")
Back to Journals » Clinical Ophthalmology » Volume 18
Effect of Simple Myopic Astigmatism and Its Axis on Near Visual Performance for Thai Alphabet in Pseudophakic Eyes
Authors Pakviwat P, Moollaong C, Borvonshivabhumi S, Roongpoovapatr V
Received 25 September 2024
Accepted for publication 13 December 2024
Published 17 December 2024 Volume 2024:18 Pages 3815—3823
DOI https://doi.org/10.2147/OPTH.S485353
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Pakpum Pakviwat, Chureeporn Moollaong, Sasinut Borvonshivabhumi, Vatookarn Roongpoovapatr
Department of Ophthalmology, Mettapracharak (Wat Rai Khing) Hospital, Nakhon Pathom, Thailand
Correspondence: Pakpum Pakviwat, Department of Ophthalmology, Mettapracharak (Wat Rai Khing) Hospital, 52 Moo 2 Rai Khing District Sampran, Nakhon Pathom, 73210, Thailand, Email [email protected]
Background: Refractive target of low simple myopic astigmatism allows increased depth-of-focus and near visual performance in monofocal intraocular lens (IOL) implants. This study investigated the effect of astigmatism and its axis on distance and near visual acuity (VA), and near visual performance for the Thai alphabet using the Thai MNREAD chart.
Design: Investigational simulation.
Methods: Distance (6.0 m) VA, near (40 cm) VA and near visual performance (maximum reading speed [MRS], threshold print size [TPS] and reading acuity [RA]), were assessed by the Thai MNREAD chart monocularly in 31 pseudophakic eyes (62.8 ± 8.55 years). Six refractive conditions were simulated using trial lenses: ± 0.00 DS [in-focus at distance], +1.00 × 90 [ATR (Against-the-Rule)], +2.00 × 90 [ATR], +1.00 × 180 [WTR (With-the-Rule)], +2.00 × 180 [WTR], and +3.00 DS [in-focus at near].
Results: Distance VA was degraded by spherical and astigmatic defocus compared with +0.00 DS [in-focus (distance)] (p < 0.001). No significant difference in distance VA was found between ATR and WTR astigmatism at the same magnitude. Near VA was better with +3.00 DS (p-value < 0.001) compared with other refractive conditions. Near visual performance (threshold print size [TPS]) was significantly better in ATR compared with WTR astigmatism (p < 0.001 for both +1.00 DC and 2.00 DC).
Conclusion: Low simple myopic astigmatism improved near visual performance in monofocal IOL implants at the expense of degradation of distance VA. ATR astigmatism provided better TPS than WTR astigmatism. This benefit of ATR over WTR astigmatism on reading performance on the Thai alphabet confirmed the role of axis orientation on near visual performance.
Keywords: low simple myopic astigmatism, monofocal intraocular lens(IOL), IOL, near visual performance, Thai MNREAD chart(Minnesota low vision reading chart), Minnesota low vision reading chart, against-the-rule astigmatism, ATR, distance visual acuity(VA), VA
Cataract extraction with intraocular lens (IOL) implantation is one of the most beneficial procedures in ophthalmology. Refraction best for distance visual outcome is commonly preferred as an endpoint. However, post-cataract removal, near visual performance is reduced due to loss of accommodative mechanism.1 Multifocal and extended depth of focus (EDOF) as alternatives to monofocal IOLs may be an option to improve depth of focus as well as near visual performance, however most patients, especially in developing countries, cannot afford these premium IOLs.
Depth of focus and near visual performance in pseudophakia with monofocal IOLs can be improved by many factors such as pupil size, corneal multifocality, anterior chamber depth, axial length, age and post-operative astigmatism (simple myopic astigmatism).2–5 A study in 20156 showed that over one-third of cataract patients had more than 1.00 D of corneal astigmatism. Improvements in near vision due to non-accommodative optical factors are known as pseudoaccommodative effects. Such factors may include astigmatism, which can be tailored at the time of surgery cataract,7 while others may be unpredictable or difficult to modify.
Huber4 proposed an optical explanation that attributing pseudoaccommodation to simple myopic astigmatism, the weaker the meridian forming an image for distance and the stronger the meridian forming an image for near, both within the conoid of Sturm as illustrated in Figure 1. Trindade et al8 suggested that low, simple myopic ATR (Against-The-Rule) astigmatism in pseudophakic eyes may improve uncorrected near visual acuity at the expense of distance visual acuity, while Bradbury et al9 proposed simple myopic WTR (With-The-Rule) astigmatism up to 2.0 DC as a refraction goal to allow adequate uncorrected distance and near visual acuity.10–12
 |
Figure 1 Pseudoaccommodative effect from low simple myopic astigmatism. The figure illustrates how the weaker Meridian forms an image for distance and the stronger meridian for near, both within the conoid of Sturm. |
Astigmatism is a refractive error that exists when the surfaces of the cornea or crystalline lens have more than one curvature in a different meridian. After cataract surgery, most astigmatism derives from the cornea. Regular astigmatism can be classified into three types based on the axis of the steepest meridian13,14 (With-the-rule (WTR) astigmatism, Against-the-rule (ATR) astigmatism and Oblique astigmatism).
Furthermore, regular astigmatism can be classified based on two different focal points of the retina (Simple myopic astigmatism, Simple hyperopic astigmatism, Compound myopic astigmatism, Compound hyperopic astigmatism, Mixed astigmatism).
Astigmatism produces meridional variations in the retinal blur pattern and alter visual performance as the axis changes. In 2018, Serra et al15 found that the astigmatic axis influences letter discrimination and that this effect depends on the alphabet in use, suggesting that the effect of astigmatism on visual performance using each language alphabet should be assessed.
This study assessed distance and near visual performance for the Thai alphabets in pseudophakic eyes with optically induced spherical and astigmatic defocus with different magnitudes and axes to determine the effects of astigmatism in promoting pseudoaccommodation of reading tasks in the Thai alphabet using the Thai MNREAD (Minnesota low vision reading) chart.
Methods
Patients who attended a tertiary eye care hospital (Mettapracharak Hospital (Wat Rai Khing), Thailand) for cataract surgery with monofocal IOL implantation were invited to volunteer at their 1-month follow-up visit. Selection was based on the following inclusion criteria: ability to read the Thai alphabet and willingness to enroll in the study. Exclusion criteria were as follows: presence of other ocular pathologies affecting visual performance, post-operative complications, post-operative astigmatism greater than 3.00 DC, and post-operative best corrected distance visual acuity (BCVA) worse than 0.2 logMAR (20/32).
Thirty-one participants (male n = 14, female n = 17) with a mean age of 62.8 ± 8.55 years (range 37–79) were enrolled in the study. Slit-lamp examination, autorefraction, and subjective refraction were performed on both eyes. In cases of bilateral surgery, the eye with better distance VA was selected for testing.
All participants were fully informed about the study’s purpose, procedures, potential risks, and benefits, and written informed consent was obtained prior to their participation in the study. The study adhered to the tenets of the Declaration of Helsinki, and the study protocol was approved by the Ethics Committee of Mettapracharak Hospital.
In this study, the independent variable was the refractive condition, and outcome measures included distance, near visual acuity, and near reading performance.
Refractive Conditions
Six refractive conditions were simulated by placing an ophthalmic lens in front of the subjective refractive correction, mounted on a trial frame.
±0.00 DS [in-focus at distance]
+1.00 x 90× 90DC [ATR simple myopic astigmatism]
+2.00 x 90× 90DC [ATR simple myopic astigmatism]
+1.00 x 180× 180DC [WTR simple myopic astigmatism]
+2.00 x 180× 180DC [WTR simple myopic astigmatism]
+3.00 DS [in-focus at near]
The refractive condition test order was randomized by a computer (using Microsoft Excel 2019).
All refractive conditions were assessed for distance (6.0 m) and near (0.4 m) visual acuity using Snellen chart and Rosenbaum near vision card (Near chart), respectively.
There are 2 minutes break between measurements to avoid fatigue.
Reading Performance
The Thai versions of the MNREAD charts (Minnesota low-vision reading test) were used to assess reading performance at near. The charts consist of a series of 60-character Thai alphabet sentences displayed on three lines. The letters decrease in size by 0.1 log unit, starting with 1.3 logMAR (equivalent to 20/400, viewed at 40 cm, held by examiner). Three different types of charts (different sentences each) were used to assess each refractive condition in a randomized sequence.
The MNREAD charts were presented in descending print size order starting with the largest (1.3 logMAR). Participants were instructed to read the sentences out loud as fast as possible, without stopping to correct any mistakes. The test continued with increasingly smaller letters until no more words could be read. Time taken to read and numbers of errors for each sentences were recorded. Paragraph reading speed (words per minutes, WPM) was defined as the number of words read correctly (total number of words minus errors) divided by the time taken (reading speed = 600/time in seconds). An MNREAD curve of reading speed versus printing size was plotted to extract three parameters. Reading speed is similar across a range of large print sizes, forming a plateau that represents the maximum reading speed (MRS, wpm). As print size decreased, a threshold print size (TPS, logMAR) was reached at which reading speed started to decline rapidly, or defined as the print size yielding 80% of the MRS.16 The smallest print size participants could read was defined as the reading acuity (RA, logMAR), and was corrected by 0.01 logMAR for each error made.
For all tests, the illumination level was maintained between 400 and 600 lux for the near reading performance.17
The protocol of this study was approved by the Ethics Committee of Mettapracharak hospital and adhered to the principles outlined in the Declaration of Helsinki.
Statistical Analysis
Sample size was calculated with 2 independent populations means for non-inferiority or superiority study method by n4Studies application based on the previous studies.
The normality of data distribution was evaluated using the Shapiro–Wilk test. One-way repeated measures analysis of variance (ANOVA) was applied to analyze VA and reading performance parameters. Bonferroni corrected post-hoc multiple comparisons between refractive conditions were used and were corrected. Statistical analysis was performed using SPSS (SPSS 26.0, IBM Corp., New York, USA).
Results
Distance Visual Acuity
Every defocus condition statistically reduced visual acuity at a distant view of 6.0 m, with the exception of +1.00 × 180 DC WTR astigmatism, which showed the least reduction of 0.11 ± 0.09 logMAR (p = 0.075). Contrarily, +1.00 × 90 DC ATR astigmatism resulted in a statistically significant 0.17± 0.11 logMAR drop in VA (p = 0.005). Higher magnitude of astigmatism significantly further reduced distance VA. There were no statistically significant differences between ATR and WTR astigmatism in distance VA when compared at the same magnitude (Figure 2a).
 |
Figure 2 The distance visual acuity between each refractive conditions. (ǂ p-value < 0.05, Bonferroni correction, calculated from ANOVA) in (a). The near visual acuity between each refractive conditions. (ǂ p-value < 0.05, Bonferroni correction, calculated from ANOVA) in (b). |
Near Visual Acuity
Near visual acuity was poorest in ±0.00 DS, marginally improved to +1.00 × 90 DC ATR (p = 0.058), +1.00 × 180 DC WTR astigmatism (p = 0.39) and statistically significantly improved to +2.00 × 90 ATR and +2.00 × 180 WTR astigmatism by 0.20 ± 0.11 logMAR (p < 0.001), and 0.14 ± 0.11 logMAR (p < 0.001), respectively. The best result was found in the in-focus (at near) +3.00 DS condition (improved near VA by 0.35 ± 0.11 logMAR) (p < 0.001). No statistically significant difference in near visual acuity was found between ATR and WTR astigmatism at the same magnitude (Figure 2b).
Reading Performance
Maximum reading speed (MRS) showed little variation between types of refraction. In-focus (near) +3.00 DS was approximately seven wpm faster than ±0.00 DS, with no statistically significant differences (Figure 3a).
 |
Figure 3 The pairwise comparisons of reading performance (MRS) depending on the type of refractive condition used was presented (ǂ p-value < 0.05, Bonferroni correction, calculated from ANOVA) in (a). The pairwise comparisons of reading performance (TPS) depending on the type of refractive condition used was presented (ǂ p-value < 0.05, Bonferroni correction, calculated from ANOVA) in (b) The pairwise comparisons of reading performance (RA) depending on the type of refractive condition used was presented (ǂ p-value < 0.05, Bonferroni correction, calculated from ANOVA) in (c). |
Threshold print size (TPS) differed between all refractive conditions compared with ±0.00 DS except for +1.00 × 180 DC WTR astigmatism (0.06 ± 0.10 logMAR). The benefit of an increase in the magnitude of astigmatism from 1.00 DC to 2.00 DC was not statistically significant in both ATR and WTR astigmatism conditions. The benefit of ATR over WTR was observed in +1.00 DC × 90 ATR compared to +1.00 DC × 180 WTR (improved by 0.17 ± 0.04 (p < 0.001)) and also in +2.00 DC × 90 ATR compared to +2.00 DC × 180 WTR (improved by 0.14 ± 0.04 (p < 0.001)). The +3.00 DS condition provided the greatest improvement in TPS compared with ±0.00 DS (0.38 ± 0.10 logMAR) (p < 0.001) (Figure 3b).
Reading acuity (RA) also significantly improved in all refractive conditions compared with ±0.00 DS except for +1.00 × 180 DC WTR. The +1.00 × 90 DC ATR astigmatism condition improved RA by 0.17 ± 0.13 logMAR(p=0.001), while the +1.00 × 180 DC WTR showed no significant improvement. Unlike TPS, no advantage of ATR over WTR astigmatism was demonstrated at the same magnitude. The +3.00 DS condition provided the best RA compared to all conditions, similar to results of near visual acuity (Figure 3c).
All parameters are shown in Table 1
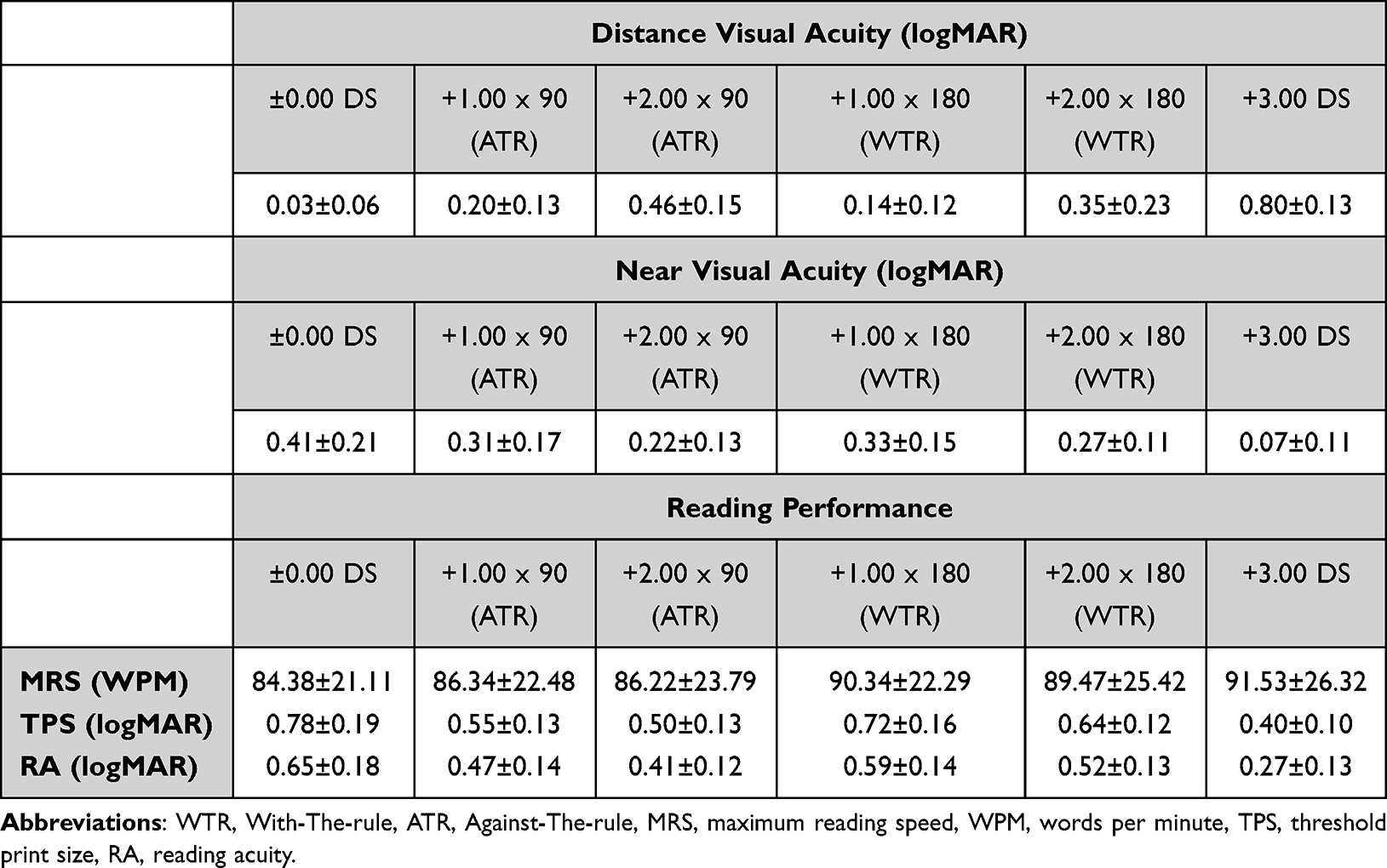 |
Table 1 Distance Visual Acuity, Near Visual Acuity and Reading Performance. The Values Indicate the Mean ± Standard Deviation |
Discussion
This study assessed the effect of simple myopic astigmatism in pseudophakic eyes with monofocal IOL implants on near visual performance for the Thai alphabet. The effects of astigmatism on the Thai alphabet were similar to previous studies which assessed on other languages (English, Spanish and Portuguese).18 In pseudophakic eyes, both near reading performance and near visual acuity improved for simple myopic astigmatism at the expense of distance visual acuity degradation. Beneficial effects of ATR astigmatism over WTR astigmatism on near visual performance (threshold print size, TPS) were also found, with no difference in degraded distance VA.
Degradation of distance visual acuity on astigmatism was not statistically significantly different by the axis but the amount of degradation increased at higher magnitude of astigmatism. This finding agreed with previous study by Serra.18 Mean distance VA values from +1.00 ATR and WTR astigmatism were 0.20 ± 0.13 and 0.14 ± 0.12 logMAR, respectively. Higher magnitude of astigmatism significantly further reduced distance VA. The mean distance VA values from the astigmatism of +2.00 ATR and WTR were 0.46 ±0.15 and 0.35 ± 0.23, respectively. According to the Thai Department of Land Transport, degradations of distance VA from +1.00 DC astigmatism (both ATR and WTR) were in the acceptable range for a professional driving license (better than 0.48 logMAR in the best eye), reflecting the minor effect of distance VA degradation on daily life.
Near visual acuity marginally improved with +1.00 DC astigmatism and significantly improved with +2.00 DC astigmatism. A non-significant small improvement in near VA was found on ATR over WTR +1.00 DC astigmatism; this effect was significantly observed in previous studies.5,8,19 Mean near VA values from +1.00 DC ATR and WTR astigmatism were 0.31 ± 0.17 and 0.33 ± 0.15 logMAR, respectively. Reading ordinary newspaper letter size N9 at 0.33 meters is made possible by this range of near VA (approximately 0.47 logMAR).
For reading performance in the Thai alphabet, most of the key findings concurred with Serra18 who studied on MNREAD charts in other languages. No significant differences were found in maximum reading speed (MRS) between refractive conditions. However, MRS was non-significantly 7.8% better with near in-focus (+3.00 DS) compared to distance in-focus (±0.00 DS). ATR astigmatism produced significantly better reading performance than WTR astigmatism when considering threshold print size (TPS), and slightly better (non-significant) reading acuity (RA) for both +1.00 and +2.00 DC astigmatism. RA values from +1.00 and +2.00 ATR astigmatism were 0.47 ± 0.14 and 0.41 ± 0.12 logMAR, respectively. These values were within the acceptable range for reading tasks (common newspaper letter size N9 at 0.33 meters, 0.47 logMAR), while WTR values (+1.00 DC and +2.00 DC) did not perform well with RA of 0.59 ± 0.14 and 0.52 ± 0.13 logMAR, respectively. These beneficial effects of ATR over WTR astigmatism for near reading performance differed from Kobashi’s study20 which conducted on the Japanese MNREAD chart and suggested no significant difference between ATR and WTR astigmatism.
The effect of astigmatic axis orientation on retinal blur pattern can explain the difference in ATR and WTR astigmatism visual performance. As illustrated by Figure 4, for near viewing the ATR simple myopic astigmatism produced a vertical blur pattern, while the WTR astigmatism produced a horizontal blur pattern. This blur pattern reverses for distance viewing. In terms of blur, our findings suggest that the Thai alphabet resembles the other languages (English, Spanish and Portuguese), with text appearing less distorted by vertical (ATR simple myopic astigmatism) than horizontal (WTR simple myopic astigmatism) blur pattern.18 The near vision simulator of The Thai version of MNREAD chart with different refractive conditions was presented as in Figure 4.
 |
Figure 4 The vision simulator of The Thai version of MNREAD chart with different refractive conditions. |
As the majority of cataract patients in Thailand are elders who more commonly have ATR than WTR astigmatism,6 the strategy of leaving ATR astigmatism uncorrected after cataract surgery benefits near visual performance at the expense of distance visual performance in patients who may not be able to afford multifocal or toric IOLs. Astigmatism over 2.0 DC may need to be corrected as distance VA enters an unacceptable range for routine daily life, while no further improvement of near visual performance is observed. For the treatment of astigmatism with toric IOLs and other methods, the decision whether or not to flip the steepest axis of astigmatism (over-correction) remains debatable. The present results demonstrating the benefit of ATR over WTR astigmatism in near visual performance may aid in this debate.
Study Limitations
The influence of pupil size on visual performance and depth of focus in pseudophakic eyes was not evaluated. In future studies, an artificial pupil could be used to eliminate the effect of pupil size variation.
The simulated astigmatic blur induced by ophthalmic lenses may not be identical to the blur induced by real corneal astigmatism. The magnification effect of the plus lens in front of rather than in the corneal plane may result in slightly larger retinal image size.
Oblique astigmatism was not included as a condition in this study, due to low prevalence. However, previous studies15,21 have shown poorer visual performance in oblique astigmatism compared with ATR and WTR astigmatism.
Conclusion
When reading the Thai alphabet, ATR simple myopic astigmatism provided better results than WTR astigmatism on near visual performance. The superiority of ATR over WTR astigmatism was more obvious in time-sensitive reading tasks. Distance visual performance degradations were not different between axes. Astigmatism at magnitude 2.0 D may not be associated with better near visual performance compared to 1.0 D, while the distance visual performance is reduced.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pieh S, Kellner C, Hanselmayer G, et al. Comparison of visual acuities at different distances and defocus curves. J Cataract Refract Surg. 2002;28(11):1964–1967. doi:10.1016/S0886-3350(02)01317-2
2. Nakazawa M, Ohtsuki K. Apparent accommodation in pseudophakic eyes after implantation of posterior chamber intraocular lenses: optical analysis. Invest Ophthalmol Vis Sci. 1984;25(12):1458–1460.
3. Hayashi K, Hayashi H, Nakao F, Hayashi F. Aging changes in apparent accommodation in eyes with a monofocal intraocular lens. Am J Ophthalmol. 2003;135(4):432–436. doi:10.1016/S0002-9394(02)02091-3
4. Huber C. Planned myopic astigmatism as a substitute for accommodation in pseudophakia. J Ame Intra-Ocular Implant Soc. 1981;7(3):244–249. doi:10.1016/S0146-2776(81)80006-7
5. Maloney WF, Grindle L, Sanders D, Pearcy D. Astigmatism control for the cataract surgeon: a comprehensive review of surgically tailored astigmatism reduction (STAR). J Cataract Refract Surg. 1989;15(1):45–54. doi:10.1016/S0886-3350(89)80139-7
6. Bradbury JA, Hillman JS, Cassells-Brown A. Optimal postoperative refraction for good unaided near and distance vision with monofocal intraocular lenses. Br J Ophthalmol. 1992;76(5):300–302. doi:10.1136/bjo.76.5.300
7. Trindade F, Oliveira A, Frasson M. Benefit of against-the-rule astigmatism to uncorrected near acuity. J Cataract Refract Surg. 1997;23(1):82–85. doi:10.1016/S0886-3350(97)80155-1
8. Sawusch MR, Guyton DL. Optimal astigmatism to enhance depth of focus after cataract surgery. Ophthalmology. 1991;98(7):1025–1029. doi:10.1016/S0161-6420(91)32182-1
9. Yamamoto S, Adachi-Usami E. Apparent accommodation in pseudophakic eyes as measured with visually evoked potentials. Invest Ophthalmol Vis Sci. 1992;33(2):443–446.
10. Verzella F, Calossi A. Multifocal effect of against-the-rule myopic astigmatism in pseudophakic eyes. Refractive Corneal Surg. 1993;9(1):58–61. doi:10.3928/1081-597X-19930101-12
11. Nagpal KM, Desai C, Trivedi RH, Vasavada AR. Is pseudophakic astigmatism a desirable goal? Ind J Ophthalmol. 2000;48(3):213–216.
12. Serra PM, Cox MJ, Chisholm CM. The effect of astigmatic axis on visual acuity measured with different alphabets in Roman alphabet readers. Clin Optom. 2018;10:93–102. doi:10.2147/OPTO.S166786
13. Nanavaty MA, Vasavada AR, Patel AS, Raj SM, Desai TH. Analysis of patients with good uncorrected distance and near vision after monofocal intraocular lens implantation. J Cataract Refract Surg. 2006;32(7):1091–1097. doi:10.1016/j.jcrs.2006.03.021
14. Sigireddi RR, Weikert MP. How much astigmatism to treat in cataract surgery. Current Opinion Ophthalmol. 2020;31(1):10–14. doi:10.1097/ICU.0000000000000627
15. Sinjab M. Introduction to astigmatism and corneal irregularities. 2018;1–64.
16. Prakairungthong N, Charukamnoetkanok P, Isipradit S. Prevalence of preoperative corneal astigmatism in patients undergoing cataract surgery at Mettapracharak hospital, Thailand. J Med Assoc Thai. 2015;98(9):878–882.
17. Tidbury LP, Czanner G, Newsham D. Fiat Lux: the effect of illuminance on acuity testing. Graefe’s archive for clinical and experimental ophthalmology =Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2016;254(6):1091–1097. doi:10.1007/s00417-016-3329-7
18. Chung ST, Jarvis SH, Cheung SH. The effect of dioptric blur on reading performance. Vision Res. 2007;47(12):1584–1594. doi:10.1016/j.visres.2007.03.007
19. Serra P, Chisholm C, Sanchez Trancon A, Cox M. Distance and near visual performance in pseudophakic eyes with simulated spherical and astigmatic blur. Clin Exp Optometry. 2016;99(2):127–134. doi:10.1111/cxo.12350
20. Kobashi H, Kamiya K, Shimizu K, Kawamorita T, Uozato H. Effect of axis orientation on visual performance in astigmatic eyes. J Cataract Refract Surg. 2012;38(8):1352–1359. doi:10.1016/j.jcrs.2012.03.032
21. Wolffsohn JS, Bhogal G, Shah S. Effect of uncorrected astigmatism on vision. J Cataract Refract Surg. 2011;37(3):454–460. doi:10.1016/j.jcrs.2010.09.022
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.