")
Back to Journals » Clinical Ophthalmology » Volume 18
Effect of Intraocular Lens Power Calculation Formula Optimization in the Sum-of-Segments Optical Biometer
Authors Kojima T, Tamaoki A , Ichikawa K, Satoh Y, Tomemori R, Watanabe K , Hasegawa A, Sawaki A, Kaga T
Received 6 May 2024
Accepted for publication 29 August 2024
Published 6 September 2024 Volume 2024:18 Pages 2545—2553
DOI https://doi.org/10.2147/OPTH.S477006
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Takashi Kojima,1,2 Akeno Tamaoki,2 Kazuo Ichikawa,3 Yuya Satoh,4 Ryota Tomemori,5 Keizo Watanabe,6 Asato Hasegawa,2 Ayako Sawaki,2 Tatsushi Kaga2
1Department of Ophthalmology, Nagoya Eye Clinic, Nagoya, Aichi, Japan; 2Department of Ophthalmology, Japanese Community Healthcare Organization Chukyo Hospital, Nagoya, Aichi, Japan; 3Department of Ophthalmology, Chukyo Eye Clinic, Nagoya, Aichi, Japan; 4Department of Ophthalmology, Satoh Yuya Eye Clinic, Sendai, Miyagi, Japan; 5Department of Ophthalmology, Tomemori Eye Clinic, Hashimoto, Wakayama, Japan; 6Department of Ophthalmology, Minami Osaka Eye Clinic, Sennangun, Osaka, Japan
Correspondence: Takashi Kojima, Email [email protected]
Purpose: We evaluated the effect of optimization of the intraocular lens (IOL) power calculation formula SRK/T and Barrett Universal II (BU II) in long eyes (≥ 26 mm: group L) and short eyes (≤ 22 mm: group S) using axial length calculated from segmented refractive indices (SRI).
Setting: Multicenter study at five sites in Japan.
Design: Retrospective observational study.
Methods: This study included 461 eyes of 461 patients (mean age 73.8 ± 8.4 years) who underwent cataract surgery. The predicted refractive error (PRE) was compared between the SRI (ARGOS) and the equivalent refractive index (ERI) biometers (IOLMasterTM 700). The patients were randomly divided into two groups, a learning group and a validation group. The optimization constants were determined in the learning group, and the optimization constants were subsequently applied to the validation group and compared with the ERI biometer results.
Results: Using both SRK/T and BU II, the validation group’s PRE using optimization constants for the SRI biometer in group L was significantly smaller than that using the ERI biometer (p< 0.001, p< 0.01). In group L, the arithmetic PRE of Barrett UII formula with SRI showed a significant improvement after optimization compared to before optimization (p< 0.0001). In group S, the arithmetic PRE of SRK/T and Barrett UII formula with SRI showed a significant improvement (p< 0.0001, p< 0.0001).
Conclusion: In long and short eyes, the current study revealed that optimization of the SRK/T and Barrett formula constants for the SRI biometer was beneficial to achieve accurate refractive outcomes after cataract surgery.
Keywords: segmented refractive index, intraocular lens power calculation, Sanders-Retzlaff-Kraff theoretic, Barrett universal II, optimization
Introduction
Modern cataract surgery, also known as refractive cataract surgery, tailors treatment to suit the patient’s lifestyle and aims to minimize the predicted refractive error (PRE) for optimal vision alignment with patient preferences.
The axial length is conventionally calculated using an equivalent refractive index using an optical biometer. Furthermore, the axial length is converted using a linear equation for segmental measurements of a water-immersion ultrasound biometer.1 This conversion equation corrects the crystalline lens occupancy rate in the eye but has limitations, leading to hyperopic PRE in long eyes and myopic PRE in short eyes even with third-generation IOL power calculations.2–5 To address this, the Wang–Koch correction formula6 was developed to correct axial length for long eyes using the Holladay I, SRK/T, HofferQ, and Haigis formulae.
The optical sum-of-segments biometer, which has been clinically used recently, measures the optical path lengths of the cornea, anterior chamber, lens, and vitreous. Additionally, it calculates the geometric length by dividing the values with the respective refractive indices and subsequently adding them together to calculate the axial length.7,8 The axial length measured using equivalent refractive indices has been shown to underestimate the short eyes and overestimate the long eyes compared to the sum-of-segments optical biometer.4 Using a sum-of-segments optical biometer reduces PRE using a third-generation IOL power calculation formula.2–4
PRE’s tendency may differ when using IOL constants optimized by conventional optical biometers. Therefore, optimizing the IOL constants in accordance with the optical biometer using segmented refractive indices is necessary. However, information regarding this consideration is limited to date.
This study aimed to investigate whether optimizing the IOL constants for the IOL power calculation formulae would lead to a PRE reduction when using a sum-of-segment optical biometer in long and short eyes.
Methods
This retrospective, multicenter study was conducted at a major cataract surgery center in Japan. The participating institutions included the Japan Community Healthcare Organization Chukyo Hospital, Satoh Yuya Eye Clinic, Minami Osaka Eye Clinic, Tomemori Eye Clinic and Chukyo Eye Clinic. This study was approved by our Institutional Review Board (20201002–01).
Patient Inclusion and Exclusion Criteria
Eyes who underwent cataract surgery and received SN60WF (Alcon) implantation during the observation period were prescreened, and those with a preoperative axial length of < 22 mm or > 26 mm were selected. In patients with both eyes selected, only 1 eye per patient were randomly selected.
Patients with corrected visual acuity of < 20/25 at 1–3 months postoperatively or missing ocular examination data at 3 months postoperatively were excluded. Patients with a history of ocular surgery, including corneal refractive surgery, poorly controlled glaucoma, progressive diabetic retinopathy, uveitis, retinal detachment, iris angiogenesis, corneal degeneration, severe dry eye, history of ocular trauma, weak zonules, corneal astigmatism of ≥ 2 D, and intraoperative or postoperative complications were excluded. Ultimately, 422 patients and 422 eyes were included in this study. Table 1 lists the demographic information of all patients.
 |
Table 1 Patient Demographic Information and Ocular Biometric Parameters. Data is Represented as Mean ± Standard Deviation |
Categorization of Cases
All patients were subsequently divided into two groups: one to optimize the IOL constant, and the other to validate its effect. Patients were first categorized into three groups based on the axial length (AL): short eyes (AL ≤ 22 mm), standard eyes (22 mm < AL < 26 mm), and long eyes (AL ≥ 26 mm) and subsequently into optimization and validation groups at a ratio of 1:1 for each axial length group. Table 2 lists the patient demographic information for these groups.
 |
Table 2 Patient Background and Ocular Parameters in the Development and Verification Groups. Data is Represented as Mean ± Standard Deviation |
Optical Biometer
The axial length measured by an optical biometer (ARGOS, Alcon) using the segmental refractive index was defined as the sum-of-segments axial lengths (ALsos). The axial length measured using an equivalent refractive index-based optical biometer (IOLMaster700, Carl Zeiss Meditec) was defined as the traditional axial length (ALtrad). Skilled, certified orthoptists assessed all patients.
Optimization of IOL Constants
The optimization of IOL constants was performed using Excel (ver. 16.88) by calculating the constants that minimized the predicted refractive error at 1 to 3 months postoperatively in the learning group. The IOL constants were optimized separately for long eyes and short eyes.
Evaluation Items
The SRK/T and Barrett Universal II (BU II) formulae were used to calculate the IOL power. The PRE was calculated for all patients by subtracting the predicted spherical equivalent power from the subjective equivalent spherical power at 1–3 months postoperatively. The PRE was subsequently compared to the ALtrad in the long (L group, 90 eyes) and short (S group, 44 eyes) eyes in the validation group.
Statistical Analyses
The Friedman test was used to compare the PRE obtained using ALsos, ALtrad, and ALsos after optimization. Statistical significance was set at a p-value of < 5%.
Results
PRE Before IOL Constant Optimization in the S Group
In all patients in the S group (N = 44), the PRE was compared between using ALsos and ALtrad using the two formulae (Figure 1). In the SRK/T and BU II formulae, the arithmetic mean of the PRE using ALsos was significantly different from that using ALtrad (SRK/T, p = 0.0002; BU II, p = 0.032). Contrastingly, the absolute errors did not differ between ALsos and ALtrad in either the SRK/T or BU II formulae (SRK/T, p = 0.4396; BU II, p = 0.2438).
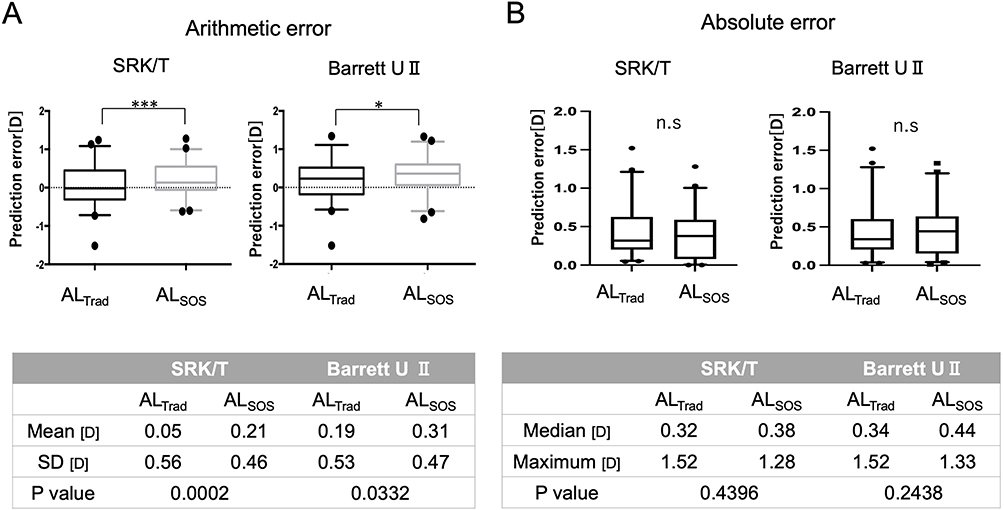 |
Figure 1 The predicted refractive error (PRE) in all short eyes. The PRE in the SRK and Barrett Universal II formulae were compared with those of traditional axial length (ALtrad) and the sum-of-The-segment axial length (ALsos), respectively. The arithmetic means of both formulae revealed that the ALsos group had a significantly larger error in the hyperopic direction than the ALtrad group (A). No difference was observed in the absolute error between the two groups for either equation (B). The box plots show the 5–95 percentile and medians. *And ***Represent p < 0.05 and p < 0.001, respectively. |
PRE Before Optimization in the L Group
In patients in the L group (N = 90), we compared PRE with ALsos and ALtrad using the two formulae (Figure 2). For the SRK/T and BU II formulae, the arithmetic mean of the PRE using ALsos was significantly different in the myopic direction compared with that using ALtrad. (SRK/T, p < 0.0001; BU II, p < 0.0001). Contrastingly, the absolute errors did not differ between using ALsos and ALtrad in either the SRK/T or BU II formulae (SRK/T, p = 0.1702; BU II, p = 0.2017).
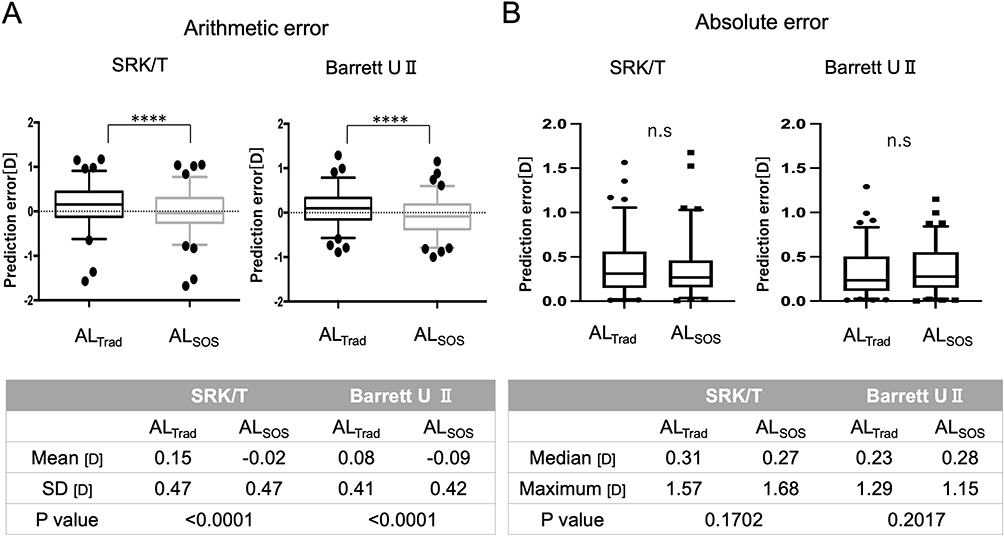 |
Figure 2 The predicted refractive error (PRE) in all long eyes. The PRE values of the SRK/T and Barrett Universal II formulae were compared with those of traditional axial length (ALtrad) and the sum-of-The-segment axial lengths (ALsos), respectively. The arithmetic means of both formulae revealed a significantly larger myopic PRE in the ALsos group than in the ALtrad group (A). No difference was observed in the absolute error between the two groups for either formula (B). The box plots show 5–95 percentile and medians. ****Represents p < 0.0001. |
PRE After Optimization in the S Group
We compared the PRE using ALsos and ALtrad before and after optimization in the short eye verification group after optimizing the IOL constants,(N = 23) (Figure 3A and B).
 |
Figure 3 Investigating the effect of optimizing the intraocular lens (IOL) constant in short eyes. The sum-of-The-segment axial length (ALsos)-opt was defined as the prediction error of applying ALsos after IOL constant optimization. The traditional axial length (ALtrad), ALsos, and ALsos-opt groups were compared with the validation group (N = 23). In both formulae, the ALsos-opt considerably reduced the hyperopic PRE compared to ALsos (A). In the SRK/T formula, the percentage of cases within ±0.5 D of the prediction using ALsos (52%) was lower than that of ALtrad (65%) but improved to 70% after optimization (C). The percentage of cases within ±0.5 D of the prediction using ALsos (52%) was lower than that of ALtrad (70%) but improved to 61% after optimization (D). The box plots show 5–95 percentile and medians. *And ****Represent p < 0.05 and p < 0.0001, respectively. |
For the SRK/T and BU II formulae, the arithmetic mean of the PRE with ALsos after optimization was significantly smaller than that before optimization (SRK/T, p < 0.0001; BU II, p ≤ 0.0001). Contrastingly, the absolute errors were not significantly different before and after optimization in either the SRK/T or BU II formulae (SRK/T, p = 0.9575; BU II, p = 0.0545).
Figure 3C and D illustrate the PRE distribution. For the SRK/T formula, the percentage of patients within ±0.5 D of prediction using ALsos (52%) was lower than using ALtrad (65%); however, it improved to 70% after optimization. For the BU II formula, the percentage of patients within ±0.5 D of prediction using ALsos (52%) was lower than using ALtrad (70%); however, it improved to 61% after optimization.
PRE After Optimization in the L Group
After optimizing the IOL constants, we compared the PRE with ALsos before and after optimization in the verification group (N = 23) of the L group, and with ALtrad (Figure 4A and B).
 |
Figure 4 Investigating the effect of optimizing the intraocular lens (IOL) constant in long eyes. The sum-of-The-segment axial length (ALsos)-opt was defined as the prediction error of applying ALsos after optimizing the IOL constant. In the validation group (N = 47), traditional axial length (ALtrad), ALsos, and ALsos-opt were compared. ALsos-opt exhibited a substantial difference in the hyperopic direction compared to ALsos. (A). The difference in the absolute error was insignificant (B). In the SRK/T formula, the percentage of eyes within ±0.5 D of prediction with ALsos (77%) was higher than with ALtrad (67%) but not significantly different from the ALsos-opt (73%) (C). In the Barret U II formula, the percentage of eyes within ±0.5 D of prediction with ALsos (65%) was lower than the ALtrad (73%) but did not significantly differ from the ALsos-opt (63%) (D). The box plots show 5–95 percentile and medians. **, ***And ****Represent p < 0.01, p < 0.001, and p < 0.0001, respectively. |
The arithmetic mean of the PRE after optimization was significantly different from that before optimization for the SRK/T formula with ALsos (SRK/T, p < 0.0001). Contrastingly, the BU II formula with ALsos demonstrated a significant improvement in the PRE’s arithmetic mean after optimization compared to before optimization (BU II, p ≤ 0.0001). The absolute errors were not significantly different before and after optimization in the SRK/T and BU II formulae (SRK/T, p = 0.127; BU II, p = 0.464).
Figure 4C and D illustrate the distribution of the PRE. The prediction percentage within ±0.5 D using ALsos (77%) was higher than ALtrad (67%); however, the value was not largely different after optimization (73%) for the SRK/T formula (Figure 4C). The BU II formula demonstrated a lower percentage (65%) within ±0.5 D of prediction with ALsos than with ALtrad (73%); however, the value was not largely different after optimization (63%) (Figure 4D).
Discussion
The IOL power calculation formula currently in clinical use is based on the ALtrad, which is calculated using equivalent refractive indices based on the ultrasonic immersion method using the segmental sound velocity. The ALsos is the axial length obtained by calculating each tissue length based on the refractive index of each ocular tissue and subsequently adding them. The existing IOL power formulae have been developed assuming the ALtrad use; however, the PRE has been reported to be satisfactory even when ALsos is used in the existing IOL power formulae.4,8 Some studies have investigated the formulae compatible with ALsos. In the short and long eyes, ALsos was applied to the BU II formula, Barrett True Axial Length (BTAL), Emmetropia Verifying Optical (EVO), Hill-RBF, Hoffer QST, Holladay 2, Holladay 2-NLR, K6, Kane, Olsen, PEARL-DGS, and T2. The VRF, BTAL, EVO, Hoffer QST, K6, Olsen, and PEARL-DGS formulae have been reported to be highly predictive.9 Additionally, the BU II and Kane formulae were reported to be slightly less accurate than the newer-generation formulae, although the results were better than those of the third-generation formulae.9 In the present study, the IOL constants were optimized using ALsos with the BU II and SRK/T formulae, the two most commonly used formulae in Japan for long and short eyes, and examined whether the prediction accuracy could be improved.
In summary, the SRK/T and BU II formulae tended toward hyperopic PRE before optimization in short eyes; however, these results improved after optimization. It is reasonable to observe hyperopic PRE using ALsos because the axial length is measured to be longer than ALtrad in short eyes. Overall, the PRE was sufficiently small in short eyes even before optimization, indicating that the IOL power calculation was highly accurate; however, optimization further reduced the hyperopic PRE. Contrastingly, the mean PRE of the SRK/T formula was almost zero in long eyes even before optimization. SRK/T is a third-generation intraocular lens power calculation formula, and the use of traditional axial length has been reported to lead to hyperopic PRE in long eyes.10–13 The same tendency was observed in the present study. Therefore, the SRK/T formula has a sufficiently low PRE even before optimization, and the effect of the optimization is not substantial. However, the BU II formula exhibited a slightly myopic PRE when the ALsos was used. This may be attributed to new-generation formulae, such as the BU II, being designed to reduce the hyperopic PRE when ALtrad is used. Optimizing the IOL constants could improve the myopic PRE, especially in the BU II formula, with excessive correction for long eyes.
In this study, for eyes with long and short axial lengths, the SRK/T formula showed an improvement in predicted refractive error using ALsos after IOL constant optimization compared to ALtrad. However, with the Barrett Universal II formula, even after optimization, ALtrad resulted in smaller predicted refractive errors. This suggests that while third-generation IOL power calculation formulas like the SRK/T formula tend to cause hyperopic shifts in long axial lengths and myopic shifts in short axial lengths, new generation formulas are already designed to correct for these tendencies. Therefore, using ALsos in the BUII formula may result in over-compensation.
The results of this study showed that the improvement in predicted refractive error through the optimization of the IOL constant was less than 0.2D. Considering that the increments of IOL power are 0.5D, the impact of IOL constant optimization alone on the predicted refractive error is not considered to be significant. The predicted refractive error is influenced by a combination of various factors, including effective lens position, preoperative biometry errors, calculation formula errors, crystalline lens refractive index, and the accuracy of postoperative refractive measurements. To minimize the predicted refractive error, it is necessary to minimize the errors from each of these factors. In this sense, we believe that the optimization of the IOL constant in this study is clinically useful and worth pursuing.
Recently, improved formulae that assume the use of the ALsos, such as the BTAL and EVO formulae, have become available. Previously, the BTAL and EVO formulae have been reported to produce satisfactory results of 72.4% and 76.1% to ±0.5 D in short eyes and 90.6% and 81.1% to ±0.5 D in long eyes.9 These results are superior to the current results obtained using BU II and SRK/T. Biometry differences according to ethnicity may be one reason for this. Previously, the long eyes were defined to be ≥ 25 mm. In the present study, the long eyes were defined to be ≥ 26 mm; therefore, a comparative study using the same standards may be necessary in the future.
This study has several limitations. The first limitation is the relatively small number of short-eye cases. Although the cases in this study were divided into a learning group and a validation group for IOL constant optimization, the small number of short-eye cases may result in lower reliability for both the optimization and validation of the IOL constants. Short axial lengths are less common than long axial lengths in Asian countries, including Japan, where the myopic population is large. Short axial length eyes need to be reexamined in a larger number of cases in the future. Secondly, our study included only Japanese patients. Since differences exist in the biometry by ethnicity,14–16 reexamining biometry in various ethnic groups is necessary in the future. Third, this study is a retrospective study, and the timing of postoperative results varied between 1 to 3 months among the cases. Although previous studies have shown that the position and refraction of the SN60WF intraocular lens, which was used in this study, do not change after 1 month postoperatively,17 it is possible that the different timing of examinations may have affected the results.
In conclusion, the accuracy of the SRK/T and BU II formulae with ALsos was satisfactory for eyes with short and long axial lengths. In short eyes, the optimization was effective with the SRK/T and BU II formulae. In long eyes, BU II formula optimization was confirmed; however, the benefit of optimizing the SRK/T formula was limited.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author.
Statement of Ethics
This retrospective study was approved by the institutional review board of Japan Community Health Care Organization Chukyo Hospital (#20201002-01). The protocol of this study followed the tenets of the Declaration of Helsinki. The opt-out method was approved by the institutional review board in place of obtaining informed consent.
Acknowledgment
The current study was presented as a poster at the annual meeting of European Society of Cataract and Refractive Surgery 2021 in Amsterdam, Netherlands.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported with an investigator-initiated study grant (IIT#59244749) from Alcon Japan Ltd.
Disclosure
Dr. Tamaoki reports receiving personal fees from Nidek and Alcon Japan outside the submitted work. Dr. Kojima reports receiving personal fees from STAAR Surgical, Santen Pharmaceutical Co. Ltd., Johnson & Johnson, and Alcon Japan outside of the submitted work. Dr. Ichikawa reports grants and provision of equipment from Alcon Japan Ltd., Alcon, and provision of equipment from Carl Zeiss Meditec, during the conduct of the study; grants, and/or personal fees from Santen Pharmaceutical Co., Ltd., STAAR Surgical, and Kowa Company, Ltd., outside the submitted work. Dr. Watanabe reports grants from Alcon Japan Ltd, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Haigis W. Optical coherence biometry. Dev Ophthalmol. 2002;34:119–130. doi:10.1159/000060791
2. Wang L, Cao D, Weikert MP, Koch DD. Calculation of axial length using a single group refractive index versus using different refractive indices for each ocular segment: theoretical study and refractive outcomes. Ophthalmology. 2019;126(5):663–670. doi:10.1016/j.ophtha.2018.12.046
3. Cooke DL, Cooke TL. A comparison of two methods to calculate axial length. J Cataract Refract Surg. 2019;45(3):284–292. doi:10.1016/j.jcrs.2018.10.039
4. Tamaoki A, Kojima T, Hasegawa A, et al. Clinical evaluation of a new swept-source optical coherence biometer that uses individual refractive indices to measure axial length in cataract patients. Ophthalmic Res. 2019;62(1):11–23. doi:10.1159/000496690
5. Goto S, Maeda N, Noda T, et al. Change in optical axial length after cataract surgery: segmental method vs composite method. J Cataract Refract Surg. 2020;46(5):710–715. doi:10.1097/j.jcrs.0000000000000149
6. Wang L, Shirayama M, Ma XJ, Kohnen T, Koch DD. Optimizing intraocular lens power calculations in eyes with axial lengths above 25.0 mm. J Cataract Refract Surg. 2011;37(11):2018–2027. doi:10.1016/j.jcrs.2011.05.042
7. Shammas HJ, Ortiz S, Shammas MC, Kim SH, Chong C. Biometry measurements using a new large-coherence-length swept-source optical coherence tomographer. J Cataract Refract Surg. 2016;42(1):50–61. doi:10.1016/j.jcrs.2015.07.042
8. Omoto MK, Torii H, Masui S, Ayaki M, Tsubota K, Negishi K. Ocular biometry and refractive outcomes using two swept-source optical coherence tomography-based biometers with segmental or equivalent refractive indices. Sci Rep. 2019;9(1):6557. doi:10.1038/s41598-019-42968-3
9. Shammas HJ, Taroni L, Pellegrini M, Shammas MC, Jivrajka RV. Accuracy of newer intraocular lens power formulas in short and long eyes using sum-of-segments biometry. J Cataract Refract Surg. 2022;48(10):1113–1120. doi:10.1097/j.jcrs.0000000000000958
10. Melles RB, Holladay JT, Chang WJ. Accuracy of Intraocular Lens Calculation Formulas. Ophthalmology. 2018;125(2):169–178. doi:10.1016/j.ophtha.2017.08.027
11. Mori Y, Minami K, Tokuda S, Lee J, Miyata K. Effect of the ratio of axial length to keratometry on SRK/T intraocular lens power calculations for eyes with long axial lengths. Sci Rep. 2019;9(1):19515. doi:10.1038/s41598-019-56116-4
12. Karabela Y, Eliacik M, Kaya F. Performance of the SRK/T formula using A-Scan ultrasound biometry after phacoemulsification in eyes with short and long axial lengths. BMC Ophthalmol. 2016;16:96. doi:10.1186/s12886-016-0271-8
13. Zhang Z, Miao Y, Fang X, Luo Q, Wang Y. Accuracy of the Haigis and SRK/T formulas in eyes longer than 29.0 mm and the influence of central corneal keratometry reading. Curr Eye Res. 2018;43(11):1316–1321. doi:10.1080/02713683.2018.1488265
14. Wang D, Amoozgar B, Porco T, Wang Z, Lin SC. Ethnic differences in lens parameters measured by ocular biometry in a cataract surgery population. PLoS One. 2017;12(6):e0179836. doi:10.1371/journal.pone.0179836
15. Lam BC, Weiss M, Jing F, Zhu C, Johnson DA, Kheirkhah A. Comparison of ocular biometric parameters between Hispanic and non-Hispanic ethnicities in white adults undergoing cataract surgery. Eye Contact Lens. 2022;48(9):391–395. doi:10.1097/ICL.0000000000000907
16. Shufelt C, Fraser-Bell S, Ying-Lai M, Torres M, Varma R; Los Angeles Latino Eye Study G. Refractive error, ocular biometry, and lens opalescence in an adult population: the los angeles latino eye study. Invest Ophthalmol Vis Sci. 2005;46(12):4450–4460. doi:10.1167/iovs.05-0435
17. Fukumitsu H, Camps VJ, Miraflores S, Piñero DP. Relationship between medium-term changes in intraocular lens position and refraction after cataract surgery with two different models of monofocal lenses. J Clin Med. 2021;27(10):3856. doi:10.3390/jcm10173856
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.