")
Back to Journals » Journal of Inflammation Research » Volume 18
Effect of Neutrophil Elastase Inhibitor (Sivelestat Sodium) on Oxygenation in Patients with Sepsis-Induced Acute Respiratory Distress Syndrome
Authors Wu T, Wang T, Jiang J, Tang Y, Zhang L, Jiang Z, Liu F, Kong G, Zhou T, Liu R, Guo H, Xiao J, Sun W, Li Y, Zhu Y, Liu Q, Xie W, Qu Y , Wang X
Received 25 November 2024
Accepted for publication 4 March 2025
Published 27 March 2025 Volume 2025:18 Pages 4449—4458
DOI https://doi.org/10.2147/JIR.S506549
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Tiejun Wu,1,* Tao Wang,2,* Jinjiao Jiang,3 Yue Tang,3 Lina Zhang,1 Zhiming Jiang,4 Fen Liu,4 Guiqing Kong,2 Tingfa Zhou,5 Ruijin Liu,5 Haipeng Guo,6 Jie Xiao,6 Wenqing Sun,7 Yuye Li,7 Yingying Zhu,8 Quan Liu,8 Weifeng Xie,9 Yan Qu,9 Xiaozhi Wang2
1Department of Critical Care Medicine, Liaocheng People’s Hospital, Liaocheng, 252004, People’s Republic of China; 2Department of Intensive Care unit, Binzhou Medical University Hospital, Binzhou, 256699, People’s Republic of China; 3Department of Critical Care Medicine, Provincial Hospital of Shandong First Medical University, Jinan, 250021, People’s Republic of China; 4Department of Critical Care Medicine, The First Affiliated Hospital of Shandong First Medical University, Jinan, 250013, People’s Republic of China; 5Department of Critical Care Medicine, Linyi People’s Hospital, Linyi, 276034, People’s Republic of China; 6Department of Critical Care Medicine, Qilu Hospital of Shandong University, Jinan, 250012, People’s Republic of China; 7Department of Respiratory Intensive Care Unit, Shandong Public Health Clinical Centre, Jinan, 250102, People’s Republic of China; 8Department of Critical Care Medicine, Tai’an Central Hospital, Taian, 271002, People’s Republic of China; 9Department of Critical Care Medicine, Qingdao Municipal Hospital, Qingdao, 266071, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaozhi Wang; Tiejun Wu, Email [email protected]; [email protected]
Objective: Neutrophil elastase (NE) plays an important role in the development of acute respiratory distress syndrome (ARDS). Sivelestat sodium, as a selective NE inhibitor, may improve the outcomes of patients with sepsis-induced ARDS in previous studies, but there is a lack of solid evidence. This trial aimed to evaluate the effect of sivelestat sodium on oxygenation in patients with sepsis-induced ARDS.
Methods: We conducted a multicenter, double-blind, randomized, placebo-controlled trial enrolling patients diagnosed with sepsis-induced ARDS admitted within 48 hours of the advent of symptoms. Patients were randomized in a 1:1 fashion to sivelestat or placebo. Trial drugs were administered as a 24-hour continuous intravenous infusion, for a minimum duration of 5 days and a maximum duration of 14 days. The primary outcome was the proportion of PaO2/FiO2 ratio improvement on Day 5 after randomization, defined by a greater than 50% improvement in PaO2/FiO2 compared with that on ICU admission or PaO2/FiO2 reached over 300 mmHg on Day 5.
Results: The study was stopped midway due to a potential between-group difference in mortality observed during the interim analysis. Overall, a total of 70 patients were randomized, of whom 34 were assigned to receive sivelestat sodium and 36 placebo. On day 5, 19/34 (55.9%) patients in the sivelestat group had PaO2/FiO2 ratio improvement compared with 7/36 (19.4%) patients in the placebo group (risk difference, 0.36; 95% CI, 0.14 to 0.56, p< 0.001). The Kaplan–Meier curves showed a significantly improved 28-day survival rate in patients receiving sivelestat than those not (hazard ratio, 0.32; 95% CI, 0.11 to 0.95; p=0.041).
Conclusion: In patients with sepsis-induced ARDS, sivelestat sodium could improve oxygenation within the first five days and may be associated with decreased 28-day mortality.
Keywords: sepsis, acute respiratory distress syndrome, neutrophil elastase, sivelestat, oxygenation
Introduction
Sepsis is an aberrant immune response to an infection and a syndrome characterized by organ dysfunction.1 Lung injury is common in sepsis, and acute respiratory distress syndrome (ARDS) is a devastating complication of sepsis.2 Sepsis is the leading cause of ARDS, accounting for approximately 75% of patients with ARDS,3 and the outcomes of patients with sepsis-induced ARDs are worse than those with ARDS from other causes.4,5 However, therapies to prevent or treat sepsis-induced ARDS remain elusive.2
During the pathogenesis of sepsis-induced ARDS, multiple circulating immune cells are activated, and inflammatory mediators are massively released into the circulation, which leads to capillary endothelium injury in the lungs.6,7 Following lung injury, immune cells such as neutrophils are recruited to the alveolar space and release large amounts of toxic mediators, including neutrophil elastase (NE).8,9 Previous studies found that systemic inflammatory response syndrome (SIRS) patients with high NE levels were prone to developing ARDS,10 and elevated NE activity was also observed in the bronchoalveolar lavage fluid (BALF) of patients with ARDS.11
Sivelestat sodium, a small molecule weight, selective and reversible NE inhibitor, was discovered in 1990s12 and may confer protective effects on pulmonary endothelial injury in sepsis animal models.13–15 Several clinical studies showed that sivelestat sodium could improve oxygenation, ameliorate lung injury, and reduce the duration of mechanical ventilation in patients with sepsis-induced ARDS.16–18 However, no causal relationship can be implicated due to the observational nature. Therefore, we conducted a multi-center, randomized controlled study to evaluate the role of sivelestat sodium on oxygenation in patients with sepsis-induced ARDS.
Materials and Methods
Trial Design and Oversight
We conducted an investigator-initiated, multicenter, double-blind, randomized, placebo-controlled trial in 12 hospitals in China between May 2022 and August 2023. The human research ethics committee at each hospital approved the protocol. Patients or their surrogates provided written informed consent before enrollment. This trial was designed by the authors, who collected and analyzed the data, vouched for the accuracy and completeness of the data and the adherence of the trial to the protocol, wrote and agreed on the submission of the manuscript. Shanghai Huilun (Jiangsu) Pharmaceutical Co., Ltd., supplied the trial drugs but had no role in designing or conducting the trial or analysing the data and did not have access to the data before publication. The trial was registered in the Chinese Clinical Trial Registry (ChiCTR2200056892) before enrollment began. This study is consistent with the Declaration of Helsinki.
Study Population
Patients diagnosed with sepsis aged between 18 and 75 years old and with ARDS admitted to any of the participating sites within 48 hours of sepsis-induced ARDS onset were eligible for inclusion. The diagnosis of sepsis was according to sepsis 3.0 criteria,19 and the diagnosis of ARDS was based on Berlin criteria.20 The inclusion criteria were (1) diagnosed with sepsis-induced ARDS, (2) diagnosed with mild to moderate ARDS, (3) age between 18 to 75 years old, (4) less than 48 hours from ARDS onset, and (5) written informed consent obtained. The exclusion criteria were (1) patients with an PaO2/FiO2 ratio <100 mmHg (PEEP ≥ 5 cm H2O), (2) pregnant or lactating women or women who may be in the midst of pregnancy, (3) diagnosed with neutropenia, (4) patients receiving chemotherapeutic agents or other immunomodulatory drugs or high-dose corticosteroid therapy for more than 5 days, (5) had a history of severe cardiovascular, respiratory, renal, or hepatic diseases, and (6) post-transplant patients, or patients with disseminated intravascular coagulation, end-stage malignancy, mental illness, etc. Detailed inclusion and exclusion criteria were provided in the Supplementary Protocol.
Randomization, Blinding and Interventions
Each eligible participant was assigned randomly from a computer-generated sequence to either the sivelestat sodium or placebo group in a 1:1 ratio, using a block size of 4 stratified by site. The random allocation sequence was generated by a third party independent of the study. Allocation concealment was achieved using blinded medication packs. Participants, data collectors, and investigators assessing outcome data will be blinded to the treatment allocation.
After randomization, treatment administration was started within 1 hour of randomization. Patients were assigned to receive a 24-hour continuous intravenous infusion of sivelestat sodium at a rate of 0.2 mg/kg/h, for a minimum duration of 5 days and a maximum duration of 14 days or a placebo during the same study period. All other treatments were administered at the discretion of the treating clinicians.
Trial Outcomes
The primary outcome was the proportion of PaO2/FiO2 ratio improvement on Day 5 after randomization. PaO2/FiO2 ratio improvement on Day 5 was defined as a greater than 50% improvement in PaO2/FiO2 compared with that on ICU admission or PaO2/FiO2 reached over 300 mmHg on Day 5. Secondary outcomes included PaO2/FiO2 ratio on Day 3, 5, 7 and 28-day mortality, ventilator-free days (28-VFDs) with 28 days, ICU and hospital-free days within 28 days.
Sample Size Estimation
Based on previous studies,16,17 it is estimated that 35% of the study patients in the control group would reach the primary endpoint (oxygenation index improvement on Day 5). We estimated that a sample size of 142 participants (71 per group) could provide 80% power at a two-sided alpha level of 0.05 to detect an absolute 25% elevation in the primary endpoint with the use of sivelestat sodium, allowing for a potential 15% withdrawal. The calculation was implemented using the PASS 11.0 software (PASS, NCSS software, Kaysville, USA). His study employed one planned interim analysis that was conducted by an independent Data and Safety Monitoring Board (DSMB) after the first 70 participants enrolled. The sample-size calculation accounted for two sequential tests with the use of the O’Brien-Fleming spending function (Supplementary Table 1 and Supplementary Figure 1). The DSMB will review the results of the interim analysis and regular safety report. The DSMB will review the safety report every six months. There were two priori stopping rules: a between-group difference in the primary outcome reaching the efficacy or futility boundaries and clear evidence of harm in one trial group over the other as adjudicated by the DSMB (safety concerns).
Statistical Analysis
Continuous data were reported as means and standard deviations (SD) when normally distributed or as medians and interquartile ranges (IQR) when not normally distributed. The normality of continuous variables will be examined using the Shapiro–Wilk test. Categorical data will be expressed as numbers and percentages.
The primary analysis was based on the intention-to-treat (ITT) population, defined as all enrolled patients from the participating sites. We used generalized linear model (GLM) to compare the difference in the primary outcome (the proportion of PaO2/FiO2 ratio improvement on Day 5) between groups. In the GLM model, the proportion of oxygenation index improvement on trial day-5 will be treated as the response variable following a binomial distribution and the sivelestat sodium intervention as a fixed effect, and the identity and log link function will be used. In the adjusted GLM model, we introduced several baseline characteristics (including diabetes, history of covid-19 infection, lung compliance and PaO2/Fio2 ratio) as covariates. However, the above log-binomial and identity-binomial regression model do not converge, and logit link function was used. We analyzed secondary outcomes also using GLM. Risk differences and its 95% confidence interval (CI) were calculated for categorical variables and mean differences (95% CI) for continuous variables. Kaplan–Meier curves were used to compare the 28-day survival curves after randomization. The difference between two-groups was calculated by Log rank test and its hazard ratio (HR), and 95% CIs were calculated by Mantel-Cox regression model.
Four pre-defined subgroup analyses were conducted for the primary endpoint according to (1) age (dichotomized at 50 years old), (2) APACHE II score at enrollment (dichotomized at 15), (3) septic shock at enrollment, and (4) PaO2/FiO2 ratio at enrollment (dichotomized at 200). Adverse event analyses were reported for all the participants who received the study treatment. Analyses were conducted using the R 4.2.3 software. Statistical tests were two-sided, and p values <0.05 were considered statistically significant.
Results
Recruitment and Baseline Characteristics
During the study period, 282 patients with sepsis combined with ARDS were assessed for eligibility, of whom 70 were enrolled in the trial from nine hospitals across China. The trial recruitment was halted by the DSMB after the interim analysis owing to observed between-group difference in mortality and a between-group difference in the primary outcome, and the DSMB requested to unblind the data. After reviewing the unblinded data, the DSMB concluded that the trial should be stopped midway due to the analysis result that sivelestat group showed improved survival and increased incidence of the primary outcome compared with the placebo group, and the trial was then formally stopped. The numbers of cases from each site were shown in online Supplemental Table 2. Among those 70 randomized patients, 34 were assigned to receive sivelestat sodium and 36 placebo. All randomized participants completed follow-up and were included in the primary analysis (Figure 1).
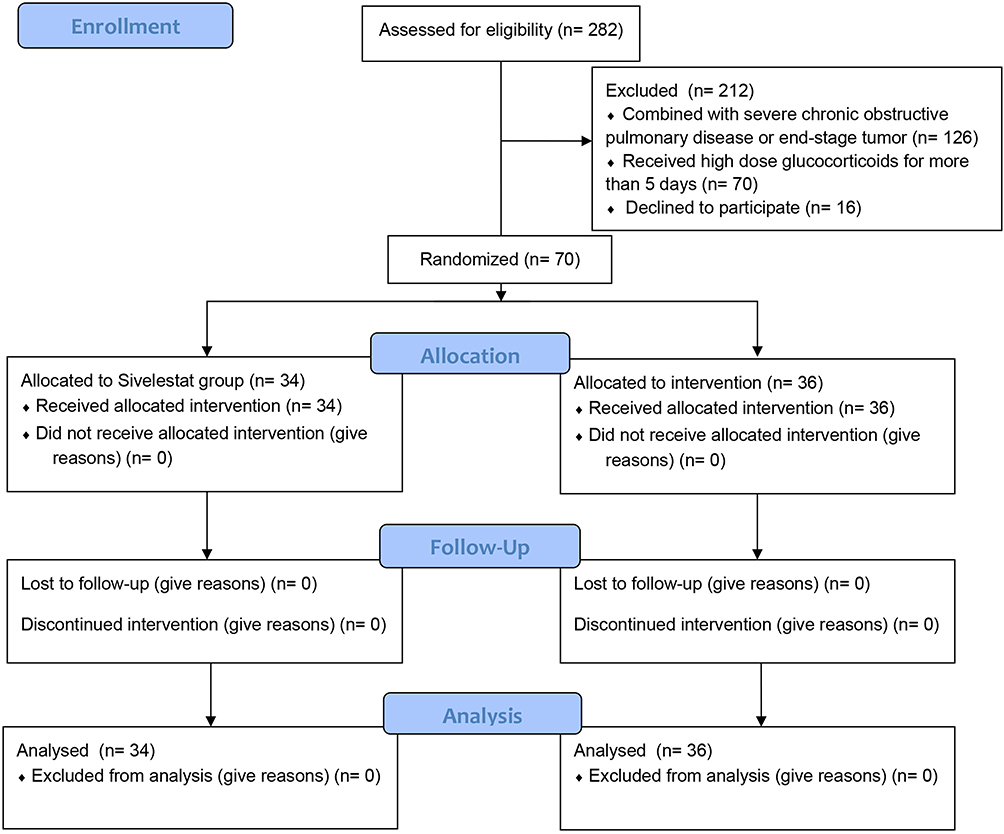 |
Figure 1 Study flowchart. |
The characteristics of the participants at baseline were evenly distributed between the two trial groups (Table 1). The majority of the trial participants required mechanical ventilation (52/70, 74.3%) at admission. The median (IQR) PaO2/FiO2 ratio was 136.0 (104.2–163.0) mmHg in the sivelestat group and 161.0 (144.0–195.0) mmHg in the placebo group.
 |
Table 1 Baseline Characteristics of the Study Subjects |
Primary and Secondary Outcomes
On day 5 after randomization, 19/34 (55.9%) patients in the sivelestat group had PaO2/FiO2 ratio improvement compared with 7/36 (19.4%) patients in the placebo group (risk difference, 0.36; 95% CI, 0.14 to 0.56, p<0.001). In addition, the PaO2/FiO2 ratio constantly differs between groups on day 3, day 5 and day 7 (Table 2).
 |
Table 2 Trial Outcomes |
Patients in the sivelestat group had a median of 21.0 VFDs (IQR, 6.5–24.5) within the first 28 days compared with 20.0 VFDs (IQR, 0–23.0) for those receiving placebo. The mean difference in VFDs between groups was 3.9 days (95% CI, −1.9 to 9.7, p=0.20). No significant difference in cumulative event of weaning from mechanical ventilation between treatment groups was observed (hazard ratio, 1.70; 95% CI, 0.87 to 3.31, p=0.12, Supplementary Figure 2). The 28-day mortality was 3/34 (8.8%) in patients receiving sivelestat and 10/36 (27.8%) in those receiving placebo (risk difference, −0.19; 95% CI, −0.37 to −0.01, p=0.03). The Kaplan–Meier curves showed a significantly improved survival rate in patients receiving sivelestat than those not (HR, 0.32; 95% CI, 0.11 to 0.95; log-rank p=0.041) (Figure 2). The ICU and hospital-free days within 28 days were both comparable between the two groups (Table 2).
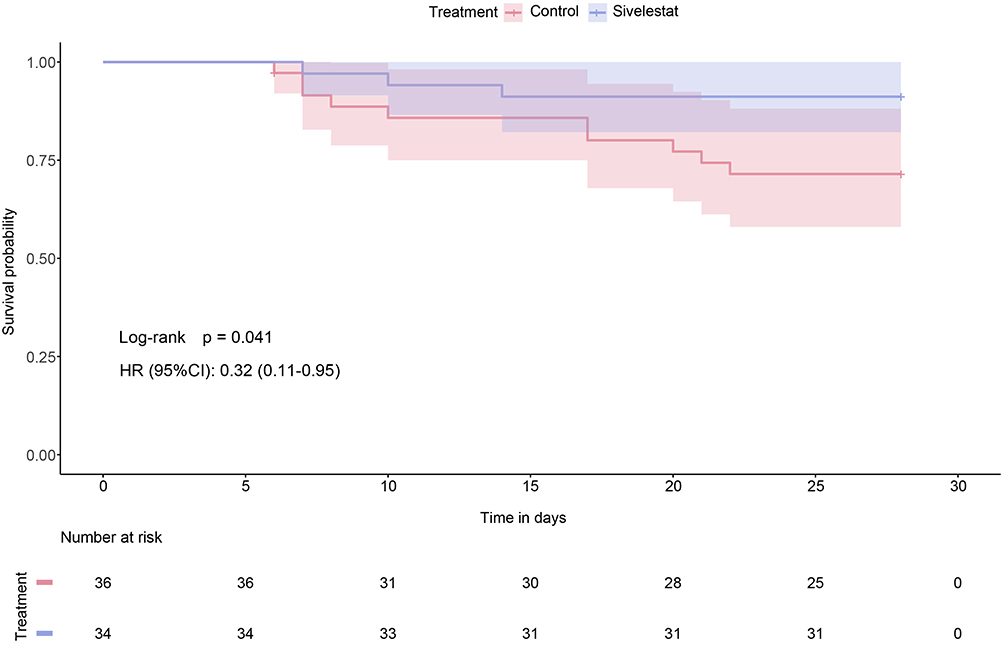 |
Figure 2 Survival curve. Abbreviations: HR, hazard ratio; CI, confidence interval. |
Subgroup Analysis
Subgroup analysis suggested that the treatment effect of sivelestat on the primary outcome had trends toward more significant in patients with APACHE II score <15 (p for interaction = 0.042) (Figure 3).
 |
Figure 3 Subgroup analysis for the primary outcome. Abbreviations: RD, risk difference; CI, confidence interval; APACHE II, Acute Physiology and Chronic Health Evaluation II. |
Adverse Events
The number of adverse events did not differ meaningfully between the trial groups. Details regarding adverse events are provided in Table 2.
Discussion
In this multicenter, double-blind, randomized, placebo-controlled trial, the use of sivelestat sodium could improve oxygenation within the first week in patients with sepsis-induced ARDS. Moreover, it was associated with decreased 28-day mortality, though there is no difference in ventilator-free days or other outcomes. Subgroup analysis showed that age, the baseline respiratory function, disease severity and septic status may affect the efficacy of sivelestat sodium, favouring sivelestat use in patients with APACHE II score <15.
Meta analysis showed that sivelestat can not only reduce the mortality, shorten the mechanical ventilation time, and increase ventilation-free days but also improve the oxygenation in ARDS patients.21 However, two recent large clinical trials demonstrated discordant effects of sivelestat sodium in patients with acute lung injury (ALI).22,23 The Phase III Japanese study by Tamakuma et al included 230 ALI/ARDS patients combined with SIRS, and sivelestat was shown to increase pulmonary function, reduce duration of mechanical ventilation, and shorten ICU stay.22 However, an international multicenter double-blind, placebo-controlled Phase II study (STRIVE study) randomized 492 mechanically ventilated patients with ALI/ARDS,23 and the results showed that sivelestat did not change 28-day mortality or VFDs. Furthermore, a negative trend in the long-term 180-day mortality rate was noted, and the trial was then stopped midway per the recommendation from the DSMB.
The discrepancy between the two studies may be due to differences in the characteristics of study patients, such as age, baseline respiratory function, disease severity, intervention time and septic status. The patients enrolled in the phase III Japanese study had a narrower age distribution and better respiratory function than those in the STRIVE study. In addition, clinical studies reporting positive results with sivelestat therapy had mainly enrolled ARDS patients with a Lung Injury Score <2.5, whereas the majority of the patients in the STRIVE study had a Lung Injury Score >2.5.24,25 A post-hoc analysis of the STRIVE patients involving those who had a mean Lung Injury Score ≤2.5, revealed favourable trends in mortality and VFDs in patients receiving sivelestat.23 On the other hand, it is suggested that the different proportions of septic patients may have contributed to the discordant results among these studies (58% vs 69%). Our results were consistent with the above findings, showing that sivelestat may confer larger treatment effects in patients with sepsis-induced ARDS, especially in patients with APACHE II score <15. Taken together, our study suggests that sivelestat could be effective in patients with mild sepsis-induced ARDS, and may be associated with survival benefits in this popualtion. In addition, the mortality rate in our placebo group was 27.8%, which was in the acceptable range compared with previous studies,26,27 implying the generalizability of our results.
The above results can also be explained from a pathophysiological point of view. Neutrophil activation and NE release are very early biological events in the pathogenesis of ARDS.28 Previous research showed a significant increase in blood NE in patients with sepsis-induced ARDS29 and a decrease in blood NE after sivelestat administration,30,31 suggesting that the therapeutic effect of sivelestat is related to the inhibition of NE. Recent studies have shown that damage to the endothelial glycocalyx is a critical factor in the development and progression of ARDS.32,33 In addition, our preclinical research has shown that sivelestat can reduce endothelial glycocalyx damage by inhibiting the production of neutrophil trapping nets (NETs), improve endothelial cell permeability, attenuate lung histopathological injury and ultimately improve survival in sepsis-induced ALI model mice. Further molecular docking and visualisation analysis showed that sivelestat could bind with high affinity to the key ferroptosis protein glutathione peroxidase (GPX4), increase the expression of GPX4 and thus interfere with the process of ferroptosis.29 Therefore, sivelestat may have pleiotropic effects on ARDS and may not be limited to interfering with NE.
The trial had several limitations. First, our study was stopped prematurely since our interim analysis reached the efficacy boundary, and the results of this study should be interpreted with caution. Second, subjective factors contribute to the decision to wean patients from mechanical ventilation, which may bring bias for the VFDs. The fact that approximately 25% of patients did not receive mechanical ventilation at randomization and the inadequate statistical power may explain the non-significant difference in VFD. Third, laboratory indexes related to inflammatory mediators were not detected in our original trial, precluding us to explore the mechanisms involved. Last, the finding that sivelestat improved survival should also be read with caution due to the possibility of a type II error.
Conclusion
In patients with sepsis-induced ARDS, sivelestat sodium could improve oxygenation within the first week and was associated with decreased 28-day mortality, particularly in patients with less severe disease, including those with APACHE II score <15 or with PaO2/FiO2 ratio ≥200 or without septic shock. Further large-scale RCTs are needed to confirm the effects of sivelestat on mortality in this population. These data also support the conduct of a large confirmatory trial with a hard clinical endpoint.
Participating Centers
(1) Liaocheng People’s Hospital; (2) Affiliated Hospital of Binzhou Medical College; (3) Provincial Hospital of Shandong First Medical University; (4) Qilu Hospital of Shandong University; (5) The First Affiliated Hospital of Shandong First Medical University; (6) Shandong Public Health Clinical Centre; (7) Qingdao Municipal Hospital; (8) Shandong Third Hospital; (9) Tai’an Central Hospital; (10) Linyi People’s Hospital; (11) Affiliated Hospital of Jining Medical College; (12) Shengli Oilfield Central Hospital.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding authors on reasonable request.
Ethics and Approval Statement
The protocol and the informed consent document have been reviewed and approved by the Institutional Ethics Committee of all participating centers. Study investigators will provide potential participants with verbal and written information prior to inclusion in the study. Informed consent will be provided from participants or their authorized representatives. The study was registered in the Clinical Trials Register (ChiCTR2200056892).
Acknowledgment
This paper has been uploaded to ResearchSquare as a preprint: https://www.researchsquare.com/article/rs-4918271/v1.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by Shanghai Huilun (Jiangsu) Pharmaceutical Co., Ltd., which is also responsible for the supply of the study drug and placebo as well as distribution to the participating centers. Funding agency had no input into the design, conduct, data collection, statistical analysis, or writing of the manuscript.
Disclosure
The authors have declared that no competing interest exists.
References
1. Singer M, Deutschman CS, Seymour CW. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
2. Beitler JR, Thompson BT, Baron RM. Advancing precision medicine for acute respiratory distress syndrome. Lancet Respir Med. 2022;10(1):107–120. doi:10.1016/S2213-2600(21)00157-0
3. Bellani G, Laffey JG, Pham T. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA. 2016;315(8):788–800. doi:10.1001/jama.2016.0291
4. Stapleton RD, Wang BM, Hudson LD, Rubenfeld GD, Caldwell ES, Steinberg KP. Causes and timing of death in patients with ARDS. Chest. 2005;128(2):525–532. doi:10.1378/chest.128.2.525
5. Sheu CC, Gong MN, Zhai R, et al. Clinical characteristics and outcomes of sepsis-related vs non-sepsis-related ARDS. Chest. 2010;138(3):559–567. doi:10.1378/chest.09-2933
6. Englert JA, Bobba C, Baron RM. Integrating molecular pathogenesis and clinical translation in sepsis-induced acute respiratory distress syndrome. JCI Insight. 2019;4(2). doi:10.1172/jci.insight.124061
7. Xu H, Sheng S, Luo W, Xu X, Zhang Z. Acute respiratory distress syndrome heterogeneity and the septic ARDS subgroup. Front Immunol. 2023;14:1277161. doi:10.3389/fimmu.2023.1277161
8. Zeiher BG, Matsuoka S, Kawabata K, Repine JE. Neutrophil elastase and acute lung injury: prospects for sivelestat and other neutrophil elastase inhibitors as therapeutics. Crit Care Med. 2002;30(5 Suppl):S281–287. doi:10.1097/00003246-200205001-00018
9. Sahebnasagh A, Saghafi F, Safdari M, et al. Neutrophil elastase inhibitor (sivelestat) may be a promising therapeutic option for management of acute lung injury/acute respiratory distress syndrome or disseminated intravascular coagulation in COVID-19. J Clin Pharm Ther. 2020;45(6):1515–1519. doi:10.1111/jcpt.13251
10. Kodama T, Yukioka H, Kato T, Kato N, Hato F, Kitagawa S. Neutrophil elastase as a predicting factor for development of acute lung injury. Intern Med. 2007;46(11):699–704. doi:10.2169/internalmedicine.46.6182
11. McGuire WW, Spragg RG, Cohen AB, Cochrane CG. Studies on the pathogenesis of the adult respiratory distress syndrome. J Clin Invest. 1982;69(3):543–553. doi:10.1172/JCI110480
12. Kawabata K, Suzuki M, Sugitani M, Imaki K, Toda M, Miyamoto T. ONO-5046, a novel inhibitor of human neutrophil elastase. Biochem Biophys Res Commun. 1991;177(2):814–820. doi:10.1016/0006-291X(91)91862-7
13. Suzuki K, Okada H, Takemura G. Neutrophil Elastase Damages the Pulmonary Endothelial Glycocalyx in Lipopolysaccharide-Induced Experimental Endotoxemia. Am J Pathol. 2019;189(8):1526–1535. doi:10.1016/j.ajpath.2019.05.002
14. Suda K, Takeuchi H, Hagiwara T. Neutrophil elastase inhibitor improves survival of rats with clinically relevant sepsis. Shock. 2010;33(5):526–531. doi:10.1097/SHK.0b013e3181cc064b
15. Hagiwara S, Iwasaka H, Togo K, Noguchi T. A neutrophil elastase inhibitor, sivelestat, reduces lung injury following endotoxin-induced shock in rats by inhibiting HMGB1. Inflammation. 2008;31(4):227–234. doi:10.1007/s10753-008-9069-z
16. Gao X, Zhang R, Lei Z, et al. Efficacy, safety, and pharmacoeconomics of sivelestat sodium in the treatment of septic acute respiratory distress syndrome: a retrospective cohort study. Ann Palliat Med. 2021;10(11):11910–11917. doi:10.21037/apm-21-3164
17. Hayakawa M, Katabami K, Wada T, et al. Sivelestat (selective neutrophil elastase inhibitor) improves the mortality rate of sepsis associated with both acute respiratory distress syndrome and disseminated intravascular coagulation patients. Shock. 2010;33(1):14–18. doi:10.1097/SHK.0b013e3181aa95c4
18. Miyoshi S, Hamada H, Ito R. Usefulness of a selective neutrophil elastase inhibitor, sivelestat, in acute lung injury patients with sepsis. Drug Des Devel Ther. 2013;7:305–316. doi:10.2147/DDDT.S42004
19. Shankar-Hari M, Phillips GS, Levy ML, et al. Developing a New Definition and Assessing New Clinical Criteria for Septic Shock: for the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):775–787. doi:10.1001/jama.2016.0289
20. Thompson BT, Chambers RC, Liu KD. Acute Respiratory Distress Syndrome. N Engl J Med. 2017;377(6):562–572. doi:10.1056/NEJMra1608077
21. Ding Q, Wang Y, Yang C, Tuerxun D, Yu X. Effect of Sivelestat in the Treatment of Acute Lung Injury and Acute Respiratory Distress Syndrome: a Systematic Review and Meta-Analysis. Intensive Care Res. 2023;1–10. doi:10.1007/s44231-023-00032-9
22. Tamakuma S, Ogawa M, Aikawa N, et al. Relationship between neutrophil elastase and acute lung injury in humans. Pulm Pharmacol Ther. 2004;17(5):271–279. doi:10.1016/j.pupt.2004.05.003
23. Zeiher BG, Artigas A, Vincent JL, et al. Neutrophil elastase inhibition in acute lung injury: results of the STRIVE study. Crit Care Med. 2004;32(8):1695–1702. doi:10.1097/01.CCM.0000133332.48386.85
24. Aikawa N, Kawasaki Y. Clinical utility of the neutrophil elastase inhibitor sivelestat for the treatment of acute respiratory distress syndrome. Ther Clin Risk Manag. 2014;10:621–629. doi:10.2147/TCRM.S65066
25. Mohamed MMA, El-Shimy IA, Hadi MA. Neutrophil Elastase Inhibitors: a potential prophylactic treatment option for SARS-CoV-2-induced respiratory complications? Crit Care. 2020;24(1):311. doi:10.1186/s13054-020-03023-0
26. Truwit JD, Bernard GR, Steingrub J. Rosuvastatin for sepsis-associated acute respiratory distress syndrome. New Engl J Med. 2014;370(23):2191–2200. doi:10.1056/NEJMoa1401520
27. Fowler AA, Truwit JD, Hite RD. Effect of Vitamin C Infusion on Organ Failure and Biomarkers of Inflammation and Vascular Injury in Patients With Sepsis and Severe Acute Respiratory Failure: the CITRIS-ALI Randomized Clinical Trial. JAMA. 2019;322(13):1261–1270. doi:10.1001/jama.2019.11825
28. Denning NL, Aziz M, Gurien SD, Wang P. DAMPs and NETs in Sepsis. Front Immunol. 2019;10:2536. doi:10.3389/fimmu.2019.02536
29. Fei Y, Huang X, Ning F, et al. NETs induce ferroptosis of endothelial cells in LPS-ALI through SDC-1/HS and downstream pathways. Biomed Pharmacother. 2024;175:116621. doi:10.1016/j.biopha.2024.116621
30. Matsuzaki K, Hiramatsu Y, Homma S, Sato S, Shigeta O, Sakakibara Y. Sivelestat reduces inflammatory mediators and preserves neutrophil deformability during simulated extracorporeal circulation. Ann Thorac Surg. 2005;80(2):611–617. doi:10.1016/j.athoracsur.2005.02.038
31. T Pan, T Tuoerxun, X Chen, et al. The neutrophil elastase inhibitor, sivelestat, attenuates acute lung injury in patients with cardiopulmonary bypass. Front Immunol. 2023;14:1082830. doi:10.3389/fimmu.2023.1082830
32. Li J, Qi Z, Li D, et al. Alveolar epithelial glycocalyx shedding aggravates the epithelial barrier and disrupts epithelial tight junctions in acute respiratory distress syndrome. Biomed Pharmacother. 2021;133:111026. doi:10.1016/j.biopha.2020.111026
33. Liu XY, Xu HX, Li JK, et al. Neferine Protects Endothelial Glycocalyx via Mitochondrial ROS in Lipopolysaccharide-Induced Acute Respiratory Distress Syndrome. Front Physiol. 2018;9:102. doi:10.3389/fphys.2018.00102
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Role of Cellular Senescence Genes and Immune Infiltration in Sepsis and Sepsis-Induced ARDS Based on Bioinformatics Analysis
Wu XL, Guo YN
Journal of Inflammation Research 2024, 17:9119-9133
Published Date: 19 November 2024
Dynamic Immune Indicator Changes as Predictors of ARDS in ICU Patients with Sepsis: A Retrospective Study

Lu X, Chen Y, Zhang G, Zeng X, Lai L, Qu C
International Journal of General Medicine 2025, 18:1163-1172
Published Date: 1 March 2025