")
Back to Journals » Biologics: Targets and Therapy » Volume 19
Effects of Dulaglutide in Doxorubicin Induced Renal Toxicity in Rats
Authors Hama Said HJ , Ahmed ZA
Received 18 February 2025
Accepted for publication 18 June 2025
Published 3 July 2025 Volume 2025:19 Pages 399—412
DOI https://doi.org/10.2147/BTT.S523547
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Shein-Chung Chow
Hogr Jasim Hama Said, Zheen Aorahman Ahmed
Department of Pharmacology and Toxicology, College of Pharmacy, University of Sulaimani, Sulaimani, Kurdistan Region, Iraq
Correspondence: Zheen Aorahman Ahmed, Email [email protected]
Objective: The present study was designed to determine the anti-inflammatory and antioxidant effects of dulaglutide (DUL) on doxorubicin (DOX) -induced acute kidney injury (AKI).
Methods: Twenty-eight male rats were randomly allocated into four groups: the negative control group (received Distilled water), the positive control group (received Distilled water and a single dose of DOX), DUL 0.2 mg/kg group (received DUL 0.2 mg/kg twice weekly and single dose of DOX), and DUL 0.6 mg/kg group (received DUL 0.2 mg/kg twice weekly and single dose of DOX). All DOX doses (20 mg/kg) were given at day 13th of the study and all treatments were administered intraperitoneally for 14 days. On day fifteenth, the rats were sacrificed, and blood was collected to measure the complete blood count (CBC), Neutrophile/Lymphocyte Ratio (NLR), Monocyte/Lymphocyte Ratio (MLR), And Platelet/Lymphocyte Ratio (PLR), C-reactive protein (CRP), blood urea nitrogen (BUN), and serum creatinine (SCr). The right kidney was used for histopathological examination, while the left kidney was homogenized to assess the renal tissue levels of malondialdehyde (MDA), total antioxidant capacity (TAOC), interleukin-1beta (IL-1β), tumor necrosis factor-alpha (TNF-α), kidney injury molecule-1 (KIM-1), and neutrophil gelatinase-associated lipocalin (NGAL).
Results: DOX induces acute kidney injury was demonstrated by significant elevations in BUN, SCr, and CRP levels. DUL significantly lowered the levels of BUN, SCr, and CRP, and reduced the levels of blood inflammation markers, including NLR and MLR. Additionally, it resulted in a significant reduction in the renal tissue levels of MDA, IL-1β, and TNF-α, while the level of TAOC was significantly elevated. These findings were supported by histopathological assessments.
Conclusion: The present study indicates that DUL mitigates doxorubicin-induced kidney damage by reducing oxidative stress and inflammation.
Keywords: nephrotoxicity, doxorubicin, GLP-1, dulaglutide, TNF-α, KIM-1
Graphical Abstract:

Introduction
Nephrotoxicity is the impairment of the kidneys due to exposure to various pharmaceuticals, diagnostic methods, and toxins, leading to functional renal disorders and impaired detoxification and excretion.1,2 Consequently exposure to nephrotoxic agent can lead to various forms of renal impairment, such as acute kidney injury (AKI) and chronic kidney disease (CKD).1,3 AKI is a condition marked by a rapid decline in excretion, resulting in buildup of unmeasured waste materials such as creatinine and urea.4 Moreover it is a common diagnosis in both hospital and pre-hospital settings, with prevalence rates reaching up to 60% among patients admitted to intensive care units.5,6 Furthermore epidemiological studies suggest that medication-related kidney toxicity is the third leading cause of AKI and contribute to the development of CKD and end-stage renal disease.7 Aditionaly risk factors for drug-induced nephrotoxicity include patient-specific factors (age and sex),8 kidney-specific factors (high exposure to drugs/metabolites),5 and drug-specific factors (high doses, prolonged use).2 Notably nephrotoxicity is a significant issue in cancer treatment, leading to delayed therapy, extended hospitalizations, and higher mortality rates among cancer patients.2
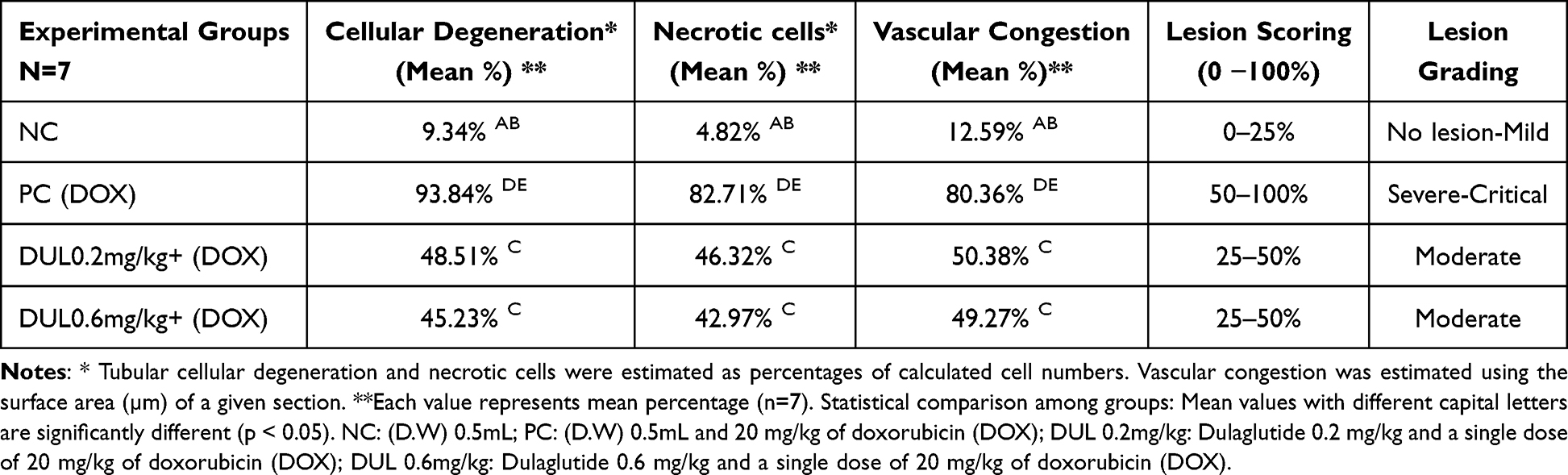 |
Table 1 Histological Quantitative Evaluation of Kidney Sections |
Doxorubicin (DOX) has been widely utilized as an antineoplastic anthracycline-derived antibiotic for treating several human cancers, including solid tumors and hematological malignancies.9,10 It exerts its antitumor effects via DNA intercalation and inhibition of topoisomerase II (TOP2) in rapidly proliferating cancer cells.11,12 Unfortunately, the therapeutic application of DOX is limited because of its dose-dependent toxicity affecting essential organs such as the heart, liver, and kidneys.13,14 Importantly, nephrotoxicity is a prevalent and severe adverse effect of DOX therapy.15,16 Furthermore, it has been reported to cause AKI and nephrotic syndrome.2,17 It can also harm the glomeruli and tubules, resulting in tubulointerstitial inflammation that ultimately leads to tubular fibrosis and atrophy.18,19
However, the precise mechanisms underlying DOX-induced nephropathy remain unclear. However, many studies have reported that the formation of free radicals, leading to oxidative damage and inflammation, is a major mechanism underlying DOX-mediated renal toxicity.11,20 Therefore, we require an adjuvant therapy for doxorubicin chemotherapy that possesses both antioxidant and anti-inflammatory properties to protect against the renal damage associated with doxorubicin treatment.17,21
Glucagon-like peptide-1 (GLP-1), an incretin hormone mainly involved in glucose homeostasis in diabetes.9 Glucagon-like peptide-1 receptor agonists (GLP-1RAs), were approved by the Food and Drug Administration (FDA) for the management of type II diabetes.22 Indeed the effects of GLP-1RAs extend beyond pancreatic β-cells, as the glucagon-like peptide-1 receptor (GLP-1R) is also expressed in different organs, including the brain, heart, liver, muscle, and kidneys. In the kidneys, GLP-1R is abundantly present in the renal cortex, proximal tubules, and renal vasculature.23 Moreover extensive in vitro and in vivo studies have confirmed the renoprotective activity of GLP-1RAs through multiple mechanisms, including enhancing natriuresis and renal vasodilation, reducing oxidative stress and inflammation, and stimulating autophagy.24 In addition, extensive research has demonstrated that GLP-1RAs show kidney-protective benefits in animal models of diabetic nephropathy and AKI.24
Dulaglutide (DUL) is a long-acting GLP-1RA approved for managing type 2 diabetes mellitus (T2DM) by enhancing the secretion of insulin in response to glucose while reducing glucagon levels through GLP-1R activation.23 Besides its hypoglycemic effects, DUL also results in weight reduction, correction of dyslipidemia, and offers protection for cardiovascular and renal health.25 Moreover numerous researchers have emphasized on the antioxidant, anti-inflammatory, and anti-apoptotic properties of DUL, suggesting its potential benefit as a therapeutic agent for conditions marked by significant inflammation, oxidative stress, and apoptosis.22,25–28 Importantly, it is hypothesized that DUL may also demonstrate specific anti-inflammatory and antioxidant effects on renal tissues, which require validation in future research.
To our knowledge, the protective effects of dulaglutide against acute kidney injury have not been studied; therefore, our objective was to explore the anti-inflammatory and antioxidant effects of DUL on DOX-induced AKI to detect its potential therapeutic properties.
Materials and Methods
Drugs
Doxorubicin vials (DOXO-cell® 50 mg solution) were obtained from STADAPHARMA GmbH (Bad Vilbel, Germany). Dulaglutide (Trulicity ® 1.5 mg prefilled pen) was purchased from Eli Lilly (Indianapolis, IN, USA) and diluted in normal saline one by one.26,29
Ethical and Experimental Animals
Twenty-eight male Wistar albino rats, each weighing between 180 and 230 g, were obtained from the animal house of Tikrit University and housed in the animal facility of the College of Pharmacy, University of Sulaimani, in well-ventilated plastic cages under standard conditions, including a temperature of 25 ± 2°C and a regular day-night cycle. Rats were fed a regular pellet diet and tap water. Before the experiment commenced, the animals were acclimatization period. All procedures were conducted in accordance with ARRIVE guidelines, and the ethical standards for animal experimentation were approved by the University of Sulaimani’s Ethics and Research Registration Committee on 28/11/2024. The study was performed by the Canadian Council on Animal Care (CCAC) guidelines.
Study Design and Treatment Protocol
Twenty-eight male rats were randomly allocated to four groups using the blocking randomization technique. Each group was comprised of seven rats.
Negative control (NC): only 0.5 mL of distilled water (DW) was administered by intraperitoneal injection (ip) twice weekly for 14 days.
The positive control (PC): received DW (0.5 mL) by (ip) twice weekly for 14 days and a single dose (ip) of DOX (20 mg/kg) on the 13th day of the study.
Dulaglutide 0.2 mg/kg group (DUL 0.2 mg/kg): received 0.2 mg/kg of DUL by (ip) twice weekly for 14 days and single dose (ip) of DOX (20 mg/kg) on the 13th day of research.
Dulaglutide 0.6 mg/kg group (DUL 0.6 mg/kg): received 0.6 mg/kg of DUL by (ip) twice weekly for 14 days and single dose (ip) of DOX (20 mg/kg) on the 13th day of study.
The dosages of DUL,23,30,31 and doxorubicin were selected based on previous research.12,32
Measurement of Weigh and Relative Kidney Weight
The weights of the rats were recorded before the start of treatment and on the day of sacrifice, using a weighing scale. Subsequently, the kidneys were gently extracted, cleaned of the surrounding tissues, and weighed. Relative kidney weight was calculated using the following formula: (kidney weight/body weight) × 1000.
Sample Collection and Tissue Homogenous
On day 15 of the experiment, the rats were euthanized, approximately 5 mL of blood was drawn via cardiac puncture and transferred to the tubes. To isolate the serum, the samples were centrifuged at 4000 RPM for 10 min, and the serum was used to analyze creatinine, urea, and C-reactive protein (CRP) levels.
Kidneys were excised, the right kidney was rinsed with ice-cold saline, placed in 10% formaldehyde for a histopathological examination, and left kidneys were rinsed with phosphate buffer saline (PBS) solution (pH 7.4), weighed, dissected, and mixed with 9 mL of PBS solution according to the enzyme-Linked Immunosorbent assay (ELISA) kit’s instruction. The sample was homogenized, centrifuged at 5000 × g for 5 min at 4°C, and stored at −80°C for later evaluation of inflammation, oxidative stress, and kidney biomarkers.
Evaluation of Biochemical Parameters
Measurement of Renal Function Test, Complete Blood Count (CBC), and CRP
Blood serum was analyzed for blood urea nitrogen (BUN), serum creatinine (SCr), and CRP using Cobas C 311 analyzers for Clinical Chemistry, and (CBC) was measured using a 5-dimensional automated hematology analyzer for Homogeneous Immunology.
Measurement of Renal Oxidative Damage Biomarkers
The supernatant from the homogenized kidney tissue was used to measure oxidative stress markers, using ELISA kits (Bioassay Technology Laboratory, Shanghai, China) including malondialdehyde (MDA), (Cat. No. E0156Ra), and Total antioxidant capacity (TAOC) (Cat. No E3901Ra).
Measurement of Renal Inflammation Markers
The supernatant from homogenized kidney tissue was used to measure inflammatory markers, using ELISA kits (Bioassay Technology Laboratory, Shanghai, China), including TNF-α, (Cat. No. E0764Ra) and Interleukin-1beta (IL-1β). (Cat. No E0119Ra).
Measurement of Kidney – Specific Markers
The supernatant from homogenized kidney tissue was used to measure kidney-specific markers using ELISA kits (Bioassay Technology Laboratory, Shanghai, China), including kidney injury molecule (KIM-1). (Cat. E0549Ra) and neutrophil gelatinase-associated lipocalin (NGAL). (Cat. No E0762Ra).
Histopathological Examination
The histological protocol was initiated after completion of the experiment. Before sacrifice, animals were deprived of food for at least 10 h. After euthanasia, necropsy was performed and tissue samples were collected for histological analysis. Briefly, kidney samples were carefully isolated, placed in tissue cassettes, and fixed in 10% neutral buffered formaldehyde solution for approximately 48 h.
Subsequently, the tissue samples were dehydrated using a graded series of ethanol concentrations (50, 60, 70, 90, and 100%), followed by two to three xylene clearance steps. Kidney tissues were infiltrated and embedded in paraffin at 60–70°C using an automated system. The paraffin blocks were then sectioned into 5 µm slices, placed on glass slides, and dried on a heated tissue holder.
The prepared slides were deparaffinized, treated with xylene for 30 min, and dried in an oven at 50°C for 5 min. Finally, the tissue sections were stained with Harris’s hematoxylin and eosin (H&E) solution, cleared with xylene, and covered with a slide before observation under a bright-field light microscope.
Semi Quantitative Lesion Scoring of Renal Samples
Lesion scoring was evaluated semi-quantitatively via image analyzer software (Am Scope, 3.7) using an ocular lens camera (MD500, 2019) fixed with a bright field light microscope (NOVEL XSZ-N107T, China). Tissue samples were examined under a light microscope, and degenerative changes in renal tubular epithelial cells were quantified at high magnification. The mean lesion values and vascular congestion were measured and expressed as percentages. On the basis of the scoring system, 0–10% indicated no lesions, 10–25% indicated mild lesions, 25–50% indicated moderate lesions, 50–75% indicated severe lesions, and 75–100% indicated critical lesions.11
Data Analysis
Statistical analyses were performed using the GraphPad Prism version 10. The data are presented as mean ± standard deviation (SD). One-way analysis of variance was performed to compare the various groups, followed by Tukey’s test for multiple comparisons. Statistical significance was set at p < 0.05.
Results
Effect of Different Doses of Dulaglutide on Total Weight of Rats and Relative Kidney Weight
Figure 1A demonstrates that a single dose of DOX, DUL 0.6 mg/kg and DUL 0.2 mg/kg produced a significant reduction in the total body weight of rats compared to NC group, (p=<0.0001, <0.0001, and <0.0001 respectively). Meanwhile, both DUL 0.6 mg/kg and DUL 0.2 mg/kg had no significant effect on total body weight compared to PC group, (p=0.4728, 0.5270 and respectively). Figure 1B shows that single dose of DOX, DUL 0.6 mg/kg and DUL 0.2 mg/kg did not significantly affect relative kidney weight compared to NC group (p=0.9762, 0.2413, and 0.6119 respectively). While DUL 0.6 mg/kg cause a significant elevation in the relative kidney weight compared to DUL 0.2 mg/kg group, (p=0.0202).
 |
Figure 1 Effect of different doses of dulaglutide (DUL) on doxorubicin (DOX)-induced renal injury as assessed by (A) The change in the weight, and (B) Relative kidney weight. Data are presented as mean ± SEM, N=7. Statistical significance indicators: ns: not significant, *p<0.05, ****p<0.0001 significantly different compared to positive control group using one-way ANOVA followed Tukey’s multi comparison test. |
Effect of Different Doses of Dulaglutide on SCr and BUN Levels
Figure 2A shows that DOX caused a significant increase in SCr levels in PC group compared with the NC group (p=0.0107). Meanwhile Only DUL 0.6 mg/kg produced a significant reduction in SCr levels compared with that in the PC group (p=0.0167). Figure 2B shows that a single dose of DOX caused a significant increase in BUN levels in PC group compared to those in the NC group (p=0.0009). Meanwhile only DUL 0.6 mg/kg results in a significant decline in BUN levels compared with the PC group (p ≤ 0.0001). DUL 0.6 mg/kg produced a significant decrease in BUN compared to DUL 0.2 mg/kg group, (p=0.453).
 |
Figure 2 Effect of different doses of dulaglutide (DUL) on doxorubicin (DOX)-induced renal injury as assessed by (A) serum creatinine (SCr), and (B) blood urea nitrogen (BUN) in the serum. Data are presented as mean ± SEM, N=7. Statistical significance indicators: ns: not significant, *p<0.05, *** p<0.001, ****p<0.0001 significantly different compared to positive control group using one-way ANOVA followed Tukey’s multi comparison test. |
Effect of Different Doses of Dulaglutide on MDA and TAOC
Figure 3A demonstrates that a single dose of DOX induced a significant increase in MDA levels in kidney tissues in PC group compared to that in the NC group (p=0.0110). Meanwhile Only DUL 0.6 mg/kg significantly reduced renal tissue MDA levels compared to the PC group (p=0.0005). Figure 3B illustrates that a single administration of DOX resulted in a significant reduction in TAOC levels in kidney tissues in PC group compared to that in the NC group (p=0.0024). Meanwhile Both DUL 0.6 mg/kg and DUL 0.2 mg/kg demonstrated a significant increase in TAOC levels in kidney tissue compared to that in the PC group (p=0.0003, and 0.0003 respectively).
 |
Figure 3 Effect of different doses of dulaglutide (DUL) on doxorubicin (DOX)-induced renal injury as assessed by (A) malondialdehyde (MDA) levels and (B) total antioxidant capacity (TAOC) in kidney tissues. Data are presented as mean ± SEM, N=7. Statistical significance indicators: ns: not significant, * p<0.05, ** p < 0.01, *** p<0.001 significantly different compared to positive control group using one-way ANOVA followed Tukey’s multi comparison test. |
Effect of Different Doses Dulaglutide on CRP, Neutrophile/Lymphocyte Ratio (NLR), Monocyte/Lymphocyte Ratio (MLR), and Platelet/Lymphocyte Ratio (PLR)
Figure 4A illustrates that a single dose of DOX led to a significant elevation in serum CRP levels in PC group relative to those in the NC group (p=0.0096). Meanwhile Only DUL 0.6 mg/kg led to a significant reduction in serum CRP levels relative to those in the PC group (p=0.0323). Figure 4B shows that a single dose of DOX led to a significant increase in the blood NLR in PC group compared with that in the NC group (p=0.0060). Meanwhile Only DUL 0.6 mg/kg produced a significant decline in blood NLR compared to the PC group (p=0.0293). Figure 4C shows that a single dose of DOX led to a significant elevation in blood MLR in PC group compared with that in the NC group (p=0.0002). Meanwhile Both DUL 0.6 mg/kg and DUL 0.2 mg/kg produced a significant decrease in blood MLR compared to the PC group (p=0.0001, and 0.0003 respectively). Figure 4D demonstrates that a single administration of DOX led to a significant increase in blood PLR levels in PC group compared with the NC group (p=0.0032). Meanwhile Both DUL 0.6 mg/kg and DUL 0.2 mg/kg had no significant effect (p=0.2050, and 0.9935).
 |
Figure 4 Effect of different doses of dulaglutide (DUL) on doxorubicin (DOX)-induced renal injury as assessed by (A) C-reactive protein (CRP), (B) Neutrophil/Lymphocyte Ratio (NLR), (C) Monocyte/Lymphocyte Ratio (MLR), And (D) Platelet/Lymphocyte Ratio (PLR) in the serum. Data are presented as mean ± SEM, N=7. Statistical significance indicators: ns: not significant, *p<0.05, ** p < 0.01, *** p<0.001 significantly different compared to positive control group using one-way ANOVA followed Tukey’s multi comparison test. |
Effect of Different Doses of Dulaglutide on IL-1β and TNF-α
Figure 5A shows that a single dose of DOX resulted in a significant elevation in IL-1β levels in the kidney tissues in PC group compared to that in the NC group (p=0.0003). Meanwhile Both DUL 0.6 mg/kg and DUL 0.2 mg/kg produced a significant drop in IL-1β in kidney tissues when compared to the PC group (p ≤ 0.0001, and 0.0053 respectively). Figure 5B shows that a single dose of DOX resulted in a significant increase in TNF-α in the kidney tissues in PC group compared to that in the NC group (p=0.0259). Meanwhile Only DUL 0.6 mg/kg produced a significant drop in TNF-α in kidney tissues compared to the PC group (p=0.0002).
 |
Figure 5 Effect of different doses of dulaglutide (DUL) on doxorubicin (DOX)-induced renal injury as assessed by (A) Interleukin-1beta (IL-1β), and (B) Tumor necrosis factor-alpha (TNF-α) in kidney tissues. Data are presented as mean ± SEM, N=7. Statistical significance indicators: ns: not significant, *p<0.05, ** p < 0.01, *** p<0.001, ****p<0.0001 significantly different compared to positive control group using one-way ANOVA followed Tukey’s multi comparison test. |
Effect of Different Doses of Dulaglutide on KIM-1 And NGAL
Figure 6A shows that a single dose of DOX led to a significant increase in KIM-1 expression in the kidney tissues in PC group compared to that in the NC group (p<0.0001). Meanwhile Only DUL 0.6 mg/kg produced a significant drop in KIM-1 in kidney tissues compared to that in the PC group (p=0.0007). Figure 6B shows that a single dose of DOX resulted in a significant elevation in NGAL levels in the kidney tissues in PC group compared to that in the NC group, ((p=0.0341). Meanwhile DUL 0.6 mg/kg and DUL 0.2 mg/kg produced a significant decline in NGAL levels in kidney tissues when compared to the PC group (p=0.0001, and 0.0366 respectively).
 |
Figure 6 Effect of different doses of dulaglutide (DUL) on doxorubicin (DOX)-induced renal injury as assessed by (A) kidney injury molecule (KIM-1), and (B) and neutrophil gelatinase associate lipocalin (NGAL) in kidney tissues. Data are presented as mean ± SEM, N=7. Statistical significance indicators: ns: not significant, *p<0.05, ***p<0.001, ****p<0.0001 significantly different compared to positive control group using one-way ANOVA followed Tukey’s multi comparison test. |
Effect of Different Doses of Dulaglutide on the Renal Histopathological Changes Induced by DOX
Initially, Table 1 illustrate the morphometric semiquantitative evaluation of kidney sections, accordingly, animals receiving different regimen doses of Dulaglutide as prophylactic measures in both low and high doses schedule 0.2 mg/kg and 0.6 mg/kg respectively, show remarkable mitigation in lesion score severity, evidenced by significant (P<0.05) mitigation in the percentage of degenerative cells within the renal tubular epithelia, as well as notable adjustment necrotic cell numbers. Furthermore, administration of DUL in rats exposed to DOX revealed a significant improvement in lesion grading in comparison with the PC group, which received only a single dose of DOX (20 mg/kg), regardless of dose regimen, which dramatically shifted from severe or critical lesion grade to moderate lesion score with significant morphological changes in the given renal tissue, as shown in Figure 7. Based on the histopathological findings, these results suggest the renal protective efficacy of DUL at different doses against doxorubicin-induced renal toxicity in a rat model.
 |
Figure 7 Photomicrograph of kidney from groups; (G1): Negative control group received (D.W) 0.5mL daily, demonstrate no obvious morphological changes, evident by characteristic renal glomeruli (RG), as well as, typical renal tubules (RT) with mild and non-significant cellular swelling, with the presence of low grade of vascular congestion (VC). (G2): Positive control group received (D.W) and 20 mg/kg of doxorubicin (DOX) at day 13th, display severe to critical vacuolar degeneration (VD) in the renal tubular epithelium (RT) with the evidence of glomerular atrophy (GA), in addition to the presence of significant vascular congestion (yellow arrows) within engorged renal vasculature as well as renal glomerular capillaries (RG). (G3): DUL 0.2 mg/kg + DOX group, received dulaglutide 0.2mg/kg and a single dose of 20 mg/kg of doxorubicin (DOX) at day 13th, reveal significant vascular congestion (yellow arrows) within the interstitial blood vessels, as well as renal glomerular (RG) microcirculations, together with the prevalence of necrotic cells (NC) in the renal tubular epithelia (RT) with slight cellular swelling. (G4): DUL 0.6 mg/kg + DOX group, received dulaglutide 0.6mg/kg and a single dose of 20 mg/kg of doxorubicin (DOX) at day 13th, show mild to moderate grade of interstitial vascular congestion (yellow arrows), together with moderate vacuolar degenerative swelling (VD) in the renal tubular epithelial cells (RT), in addition to low grade of blood engorgement in the renal glomerular capillaries (RG). H&E. MP: 400X. |
Discussion
The kidneys regulate vital body functions and eliminate waste and drugs but are highly sensitive to toxins and prone to inflammation and oxidative damage.33 Doxorubicin (DOX) is a powerful cytotoxic drug, but its use is limited because of dose-dependent toxicity, including nephropathy.19 The present study demonstrated that dulaglutide mitigates DOX-induced kidney damage by inhibiting inflammation and oxidative damage.
The findings of the present study indicates that the PC group and DUL treatment groups showed a reduction in the total body weight of rats, while the relative kidney weight remained unchanged, these outcomes were accordance with previous study.15,30,31,34 These results can be elucidated by the weight loss in DOX-injected rats is associated with anorexia and increasing fatigue, resulting in less physical activity.20 Also several studies have demonstrated that DUL act as a GLP-1RA to facilitate weight reduction by suppression of appetite and enhancing stomach emptying.35 Moreover DOX-induced kidney impairment was detected by increased BUN and SCr levels these renal function parameters are dependable and highly sensitive markers of drug-induced nephrotoxicity,34,36 importantly in the present study, DOX administration resulted in a significant decline in renal function as manifested by increased SCr and BUN levels in the DOX control group when compared to the NC group, and these results align with previous studies.15,36,37 Conversely Our data indicated that pretreatment with DUL followed by DOX improves renal function, evidenced by significantly lower serum levels of BUN and creatinine in the DUL + DOX group compared to the DOX control group, so this finding is accordance with the findings of previous studies about the nephroprotective properties of DUL in diabetic chronic kidney disease rat models, showed noticeable maintenance of renal functions.23,31
Renal oxidative stress is now widely recognized as the main pathogenic mechanism underlying DOX-induced nephrotoxicity in cancer patients.20 Additionally, malondialdehyde (MDA) is a byproduct of lipid peroxidation generated by free radicals and serves as a marker of oxidative damage.13,37,38 Also, an elevated level of the oxidative stress marker MDA may serve as an early indicator of potential toxicity.39 Accordingly our study confirmed the critical role of oxidative damage as a significant factor in DOX-induced nephrotoxicity, as demonstrated by an increase in MDA levels and a decline in TAOC within renal tissue in PC group, and this finding is accordance with the findings of previous research.14,36 A possible explanation for these results is that DOX- induces oxidative stress and renal dysfunction by generating free radicals via its one-electron reduction, which leads to ROS production. ROS cause cellular damage, including lipid peroxidation, protein oxidation, DNA damage, and mitochondrial dysfunction, ultimately resulting in structural and functional alterations in the renal tubules and glomeruli.20,40,41
In addition to their antihyperglycemic actions, recent evidence indicates that GLP-1RAs could also have antioxidative benefits,42 thus the findings of this study demonstrated that the administration of DUL exerts a protective antioxidant effect by reducing MDA levels and increasing TAOC in the renal tissue of the DUL + DOX group, which is in agreement with a previous study reporting that DUL diminishes MDA levels and increases antioxidant enzymes in a rotenone-induced model of Parkinson’s disease.26 Furthermore, DUL ameliorated LPS-induced oxidative stress in H9c2 myocardial cells,22 and attenuated TNF-α-induced oxidative stress in human fibroblast-like synoviocytes,28 because incretin-based therapy was found to exert antioxidant effects through the upregulation of renal Nuclear Factor Erythroid 2-Related Factor 2 (Nrf2), which augments the transcription of antioxidant enzymes that scavenge free radicals, indeed Nrf2 is a major regulator of oxidative state, enhancing cellular defenses against oxidative damage by upregulating the transcription of antioxidant enzymes.18,42
Inflammation is the biological response of the immune system to various stimuli and can be triggered by harmful agents such as infections, irritants, antibodies, and physical injuries.43 Importantly, many studies have shown that inflammation is considered a primary contributor to DOX-induced nephrotoxicity.33,41 Accordingly, the present study confirmed the critical role of inflammation in the mechanism of DOX-induced nephrotoxicity, as demonstrated by a significant increase in inflammatory markers, including serum CRP, NLR, MLR, and renal tissue TNF-α and IL-1β in the DOX control group. These findings are in agreement with the outcomes of previous studies,19,40,41 and this inflammatory reactions can be attributed to oxidative stress induced by DOX, which may provoke renal inflammation by elevating pro-inflammatory cytokines through the activation of inflammatory proteins, including mitogen-activated protein kinase (MAPK), nuclear factor kappa B (NF-κB), and NOD-like receptor family pyrin domain containing 3 (NLRP3 inflammasome).19,37,41 GLP-1R signals have been explored as therapeutic targets for inflammation-related disorders because of their anti-inflammatory properties.28,44 Therefore, in the present study, pretreatment with DUL followed by DOX results in reduction in serum levels of CRP, NLR, and MLR, as well as renal tissue levels of TNF-α and IL-1β, compared to the DOX control group. This anti-inflammatory effect of DUL has been reported in previous studies, indicating that it exerts significant anti-inflammatory effects by decreasing the expression of TNF-α, IL-1β, and IL-6 via multiple pathways across various organs. In lung injury, it inhibits NLRP3 and signal transducer and activator transcription (STAT3) expression.25 In cardiomyocytes, it suppresses the Toll-like receptor 4 (TLR4/NF-κB) pathway. In endometrial injury, it prevents M1 macrophage polarization.44 In skeletal muscle and fibroblast-like synoviocytes, it inhibits the phosphorylation of inhibitor of kappa B (p-IκB), thereby blocking NF-κB activation.27,28
Kidney injury molecule-1 (KIM-1) is a type I transmembrane glycoprotein that is highly expressed in damaged renal tubular cells, especially in proximal tubules,34,41 and NGAL is one of the earliest and most significantly increased proteins in the kidney following AKI caused by nephrotoxic agents in animal models, and it is a sensitive marker for tubular injury and inflammation.19,34 Furthermore both KIM-1 and NGAL have been validated as early prediction biomarkers of renal tubular damage.34 Moreover in the current study, DOX administration caused significant tubular damage, as evidenced by the increased levels of KIM-1 and NGAL in renal tissue of PC group relative to the NC group. These findings are in agreement with the outcomes of previous studies,14,19 importantly the results of the present study suggest that DUL- mitigates renal tubular injury in the DUL+DOX group, as evidenced by the significantly reduced renal injury markers KIM-1 and NGAL in renal tissue. These results are supported by earlier study of.23,31 It is worth mentioning that the histopathological findings support the biochemical results, confirming that a single dose of DOX (20 mg/kg) induces kidney damage, including lesions, tissue degeneration, necrosis, glomerular atrophy and vascular congestion. The same result was obtained in a previous study.34,41 In addition, Histopathological changes due to DOX were only partially prevented by DUL 02 mg/kg, while DUL 0.6 mg/kg significantly mitigated lesion scoring, tissue degeneration, glomerular atrophy, and vascular congestion in the kidney structure.
Limitations of the Study
This self-funded study was limited by financial and time constraints, restricting additional investigations and long-term follow-up. While the findings in rats are promising, they may not directly translate to humans, underscoring the need for future clinical trials to evaluate long-term renal outcomes and therapeutic relevance.
Conclusion
The present study demonstrated a strong association between oxidative stress, inflammation, and DOX-induced renal injury as evidenced by biochemical markers and histopathological findings. These findings are suggesting that DUL may help alleviate the complications of DOX induced kidney damage by reducing oxidative damage and inflammation. Further experimental and clinical studies are required to validate these results.
Acknowledgments
The authors would like to thank the College of Pharmacy, University of Sulaimani, for providing the support and facilities for this project.
Funding
No funding was received by the authors for this work.
Disclosure
No conflicts of interest are disclosed by the authors.
References
1. Džidić-Krivić A, Sher EK, Kusturica J, Farhat EK, Nawaz A, Sher F. Unveiling drug induced nephrotoxicity using novel biomarkers and cutting-edge preventive strategies. Chem Biol Interact. 2024;388:110838. doi:10.1016/j.cbi.2023.110838
2. Chen C, Xie D, Gewirtz DA, Li N. Nephrotoxicity in cancer treatment: an update. In: Advances in Cancer Research. Vol. 155. Elsevier;2022:77–129. doi:10.1016/bs.acr.2022.03.005
3. Mody H, Ramakrishnan V, Chaar M, et al. A review on drug‐induced nephrotoxicity: pathophysiological mechanisms, drug classes, clinical management, and recent advances in mathematical modeling and simulation approaches. Clinical Pharm in Drug Dev. 2020;9(8):896–909. doi:10.1002/cpdd.879
4. Leowattana W. Antiviral Drugs and Acute Kidney Injury (AKI). IDDT. 2019;19(4):375–382. doi:10.2174/1871526519666190617154137
5. Sales GTM, Foresto RD. Drug-induced nephrotoxicity. Rev Assoc Med Bras. 2020;66(suppl 1):s82–s90. doi:10.1590/1806-9282.66.s1.82
6. Pickkers P, Darmon M, Hoste E, et al. Acute kidney injury in the critically ill: an updated review on pathophysiology and management. Intensive Care Med. 2021;47(8):835–850. doi:10.1007/s00134-021-06454-7
7. Ali HH, Ahmed ZA, Aziz TA. Effect of Telmisartan and Quercetin in 5 Fluorouracil-induced renal toxicity in rats. JIR. 2022;15:6113–6124. doi:10.2147/JIR.S389017
8. Dobrek L. A synopsis of current theories on drug-induced nephrotoxicity. Life. 2023;13(2):325. doi:10.3390/life13020325
9. HamaSalih R. Effects of Semaglutide in doxorubicin-induced cardiac toxicity in Wistar Albino rats. CMAR. 2024;16:731–740. doi:10.2147/CMAR.S468453
10. Aziz TA. Cardioprotective effect of Quercetin and Sitagliptin in doxorubicin-induced cardiac toxicity in rats. CMAR. 2021;13:2349–2357. doi:10.2147/CMAR.S300495
11. Ahmed ZA, Abtar AN, Othman HH, Aziz TA. Effects of quercetin, sitagliptin alone or in combination in testicular toxicity induced by doxorubicin in rats. DDDT. 2019;13:3321–3329. doi:10.2147/DDDT.S222127
12. Ali N, AlAsmari AF, Imam F, et al. Protective effect of diosmin against doxorubicin-induced nephrotoxicity. Saudi J Biol Sci. 2021;28(8):4375–4383. doi:10.1016/j.sjbs.2021.04.030
13. Bilgic S, Armagan I. Effects of misoprostol treatment on doxorubicin induced renal injury in rats. Biotech Histochem. 2020;95(2):113–120. doi:10.1080/10520295.2019.1645356
14. Asaad GF, Hassan A, Mostafa RE. Antioxidant impact of Lisinopril and Enalapril against acute kidney injury induced by doxorubicin in male Wistar rats: involvement of kidney injury molecule-1. Heliyon. 2021;7(1):e05985. doi:10.1016/j.heliyon.2021.e05985
15. Patel D, Yadav P, Singh SK, et al. Betaine alleviates doxorubicin‐induced nephrotoxicity by preventing oxidative insults, inflammation, and fibrosis through the modulation of Nrf2/HO−1/NLRP3 and TGF‐β expression. J Biochem Molecular Tox. 2024;38(1):e23559. doi:10.1002/jbt.23559
16. Wu Q, Li W, Zhao J, et al. Apigenin ameliorates doxorubicin-induced renal injury via inhibition of oxidative stress and inflammation. Biomed. Pharmacother. 2021;137:111308. doi:10.1016/j.biopha.2021.111308
17. Soltani Hekmat A, Chenari A, Alipanah H, Javanmardi K. Protective effect of alamandine on doxorubicin‑induced nephrotoxicity in rats. BMC Pharmacol Toxicol. 2021;22(1):31. doi:10.1186/s40360-021-00494-x
18. Botros SR, Matouk AI, Amin A, Heeba GH. Comparative effects of incretin-based therapy on doxorubicin-induced nephrotoxicity in rats: the role of SIRT1/Nrf2/NF-κB/TNF-α signaling pathways. Front Pharmacol. 2024;15:1353029. doi:10.3389/fphar.2024.1353029
19. Mostafa RE, Morsi AH, Asaad GF. Anti-inflammatory effects of saxagliptin and vildagliptin against doxorubicin-induced nephrotoxicity in rats: attenuation of NLRP3 inflammasome up-regulation and tubulo-interstitial injury. Res Pharm Sci. 2021;16(5):547–558. doi:10.4103/1735-5362.323920
20. Arunachalam S, Nagoor Meeran MF, Azimullah S, et al. α-Bisabolol Attenuates Doxorubicin Induced Renal Toxicity by Modulating NF-κB/MAPK Signaling and Caspase-Dependent Apoptosis in Rats. IJMS. 2022;23(18):10528. doi:10.3390/ijms231810528
21. Hussain MA, Abogresha NM, AbdelKader G, Hassan R, Abdelaziz EZ, Greish SM. Antioxidant and Anti‐Inflammatory Effects of Crocin Ameliorate Doxorubicin‐Induced Nephrotoxicity in Rats. Oxid Med Cell Longev. 2021;2021(1):8841726. doi:10.1155/2021/8841726
22. Wang R, Wang N, Han Y, Xu J, Xu Z. Dulaglutide alleviates LPS-induced injury in cardiomyocytes. ACS Omega. 2021;6(12):8271–8278. doi:10.1021/acsomega.0c06326
23. Mohamad HE, Abdelhady MA, Abdel Aal SM, Elrashidy RA. RETRACTED: dulaglutide mitigates high dietary fructose-induced renal fibrosis in rats through suppressing epithelial-mesenchymal transition mediated by GSK-3β/TGF-β1/Smad3 signaling pathways. Life Sci. 2022;309:120999. doi:10.1016/j.lfs.2022.120999
24. Kheira HS, Elsayed GR, El-Adl M. Liraglutide and resveratrol alleviated cyclosporin A induced nephrotoxicity in rats through improving antioxidant status, apoptosis and pro-inflammatory markers. Biochem Biophys Res Commun. 2024;730:150337. doi:10.1016/j.bbrc.2024.150337
25. Wang Y, Deng F, Zhong X, et al. Dulaglutide provides protection against sepsis-induced lung injury in mice by inhibiting inflammation and apoptosis. Eur J Pharmacol. 2023;949:175730. doi:10.1016/j.ejphar.2023.175730
26. Khalaf MM, El-Sayed MM, Kandeil MA, Ahmed S. A novel protective modality against rotenone-induced Parkinson’s disease: a pre-clinical study with dulaglutide. Int Immunopharmacol. 2023;119:110170. doi:10.1016/j.intimp.2023.110170
27. Nguyen TTN, Choi H, Jun HS. Preventive effects of Dulaglutide on disuse muscle atrophy through inhibition of inflammation and apoptosis by induction of Hsp72 expression. Front Pharmacol. 2020;11:90. doi:10.3389/fphar.2020.00090
28. Zheng W, Pan H, Wei L, Gao F, Lin X. Dulaglutide mitigates inflammatory response in fibroblast-like synoviocytes. Int Immunopharmacol. 2019;74:105649. doi:10.1016/j.intimp.2019.05.034
29. Park HJ, Han H, Oh EY, et al. Empagliflozin and Dulaglutide are effective against obesity-induced airway hyperresponsiveness and fibrosis in A Murine Model. Sci Rep. 2019;9(1):15601. doi:10.1038/s41598-019-51648-1
30. Shamardl HAMA, Ibrahim NA, Merzeban DH, Elamir AM, Golam RM, Elsayed AM. Resveratrol and Dulaglutide ameliorate adiposity and liver dysfunction in rats with diet-induced metabolic syndrome: role of SIRT-1 / adipokines / PPARγ and IGF-1. DARU J Pharm Sci. 2023;31(1):13–27. doi:10.1007/s40199-023-00458-y
31. Yeung HYM. Glucagon-like peptide-1 receptor agonist, dulaglutide, ameliorates kidney function in diet-induced obese mice by regulating lipids and metabolites; 2022. Available from: https://theses.lib.polyu.edu.hk/handle/200/12973.
32. Arora MK, Singh M, Tomar R, Singh L, Jangra A. Amla (Emblica officinalis) alleviates doxorubicin-induced cardiotoxicity and nephrotoxicity in rats. Pharmacol Res Modern Chin Med. 2024;11:100443. doi:10.1016/j.prmcm.2024.100443
33. Benzer F, Kandemir FM, Kucukler S, Comaklı S, Caglayan C. Chemoprotective effects of curcumin on doxorubicin-induced nephrotoxicity in Wistar rats: by modulating inflammatory cytokines, apoptosis, oxidative stress and oxidative DNA damage. Arch Physiol Biochem. 2018;124(5):448–457. doi:10.1080/13813455.2017.1422766
34. Abdelrahman AM, Al Suleimani YM, Manoj P, Ashique M, Ali BH, Schupp N. Effect of infliximab, a tumor necrosis factor-alpha inhibitor, on doxorubicin-induced nephrotoxicity in rats. Naunyn-Schmiedeberg’s Arch Pharmacol. 2020;393(1):121–130. doi:10.1007/s00210-019-01719-x
35. Lazzaroni E, Ben Nasr M, Loretelli C, et al. Anti-diabetic drugs and weight loss in patients with type 2 diabetes. Pharmacol Res. 2021;171:105782. doi:10.1016/j.phrs.2021.105782
36. Mohamed EA, Ahmed HI, Zaky HS. Protective effect of irbesartan against doxorubicin-induced nephrotoxicity in rats: implication of AMPK, PI3K/Akt, and mTOR signaling pathways. Can J Physiol Pharmacol. 2018;96(12):1209–1217. doi:10.1139/cjpp-2018-0259
37. Mohamed HK, Mobasher MA, Ebiya RA, et al. Anti-inflammatory, anti-apoptotic, and antioxidant roles of Honey, Royal Jelly, and propolis in suppressing nephrotoxicity induced by Doxorubicin in Male Albino rats. Antioxidants. 2022;11(5):1029. doi:10.3390/antiox11051029
38. Altinoz E, Oner Z, Elbe H, Uremis N, Uremis M. Linalool exhibits therapeutic and protective effects in a rat model of doxorubicin-induced kidney injury by modulating oxidative stress. Drug Chem Toxicol. 2022;45(5):2024–2030. doi:10.1080/01480545.2021.1894751
39. Ahmed AZ. Relationship between renal function tests and the levels of MDA, Zinc, and Cadmium among Painters in Sulaimani. IJPS. 2017;35–39. doi:10.31351/vol25iss2pp35-39
40. Khames A, Khalaf MM, Gad AM, Abd El-raouf OM, Kandeil MA. Nicorandil combats doxorubicin–induced nephrotoxicity via amendment of TLR4/P38 MAPK/NFκ-B signaling pathway. Chem Biol Interact. 2019;311:108777. doi:10.1016/j.cbi.2019.108777
41. Abd-Ellatif RN, Nasef NA, El-Horany HES, et al. Adrenomedullin Mitigates Doxorubicin-induced nephrotoxicity in rats: role of oxidative stress, inflammation, apoptosis, and pyroptosis. IJMS. 2022;23(23):14570. doi:10.3390/ijms232314570
42. Yaribeygi H, Maleki M, Sathyapalan T, Jamialahmadi T, Sahebkar A. Antioxidative potentials of incretin‐based medications: a review of molecular mechanisms. Oxid Med Cell Longev. 2021;2021(1):9959320. doi:10.1155/2021/9959320
43. Aziz TA, Kareem AA, Othman HH, Ahmed ZA. The anti-inflammatory effect of different doses of Aliskiren in rat models of inflammation. DDDT. 2020;14:2841–2851. doi:10.2147/DDDT.S255607
44. Wang Y, Wang Y, Wu Y, Wang Y. Dulaglutide ameliorates intrauterine adhesion by suppressing inflammation and epithelial–mesenchymal transition via inhibiting the TGF-β/Smad2 signaling pathway. Pharmaceuticals. 2023;16(7):964. doi:10.3390/ph16070964
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Telmisartan and Quercetin in 5 Fluorouracil-Induced Renal Toxicity in Rats

Ali HH, Ahmed ZA, Aziz TA
Journal of Inflammation Research 2022, 15:6113-6124
Published Date: 7 November 2022