")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
Efficacy and Safety of Hepatic Artery Infusion Chemotherapy Combined with Donafenib and Camrelizumab in the Treatment of Patients with Unresectable Hepatocellular Carcinoma: A Retrospective, Single-Arm Study
Authors Wu C, Fu Z, Pan L, Li J, Zhou Y , Sun R, Gou Y, Zhao Y, Wang Z, Qiu Y, Huang P
Received 20 March 2025
Accepted for publication 27 June 2025
Published 10 July 2025 Volume 2025:12 Pages 1353—1367
DOI https://doi.org/10.2147/JHC.S525454
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr David Gerber
Chenrui Wu,1,* Zixuan Fu,1,* Long Pan,1 Jiachu Li,2 Yin Zhou,3 Ruirui Sun,1 Yang Gou,1 Yaowu Zhao,1 Zhouyan Wang,1 Yuhao Qiu,1 Ping Huang1
1Department of Hepatobiliary Surgery, First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2Department of Oncology, First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 3Department of Radiology, First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ping Huang, Department of Hepatobiliary Surgery, The First Affiliated Hospital of Chongqing Medical University, No. 1, Youyi Road, Yuzhong District, Chongqing, 400016, People’s Republic of China, Email [email protected]
Purpose: To evaluate the efficacy and safety of hepatic artery infusion chemotherapy with oxaliplatin, fluorouracil, and leucovorin (FOLFOX-HAIC) combined with donafenib and camrelizumab in patients with unresectable hepatocellular carcinoma (uHCC).
Patients and Methods: This retrospective study analyzed clinical data from 49 uHCC patients treated with FOLFOX-HAIC, donafenib tablets, and camrelizumab at the First Affiliated Hospital of Chongqing Medical University between November 1, 2021, and November 30, 2024. The primary endpoint was the objective response rate (ORR), assessed according to Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 and modified RECIST (mRECIST). Secondary endpoints included surgical conversion rate, disease control rate (DCR), progression-free survival (PFS), overall survival (OS), duration of response (DOR), and safety.
Results: The median follow-up duration was 20.3 months. Patients had a mean age of 55.9 years and a mean tumor diameter of 9.9 cm, with 25 patients (51%) presenting with extrahepatic metastasis. According to RECIST v1.1, the ORR was 57.1%, and the DCR was 79.6%. Under mRECIST criteria, the ORR increased to 59.2%, while the DCR remained at 79.6%. The median PFS was 12.1 months, and the median OS was 26.0 months. Twelve patients (24.5%) achieved successful conversion, with five patients (10.2%) undergoing surgery achieving R0 resections. Two patients (4.1%) achieved a pathological complete response (pCR). All patients experienced treatment-related adverse events (TRAEs), with Hypoalbuminemia (87.8%) and Hand-foot skin reaction (79.6%) being the most common. Grade 3 or higher TRAEs were observed in 61.2% of patients.
Conclusion: For patients with uHCC, the combination therapy of FOLFOX-HAIC with donafenib and camrelizumab demonstrates favorable efficacy and manageable adverse events.
Keywords: hepatocellular carcinoma, donafenib, camrelizumab, oxaliplatin, leucovorin, fluorouracil
Introduction
Primary liver cancer is a prevalent malignant tumor globally. In 2022, it was responsible for over 750,000 deaths worldwide, ranking as the third leading cause of cancer-related mortality after lung and colorectal cancers, and the sixth most common cancer overall. Hepatocellular carcinoma (HCC) constitutes 75% to 85% of all primary liver cancer cases.1 Due to its insidious onset and challenges in early diagnosis, many patients are diagnosed at intermediate or advanced stages, thereby missing opportunities for curative treatment. In China, surgical resection is employed in only 15% to 30% of initial HCC treatments, while the remaining unresectable hepatocellular carcinomas (uHCC) are typically managed with non-surgical approaches, resulting in a 5-year survival rate of merely 14.1%.2
In recent years, for patients with advanced uHCC, systemic therapy has emerged as the principal clinical management strategy. Tyrosine kinase inhibitors (TKIs), such as donafenib and lenvatinib, have manifested significant efficacy in prolonging the median survival in crucial clinical trials and have exhibited favorable safety profiles.3,4 Furthermore, treatment regimens based on the combination of immune checkpoint inhibitors (ICIs) and anti-angiogenic drugs, such as atezolizumab in combination with bevacizumab, sintilimab in combination with bevacizumab analogues, and apatinib in combination with camrelizumab, have surpassed traditional sorafenib monotherapy in multiple Phase III trials, attaining superior progression-free survival (PFS) and objective response rates (ORR), offering more efficacious treatment alternatives for advanced liver cancer.5–7 Concurrently, for patients with uHCC, conventional local treatment modalities, such as transcatheter arterial chemoembolization (TACE), radiotherapy (RT), and hepatic artery infusion chemotherapy (HAIC), have been extensively applied and achieved certain therapeutic efficacies.8
Currently, locoregional-systemic combination therapy has emerged as a pivotal focus in the management of uHCC in China.2 This integrated therapeutic paradigm not only achieves effective tumor progression control but also enhances both survival rates and conversion therapy success. FOLFOX-HAIC (hepatic artery infusion chemotherapy with oxaliplatin, fluorouracil, and leucovorin), a cornerstone of transarterial interventions, delivers high-concentration chemotherapeutic agents directly via the hepatic arterial system, enhancing tumoral cytotoxicity while minimizing systemic toxicity through targeted drug delivery.9 Donafenib, a novel oral multikinase inhibitor targeting Vascular Endothelial Growth Factor (VEGF) Receptor, Platelet-Derived Growth Factor (PDGF) Receptor, and Raf kinase signaling pathways, demonstrates promising clinical potential by dual inhibition of tumor angiogenesis and cellular proliferation.10 In the ZGDH3 trial, donafenib exhibited superior efficacy over sorafenib, achieving a median overall survival (OS) of 12.1 months in advanced HCC patients.3 Concurrently, camrelizumab, a humanized anti–programmed cell death protein 1 (PD-1) monoclonal antibody, potentiates antitumor immunity by disrupting PD-1/PD-L1 interactions, thereby reversing T-cell exhaustion.11 This immunomodulatory mechanism underlies its demonstrated capacity to improve tumor response and prolong survival outcomes in uHCC populations.
Based on the above background, we conducted a retrospective single-arm study to evaluate the clinical efficacy and safety of this triple therapy and to provide additional clinical evidence for the treatment of uHCC.
Materials and Methods
Study Design and Patients
This retrospective study collected the clinical data of 49 patients with uHCC who received the FOLFOX-HAIC combined with donafenib and camrelizumab treatment regimen at the First Affiliated Hospital of Chongqing Medical University from November 1, 2021 to November 30, 2024. All patients were included in the efficacy and safety analyses. The diagnosis of uHCC in each case was confirmed by a multidisciplinary team (MDT) from the Department of Hepatobiliary Surgery, which comprised specialists in hepatobiliary surgery, medical oncology, infectious diseases, gastroenterology, radiology, pathology, and clinical nutrition. The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Institutional Review Board of the First Affiliated Hospital of Chongqing Medical University (approval number: 2025–282-01). Given the retrospective design and the use of anonymized patient data, the requirement for informed consent was waived by the ethics committee.
Inclusion criteria: Age ≥ 18 years; diagnosed with HCC through radiology or pathology according to the National Comprehensive Cancer Network (NCCN) clinical practice guidelines; at least one measurable lesion (tumor lesion with a computed tomography (CT) scan long diameter ≥ 10mm, lymph node lesion with a CT scan short diameter ≥ 15mm) based on the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1; initially diagnosed with unresectable advanced HCC and completed at least one course of FOLFOX-HAIC combined with donafenib and camrelizumab treatment; Eastern Cooperative Oncology Group (ECOG) performance status score ≤ 1; Child-Pugh score ≤ 8; normal major organ function.
Exclusion criteria: Pathologically confirmed as the following types: fibrolamellar HCC, sarcomatoid HCC, or HCC-intrahepatic cholangiocarcinoma (HCC-ICC) mixed type; previously received other systemic anti-tumor treatments (such as targeted drugs, immune checkpoint inhibitors, etc). or local treatments (such as transcatheter arterial chemoembolization, radiotherapy or ablation therapy). Other serious diseases that may affect the assessment of the study’s efficacy or safety (such as uncontrolled cardiovascular diseases, active infections, etc).; incomplete medical records, unable to provide key information required for the study; currently receiving other anti-tumor treatments (excluding antiviral treatments).
Therapeutic Regimen
FOLFOX-HAIC: A femoral artery puncture was performed using the Seldinger technique, and a catheter or microcatheter was inserted into the main feeding artery of the tumor under the guidance of digital subtraction angiography (DSA). For tumors with rich blood supply, the main feeding artery will receive chemotherapy perfusion, while the treatment of secondary feeding arteries will be determined through MDT discussion, potentially involving iodized oil embolization. After the arterial catheterization was completed, the patient was returned to the ward to receive FOLFOX chemotherapy perfusion: oxaliplatin (Sanofi (Hangzhou) Pharmaceutical Co., Ltd., Hangzhou, Zhejiang Province, China), at a dose of 85 mg/m² for tumors less than 10 cm in diameter and 130 mg/m² for tumors greater than or equal to 10 cm, administered for 2–3 hours via arterial infusion ; leucovorin (Jiangsu Hengrui Pharmaceuticals Co., Ltd., Lianyungang, Jiangsu Province, China), at a dose of 400 mg/m², administered for 1–2 hours via arterial infusion; followed by an arterial push injection of 5-fluorouracil (Hainan Poly Pharm Co., Ltd., Haikou, Hainan Province, China) at a dose of 400 mg/m² and continuous arterial infusion at a dose of 2400 mg/m² for 46 hours. Thirty minutes before starting HAIC treatment, flurbiprofen, tropisetron, and dexamethasone were routinely used for pain relief and antiemesis; during HAIC, symptomatic treatments such as liver and stomach protection and nutritional support were provided as needed. HAIC was administered every 3 weeks, with patients receiving up to six cycles. Following the HAIC phase, maintenance therapy with targeted agents and immune checkpoint inhibitors was continued. Discontinuation or modification of HAIC was based on the following criteria: Occurrence of grade ≥3 treatment-related adverse events (as per Common Terminology Criteria for Adverse Events, version 5.0), particularly hematologic toxicity or liver function deterioration; Radiographic evidence of disease progression according to RECIST v1.1 or modified RECIST (mRECIST); Patient refusal or deterioration in ECOG performance status; Physician assessment that further HAIC may pose undue risk or limited additional benefit.
Donafenib (Zelgen Biopharmaceuticals Co., Ltd., Suzhou, Jiangsu, China): Starting from the first day after the first FOLFOX-HAIC, take 0.2g orally twice a day (1 hour before meals or more than 2 hours after meals), with an interval of approximately 12 hours between the two doses. Continuous medication is required, and the medication should be suspended during the HAIC treatment period. If the subject experiences grade 3 or higher adverse events related to the trial drug during the treatment period, short-term suspension of the drug or dose adjustment is allowed. Camrelizumab (Jiangsu Hengrui Pharmaceuticals Co., Ltd., Lianyungang, Jiangsu, China): Starting from the first day after each FOLOFX-HAIC, intravenous infusion of 200mg once every three weeks. If severe treatment-related adverse reactions occur, the immunotherapy plan can be appropriately adjusted after discussion by the liver cancer MDT expert group (For specific drug treatment management, please refer to the please refer to the Treatment Management section of the supplementary materials). Antiviral treatment: All patients with positive hepatitis B surface antigen (HBsAg) need to receive antiviral treatment, using entecavir 0.5mg once a day (qd) or tenofovir 300mg QD. For patients with hepatitis C, use sofosbuvir 400mg and velpatasvir 100mg QD for antiviral treatment.
Surgery and subsequent treatment: After combined treatment, if the patient’s condition is assessed by the MDT team to meet the following conditions, it is considered that the conversion treatment is successful and the patient has the opportunity for surgical intervention:12–14 tumor assessment is PR or SD, extrahepatic lesions and vascular tumor thrombus are technically resectable (PVTT resolves to the primary or secondary branches in the main trunk, or is completely inactivated); the residual liver volume is sufficient (40% of the standard liver volume in patients with cirrhosis and 30% of the standard liver volume in non-cirrhosis patients); R0 resection can be achieved; liver function is stable or improved (liver function Child-Pugh Class A or B; Indocyanine Green Retention Rate at 15 Minutes < 20%); no serious or persistent adverse reactions occurred with FOLFOX-HAIC, donafenib, and camrelizumab (Donafenib should be stopped at least one week before surgery); The patient has no contraindications for hepatectomy. The decision on whether to proceed with surgery will be made jointly by the patient and their family. For patients who choose not to undergo surgical treatment, they will continue to receive maintenance therapy with donafenib and camrelizumab, and receive local radiotherapy as needed. They will return to the hospital for re-examination and tumor assessment every two months. For patients who choose surgical treatment, they will continue to receive adjuvant therapy with donafenib and camrelizumab after surgery for a period of 6 to 12 months. The specific time to discontinue the medication will be determined by the MDT. They will also return to the hospital for re-examination every two to three months and have their tumor recurrence evaluated. For patients with tumor recurrence, subsequent treatment plans will be formulated based on the specific recurrence situation.
Data Collection and Follow-Up
Based on the medical records, the baseline characteristics, laboratory indicators and imaging examination results of the patients before and after treatment were collected, including age, gender, ECOG performance status score, alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin (TBIL), albumin (ALB), international normalized ratio (INR), Child-Pugh classification of liver function, hepatitis B virus infection status, whether combined with liver cirrhosis, the longest diameter of tumor lesions, alpha-fetoprotein (AFP), major vascular invasion and/or extrahepatic metastasis, Chinese Liver Cancer (CNLC) staging, Barcelona Clinic Liver Cancer (BCLC) staging, tumor response and treatment-related adverse events. The survival status and subsequent treatment of the patients after discharge were followed up by telephone.
Assessment and Outcomes
During treatment, patients underwent imaging assessments after every two cycles of HAIC. After completion of HAIC, imaging and clinical follow-up were conducted every 2 to 3 months. Tumor evaluation routinely included both contrast-enhanced CT and magnetic resonance imaging (MRI) to offer complementary anatomical and functional information. To ensure consistency, the same imaging modality combination was maintained throughout follow-up for each patient. In cases where MRI was contraindicated (eg, due to metallic implants), contrast-enhanced CT was used as the sole imaging modality. Tumor response was independently evaluated by two radiologists, each with more than 5 years of experience in hepatobiliary imaging. Discrepancies were resolved through consultation with a third senior radiologist, and final evaluations were reached by consensus to minimize inter-observer variability. If distant metastasis was suspected, additional examinations such as chest CT, whole-body bone scan, or positron emission tomography–CT (PET-CT) were selectively performed. Final treatment decisions were made by the MDT based on comprehensive radiologic and clinical evaluation.
The primary endpoint of the study was the ORR, and the secondary endpoints included disease control rate (DCR), OS, PFS, duration of response (DOR), 6-month and 12-month PFS rates, 6-month, 12-month, and 24-month OS rates, conversion resection rate, and the incidence of treatment-related adverse events. Tumor responses were evaluated according to the mRECIST and RECIST v1.1. ORR was defined as the proportion of patients achieving complete response (CR) or partial response (PR), while DCR included patients with CR, PR, and stable disease (SD). OS was the time from the initiation of HAIC treatment to death due to any cause, and PFS was the time interval from the initiation of HAIC treatment to disease progression or death (whichever occurred first). For patients lost to follow-up, survival data were right-censored, with the last effective follow-up date as the censoring time. Their survival status was treated as a censored event in subsequent survival analyses.
Adverse events were recorded according to the CTCAE 5.0, including the occurrence and end time of adverse events, severity, correlation with treatment, and final outcome.
Statistical Analysis
Continuous variables with non-normal distribution were expressed as median (interquartile range), and those with normal distribution were expressed as mean (standard deviation). Categorical variables were presented as frequency and percentage. ORR and DCR and their 95% confidence intervals (CI) were calculated using the Clopper-Pearson method. Chi-square test or Fisher’s exact test was used for the analysis of categorical variables. Survival analysis was performed using the Kaplan-Meier method to calculate survival curves and estimate median survival time and its 95% CI. Univariate and multivariate Cox proportional hazards regression models were used to evaluate the factors influencing PFS and OS (After univariate analysis, factors with p < 0.05 and those clinically deemed closely related to prognosis were included in a multivariate Cox proportional hazards model for further evaluation). Statistical analysis and graph plotting were conducted using R software (version 4.4.1) and GraphPad Prism software (version 10.1.2). All statistical tests were two-sided, and P values < 0.05 were considered statistically significant.
Results
Characteristics
Forty-nine eligible patients were enrolled in this prospective study between November 2021 and November 2024 (Baseline demographic and clinical characteristics are summarized in Table 1). The follow-up was concluded on November 30, 2024 (The patient enrollment and follow-up procedures are depicted in Figure 1). The mean age of all patients was 55.9 years (standard deviation: 10.8). Among them, 41 were male (83.7%) and 8 were female (16.3%). During the study period, all patients received a total of 214 cycles of FOLFOX-HAIC treatment, with a median of 5 cycles (range: 1–6). Additionally, 44 patients (89.8%) were hepatitis B patients and 3 patients (6.1%) were hepatitis C patients. According to the Child-Pugh score, 85.7% of the patients were classified as grade A and 14.3% as grade B. The average diameter of measurable target lesions at baseline was 9.9 cm (standard deviation: 4.1). Vascular invasion was present in 36 patients (73.5%), and 25 patients (51.0%) had extrahepatic metastasis.
 |
Table 1 Baseline Characteristics of Patients |
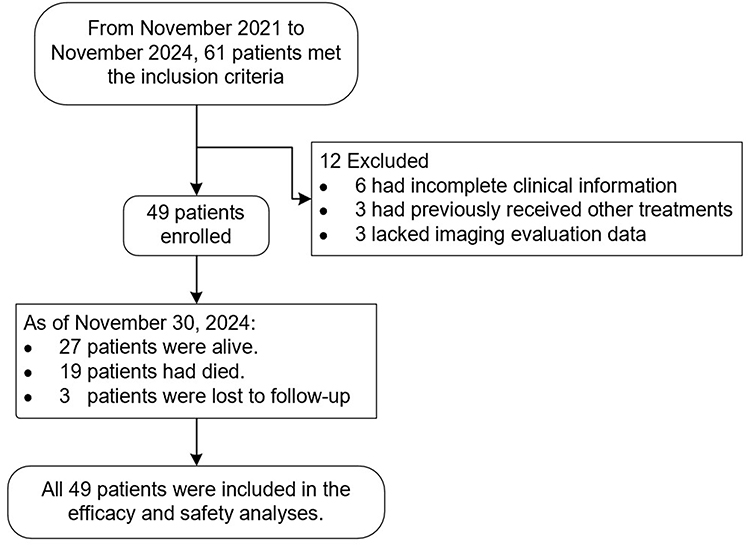 |
Figure 1 Study Flowchart. |
Tumor Response and Survival Outcome
As of November 2024, the median follow-up time was 20.3 months (95% CI: 15.5–25.1). At the final follow-up, 27 patients (55.1%) remained alive, 19 (38.8%) died, and 3 (6.1%) were lost to follow-up. The overall best tumor response (Figure 2a, b, and Table 2) was evaluated according to RECIST v1.1 criteria, showing 1 CR, 27 PRs, 11 SDs, and 10 Progressive diseases (PDs), with an ORR of 57.1% (95% CI: 42.2–71.2) and a DCR of 79.6% (95% CI: 65.7–89.8). According to mRECIST criteria, there were 7 CRs, 22 PRs, 10 SDs, and 10 PDs, with an ORR of 59.2% (95% CI: 44.2–73.0) and a DCR of 79.6% (95% CI: 65.7–89.8). Longitudinal changes in tumor diameter over time are illustrated in Figure S1. In addition, the median time to response (TTR) in this study was 2.0 months (range: 1.4–9.9); the median DOR was 22.2 months (95% CI: 13.6–30.8); and the median time to progression (TTP) was 13.1 months (95% CI: 11.7–14.5).
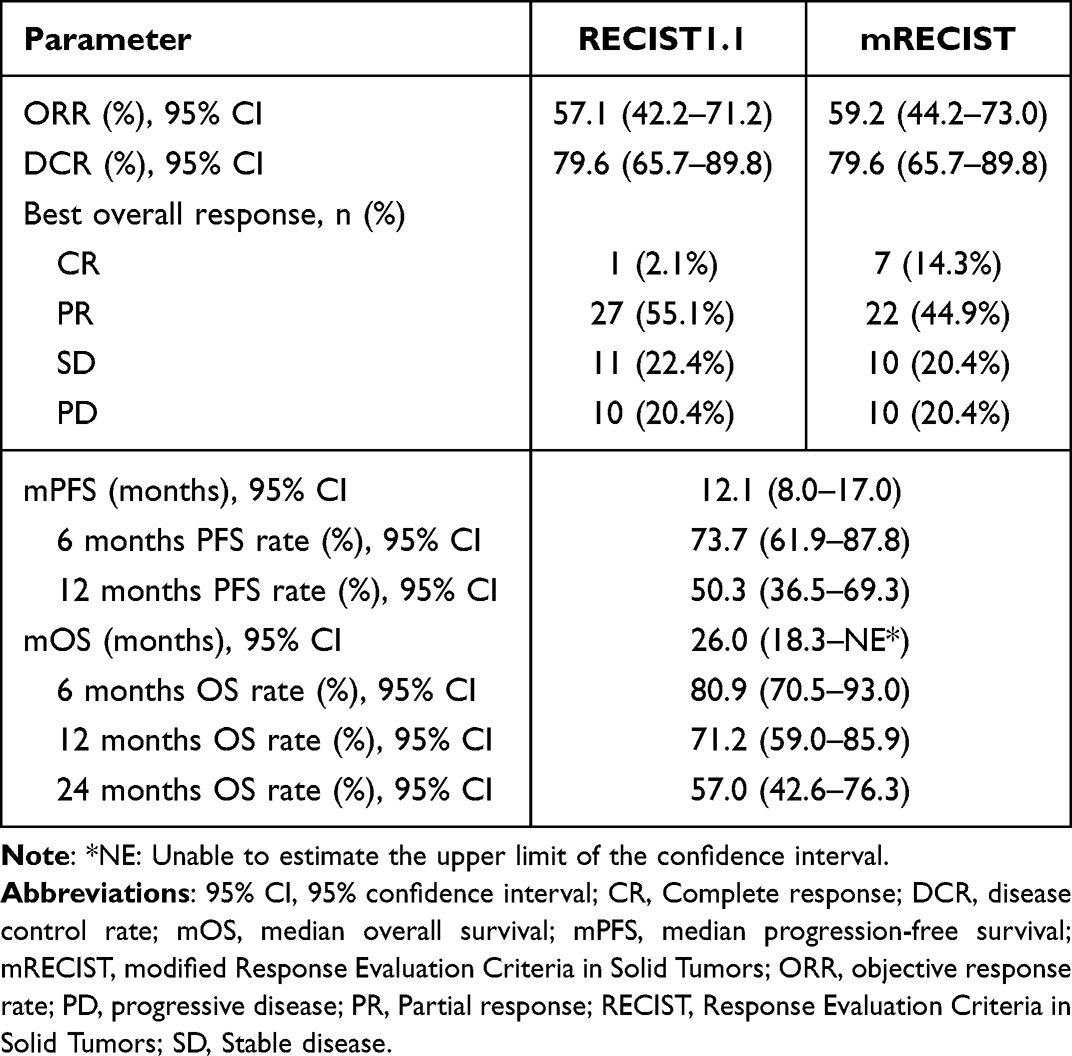 |
Table 2 Tumor Response and Survival |
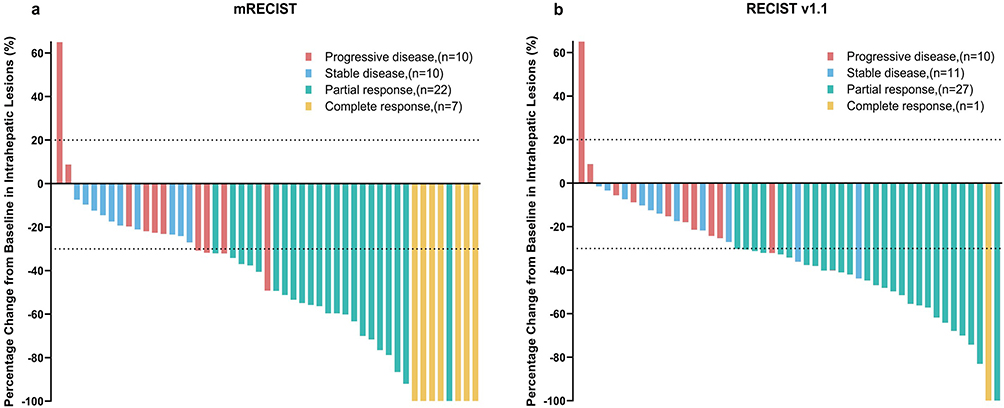 |
Figure 2 Waterfall plot of the best response of tumors. (a) The best percentage changes from baseline in target lesions per RECIST v1.1; (b) The best percentage changes from baseline in target lesions per mRECIST. Each bar represents an individual patient, and bars are color-coded according to best radiologic response: red indicates progressive disease (PD), blue indicates stable disease (SD), green indicates partial response (PR), and yellow indicates complete response (CR). |
The median PFS was 12.1 months (95% CI: 8.0–17.0), and the median OS was 26.0 months (95% CI: 18.3 - Not Estimable) (Figure 3a and b). The PFS rates at 6 and 12 months were 73.7% (95% CI: 61.9–87.8) and 50.3% (95% CI: 36.5–69.3), respectively; the survival rates at 6, 12, and 24 months were 80.9% (95% CI: 70.5–93.0), 71.2% (95% CI: 59.0–85.9), and 57.0% (95% CI: 42.6–76.3), respectively (Table 2). Additionally, we drew a survival swimmer plot to show the different survival statuses, treatment responses, surgeries, and recurrences of each patient during the clinical study (Figure 3c).
 |
Figure 3 Survival Outcomes. (a) Kaplan-Meier curves of Progression-Free Survival, (b) Kaplan-Meier curves of Overall Survival, (c) Waterfall Plot of Patient Survival Outcomes and Treatment Responses. Each horizontal bar represents one patient; Orange indicates progression-free survival, red indicates recurrence-free survival, green indicates post-progression survival, blue indicates post-recurrence survival, and gray indicates survival during the follow-up period without recurrence or progression. Symbols represent clinical events as follows: ▯, progressive disease (PD); ●, stable disease (SD); ▼, partial response (PR); ▲, complete response (CR); ♦, tumor recurrence, ◆, R0 surgical resection; |, change of molecular targeted therapy; →, ongoing follow-up; ⇥, lost to follow-up; and ✖ death. All colors and symbols are also indicated in the figure legend panel for reference. Abbreviations: NE, Not Estimable, Not Estimable due to censoring; mPFS, median Progression-Free Survival; mOS, median Overall Survival. |
Surgical Conversion
A total of 12 patients (24.49%) achieved successful conversion in this study. Among them, 5 patients (10.2%) underwent partial hepatectomy after conversion, and all achieved R0 resection. Of the 5 resected patients, 2 (5.7%) achieved pathological complete response (pCR), while 2 others exhibited <30% residual tumor cells in the tumor bed, fulfilling the criteria for major pathological response (MPR).
To illustrate the post-surgical course, a swimmer plot (Figure 4a) was used to depict individual treatment timelines and the administration of adjuvant systemic therapy. All five patients received maintenance therapy with donafenib and camrelizumab following surgery. During adjuvant treatment, two patients experienced grade 3 adverse events—hepatic encephalopathy and peptic ulcer, respectively. These events were effectively managed through temporary treatment interruption and dose adjustment, with subsequent symptom resolution.
 |
Figure 4 Survival Outcomes in Patients Undergoing Conversion Therapy.(a) Swimmer plot of patients who underwent R0 surgical resection after successful conversion; (b) Kaplan–Meier curves comparing overall survival between patients with and without successful conversion. Each horizontal bar represents one patient; Orange indicates progression-free survival; green indicates adjuvant systemic therapy; light green indicates follow-up period; blue indicates post-recurrence survival. Clinical events are marked by symbols: ◆, R0 surgical resection; ♦, tumor recurrence; ✖, death; →, keeping follow-up; ●, stable disease (SD); and ▼, partial response (PR). Patients who underwent successful conversion (n = 12) had a significantly longer OS than those without (n = 37), with median OS not reached versus 18.3 months, respectively (log-rank P = 0.012). Abbreviations: NE, Not Estimable, Not Estimable due to censoring; mOS, median Overall Survival. |
Regarding recurrence patterns, three patients remained recurrence-free at the final follow-up. One patient developed solitary intrahepatic recurrence 11 months after surgery. Although the disease was initially controlled with local interventional therapy and second-line systemic treatment, subsequent disease progression led to major vascular invasion. The patient ultimately died due to liver function deterioration 9.2 months after recurrence. Another patient experienced intrahepatic recurrence at 23.2 months postoperatively and achieved stable disease following additional treatment.
The remaining 7 patients were deemed eligible for resection following successful conversion but declined surgery or radiotherapy due to personal preferences. Nevertheless, they all maintained good adherence to donafenib and camrelizumab maintenance therapy.
Notably, patients in the conversion group demonstrated significantly longer median overall survival than those in the non-conversion group (not reached vs 18.3 months, P < 0.01) (Figure 4b).
Safety
All 49 patients were included in the safety analysis (Table 3). All patients (100%) experienced treatment-related adverse event (TRAE). The most common TRAEs of any grade were hypoalbuminemia in 29 cases (87.8%), Hand-foot skin reaction (HFSR) in 28 cases (79.6%), thrombocytopenia in 27 cases (73.5%), abdominal pain in 26 cases (73.5%), and elevated aspartate aminotransferase in 24 cases (71.4%). Thirty patients (61.2%) experienced grade 3 or 4 TRAEs. The most common grade 3 or higher adverse events were thrombocytopenia in 13 cases (26.5%), elevated aspartate aminotransferase in 11 cases (22.5%), HFSR in 9 cases (18.4%), and elevated bilirubin in 6 cases (12.2%). Three patients experienced grade 4 treatment-related thrombocytopenia, and the indicators were all reduced to below grade 3levels after platelet production promotion and platelet apheresis transfusion. One patient died due to liver failure and persistent elevated bilirubin caused by the accumulation of chemotherapy drug toxicity.
 |
Table 3 Treatment-Related Adverse Events |
Thirty patients (61.2%) experienced immune-related adverse events (irAEs) of varying grades. The most common irAEs included proteinuria in 8 cases (16.3%), thyroid dysfunction in 16 cases (32.7%), reactive cutaneous capillary endothelial proliferation (RCCEP) in 15 cases (30.6%), abnormal myocardial enzymes in 12 cases (24.5%), and cetuximab allergy in 3 cases (6.1%). All patients with RCCEP and proteinuria were mild cases and did not require special treatment. Among the patients with thyroid dysfunction, only 3 cases required oral levothyroxine treatment. All patients with abnormal myocardial enzymes only showed a mild increase in troponin T, and there were no other clinical symptoms or diagnostic basis for immune myocarditis.
Subgroup Analysis
Subgroup analysis of ORR, as illustrated by the forest plots in Figure S2, revealed that according to mRECIST, patients receiving HAIC for ≥4 sessions had an ORR of 78.8% (95% CI: 61.1–91), which was significantly higher than the 18.8% (95% CI: 4.1–45.7, P < 0.01) in those receiving HAIC for <4 sessions. Furthermore, the ORR in the group without combined embolization was 73.3% (95% CI: 54.1–87.7), significantly surpassing the 36.8% (95% CI: 16.3–61.6, P = 0.03) in the group with combined embolization. According to RECIST v1.1, the ORR of patients receiving HAIC ≥4 sessions was 75.8% (95% CI: 57.7–88.9), notably higher than the 18.8% (95% CI: 4.1–45.7, P < 0.01) observed in patients receiving HAIC <4 sessions. Additionally, the ORR in the group without combined embolization was 73.3% (95% CI: 54.1–87.7), significantly better than the 31.6% (95% CI: 12.6–56.6, P = 0.01) in the group with combined embolization.
In the subgroup analysis of PFS, as presented in Table S1, univariate Cox regression identified tumor number (HR: 3.71; 95% CI: 1.38–9.99; P = 0.009), maximum tumor diameter (HR: 2.50; 95% CI: 1.16–5.42; P = 0.020), and presence of metastasis (HR: 2.52; 95% CI: 1.16–5.47; P = 0.020) as significant predictors of PFS. However, in the multivariate Cox regression model, after adjusting for potential confounders, only having multiple tumors remained statistically significant (HR: 2.99; 95% CI: 1.10–8.12; P = 0.032), indicating it as an independent risk factor for shorter PFS.
For OS, as shown in Table S2, univariate analysis revealed that metastasis (HR: 3.95; 95% CI: 1.40–11.18; P = 0.010) and hepatitis status (HR: 0.15; 95% CI: 0.03–0.69; P = 0.015) were significantly associated with OS. After multivariate adjustment, only metastasis remained an independent risk factor for poorer OS (HR: 3.60; 95% CI: 1.24–10.45; P = 0.019).
Discussion
The prognosis for patients with advanced uHCC is generally poor. The current first-line standard treatments for advanced HCC, such as atezolizumab plus bevacizumab, lenvatinib, and durvalumab plus ipilimumab, have demonstrated significant survival benefits in their respective phase III clinical trials (IMbrave150, REFLECT, HIMALAYA), with ORR reaching 30%, 24.1%, and 20.1%, respectively, and median OS of 19.2 months, 13.6 months, and 16.4 months, respectively.4,15,16 This has established a new benchmark for the treatment of uHCC. Targeted therapy may develop resistance due to the genomic instability of tumors when used for a long time, and the efficacy of immunotherapy is significantly heterogeneous due to the presence of immunosuppressive factors in the tumor microenvironment.8,17 These issues make it difficult to further meet the clinical needs of patients with uHCC by relying solely on systemic therapy, highlighting the potential value of combined local and systemic therapy. In recent years, combined regimens of local and systemic therapy have shown more significant efficacy and survival benefits compared to single-agent therapy. Real-world studies have shown that in patients with unresectable HCC, the treatment regimen of HIAC combined with lenvatinib and toripalimab has an ORR of 66.7% and a median PFS of 10.4 months.18 The combination of SBRT with apatinib and camrelizumab has an ORR of 69.4% and a DCR of 72.5%, with a median PFS of 4.6 months.19 30 Additionally, the treatment regimen of TACE combined with lenvatinib and envafolimab for uHCC patients has also shown good efficacy, with an ORR of 50%, a DCR of 83.3%, and a median PFS of 7.58 months.20 A large number of such research results indicate that combined regimens of local and systemic therapy have obvious advantages in improving the survival and response rates of patients with advanced HCC.21
In this study, the enrolled patients exhibited a substantial tumor burden. Among the 49 patients, 44 (89.8%) presented with portal vein tumor thrombus or extrahepatic metastasis, among which 26 (53.1%) had portal vein tumor thrombus at stage Vp3 or above (with 3 patients having tumor thrombus in the hepatic vein system). Nevertheless, the ORR of the combination of FOLFOX-HAIC, donafenib, and camrelizumab in this study was 59.2%, the DCR was 79.6%, and the median PFS was 12.1 months, while the median OS was 26.0 months. Preliminary data analysis suggests that the observed outcomes appear favorable when compared to historical results of current first-line therapies, including atezolizumab plus bevacizumab, lenvatinib, and durvalumab plus tremelimumab. Notably, this study demonstrated a relatively lower ORR compared to some trials involving locoregional and systemic therapies, while OS was notably prolonged. This discrepancy may be related to the high baseline tumor burden in our cohort, as 89.8% of patients had portal vein tumor thrombus or extrahepatic metastases. These features likely limited the radiological response, although the DCR remained high at 79.6%. In addition, deep responses in key anatomical regions, especially the regression of macrovascular invasion, enabled successful conversion therapy in 24.5% of patients. Those who underwent surgery after conversion achieved notably longer OS. The MDT ensured standardized surveillance and facilitated early detection of disease progression. This allowed for timely initiation of personalized second-line therapies such as kinase inhibitors and locoregional interventions, thereby extending the therapeutic benefit. Moreover, the biological synergy of the triple combination regimen may have contributed to meaningful treatment effects beyond conventional radiographic assessments, including tumor thrombus regression and modulation of the tumor immune microenvironment. These effects were reflected in the median PFS of 12.1 months.
We posit that the higher effectiveness demonstrated in this study in terms of tumor response and survival benefit might be attributed to the local highly efficient action of hepatic artery infusion chemotherapy and the potential synergistic effect among donafenib and immune checkpoint inhibitors. FOLFOX-HAIC intensifies the direct cytotoxic effect on tumors by elevating the local drug concentration in the liver, facilitating tumor antigen exposure and providing a more favorable basis for systemic treatment.8,22 Donafenib, a novel oral multi-kinase inhibitor, not only suppresses tumor angiogenesis and promotes vascular normalization but also modulates the tumor immune microenvironment to augment immune responses.23 Specifically, by inhibiting VEGFR, donafenib reduces the infiltration of immunosuppressive cells such as regulatory T cells (Tregs) and myeloid-derived suppressor cells (MDSCs), thus reversing the immune-tolerant state.24 It also enhances dendritic cell (DC) maturation and antigen-presenting capacity and promotes CD8+ T cell trafficking and infiltration into tumor tissues through upregulation of adhesion molecules.25 Similar to other VEGF-targeting agents such as lenvatinib, donafenib may also enhance the efficacy of ICIs by downregulating T-cell exhaustion markers (eg, PD-1, TIM-3) and increasing immunostimulatory cytokine production.26 Finally, camrelizumab blocks the PD-1/PD-L1 signaling pathway, thereby restoring T cell function and reactivating antitumor immune responses.27 The combination of the three exerts a synergistic effect in suppressing tumor proliferation, ameliorating the immune microenvironment and enhancing the local anti-tumor effect, which constitutes a crucial reason for the remarkable improvement in the efficacy of the combined treatment.
Based on the significant efficacy of the combined treatment, the tumor burden was effectively reduced, the vascular tumor thrombus exhibited marked regression, and the volume of the residual liver increased, providing more opportunities for conversion surgery for uHCC patients. In comparison with the conversion rates (typically ranging from 12% to 34.5%) reported in previous clinical trials of various combined conversion treatments for uHCC,28–32 this study also achieved comparable results, with 12 patients (24.5%) successfully achieving conversion and obtaining surgical treatment opportunities. Furthermore, the median OS of patients who successfully converted was not reached, significantly longer than that of those who did not (P < 0.01). Evidently, successful conversion can confer substantial survival benefits to uHCC patients.
Through subgroup analysis, patients who received ≥ 4 HAIC treatments had a significantly higher ORR than those who received < 4 treatments, and the ORR in the non-embolization group was significantly higher than that in the embolization group. These findings suggest that increasing the number of HAIC treatments may enhance the therapeutic effect through more sustained drug delivery, while the combination of embolization may reduce the treatment response due to excessive blockade of blood flow. However, the functional status of organs and the tumor burden often restrict the number of treatments and doses. Furthermore, we examined the influence of multiple baseline characteristics and treatment-related factors on PFS and OS. In the univariate Cox regression analysis of PFS, tumor number, maximum tumor diameter, and presence of distant metastasis were significantly associated with PFS (P < 0.05). However, in the multivariate model, only tumor number remained an independent prognostic factor (HR: 2.99; 95% CI: 1.10–8.12; P = 0.032), suggesting that multiple tumors are a key determinant of disease progression after adjusting for other variables. This finding supports the consideration of more aggressive treatment strategies for patients with multifocal disease, such as combining HAIC with TACE.9 For OS, hepatitis status and distant metastasis were significant in univariate analysis, but only distant metastasis retained statistical significance in the multivariate model (HR: 3.60; 95% CI: 1.24–10.45; P = 0.019). As extrahepatic disease is generally less responsive to locoregional therapy, this underscores the importance of systemic treatment and vigilant monitoring in patients with metastases. Early identification of progression and prompt therapeutic adjustment are critical to improving long-term outcomes.
In terms of adverse reactions, the adverse reactions observed in this study were consistent with those reported in previous studies involving donafenib, camrelizumab, and FOLFOX-HAIC treatment.3,11,33 All patients experienced varying degrees of TRAEs, and the higher incidence of adverse events was similar to that in previous clinical studies of local combined systemic therapy, which was attributed to the cumulative and synergistic toxic effects of the three treatment modalities. The most common grade 3 or higher TRAEs in this study were thrombocytopenia, elevated aspartate aminotransferase, and HFSR, which were effectively managed through dose adjustment of donafenib, delay or suspension of HAIC cycles, and symptomatic treatment. However, one patient experienced liver function deterioration due to the background of underlying liver disease and the accumulation of drug-induced liver toxicity after multiple FOLFOX-HAIC treatments. The family eventually gave up further treatment, and the patient died of liver failure. Regarding irAEs, thyroid dysfunction, telangiectasia, and abnormal myocardial enzymes were relatively common, but most patients only had abnormal laboratory indicators without corresponding clinical manifestations. These could be relieved through symptomatic treatment or discontinuation of camrelizumab. While the overall safety profile was acceptable, the findings underscore the importance of vigilant toxicity management in combination therapies, especially in advanced uHCC patients with underlying liver cirrhosis and limited hepatic reserve. In clinical settings, this necessitates close monitoring of hematologic and hepatic function, timely dose modifications or treatment delays, and proactive supportive interventions. Although biomarker-guided toxicity prediction was not applied in this study due to technical and economic constraints, future investigations incorporating such strategies may further improve the safety and individualization of treatment, especially in cirrhotic populations.
This study has several limitations. First, it was a single-center, retrospective, single-arm study with a relatively small sample size, which may result in insufficient statistical power and limit the generalizability of the findings. Second, the absence of a control group, such as monotherapy or alternative combination regimens, restricts direct efficacy comparisons and causal inferences. Third, the relatively short follow-up period restricts a comprehensive evaluation of long-term survival outcomes and cumulative adverse events. Furthermore, the patient population was primarily from Southwest China, where HBV is the predominant etiology of HCC. This contrasts with regions such as Western countries, where nonalcoholic steatohepatitis (NASH) is more common. Such geographic and etiological differences may influence tumor biology and treatment response, limiting the applicability of our findings to broader populations. Finally, biomarker analyses, including PD-L1 expression, tumor mutational burden (TMB), circulating tumor DNA (ctDNA), and quality-of-life (QoL) assessments were not conducted. Given the importance of these parameters in guiding personalized treatment and evaluating therapeutic benefit, future prospective studies incorporating molecular profiling and standardized QoL instruments are necessary to optimize treatment strategies and facilitate balanced risk–benefit assessments for patients with uHCC.
Conclusion
The combination of FOLFOX-HAIC, donafenib, and camrelizumab demonstrated promising efficacy and manageable safety in patients with uHCC. Notably, this regimen enabled tumor downstaging and successful conversion to a resectable state in a proportion of patients, thereby offering curative surgical opportunities for some individuals with advanced-stage disease. However, given the retrospective single-arm design and limited sample size, the findings should be interpreted with caution. Further large-scale, multicenter randomized controlled trials are warranted to validate these results and refine individualized treatment strategies for uHCC.
Abbreviations
CT, computed tomography; DC, dendritic cell; DOR, duration of response; HAIC, hepatic artery infusion chemotherapy; HBsAg, hepatitis B surface antigen; HCC, hepatocellular carcinoma; ICIs, immune checkpoint inhibitors; irAEs, immune-related adverse events; MDT, multidisciplinary team; MDSCs, myeloid-derived suppressor cells; MRI, magnetic resonance imaging; NASH, nonalcoholic steatohepatitis; PD-1, programmed cell death protein 1; PD-L1, programmed death-ligand 1; PET-CT, positron emission tomography–computed tomography; pCR, pathological complete response; QoL, quality of life; RECIST, Response Evaluation Criteria in Solid Tumors; SBRT, stereotactic body radiation therapy; TACE, transcatheter arterial chemoembolization; TKI, tyrosine kinase inhibitor; TIM-3, T-cell immunoglobulin and mucin-domain containing-3; TMB, tumor mutational burden; TTR, time to response; TTP, time to progression; uHCC, unresectable hepatocellular carcinoma; VEGF, vascular endothelial growth factor; VEGFR, vascular endothelial growth factor receptor.
Data Sharing Statement
The anonymized datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request, subject to institutional data sharing policies and ethical compliance.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of the First Affiliated Hospital of Chongqing Medical University (approval number: 2025-282-01). Owing to the retrospective design and the use of anonymized patient data, the requirement for informed consent was waived by the ethics committee.
Acknowledgments
We would like to express our gratitude to the MDT team of the First Affiliated Hospital of Chongqing Medical University for their comprehensive management of patients.
Author Contributions
Chenrui Wu and Zixuan Fu contributed equally to this manuscript and share first authorship. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors did not receive any financial support from any organization for the submitted work.
Disclosure
The authors declare no competing financial interests or personal relationships that could be perceived to influence the design, execution, or reporting of this study. All authors have confirmed the absence of any potential conflicts of interest.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Bi X, Lu Y, Chen B, et al. Chinese Expert Consensus on the Combination of Targeted Therapy and Immunotherapy with Locoregional Therapy for Intermediate/Advanced Hepatocellular Carcinoma. Liver Cancer. 2024:1–25. doi:10.1159/000540857
3. Qin S, Bi F, Gu S, et al. Donafenib versus sorafenib in first-line treatment of unresectable or metastatic hepatocellular carcinoma: a randomized, open-label, parallel-controlled phase II-III trial. J Clin Oncol. 2021;39(27):3002–3011. doi:10.1200/JCO.21.00163
4. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised Phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173. doi:10.1016/S0140-6736(18)30207-1
5. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–1905. doi:10.1056/NEJMoa1915745
6. Ren Z, Xu J, Bai Y, et al. Sintilimab plus a bevacizumab biosimilar (IBI305) versus sorafenib in unresectable hepatocellular carcinoma (ORIENT-32): a randomised, open-label, Phase 2-3 study. Lancet Oncol. 2021;22(7):977–990. doi:10.1016/S1470-2045(21)00252-7
7. Qin S, Chan SL, Gu S, et al. Camrelizumab plus rivoceranib versus sorafenib as first-line therapy for unresectable hepatocellular carcinoma (CARES-310): a randomised, open-label, international phase 3 study. Lancet. 2023;402(10408):1133–1146. doi:10.1016/S0140-6736(23)00961-3
8. Llovet JM, De Baere T, Kulik L, et al. Locoregional therapies in the era of molecular and immune treatments for hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2021;18(5):293–313. doi:10.1038/s41575-020-00395-0
9. Zhao M, Guo Z, Zou YH, et al. Arterial chemotherapy for hepatocellular carcinoma in China: consensus recommendations. Hepatol Int. 2024;18(1):4–31. doi:10.1007/s12072-023-10599-6
10. Keam SJ, Duggan S. Donafenib: first Approval. Drugs. 2021;81(16):1915–1920. doi:10.1007/s40265-021-01603-0
11. Qin S, Ren Z, Meng Z, et al. Camrelizumab in patients with previously treated advanced hepatocellular carcinoma: a multicentre, open-label, parallel-group, randomised, phase 2 trial. Lancet Oncol. 2020;21(4):571–580. doi:10.1016/S1470-2045(20)30011-5
12. Sun HC, Zhou J, Wang Z, et al. Chinese expert consensus on conversion therapy for hepatocellular carcinoma (2021 edition). Hepatobiliary Surg Nutr. 2022;11(2):227–252. doi:10.21037/hbsn-21-328
13. Tang H, Zhang W, Cao J, et al. Chinese expert consensus on sequential surgery following conversion therapy based on combination of immune checkpoint inhibitors and antiangiogenic targeted drugs for advanced hepatocellular carcinoma (2024 edition). Biosci Trends. 2025;18(6):505–524. doi:10.5582/bst.2024.01394
14. Zhao HT, Cai JQ. Chinese expert consensus on neoadjuvant and conversion therapies for hepatocellular carcinoma. World J Gastroenterol. 2021;27(47):8069–8080. doi:10.3748/wjg.v27.i47.8069
15. Cheng AL, Qin S, Ikeda M, et al. Updated efficacy and safety data from IMbrave150: atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J Hepatol. 2022;76(4):862–873. doi:10.1016/j.jhep.2021.11.030
16. Abou-Alfa GK, Lau G, Kudo M, et al. Tremelimumab plus durvalumab in unresectable hepatocellular carcinoma. NEJM Evidence. 2022;1(8). doi:10.1056/EVIDoa2100070
17. Petroni G, Buqué A, Coussens LM, Galluzzi L. Targeting oncogene and non-oncogene addiction to inflame the tumour microenvironment. Nat Rev Drug Discov. 2022;21(6):440–462. doi:10.1038/s41573-022-00415-5
18. Lai Z, He M, Bu X, et al. Lenvatinib, toripalimab plus hepatic arterial infusion chemotherapy in patients with high-risk advanced hepatocellular carcinoma: a biomolecular exploratory, Phase II trial. Eur J Cancer. 2022;174:68–77. doi:10.1016/j.ejca.2022.07.005
19. Hu Y, Zhou M, Tang J, et al. Efficacy and safety of stereotactic body radiotherapy combined with camrelizumab and apatinib in patients with hepatocellular carcinoma with portal vein tumor thrombus. Clin Cancer Res. 2023;29(20):4088–4097. doi:10.1158/1078-0432.CCR-22-2592
20. Chen Y, Zhang J, Hu W, et al. Envafolimab plus lenvatinib and transcatheter arterial chemoembolization for unresectable hepatocellular carcinoma: a prospective, single-arm, phase II study. Signal Transduct Target Ther. 2024;9(1):280. doi:10.1038/s41392-024-01991-1
21. Zhong BY, Fan W, Guan JJ, et al. Combination locoregional and systemic therapies in hepatocellular carcinoma. Lancet Gastroenterol Hepatol. 2025;10(4):369–386. doi:10.1016/S2468-1253(24)00247-4
22. Ding Y, Wang S, Qiu Z, et al. The worthy role of hepatic arterial infusion chemotherapy in combination with anti-programmed cell death protein 1 monoclonal antibody immunotherapy in advanced hepatocellular carcinoma. Front Immunol. 2023;14:1284937. doi:10.3389/fimmu.2023.1284937
23. Chen R, Ielasi L, Di Carlo A, Tovoli F. Donafenib in hepatocellular carcinoma. Drugs Today. 2023;59(2):83–90. doi:10.1358/dot.2023.59.2.3507751
24. Tong J, Tan Y, Ouyang W, Chang H. Targeting immune checkpoints in hepatocellular carcinoma therapy: toward combination strategies with curative potential. Exp Hematol Oncol. 2025;14(1):65. doi:10.1186/s40164-025-00636-5
25. Oura K, Morishita A, Tadokoro T, Fujita K, Tani J, Kobara H. Immune microenvironment and the effect of vascular endothelial growth factor inhibition in hepatocellular carcinoma. IJMS. 2024;25(24):13590. doi:10.3390/ijms252413590
26. Rimassa L, Finn RS, Sangro B. Combination immunotherapy for hepatocellular carcinoma. Journal of Hepatology. 2023;79(2):506–515. doi:10.1016/j.jhep.2023.03.003
27. Xu B, Sun HC. Camrelizumab: an investigational agent for hepatocellular carcinoma. Expert Opin Investig Drugs. 2022;31(4):337–346. doi:10.1080/13543784.2022.2022121
28. Chang X, Li X, Sun P, Li Z, Sun P, Ning S. HAIC combined with lenvatinib plus PD-1 versus lenvatinib Plus PD-1 in patients with high-risk advanced HCC: a real-world study. BMC Cancer. 2024;24(1):480. doi:10.1186/s12885-024-12233-6
29. Chiang CL, Chiu KWH, Chan KSK, et al. Sequential transarterial chemoembolisation and stereotactic body radiotherapy followed by immunotherapy as conversion therapy for patients with locally advanced, unresectable hepatocellular carcinoma (START-FIT): a single-arm, phase 2 trial. Lancet Gastroenterol Hepatol. 2023;8(2):169–178. doi:10.1016/S2468-1253(22)00339-9
30. Kudo M, Aoki T, Ueshima K, et al. Achievement of complete response and drug-free status by atezolizumab plus bevacizumab combined with or without curative conversion in patients with transarterial chemoembolization-unsuitable, intermediate-stage hepatocellular carcinoma: a multicenter proof-of-concept study. Liver Cancer. 2023;12(4):321–338. doi:10.1159/000529574
31. Liu W, Xie Z, Shen K, et al. Analysis of the safety and effectiveness of TACE combined with targeted immunotherapy in the treatment of intermediate and advanced hepatocellular carcinoma. Med Oncol. 2023;40(9):251. doi:10.1007/s12032-023-02082-x
32. Sun R, Gou Y, Pan L, et al. Hepatic arterial infusion chemotherapy (HAIC) combined with Tislelizumab and Lenvatinib for unresectable hepatocellular carcinoma: a retrospective single-arm study. Cell Oncol. 2024;47(6):2265–2276. doi:10.1007/s13402-024-01015-8
33. Lyu N, Wang X, Li JB, et al. Arterial chemotherapy of oxaliplatin plus fluorouracil versus sorafenib in advanced hepatocellular carcinoma: a biomolecular exploratory, randomized, phase III trial (FOHAIC-1). J Clin Oncol. 2022;40(5):468–480. doi:10.1200/JCO.21.01963
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.