")
Back to Journals » Journal of Pain Research » Volume 18
Effects of Electroacupuncture and Mecobalamin for Utidelon-Induced Peripheral Neuropathy in Breast Cancer Patients: A Randomized Controlled Clinical Trial
Authors Lu C , Shen Q, Deng D, Zhang Y, Wang P, Shao X, Deng Y, Bao W, Chen W, Li G
Received 5 March 2025
Accepted for publication 10 July 2025
Published 16 July 2025 Volume 2025:18 Pages 3593—3608
DOI https://doi.org/10.2147/JPR.S526405
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Amitabh Gulati
Chao Lu,1,* Qiongying Shen,2,* Dehou Deng,1,* Yajun Zhang,2 Peipei Wang,1 Xiying Shao,3 Yaping Deng,3 Wenlong Bao,1 Weiji Chen,4 Guangliang Li3
1Department of Traditional Chinese Medicine, Zhejiang Cancer Hospital, Hangzhou, People’s Republic of China; 2The Third Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 3Department of Breast Medical Oncology, Zhejiang Cancer Hospital, Hangzhou, People’s Republic of China; 4Department of Acupuncture and Moxibustion, The Third Affiliated Hospital of Zhejiang Chinese Medical University (Zhongshan Hospital of Zhejiang Province), Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guangliang Li; Chao Lu, Email [email protected]; [email protected]
Objective: The chemotherapy agent Utidelone (UTD1), as a novel option for drug-resistant breast cancer patients, is prone to cause severe neurotoxicity. This study aims to evaluate the clinical effects of electroacupuncture (EA) and Mecobalamin (MeCbl) in treating Utidelone-induced peripheral neuropathy (UIPN), providing preliminary evidence to optimize clinical management strategies.
Methods: A total of 60 eligible breast cancer patients with UIPN were randomly assigned in a 1:1 ratio to either the EA group or the MeCbl group. Evaluations were conducted after 4 weeks of treatment and again following a 4-week follow-up period (week 8). The primary outcome was the overall response rate of the Patient Neurotoxicity Questionnaire (PNQ), which was defined as a reduction of at least one grade in PNQ sensory or motor symptoms at week 4 compared to baseline. Secondary outcomes included the PNQ sensory, PNQ motor, and NCI-CTCAE grades, the EORTC QLQ-CIPN20 and QLQ-C30 scales.
Results: 28 of 30 participants in the EA group and 29 of 30 participants in the MeCbl group completed the study. The responder rate of PNQ overall in the EA group was significantly higher than that in the MeCbl group at week 4 (P=0.015) and at week 8 (P=0.01). EA group exhibited significant improvements in PNQ sensory, PNQ motor, and NCI-CTCAE grades compared to baseline at week 4 (all P< 0.05). EA treatment also demonstrated the ability to alleviate UIPN symptoms and improve the quality of life in several aspects, as indicated by the EORTC QLQ-CIPN20 and QLQ-C30 scales. There were no serious treatment-related adverse events in either group.
Conclusion: This randomized clinical trial indicated that EA therapy showed a potential benefit to alleviate symptoms of UIPN in breast cancer patients. Nevertheless, further research involving larger sample sizes and extended follow-up periods is warranted to elucidate these effects.
Trial registration: No. ChiCTR2200062741.
Keywords: electroacupuncture, EA, breast cancer, Utidelon-induced peripheral neuropathy, UIPN, Mecobalamin, MeCbl, randomized controlled trial
Introduction
Breast cancer ranks among the most prevalent malignant neoplasms in China and globally.1,2 Chemotherapy serves an irreplaceable role in the management of breast cancer, due to its remarkable efficacy in systemic treatment, particularly for advanced cancers. However, it often brings a series of adverse reactions that harm the physical and mental health of patients.3 Chemotherapy-induced peripheral neuropathy (CIPN) is a difficult clinical problem that warrants significant attention.
Utidelone (UTD1) is a chemotherapy drug primarily used to treat patients with advanced metastatic breast cancer. It belongs to a novel class of non-taxane anti-microtubule polymerization antitumor agents. The antitumor mechanism of utidelone involves binding to microtubule proteins, which prevents cancer cells from undergoing normal mitosis, thereby inducing apoptosis in the cancer cells.4 Previous studies have demonstrated that UTD1 combined with capecitabine chemotherapy could extend survival by approximately four months compared to capecitabine monotherapy.5,6 However, a prominent side effect of UTD1 is inducing severe peripheral neuropathy (UIPN).7 The incidence of peripheral neuropathy (PN) associated with UTD1 in conjunction with capecitabine is reported to be 85.4%, with the occurrence of grade 3 CIPN reaching as high as 25.1%, in stark contrast to an incidence of 9.2% for CIPN with capecitabine alone, where the incidence of grade 3 CIPN is less than 1%.5 UIPN not only precipitates severe numbness in patients’ hands and feet, but also manifests as soreness, pain, or weakness in the limbs. Some patients even reduce or withdraw chemotherapy due to severe UIPN, which affects the progress of anti-tumor treatment. Currently, effective prevention and therapeutic strategies for UIPN remain scarce in clinical practice, and pertinent research is also limited. Neuroprotective agents or nutritive agents, antioxidants, antiepileptic drugs, etc. are commonly used but may have unsatisfactory efficacy or side effects.8,9
Acupuncture has emerged as a significant modality in the management of cancer-related diseases, especially those arising from chemotherapeutic agents.3,10 Previous studies have validated its efficacy in treating PN caused by various diseases, demonstrating improvements in peripheral nerve conduction velocity and alleviating sensory abnormalities or limb pain in affected patients.11,12 Additionally, acupuncture has shown potential in ameliorating neuropathic symptoms associated with CIPN.13,14 Electroacupuncture (EA), which combines electrical stimulation with traditional acupuncture can promote nerve regeneration through multiple mechanisms in the treatment of neurological-related diseases15 and cancer-related diseases.16 EA may facilitate the repair of damaged nerves by regulating the regeneration and function of Schwann cells. Schwann cells play a crucial role in the regeneration process following peripheral nerve injury.17 In addition, EA stimulation may further support nerve regeneration by promoting the expression of nerve growth factors and improving local blood circulation.18 EA has been suggested to be a potential therapeutic intervention for CIPN, as per guidelines, although larger-scale studies are required to confirm.19 Mecobalamin (MeCbl) is an endogenous vitamin B12 involved in the synthesis of thymidine during deoxyribonucleic acid synthesis, thereby promoting nucleic acid and protein synthesis. It also facilitates axonal transport, axonal regeneration, and myelin sheath formation, contributing to the repair of damaged nerve tissue. As a neuroprotective agent, it has been suggested to be beneficial in improving peripheral nerve symptoms20 and recommended as a medium evidence drug for preventing CIPN in the China clinical guidelines. Numerous clinical studies have indicated that MeCbl can improve symptoms of peripheral neuropathy21,22 and is regarded as a safe, effective, and well-tolerated drug in treating CIPN.23–25 However, the efficacy of MeCbl for UIPN is unclear. Accordingly, we designed this randomized clinical trial to explore the effects of EA and MeCbl for UIPN in breast cancer patients.
Methods
Study Design
This single-center, randomized, controlled study was conducted at Zhejiang Cancer Hospital from September 1, 2022, to January 31, 2025. The study adhered to the principles of the Declaration of Helsinki26 and was approved by the Medical Ethics Committee of Zhejiang Cancer Hospital (license number IRB-2022-425). Written informed consent was obtained from all participating patients. The study followed the Consolidated Standards of Reporting Trials (CONSORT) reporting guideline and the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) guideline.27 The study was registered in the Chinese Clinical Trial Registry (17/08/2022, https://www.chictr.org.cn/, ChiCTR2200062741).
Participants
Female breast cancer patients aged 18 to 70 years with CIPN symptoms were screened for the following: diagnosis of CIPN, the National Cancer Institute-Common Terminology Criteria for Adverse Events Version 5.0 (NCI-CTCAE) grade I or higher occurred after receiving chemotherapy drugs of UTD1.
Patients were included with the following inclusion criteria: No obvious symptoms of peripheral neuropathy before using UTD1; Ability to perform daily living activities and cooperate in completing all examinations independently; No serious heart, brain, liver, and kidney diseases and Karnofsky functional status score (KPS) greater than 70; No mental illness or cognitive impairment; No use any analgesics in the two weeks preceding the study; Voluntary participation and signed the written informed consent.
Exclusion criteria included: Severe hemorrhagic disorders, severe infections, or severe cardiogenic/renal edema; Severe mental disorders or cognitive impairment; Diabetic peripheral neuropathy, traumatic peripheral nerve injury, or HIV-associated neuropathy; Pregnant and lactating women; Alcohol and/or other drug abuse or dependent; Participating in other clinical trials within the preceding 4 weeks.
Randomization
Eligible patients were randomly assigned to receive EA or MeCbl treatment in a ratio of 1:1 by using the envelope randomization method. The randomization method was employed to generate two groups of allocation sequences consisting of 60 non-repeating numbers. The two groups of random serial numbers were randomly placed in opaque sealed envelopes by an independent researcher to ensure the concealment of distribution. Each envelope was sequentially numbered and contained the screening sequence number of participants on the outside, while the randomly assigned groups were indicated on the inside. The envelope was opened corresponding to the subject’s visit order.
Blinding
Due to the significant difference between EA and MeCbl treatment, acupuncturists and participants could not be blinded to the group assignments. However, they were not involved in the outcome assessments or data analyses. Other researchers, including the statisticians, outcome assessors, and data analysts, were all blinded to the group assignments.
Interventions
Patients in the EA group received twelve 30-minute sessions of EA treatment, once every other day (3 times a week) for 4 consecutive weeks. The acupuncture treatments were administered by two licensed acupuncturists, each with a minimum of 8 years of clinical experience. Prior to the study commencement, both practitioners underwent standardized training on the study protocol and passed a qualification assessment to ensure treatment consistency and quality control throughout the trial.
For patients with UIPN symptoms in the upper limbs, the acupoints selected were Quchi (LI11), Waiguan (TE5), Hegu (LI4), Houxi (SI3), and Baxie (EX-UE9) bilaterally. EA was connected between Quchi (LI11) and Waiguan (TE5) points. For lower limbs symptoms, the acupoints chosen were Yanglingquan (GB34), Zusanli (ST36), Yinlingquan (SP9), Sanyinjiao (SP6), Taichong (LR3), and Bafeng (EX-LE10) points bilaterally. EA was connected between Yanglingquan (GB34) and Sanyinjiao (SP6) points (Figure 1). If patients with UIPN symptoms in all limbs, both the upper and lower limb acupoints were selected and the EA treatment method mentioned above was applied. The location of all selected acupoints followed the national standards of China (GB/T 123456–2021) as outlined in the trial protocol.28 The above-mentioned acupoints were routinely punctured with disposable acupuncture needles, with a depth ranging from 1 cm to 3.5 cm. The EA frequency was 2Hz and the stimulation intensity ranged from 0.5 to 4 mA, based on the patient’s tolerance, with clear feeling, but no discomfort. All the patients were followed up for 4 weeks after the last intervention. (The acupuncture needles were Hwato brand needles produced by Suzhou Medical Apparatus Plant, with a model of 0.25 * 40mm. The EA equipment adopted the HANS acupoint nerve stimulator, model HANS-200E, produced by Nanjing Jisheng Medical Technology Co., Ltd).
 |
Figure 1 Location of acupoints. |
Patients in the MeCbl group received treatment with MeCbl tablets orally (produced by Misato Plant of Eisai Co., Ltd). They were instructed to take 0.5 mg at a time, three times daily, a total of 1.5 mg a day for 4 consecutive weeks. And were also followed up for 4 weeks after the last intervention.
Outcomes
The primary outcome was the overall response rate of the Patient Neurotoxicity Questionnaire (PNQ), which was defined as a decline of at least one grade in either PNQ sensory or motor symptoms at week 4 compared to baseline. The scale of PNQ is a questionnaire for diagnosis and quantification of CIPN in cancer patients,29,30 which most widely used assessment for peripheral neuropathy.14,31 It evaluates both sensory and motor nerve functions, grading symptoms from grade A (no neuropathy) to grade E (very severe neuropathy). Additionally, we also analyzed the sustained response, defined as patients maintaining at least a one-grade decline in symptoms from baseline at week 8.
Secondary outcomes included changes in PNQ sensory, PNQ motor, and NCI-CTCAE grades over time, which were construed as a comparison to the baseline within each group and also a comparison between the two groups at different time points. The NCI-CTCAE grade ranges from grade I (slight) to grade IV (severe)32 and was assessed by a professional neurologist. The secondary outcomes also included the change of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-CIPN 20-item (EORTC QLQ-CIPN20) scale33 and the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30 (EORTC QLQ-C30) scale.34 These two scales were linearly converted into standardized scores ranging from 0 to 100 for comparative analysis.35
All kinds of adverse reactions were recorded during the study period, including the occurrence time, manifestations, treatment measures, results, and follow-up, and indicated whether the participant withdrew from the trial. Additionally, if patients required analgesics for pain management during the study, the type and dosage of the medication were recorded.
Sample Size
This was a pilot exploratory study. The sample size calculation was based on the research by Sam,36 which suggested that a minimum of 25 participants per group is required to detect a medium effect size. Considering a potential dropout rate of 15% and a 1:1 allocation ratio between groups, the adjusted sample size was calculated to be 30 participants per group, resulting in a total of 60 participants.
Statistical Analysis
De-identified outcome data were analyzed by a statistician who was blinded to group allocations, utilizing the SPSS statistical software (Version 26.0, IBM, USA). Baseline characteristics were described as mean (standard deviation, SD) or median (interquartile range, IQR) for continuous variables and frequencies and percentages for discrete variables. The analysis was based on the intention-to-treat (ITT) principle, including all randomized patients with baseline data. The response rate of PNQ and NCI-CTCAE, the use of analgesics, and the incidence of adverse events were evaluated with the chi-square test, nonparametric test, or Fisher’s exact test described by frequencies and percentages. Pairwise analysis was performed using an adjusted Bonferroni or nonparametric test. For EORTC QLQ-CIPN20 and QLQ-C30 scales scores, independent t-test was used to analyze the differences for continuous variable data that conforms to a normal distribution between groups. Paired t-tests were used to analyze differences from baseline after intervention and during the follow-up period. For continuous variable data that did not follow a normal distribution, nonparametric test or Fisher’s exact test was used to compare within-group and between-group comparisons. All statistical analyses were two-sided tests and the level of significance was established at 0.05. Data were analyzed from February 2025 to May 2025.
Results
From September 1, 2022, to January 31, 2025, we screened 131 participants, and 71 were excluded due to various reasons (detailed in Figure 2). A total of 60 participants (mean [SD] age, 54.2 [8.8] years; all women [100%]) were enrolled and randomly assigned to receive either EA or MeCbl treatment, with 30 in each group, all delivered baseline data. Among the randomized participants, 28 (93.3%) in the EA group completed the study, and 29 (96.7%) in the MeCbl group completed the study. The study flow chart was shown in Figure 2. Baseline characteristics were similar between groups, as shown in Table 1.
 |
Table 1 Baseline Characteristics of Participants in ITT Analysis |
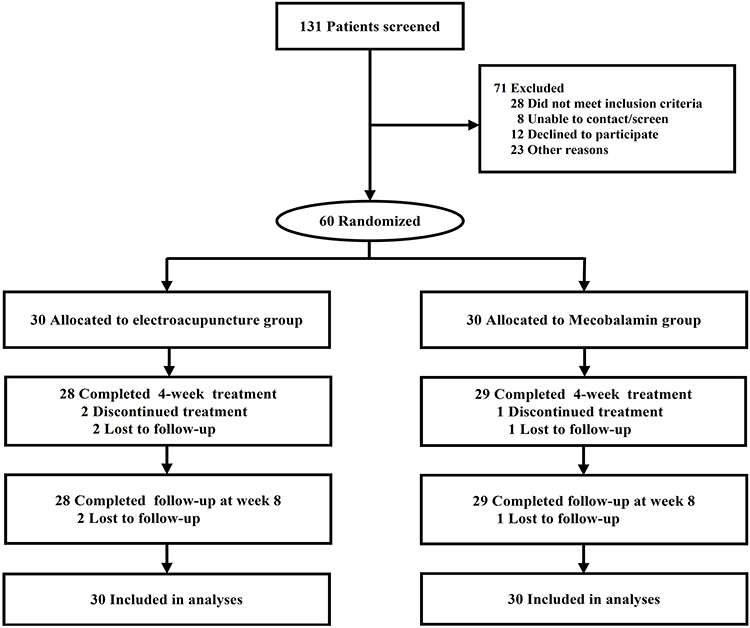 |
Figure 2 Flow chart of the study process. |
For the primary outcome, 16/30 (53.3%) participants in the EA group and 6/30 (20.0%) participants in the MeCbl group declined at least one grade in PNQ sensory or motor symptoms at week 4 compared to baseline, and 14/30 (46.7%) participants in the EA group and 4/30 (13.3%) participants in the MeCbl group still declined at week 8. The responder rate of PNQ overall in the EA group was significantly higher than that in the MeCbl group at week 4 (EA, 53.3% [95% CI, 34.3% to 71.7%] vs MeCbl, 20.0% [95% CI, 7.7% to 38.6%]; P=0.015), and this difference still persisted at week 8 (EA, 46.7% [95% CI, 28.3% to 65.7%] vs MeCbl, 13.3% [95% CI, 3.8% to 30.7%]; P=0.01). Shown in Figure 3.
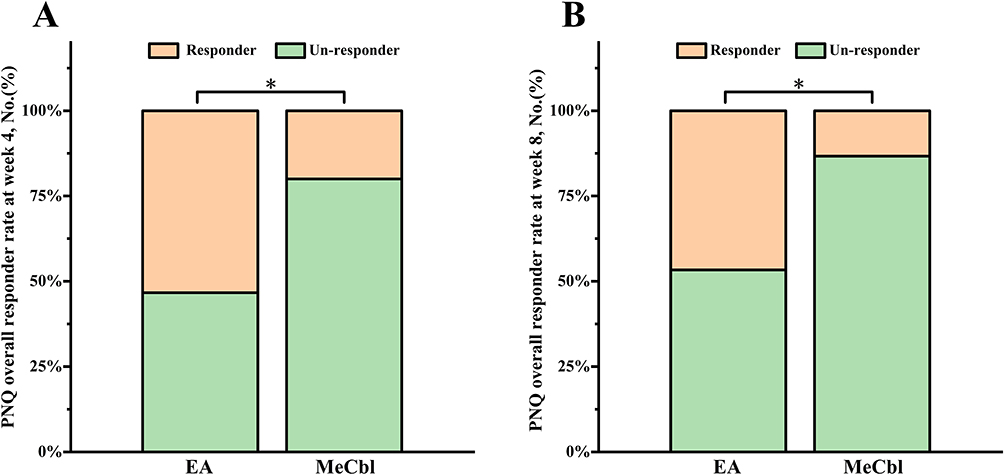 |
Figure 3 The primary outcome of PNQ response rate. (A) PNQ overall responder rate at week 4; (B) PNQ overall responder rate at week 8. Bonferroni was used to compare and adjust P-values. *implies a statistical difference compared to baseline data within the same group. Abbreviations: PNQ, Participant Neurotoxicity Questionnaire; EA, Electroacupuncture; MeCbl, Mecobalamin. |
For the secondary outcomes, the EA group showed significant improvements in the PNQ sensory, PNQ motor, and NCI-CTCAE grades compared to baseline at week 4 (PNQ sensory, Z=−2.887, P=0.004; PNQ motor, Z=−2.887, P=0.006; NCI-CTCAE, Z=−2.496, P=0.02;), while the MeCbl group did not show significant changes over time. Additionally, there were no significant differences observed between the two groups at all time points (Figure 4).
 |
Figure 4 Change in PNQ and NCI-CTCAE grades over time. (A) PNQ sensory grade; (B) PNQ motor grade; (C) NCI-CTCAE grade. Fisher’s exact test was used to compare and adjust P-values. * implies a statistical difference compared to baseline data within the same group. Abbreviations: PNQ, Participant Neurotoxicity Questionnaire; NCI-CTCAE, National Cancer Institute-Common Terminology Criteria for Adverse Events; EA, Electroacupuncture; MeCbl, Mecobalamin. |
The QLQ-CIPN20 in total score, sensory, motor and autonomic scores declined significantly in the EA group at week 4 (compared to baseline, total score, 7.65 [95% CI, 5.19 to 10.11], P<0.001; sensory score, 7.53 [95% CI, 4.85 to 10.21], P<0.001; motor score, 7.14 [95% CI, 4.20 to 10.09], P<0.001; autonomic score, 10.00 [95% CI, 4.68 to 15.32], P=0.001), and still declined at week 8 (compared to baseline, total score, 4.63 [95% CI, 1.94 to 7.32], P=0.001; sensory score, 4.44 [95% CI, 1.55 to 7.34], P=0.004; motor score, 4.29 [95% CI, 1.04 to 7.53], P=0.011; autonomic score, 6.67 [95% CI, 0.87 to 12.47], P=0.026). While the MeCbl group only showed a decrease in QLQ-CIPN20 total score at week 4 (compared to baseline, total score, 2.84 [95% CI, 0.19 to 5.49], P=0.037). Another hand, the QLQ-C30 score in physical function, cognitive function, and fatigue symptom improved significantly in the EA group at week 4 (compared to baseline, physical function, 8.44 [95% CI, 3.92 to 12.97], P=0.001; cognitive function, 5.56 [95% CI, 1.13 to 9.98], P=0.016; fatigue, 8.15 [95% CI, 1.53 to 14.77], P=0.018), and physical function still improved at week 8 (compared to baseline, physical function, 5.56 [95% CI, 0.36 to 10.75], P=0.037). However, there were no significant changes in the score of the QLQ-C30 scale in the MeCbl group when compared to the baseline. There was also no significant difference in QLQ-CIPN20 and C30 scores between the two groups at week 4 and week 8 (Figure 5).
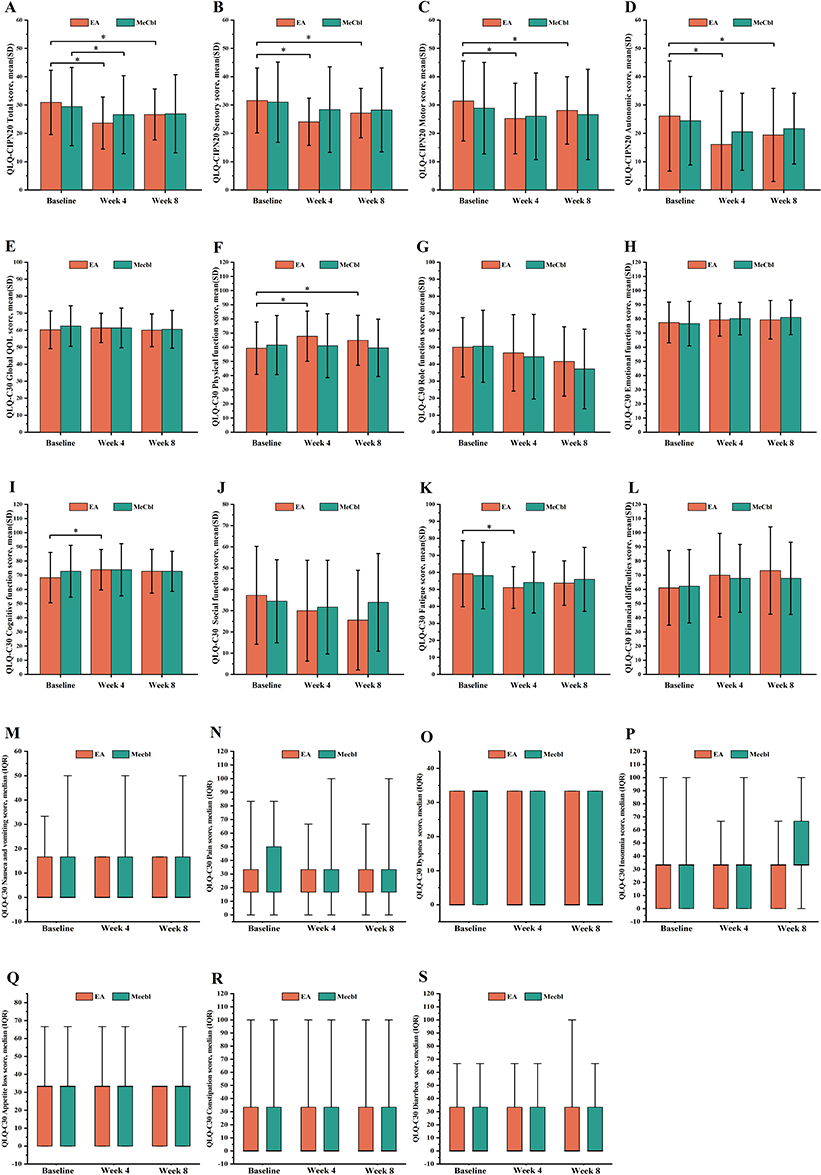 |
Figure 5 Changes in EORTC QLQ-CIPN20 & C30 scores over time. (A) QLQ-CIPN20 Total score; (B) QLQ-CIPN20 Sensory score; (C) QLQ-CIPN20 Motor score; (D) QLQ-CIPN20 Autonomic score; (E) QLQ-C30 Global quality of life score; (F) QLQ-C30 Physical function score; (G) QLQ-C30 Role function score; (H) QLQ-C30 Emotional function score; (I) QLQ-C30 Cognitive function score; (J) QLQ-C30 Social function score; (K) QLQ-C30 Fatigue score; (L) QLQ-C30 Financial difficulties score; (M) QLQ-C30 Nausea and vomiting score; (N) QLQ-C30 Pain score; (O) QLQ-C30 Dyspnea score; (P) QLQ-C30 Insomnia score; (Q) QLQ-C30 Appetite loss score; (R) QLQ-C30 Constipation score; (S) QLQ-C30 Diarrhea score. Data that conforms to a normal distribution is represented by mean and standard deviation (A–L). The highest of the bar chart represents the mean value and the vertical line indicates the standard deviation. Data that does not follow a normal distribution is represented by the median and interquartile range (M–S). The bold horizontal line in the boxplot represents the median, the low bottom of the box represents the 25% interval value, and the top bottom represents the 75% interval value. The low bottom of the vertical line represents the minimum value, and the top of the vertical line represents the maximum value. *implies a statistical difference compared to baseline data within the same group. Abbreviations: EORTC QLQ-CIPN20 & C30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-chemotherapy-induced peripheral neuropathy 20-item and Core 30; EA, Electroacupuncture; MeCbl, Mecobalamin; SD, standard deviation; IQR, interquartile range. |
In addition, we also compared the change scores from baseline in QLQ-CIPN20 and C30 scales to further analyze the differences in the effects of EA and MeCbl treatment. The result showed that the EA group had better improvements in the QLQ-CIPN20 total score and sensory score compared to the MeCbl group at week 4 (EA vs MeCbl, total score, Z=−2.931, P=0.003; sensory score, Z=−2.548, P=0.01); and the EA group had better improvement in the QLQ-C30 physical function score compared to the MeCbl group at week 4 (EA vs MeCbl, Z=−2.528, P=0.011) and week 8 (EA vs MeCbl, Z=−2.279, P=0.022). Shown in Figure 6.
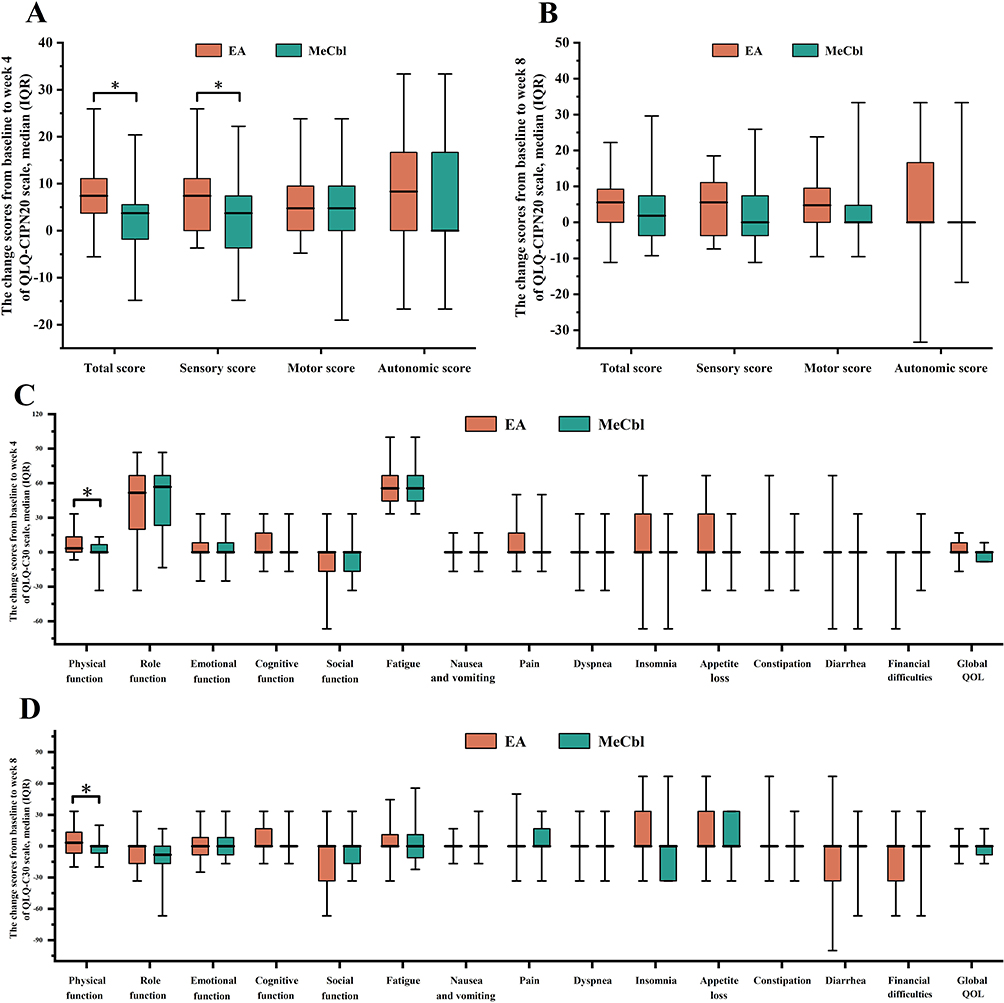 |
Figure 6 The change scores in EORTC QLQ-CIPN20 & C30 scales from baseline to week 4 and week 8. (A) The change score from baseline to week 4 of QLQ-CIPN20 scale; (B) The change score from baseline to week 8 of QLQ-CIPN20 scale; (C) The change score from baseline to week 4 of QLQ-C30 scale; (D) The change score from baseline to week 8 of QLQ-C30 scale. Data that does not follow a normal distribution is represented by the median and interquartile range. The bold horizontal line in the boxplot represents the median, the low bottom of the box represents the 25% interval value, and the top bottom represents the 75% interval value. The low bottom of the vertical line represents the minimum value, and the top of the vertical line represents the maximum value. *implies a statistical difference compared to MeCbl group. Abbreviations: EORTC QLQ-CIPN20 & C30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-chemotherapy-induced peripheral neuropathy 20-item and Core 30; EA, Electroacupuncture; MeCbl, Mecobalamin; SD, standard deviation; IQR, interquartile range; QOL, quality of life. |
During the study period, 8/30 (26.7%) participants in the EA group and 7/30 (23.3%) participants in the MeCbl group used analgesics, with no difference between groups (EA, 16.7% [95% CI, 5.6% to 34.7%] vs MeCbl, 23.3% [95% CI, 9.9% to 42.3%], P=0.748). Adverse events also occurred similarly in frequencies in the two groups (EA, 30.0% [95% CI,14.7% to 49.4%] vs MeCbl, 10.0% [95% CI, 2.1% to 26.5%]; P=0.104). EA-related treatment mainly resulted in pain, subcutaneous bruising, or slight bleeding. The MeCbl group mainly occurs in other events (Supplementary Table 1).
Discussion
In this randomized clinical trial comparing the effects of EA and MeCbl treatment for UIPN in breast cancer patients, both therapies could reduce CIPN-related scale scores and relieve numbness and pain symptoms in limbs after 4 weeks of treatment. However, EA therapy demonstrated superior efficacy compared to oral MeCbl tablets. Both therapies were delivered safely with only mild adverse events.
CIPN is a neurological disorder caused by direct damage to peripheral nerves from chemotherapy agents. Commonly associated drugs include platinum compounds, vinblastine, paclitaxel, and others.37,38 Symptoms of CIPN often include numbness in the limbs, sensory abnormalities (such as stabbing pain, electric shock sensations, crawling sensations, and the feeling of a foreign body, etc)., as well as decreased tendon reflexes and sensory ataxia.19 The underlying mechanisms of CIPN are not yet fully understood, but they may involve several factors, including oxidative stress responses triggered by chemotherapeutic agents, damage to nuclear and mitochondrial DNA, disruption of ion channels, and axonal degeneration.19 UTD1, a novel microtubule inhibitor derived from epomycin through genetic engineering, demonstrates broad anti-tumor activity in various solid tumors.39 However, there is still a notable lack of effective prevention and treatment strategies for UIPN. Only one study40 has suggested that ganglioside monosialic acid GM1 might alleviate symptoms of UIPN in patients with metastatic breast cancer, but further studies are warranted to corroborate these findings. Given the pressing need for effective treatment options to improve the quality of life for advanced cancer patients suffering from UIPN, our trial seeks to explore the clinical efficacy of EA and MeCbl for this purpose. To enhance the potential efficacy of acupuncture, we specifically selected high-frequency acupoints known to be effective for treating CIPN based on existing literature41 and consultations with professional acupuncturists to optimize the combination of acupoints used in our study. This approach aims to provide a more targeted and effective intervention for patients experiencing UIPN.
In this trial, we found that EA therapy significantly reduced the PNQ sensory and motor nerve symptoms grades after 4 weeks of treatment, while MeCbl did not demonstrate comparable efficacy. Although there was no difference between the two groups at any time point, the overall responder rate of PNQ was markedly higher in the EA group than in the MeCbl group. Furthermore, EA therapy led to a significant reduction in both the NCI-CTCAE grade and the QLQ-CIPN20 scores. Numerous animal experiments have suggested that EA therapy possesses potential therapeutic benefits for CIPN. For instance, Meng, et al42 reported that EA therapy effectively inhibited mechanical allodynia and hyperalgesia in a rat model of paclitaxel-induced peripheral neuropathy, through mechanisms involving spinal opioid receptors. Similarly, Zhang, et al43 discovered that low-frequency EA could activate 5-HT 1A receptors in the spinal cord and inhibit p-CaMKII to alleviate both allodynia and hyperalgesia associated with paclitaxel-induced peripheral neuropathy in rats. In our previous clinical research,44 we observed that low-frequency (2Hz) EA therapy had better advantages for treating paclitaxel-induced peripheral neuropathy in breast cancer patients. Additionally, Chan, et al45 indicated that low-frequency EA could effectively reduce symptoms associated with oxaliplatin-induced peripheral neuropathy in patients with colorectal cancer. While, the mechanisms by which electroacupuncture improves nerve injury-like disorders are currently unclear. Electrical stimulation may enhance nerve repair by modulating miRNA,46 it has been shown that electroacupuncture can significantly increase the number of myelinated fibers, axonal and fiber diameters, and the thickness of the myelin sheath in our rat model of sciatic nerve injury.47 In addition, we observed that MeCbl alleviated some symptoms of UIPN), as measured by the QLQ-CIPN20 scale, when compared to baseline; however, its overall efficacy was limited. Zhang, et al48 demonstrated that high-dose intravenous MeCbl exhibited marked efficacy in the prophylaxis of bortezomib-induced peripheral neuropathy without causing serious adverse effects. Furthermore, Hiramoto, et al49,50 indicated that although evidence supporting the efficacy of MeCbl is insufficient, it remains a commonly used treatment for preventing and managing peripheral neuropathy induced by paclitaxel and oxaliplatin in Japan. Based on our findings, MeCbl may be appropriate for patients with mild UIPN but is not recommended for those exhibiting severe UIPN symptoms due to its limited therapeutic impact.
According to the QLQ-C30 scale, EA therapy not only alleviates patients’ UIPN symptoms but also enhances their quality of life in several dimensions. The result indicate that EA therapy provides a significantly greater improvement in physical function compared to oral MeCbl tablets. Physical function encompasses everyday activities such as walking, lifting, and other daily tasks. Improvements in physical function are associated with enhanced peripheral nerve function in the extremities, thus, as UIPN symptoms improve, EA therapy can yield favorable therapeutic outcomes. Chan, et al45 reported that low-frequency EA positively impacted physical, cognitive, and social functions in colorectal cancer patients experiencing CIPN. Similarly, Mao, et al51 demonstrated that 2Hz EA significantly alleviated symptoms of fatigue, sleep disturbances, and psychological distress in breast cancer patients suffering from aromatase inhibitor-related arthralgia when compared to usual care. These studies collectively suggest that EA offers benefits in improving the quality of life for cancer patients from several aspects. Conversely, our results did not show a definitive effect of EA on pain symptoms. This lack of clarity may be attributed to the fact that many patients in both groups were concurrently taking analgesics during the study period due to peripheral neuralgia or other forms of pain, and there was no significant difference in analgesic use between the two groups. Additionally, EA was generally well tolerated, as only a few patients reported minor adverse events, such as needle discomfort, subcutaneous hematoma, and slight bleeding, all of which resolved quickly.
During the follow-up phase, we noted that the symptoms of UIPN and quality of life of patients were significantly worse than they were after treatment. This decline is likely attributed to the fact that most participants had advanced breast cancer and were undergoing continuous chemotherapy as part of their anti-tumor regimen. For early-stage breast cancer patients who had completed UTD1 chemotherapy treatment appeared to derive more substantial benefits from EA therapies, with significant improvements observed in their UIPN symptoms following a period of treatment. However, for advanced breast cancer patients undergoing continuous chemotherapy, the effects of EA were comparatively poor. Nonetheless, EA therapy still demonstrated the capability to alleviate certain symptoms, such as limb numbness, pain, and weakness, to some extent. Additionally, it appeared to help maintain the patient’s current symptom levels, potentially preventing the further deterioration of UIPN symptoms.
Limitations
This trial had several limitations that should be acknowledged. First, it was a single-center study with a relatively small sample size in each treatment group, which may limit the generalizability of the results. Second, while sham EA controls are widely adopted in contemporary acupuncture research,52 this exploratory pilot study intentionally omitted such a control group due to its preliminary nature. However, we acknowledge that the absence of a sham EA arm limits our capacity to differentiate the specific effects of EA from those of manual acupuncture, representing an important limitation in the current study design. Third, the acupuncturists were not blinded to group assignments due to the nature of the treatment procedures, which could introduce bias. Additionally, the outcomes relied on subjective reporting from participants, which raises the possibility of reporting bias. While incorporating objective measures, such as nerve conduction velocity (NCV), could have strengthened the data, patient reluctance to undergo such testing limited its inclusion. Considering ethical principles, patients were not required to complete NCV testing. Finally, the observation period of the study was relatively short, consisting of only 4 weeks of treatment followed by 4 weeks of follow-up. This limited timeframe precluded any assessment of the long-term effects of EA. Another important limitation is that the number of prior treatment lines in multi-line chemotherapy may serve as a significant confounding factor influencing both the development of peripheral neuropathy and the therapeutic efficacy of interventions. However, since the study design did not systematically document patients’ specific chemotherapy lines and medication history, we were unable to perform stratified analysis or subgroup comparisons for this potential influencing factor. This methodological limitation may affect the accurate assessment of the true treatment effects of the interventions. Despite these limitations, the findings from this trial provide valuable insights and can serve as a reference for future clinical research and treatment of UIPN.
Conclusions
This randomized clinical trial demonstrated that EA therapy showed potential superiority over MeCbl tablets in alleviating symptoms of UIPN and improving physical function in breast cancer patients. However, further large-scale, multicenter studies incorporating sham controls and long-term follow-up are needed to definitively establish its therapeutic effects.
Abbreviations
UTD1, Utidelon; PN, Peripheral Neuropathy; UIPN, Utidelon-induced Peripheral Neuropathy; EA, Electroacupuncture; MeCbl, Mecobalamin; ITT, Intention-to-Treat; PNQ, Patient Neurotoxicity Questionnaire; NCI-CTCAE, National Cancer Institute-Common Terminology Criteria for Adverse Events; EORTC QLQ-CIPN20, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-CIPN 20-item; EORTC QLQ-C30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study adhered to the principles of the Declaration of Helsinki and was approved by the Medical Ethics Committee of Zhejiang Cancer Hospital (license number IRB-2022-425). Written informed consent was obtained from all participating patients. The study was registered in the Chinese Clinical Trial Registry (17/08/2022, https://www.chictr.org.cn/,ChiCTR2200062741).
Acknowledgment
We thank all the participants and collaborators who contributed to this study, especially Professor Jiaoqiao Fang, Zhejiang Chinese Medical University, for providing constructive advice, with no compensation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work was supported by the Program of Science Research Foundation of Zhejiang Provincial TCM Administration (No. 2022ZB058, No.2023ZL019 and No.2025ZL207). The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Xia C, Dong X, Li H, et al. Cancer statistics in China and United States, 2022: profiles, trends, and determinants. Chin Med J. 2022;135(5):584–590. doi:10.1097/CM9.0000000000002108
3. Han G, Lee YS, Jang HJ, Kim SY, Lee YJ, Ha IH. Symptom management and quality of life of breast cancer patients using acupuncture-related therapies and herbal medicine: a scoping review. Cancers. 2022;14(19):4683. doi:10.3390/cancers14194683
4. Zhang P, Tong Z, Tian F, et al. Phase II trial of utidelone as monotherapy or in combination with capecitabine in heavily pretreated metastatic breast cancer patients. J Hematol Oncol. 2016;9(1):68. doi:10.1186/s13045-016-0297-7
5. Xu B, Sun T, Zhang Q, et al. Efficacy of utidelone plus capecitabine versus capecitabine for heavily pretreated, anthracycline- and taxane-refractory metastatic breast cancer: final analysis of overall survival in a phase III randomised controlled trial. Ann Oncol. 2021;32(2):218–228. doi:10.1016/j.annonc.2020.10.600
6. Zhang P, Sun T, Zhang Q, et al. Utidelone plus capecitabine versus capecitabine alone for heavily pretreated metastatic breast cancer refractory to anthracyclines and taxanes: a multicentre, open-label, superiority, phase 3, randomised controlled trial. Lancet Oncol. 2017;18(3):371–383. doi:10.1016/S1470-2045(17)30088-8
7. Zhang P, Sun M, Qiu R, Tang L, Dou G, Xu B. Phase I clinical and pharmacokinetic study of UTD1, a genetically engineered epothilone analog in patients with advanced solid tumors. Cancer Chemother Pharmacol. 2011;68(4):971–978. doi:10.1007/s00280-011-1571-6
8. Hou S, Huh B, Kim HK, Kim HK, Abdi S. Treatment of chemotherapy-induced peripheral neuropathy: systematic review and recommendations. Pain Physician. 2018;21(6):571–592.
9. Hu LY, Mi WL, Wu GC, Wang YQ, Mao-Ying QL. Prevention and treatment for chemotherapy-induced peripheral neuropathy: therapies based on CIPN mechanisms. Curr Neuropharmacol. 2019;17(2):184–196. doi:10.2174/1570159X15666170915143217
10. Zhao YX, Yu XC, Gao JH, Yao MJ, Zhu B. Acupuncture for paclitaxel-induced peripheral neuropathy: a review of clinical and basic studies. J Pain Res. 2021;14:993–1005. doi:10.2147/JPR.S296150
11. Schröder S, Liepert J, Remppis A, Greten JH. Acupuncture treatment improves nerve conduction in peripheral neuropathy. Eur J Neurol. 2007;14(3):276–281. doi:10.1111/j.1468-1331.2006.01632.x
12. Dimitrova A, Murchison C, Oken B. Acupuncture for the treatment of peripheral neuropathy: a systematic review and meta-analysis. J Altern Complement Med. 2017;23(3):164–179. doi:10.1089/acm.2016.0155
13. Bao T, Patil S, Chen C, et al. Effect of acupuncture vs sham procedure on chemotherapy-induced peripheral neuropathy symptoms: a randomized clinical trial. JAMA Network Open. 2020;3(3):e200681–e200681. doi:10.1001/jamanetworkopen.2020.0681
14. Lu W, Giobbie-Hurder A, Freedman RA, et al. Acupuncture for chemotherapy-induced peripheral neuropathy in breast cancer survivors: a randomized controlled pilot trial. Oncologist. 2020;25(4):310–318. doi:10.1634/theoncologist.2019-0489
15. Zhao ZQ. Neural mechanism underlying acupuncture analgesia. Prog Neurobiol. 2008;85(4):355–375. doi:10.1016/j.pneurobio.2008.05.004
16. Mao JJ, Liou KT, Baser RE, et al. Effectiveness of electroacupuncture or auricular acupuncture vs usual care for chronic musculoskeletal pain among cancer survivors: the PEACE randomized clinical trial. JAMA Oncol. 2021;7(5):720–727. doi:10.1001/jamaoncol.2021.0310
17. Tan C, Yang C, Liu H, Tang C, Huang S. Effect of Schwann cell transplantation combined with electroacupuncture on axonal regeneration and remyelination in rats with spinal cord injury. Anatomical Record. 2021;304(11):2506–2520. doi:10.1002/ar.24721
18. Fei J, Gao L, Li HH, Yuan QL, Li LJ. Electroacupuncture promotes peripheral nerve regeneration after facial nerve crush injury and upregulates the expression of glial cell-derived neurotrophic factor. Neu Regener Res. 2019;14(4):673–682. doi:10.4103/1673-5374.247471
19. Loprinzi CL, Lacchetti C, Bleeker J, et al. Prevention and management of chemotherapy-induced peripheral neuropathy in survivors of adult cancers: ASCO guideline update. J Clin Oncol. 2020;38(28):3325–3348. doi:10.1200/JCO.20.01399
20. Zhang D, Yang W, Wang C, et al. Methylcobalamin-Loaded PLCL Conduits Facilitate the Peripheral Nerve Regeneration. Macromol Biosci. 2020;20(3):e1900382. doi:10.1002/mabi.201900382
21. Han Y, Wang M, Shen J, et al. Differential efficacy of methylcobalamin and alpha-lipoic acid treatment on symptoms of diabetic peripheral neuropathy. Minerva Endocrinologica. 2018;43(1):11–18. doi:10.23736/S0391-1977.16.02505-0
22. Sawangjit R, Thongphui S, Chaichompu W, Phumart P. Efficacy and safety of mecobalamin on peripheral neuropathy: a systematic review and meta-analysis of randomized controlled trials. J Altern Complement Med. 2020;26(12):1117–1129. doi:10.1089/acm.2020.0068
23. Huang H, Zhao M, Liu X, et al. Glutathione combined with mecobalamin in the treatment of chemotherapy-induced peripheral neuropathy in multiple myeloma: a retrospective clinical study. Ann Palliat Med. 2021;10(12):12335–12346. doi:10.21037/apm-21-3313
24. Li Y, Gu J, Yu Q. Efficacy of mecobalamin tablets combined with troxerutin in the treatment of NSCLC chemotherapy-induced peripheral neuropathy. Evid-Based Complement Alternat Med. 2022;2022:7946934. doi:10.1155/2022/7946934
25. Schloss JM, Colosimo M, Airey C, Masci P, Linnane AW, Vitetta L. A randomised, placebo-controlled trial assessing the efficacy of an oral B group vitamin in preventing the development of chemotherapy-induced peripheral neuropathy (CIPN). Support Care in Cancer. 2017;25(1):195–204. doi:10.1007/s00520-016-3404-y
26. World Medical Association. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
27. MacPherson H, Altman DG, Hammerschlag R, et al. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): extending the CONSORT statement. Acupunct Med. 2010;28(2):83–93. doi:10.1136/aim.2009.001370
28. Lu C, Bao W, Deng D, et al. Efficacy of electroacupuncture with different frequencies in the treatment of chemotherapy-induced peripheral neuropathy: a study protocol for a randomized controlled trial. Front Neurol. 2022;13:843886. doi:10.3389/fneur.2022.843886
29. Shimozuma K, Ohashi Y, Takeuchi A, et al. Feasibility and validity of the patient neurotoxicity questionnaire during taxane chemotherapy in a phase III randomized trial in patients with breast cancer: n-SAS BC 02. Support Care in Cancer. 2009;17(12):1483–1491. doi:10.1007/s00520-009-0613-7
30. Kuroi K, Shimozuma K, Ohashi Y, et al. A questionnaire survey of physicians’ perspectives regarding the assessment of chemotherapy-induced peripheral neuropathy in patients with breast cancer. Japan J Clin Oncol. 2008;38(11):748–754. doi:10.1093/jjco/hyn100
31. McCrary JM, Goldstein D, Boyle F, et al. Optimal clinical assessment strategies for chemotherapy-induced peripheral neuropathy (CIPN): a systematic review and Delphi survey. Support Care in Cancer. 2017;25(11):3485–3493. doi:10.1007/s00520-017-3772-y
32. Basch E, Reeve BB, Mitchell SA, et al. Development of the national cancer institute’s patient-reported outcomes version of the common terminology criteria for adverse events (PRO-CTCAE). J Natl Cancer Inst. 2014;106(9):dju244–dju244. doi:10.1093/jnci/dju244
33. Postma TJ, Aaronson NK, Heimans JJ, et al. The development of an EORTC quality of life questionnaire to assess chemotherapy-induced peripheral neuropathy: the QLQ-CIPN20. Eur J Cancer. 2005;41(8):1135–1139. doi:10.1016/j.ejca.2005.02.012
34. Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365–376. doi:10.1093/jnci/85.5.365
35. Fayers PM, Aaronson NK, Bjordal K, Curran D, Grønvold M. The EORTC QLQ-C30 Scoring Manual.
36. Sim J, Lewis M. The size of a pilot study for a clinical trial should be calculated in relation to considerations of precision and efficiency. J Clin Epidemiol. 2012;65(3):301–308. doi:10.1016/j.jclinepi.2011.07.011
37. Carvalho LF, Silva AMF, Carvalho AA. The use of antioxidant agents for chemotherapy-induced peripheral neuropathy treatment in animal models. Clin Experiment Pharmacol Physiol. 2017;44(10):971–979. doi:10.1111/1440-1681.12803
38. Carozzi VA, Canta A, Chiorazzi A. Chemotherapy-induced peripheral neuropathy: what do we know about mechanisms? Neurosc Lett. 2015;596:90–107. doi:10.1016/j.neulet.2014.10.014
39. Li F, Huang T, Tang Y, et al. Utidelone inhibits growth of colorectal cancer cells through ROS/JNK signaling pathway. Cell Death Dis. 2021;12(4):338. doi:10.1038/s41419-021-03619-6
40. Xu J, Wang Y, Jiang C, et al. Ganglioside monosialic acid alleviates peripheral neuropathy induced by utidelone plus capecitabine in metastatic breast cancer from a phase III clinical trial. Front Oncol. 2020;10:524223. doi:10.3389/fonc.2020.524223
41. Shi H, Yuan X, Fan W, Yang X, Liu G. An umbrella review of the evidence to guide decision-making in acupuncture therapies for chemotherapy-induced peripheral neuropathy. J Cancer Res Clin Oncol. 2023;149(17):15939–15955. doi:10.1007/s00432-023-05369-8
42. Meng X, Zhang Y, Li A, et al. The effects of opioid receptor antagonists on electroacupuncture-produced anti-allodynia/hyperalgesia in rats with paclitaxel-evoked peripheral neuropathy. Brain Res. 2011;1414:58–65. doi:10.1016/j.brainres.2011.08.004
43. Zhang Y, Li A, Xin J, et al. Electroacupuncture alleviates chemotherapy-induced pain through inhibiting phosphorylation of spinal CaMKII in rats. Eur J Pain. 2018;22(4):679–690. doi:10.1002/ejp.1132
44. Lu C, Feng X, Shen Q, et al. Electroacupuncture with different frequencies for paclitaxel-induced peripheral neuropathy: a randomized controlled trial. Zhongguo zhen jiu. 2024;44(10):1139–1145.
45. Chan K, Lui L, Lam Y, et al. Efficacy and safety of electroacupuncture for oxaliplatin-induced peripheral neuropathy in colorectal cancer patients: a single-blinded, randomized, sham-controlled trial. Acupunct Med. 2023;41(5):268–283. doi:10.1177/09645284221125421
46. Liu YP, Luo ZR, Wang C, et al. Electroacupuncture promoted nerve repair after peripheral nerve injury by regulating miR-1b and its target brain-derived neurotrophic factor. Front Neurosci. 2020;14:525144. doi:10.3389/fnins.2020.525144
47. Chen M, Xiong HR, Hu Y, et al. Electroacupuncture alleviates sciatic nerve injury and inhibits autophagy in rats. Acupunct Med. 2024;42(5):268–274. doi:10.1177/09645284241280074
48. Zhang LL, Wang YH, Shao ZH, Ma J. Prophylaxis of bortezomib-induced peripheral neuropathy in patients with multiple myeloma by high-dose intravenous mecobalamin]. Zhongguo shi yan xue ye xue za zhi. 2017;25(2):480–484. doi:10.7534/j.issn.1009-2137.2017.02.031
49. Hiramoto S, Asano H, Miyamoto T, Takegami M, Kawabata A. Risk factors and pharmacotherapy for chemotherapy-induced peripheral neuropathy in paclitaxel-treated female cancer survivors: a retrospective study in Japan. PLoS One. 2021;16(12):e0261473. doi:10.1371/journal.pone.0261473
50. Yokoyama S, Nakagawa C, Hosomi K. Treatment strategy of oxaliplatin-induced peripheral neuropathy: a retrospective, nationwide study. Support Care in Cancer. 2022;30(2):1765–1773. doi:10.1007/s00520-021-06585-z
51. Mao JJ, Farrar JT, Bruner D, et al. Electroacupuncture for fatigue, sleep, and psychological distress in breast cancer patients with aromatase inhibitor-related arthralgia: a randomized trial. Cancer. 2014;120(23):3744–3751. doi:10.1002/cncr.28917
52. Shen G, Ren D, Zhao F, et al. Effect of adding electroacupuncture to standard triple antiemetic therapy on chemotherapy-induced nausea and vomiting: a randomized controlled clinical trial. J Clin Oncol. 2024;42(34):4051–4059. doi:10.1200/JCO.24.00099
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.