")
Back to Journals » Clinical Ophthalmology » Volume 18
Efficacy and Safety of Ab-Interno Canaloplasty in Post-Keratoplasty Patients: 3-Year Results
Authors Redden LD , Riaz KM , Murphy DA, Ding K, Khaimi MA
Received 28 August 2024
Accepted for publication 26 November 2024
Published 30 November 2024 Volume 2024:18 Pages 3567—3577
DOI https://doi.org/10.2147/OPTH.S487384
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Liam D Redden, Kamran M Riaz, David A Murphy, Kai Ding, Mahmoud A Khaimi
Dean McGee Eye Institute, University of Oklahoma Health Sciences Center, Oklahoma City, OK, USA
Correspondence: Kamran M Riaz, Dean McGee Eye Institute, University of Oklahoma Health Sciences Center, Oklahoma City, OK, 73104, USA, Tel +1-405-271-1095, Fax +1-405-271-3680, Email [email protected]
Purpose: To evaluate the effectiveness and safety of ab-interno canaloplasty (ABiC) for managing intraocular pressure (IOP) in patients following keratoplasty over a three-year period.
Methods: This retrospective analysis focused on post-keratoplasty patients treated with ABiC with the iTrack microcatheter (Nova Eye Medical, Fremont, CA, USA) at a single institution. The study assessed the procedure’s impact on IOP control, graft survival, and reliance on topical hypotensive medications, with additional observation for any postoperative complications. Surgical success criteria included the percentage of eyes with IOP ≤ 15 mmHg, IOP ≤ 18 mmHg, ≥ 20% IOP reduction, medication-free eyes, and eyes with concurrent IOP and medication reductions.
Results: ABiC was performed successfully in a cohort of 16 post-keratoplasty (7 penetrating keratoplasty and 9 endothelial keratoplasty (EK)) eyes. Preoperative mean IOP of 25.8± 7.2 mmHg was significantly reduced to 13.4± 2.9 mmHg (p< 0.001) at 1 year postoperatively and maintained at 13.1± 3.9 mmHg (p=0.009) at 3 years postoperatively. The mean number of glaucoma medications was 3.5± 1.7 at baseline, 2.8± 1.3 at 1 year (p=0.107), and 2.5± 1.2 at 3 years postoperatively (p=0.088). Eight eyes (66.7%) maintained IOP ≤ 15 mmHg, and 10 eyes (83.3%) maintained ≥ 20% IOP reduction at 3 years. The mean IOP and medication reductions from baseline at 3 years were − 49.2% and − 28.6%, respectively. Graft clarity was preserved in all patients except for one case of late graft failure that necessitated a repeat EK procedure. Post-ABiC complications included transient hyphema in two patients, neither of which led to long-term adverse outcomes.
Conclusion: ABiC appears to be an effective and safe surgical intervention for sustained IOP reduction in post-keratoplasty patients. Graft survival trends are encouraging, and there was a low incidence of complications over a three-year follow-up period.
Keywords: ab-interno canaloplasty, keratoplasty, intraocular pressure, glaucoma
Introduction
Corneal transplantation (full and partial-thickness procedures) is a commonly performed procedure for numerous corneal pathologies. Elevated intraocular pressure (IOP) is a frequently encountered complication after keratoplasty. Elevated IOP may stem from pre-existing glaucoma or arise as a new complication, either from the surgery itself or from prolonged use of topical steroids.1,2 The incidence of elevated IOP following keratoplasty is notably lower in endothelial keratoplasty compared to penetrating keratoplasty (PKP).3,4 However, uncontrolled glaucoma remains a significant cause of graft failure, leading to suboptimal visual outcomes.5,6
Effectively managing elevated IOP is crucial due to the potential loss of endothelial cells associated with uncontrolled glaucoma, which stands as the second most common cause of keratoplasty failure.5,6 Typically, the treatment approach for elevated IOP begins with topical hypotensive medications and in-office laser treatments (eg, selective laser trabeculoplasty, etc). In cases where these measures prove insufficient, incisional procedures, such as glaucoma drainage devices (GDDs) and trabeculectomy, may be necessary.7 Given the variable success rates of incisional procedures, along with the common occurrence of graft failure and rejection associated with glaucoma drainage devices,8,9 there has been a shift towards adopting less invasive techniques, notably minimally invasive glaucoma surgeries (MIGS) in post-keratoplasty patients.10
Ab-interno canaloplasty (ABiC) is a type of MIGS designed to address all points of outflow resistance within the conventional outflow pathway. It targets three key areas: Schlemm’s canal, the trabecular meshwork, and the distal collector channels. ABiC is claimed to reduce IOP by restoring the natural trabeculo-canalicular outflow through employing a flexible microcatheter to perform 360-degree catheterization and viscodilation of Schlemm’s canal,11,12 which leads to expansion of juxtacanalicular trabecular meshwork with pore formation in the endothelium of Schlemm’s canal. Both were found to reduce outflow resistance.13,14 Many studies have shown that ABiC stands out among other MIGS procedures for its tissue preservation, stent-free, and comprehensive viscodilation approach, rendering it a potentially safe and successful procedure.15 Additionally, ABiC does not preclude performing other glaucoma surgeries (MIGS or incisional) should they be considered in the future for additional IOP reduction.
In our earlier study, we demonstrated the effectiveness and safety of ABiC, both standalone and in combination with phacoemulsification, for reducing IOP while ensuring graft survivability over a 12-month post-canaloplasty period.16 Here, we present the 3-year outcomes of ABiC in post-keratoplasty eyes regarding its impact on IOP reduction, medication reduction, and longer-term corneal graft survival.
Materials and Methods
Ethics
Our study adhered to the principles outlined in the Declaration of Helsinki. The Institutional Review Board of the University of Oklahoma Health Sciences Center (IRB#61730) granted ethical approval for this research. Given the nature of the study, which involved a retrospective review of clinical and surgical data, the IRB waived the requirement for informed consent. All patient data were handled in compliance with confidentiality standards to ensure the protection of patient privacy.
Design
We conducted a retrospective case series study involving multiple surgeons at our institution, building upon our earlier research,16 to identify patients who had undergone keratoplasty and were experiencing uncontrolled elevated IOP despite medical treatment. These patients subsequently underwent ABiC using the iTrack microcatheter (Nova Eye Medical, Fremont, USA). All ABiC procedures and previous keratoplasties were performed at our institution. Data was gathered from medical records spanning from May 2015 to May 2023.
Prior to ABiC, each patient underwent a baseline comprehensive ophthalmic examination, which included a review of their glaucoma history, previous ocular surgeries, medication use, IOP, best-corrected visual acuity (BCVA), gonioscopy, slit lamp examination, and fundus examination. Follow-up examinations were scheduled for postoperative day one, as well as at 1 week, 1 month, 6 months, 12 months, 24 months, and 36 months after ABiC. These follow-ups involved measuring IOP, assessing BCVA (recorded in Snellen and converted to logMAR), conducting slit lamp examinations, gonioscopy, and monitoring the use of topical hypotensive medication. Surgical success criteria included the percentage of eyes with IOP ≤15 mmHg, IOP ≤18 mmHg, a ≥20% reduction in IOP, medication-free eyes, and eyes with simultaneous reductions in both IOP and medication use. Any adverse events were documented. In cases where a patient missed a scheduled visit, the data for that time point was treated as missing.
Patient Selection
We enrolled patients aged 18 years and older who had undergone keratoplasty and were experiencing uncontrolled IOP despite the maximum tolerated use of topical hypotensive drops. Patients with angle-closure glaucoma, mixed-mechanism glaucoma (prior glaucoma, surgical or steroid induced), or a history of any other prior glaucoma surgery were excluded from the study.
Ab Interno Canaloplasty Surgical Technique
The surgical procedure was similar to that performed on non-keratoplasty eyes.17 A small goniotomy is used to introduce the iTrack microcatheter into Schlemm’s canal. The microcatheter then navigates the entire 360-degree circumference of the canal. Should an obstruction impede the microcatheter’s progress, it is removed from the eye, and a second paracentesis is performed to approach from the opposite direction. After completing the full circuit, the iTrack microcatheter is gradually extracted. During this withdrawal process, a manually operated viscoinjector device delivers precisely measured amounts of high-molecular-weight hyaluronic acid (HA)-based ophthalmic viscosurgical device (OVD) into Schlemm’s canal. Approximately 11 notches of OVD are administered per quadrant, covering the entire 360-degree span of the canal. Once this viscodilation procedure is finished, the iTrack microcatheter is removed from the eye.
Among the 16 study eyes, 11 underwent ABiC as a standalone procedure, and 5 underwent ABiC in combination with phacoemulsification and intraocular lens (IOL) implantation. In these cases, cataract surgery and IOL placement were completed prior to the canaloplasty procedure. Our previous study described additional details regarding the canaloplasty procedure and postoperative pharmacological treatments as well as a surgical video of the procedure.16
Statistics
We utilized descriptive statistics, including mean, standard deviation, and range, to analyze IOP, visual acuity, and the number of medications at the following visits (baseline, 1 month, 6 months, 12 months, 24 months, 36 months). For comparative analysis between visits, we employed the non-parametric Friedman test, followed by the Wilcoxon signed rank test for multiple comparisons. We considered a p-value less than 0.05 to be statistically significant, and we indicated p-values where applicable. All statistical analyses were conducted using SPSS statistical software, release 23 (IBM, New York, USA).
Results
Demographics
Detailed demographic information is presented in Table 1. The study cohort included 16 eyes from 13 patients with a mean age of 63.8±11.8 years. All eyes underwent ABiC approximately 2.23±1.81 years after keratoplasty procedures, distributed as follows: 7 penetrating keratoplasty (PKP), 8 Descemet Stripping Automated Endothelial Keratoplasty (DSAEK), and 1 (Descemet Membrane Endothelial Keratoplasty) DMEK. Two of the 8 DSAEK were performed under previous PKP for endothelial failure. The majority of patients were of Caucasian descent (69.2%). Eleven of the 16 eyes (69%) had a diagnosis of glaucoma before keratoplasty.
 |
Table 1 Patient Demographics |
Intraocular Pressure
At all postoperative time points, the IOP consistently showed a significant reduction compared to the baseline (Table 2). Initially, the mean IOP was 25.8±7.2 mmHg preoperatively, which decreased to 14.1±2.8 mmHg at 24 months (p=0.004) and further to 13.1±3.9 mmHg at 36 months (p=0.009) (Figures 1 and 2A).
 |
Table 2 Measurements at All Timepoints (mean±SD (n) [Min; Max]). P values are at Time Point Vs Baseline, Calculated Using Wilcoxon Signed-Rank Test |
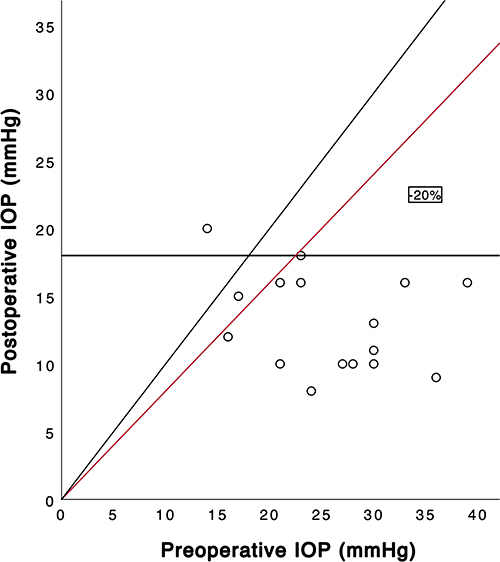 |
Figure 1 Scatterplot of intraocular pressure (IOP) at baseline vs postop (mean postop follow-up: 28.9±13 months). Points below the red line represent eyes with ≥20% reduction in IOP. The diagonal line indicates the same IOP at preop and postop. |
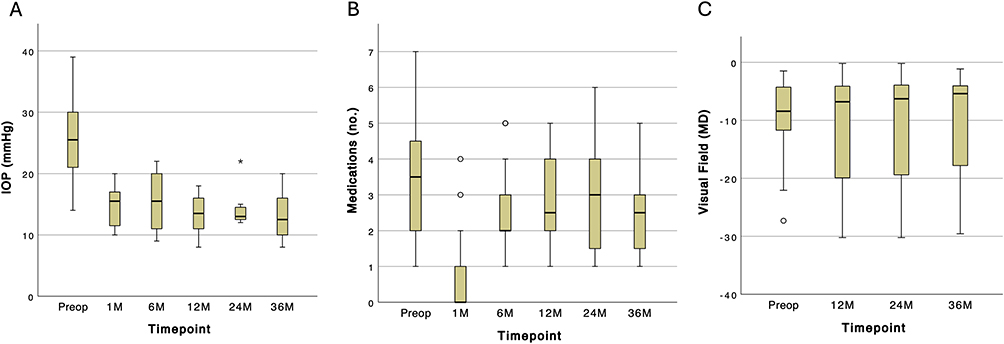 |
Figure 2 Whisker plots of (A) IOP, (B) medications, and (C) visual field data of all eyes. * statistical significance. Abbreviations: IOP, intraocular pressure; MD, mean deviation. |
This trend was also consistent among the 11 eyes (69%) that underwent standalone ABiC treatment (Table 3). Preoperatively, mean IOP was 26.1±6.52 mmHg, which significantly decreased to 13.1±1.07 mmHg (p=0.022) at 24 months and 12.4±3.21 mmHg (p=0.016) at 36 months. In the subgroup receiving combined ABiC and phacoemulsification, although direct statistical comparison of mean IOP changes at baseline (25±9.19) was not feasible, lower values were observed at 24 months (15.8±4.35) and 36 months (14±4.9) (Figure 3A).
 |
Table 3 Measurements at All Time Points (mean±SD (n) [Min; Max]) by Type of Procedure. P values are at Time Point Vs Baseline, Calculated Using Wilcoxon Signed-Rank Test (Not Available for Combined with Phacoemulsifcation Group Due to Small Number of Observations, n=5 or Less) |
 |
Figure 3 Whisker plots of (A) IOP, (B) medications and (C) visual field data of all eyes grouped by type of procedure. Abbreviations: IOP, intraocular pressure; MD, mean deviation. |
Table 4 displays IOP results for patients divided into subgroups of glaucoma before keratoplasty and no glaucoma before keratoplasty. For the 5 eyes with preexisting glaucoma, although lower mean IOP values were observed at all postoperative visits, statistical significance could not be established due to a low number of eyes in this subgroup. Among the 11 patients with steroid-induced glaucoma, the mean pre-ABiC IOP was 23.4±6.6 mmHg. Following ab interno canaloplasty, this decreased significantly at 12 months (14±2.31 mmHg, p=0.002), 24 months (14.4±3.3 mmHg, p=0.0014), and 36 months (12.2±4 mmHg, p=0.027).
 |
Table 4 Measurements at All Time Points (mean±SD (n) [Min; Max]) by Glaucoma Status Before Keratoplasty. P values are at Time Point Vs Baseline, Calculated Using Wilcoxon Signed-Rank Test (Not Available for Glaucoma Group Due to Small Number of Observations, n=5 or Less) |
Medications
While the mean number of medications required to manage IOP decreased at 24 months (2.8±1.6) and 36 months (2.5±1.2) compared to baseline (3.5±1.7) (Figure 2B), no statistically significant difference was observed across all postoperative visits (Table 2). Similar, non-statistically significant trends were observed when comparing baseline to the 24- and 36-month follow-ups in both standalone and combined ABiC groups as well as in eyes with and without a history of glaucoma before keratoplasty (Tables 3 and 4, Figure 3B).
Visual Field Changes
Across all eyes, we observed no statistically significant changes in the visual field mean deviation (VF-MD) at various time points throughout the study (Table 2 and Figure 2C). Notably, patients previously diagnosed with glaucoma demonstrated improvement in VF-MD following ABiC, with values changing from −6.9±4.8 at baseline to −3.4±1.9 at 36 months (see Table 4 and Figure 3C for detailed data).
Visual Acuity (VA)
Compared to the preoperative visit (mean VA = 0.57±0.47 logMAR), the mean VA significantly improved at 12 months (0.39±0.63 logMAR, p=0.025) and 24 months (0.3±0.4 logMAR, p=0.041) (Table 2). However, this improvement was no longer statistically significant at 36 months (0.31±0.36 logMAR, p=0.196). Eight eyes gained logMAR VA lines, five of which gained 2–5 lines while only 3 eyes lost one or more lines of logMAR VA.
Corneal Thickness
The mean central corneal thickness (CCT) measured 599.2±75.95 µm pre-operatively and 610.8±66.4 µm at 36 months, showing no statistical difference (p=0.398).
Success Rates
Various success endpoints were defined and are displayed in Table 5. Initially, we observed an increase in the number of eyes with IOP ≤15 mmHg, from 1 eye preoperatively to 10 eyes at 24 months and 8 eyes at 36 months. Additionally, at 24 months, 10 eyes had an IOP ≤18 mmHg, increasing to 11 eyes at 36 months, compared to only three eyes preoperatively. The mean reduction in IOP from baseline was 45.3% and 49.2% at 24 months and 36 months, respectively.
 |
Table 5 Success at Each Timepoint (Baseline, Month 12, Month 24, Month 36) |
Although no eyes were free of medication at any of the time points, the mean number of medications from baseline was reduced by −19.5% at 24 months and −28.6% at 36 months. Lastly, a reduction in both IOP and medication burden was achieved for 7 eyes (43.8%) at 2 and 3 years after surgery.
Complications
Two eyes experienced hyphema, necessitating anterior chamber irrigation. One of the DSAEK eyes required a repeat DSAEK three years after ABiC due to late-term endothelial failure. One eye did not have adequate IOP control after ABiC, necessitating a second glaucoma procedure using the EX-PRESS glaucoma filtration device (Alcon Laboratories Inc., Fort Worth, TX, USA) with Mitomycin C (MMC) approximately two months after ABiC: this eye was included in the preoperative data and at month 1 and excluded afterward.
Discussion
Keratoplasty remains a quintessential procedure for corneal specialists, with reports indicating an increasing trend in recent years.18 Elevated IOP ranks among the most frequent complications following keratoplasty, inclusive of keratoplasty types and pre-existing glaucoma.1,19–21 Oruçoglu et al highlighted a significant incidence of elevated IOP post-PKP, particularly in cases of preexisting glaucoma or when additional procedures were combined with PKP.22 While endothelial keratoplasty is less invasive, ocular hypertension remains a notable complication.23 Several factors contribute to post-operative elevated IOP, including retained viscoelastic material, inflammation, peripheral anterior synechiae, iatrogenic damage to the trabecular meshwork, and angle distortion.19 However, the prolonged use of steroids is among the most commonly implicated causes of ocular hypertension.24–26 Uncontrolled IOP poses a significant risk to visual outcomes and correlates with heightened rates of graft failure.27,28
Managing IOP in keratoplasty eyes typically involves the use of topical hypotensive medications. However, this approach presents two challenges. First, many antiglaucoma drops contain preservatives (eg benzalkonium chloride, etc). that can alter the ocular surface, exacerbating issues in post-keratoplasty eyes and leading to chronic inflammation, which can compromise graft survivability and visual acuity.29,30 Secondly, relying solely on eye drops to achieve target IOP levels may prove unsuccessful or insufficient. Traditional incisional glaucoma procedures are well known to increase the risk of graft failure).31–33
One emerging option in recent years is ABiC. Due to its minimally invasive nature, lack of intraocular device placement, and minimal manipulation of the iridocorneal angle, this MIGS procedure offers several advantages over traditional approaches, especially in post-keratoplasty eyes. In our previous study, we demonstrated the efficacy and safety of ABiC in reducing IOP and medication burden over 12 months following keratoplasty.16 However, efficacy and safety assessments of any surgical procedure require longer follow-up data. Long-term results with ABiC have recently been reported in the literature. A recent study by Koerber et al reported a statistically significant reduction in mean IOP and a decrease in the number of medications from 6 years post-ABiC with iTrack in eyes without keratoplasty.34 Another review article highlighted the consistency of ABiC across various studies, reporting a mean IOP decrease from 20±2.5 mmHg to 14±0.9 mmHg and a reduction in the number of glaucoma eye drops from 2.5±0.5 to 0.9±0.6 at 24 months postoperatively.35
In this study, we aimed to further establish the durability of ABiC in post-corneal transplant eyes with a longer follow-up over a 3-year period. Our study findings are consistent with these previous reports and others,11,17 affirming the long-term efficacy of ab-interno canaloplasty in reducing IOP. We also observed favorable and maintained outcomes regarding VA and VF-MD in the study’s eyes (Tables 2 and 5). Additionally, many cornea and anterior segment surgeons may be familiar with MIGS procedures, including ABiC. In our study, ABiC procedures were performed by both cornea and glaucoma specialists at our institution, suggesting that this procedure can be readily performed by anterior segment surgeons familiar with intraoperative gonioscopy and other required maneuvers.
Our results suggest that post-keratoplasty patients can maintain an acceptable IOP after ABiC with the same or fewer medications over three years. This alleviates cost, compliance, and other logistical burdens on patients, particularly when long-term use of steroid drops for keratoplasty survival is necessary. Though we observed surgical success in most patients, we note that one patient required repeat endothelial keratoplasty (DSAEK) after three years and one required an additional incisional glaucoma procedure. This suggests that while ABiC offers many advantages in post-keratoplasty eyes, it is not a panacea procedure for all cases and all circumstances to control IOP surgically.
Although there was a significant reduction in IOP, the decrease in medication use was less substantial. Combining ABiC with other minimally invasive techniques, such as gonioscopy-assisted transluminal trabeculotomy (GATT), has been shown in several studies to achieve further reductions in both IOP and medication requirements.36–38 For managing post-keratoplasty glaucoma, patients may benefit from the synergistic effect of these two approaches while preserving healthy conjunctiva for potential future trabeculectomy if needed.
Descemet membrane detachment (DMD) is a recognized complication of ABiC,39 that may be particularly concerning in post-keratoplasty eyes, as it could cause corneal decompensation.40 While no previous studies have specifically examined ABiC in post-keratoplasty cases, the reported incidence of DMD with ABiC generally ranges from 1.6% to 9.1%.11,41 This complication may result from excessive pressure during vasodilation or surgical trauma to the Descemet membrane or endothelium.42 Notably, no cases of DMD were observed in this cohort.
This study had several limitations, including its small sample size and retrospective nature, which restricted access to certain data, such as cup/disc ratio and optical coherence tomography data, particularly nerve fiber layer thickness. Future prospective studies with larger sample sizes (with further stratification for full-thickness, lamellar, and endothelial keratoplasties) are warranted to validate our findings. Additionally, including a broader range of corneal diseases or ocular conditions associated with elevated IOP would help further demonstrate the potential efficacy of ABiC in managing fragile eyes.
In summary, ABiC significantly reduced IOP, partially reduced eyedrop burden, effectively maintained VF-MD, and favorably maintained VA in eyes following keratoplasty for three years. These findings align with other studies demonstrating the long-term effectiveness of ABiC in eyes without prior keratoplasty. While no MIGS procedure is perfect in all cases, we propose that ABiC has certain features and characteristics, including adaptability, in post-corneal transplant eyes that merit consideration by corneal specialists.
Disclosure
Dr. Khaimi is Chief Medical Consultant for iTrack at Nova Eye Medical. The other authors have no financial or proprietary interest in any material or method mentioned in this manuscript. Dr Riaz reports speaking fees from AudioDigest, Bausch and Lomb, CorneaGen, and Medscape; consulting fees from Ambrx, Inc., Bausch and Lomb, Exelixis, Inc., ImmunoGen, Neuromora Therapeutics; and travel fees from Aurion Therapeutics.
References
1. Allen MB, Lieu P, Mootha VV. et al. Risk factors for intraocular pressure elevation after descemet stripping automated endothelial keratoplasty. Eye Contact Lens. 2010;36(4):223–227. doi:10.1097/ICL.0b013e3181e6ae30
2. Nguyen NX, Seitz B, Martus P, et al. Long-term topical steroid treatment improves graft survival following normal-risk penetrating keratoplasty. Am J Ophthalmol. 2007;144(2):318–319. doi:10.1016/j.ajo.2007.03.028
3. Kornmann HL, Gedde SJ. Glaucoma management after corneal transplantation surgeries. Curr Opin Ophthalmol. 2016;27(2):132–139. doi:10.1097/ICU.0000000000000237
4. Abdelghany AA, D’Oria F, Alio JL. Surgery for glaucoma in modern corneal graft procedures. Surv Ophthalmol. 2021;66(2):276–289. doi:10.1016/j.survophthal.2020.08.002
5. Irvine AR, Kaufman HE. Intraocular pressure following penetrating keratoplasty. Am J Ophthalmol. 1969;68(5):835–844. doi:10.1016/0002-9394(69)94577-2
6. Aldave AJ, Rudd JC, Cohen EJ, et al. The role of glaucoma therapy in the need for repeat penetrating keratoplasty. Cornea. 2000;19(6):772–776. doi:10.1097/00003226-200011000-00002
7. Banitt M, Lee RK. Management of patients with combined glaucoma and corneal transplant surgery. Eye. 2009;23(10):1972–1979. doi:10.1038/eye.2008.377
8. Tandon A, Espandar L, Cupp D, et al. Surgical management for postkeratoplasty glaucoma: a meta-analysis. J Glaucoma. 2014;23(7):424–429. doi:10.1097/IJG.0b013e31827a0712
9. Kwon YH, Taylor JM, Hong S, et al. Long-term results of eyes with penetrating keratoplasty and glaucoma drainage tube implant. Ophthalmology. 2001;108(2):272–278. doi:10.1016/S0161-6420(00)00496-6
10. Rahmania N, Rampat R, Moran S, et al. Outcomes of gel stent implantation for glaucoma in patients with previous corneal graft surgery: a case series. Cornea. 2020;39(4):417–421. doi:10.1097/ICO.0000000000002253
11. Khaimi MA. Canaloplasty: a minimally invasive and maximally effective glaucoma treatment. J Ophthalmol. 2015;2015:1–5. doi:10.1155/2015/485065
12. Stegmann R, Pienaar A, Grieshaber MC. Schlemm’s Canal Surgery: Restoring Physiological Aqueous Outflow. Glaucoma Therapy—State of the Art. Basel, Switzerland: Association for Continuing Education in Ophthalmology; 2009:113–120.
13. Johnson DH, Lutjen-Drecoll E. Glaucomatous Changes in the Trabecular Meshwork. In: Mechanisms of the Glaucomas. Totowa, NJ: Humana Press;1997:
14. Huang J, Camras LJ, Yuan F. Mechanical analysis of rat trabecular meshwork. Soft Matter. 2015;11(14):2857–2865. doi:10.1039/C4SM01949K
15. Koerber N, Ondrejka S. Clinical outcomes of canaloplasty via an ab-interno surgical technique using the iTrack device: a narrative review. Int Ophthalmol. 2022;43(6):2017–2027. doi:10.1007/s10792-022-02601-1
16. Riaz KM, Gill MS, Murphy DA, et al. Surgical management of intraocular pressure with ab interno canaloplasty in postkeratoplasty patients: 12-month results. Cornea. 2022. doi:10.1097/ICO.0000000000003009
17. Gallardo MJ. 24-month efficacy of viscodilation of schlemm’s canal and the distal outflow system with itrack ab-interno canaloplasty for the treatment of primary open-angle glaucoma. Clin Ophthalmol. 2021;15:1591–1599. doi:10.2147/OPTH.S272506
18. Xiao G, Tsou BC, Soiberman US, et al. Keratoplasty in the United States: trends and indications from 2015 to 2020. Cornea. 2023;42(11):1360–1364. doi:10.1097/ICO.0000000000003180
19. Huber KK, Maier AKB, Klamann MKJ, et al. Glaucoma in penetrating keratoplasty: risk factors, management and outcome. Graefes Arch Clin Exp Ophthalmol. 2013;251(1):105–116. doi:10.1007/s00417-012-2065-x
20. Chien AM, Schmidt CM, Cohen EJ, et al. Glaucoma in the immediate postoperative period after penetrating keratoplasty. Am J Ophthalmol. 1993;115(6):711–714. doi:10.1016/S0002-9394(14)73636-0
21. Vajaranant TS, Price MO, Price FW, et al. Visual acuity and intraocular pressure after descemet’s stripping endothelial keratoplasty in eyes with and without preexisting glaucoma. Ophthalmology. 2009;116(9):1644–1650. doi:10.1016/j.ophtha.2009.05.034
22. Oruçoglu F, Blumenthal EZ, Frucht-Pery J, et al. Risk factors and incidence of ocular hypertension after penetrating keratoplasty. J Glaucoma. 2014;23(9):599–605. doi:10.1097/IJG.0b013e31828700f5
23. Elalfy M, Maqsood S, Soliman S, et al. Incidence and risk factors of ocular hypertension/glaucoma after descemet stripping automated endothelial keratoplasty. Clin Ophthalmol. 2021;Volume 15:2179–2188. doi:10.2147/OPTH.S299098
24. Price MO, Price DA, Price FW. Long-term risk of steroid-induced ocular hypertension/glaucoma with topical prednisolone acetate 1% after descemet stripping endothelial keratoplasty. Cornea. 2024;43(3):323–326. doi:10.1097/ICO.0000000000003312
25. Liesenborghs I, Schouten JSAG, Berendschot TTJM, et al. Risk factors for the development of ocular hypertension after keratoplasty: a systematic review. Cornea. 2020;39(3):394–402. doi:10.1097/ICO.0000000000002209
26. Baltaziak M, Chew HF, Podbielski DW, et al. Glaucoma after corneal replacement. Surv Ophthalmol. 2018;63(2):135–148. doi:10.1016/j.survophthal.2017.09.003
27. Ang M, Mehta JS, Lim F, et al. Endothelial cell loss and graft survival after descemet’s stripping automated endothelial keratoplasty and penetrating keratoplasty. Ophthalmology. 2012;119(11):2239–2244. doi:10.1016/j.ophtha.2012.06.012
28. Gómez‐Benlloch A, Montesel A, Pareja‐Aricò L, et al. Causes of corneal transplant failure: a multicentric study. Acta Ophthalmol. 2021:99. doi:10.1111/aos.14708.
29. Holland EJ, Djalilian AR, Sanderson JP. Attenuation of ocular hypertension with the use of topical loteprednol etabonate 0.5% in steroid responders after corneal transplantation. Cornea. 2009;28(10):1139–1143. doi:10.1097/ICO.0b013e3181a3c52f
30. Tomić M, Kaštelan S, Metež Soldo K, et al. Influence of BAK-preserved prostaglandin analog treatment on the ocular surface health in patients with newly diagnosed primary open-angle glaucoma. Biomed Res Int. 2013;2013:1–7. doi:10.1155/2013/603782
31. Price MO, Thompson RW, Price FW. Risk factors for various causes of failure in initial corneal grafts. Archives of Ophthalmology. 2003;121(8):1087–1092. doi:10.1001/archopht.121.8.1087
32. Elhofi A, Helaly HA. Graft survival after penetrating keratoplasty in cases of trabeculectomy versus Ahmed valve implant. J Ophthalmol. 2018;2018. doi:10.1155/2018/9034964.
33. Boey PY, Mehta JS, Ho CL, et al. Outcomes of trabeculectomy after descemet stripping automated endothelial keratoplasty: a comparison with penetrating keratoplasty. Am J Ophthalmol. 2012;153(6):1091–1098.e2. doi:10.1016/j.ajo.2011.12.014
34. Wang M-S, Zheng M-Y, Fan X, et al. Glaucoma drainage device implantation and cyclophotocoagulation in the management of refractory glaucoma after Descemet-stripping automated endothelial keratoplasty. Int J Ophthalmol. 2024;17(2):257–264. doi:10.18240/ijo.2024.02.05
35. Koerber N, Ondrejka S. 6-year efficacy and safety of itrack ab-interno canaloplasty as a stand-alone procedure and combined with cataract surgery in primary open angle and pseudoexfoliative glaucoma. J Glaucoma. 2024;33(3):176–182. doi:10.1097/IJG.0000000000002311
36. Gallardo MJ, Pyfer MF, Vold SD, et al. Canaloplasty and trabeculotomy combined with phacoemulsification for glaucoma: 12-month results of the GEMINI study. Clin Ophthalmol. 2022;Volume 16:1225–1234. doi:10.2147/OPTH.S362932
37. Voykov B, Szurman P, Dimopoulos S, et al. Micro‐invasive suture trabeculotomy after canaloplasty: preliminary results. Clin Exp Ophthalmol. 2015;43(5):409–414. doi:10.1111/ceo.12482
38. Al Habash A, Alrushoud M, Al Abdulsalam O, et al. Combined Gonioscopy-Assisted Transluminal Trabeculotomy (GATT) with Ab Interno Canaloplasty (ABiC) in Conjunction with Phacoemulsification: 12-Month Outcomes. Clin Ophthalmol. 2020;Volume 14:2491–2496. doi:10.2147/OPTH.S267303
39. Lewis RA, Von Wolff K, Tetz M, et al. Canaloplasty: three-year results of circumferential viscodilation and tensioning of Schlemm canal using a microcatheter to treat open-angle glaucoma. J Cataract Refract Surg. 2011;37(4):682–690. doi:10.1016/j.jcrs.2010.10.055
40. Kramer N, Unterlauft JD, Girbardt C. The need of rebubbling in case of small graft detachments after Descemet Membrane Endothelial Keratoplasty (DMEK). Eur J Ophthalmol. 2023;33(3):1347–1353. doi:10.1177/11206721221146579
41. Jaramillo A, Foreman J, Ayyala RS, Duong M-H, Lorenceau J. Descemet membrane detachment after canaloplasty. J Glaucoma. 2014;23(1):23. doi:10.1097/IJG.0b013e318279ca7f
42. Izquierdo Villavicencio JC, Mejías Smith JA, Cañola Ramírez LA, et al. Hemorrhagic descemet membrane detachment during Ab interno canaloplasty. Case Rep Ophthalmol Med. 2019;2019:1–4. doi:10.1155/2019/3653954
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.