")
Back to Journals » Clinical Ophthalmology » Volume 19
Efficacy and Safety of Epi-On vs Epi-Off Corneal Cross-Linking in Corneal Ectasia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Authors Nughays RO, Bazayd AS, Alshamekh LA , Alshammari RA, Alanazi MA , Dahlan HY, Alsubhi JA, Alshammri SG, AlQurashi NA, Aldajani AH, Alrammah AH , Alenezi MN , Almutairi AA, Alomayri AF, Alghamdi S
Received 30 December 2024
Accepted for publication 13 March 2025
Published 8 May 2025 Volume 2025:19 Pages 1531—1541
DOI https://doi.org/10.2147/OPTH.S508618
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Reem O Nughays,1 Abdullah S Bazayd,1 Lujain A Alshamekh,2 Reemas A Alshammari,3 Mohammed A Alanazi,4 Hashem Y Dahlan,5 Jana A Alsubhi,6 Sara G Alshammri,7 Nouf A AlQurashi,8 Abdulaziz H Aldajani,9 Abdulrahman H Alrammah,9 Mariam N Alenezi,10 Areej Abdullah Almutairi,11 Abdulaziz F Alomayri,12 Saeed Alghamdi13
1College of Medicine, King Saud bin Abdulaziz for Health Sciences, Jeddah, Saudi Arabia; 2College of Medicine, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia; 3College of Medicine, Imam Mohammed bin Saud Islamic University, Riyadh, Saudi Arabia; 4College of Medicine, Northern Border University, Arar, Saudi Arabia; 5College of Medicine, Umm-Al Qura University, Makkah, Saudi Arabia; 6College of Medicine, University of Jeddah, Jeddah, Saudi Arabia; 7College of Medicine, Vision College, Riyadh, Saudi Arabia; 8College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 9College of Medicine, King Faisal University, Al-Hasa, Saudi Arabia; 10General Surgery Department, Farwaniya Hospital, Farwaniya, Kuwait; 11College of Medicine, Taif University, Taif, Saudi Arabia; 12College of Medicine, King Saud University, Riyadh, Saudi Arabia; 13Ophthalmology Department, King Abdulaziz Medical City, Jeddah, Saudi Arabia
Correspondence: Reem O Nughays, College of Medicine, King Saud bin Abdulaziz for Health Sciences, Jeddah, Saudi Arabia, Tel +966543200330, Email [email protected] Saeed Alghamdi, Ophthalmology Department, King Abdulaziz Medical City, Jeddah, Saudi Arabia, Email [email protected]
Abstract: Corneal ectasias are progressive conditions that impair vision and quality of life. Corneal collagen cross-linking (CXL) aims to halt disease progression by strengthening the cornea. This review compares two CXL methods, epithelium-on (epi-on) and epithelium-off (epi-off), to assess their safety and effectiveness for managing corneal ectasia. A systematic search up to July 2024 of PubMed, Medline, Web of Science, Cochrane Central, Google Scholar, and Scopus identified 13 randomized controlled trials (RCTs) involving 872 patients and 1041 eyes. Data were analyzed following PRISMA guidelines using fixed-effects and random-effects models. The primary outcome was the change in maximal keratometry (Kmax) at 12 months, with secondary outcomes including safety profile, best-corrected visual acuity (BCVA), uncorrected visual acuity (UCVA), spherical equivalent (SE), and endothelial cell count (ECC). The findings revealed no statistically significant differences between epithelium-on (epi-on) and epithelium-off (epi-off) CXL in Kmax, BCVA, UCVA, SE, or corneal curvature parameters. However, epithelium-off (epi-off) CXL was associated with less endothelial cell loss and higher rates of side effects, including corneal haze and postoperative discomfort. The choice of treatment should be tailored to individual patient needs, balancing clinical goals and safety considerations. This review highlights the need for further studies to optimize CXL approaches and improve outcomes while minimizing complications.
Keywords: corneal ectasia, corneal collagen cross-linking (CXL), epi-on, epi-off, keratoconus, maximal keratometry (Kmax), visual acuity, endothelial cell count (ECC)
Introduction
Corneal ectasia, including keratoconus, is a condition in which progressive thinning of the corneal stroma causes the cornea to become increasingly protruded, potentially leading to severe visual impairment.1 Keratoconus is the most common form of primary corneal ectasia.1 Keratoconus prevalence was higher in the Black population, followed by the Hispanic population.2 Genetic predisposition, particularly a family history of the condition, and environmental factors like eye rubbing and atopy are each associated with an increased risk of corneal ectasia.3 Corneal cross-linking (CXL) is among the limited interventions capable of halting the progression of this disease.4 The traditional epithelium-off corneal collagen cross-linking (epi-off CXL), where the corneal epithelium is removed, allows better penetration of riboflavin (vitamin B2), the photosensitizer used in CXL, and UV light.5 This UV light exposure induces the formation of reactive oxygen species, leading to the formation of additional cross-links between collagen fibers, strengthening the corneal structure.5 However, this technique carries risks like infection, pain, and longer recovery time.5 The newer transepithelial or epithelium-on corneal collagen cross-linking (epi-on CXL), where the epithelium is left intact, aims to reduce these risks, however, its effectiveness compared to epi-off CXL remains debated.6 CXL can be performed using two different approaches based on the duration of the procedure: standard and accelerated.7 Safety is paramount in these procedures, as it helps develop personalized treatment plans that maximize benefits and minimize risks.8 A systematic review and meta-analysis are necessary to synthesize existing evidence and clarify the safety and efficacy of epithelium-on (epi-on) and epithelium-off (epi-off) CXL techniques. Thus, this review aims to evaluate and compare these methods in corneal ectasia patients, focusing on changes in maximal keratometry (Kmax) within 12 months, visual acuity, and safety outcomes to inform clinical decision-making.
Methods
This systematic review and meta-analysis of randomized controlled trials (RCTs) was registered with the PROSPERO online database (identifier: CRD42024569437) and performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) checklist.
Search Strategy
We conducted a comprehensive search to identify relevant studies for inclusion in this systematic review and meta-analysis. The search was performed across the following electronic databases: PubMed, Medline, Web of Science, Cochrane Central Register of Controlled Trials, Google Scholar, and Scopus from their inception until July 2024. The search strategy was developed using a combination of Medical Subject Headings (MeSH) terms and relevant keywords to ensure the inclusion of related studies. It was conducted using the following terms: (“transepithelial corneal cross-linking” OR “epithelium-off corneal cross-linking” OR “corneal cross-linking”) AND (“corneal ectasia” OR “keratoconus” OR “ectatic corneal diseases”). The search was restricted to English-language publications to maintain consistency in the language of the included studies. No restrictions were placed on study design, population, or setting to capture all relevant studies. Additionally, we reviewed the reference lists of included studies and relevant reviews to identify any additional studies that the initial database search may not have captured.
Study Selection, Inclusion, and Exclusion Criteria
This study focused on full-text articles examining patients with any type of corneal ectasia, comparing epi-on with epi-off CXL. The primary outcome was the change in maximal keratometry (Kmax) at 12 months, with secondary outcomes including uncorrected and corrected distance visual acuity, as well as safety outcomes like complications and disease progression. Search results from electronic databases were exported as .RIS or .CSV files and imported into Rayyan software to remove duplicates. Four reviewers, working in pairs, screened titles and abstracts independently, and two other reviewers evaluated full-text articles that met the inclusion criteria: English-language RCTs focusing on epi-on vs epi-off techniques for corneal ectasia, with relevant clinical outcomes. Exclusion criteria involved non-English publications, non-ectasia conditions, non-comparative studies, unsuitable designs, and studies that report no outcomes of interest. In the event of any disagreements, a third author was designated to resolve the conflicts, achieve a consensus, and contact the study authors if needed.
Data Extraction and Risk of Bias Assessment
Two reviewers developed a data extraction sheet to document study details such as the title, first author, publication year, journal, and study location. Extracted information included study design, sample sizes, patient demographics (mean age, gender distribution), and criteria for inclusion and exclusion. Key clinical data collected encompassed keratometry values (Kmax, and steep/flat) central and thinnest corneal thickness, corneal power, spherical equivalent, demarcation line depth, and visual acuity (UCVA and BCVA) at baseline and 12 months. Endothelial cell counts and any adverse events were also noted, as was whether each study used an accelerated technique. Four authors handled data extraction, with two overseeing accuracy. The risk of bias assessment was carried out by two groups of two members. Each author evaluated the article independently using the Cochrane Risk of Bias Tool for RCTs without consulting the members of their group to minimize bias. This tool assesses several domains, including the randomization process, intervention process, missing data, measuring outcome, and selection of reported results. Each domain helps identify specific types of bias, such as selection bias, performance bias, detection bias, attrition bias, and reporting bias. In case of discrepancies, the group members discussed their assessment to achieve a consensus.
Outcome Measures
The primary outcome measure was to compare the maximum keratometry (Kmax) at 12 months follow-up between the epi-on and epi-off groups. Our secondary outcomes included the measurement of uncorrected visual acuity (UCVA) and best-corrected visual acuity (BCVA) at 12 months postoperatively. Additionally, examined flat (Kflat) and steep (Ksteep) keratometry values, and endothelial cell density (ECC) at 12 months after treatment in both groups. Moreover, the identification of any adverse events is a key component, essential for evaluating safety. Corneal thickness, and spherical equivalent (SE) were provided as supplementary materials Figures S1 and S2, respectively.
Data Synthesis and Analysis
The data synthesis was conducted using Review Manager (RevMan) software version 5.4. The Cochrane Collaboration, 2020. For continuous outcomes, we calculated the mean differences with 95% confidence intervals (CIs). To assess variability among studies, we used the I² statistic along with its associated p-value to evaluate heterogeneity. A random-effects model was used when the I² value exceeded 50%, indicating significant heterogeneity. In cases of low heterogeneity (I² ≤ 50%), a fixed-effects model was applied. For the random-effects analysis, the DerSimonian and Laird model was used, with weights calculated using the inverse variance method to appropriately balance the influence of different studies. Subgroup analyses were initially planned to explore differences related to the timing of procedures (accelerated vs standard CXL). However, subgroup analysis was omitted when only one study was available for a particular subgroup, as limited data precluded drawing meaningful conclusions. Sensitivity analyses were conducted for outcomes demonstrating high heterogeneity to ensure the robustness of the findings. Qualitative analysis was conducted on all studies, whether included in meta-analysis or not, to provide a broader understanding of the evidence. Lastly, we visually analyzed the asymmetry of funnel plots when at least 10 studies were obtained. Statistical significance was determined with p-values, considering a threshold of p < 0.05. This thorough approach allowed us to provide a detailed and reliable analysis, accounting for the variability across studies and ensuring that the study quality was rigorously evaluated.
Results
Study Selection
A total of 1403 records were initially identified from various databases, including PubMed, Medline, Web of Science, the Cochrane Central Register of Controlled Trials, Google Scholar, and Scopus. These records were located using a combination of Medical Subject Headings (MeSH) terms and relevant keywords. After removing 430 duplicates, 973 records remained for screening based on their titles and abstracts. From these, 54 articles were selected for a more detailed eligibility assessment. Upon comprehensive full-text review, 41 articles were excluded because they did not meet the inclusion criteria for several reasons, such as not reporting the outcome of interest, not being RCTs, or not being completed studies. Ultimately, 13 studies were included in the final review and 10 in the meta-analysis. See flow diagram Figure 1
 |
Figure 1 PRISMA flow diagram showing the process of study selection of the quality of individual trials. Notes: PRISMA figure adapted from Liberati A, Altman D, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of clinical epidemiology. 2009;62(10). Creative Commons.9 |
Characteristics of Included Studies
We included 13 RCTs comprising a total of 872 patients and 1041 eyes, with 478 eyes receiving epi-on CXL and 563 eyes receiving epi-off CXL.10–22 However, one study did not specify the number of eyes treated. Participants’ mean ages ranged from 14 to 31.5 years across all studies. The procedure examined included both standard and accelerated CXL protocols. These studies were conducted in various countries, including Egypt, Italy, the USA, Sweden, Norway, Saudi Arabia, the Netherlands, Jordan, and Russia. All 13 studies were included in the qualitative analysis, while 11 studies were included in the meta-analysis, depending on the outcome measures. Details of studies’ characteristics and quality ratings are provided in Table S1 of the supplementary material.
Qualitative Analysis
Kmax
Most studies showed no significant difference in Kmax between epi-on and epi-off groups.10,11,14,15 However, some reported significant differences at specific time points.12,13,16 Pediatric studies comparing SCXL, ACXL, and TCXL indicated that SCXL had greater Kmax improvement, with TCXL showing less improvement and even deterioration.17,18
Visual Acuity
Several studies found no significant difference in BCVA between epi-on and epi-off groups.10,11,16,21 Though others reported the epi-off group achieving better outcomes over time.12,13,19,20 In pediatric cases, SCXL led to more consistent improvement in CDVA compared to ACXL and TCXL, with TCXL often showing minimal gains or worsening.17,18
Endothelial Cell Count
One study observed minimal changes in endothelial cell density in both epi-on and epi-off groups from baseline to 12 months, with no statistically significant difference within or between groups.10 Other studies similarly found no significant ECC changes over time in either group.13,14,22 One study noted a temporary decrease in ECC three days postoperatively in the control group, but this effect was short-lived, with differences being significant only at the three-day mark.15
Adverse Events
The adverse events associated with epi-on and epi-off CXL were analyzed across several studies. Epi-Off CXL generally resulted in more complications, such as bacterial conjunctivitis, delayed epithelial healing, stromal haze, and corneal scarring. On the other hand, epi-on CXL was linked to fewer adverse events, with most patients experiencing less pain, fewer instances of epithelial erosion, and lower rates of corneal haze. This suggests that epi-on CXL may be associated with a more favorable safety profile Table 1.
 |
Table 1 Adverse Events in Epithelium-on (Epi-On) vs Epithelium-off (Epi-Off) |
Quantitative Analysis
Kmax
Eight studies assessed the Kmax of the CXL epi-on and epi-off subgroups by applying standard and accelerated methods using a fixed-effect model.10,11,13–18 The meta-analysis indicated an improvement in the epi-off group compared to epi-on, but the pooled mean difference was non-significant 0.06 diopters (D) (95% confidence interval: −0.30 D, 0.42 D; p = 0.76). The included studies showed consistent results, with no substantial heterogeneity (I² = 14%, p = 0.32) Figure 2A.
 |
Figure 2 Forest plots comparing (A) Kmax (D), (B) Ksteep (D), and (C) Kflat (D) of epi-on and epi-off CXL after 12 months follow-up. Abbreviations: Chi², chi-square statistic; CI, confidence interval; Epi-off, epithelium-off; Epi-on, epithelium-on; IV, inverse variance; I², I-square heterogeneity statistic; Z, Z statistic. |
Ksteep
Five studies compared the Ksteep in the CXL epi-on and epi-off using a fixed-effect model.10,13,16,19,22 The meta-analysis found no significant pooled mean difference of 0.33 D (95% CI: −0.03 D, 0.69 D; p= 0.07), with improvement noticed more in the epi-off group. The studies revealed no substantial heterogeneity (I² = 36%, p = 0.18), indicating consistent results Figure 2B.
Kflat
Four studies evaluated Kflat in both the CXL epi-on and CXL epi-off groups using a fixed-effect model. The meta-analysis demonstrated greater improvement in the epi-on group.10,13,16,22 However, no significant difference was found between the groups, with a pooled mean difference of −0.35 D (95% confidence interval: −0.88 D, −0.19 D; p = 0.20). There was no significant variation among the studies (I² = 0%, p = 0.55), indicating uniform findings Figure 2C.
Best Corrected Visual Acuity (BCVA)
Ten studies were considered to examine BCVA between the CXL epi-on and CXL epi-off subgroups under both standard and accelerated techniques using a random-effects model.10,11,13–19,22 In the subgroup meta-analysis, the standard group showed no significant difference, with a p-value of 0.62. However, the accelerated group showed a significant difference with a p-value of 0.02. On the other hand, the overall meta-analysis revealed a non-significant pooled mean difference of 0.03 logMAR (95% confidence interval: −0.05 to 0.11 logMAR; p = 0.48) favoring epi off group. The studies showed significant heterogeneity (I² = 91%, p < 0.01), indicating heterogeneous outcomes Figure 3A.
 |
Figure 3 Forest plots comparing (A) BCVA (logMar), (B) UCVA (logMar), and (C) ECC (cells/mm²) of epi-on and epi-off CXL after 12 months of follow-up. Abbreviations: Chi², chi-square statistic; CI, confidence interval; Epi-off, epithelium-off; Epi-on, epithelium-on; IV, inverse variance; I², I-square heterogeneity statistic; Z, Z statistic. |
Uncorrected Visual Acuity (UCVA)
Eight studies evaluated UCVA in the CXL epi-on and epi-off subgroups under standard and accelerated procedures using a random-effects model.10,11,13–18 The meta-analysis found no significant difference in the subgroup analysis, and a non-significant pooled mean difference of 0.05 logMAR (95% confidence interval: −0.08 to 0.17 logMAR; p = 0.49) was observed for the overall result. However, the epi-off group showed a more pronounced enhancement in outcomes. The studies demonstrated significant heterogeneity (I² = 85%, p < 0.001), indicating a wide range of outcomes Figure 3B.
Endothelial Cell Count (ECC)
Six studies assessed ECC in the CXL epi-on and epi-off using a fixed-effect model.10,11,13–15,22 The meta-analysis revealed a significant pooled mean difference of −84.71 cells/mm² (95% confidence interval: −137.17 to −32.26 cells/mm²; p < 0.01) favoring epi-off. The studies showed no substantial heterogeneity (I² = 37%, p = 0.16), indicating consistent effect estimates Figure 3C.
Publication Bias
The funnel plot shows a symmetrical distribution of studies around the central vertical line (MD = 0), indicating a low likelihood of publication bias. The clustering of studies near the top, where the standard error is small, suggests that the studies are generally large and provide more precise effect size estimates. Funnel plot is shown in Figure S3 of the supplementary material.
Risk of Bias
A total of 10 studies were classified as having a low risk of bias, as they received low-risk ratings in most domains, ensuring methodological robustness.10–13,15–19,22 Additionally, three studies were categorized as having a high risk of bias.14,20,21 The risk of bias assessment indicates that most studies were generally well-conducted, with no concerns regarding randomization, data completeness, and outcome reporting. However, blinding of participants, staff and outcome assessment was often absent, raising concerns about potential performance and detection bias Figure 4.
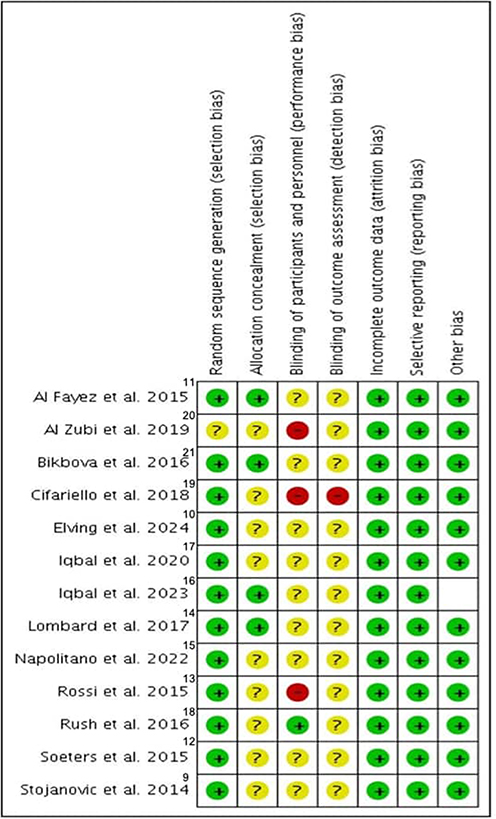 |
Figure 4 Diagram showing an assessment of the quality of individual trials. The red color represents a high risk of bias, yellow indicates some concern, green represents a low risk of bias. |
Discussion
In this systematic review and meta-analysis, we compared the safety and efficacy of epi-on versus epi-off CXL in patients with corneal ectasia. While both techniques are known to halt the progression of corneal ectasia, this review provides a nuanced comparison of their relative advantages and limitations. Among the studies reviewed, three employed accelerated protocol,11,17,18 while the remaining ten employed standard protocol.10,12–16,19–22 Most of these studies focused on adult age groups,10–16,20–22 with two specifically addressed pediatric populations,17,18 and one assessed both groups.19 All studies included data for a follow-up period of 12 months,10–19,21,22 except for one study that only provided data for a 24-month follow-up without documenting data for the 12-month period.20 The primary outcome measure, Kmax, showed a non-significant mean difference between epi-on and epi-off techniques. However, the majority of studies indicated a greater reduction in Kmax with the epi-off technique. We found no significant differences in Kmax, Kflat, Ksteep, UCVA, BCVA, between epi-on and epi-off CXL techniques. This could be due to the small sample sizes in the included studies, ranging from 70 eyes in one arm to 12 eyes, which may have lacked sufficient statistical power to detect meaningful differences. These findings align with those of Wen et al23 and D’Oria et al24 who similarly reported no differences in UDVA, CDVA, and Kmax at one year. Contrastingly, Kobashi et al25 observed better Kmax measurements with epi-off CXL, a result differing from our study. Despite this, they also noted a higher incidence of adverse events with epi-off CXL, consistent with our finding of more complications in the epi-off group. Nath et al5 were consistent with our results in terms of safety, highlighting epi-on CXL as safer and comparable in visual outcomes. However, they found it less effective in halting disease progression, which diverges from our findings of no significant difference in progression. D’Oria et al24 also reported comparable results in endothelial parameters, but our study identified significant differences in ECC, suggesting potential variability that warrants further investigation. Despite the non-significant results, the clinical implications remain important. While the epi-off technique may lead to slightly greater reductions in Kmax, its overall effect on visual acuity and corneal parameters appears comparable to the epi-on approach. This means that the decision between the two techniques should also take into account the real-world factors such as patient safety, recovery time, and accessibility, especially in resource-limited settings. The preservation of the epithelial layer likely contributes to offer a natural barrier against infection and other complications, making epi-on CXL more suitable for patients with compromised corneas. The epi-on CXL would, therefore, be more favorable to such patients due to safety and speedy recovery aspects. This systematic review’s strengths include a search approach that includes six databases. Furthermore, rigorous methodological assessment for study quality. Moreover, this systematic review includes a randomized controlled trial design that directly compares epi-off and epi-on CXL procedures, reducing bias and increasing dependability. It assesses multiple outcome indicators, including visual acuity, keratometry, and postoperative complications. The 12-month follow-up period provides strong longitudinal data, increasing the generalizability of the findings and aiding therapeutic decision-making in corneal ectasia treatment. However, this systematic review also has a few limitations. The differences in patient populations, study methods, and procedural protocols contributed to the heterogeneity seen across studies. Factors such as variations in riboflavin concentration, UV exposure times, and the use of either standard or accelerated CXL techniques may have influenced the results. Additionally, most studies focused on adults, with only a few including pediatric populations, further contributing to the variability, particularly in visual acuity outcomes. However, sensitivity analysis, where individual studies were systematically removed, showed no significant changes in the overall results.Another limitation was the potential for publication bias. Although the funnel plot suggested a low risk, the lack of Egger’s test prevents a definitive confirmation. One last drawback was the small sample size per study; on the other hand, the total number of cases included in the meta-analysis provided sufficient statistical power for the analysis. This underlines the need for future studies, in particular RCTs, with uniform methodologies and longer follow-up periods so that more definite conclusions can be drawn.
Conclusion
This systematic review and meta-analysis compared the safety and efficacy of epi-on and epi-off CXL in corneal ectasia. While significant differences were found in endothelial cell count, other outcomes showed no notable variation between the techniques. Epi-off CXL reduced keratometry parameters but had a higher incidence of complications such as delayed epithelial healing, stromal haze, and corneal scarring. Epi-on CXL, however, demonstrated a more favorable safety profile with fewer adverse events. These findings emphasize the need for personalized treatment decisions, balancing desired outcomes with potential risks.
Funding
This study did not receive any financial support.
Disclosure
The authors declare no conflicts of interest.
References
1. Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42(4):297–319. doi:10.1016/s0039-6257(97)00119-7
2. Singh RB, Parmar UPS, Jhanji V. Prevalence and economic burden of keratoconus in the United States. Am J Ophthalmol. 2024;259:71–78. doi:10.1016/j.ajo.2023.11.009
3. Gordon-Shaag A, Millodot M, Shneor E, Liu Y. The genetic and environmental factors for keratoconus. Biomed Res Int. 2015;2015:795738. doi:10.1155/2015/795738
4. Gomes JA, Tan D, Rapuano CJ, et al. Global consensus on keratoconus and ectatic diseases. Cornea. 2015;34(4):359–369. doi:10.1097/ICO.0000000000000408
5. Nath S, Shen C, Koziarz A, et al. Transepithelial versus epithelium-off corneal collagen cross-linking for corneal ectasia: a systematic review and meta-analysis. Ophthalmology. 2021;128(8):1150–1160. doi:10.1016/j.ophtha.2020.12.023
6. Hersh PS, Stulting RD, Muller D, Durrie DS, Rajpal RK; United States Crosslinking Study Group. United States multicenter clinical trial of corneal collagen crosslinking for keratoconus treatment [published correction appears in Ophthalmology. 2017 Dec;124(12):1878. doi: 10.1016/j.ophtha.2017.09.014]. Ophthalmology. 2017;124(9):1259–1270. doi:10.1016/j.ophtha.2017.03.052
7. Khairy HA, Elsawy MF, Said-Ahmed K, Zaki MA, Mandour SS. Accelerated versus standard corneal cross linking in the treatment of ectasia post refractive surgery and penetrating keratoplasty: a medium term randomized trial. Int J Ophthalmol. 2019;12(11):1714–1719. doi:10.18240/ijo.2019.11.08
8. Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003;135(5):620–627. doi:10.1016/s0002-9394(02)02220-1
9. Liberati A, Altman D G, Tetzlaff J, Mulrow C, Gotzsche P C, Ioannidis J P, Clarke M, Devereaux P J, Kleijnen J and Moher D. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ, 339(jul21 1), b2700–b2700. 10.1136/bmj.b2700
10. Stojanovic A, Zhou W, Utheim TP. Corneal collagen cross-linking with and without epithelial removal: a contralateral study with 0.5% hypotonic riboflavin solution. Biomed Res Int. 2014;2014:619398. doi:10.1155/2014/619398
11. Elving S, Fredriksson A, Beckman Rehnman J, Behndig A. Randomized clinical trial comparing customized corneal crosslinking: epi-on in high oxygen and epi-off in room air for keratoconus. J Cataract Refract Surg. 2024;50(7):746–753. doi:10.1097/j.jcrs.0000000000001442
12. Al Fayez MF, Alfayez S, Alfayez Y. Transepithelial versus epithelium-off corneal collagen cross-linking for progressive keratoconus: a prospective randomized controlled trial. Cornea. 2015;34(Suppl 10):S53–S56. doi:10.1097/ICO.0000000000000547
13. Soeters N, Wisse RP, Godefrooij DA, Imhof SM, Tahzib NG. Transepithelial versus epithelium-off corneal cross-linking for the treatment of progressive keratoconus: a randomized controlled trial. Am J Ophthalmol. 2015;159(5):821–8.e3. doi:10.1016/j.ajo.2015.02.005
14. Rossi S, Orrico A, Santamaria C, et al. Standard versus trans-epithelial collagen cross-linking in keratoconus patients suitable for standard collagen cross-linking. Clin Ophthalmol. 2015;9:503–509. doi:10.2147/OPTH.S73991
15. Lombardo M, Giannini D, Lombardo G, Serrao S. Randomized controlled trial comparing transepithelial corneal cross-linking using iontophoresis with the Dresden protocol in progressive keratoconus. Ophthalmology. 2017;124(6):804–812. doi:10.1016/j.ophtha.2017.01.040
16. Napolitano P, Tranfa F, D’Andrea L, et al. Topographic outcomes in keratoconus surgery: epi-on versus epi-off iontophoresis corneal collagen cross-linking. J Clin Med. 2022;11(7):1785. doi:10.3390/jcm11071785
17. Iqbal M, Gad A, Kotb A, Abdelhalim M. Analysis of the outcomes of three different cross-linking protocols for treatment of paediatric keratoconus: a multicentre randomized controlled trial. Acta Ophthalmol. 2024;102(1):e105–e116. doi:10.1111/aos.15686
18. Iqbal M, Elmassry A, Saad H, et al. Standard cross-linking protocol versus accelerated and transepithelial cross-linking protocols for treatment of paediatric keratoconus: a 2-year comparative study. Acta Ophthalmol. 2020;98(3):e352–e362. doi:10.1111/aos.14275
19. Rush SW, Rush RB. Epithelium-off versus transepithelial corneal collagen crosslinking for progressive corneal ectasia: a randomised and controlled trial. Br J Ophthalmol. 2017;101(4):503–508. doi:10.1136/bjophthalmol-2016-308914
20. Cifariello F, Minicucci M, Di Renzo F, et al. Epi-Off versus epi-on corneal collagen cross-linking in keratoconus patients: a comparative study through 2-year follow-up. J Ophthalmol. 2018;2018:4947983. doi:10.1155/2018/4947983
21. Al Zubi K. Transepithelial versus epithelium off crosslinking for treating keratoconus among Jordanians.pdf, Google Drive. 2019. Available from: https://drive.google.com/file/d/1I9PVi7kO5Nmw0v3DgAYRxkB_KJIzyefw/view?usp=sharing.
22. Bikbova G, Bikbov M. Standard corneal collagen crosslinking versus transepithelial iontophoresis-assisted corneal crosslinking, 24 months follow-up: randomized control trial. Acta Ophthalmol. 2016;94(7):e600–e606. doi:10.1111/aos.13032
23. Wen D, Song B, Li Q, et al. Comparison of epithelium-off versus transepithelial corneal collagen cross-linking for keratoconus: a systematic review and meta-analysis. Cornea. 2018;37(8):1018–1024. doi:10.1097/ICO.0000000000001632
24. D’Oria F, Palazón A, Alio JL. Corneal collagen cross-linking epithelium-on vs. epithelium-off: a systematic review and meta-analysis. Eye Vis. 2021;8(1):34. doi:10.1186/s40662-021-00256-0
25. Kobashi H, Rong SS, Ciolino JB. Transepithelial versus epithelium-off corneal crosslinking for corneal ectasia. J Cataract Refract Surg. 2018;44(12):1507–1516. doi:10.1016/j.jcrs.2018.08.021
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.