients (20 males, 3 females) who suffered traumatic ciliary body detachment had single-eye injuries, and their disease course ranged from 2 to 4 months. The age range of the patients was from 12 to 57 years with a mean age of 42.5±2.8 years. Among these patients, eight were wounded by fist blows, five were slapped by bamboo and wood, three were hit by plastic sheets, two were beaten by rocks, one was injured by football, one was injured by badminton, and one was injured by firecrackers. Surgeries were performed approximately 14 days to 4 months after injury according to the different ranges of the cyclodialysis cleft.
Nineteen patients were injured, mainly in the anterior segment, some combined with hyphema, discoria, and iridodialysis. Four patients had posterior segment injuries such as retinal detachment, choroid detachment, subretinal hemorrhage, and massive vitreous hemorrhage. Sixteen patients had retinochoroidal folds and optic disc edema. The cyclodialysis cleft angle ranged from 50°-270° detected by UBM examination. The range of clefts in five cases was less than one quadrant, accounting for 21.7% of all patients; 12 cases (52.2%) ranged from to 1–2 quadrants, and six cases (26.1%) ranged from to 2–3 quadrants. Among the 23 patients undergoing direct cyclopexy for traumatic cyclodialysis, cleft closure was achieved in 22 cases (Figure 2), including four cases with vitrectomy simultaneously; in one case, a small residual cleft persisted due to loose stitches (Figure 3) and underwent a second cyclopexy operation 2 weeks later. The apposition of the detached ciliary body to the sclera was successfully restored in 22 of the 23 patients after one operation. The differences before and after surgery were statistically significant (P<0.01).
 |
Figure 2 The preoperative and postoperative UBM images of cyclodialysis cleft. (A) Obvious cyclodialysis cleft before surgery in a patient. (B) Well-reattached ciliary body of the same patient one month after surgery. |
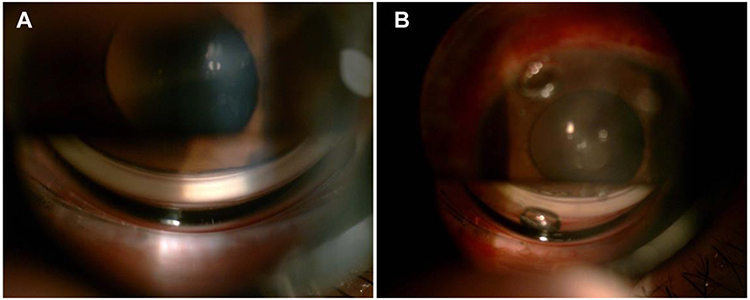 |
Figure 3 Images of cyclodialysis cleft on gonioscope. (A) image shows a narrow cyclodialysis cleft at the bottom. (B) image shows two visible stitches at the bottom after repair. |
The preoperative mean IOP was 6.48 ±1.62 mm Hg (range, 4–9 mmHg) (Table 1). IOP increased significantly to 14.57 ± 3.09 mmHg (t =12.74, P < 0.01) at one day after surgery and to 13.29 ± 2.11 mmHg on 6 months after operation (t =10.594, P < 0.01). Six patients experienced transient high IOP (> 21 mmHg) after surgery and the IOP subsequently decreased to normal range (<21 mmHg) within 5 days (Table 1) by using antiglaucoma agents. Among the two patients whose IOP did not rise to the normal range on one day after surgery, one still had a narrow cleft left without complete reattachment and the IOP returned to the normal range after the second surgery, and the other patient did not recover until 8 months after surgery.
 |
Table 1 Comparision of Intraocular Pressure (IOP) of Patients With Cyclodialysis Before and After Cyclopexy |
The mean BCVA was 0.60 ± 0.21 logMAR preoperatively and improved to 0.38 ± 0.26 logMAR 6 months postoperatively (Table 2). 65.2% of post-operative patients had visual acuity better than 0.52 logMAR. Visual acuity before and after surgery was significantly different (t = 5.04, P < 0.01).
 |
Table 2 Comparison of Best-Corrected Vision Acuity (BCVA) in Patients With Cyclodialysis Before and After Cycloplexy |
After operation, the anterior chamber deepened (Figure 4) and posterior retinal edema faded gradually (Figure 5). Only one patient with persisting low IOP presented retinal abnormalities six months after surgery. Except for transient IOP elevation, no other serious postoperative complications, such as ciliary body hemorrhage, anterior segment ischemia, or endophthalmitis, were observed in this series.
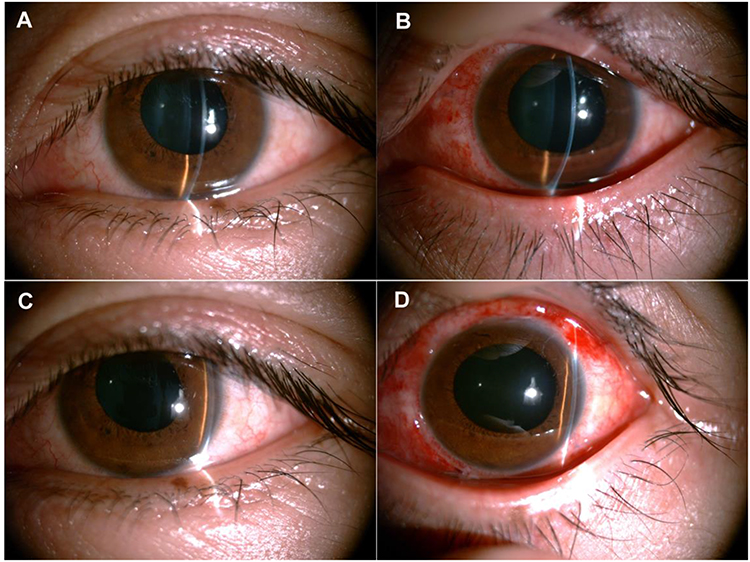 |
Figure 4 Anterior chamber changes before and after direct cyclopexy surgery. (A) image shows the shallow central and peripheral anterior chambers, approximately 1/4CT below. (B) image shows the deepened central and peripheral anterior chambers of the same patient 10 days after surgery, approximately 3/4CT below. (C) shows shallow preoperative temporal anterior chamber. (D) shows a deepened temporal anterior chamber 7 days after surgery. |
 |
Figure 5 Eye fundus images before and after surgery. (A) image shows preoperative retinal edema, retinal radial wrinkles in the macular area, and unclear optic disk boundaries in one patient. (B) image shows the changes in the same patient A 1.5 month after surgery: posterior retinal edema, optic disc edema, and retinal radial wrinkles disappear. (C) image shows a preoperative fundus image of another patient with cyclodialysis cleft after blunt trauma. Macular edema, wrinkles, choroid arc-shaped lacerations across the macular area, and subretinal hemorrhage in the macular area were observed. (D) image shows the changes in the same patients at C 10 days after cyclopexy: posterior retinal edema decreased obviously, and white stripe at the choroid arc-shaped laceration is clear. |
Discussion
Although numerous surgical treatment strategies have been employed in clinical settings, there remains no standardized protocol for managing traumatic cyclodialysis clefts. Direct cyclopexy is often the definitive procedure when conservative management fails to close the cleft.10 The first surgical intervention for traumatic cyclodialysis was performed by Vannas and Boerkenheim in 1952.11 Since then, various modifications have been introduced to improve tissue apposition and cleft closure. For instance, full-thickness or partial-thickness scleral flaps have been utilized depending on the size and extent of the cyclodialysis cleft. McCannel described an alternative technique involving a suture placed through the sclera and ciliary body base, followed by radial passage through the cornea.12 Other authors have reported approaches using horizontal stack suturing without scleral incision and continuous suturing with a scleral flap.11,12
The principles underlying all surgical repairs include obliteration of the cyclodialysis space and apposition between the sclera and the ciliary body wall.9 Continuous sutures offer simplicity and reduced operative time but carry a higher risk of stitch loss. Techniques without scleral flap incisions provide poor visibility during surgery, thus requiring high operator skill in controlling suture depth. Traditional interrupted sutures and reattachment surgeries offer better visibility and precise tissue repositioning, as demonstrated in.13 In this study, we opted for traditional ciliary body suture and reattachment surgery to treat patients with traumatic cyclodialysis clefts. Clefts were successfully closed in 22 out of 23 eyes after a single operation, with intraocular pressures (IOP) returning to normal and varying degrees of visual improvement observed. The outcome of direct cyclopexy for treating traumatic cyclodialysis clefts in our study was acceptable.
In other studies, Kijima reported successful closure in 5 out of 5 cases following direct cyclopexy,5 Agrawal and Shah reported success in 11 out of 12 cases,14 and Kuchle reported success in 28 out of 29 cases.15 These variations in outcomes may be attributed to differences in surgical experience, accurate incision site location, completeness of suturing, and suture firmness. Regardless of the method used, precise identification of the cyclodialysis cleft’s size and extent is crucial. Ultrasound biomicroscopy (UBM) provides valuable information for diagnosis, defining the location of cyclodialysis, and monitoring postoperative progress.16
Regarding optimal timing and indications for surgery, it appears that moderate-to-large clefts where medical or non-invasive treatments have failed are best managed surgically.17,18 Most authors agree that treatment should not be delayed due to the risk of permanent vision loss from retinal damage.2 When deciding on the optimal therapy for cyclodialysis, factors such as the duration of hypotony, the extent of cyclodialysis, and the degree of visual impairment should be considered. In our practice, if the cleft extent is less than 60°, we prefer medical treatment, primarily using atropine to paralyze the ciliary muscle and facilitate attachment to the sclera. If reattachment does not occur within two weeks, surgery is considered. For clefts between 60°-90°, we typically observe for approximately 7–10 days before opting for surgery. For clefts greater than 90°, we recommend immediate surgery. The cleft extents in this group ranged from 50° to 270°, with surgery performed 14 days to 4 months post-diagnosis. One patient had two clefts, measuring 30° and 50° respectively. Due to fear of surgery, this patient did not undergo surgery until four months later. Although the ciliary body reattachment surgery was successful, IOP remained low, potentially leading to severe visual function injury due to prolonged detachment weakening the aqueous humor secretion function of ciliary epithelial cells. For patients who also underwent vitrectomy for posterior segment injuries, surgery was ideally performed about two weeks post-injury to facilitate the procedure and reduce complications. Four patients in this study underwent vitrectomy approximately two weeks post-injury, with all clefts successfully closed.
An increase in IOP post-surgery indicates successful repair. In some cases, IOP exceeded the normal value of 21 mmHg. Possible reasons include: ① Blockage of abnormal aqueous humor outflow pathways, preventing direct drainage into the suprachoroidal space while impaired trabecular filtration function recovers; ② Recovery of ciliary body epithelial cell function; ③ Postoperative inflammatory reactions causing blockage of the trabecular meshwork and reduced filtration; ④ Sutures placed too close to the corneal limbus combined with postoperative inflammation leading to iris root adhesion and angle closure. In the first three scenarios, IOP usually returns to normal within 3–5 days of treatment; however, the fourth scenario may require surgical intervention. Given attention to suture placement, none of our patients experienced the fourth scenario. Additionally, four out of six patients with postoperative high IOP exhibited significant anterior chamber inflammation and Tyndall (+++), suggesting that postoperative IOP increases are more likely in patients with severe inflammation. Strengthened anti-inflammatory measures can quickly control IOP, though excessive anti-inflammatory measures are unnecessary as postoperative inflammation aids in restoring ciliary body-scleral apposition.19
Concerning whether to incise and suture at the 3 o’clock and 9 o’clock positions during surgery, most scholars recommend avoiding these directions to prevent injury to ciliary body nerves and blood vessels.9 However, some reports indicate that incisions in these directions do not cause significant complications, and our study found no obvious bleeding or other complications in patients cut at these positions. Therefore, we propose that the 3 o’clock and 9 o’clock positions are not surgical “forbidden zones”. However, if clefts exist in both directions, we suggest suturing in only one direction to avoid potential risks.
Clinically, traumatic patients with other anterior or posterior segment injuries, especially those with initially mild hypotony, may overlook the diagnosis of cyclodialysis clefts. Therefore, careful attention should be paid to the possibility of ciliary body detachment and other emergencies such as scleral rupture and angle recession. UBM and anterior OCT can provide clear images to detect hidden ciliary detachments and enable timely treatment.16,20 Four patients in this study with severe posterior injuries were diagnosed using UBM, facilitating correct treatment.
Despite the effectiveness of direct cyclopexy in treating cyclodialysis clefts, limitations remain. The optimal timing for surgery post-trauma is undefined. Currently, we adopt a conservative approach if the patient’s vision and hypotony are stable Our study supports existing evidence that direct cyclopexy, with or without vitrectomy, is an efficacious, safe, and adoptable surgical approach for traumatic cyclodialysis clefts. Further case-control studies with larger sample sizes and longer follow-up periods are needed to verify its efficacy and safety.
In conclusion, under current medical technology and equipment, cyclodialysis clefts can be accurately diagnosed. With more cases and data accumulation, more effective and noninvasive treatment methods are expected to emerge in the future.
Data Sharing Statement
All data generated or analyzed during this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was reviewed and approved by the Ethics Committee of Tianjin Eye Hospital (KY2023087) and was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from the Review Board of Tianjin Eye Hospital.
Acknowledgment
This paper has been uploaded to Research Square as a preprint: https://www.researchsquare.com/article/rs-3848474/v1
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (32200684), the Tianjin Science & Technology Foundation (21JCQNJC01030), the Tianjin Health Research Project (TJWJ2022QN078), the Tianjin Key Medical Discipline (Specialty) Construction Project (TJYXZDXK-016A). The funders were involved with the study design, data collection, analysis, interpretation, and writing.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. González-Martín-Moro J, Contreras-Martín I, Muñoz-Negrete FJ, Gómez-Sanz F, Zarallo-Gallardo J. Cyclodialysis: an update. Int Ophthalmol. 2017;37(2):441–457. doi:10.1007/s10792-016-0282-8
2. Ioannidis AS, Barton K. Cyclodialysis cleft: causes and repair. Curr Opin Ophthalmol. 2010;21(2):150–154. doi:10.1097/ICU.0b013e3283366a4d
3. Popovic M, Shareef S, Mura JJ, et al. Cyclodialysis cleft repair: a multicenter, retrospective case series. Clin Exp Ophthalmol. 2019;47(2):201–211. doi:10.1111/ceo.13378
4. Zhang X, Wang N, Zheng G, et al. A modified single-armed suture technique for traumatic cyclodialysis cleft with vitreoretinal injury. J Clin Med. 2023;12(13):4252. doi:10.3390/jcm12134252
5. Kijima R, Shinmei Y, Shinkai A, Kanaya R, Chin S, Ishida S. Surgical outcomes of partial ciliary body direct suturing under the scleral flap for traumatic cyclodialysis cleft: a five-case series. Eur J Ophthalmol. 2022;32(6):3712–3719. doi:10.1177/11206721221083718
6. Selvan H, Gupta V, Gupta S. Cyclodialysis: an updated approach to surgical strategies. Acta Ophthalmol. 2019;97(8):744–751. doi:10.1111/aos.14210
7. Popovic M, Shareef S, Mura JJ, et al. Cyclodialysis cleft repair: a multi-centered, retrospective case series response. Clin Exp Ophthalmol. 2019;47(2):304–308. doi:10.1111/ceo.13427
8. Malandrini A, Balestrazzi A, Martone G, Tosi GM, Caporossi A. Diagnosis and management of traumatic cyclodialysis cleft. J Cataract Refract Surg. 2008;34(7):1213–1216. doi:10.1016/j.jcrs.2008.02.038
9. Morin A, Delbarre M, Friang C, Marechal M, Froussart-Maille F. Cyclodialysis, a therapeutic challenge: review of the literature on current practices. J Fr Ophtalmol. 2019;42(8):852–863. doi:10.1016/j.jfo.2019.03.021
10. Wang M, Hu S, Zhao Z, et al. A novel method for the localization and management of traumatic cyclodialysis cleft. J Ophthalmol. 2014;2014:761851. doi:10.1155/2014/761851
11. Vannas M, Bjorkenheim B. On hypotony following cyclodialysis and its treatment. Am Acta Ophthalmol. 1952;30:63–64.
12. McCannel A. A retrievable suture idea for anterior uveal problems. Ophthalmic Surg. 1966;17(11):739–741.
13. Murta F, Mitne S, Allemann N, Paranhos Junior A. Direct cyclopexy surgery for post-traumatic cyclodialysis with persistent hypotony: ultrasound biomicroscopic evaluation. Arq Bras Oftalmol. 2014;77(1):50–53. doi:10.5935/0004-2749.20140013
14. Agrawal P, Shah P. Long-term outcomes following the surgical repair of traumatic cyclodialysis clefts. Eye. 2013;27(12):1347–1352. doi:10.1038/eye.2013.183
15. Kuchle M, Naumann GOH. Direct cycloplexy for traumatic cyclodialysis with persisting hypotony; report in 29 consecutive patients. Ophthalmology. 1995;102(2):322–333. doi:10.1016/S0161-6420(95)31021-4
16. Ning L, Wen Y, Lan L, et al. Effect of different preoperative intraocular pressures on the prognosis of traumatic cyclodialysis cleft associated with lens subluxation. Ophthalmol Ther. 2022;11(2):689–699. doi:10.1007/s40123-022-00468-0
17. Wang A, Zhao Z. Comparing vitrectomy, silicone oil endotamponade with/without cyclopexy to treat cyclodialysis clefts with severe ocular trauma. Retina. 2021;41(6):1174–1181. doi:10.1097/IAE.0000000000002996
18. Augsten R, Königsdörffer E. Surgical treatment of cyclodialysis. Klin Monbl Augenheilkd. 2005;222(6):509–512. doi:10.1055/s-2005-858361
19. Joussen AM, Strauß O, Winterhalter S, Klamann M, Dietrich-Ntoukas T, Müller B. Ocular hypotension: how the retina surgeon sees the causes and therapeutic options. Klin Monbl Augenheilkd. 2016;233(9):1024–1032. doi:10.1055/s-0042-109708
20. Berk TA, Peretz D, Mofti A, et al. Non-invasive monitoring of cyclodialysis cleft using anterior segment optical coherence tomography and its role in informing clinical treatment decisions. Am J Ophthalmol Case Rep. 2022;26:101410. doi:10.1016/j.ajoc.2022.101410
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.