")
Back to Journals » Journal of Inflammation Research » Volume 17
Effect of Laparoscopic Inguinal Hernia Repairs on Inflammatory Factors, Oxidative Stress Levels and Postoperative Recovery
Authors Yang B, Xie C, Lv Y, Wang Y
Received 27 May 2024
Accepted for publication 27 September 2024
Published 29 October 2024 Volume 2024:17 Pages 7929—7937
DOI https://doi.org/10.2147/JIR.S480105
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Bo Yang, Changhu Xie, Yuxing Lv, Yinquan Wang
Department of Hernia and Abdominal Wall Surgery, Shanxi Bethune Hospital, Shanxi Academy of Medical Science, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, Shanxi, 030032, People’s Republic of China
Correspondence: Yinquan Wang, Department of Hernia and Abdominal Wall Surgery, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongi Shanxi Hospital, Third Hospital of Shanxi Medical University, No. 99 Longcheng Street, Xiaodian District, Taiyuan, Shanxi, 030032, People’s Republic of China, Tel +86-13834046996, Email [email protected]
Objective: To unravel the effects of different laparoscopic inguinal hernia repairs (IHRs) on inflammatory factors, oxidative stress, and postoperative recovery of inguinal hernia (IH) patients.
Methods: A total of 88 patients for laparoscopic treatment of IH were studied in a retrospective cohort, and were randomized into the transabdominal preperitoneal (TAPP) repair group (n = 44) and the total extraperitoneal (TEP) repair group (n = 44) according to the method of treatment. Patients in the TAPP group underwent laparoscopic TAPP IHR, while patients in the TEP group underwent laparoscopic TEP IHR. Visual analogue scores (VAS) were measured at 1, 3, and 7 d after repair. Gastrin (GAS), motilin (MTL), matrix metalloproteinase (MMP)-2, MMP-9, and tissue inhibitor of metalloproteinases-1 (TIMP-1) were assessed by enzyme-linked immunosorbent assay. Superoxide dismutase (SOD) was tested by spectrophotometry and malondialdehyde (MDA) and β-endorphin (β-EP) were examined by radioimmunoprecipitation. Total antioxidant capacity (T-AOC) was evaluated by chemical colorimetry, quality of life was evaluated by SF-36, and fibrinogen (FIB), C-reactive protein (CRP), antitrypsin (al-AT), and interleukin-6 (IL-6) levels were determined by immunoturbidimetry. Complications and postoperative recurrence were recorded.
Results: VAS scores in the TEP group were lower than those in the TAPP group. Operative time, hospital stay, time for postoperative activity out of bed, and time taken to exhaust were shorter in the TEP group than in the TAPP group. Intraoperative blood loss was less in the TEP group than in the TAPP group. GAS, MTL, SOD, and T-AOC were higher, and MDA, β-EP, CRP, FIB, alAT, IL-6, MMP-2, MMP-9, and TIMP-1 were lower in the TEP group than the TAPP group. Quality of life was improved in the TEP group compared with the TAPP group. There was no significant difference in the rate of postoperative complications and recurrence rates between both groups of patients.
Conclusion: For IHs, laparoscopic TEP repair can effectively relieve pain, reduce inflammatory factors and oxidative stress indices, and facilitate postoperative recovery.
Keywords: laparoscopic transabdominal preperitoneal inguinal hernia repair, laparoscopic total extraperitoneal inguinal hernia repair, inguinal hernia, inflammatory factors, oxidative stress
Introduction
Inguinal hernias (IHs) are caused by a defect in the abdominal wall of the inguinal region.1 Patients with mild or asymptomatic IHs may have a significant bulge in the groin area with or without pain. With sudden IHs, the pain is usually unilateral, sharp, or burning and radiates to the lower abdomen, proximal thigh, lower back, perineum, or scrotum. However, the onset is more likely to be latent.2 Small, painless hernias may not require treatment. Surgery is usually needed to treat a large hernia or hernia that is causing pain and is trapped.3 An improved method of management of IHs is clinically required to improve the quality of life.
Although some authors believe that the open approach is still the gold standard for inguinal hernia repair (IHR),4 there are data demonstrating that laparoscopic repair has a lower incidence of chronic inguinal pain and allows for a quicker return to daily activities compared to open repair.5,6 Laparoscopic repair takes advantage of short recovery time, early resumption of daily activities, less pain, and low recurrence rates.7,8 Laparoscopic IHRs include total extraperitoneal (TEP) repair and transabdominal preperitoneal (TAPP) repair, both of which make extensive use of mesh; however, the TAPP technique requires access to the abdominal cavity to place the mesh, whereas, with the TEP technique, the entire surgical procedure is performed outside the peritoneum of the abdominal wall.9 TEP and TAPP are recommended by the new International Guidelines of the Hernia-Surge Group to treat inguinal and femoral hernias.10 A review unveiled that there may be little difference between TAPP and TEP techniques in terms of serious adverse events, hernia recurrence or chronic pain.9 However, other reports have stated the superiority of laparoscopic TEP to TAPP in terms of operative pain11 and hospital stays,12,13 but there is still a lack of sufficient data to prove which laparoscopic TEP and TAPP are more effective. At the same time, hernia repair induces a systemic inflammatory response,14 and it is always the case that surgical treatment causes tissue damage, leading to an increase in oxidative stress.15 In a treatment dilemma, it is crucial to compare different repair methods and minimize inflammation and oxidative stress in patients with IHs. Hence, the aim of this trial was to ascertain the clinical outcomes and safety of TEP and TAPP repair of IHs, as well as the effects on inflammatory factors and oxidative stress-related markers and postoperative recovery, with the aim of providing some data to help clinical patients choose the appropriate surgical method.
Materials and Methods
Ethics Statement
The study complied with the Declaration of Helsinki and was ratified by the ethics committee of Shanxi Bethune Hospital (approval number: 20180127), and patients and their families were informed of the study and signed consent forms.
Study Design and Subjects
We conducted a retrospective cohort study of 88 adult patients with IH who underwent IH repair at Shanxi Bethune Hospital from March 2018 to May 2021, and were divided into the TAPP group (n = 44) and TEP group (n = 44) according to the method of treatment. Patients in the TAPP group underwent laparoscopic TAPP IHR, while those in the TEP group underwent laparoscopic TEP IHR. Data were obtained by reviewing computerized medical records.
Inclusion criteria: ① Patients met the relevant diagnostic criteria in the Guidelines for Diagnosis and Treatment of Adult IHs; ② Patients were over 18 years old; ③ Patients with complete clinical data and surgical indications; ④ Patients with normal cognitive and communication skills.
Exclusion criteria: ① Patients with malignant tumors; ② Patients with severe liver and kidney insufficiency; ③ Patients who could not tolerate surgery; ④ Patients with coagulation dysfunction.
Treatment Methods
Repair surgeries in both groups were performed by the same team of surgeons with more than 5 years of experience in laparoscopic surgery for IH.
All patients in both groups underwent routine examination and fasting 8 h before surgery. All patients under general anesthesia were posed in a trendelenburg position and tilted to the healthy side about 30°. In the TAPP group, an observation hole of about 10 mm was inserted into the umbilicus to establish pneumoperitoneum at 12 mmHg, and a 5 mm operating hole was established at the outer edge of the left and right rectus abdominis, parallel to the umbilicus. The bilateral groin was explored and opened 2 cm above the upper margin of the internal inguinal ring on the affected side. The peritoneum was then separated into the preperitoneal space and fully dissociated. For direct/indirect hernias that did not enter the scrotum, complete separation was performed, otherwise, partial separation was conducted. Polyester non-stapled mesh (10 cm × 15 cm) was trimmed to completely cover the internal inguinal ring and Hesselbach triangle. It was fixed at the pubic tubercle and Poupart’s ligament. In the absence of bleeding, CO2 was discharged, the peritoneum was relocated, and the incision was sutured. In the TEP group, an observation hole of about 10 mm was inserted into the lower umbilical margin to establish pneumoperitoneum at 12 mmHg, and an operating hole of 5 mm was made in the middle lower and middle-upper third of the pubic tubercle and umbilicus. It was separated down the operating hole to the pectineal ligament to fully free Retzius space and Bogros space, inwards to the end of the pubic tubercle, and outwards to the outer edge of the anterior superior iliac spine, so that the spermatic cord, Poupart’s ligament, iliac blood vessels, etc., were completely exposed. The peritoneum on both sides of the spermatic cord was cut and then sutured. The hernia sac was treated in the same way as above. Polyester non-stapled mesh (8 cm × 15 cm) was placed through the observation hole, and the myopectineal orifice was completely covered without fixation. Follow-up procedures were the same as above.
Observation Indices
- Visual Analogue Scale (VAS) was utilized to evaluate patients’ pain at 1, 3, and 7 d after surgery. VAS scale ranged from 0 to 10, with 0 being painless and 10 being severe pain.
- Gastrin (GAS) and motilin (MTL) were assessed by enzyme-linked immunosorbent assay (ELISA) before and 3 days after repair.
- Superoxide dismutase (SOD) and malondialdehyde (MDA) were examined by spectrophotometry and radioimmunoprecipitation, and β-endorphin (β-EP) was evaluated by radioimmunoassay. Total antioxidant capacity (T-AOC) was tested by chemical colorimetry.
- Matrix metalloproteinase (MMP)-2, MMP-9, and tissue inhibitor of metalloproteinases-1 (TIMP-1) were assessed by ELISA kit (Shanghai Shuangying Biotechnology Co., Ltd).
- At the time of discharge, patients’ quality of life was evaluated using the MOS 36-Item Short Form Health Survey (SF-36), which included eight dimensions including physical functioning, role functioning/physical, pain, general health, energy/fatigue, social functioning, role functioning/emotional, and emotional well-being. Each dimension was scored on a percentage scale, and the score was proportional to the quality of life.
- C-reactive protein (CRP), interleukin-6 (IL-6), fibrinogen (FIB), and antitrypsin (al-AT) were examined by immunoturbidimetry.
- Postoperative complications such as urinary retention, scrotal edema, intestinal adhesion, and incision infection were recorded. Patients were followed up for 1 year after surgery and postoperative recurrence was compared between the two groups.
Statistical Methods
Data analysis was conducted with SPSS22.0 software. Measurement data were represented by (x ± s) and compared by t-test. Enumeration data were represented by N, and the χ2 test was performed. P < 0.05 indicated a statistically significant difference.
Results
General Data
A total of 88 patients who received LIHR were included in this study, 44 patients underwent TAPP, and 44 patients underwent TEP. The flow chart for the selection of the study population is shown in Figure 1. No statistically significant differences were found in baseline data such as age, gender, body mass index, disease course, maximum diameter of hernia sac, hernia type, and hernia location between the two groups (P > 0.05, Table 1).
 |
Table 1 General Data |
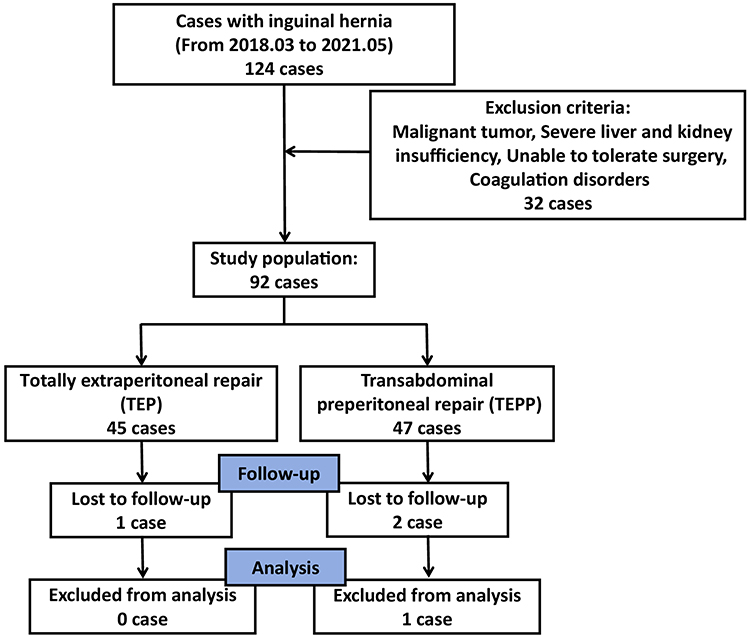 |
Figure 1 The flow chart for the selection of the study population. |
Postoperative VAS Scores
VAS scores of the TEP group at 1 d (4.31 ± 0.33 vs 4.77 ± 0.48), 3 d (2.78 ± 0.23 vs 4.52 ± 0.44), and 7 d (2.39 ± 0.19 vs 4.02 ± 0.37) after repair were lower than those of the TAPP group (P < 0.05).
Clinical Recovery
The operative time, hospital stay, time for postoperative activity out of bed, and time taken to exhaust in the TEP group were shorter and intraoperative blood loss was lower than that in the TAPP group (P < 0.05, Table 2).
 |
Table 2 Comparison of Clinical Conditions |
Oxidative Stress Indices
After repair, MDA and β-EP levels in the two groups were higher and SOD and T-AOC levels were lower than before repair. MDA and β-EP levels in the TEP group were lower, while SOD and T-AOC levels were higher than in the TAPP group (P < 0.05, Table 3).
 |
Table 3 Comparison of Stress Indices |
Inflammatory Factors
Compared with before repair, serum CRP, FIB, alAT, and IL-6 in the two groups were increased after repair, but the increase was more markedly in the TAPP group (P < 0.05, Table 4).
 |
Table 4 Comparison of Inflammatory Factors |
Intestinal Dynamics Recovery Indices and MMP-2, MMP-9, and TIMP-1 Levels
After surgery, GAS and MTL were higher in the TEP group than in the TAPP group (P < 0.05). Compared with the preoperative period, MMP-2, MMP-9, and TIMP-1 reduced after surgery, and the levels of MMP-2, MMP-9, and TIMP-1 in the TEP group were lower than those in the TAPP group (P < 0.05, Table 5).
 |
Table 5 Comparison of Intestinal Motility Recovery Indices and Levels of MMP-2, MMP-9 and TIMP-1 |
Quality of Life
Before repair, there were no significant differences in the scores of physical functioning, role functioning/physical, pain, general health, energy/fatigue, social functioning, role functioning/emotional, and emotional well-being between the TEP group and TAPP group (P > 0.05). After repair, scores of all these aspects in the TEP group and TAPP group were increased. Scores of the TEP group were higher than those of the TAPP group (P < 0.05, Table 6).
 |
Table 6 Comparison of Quality of Life Scores |
Complications and Recurrence
The incidence of postoperative complications in the TAPP group (15.91%) was higher than that in the TEP group (4.55%), indicating no statistical significance (P > 0.05). Postoperative recurrence occurred in 1 case in the TAPP group due to postoperative hematoma and mesh dislocation and 0 case in the TEP group, with no significant difference in recurrence rate (P > 0.05, Table 7).
 |
Table 7 Comparison of complications and recurrence |
Discussion
Laparoscopic TEP and TAPP have been trained in patient cases with IHs which show different efficacy and clinical outcomes. With this regard, this trial was performed to compare inflammation, oxidative stress, and recovery of IH patients undergoing TEP and TAPP.
This trial displayed that the VAS scores of the TEP group were lower than those of the TAPP group at 1 d, 3 d, and 7 d after repair. Besides, this trial also evaluated postoperative recovery and ultimately found that patients who received TEP had shorter operative time, hospitalization time, time for postoperative activity out of bed, and time to exhaustion, as well as less surgical bleeding. Furthermore, in this trial, the levels of oxidative stress indicators MDA and β-EP in the postoperative TEP group were lower than those in the TAPP group, while the levels of SOD and T-AOC were higher than those in the TAPP group; serum inflammatory factors CRP, FIB, alAT, and IL-6 were elevated in both groups of patients after restoration, but in the TEP group was lower than in the TAPP group; postoperatively, GAS and MTL were higher in the TEP group than in the TAPP group, and the levels of MMP-2, MMP-9, and TIMP-1 were lower in the TEP group than in the TAPP group; the scores of quality of life were higher in the TEP group than in the TAPP group, but the insignificant differences between the two groups in terms of the complications and recurrence of IHs repair were uncovered. The above manifests that compared with TAPP, the TEP repair may be more advantageous in reducing postoperative pain, helping patients return to normal activities earlier, causing less oxidative stress and inflammatory response, improving gastric motility and quality of life, and inhibiting MMP-2, MMP-9, and TIMP-1 more significantly. These results may be related to the fact that TEP surgery does not enter the abdominal cavity and is less traumatic to the abdominal wall.
It has been indicated that TEP repair can reduce secondary outcomes including chronic inguinal pain in patients with IHs compared to TAPP repair.11 A systematic review and meta-analysis have concluded that both TAPP and TEP repairs facilitate early return to activities and reduce hematoma in IH patients,16 and that patients with unilateral IH who underwent TEP repair had less postoperative pain and shorter operative time compared with those who underwent TAPP repair.13 It is well-identified that hernia repair causes systemic inflammatory response characterized by increased CRP, IL-6, FIB and al-AT,14 and TEP is associated with less high sensitivity CRP and IL-6 versus Lichtenstein repair.17,18 Further, TEP has been tested to manage oxidative stress in IH repair.15 The interaction between TIMPs and MMPs acts by forming a transmembrane complex, leading to the activation and degradation of extracellular matrix components and contributing to the onset of IHs.19 In this trial, TEP and TAPP suppressed MMP-2, MMP-9, and TIMP-1 levels, with TEP showing a greater inhibition effect. Furthermore, TEP and TAPP improved quality of life and shared no significance in complications and recurrence in IH repair. Similarly, a prospective and randomized report has discovered the improvement in quality of life in IH repair by TEP and TAPP, but the two methods result in no difference in postoperative quality of life.20 This is may due to the different population sizes. Other reports have found no difference in postoperative complications and recurrence between the choice of TEP and TAPP in bilateral IH repair.21,22 The above are similar to the results of this study.
Surgical treatment is always associated with tissue damage and subsequent oxidative stress. One investigation displayed that undergoing either Lichtenstein tension-free hernioplasty (LH) or laparoscopic preperitoneal hernia (LPPH) repair results in a significant increase in oxidative stress markers; nevertheless, the oxidative stress concerned with LH is greater than that associated with LPPH repair.23 One study compared oxidative stress in patients with IH treated with multi-incision laparoscopic TEP or single-incision laparoscopic TEP (TEP-SI) surgery. The results unveiled that the level of oxidative stress is lower in patients surgically treated with the TEP-SI technique than with TEP. TEP-SI can be considered a less invasive technique with less tissue damage.15 However, to our knowledge, there are no published studies comparing the efficacy of TEP and TAPP repair of IHs in terms of inflammation and oxidative stress, which supports the innovative nature and strength of the study. In addition, laparoscopic surgery has the significant advantages of being less invasive, quicker recovery, providing the surgeon with a good surgical field of view, and having fewer complications and lower recurrence rates. Accordingly, this study probes the effects of laparoscopic TEP and TAPP on the relevant indices of IH patients with certain research advantages, and provides certain data to help clinical patients choose the appropriate surgical method. Whereas, there may be patient selection bias during the study, for example, patients with milder disease, younger age, and better economic conditions may be more inclined to choose laparoscopic surgery, which may lead to a certain bias in the results of the study; in addition, some studies may be difficult to comprehensively assess the long-term effects of laparoscopic surgery due to the short follow-up time. Meanwhile, laparoscopic surgery is technically demanding for surgeons and requires a long learning curve and extensive clinical experience, which limits the popularity of laparoscopic surgery to some extent; this study did not perform sample size calculations and was only a small-sample, single-center, retrospective cohort study. These are limitations of this study, and we will expand the sample size and conduct a multicenter, prospective, randomized controlled trial when subsequent conditions permit.
Conclusion
In summary, this trial evaluated two laparoscopic methods in IH repair and discovered that TEP is more advantageous than TAPP repair in reducing inflammatory factor levels, attenuating oxidative stress, and promoting postoperative recovery. The data collected from this trial provide informative support to select an appropriate laparoscopic approach to repair IHs to a certain extent. Nevertheless, there are still some challenges to overcome in this field of research. More high-quality studies are needed in the future to further validate and refine the findings.
Ethics approval and consent to participate
The study complied with the Declaration of Helsinki and was ratified by the ethics committee of Shanxi Bethune Hospital (approval number: 20180127), and patients and their families were informed of the study and signed consent forms.
Acknowledgment
We thank the associate editor and the reviewers for their useful feedback that improved this paper.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no competing interests in this work.
References
1. Shakil A, Aparicio K, Barta E, Munez K. Inguinal Hernias: Diagnosis and Management. Am Family Phys. 2020;102(8):487–492.
2. Vacca VM Jr. Inguinal hernia: a battle of the bulge. Nursing. 2017;47(8):28–35. doi:10.1097/01.NURSE.0000521020.84767.54
3. Inguinal (Groin) Hernias. Am Family Phys. 2020;102(8).
4. Huerta S. The gold-standard technique for inguinal hernia repair is the open approach. Hernia. 2020;24(5):1125–1126. doi:10.1007/s10029-019-01997-7
5. Haladu N, Alabi A, Brazzelli M, et al. Open versus laparoscopic repair of inguinal hernia: an overview of systematic reviews of randomised controlled trials. Surg Endosc. 2022;36(7):4685–4700. doi:10.1007/s00464-022-09161-6
6. Furtado M, Claus CMP, Cavazzola LT, Malcher F, Bakonyi-Neto A, Saad-Hossne R. Systemization of Laparoscopic Inguinal Hernia Repair (Tapp) Based on a New Anatomical Concept: inverted Y and Five Triangles. Arquivos brasileiros de cirurgia digestiva. 2019;32(1):e1426. doi:10.1590/0102-672020180001e1426
7. Esposito C, Escolino M, Turra F, et al. Current concepts in the management of inguinal hernia and hydrocele in pediatric patients in laparoscopic era. Semi Pediatric Surg. 2016;25(4):232–240. doi:10.1053/j.sempedsurg.2016.05.006
8. Abbas AE, Abd Ellatif ME, Noaman N, et al. Patient-perspective quality of life after laparoscopic and open hernia repair: a controlled randomized trial. Surg Endosc. 2012;26(9):2465–2470. doi:10.1007/s00464-012-2212-9
9. Andresen K, Rosenberg J. Transabdominal pre-peritoneal (TAPP) versus totally extraperitoneal (TEP) laparoscopic techniques for inguinal hernia repair. Cochrane Database Syst Rev. 2024;7(7):CD004703. doi:10.1002/14651858.CD004703.pub3
10. Kockerling F, Simons MP. Current Concepts of Inguinal Hernia Repair. Visceral Medicine Apr. 2018;34(2):145–150. doi:10.1159/000487278
11. Varcus F, Duta C, Dobrescu A, Lazar F, Papurica M, Tarta C. Laparoscopic Repair of Inguinal Hernia TEP versus TAPP. Chirurgia. 2016;111(4):308–312.
12. Bracale U, Melillo P, Pignata G, et al. Which is the best laparoscopic approach for inguinal hernia repair: TEP or TAPP? A systematic review of the literature with a network meta-analysis. Surg Endosc. 2012;26(12):3355–3366. doi:10.1007/s00464-012-2382-5
13. Goksoy B, Yilmaz G, Azamat IF, Ozata IH, Duman K. Laparoscopic Inguinal Hernia Repair-TAPP versus TEP: results of 301 Consecutive Patients. Surgi tech int. 2021;39:191–195. doi:10.52198/21.STI.39.HR1427
14. Kokotovic D, Burcharth J, Helgstrand F, Gogenur I. Systemic inflammatory response after hernia repair: a systematic review. Langenbecks Arch Surg. 2017;402(7):1023–1037. doi:10.1007/s00423-017-1618-1
15. Bialecki JT, Myszka W, Wysocka E, et al. A comparison of the oxidative stress response in single-incision laparoscopic versus multi-trocar laparoscopic totally extraperitoneal inguinal hernia repair. Wideochirurgia inne techniki maloinwazyjne. 2020;15(4):567–573. doi:10.5114/wiitm.2020.93202
16. Aiolfi A, Cavalli M, Ferraro SD, et al. Treatment of Inguinal Hernia: systematic Review and Updated Network Meta-analysis of Randomized Controlled Trials. Ann Surg. 2021;274(6):954–961. doi:10.1097/SLA.0000000000004735
17. Vats M, Pandey D, Saha S, et al. Assessment of systemic inflammatory response after total extraperitoneal repair and Lichtenstein repair for inguinal hernia. Hernia. 2017;21(1):65–71. doi:10.1007/s10029-016-1543-1
18. Yigit B, Liman RK, Agackiran I, Citgez B. Comparison of Early Postoperative Outcomes Between Totally Extraperitoneal and Lichtenstein Repair of Inguinal Hernia: a Prospective Randomized Study. J Laparoendoscopic Adv Surg Tech Part A. 2023. doi:10.1089/lap.2023.0199
19. Bracale U, Peltrini R, Iacone B, et al. A Systematic Review on the Role of Matrix Metalloproteinases in the Pathogenesis of Inguinal Hernias. Biomolecules. 2023;13(7). doi:10.3390/biom13071123
20. Bansal VK, Misra MC, Babu D, et al. A prospective, randomized comparison of long-term outcomes: chronic groin pain and quality of life following totally extraperitoneal (TEP) and transabdominal preperitoneal (TAPP) laparoscopic inguinal hernia repair. Surg Endosc. 2013;27(7):2373–2382. doi:10.1007/s00464-013-2797-7
21. Hidalgo NJ, Guillaumes S, Bachero I, et al. Bilateral inguinal hernia repair by laparoscopic totally extraperitoneal (TEP) vs. laparoscopic transabdominal preperitoneal (TAPP). BMC Surgery. 2023;23(1):270. doi:10.1186/s12893-023-02177-2
22. Ortenzi M, Williams S, Solanki N, Guerrieri M, Haji A. Laparoscopic repair of inguinal hernia: retrospective comparison of TEP and TAPP procedures in a tertiary referral center. Minerva chirurgica. 2020;75(5):279–285. doi:10.23736/S0026-4733.20.08518-1
23. Polat C, Kahraman A, Yilmaz S, et al. A comparison of the oxidative stress response and antioxidant capacity of open and laparoscopic hernia repairs. J Laparoendoscopic Adv Surg Tech Part A. 2003;13(3):167–173. doi:10.1089/109264203766207681
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.