")
Back to Journals » Clinical Ophthalmology » Volume 19
Effects of Switching to Netarsudil/Latanoprost Fixed Dose Combination from Various Latanoprost Regimens: The Phase 4 MORE Study
Authors Bacharach J, Sadri E, Sawhney G, Kopczynski C , Merchea MM
Received 4 September 2024
Accepted for publication 20 December 2024
Published 21 January 2025 Volume 2025:19 Pages 175—186
DOI https://doi.org/10.2147/OPTH.S491636
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jason Bacharach,1 Ehsan Sadri,2 Gagan Sawhney,3 Casey Kopczynski,4 Mohinder M Merchea4
1North Bay Eye Associates, Inc, Petaluma, CA, USA; 2Visionary Eye Institute, Newport Beach, CA, USA; 3Georgia Eye Partners, Atlanta, GA, USA; 4Alcon, Inc, Fort Worth, TX, USA
Correspondence: Jason Bacharach, North Bay Eye Associates, Inc, 104 Lynch Creek Way, Suite 15, Petaluma, CA, USA, Tel +1(707) 762-3573, Fax +1 (707) 762-6873, Email [email protected]
Purpose: To determine the effect on intraocular pressure (IOP) of switching to a once-daily netarsudil/latanoprost fixed dose combination (FDC) from various topical treatment regimens including latanoprost monotherapy or latanoprost combined with other IOP-lowering agents for the treatment of open-angle glaucoma or ocular hypertension.
Methods: A total of 136 participants enrolled. Eligible participants were aged ≥ 18 years and had a current diagnosis of open-angle glaucoma or ocular hypertension. Additional inclusion criteria were current treatment regimens with latanoprost monotherapy, latanoprost plus 1 additional IOP-lowering agent, or latanoprost plus 2 agents; current IOP-lowering regimen stable for ≥ 30 days prior to baseline visit; treated morning IOP ≥ 20 mmHg at baseline visit; and best corrected visual acuity (BCVA) of 20/100 or better in both eyes. Regardless of their initial regimens, all participants stopped their IOP-lowering medication(s) and were switched directly to netarsudil/latanoprost FDC alone.
Results: Participants experienced substantial reductions in IOP. At week 12, the mean percent change from baseline in IOP was − 18.5% (SD 18.96) in the overall study population and was similar in the latanoprost monotherapy group (− 21.2% [SD 17.46]), the latanoprost +1 agent group (− 15.7% [SD 21.91]), and the latanoprost +2 agents group (− 16.9% [SD 17.31]). Less than one-third of participants (31.6%) experienced any ocular adverse event or an ocular adverse event related to treatment (27.2%). The most common ocular adverse event was conjunctival hyperemia (18.4%). Most ocular adverse events were mild, and two severe ocular adverse events of hyperemia (1.5%) were reported; no serious ocular adverse events were reported.
Conclusion: In this study, additional IOP lowering was achievable when patients switched to netarsudil/latanoprost FDC after treatment with latanoprost alone or latanoprost with 1 or 2 additional agents. The once-daily administration of netarsudil/latanoprost FDC and reduced treatment burden for those on latanoprost combined with additional agents may prove more manageable for patients.
Keywords: glaucoma, intraocular pressure, prostaglandin analog, rho-kinase inhibitor
Introduction
Glaucoma, a leading cause of permanent blindness in the United States, is characterized by a progressive degeneration of the optic nerve with corresponding visual field loss.1,2 Controlling intraocular pressure (IOP), a major risk factor for development and progression of glaucoma, remains the foundational goal for treating patients to prevent further damage to the optic nerve, and clinicians seek to achieve this goal without sacrificing safety or convenience.3
Glaucoma is treated with several different IOP lowering medication classes that have different levels of efficacy and different mechanisms of action, the most common being prostaglandin analogs, α2‐adrenergic agonists (AA), β-blockers (BB), carbonic anhydrase inhibitors (CAI), and miotics.4 Topical prostaglandin analogs, specifically latanoprost, are a common first-line treatment for glaucoma to lower IOP by increasing aqueous outflow through the uveoscleral pathway.5 Rho-kinase inhibitors are the newest class of IOP-reducing agents with a novel mechanism of action: increasing trabecular outflow, decreasing acto-myosin-driven cellular contraction, and reducing production of extracellular matrix proteins.6,7 Individual topical glaucoma treatments are often not sufficiently effective as monotherapy, and use of multiple medications is common. Unfortunately, more complex dosing regimens in patients with glaucoma have been shown to result in poorer adherence.8 Recently, the use of fixed-dose combinations (FDCs) has gained popularity as a way for multiple medications to be used simultaneously with a simplified instillation regimen.9
When used in combination with a prostaglandin analog like latanoprost, the rho-kinase inhibitor netarsudil has demonstrated additional IOP lowering.10,11 The commercially available, novel FDC of netarsudil and latanoprost has been developed to optimize complementary IOP-lowering mechanisms. Netarsudil/latanoprost is the only available FDC in the United States with a prostaglandin (latanoprost) combined with any agent (including netarsudil). Both prostaglandin analogs and netarsudil reduce IOP, but through different pathways; prostaglandin analogs mainly increase uveoscleral outflow through ciliary muscle relaxation, while netarsudil mainly increases conventional outflow by relaxing cells in the trabecular meshwork, the tissue responsible for elevated IOP. Unlike other agents included in FDCs, they do not reduce the production of aqueous humor, which plays an important role in maintaining eye health by supplying nutrients and oxygen to avascular tissues and removing waste products from the posterior cornea and anterior lens.12,13 Netarsudil/latanoprost is also the only FDC option that is administered once daily, which may help ensure adherence.8,14
The efficacy of this combination has been demonstrated in two phase 3 studies. MERCURY-1 (NCT02558400) and MERCURY-2 (NCT02674854) were 12- and 3-month studies, respectively, which demonstrated that the FDC of netarsudil 0.02%/latanoprost 0.005% (Rocklatan®; Alcon, Fort Worth, TX, USA) resulted in IOP reductions 1 to 3 mmHg greater than either agent alone.10,11 As a result of these studies, netarsudil/latanoprost FDC was approved by the United States Food and Drug Administration in 2019 for reducing elevated IOP in patients with open-angle glaucoma or ocular hypertension.
Although the efficacy of netarsudil 0.02%/latanoprost 0.005% FDC has been previously demonstrated, there is currently no available evidence supporting its use in real-world clinical settings when patients are switched to netarsudil/latanoprost FDC from regimens containing latanoprost alone or latanoprost with one or two adjunctive agents.
Methods
Study Design and Participants
The MORE study (ClinicalTrials.gov identifier: NCT05283395) was a 12-week, multicenter, prospective, interventional, open-label, phase 4 study involving adult patients (N=135) diagnosed with open-angle glaucoma or ocular hypertension. Reflecting real-world practice, participants were not asked to stop their existing IOP-lowering therapy in the weeks prior to being enrolled. Upon enrollment, all participants’ various latanoprost regimens were stopped and switched directly to netarsudil 0.02%/latanoprost 0.005% once daily. The study was conducted from March 28, 2022 to March 22, 2023 and involved 21 study centers in the United States.
Eligible participants were aged ≥18 years and had a current diagnosis of open-angle glaucoma or ocular hypertension. Additional criteria for inclusion in the study were current treatment regimens with latanoprost monotherapy, latanoprost plus 1 additional IOP-lowering agent, or latanoprost plus 2 agents; current IOP-lowering regimen stable for ≥30 days prior to baseline visit; treated morning IOP ≥20 mmHg at baseline visit; and best corrected visual acuity (BCVA) of 20/100 or better in both eyes. Additional IOP-lowering agents used by participants on latanoprost could include BB, AA, CAI, or FDC agents. Fixed-dose combination agents combining two active ingredients were considered as two IOP-lowering agents.
Excluded individuals were treatment naïve or treated with agents not including latanoprost at baseline; patients who had a mean central corneal thickness >620 μm in either eye, active ocular infection, inflammation, or history of uveitis; history of corneal refractive surgery or intraocular surgery in the study eye within 3 months prior to baseline (including minimally invasive glaucoma surgery); or visual field loss determined by the investigator to be end-stage glaucomatous. Additional exclusion criteria were use of systemic medications that may have a substantial effect on IOP, unless the medication(s) were taken for ≥3 months prior to baseline and expected to remain constant throughout the study; use of topical, periorbital, intravitreal, or systemic steroids within 3 months prior to baseline or expected steroid use during the study; or known sensitivity to any component of the study medication. Women of childbearing potential who were pregnant, nursing, planning a pregnancy, or not using a medically acceptable form of birth control were also excluded.
All enrolled participants were dispensed the FDC of netarsudil 0.02%/latanoprost 0.005% ophthalmic solution. Participants stopped their previous IOP-lowering medications and self-administered netarsudil/latanoprost FDC at the recommended dosage, 1 drop in each eye daily in the evening for 12 weeks, starting on the day of their baseline visit. In the latanoprost +1 agent group, both latanoprost and the additional agent were stopped, and netarsudil/latanoprost FDC was started in their place. In the latanoprost +2 agents group, latanoprost plus the two agents were completely stopped, and only netarsudil/latanoprost FDC was initiated.
All participants provided written informed consent and signed authorization for the Health Insurance Portability and Accountability Act before initiation of any study procedure or treatment. The study protocol and informed consent were approved by a central institutional review board (Advarra IRB, Columbia, MD, USA), conducted in accordance with Good Clinical Practice Guidelines, and adhered to the Declaration of Helsinki.
Endpoints
The primary efficacy endpoint was mean percent reduction from baseline in IOP in the study eye at week 12. Other assessments included overall mean reduction in IOP and responder analyses, as well as questionnaires for investigators and participants. Safety was also evaluated.
Procedures
The study schedule consisted of 3 visits: a baseline visit (day 0), a follow-up visit at week 6 (±7 days), and a final visit at week 12 (±7 days). Informed consent, demographic information, participant eligibility, a urine pregnancy test for women of childbearing potential, pachymetric data, and medical and IOP history were collected at the baseline visit. Information on prior and concomitant medications and procedures were reported at baseline and updated at each follow-up visit.
To evaluate efficacy, IOP was measured in both eyes in the morning (before noon), using a Goldmann applanation tonometer affixed to a slit lamp at the baseline visit, week 6 (visit 2), and week 12 (visit 3). The same investigator or designee was to complete all tonometric evaluations. After 1 drop of topical anesthetic was administered into each eye, the assessor waited 4 minutes before evaluating the participant in a seated position. The assessor performed the measurement, read the result, and recorded the IOP. Investigators were requested to schedule study visits at the same time of day.
Safety measurements conducted at baseline, week 6, and week 12 visits were BCVA, measured for both eyes using a Snellen Visual Acuity Chart at a distance of 20 feet, and biomicroscopy for both eyes by slit lamp examination. Biomicroscopic examination of eyelids, conjunctiva, cornea, anterior chamber, and lens of both eyes was conducted and recorded at each study visit. Based on the results of the biomicroscopy, participants’ levels of hyperemia were graded on the following scale: 0, none (normal appearance); 0.5, trace (minimal flush, reddish color predominantly confined to palpebral or bulbar conjunctiva); 1, mild (flush, reddish color predominantly confined to the palpebral or bulbar conjunctiva); 2, moderate (bright red color of the palpebral or bulbar conjunctiva); or 3, severe (deep, bright diffuse redness of the palpebral or bulbar conjunctiva). Participants were asked at weeks 6 and 12 if they experienced any adverse events, and all reports were recorded, including severity, action taken, and investigator determination of relationship to the study medication.
Other assessments conducted at week 12 included a series of questionnaires administered by the investigator. These were developed for the purpose of this study and were not part of any validated questionnaire; they included a study eye medication evaluation questionnaire, a treatment adherence questionnaire, and a clinical success questionnaire. Participants were asked to rate comfort, eye redness, tolerability, overall satisfaction, and convenience of the study medication.
Participants were dispensed study medication bottles at baseline and week 6, and the used/unused study medication bottles were collected at weeks 6 and 12. If a participant discontinued from the study after the baseline visit, they were requested to return for a final early exit visit where all week-12 assessments were performed.
Statistical Analysis
Efficacy and safety data are presented descriptively. Participants were grouped according to their IOP-lowering medication regimen at baseline. The primary efficacy analysis was calculated using data from all participants and within each baseline IOP-lowering therapy participant group with complete data at both baseline and final visits. No sample size calculation was performed, given that no statistical comparisons between treatments were planned. Efficacy analysis was done with assessments from the study eye, which was determined to be the more severely affected eye at baseline (ie, the eye with higher IOP) or the right eye if both were the same. All analyses were performed using SAS Version 9.4 or higher.
Summary statistics included mean, median, standard deviations, minimum and maximum ranges, and frequency distributions of IOP and percent reduction in IOP. The modified intent-to-treat (mITT) population was the primary study population used in the assessment of efficacy endpoints and included participants who were treated and had at least 1 follow-up visit with a completed IOP measurement. As outlined in the statistical analysis plan, efficacy analyses were performed on mITT participants who completed the study through week 12. The population for safety analyses included all participants who received at least 1 dose of study medication.
Results
Participant Disposition and Baseline Characteristics
A total of 136 participants were enrolled (Figure 1). One participant was inappropriately enrolled and treated and was included in the safety analysis (n=136) but not the intent-to-treat (ITT) analysis (n=135). The mITT population comprised participants who attended 1 or more follow-up visits with a completed IOP measurement (n=121). Of the 136 participants who were treated, 20 (14.7%) discontinued treatment and 8 (5.9%) discontinued due to adverse events. Details on the adverse events observed in this study are covered under the safety section. Baseline characteristics and efficacy results are reported for the mITT population participants who completed week 12 of the study (n=116).
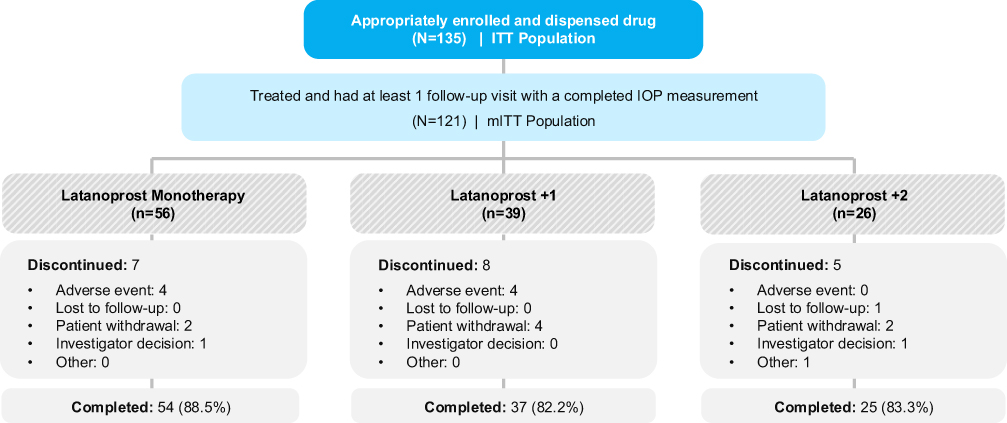 |
Figure 1 Participant disposition. Study population: mITT population. Abbreviations: IOP, intraocular pressure; mITT, modified intent to treat. |
The baseline characteristics of the mITT population were similar among treatment groups (Table 1). Within the mITT population, 110 participants (90.9%) had a diagnosis of open angle glaucoma, and 69 (57.0%) had elevated IOP for 6 or more years. The IOP-lowering treatment history of the mITT population is summarized in Table 2. At baseline, 54 (46.6%) participants were on latanoprost monotherapy. Of the 37 (31.9%) participants who were using latanoprost with 1 additional agent, 18 (48.6%) were using a BB, 14 (37.8%) were using an AA, and 5 (13.5%) were using a CAI. In the group of 25 (21.6%) participants using latanoprost with 2 additional agents before switching to netarsudil/latanoprost FDC, 5 (20.0%) were on an FDC, 9 (36.0%) were on a BB + CAI, 6 (24.0%) were on a BB + AA, and 5 (20.0%) were on an AA + CAI.
 |
Table 1 Baseline Demographics and Ocular Characteristics |
 |
Table 2 IOP-Lowering Medication Treatment History |
All participants in the study had elevated IOP (≥20 mmHg) on their existing regimens and were thus determined to have benefitted from further IOP reduction.
Efficacy
The mean baseline IOP in all study eyes was approximately 22.5 mmHg (SD 2.76), and values were comparable across all treatment groups (Table 1). At week 12, the mean percent change from baseline in IOP was −18.5% (SD 18.96) in the overall study population (Figure 2A) and was similar in the latanoprost monotherapy group (−21.2% [SD 17.46]), the latanoprost +1 agent group (−15.7% [SD 21.91]), and the latanoprost +2 agents group (−16.9% [SD 17.31]).
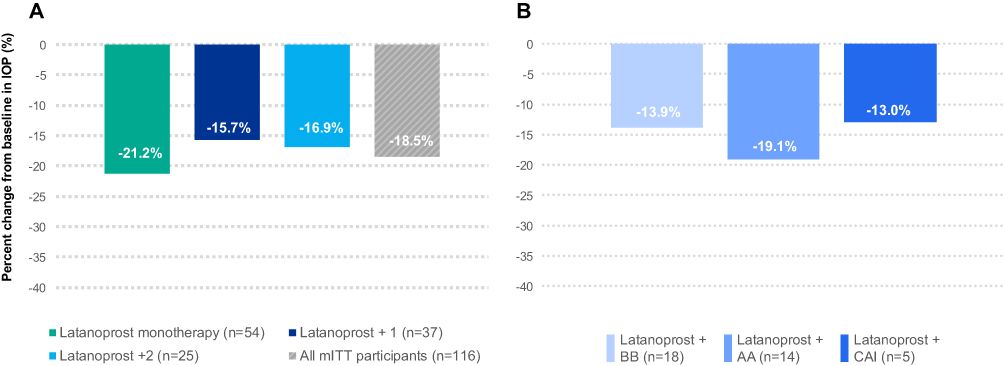 |
Figure 2 Mean percent change in IOP from baseline to week 12 in (A) the full study population and (B) the latanoprost + 1 subgroups. Study population: mITT population. Abbreviations: AA, alpha-adrenergic agonist; BB, beta blocker; CAI, carbonic anhydrase inhibitor; IOP, intraocular pressure; mITT, modified intent to treat. |
Within the composition of the latanoprost +1 agent group, the percent change in IOP at week 12 for the specific latanoprost regimens was −13.9% (SD 21.96) in the latanoprost + BB group, −19.1% (SD 24.64) in the latanoprost + AA group, −13.0% (SD 15.24) in the latanoprost + CAI group (Figure 2B). The small sample sizes in each of the latanoprost +2 agents subgroups (<10) limit the interpretation of the data.
The IOP-lowering effect of netarsudil/latanoprost FDC was observed as early as week 6, as the mean percent change from baseline in IOP was −21.9% (SD 14.97) in the overall study population. In the latanoprost monotherapy, the latanoprost +1 agent, and the latanoprost +2 agents groups, the percent changes in IOP at week 6 were −25.4% (SD 13.17), −19.2% (SD 13.96), and −18.6 (SD 18.63), respectively. IOP lowering was consistently observed from weeks 6 through 12, therefore there was no carry-over effect of baseline IOP-lowering therapy observed in this study.
In the overall population, participants experienced a substantial reduction in IOP, as the absolute mean change was −4.2 mmHg (SD 4.57) at week 12 (Figure 3A). In participants using latanoprost alone, with 1 additional agent, and with 2 additional agents, the mean changes in IOP at week 12 were −4.9 mmHg (SD 4.13), −3.6 mmHg (SD 5.43), and −3.7 mmHg (SD 4.02), respectively. In the latanoprost +1 agent group, the type of adjunctive medications used in participants’ previous regimens did not meaningfully affect the magnitude of IOP reduction (Figure 3B).
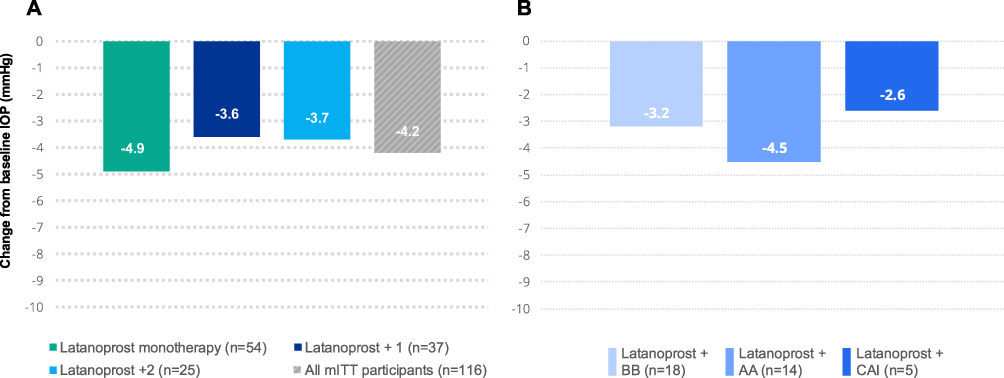 |
Figure 3 Mean absolute change in IOP from baseline to week 12 in (A) the full study population and (B) the latanoprost + 1 subgroups. Study population: mITT population. Abbreviations: AA, alpha-adrenergic agonist; BB, beta blocker; CAI, carbonic anhydrase inhibitor; IOP, intraocular pressure; mITT, modified intent to treat. |
Similar results were observed at week 6: the absolute mean change in IOP was −4.9 mmHg (SD 3.49) in the overall study population, −5.8 mmHg (SD 2.95) in the latanoprost monotherapy group, −4.3 mmHg (SD 3.16) in the latanoprost +1 agent group, and −4.1 mmHg (SD 4.60) in the latanoprost +2 agents group.
At week 12, more than half of participants achieved IOP ≤18 mmHg (Figure 4). An IOP ≤18 mmHg was achieved by 64.8%, 56.8%, and 64.0% of those switching from latanoprost monotherapy, latanoprost +1 agent, and latanoprost +2 agents, respectively. Over half (54.3%) of all participants achieved at least a 20% reduction in IOP at week 12, and nearly a third (29.3%) achieved a 30% or more reduction from their baseline treated IOP (Figure 5).
 |
Figure 4 Proportion of participants at or below IOP thresholds at week 12. Study population: mITT population. Abbreviations: IOP, intraocular pressure; mITT, modified intent to treat. |
 |
Figure 5 Proportion of participants at or below IOP percent reduction thresholds at week 12. Study population: mITTpopulation. Abbreviations: IOP, intraocular pressure; mITT, modified intent to treat. |
Safety
Conjunctival hyperemia (bulbar and palpebral) was assessed using slit lamp biomicroscopy and graded at all visits. Though hyperemia did increase from baseline (44.1%) to week 12 (73%), 57% of cases at week 12 were graded as trace or mild. The mean hyperemia scores remained under 1 (from 0.4 [SD 0.53] at baseline to 0.7 [SD 0.68] at week 12), which is consistent with the MERCURY phase 3 trials. Most participants had no or trace changes in hyperemia grade from baseline to week 12, while only 20.7% had an increase of 1 or more units.
A total of 52 (38.2%) participants experienced an adverse event of any kind (Table 3). Less than a third of participants (31.6%) experienced any ocular adverse event or an ocular adverse event related to treatment (27.2%). The most common ocular adverse events were conjunctival hyperemia (18.4%), eye irritation (2.9%), and blurred vision (2.9%). Most ocular adverse events were mild, and two severe ocular adverse events of hyperemia (1.5%) were reported; no serious ocular adverse events were reported.
 |
Table 3 Summary of Ocular Adverse Events |
Few non-ocular adverse events were reported in the study, and most were mild or moderate in severity—the most common were COVID-19 (1.5%) and headache (1.5%). A total of 8 participants (5.9%) experienced adverse events that led to discontinuation, which were conjunctival hyperemia (3.7%), conjunctivitis (1.5%), and eye pruritis (0.7%). One participant experienced a serious adverse event (closed fracture of right femur) that was not considered related to treatment.
Participant and Investigator Assessment of Treatment
When participants were asked, “How well are you able to tolerate the study eye medication?” 86.2% reported that they tolerated the medication well (including 18.5% well, 23.1% mostly well, and 44.6% very well).
When asked, “Did you notice any eye redness from using the study eye medication?” a majority of participants reported mild redness (21.5%), “just a hint of redness” (20.8%), or no redness (23.1%). Of those who noticed redness, 76% reported being “not bothered at all” or “only a little bothered” by the eye redness, and 80% said that they would tolerate the eye redness if their doctor said their eye pressure was under control.
Approximately 75% of participants reported that they would be willing to continue taking the study medication if their doctor prescribed it, and investigators reported that they would be willing to continue over 75% (76.7%) of participants on netarsudil/latanoprost FDC. Importantly, investigators also reported that 75% of participants achieved the target level of IOP.
Factors Affecting Patient Adherence
When surveyed about their daily drop burden, 53% of those in the baseline latanoprost +1 agent group reported using 3 drops per day, while in the baseline latanoprost +2 agents group, 70% were using 4 to 7 drops per day. Additionally, when asked at week 12, 95.3% of subjects reported not needing reminders or help taking or using netarsudil/latanoprost FDC, and all but 4 subjects reported that the convenience of once-daily dosing from a single bottle was important to them.
Discussion
Direct switching between IOP-lowering agents in clinical practice routinely does not involve washout from prior agents, and this study was intended to demonstrate the efficacy of netarsudil/latanoprost FDC under these typical real-world conditions. Under these conditions, the present study demonstrates the additional IOP lowering that is achievable when patients switch to netarsudil/latanoprost FDC after treatment with latanoprost alone or latanoprost with 1 or 2 additional agents.
After switching to netarsudil/latanoprost FDC, IOP was reduced at 12 weeks by an average of 4.2 mmHg, a 19% decrease from the baseline treated IOP of ≥20 mmHg, and additional IOP lowering was also observed at week 6, with an average reduction of 4.9 mmHg in the overall study population regardless of previous treatment regimen. The percent changes in IOP at week 12 for each treatment group were −21%, −16%, and −17% in the latanoprost monotherapy, latanoprost +1 agent, and latanoprost +2 agents groups, respectively. These results were also comparable regardless of adjunctive treatment classes; patients taking a BB, AA, or CAI experienced reductions of −14%, −19%, and −13%, respectively. It should be noted that the small numbers of participants (<10) in each of the latanoprost +2 agents subgroups limit the interpretation of these data.
The complementary mechanisms of action of netarsudil and latanoprost may explain the observed reductions of IOP with the FDC. While latanoprost and other prostaglandin analogs lower IOP by increasing uveoscleral aqueous outflow,5 rho-kinase inhibitors like netarsudil exert efficacy by increasing outflow through the conventional trabecular pathway.10
Another potential benefit of netarsudil/latanoprost FDC is its simplified instillation regimen, which is critical in this disease state, as a substantial proportion of patients require multiple IOP-lowering agents. An increased number of drops is negatively correlated with patient adherence, and nonadherence to topical therapies has been demonstrated in 23% to 59% of patients with glaucoma.15,16 By providing 2 medications within one drop that is administered only once daily, netarsudil/latanoprost FDC can substantially reduce treatment burden. Prior to study initiation, over half (53%) of patients in the latanoprost +1 agent group were using a regimen of 3 drops per day, and almost three-quarters (70%) of patients in the latanoprost +2 agents group were using a regimen of 4 to 7 drops per day. Additionally, nearly all (95.3%) subjects reported not needing reminders or help taking or using the FDC, and all but 4 subjects reported the convenience of once-daily dosing from a single bottle as important to them.
Netarsudil/latanoprost FDC appeared to be well tolerated throughout the duration of treatment. The types of ocular adverse events observed were similar to those observed in phase 3 studies of netarsudil/latanoprost FDC; the most common adverse event was conjunctival hyperemia (21%), a known side effect of vasodilatory rho-kinase inhibitors.17 However, 80% of participants in this study had no or trace changes from baseline in slit lamp biomicroscopy grading of hyperemia. Participant and investigator assessments also reinforced the tolerability of this approach: approximately three quarters of participants reported that they would be willing to continue taking the study medication if prescribed it by their doctor. Investigators also reported they would be willing to continue 76.7% of participants on the FDC, which is similar to the proportion of patients reported to have achieved the target level of IOP.
Several aspects of this study design may hinder our ability to interpret its conclusions. Firstly, the study did not include a control arm, making it difficult to discern a possible placebo effect. Secondly, though IOP varies throughout the day, in this study it was measured at a single timepoint in the morning consistently for each subject at all visits. In addition, the lack of using a washout period in this study, due to the substantial variation in recommended washout times—up to 8 weeks—for different IOP-lowering medications, may limit the ability to assess the absolute change in IOP due to changing to the netarsudil/latanoprost FDC.18 Lastly, the study was not powered for inferential statistics, so conclusions cannot be drawn about study population, baseline treatment regimens, or individual adjunctive agents.
In this study, the use of netarsudil/latanoprost FDC in real world conditions was demonstrated to be an effective treatment option for additional lowering of IOP in patients with open-angle glaucoma or ocular hypertension, regardless of the adjunctive class or number of adjunctive agents used prior to switching. This result supports the conclusion that netarsudil lowers IOP through a mechanism of action that is distinct from the glaucoma medications used at baseline by patients in this study. The once-daily dosing and reduced treatment burden may improve adherence and prove more manageable for patients throughout the lifelong treatment these conditions require. Additional studies comparing netarsudil/latanoprost FDC with other IOP-lowering regimens may help further characterize the clinical effects attributable to this specific combination of pharmacologic agents.
Acknowledgments
Medical writing support provided by Jessie Riederer, PharmD, of Ethis, Inc.
Disclosure
Drs. Bacharach and Sawhney report receiving honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Alcon. Dr Bacharach also reports research grant from Aerie. Drs. Kopczynski and Merchea report being employed by Alcon. Dr. Sadri reports receiving grant funding from Alcon. Dr. Kopczynski reported receiving travel and material support from Alcon and owning stock in Alcon. Dr Kopczynski reports patents US11707460B2, US11185538B2, US11197853B2, US10588901B2, US9993470B2, US9931336B2, and US9415043B2 issued to Alcon. Dr. Sadri reported having a leadership or fiduciary role at Visionary Ventures. The authors report no other conflicts of interest in this work.
References
1. Dietze J, Blair K, Havens SJG. StatPearls. Treasure Island (FL): StatPearls Publishing; 2022.
2. Storgaard L, Tran TL, Freiberg JC, Hauser AS, Kolko M. Glaucoma clinical research: trends in treatment strategies and drug development. Front Med. 2021;8:733080. doi:10.3389/fmed.2021.733080
3. The AGIS investigators. the advanced glaucoma intervention study (AGIS): 7. the relationship between control of intraocular pressure and visual field deterioration. Am J Ophthalmol. 2000;130(4):429–440. doi:10.1016/S0002-9394(00)00538-9
4. Li F, Huang W, Zhang X. Efficacy and safety of different regimens for primary open-angle glaucoma or ocular hypertension: a systematic review and network meta-analysis. Acta Ophthalmol. 2018;96(3):e277–e284. doi:10.1111/aos.13568
5. Toris CB, Gabelt BT, Kaufman PL. Update on the mechanism of action of topical prostaglandins for intraocular pressure reduction. Surv Ophthalmol. 2008;53(suppl1):S107–S120. doi:10.1016/j.survophthal.2008.08.010
6. Kazemi A, McLaren JW, Kopczynski CC, Heah TG, Novack GD, Sit AJ. The effects of netarsudil ophthalmic solution on aqueous humor dynamics in a randomized study in humans. J Ocul Pharmacol Ther. 2018;34:380–386. doi:10.1089/jop.2017.0138
7. Lin CW, Sherman B, Moore LA, et al. Discovery and preclinical development of netarsudil, a novel ocular hypotensive agent for the treatment of glaucoma. J Ocul Pharmacol Ther. 2018;34(1–2):40–51. doi:10.1089/jop.2017.0023
8. Robin AL, Novack GD, Covert DW, Crockett RS, Marcic TS. Adherence in glaucoma: objective measurements of once-daily and adjunctive medication use. Am J Ophthalmol. 2007;144(4):533–540. doi:10.1016/j.ajo.2007.06.012
9. Lerner SF, Oddone F, Lu DW, et al. Maximum medical therapy: brinzolamide/brimonidine and travoprost/timolol fixed-dose combinations in glaucoma and ocular hypertension. Clin Ophthalmol. 2019;13:2411–2419. doi:10.2147/OPTH.S228777
10. Brubaker JW, Teymoorian S, Lewis RA, et al. One year of netarsudil and latanoprost fixed-dose combination for elevated intraocular pressure: phase 3, randomized MERCURY-1 study. Ophthalmol Glaucoma. 2020;3(5):327–338. doi:10.1016/j.ogla.2020.05.008
11. Walters TR, Ahmed IIK, Lewis RA, et al. Once-daily netarsudil/latanoprost fixed-dose combination for elevated intraocular pressure in the randomized phase 3 MERCURY-2 study. Ophthalmol Glaucoma. 2019;2(5):280–289. doi:10.1016/j.ogla.2019.03.007
12. Liu P, Wang F, Song Y, Wang M, Zhang X. Current situation and progress of drugs for reducing intraocular pressure. Ther Adv Chronic Dis. 2022;13:20406223221140392. doi:10.1177/20406223221140392
13. Sunderland DK, Physiology SA. Aqueous humor circulation. StatPearls. 2023.
14. Buchan JC, Siddiqui S, Gilmour D. Once daily drop regimes help reduce involuntary non-compliance. Graefes Arch Clin Exp Ophthalmol. 2007;245(2):327–328. doi:10.1007/s00417-006-0438-8
15. Zhang X, Vadoothker S, Munir WM, Saeedi O. Ocular surface disease and glaucoma medications: a clinical approach. Eye Contact Lens. 2019;45(1):11–18. doi:10.1097/ICL.0000000000000544
16. Schwartz GF, Quigley HA. Adherence and persistence with glaucoma therapy. Surv Ophthalmol. 2008;53(Suppl1):S57–68. doi:10.1016/j.survophthal.2008.08.002
17. Watabe H, Abe S, Yoshitomi T. Effects of Rho-associated protein kinase inhibitors Y-27632 and Y-39983 on isolated rabbit ciliary arteries. Jpn J Ophthalmol. 2011;55:411–417. doi:10.1007/s10384-011-0048-9
18. Stewart WC, Holmes KT, Johnson MA. Washout periods for brimonidine 0.2% and latanoprost 0.005%. Am J Ophthalmol. 2001;131(6):798–799. doi:10.1016/S0002-9394(00)00930-2
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.