")
Back to Journals » Clinical Ophthalmology » Volume 19
Efficacy and Safety of Ophthalmic Steroids in the Management of Polypoidal Choroidal Vasculopathy: A Systematic Review
Authors Adriono GA, Triyoga IF , Kadharusman MM, Victor AA , Djatikusumo A, Yudantha AR, Hutapea MM
Received 13 January 2025
Accepted for publication 10 March 2025
Published 15 March 2025 Volume 2025:19 Pages 915—931
DOI https://doi.org/10.2147/OPTH.S517296
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Gitalisa Andayani Adriono,1,2,* Ichsan Fauzi Triyoga,3,* Marcello Mikhael Kadharusman,3,* Andi Arus Victor,1 Ari Djatikusumo,1 Anggun Rama Yudantha,1 Mario Marbungaran Hutapea1
1Department of Ophthalmology, Kirana Eye Centre - Cipto Mangunkusumo National General Hospital, Jakarta, Indonesia; 2JEC Eye Hospitals and Clinics, Jakarta, Indonesia; 3Faculty of Medicine, University of Indonesia, Jakarta, Indonesia
*These authors contributed equally to this work
Correspondence: Gitalisa Andayani Adriono, Department of Ophthalmology, Kirana Eye Centre - Cipto Mangunkusumo National General Hospital, Jakarta, Indonesia, Kimia Street, Jakarta, 10320, Indonesia, Tel +62 811 131 660, Email [email protected]
Purpose: This review aims to clarify the role of ophthalmic steroids in polypoidal choroidal vasculopathy (PCV) treatment.
Methods: A systematic literature search was performed using Scopus, PubMed, MEDLINE, Cochrane, ProQuest, and manual searches. The primary outcome was changes in best-corrected visual acuity. The secondary outcomes were anatomical changes and incidence of adverse events.
Results: Of the 100 articles identified, 9 studies were included: six treatment-naive studies, two anti-VEGF resistant studies, and one involving hemorrhagic retinal detachment. Triamcinolone acetonide was administered in seven studies, and dexamethasone in two. Altogether, 194 eyes received ophthalmic steroids in the form of intravitreal solution and slow-released implant. Overall, eight out of nine studies revealed visual acuity improvement from baseline to final follow-up, although only two studies reported significant results (0.33 ± 0.29 logMAR and 0.66 ± 0.28 logMAR) to final follow-up (0.16 ± 0.27 logMAR and 0.36 ± 0.31 logMAR). Adverse events were documented in six studies, with cataracts (6/96) and ocular hypertension (10/96) being the most common. Polyp regression and pigment epithelial detachment rates demonstrated a decline ranging from 50% to 100%. The maximum reduction observed in the central foveal thickness and central retinal thickness was − 131.4 μm and − 261.7 μm, respectively.
Conclusion: Ophthalmic steroids may serve as an effective adjunctive treatment for PCV patients, irrespective of anti-VEGF resistance or hemorrhagic involvement, and may be considered as a potential monotherapy in resource-limited settings, with minimal side effects.
Keywords: polypoidal choroidal vasculopathy, ophthalmic steroids, dexamethasone, triamcinolone acetonide
Introduction
Polypoidal choroidal vasculopathy (PCV) is a vascular disease of the choroid characterized by serosanguineous retinal pigment epithelial detachment. In the natural progression of PCV, approximately 50% of the patients experienced ongoing leakage or recurrent bleeding, thus leading to poor visual outcomes and potentially irreversible vision loss.1 Sho et al reported that 35% of eyes with idiopathic polypoidal choroidal vasculopathy (IPCV) suffered severe visual loss.2 Previous studies have identified a higher prevalence of PCV among the Asian population compared to the Caucasian, at 61.6% and 8.7%, respectively.3,4 This growing prevalence, particularly in Asia, has contributed to the increasing global attention on PCV.5
Despite its morbidity, there is no clear consensus regarding the best practice for managing PCV in clinical practice. Several treatment options have been recommended for PCV, including thermal laser photocoagulation, photodynamic therapy (PDT) with verteporfin, anti-VEGF monotherapy, and combination therapy.6–8 However, most recent potent anti-VEGFs (eg Aflibercept and Faricimab) and PDT are not widely available in several countries, thus pushing ophthalmologists to seek out easily accessed therapeutic agents for management. Steroids are highly accessible, and their use in PCV, specifically triamcinolone acetonide and dexamethasone, has been reported to generate promising visual outcomes.
Despite the positive results, the role of steroids in PCV remains unclear. Several studies have reported that inflammation contributes to the pathogenesis of PCV.9–12 Through an animal model and human specimen, Kumar et al discovered immune complex deposition, complement activation, and elevated infiltration of inflammatory cells in severe PCV, thus suggesting that inflammation plays a crucial role in the progression of PCV.9 Several studies have also identified elevated levels of the systemic inflammatory marker C-reactive protein (CRP) in PCV patients, which has been significantly associated with an increased risk of developing the disease.10,11
Moreover, anti-inflammatory glucocorticoids were effective in slowing the progression of PCV as they prevented the formation of large lesions in the mouse model.9 This approach is based on findings that suggest an inflammatory process in PCV. With promising benefits, several observational studies have reported the use of ophthalmic steroids for PCV patients. However, the role of local steroids in PCV remains uncertain, with no guidelines recommending its use. Here, we conducted a systematic review to clarify the role of ophthalmic steroids in managing PCV in terms of improvement in BCVA, anatomical changes, and safety.
Methods
Protocol and Registration
An a priori protocol was established and registered to PROSPERO (CRD42024560587). Afterward, systematic review was conducted according to the Cochrane Handbook for Systematic Reviews of Interventions and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Eligibility Criteria
The criteria for including evidence were as follows: (1) original research papers (randomized controlled trials [RCTs] and nonrandomized controlled trials [NRCTs]) or observational studies; (2) studies involving patients with active PCV; (3) use of an intervention regimen that includes local steroid injections; and (4) outcomes measured include changes in visual acuity, anatomical changes, and safety or adverse events. The primary outcome of interest is changes in visual acuity, as this reflects the patient’s visual function. Secondary outcomes include the incidence of adverse events and anatomical changes. Exclusion criteria were (1) animal studies, (2) review articles, and (3) studies not published in English.
Search Methods
Relevant studies were identified through a search of databases including MEDLINE, PubMed, Scopus, Cochrane, ProQuest, and manual searches, using Medical Subject Headings (MeSH) and keywords without any date restrictions. The keywords used included “polypoidal choroidal vasculopathy”, “steroid injections”, “triamcinolone”, “dexamethasone”, “visual acuity”, “adverse effect”, “optical coherence tomography”, “fluorescein angiography”, and “indocyanine green angiography”. Institutional Review Board approval was not required as this study is a systematic review. The study followed the principles outlined in the Declaration of Helsinki.
Study Selection and Data Collection
Two independent reviewers (IT, MK) conducted all the assessments (selection based on the title or abstract, full-text screening, data collection, and risk of bias assessment). Any disagreement between the reviewers was resolved through discussion between them. After removing duplicates, irrelevant studies were excluded by screening titles and abstracts. Studies that were selected by both reviewers were then retrieved and subjected to a full-text screen.
We then independently identified and extracted relevant information:
- Study design, year, duration, and follow-up time.
- Study population: population characteristics, type of PCV.
- Treatment methods: monotherapy, double therapy, or triple therapy.
- Outcomes: final best-corrected visual acuity (BCVA), the incidence of adverse events, rate of polyp regression, changes in central retinal thickness (CRT) and central foveal thickness (CFT), and the proportion of patients with improved pigment epithelial detachment (PED). For continuous outcomes, the mean and standard deviation (SD) were extracted. For binary outcomes, the total number of participants and the number of events were documented.
- Statistical analysis: p-value.
Assessment of Methodological Quality
The two reviewers assessed the risk of bias for single-arm studies using the 12-item Quality Assessment Tool for Before-After (Pre-Post) Studies with No Control Group from the National Institutes of Health (NIH).13 Meanwhile, for cohort studies, Newcastle-Ottawa Scale (NOS) was used to assess the risk of bias.14 Any disagreements were resolved through discussion. The level of bias was taken into account when synthesizing the data.
Data Synthesis and Analysis
Covidence systematic review software (Veritas Health Innovation, Australia) was utilized to import references from each database, handle duplicate removal, and conduct the screening process. Due to the clinical and methodological differences among the studies, a meta-analysis was not performed.
Results
Study Selection
A literature search from electronic databases identified 100 potential papers. After removing 41 duplicates, 59 articles underwent title and abstract screening. Additional 44 articles were excluded for not meeting the inclusion and exclusion criteria. Full-text screening eliminated 6 articles, leaving 9 papers for synthesis and analysis (Figure 1).
 |
Figure 1 Summary flowchart of search results and study selection. |
Study Characteristics
Out of the 9 studies that met the inclusion criteria, only 2 were prospective cohorts, and 4 were comparative. Four studies included treatment-naive patients, while two studies assessed anti-VEGF-resistant patients, another two evaluated patients with subretinal/macular hemorrhage or serous neurosensory detachment, and one study recruited patients with pre-existing cerebrovascular or cardiovascular ischemia. A total of 188 patients (194 eyes) were analyzed, 140 participants (74.5%) were males and 48 (25.5%) were females. The intervention was mostly done with a triple therapy regimen (four studies), consisting of ophthalmic steroids, anti-VEGF ophthalmic injection, and photodynamic therapy with verteporfin. Lens status and baseline intraocular pressure (IOP) were only recorded in three studies with mixed baseline results.15–23 Details of general study characteristics and baseline measurements can be seen in Table 1.
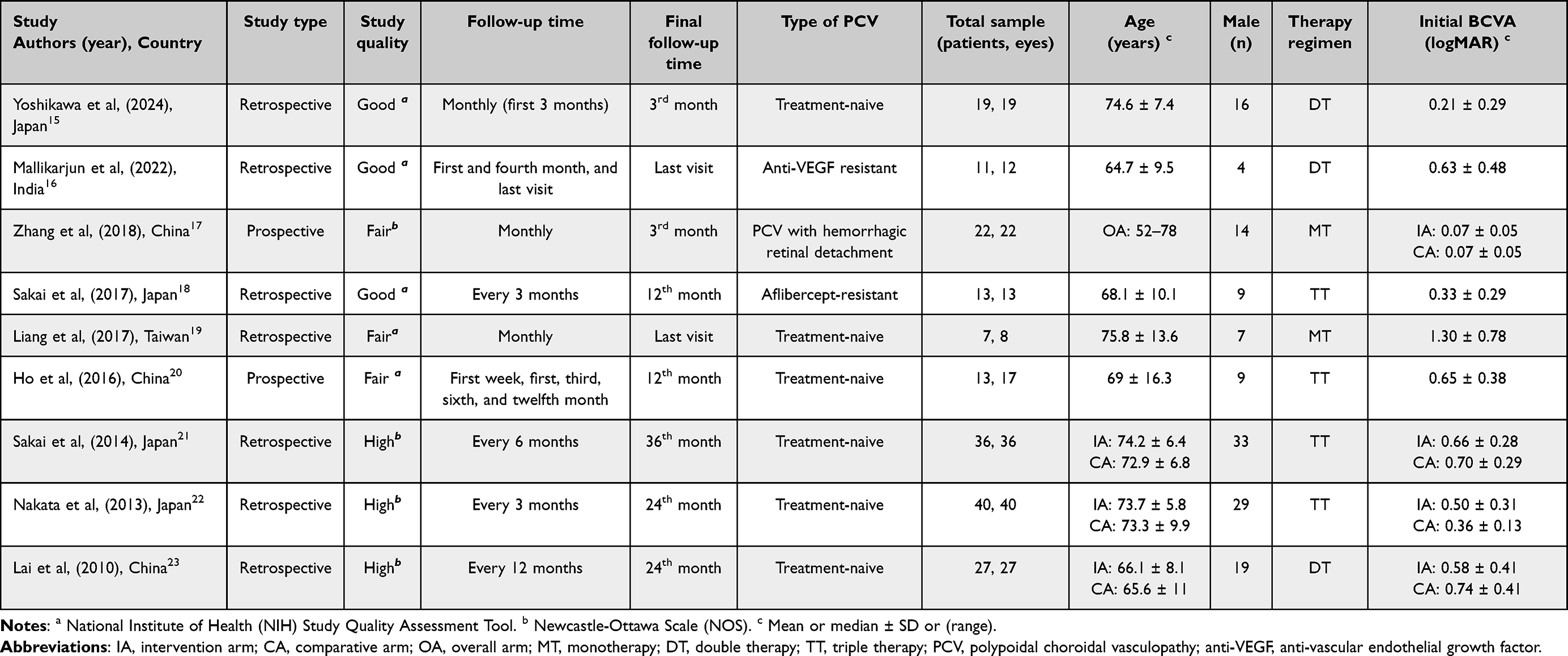 |
Table 1 Demographic and Baseline Characteristics of Included Studies |
Single-Arm Studies
A total of 5 single-arm studies were evaluated. Monotherapy was employed in one study, whereas double and triple therapy regimens were applied in two studies each. Three studies utilized triamcinolone acetonide (TA), administered as an intravitreal (IV) or subtenon (ST) injection. Intravitreal triamcinolone acetonide (IVTA) was dosed at 1 milligram (mg), while subtenon triamcinolone acetonide (STTA) was set at 20mg. Intravitreal dexamethasone was used in two cohorts, one of which was done with an implant. Dexamethasone IV implant (DII) dosage was set at 0.7 mg, whereas the suspension version was at 600 micrograms (ug). All studies employed a pro re nata (PRN) regimen. Additional therapies include different kinds of anti-VEGF injections, dosed according to the chosen anti-VEGF agent (0.5–2 mg), and PDT (50 J/cm2 or 600 mW/cm2 for 83 seconds) with verteporfin (6 mg/m2).15,16,18–20 Details can be seen in Table 2.
 |
Table 2 Characteristics of Single-Arm Cohort Studies |
Double-Arm Studies
Triamcinolone acetonide was the steroid agent utilized in all studies, albeit with different routes of administration. Periocular TA (POTA) was given as a single therapy at 1 mg once a month for the first 3 months, while IVTA and STTA were given in combination with other therapies at 600 ug, 2 mg, and 4 mg. Double therapy was given with a PDT (50 J/cm2 or 600 mW/cm2 for 83 seconds) with verteporfin (6 mg/m2). Triple therapy added a bevacizumab intravitreal injection (IVB) dosed at 2 mg. Two studies utilized PDT monotherapy for the comparator group, while the rest either used an anti-VEGF monotherapy or a double therapy of anti-VEGF and PDT. All studies, except for Zhang et al (2018), employed a pro re nata (PRN) treatment principle for their intervention and comparator groups.17,21–23 Details are in Table 3.
 |
Table 3 Characteristics of Double-Arm Cohort Studies |
Study Quality Assessments
The NIH “Before-After Studies with No Control Group” study quality assessment was used to assess single-arm studies, and a summary of quality assessment is presented in Table 4. Three of the five studies were of high-quality studies, while two others posed some risks of bias, mainly due to lack of reports on the blinding of assessors, sample size formula, and unreported statistical test values.15,16,18–20
 |
Table 4 Summary of National Institute of Health – Before–After Studies With No Control Group Scores for Single-Arm Studies |
Four cohorts were evaluated using the NOS scoring tool, where a summary is presented in Table 5. Three studies were of high quality, whereas one study received a moderate score (6) due to the lack of control over important variables during analysis and insufficient length of follow-up.17,21–23
 |
Table 5 Summary of Newcastle-Ottawa Scores for Double-Arm Studies |
GRADE Assessment
GRADE evaluations found moderate and low rating outcomes. Most outcomes started with a low rating due to the observational design of included studies. Several outcomes were upgraded due to larger effect sizes. Summary of GRADE evaluations and rationale is presented in Table 6.
 |
Table 6 Summary of Findings From Grading of Recommendations, Assessment, Development and Evaluation (GRADE) Evaluation |
Final BCVA
All studies reported baseline BCVA results, predominantly under 1.00 logMAR except for Liang et al (2017), which started with a mean BCVA of 1.30 (0.76, 1.84).15–23
Within the non-comparative study pool, Mallikarjun et al (2022) and Liang et al (2017) reported mean final BCVA at last visit, with a range of last-follow up time at 6.6–41.6 months and 9–35 months, respectively. All studies, except Mallikarjun et al (2022), reported final BCVA improvement, although the significance of final BCVA result was only seen in the triple therapy study by Sakai et al (2017).15,16,18–20 Details from single-arm studies’ conclusions on the intervention’s efficacy to BCVA are presented in Table 7.
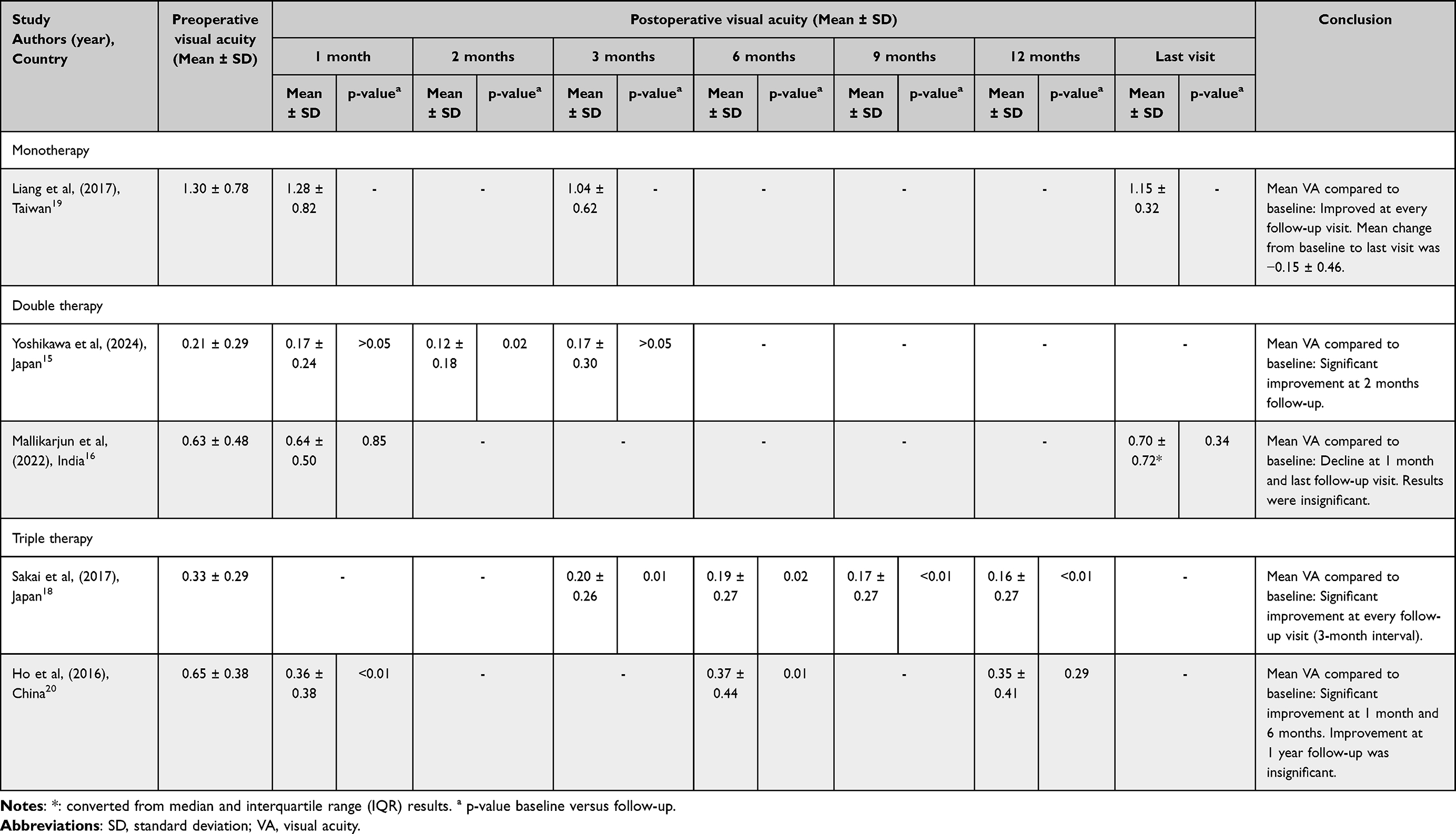 |
Table 7 Summary of BCVA Findings in Single-Arm Studies |
As for the comparative studies, three out of four studies showed lower mean BCVA results compared to the no-steroid cohorts. Double therapy studies did not report any significant results for BCVA comparison between every follow-up result to the baseline value.17,21–23 VA results of comparative studies and each study’s conclusion on VA efficacy are presented in Table 8.
 |
Table 8 Summary of BCVA Findings in Double-Arm Studies |
Adverse Events
Ten ophthalmic complications were recorded from nine included studies. Ocular hypertension was reported in seven studies, with two articles documenting a total of 10 previously non-glaucomatous samples that suffered an increase in IOP with a need for an IOP-lowering medication. However, only Lai et al (2010) demonstrated a significant association between ocular hypertension and a steroids-based therapy regimen (7/15; p < 0.05) compared to a non-steroid-based therapy regimen. There was also a significantly higher incidence of cataracts in the study by Lai et al (2010), with five out of 15 patients in the intervention group developing cataracts after therapy (p < 0.05). Additionally, cataract complications were reported in two other studies: Liang et al (2017) observed cataracts in two participants, and Nakata et al (2013) reported only one participant.19,22,23 In Nakata et al (2013), the incidence of cataract-related adverse events was not significantly different between eyes treated with or without ophthalmic steroids. Other complications, such as various posterior segment hemorrhages, retinal tears, and other subjective complaints post-therapy, were documented in detail in Table 9.
 |
Table 9 Adverse Events Incidence in Groups Treated With Ophthalmic Steroids |
Polyp Regression
The rate of polypoidal lesion regression was documented in four studies, defined as complete disappearance of lesions through fluorescence angiography (FA) and indocyanine green angiography (ICGA). Yoshikawa et al (2024) suggested a complete regression on 89.5% (17/19) of their populations at 3 months (17/19 eyes), while Ho et al (2016) achieved less at 6 months post-intervention despite a lower sample size (82%; 13/17). At 12 months, Sakai et al (2017) reported a total regression rate on all participants (13/13), while at 24 months, Nakata et al (2013) suggested that 91.7% of eyes included in their study (22/24) showed complete disappearance of polypoidal lesions. Nakata et al (2013) also compared their intervention group’s polyp regression rate to the rate achieved in the comparator group at a 2-year follow-up, which revealed no significant difference (22/24 [91.7%] vs 13/16 [81.3%]).15,18,20,22
Central Retinal Thickness (CRT)
Mallikarjun et al (2022) and Sakai et al (2017) were the only articles to measure and compare CRT between baseline values. At presentation, mean CRT was measured at 583 ± 285.12 μm and 569 ± 262 μm for Mallikarjun et al (2022) and Sakai et al (2017), respectively. One month after intervention, a significant change in mean CRT was witnessed in Mallikarjun et al (2022), specifically, down −261.7 μm from baseline thickness (321.3 ± 134.18 μm; p < 0.01). As for Sakai et al (2017), changes in mean CRT were recorded every 3 months until 12 months after the intervention, all of which showed significant reduction compared to its baseline value (p < 0.01). The lowest mean thickness was seen 3 months after intervention (226 ± 39 μm), although the final mean measurement (239 ± 43 μm) was not far different from the lowest measurement recorded.16,18
Central Foveal Thickness (CFT)
Three studies measured central foveal thickness as a therapeutic response parameter. At baseline, Yoshikawa et al (2024), Ho et al (2016), and Nakata et al (2013) reported similar CFT measurements; 329.2 ± 128.8 μm, 394.7 ± 70.6 μm, and 392.1 ± 129.5 μm, respectively. One-month post-treatment, Yoshikawa et al (2024) found a −131.4 μm reduction in mean thickness (197.8 ± 64.2 μm), whereas Ho et al (2016) achieved 20 μm less in mean thickness reduction than Yoshikawa et al (−102.7 μm; 292 ± 77 μm). Two years after intervention, Nakata et al produced a significant difference between the mean thickness of 230 ± 66 μm in the intervention group and 283 ± 204 μm in the comparator group. When compared to their baseline values, all studies reported significance, except for Ho et al’s (2016) result at one-year follow-up.15,20,22
Presence of Pigment Epithelial Detachment (PED)
Four studies reported the number of eyes with PEDs among participants. Mallikarjun et al (2022) showed a reduction from 9 eyes (75%) with PEDs initially to 3 eyes (25%) at the final follow-up. Sakai et al (2017) started with 13 eyes (100%) and observed a decrease to 4 eyes (30.8%) after one year of treatment. Nakata et al (2013) began with 23 eyes (57.5%) and found 5 eyes (12.5%) with persistent PEDs after two years. Ho et al (2016), who started with 12 eyes (70.6%), was the only study to record a complete resolution of PEDs in all cases after one year.16,18,20,22
Discussion
This systematic review evaluated the efficacy and safety of ophthalmic steroids for PCV. Our analysis revealed that the use of ophthalmic steroids as a monotherapy or a combination therapy regimen for PCV patients may provide significant VA improvements and other additional benefits, namely better regression rate of polypoidal lesions, reduction of RT, and elimination of PEDs, with tolerable side effects.
While previous studies suggested the use of anti-VEGF and/or PDT as an effective treatment for PCV, there has not been a consensus on which therapy is recommended as a first line. It is mainly due to the lack of understanding of the mechanisms underlying the development and progression of PCV. However, numerous studies support that inflammation plays a role in the development and progression of PCV. Several studies showed increased cytokines related to inflammation and angiogenesis (eg IL-31, LIF, VEGF, SDF1-ɑ, IL-23, MCP-1, TNF-ɑ) in the aqueous humor of patients with PCV that may play a role in the pathogenesis of PCV.24–27 A study also showed increased IL-1β expression in the vitreous body.28 These findings suggested that PCV may be mediated by an inflammatory process, where inflammatory agents could disrupt the blood-retinal barrier, resulting in vascular leakage. Therefore, targeting inflammation could be a potential treatment strategy for managing PCV patients. One of the most common drugs used to treat ocular inflammation is corticosteroids, known for their anti-inflammatory, anti-exudation, and anti-hyperplasia properties. To limit the systemic side effects of systemic corticosteroids, local routes of administration are often used to manage posterior ocular inflammation. In our included studies, ophthalmic steroids administered were TA and dexamethasone. TA was delivered intravitreally (IV) or via subtenon (ST) injection, while dexamethasone was given either as an intravitreal implant or solution.
Visual Outcomes
To this day, no randomized controlled trial has ever been conducted to assess the efficacy of corticosteroids in managing PCV, despite its inflammation-associated pathogenesis.9,10,12,24,28 In our treatment-naive population studies, groups treated with steroids showed improvements, although not all were significant. Notably, one monotherapy study employing monotherapy IVTA documented a mean BCVA reduction of −0.26 and −0.15 at the 3rd month and last follow-up examination, respectively. This study indicated that IVTA could be a stand-alone therapeutic management for treatment-naive PCV, where the availability of the latest therapeutic recommendation (eg anti-VEGF, PDT) is limited. A study comparing the pharmacokinetic profile of IVTA and STTA revealed that the former could last as long as 91 days within the vitreous, compared to 54 days for the latter. Moreover, IVTA concentration therapeutic effect (2000–5000 ng/g) would typically remain for 28 days, whereas TA therapeutic effect in the chorioretinal area would only last for 7 days.29 Such evidence might suggest that the IV method is a superior route of administration compared to ST for ophthalmic steroids.
Several studies have labelled the combination of PDT and anti-VEGF to be the best treatment for PCV compared to an anti-VEGF or PDT monotherapy.8,30–32 However, our steroid-based combination therapy studies revealed mean BCVA improvement and better mean change compared to the non-steroid groups, except for one study employing dexamethasone intravitreal implants (DXI).16 Despite the DXI mechanism of releasing higher dose of steroids in the first 6 weeks, a decline in BCVA a month after intervention and at the last follow-up were observed.16,33 It must be recognized that Mallikarjun et al (2022)’s participants were given DXI after anti-VEGF had been started. However, Sakai et al (2017) administered Aflibercept-resistant participants with STTA and documented significant mean BCVA improvements up to 1 year after. This might suggest an inferiority of DXM in the management of PCV. Reverting back to theory, compared to dexamethasone, TA is less water-soluble, has higher lipophilicity, and forms crystalline structures. These properties enhance diffusion into the vitreous, allowing a longer duration of effect in the vitreoretinal area compared to the injection of non-implant DXM solutions, which could explain the discrepancy discussed previously. If combined with a PRN prescription, TA injection could potentially provide more benefits than other corticosteroid agents in cases like PCV, where chronic and refractory inflammation contributes to disease pathogenesis.24,28,34,35 Moreover, the addition of ophthalmic steroid, like sub-tenon’s space injection, to the best current existing therapy, may also have a role in preventing intraocular inflammation that has been observed in brolucizumab therapy.15
Zhang et al (2018) also suggested IV steroid injection for PCV cases in the treatment of subretinal hemorrhage.17 As discussed above, inflammatory factors contributed to the occurrence of PCV, one of which is by interrupting the blood-retinal barrier integrity, leading to vascular exudation and the manifestation of massive subretinal hemorrhage. Triamcinolone acetonide works by modulating inflammatory pathways, as well as attenuating angiogenesis through the modulation of VEGF expression, thus stabilizing the blood–retinal barrier and reducing hemorrhagic occurrence. Hence, the administration of monotherapy POTA led to successful visual improvements and could be an alternative treatment in areas with limited access to anti-VEGF and/or PDT.
Adverse Events
Incidence of steroid-induced cataracts and IOP-related adverse events were increased in studies that employed IVTA, which is consistent with previously published literature applying IVTA as a main intervention.36–39 Periocular injection of steroids was also correlated with a higher risk of ocular hypertension and cataract formation, but studies that utilized STTA did not report any incidents of the two complications.40,41 Most side effects that arise after DII injection are commonly seen in the posterior segment, such as retinal tear or detachment and vitreous hemorrhage.33 Yet, Mallikarjun et al (2022) did not report any side effects relating to the vitreoretinal structures, thus hindering the analysis of the mentioned complications.16 Although intravitreal corticosteroids demonstrated the most side effects, future studies that consider the efficacy and safety of each route of administration are needed to consider the viability of ophthalmic steroids in PCV.
Anatomical Changes
Polypoidal regression rate is an important determinant in achieving therapy success. Our study found that, at three months, a steroid-based double therapy achieved an 89.5% polyp regression rate at three months, which was higher than the 69.7% and 71.4% rates seen with non-steroidal double therapies.8,15,42 Furthermore, one steroid-based triple therapy study demonstrated a total regression rate (100%) at 12 months, whereas non-steroidal double therapy could only reach 55.4% and 66.2% regression rates.18,43,44 Another important anatomical marker is CRT, and steroid-based therapy also depicted more substantial mean CRT reduction at 12 months than those observed in non-steroidal double therapy.18,42,45 Similar findings were also seen in CFT, where findings from our review showed higher mean CFT reduction at one month compared to a non-steroidal double therapy study at six months.15,20,46 In terms of PED resolution, our review showed a 69.2%–78.3% PED resolution at one to two years after a double-therapy or triple-therapy steroid-based intervention, while the non-steroidal monotherapy study only demonstrated a 61.3% reduction in one year.16,18,20,22,43 These anatomical findings suggest that steroid-based therapies may offer more significant improvements compared to non-steroidal regimens. Steroid-based treatments appear to provide greater reductions in polyp regression rate, CRT, and CFT, as well as more effective resolution PEDs.
A key strength of this review is its systematic approach in analyzing the different methods of corticosteroid administration for PCV patients. Through this analysis, we aimed to recommend the most effective approach for using ophthalmic steroids in the treatment of PCV. On the other hand, this review’s limitation is our inability to perform a meta-analysis, primarily due to the high heterogeneity among the studies. This variability stems from differences in steroid agents, dosages, frequencies, and additional therapies used within double or triple therapy regimens. Additionally, all included studies were observational with small sample sizes, which may affect the potential risk of bias and generalizability of the findings. Furthermore, some studies lack adequate follow-up periods, limiting the report of long-term treatment effects.
Conclusion
In conclusion, ophthalmic steroids could be considered as a monotherapy in resource-limited setting or as an adjunctive therapy alongside anti-VEGF and PDT with verteporfin as a triple therapy for PCV patients due to its promising benefit, minimal side effects, and economic practicability. Future research should include a randomized controlled trial consisting of steroid-based therapy for treatment-naive and/or anti-VEGF resistant PCV that may be needed to accurately determine its efficacy.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Uyama M, Wada M, Nagai Y. et al. Polypoidal choroidal vasculopathy: natural history. Am J Ophthalmol. 2002;133(5):639–648. doi:10.1016/S0002-9394(02)01404-6
2. Sho K, Takahashi K, Yamada H, et al. Polypoidal choroidal vasculopathy: incidence, demographic features, and clinical characteristics. Arch Ophthalmol. 2003;121(10):1392–1396. doi:10.1001/archopht.121.10.1392
3. Lorentzen TD, Subhi Y, Sorensen TL. Prevalence of polypoidal choroidal vasculopathy in white patients with exudative age-related macular degeneration: systematic review and meta- analysis. Retina. 2018;38(12):2363–2371. doi:10.1097/IAE.0000000000001872
4. Wong CW, Yanagi Y, Lee WK, et al. Age-related macular degeneration and polypoidal choroidal vasculopathy in Asians. Prog Retin Eye Res. 2016;53:107–139. doi:10.1016/j.preteyeres.2016.04.002
5. Chaikitmongkol V, Cheung CMG, Koizumi H, Govindahar V, Chhablani J, Lai TYY. Latest developments in polypoidal choroidal vasculopathy: epidemiology, etiology, diagnosis, and treatment. Asia Pac J Ophthalmol. 2020;9(3):260–268. doi:10.1097/01.APO.0000656992.00746.48
6. Sen P, Manayath G, Shroff D, Salloju V, Dhar P. Polypoidal choroidal vasculopathy: an update on diagnosis and treatment. Clin Ophthalmol. 2023;17:53–70. doi:10.2147/OPTH.S385827
7. Lee WK, Iida T, Ogura Y, et al. Efficacy and safety of intravitreal aflibercept for polypoidal choroidal vasculopathy in the PLANET study: a randomized clinical trial. JAMA Ophthalmol. 2018;136(7):786–793. doi:10.1001/jamaophthalmol.2018.1804
8. Lim TH, Lai TYY, Takahashi K, et al. Comparison of ranibizumab with or without verteporfin photodynamic therapy for polypoidal choroidal vasculopathy: the EVEREST II randomized clinical trial. JAMA Ophthalmol. 2020;138(9):935–942. doi:10.1001/jamaophthalmol.2020.2443
9. Kumar S, Nakashizuka H, Jones A, et al. Proteolytic degradation and inflammation play critical roles in polypoidal choroidal vasculopathy. Am J Pathol. 2017;187(12):2841–2857. doi:10.1016/j.ajpath.2017.08.025
10. Kumar A, Kumawat D, Dheepak SM, et al. Polypoidal choroidal vasculopathy: a comprehensive clinical update. Therapeutic Advances in Ophthalmology [Internet]. 2019; Available from: https://journals.sagepub.com/doi/10.1177/2515841419831152?cookieSet=1.
11. Subhi Y, Nielsen MK, Molbech CR, et al. Plasma markers of chronic low-grade inflammation in polypoidal choroidal vasculopathy and neovascular age-related macular degeneration. Acta Ophthalmol. 2019;97(1):99–106. doi:10.1111/aos.13886
12. Borgersen NJ, Møller-Lorentzen T, Sørensen TL, Subhi Y. Association between C-reactive protein and polypoidal choroidal vasculopathy: a systematic review and meta-analysis. Acta Ophthalmol. 2021;99(5):470–477. doi:10.1111/aos.14655
13. Study Quality Assessment Tools. [Internet]. NHLBI, NIH. Available from: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools.
14. Ottawa Hospital Research Institute. [Internet].Available from: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
15. Yoshikawa Y, Sakaki Y, Shinoda K, Kataoka K. Safety and effectiveness of intravitreal brolucizumab injection in combination with sub-tenon’s capsule triamcinolone acetonide injection for polypoidal choroidal vasculopathy during the loading phase. Cureus. 2024;16(5):e59481. doi:10.7759/cureus.59481
16. Mallikarjun K, Narayanan R, Raman R, et al. Dexamethasone implant improves anatomic response to anti-VEGF therapy in treatment-resistant polypoidal choroidal vasculopathy. Int Ophthalmol. 2022;42(4):1263–1272. doi:10.1007/s10792-021-02113-4
17. Zhang K, Chen Y, Sun X, et al. Periocular triamcinolone acetonide injection for treating polypoidal choroidal vasculopathy concurrent with hemorrhagic retinal detachment. Medicine. 2018;97(39):e12464. doi:10.1097/MD.0000000000012464
18. Sakai T, Kato N, Kubota M, Tsuneoka H. Effects of photodynamic therapy plus intravitreal aflibercept with subtenon triamcinolone injections for aflibercept-resistant polypoidal choroidal vasculopathy. Graefes Arch Clin Exp Ophthalmol. 2017;255(8):1565–1571. doi:10.1007/s00417-017-3700-3
19. Liang IC, Lin YR, Chien HW, Liu KR. Vision preservation in eyes of polypoidal choroidal vasculopathy with low-dose intravitreal triamcinolone acetonide. J Ocul Pharmacol Ther. 2017;33(1):42–49. doi:10.1089/jop.2015.0150
20. Ho M, Woo DCF, Chan VCK, Young AL, Brelen ME. Treatment of polypoidal choroidal vasculopathy by photodynamic therapy, aflibercept and dexamethasone triple therapy. Sci Rep. 2016;6(1):36870. doi:10.1038/srep36870
21. Sakai T, Ohkuma Y, Kohno H, Hayashi T, Watanabe A, Tsuneoka H. Three-year visual outcome of photodynamic therapy plus intravitreal bevacizumab with or without subtenon triamcinolone acetonide injections for polypoidal choroidal vasculopathy. Br J Ophthalmol. 2014;98(12):1642–1648. doi:10.1136/bjophthalmol-2014-305189
22. Nakata I, Tsujikawa A, Yamashiro K, et al. Two-year outcome of photodynamic therapy combined with intravitreal injection of bevacizumab and triamcinolone acetonide for polypoidal choroidal vasculopathy. Graefes Arch Clin Exp Ophthalmol. 2013;251(4):1073–1080. doi:10.1007/s00417-012-2137-y
23. Lai TYY, Lam CPS, Luk FOJ, et al. Photodynamic therapy with or without intravitreal triamcinolone acetonide for symptomatic polypoidal choroidal vasculopathy. J Ocul Pharmacol Ther. 2010;26(1):91–95. doi:10.1089/jop.2009.0073
24. Sasaki SI, Miyazaki D, Miyake KI, et al. Associations of IL-23 with polypoidal choroidal vasculopathy. Invest Ophthalmol Vis Sci. 2012;53(7):3424–3430. doi:10.1167/iovs.11-7913
25. Kikuchi M, Nakamura M, Ishikawa K, et al. Elevated C-reactive protein levels in patients with polypoidal choroidal vasculopathy and patients with neovascular age-related macular degeneration. Ophthalmology. 2007;114(9):1722–1727. doi:10.1016/j.ophtha.2006.12.021
26. Hu J, Leng X, Hu Y, et al. The features of inflammation factors concentrations in aqueous humor of polypoidal choroidal vasculopathy. PLoS One. 2016;11(1):e0147346. doi:10.1371/journal.pone.0147346
27. Zhou H, Zhao X, Yuan M, Chen Y. Comparison of cytokine levels in the aqueous humor of polypoidal choroidal vasculopathy and neovascular age-related macular degeneration patients. BMC Ophthalmol. 2020;20(1):1–7. doi:10.1186/s12886-019-1278-8
28. Zhao M, Bai Y, Xie W, et al. Interleukin-1β level is increased in vitreous of patients with neovascular age-related macular degeneration (nAMD) and polypoidal choroidal vasculopathy (PCV). PLoS One. 2015;10(5):e0125150. doi:10.1371/journal.pone.0125150
29. Arie Y, Miyai H, Suzuki A, et al. Comparative study on pharmacokinetics and toxicity of intravitreal and sub-tenon injection of triamcinolone acetonide in ocular tissues. Int J Ophthalmol. 2020;13(12):1864–1871. doi:10.18240/ijo.2020.12.04
30. Koh A, Lee WK, Chen LJ, et al. EVEREST study: efficacy and safety of verteporfin photodynamic therapy in combination with ranibizumab or alone versus ranibizumab monotherapy in patients with symptomatic macular polypoidal choroidal vasculopathy. Retina. 2012;32(8):1453–1464. doi:10.1097/IAE.0b013e31824f91e8
31. Lee YA, Yang CH, Yang CM, et al. Photodynamic therapy with or without intravitreal bevacizumab for polypoidal choroidal vasculopathy: two years of follow-up. Am J Ophthalmol. 2012;154(5):872–80.e2. doi:10.1016/j.ajo.2012.03.051
32. Kim SJ, Yu HG. Efficacy of combined photodynamic therapy and intravitreal bevacizumab injection versus photodynamic therapy alone in polypoidal choroidal vasculopathy. Retina. 2011;31(9):1827–1834. doi:10.1097/IAE.0b013e318214d01e
33. Fung AT, Tran T, Lim LL, et al. Local delivery of corticosteroids in clinical ophthalmology: a review. Clin Experiment Ophthalmol. 2020;48(3):366–401. doi:10.1111/ceo.13702
34. Edelman JL. Differentiating intraocular glucocorticoids. Ophthalmologica. 2010;224(Suppl 1):25–30. doi:10.1159/000315158
35. Cheung CMG, Lai TYY, Ruamviboonsuk P, et al. Polypoidal choroidal vasculopathy: definition, pathogenesis, diagnosis, and management. Ophthalmology. 2018;125(5):708–724. doi:10.1016/j.ophtha.2017.11.019
36. Ip MS, Scott IU, VanVeldhuisen PC, et al. A randomized trial comparing the efficacy and safety of intravitreal triamcinolone with observation to treat vision loss associated with macular edema secondary to central retinal vein occlusion: the Standard Care vs Corticosteroid for Retinal Vein Occlusion (SCORE) study report 5. Arch Ophthalmol. 2009;127(9):1101–1114. doi:10.1001/archophthalmol.2009.234
37. Scott IU, Ip MS, VanVeldhuisen PC, et al. A randomized trial comparing the efficacy and safety of intravitreal triamcinolone with standard care to treat vision loss associated with macular edema secondary to branch retinal vein occlusion: the Standard Care vs Corticosteroid for Retinal Vein Occlusion (SCORE) study report 6. Arch Ophthalmol. 2009;127(9):1115–1128. doi:10.1001/archophthalmol.2009.233
38. Islam MS, Vernon SA, Negi A. Intravitreal triamcinolone will cause posterior subcapsular cataract in most eyes with diabetic maculopathy within 2 years. Eye. 2007;21(3):321–323. doi:10.1038/sj.eye.6702304
39. Chawan-Saad J, Wu M, Wu A, Wu L. Corticosteroids for diabetic macular edema. Taiwan J Ophthalmol. 2019;9(4):233–242. doi:10.4103/tjo.tjo_68_19
40. Polski A, Liu KC, Gupta D, et al. Incident glaucoma and ocular hypertension after periocular and intravitreal steroid injections: a claims-based analysis. BMJ Open Ophthalmol. 2023;8(1):e001508. doi:10.1136/bmjophth-2023-001508
41. Sen HN, Vitale S, Gangaputra SS, et al. Periocular corticosteroid injections in uveitis: effects and complications. Ophthalmology. 2014;121(11):2275–2286. doi:10.1016/j.ophtha.2014.05.021
42. Gomi F, Oshima Y, Mori R, et al. Initial versus delayed photodynamic therapy in combination with ranibizumab for treatment of polypoidal choroidal vasculopathy: the Fujisan study. Retina. 2015;35(8):1569–1576. doi:10.1097/IAE.0000000000000526
43. Yamamoto A, Okada AA, Kano M, et al. One-year results of intravitreal aflibercept for polypoidal choroidal vasculopathy. Ophthalmol. 2015;122(9):1866–1872. doi:10.1016/j.ophtha.2015.05.024
44. Cho JH, Park YJ, Cho SC, et al. Posttreatment polyp regression and risk of massive submacular hemorrhage in eyes with polypoidal choroidal vasculopathy. Retina. 2020;40(3):468–476. doi:10.1097/IAE.0000000000002384
45. Sayanagi K, Fujimoto S, Hara C, et al. Effect of polyp regression and reduction on treatment efficacy in polypoidal choroidal vasculopathy treated with aflibercept. Sci Rep. 2024;14(1):1833. doi:10.1038/s41598-024-52448-y
46. Ho M, Lo ECF, Young AL, Liu DTL. Outcome of polypoidal choroidal vasculopathy at 1 year by combined therapy of photodynamic therapy with ranibizumab and predictive factors governing the outcome. Eye. 2014;28(12):1469–1476. doi:10.1038/eye.2014.222
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.