")
Back to Journals » Clinical Ophthalmology » Volume 18
Efficacy and Systemic Effects of a Single Deep Orbital Triamcinolone Injection for Thyroid Eye Disease
Authors Yamana Y , Kashima T, Mimura M
Received 2 May 2024
Accepted for publication 3 September 2024
Published 6 September 2024 Volume 2024:18 Pages 2567—2574
DOI https://doi.org/10.2147/OPTH.S476562
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yuji Yamana,1 Tomoyuki Kashima,1 Masashi Mimura1– 3
1Department of Ophthalmology, Oculofacial Clinic Group, Tokyo, Japan; 2Department of Ophthalmology, Hyogo Medical University, Nishinomiya, Japan; 3Department of Ophthalmology, Toho University Sakura Medical Center, Sakura, Japan
Correspondence: Yuji Yamana, Oculofacial Clinic, Tokyo, Japan, Email [email protected]
Purpose: Orbital steroid injections offer a potential therapeutic avenue for managing Thyroid Eye Disease (TED). This study aimed to assess the effectiveness and potential systemic impacts of a single deep orbital triamcinolone injection in TED patients.
Methods: In a prospective investigation conducted from January 2021 to March 2023, patients diagnosed with TED were enrolled. Inclusion criteria encompassed a Clinical Activity Score (CAS) of ≥ 3, extraocular muscle inflammation, and upper eyelid retraction. A total of 1 mL of triamcinolone acetonide (40 mg/mL) was administered posterior to the orbital septum at both the medial and lateral aspects of both the upper and lower eyelids. Parameters, including CAS, margin-reflex distances (MRD1 and MRD2), intraocular pressure (IOP), ocular motility (Hess area ratio [HAR%]), exophthalmometry, extraocular muscle size, and blood and urinary indices, were evaluated before and at 2 and 4 weeks after a single injection.
Results: Analysis included 28 patients (23 women, 5 men; mean age (SD): 38.7 (11.1) years), representing 56 eyes. Following the injection at 4 weeks, the mean CAS and MRD1 significantly decreased by 2 points and 0.8 mm, respectively. There was a 4.5% increase in HAR%, and extraocular muscle size decreased by 4 to 15.3 mm². Neutrophil count, C-reactive protein, and thyroid antibodies significantly decreased. No severe adverse ophthalmic or systemic effects, including IOP increases or liver damage, were observed.
Conclusion: Bilateral single orbital triamcinolone injections provided relief from TED symptoms through both direct effects on orbital soft tissue and systemic effects by decreasing antibody reactions.
Keywords: thyroid eye disease, orbital steroid injections, triamcinolone, extraocular muscles
Introduction
Thyroid eye disease (TED) represents a prevalent type of orbital tissue inflammation associated with autoimmune disorders linked to thyroid dysfunction, which is characterized by a spectrum of metabolic and immunologic disturbances.1,2 Because of their potent anti-inflammatory and immunosuppressive properties, systemic glucocorticoids have traditionally served as the first-line treatment for TED to mitigate inflammation. However, their use is fraught with a plethora of adverse effects, encompassing hyperglycemia, hypertension, metabolic disorders leading to the characteristic “moon face”, gastric ulcers, osteoporosis, and an increased susceptibility to infectious diseases.3,4
To circumvent these adverse effects, local administration of glucocorticoids has been explored since Gebertt first reported this approach in 1961.5,6 Localized delivery is accomplished through subconjunctival, and sub-Tenon injections. In contrast, retro-orbital-septal injection, introduced since Ebner’s report in 2004, offers an alternative method. This procedure, performed transcutaneously using a half-inch, 27-G needle, facilitates the precise delivery of medication into the lateral lower deep orbital fat, yielding promising results in the anti-inflammatory treatment of orbital tissue.7 Furthermore, Bagheri et al reported retro-orbital-septal injection of triamcinolone and dexamethasone into both the upper and lower quadrants of the orbital soft tissue.8 In this report, this approach was applied for patients with active TED who were resistant to or dependent on systemic steroids or faced complications related to systemic steroid use. The results demonstrated a significant reduction in orbital inflammation, including upper and lower eyelid retraction, ocular motility issues, and inflammatory markers such as the Clinical Activity Score (CAS) and NOSPECS classification. An intriguing aspect of the retro-orbital-septal delivery method is its capacity to produce a dramatic effect after only one or two injections.7,8
Thus, this novel procedure may have advantages not only in local control of orbital inflammation but also in mitigating systemic adverse effects. However, no study to date has comprehensively evaluated the systemic effects of orbital corticosteroid injections, primarily because of the systemic absorption of the medication. The current report aims to address this gap by focusing on the efficacy and systemic effects of deep orbital injection of triamcinolone, with the intent of promoting and advancing this procedure. To achieve this goal, we conducted a prospective clinical investigation involving TED patients who underwent a single deep orbital injection of triamcinolone, followed by comprehensive ophthalmic and pharmacological assessments, including blood and urinary panels.
Patients and Methods
This prospective study enrolled Japanese individuals diagnosed with TED who underwent single, bilateral, deep orbital triamcinolone injections between January 2021 and March 2023. The study adhered to the principles outlined in the Declaration of Helsinki, with all patients providing signed informed consent. The Institutional Review Boards of the Oculofacial Clinic Group approved the study protocol, and the study was registered with the Ethical Committee of the Oculofacial Clinic Group (Approval Number: 2023072801).
The inclusion criteria consisted of a CAS of 3 or higher and localized inflammation affecting the extraocular muscles and upper eyelid retraction. The exclusion criteria included compressive optic neuropathy, severe TED (including dysthyroid optic neuropathy and corneal breakdown) necessitating intravenous methylprednisolone pulse therapy.
Injection Procedure
A total of 1 mL of triamcinolone acetonide (40 mg/mL) was administered posterior to the orbital septum using a 27-G, half-inch, disposable needle (0.30×12 mm, Dentronics, Tokyo, Japan) at four distinct sites, covering both the medial and lateral aspects of both the upper and lower eyelids (Figure 1).
 |
Figure 1 Deep Orbital Injection of Triamcinolone Acetonide. |
Assessment Metrics
Evaluation metrics included the CAS, margin-reflex distances (MRD1 and MRD2), intraocular pressure (IOP) measured via non-contact tonometry, hematological parameters (thyroid panel, comprehensive metabolic panel, and serum cortisol), urinary cortisol levels, and ocular motility assessed using the Hess area ratio (HAR%). The extent of proptosis was determined via magnetic resonance imaging (MRI), including measurements related to extraocular muscle sizes. All ophthalmic and systemic assessments were performed before injection and at 2 and 4 weeks post-injection.
Ophthalmic Data Analysis
The CAS and systemic adverse effects were evaluated through standardized questionnaires. The MRD1 and MRD2 measurements were conducted in millimeters using ImageJ software (https://imagej.net/ij/index.html), with pupil diameter derived from non-contact tonometry data.
The extent of proptosis was assessed using MRI by measuring the distance between the corneal eminence and the connecting lines of the zygomatic bones in a horizontal section of a T1-weighted image.
The sizes of the inferior oblique, superior rectus, medial rectus, lateral rectus, and inferior rectus muscles were also assessed by MRI. The muscle size was determined at the point of greatest enlargement within the coronal section of the T1-weighted MRI image. Because of challenges in detecting the superior oblique muscle via MRI in most patients, this muscle was not investigated. Three-dimensional MRI reconstructions were generated using SYNAPSE VINCENT Ver. 5 software (Fujifilm Medical, Tokyo, Japan).
Ocular motility was quantified using the HAR% technique, which involves calculating the percentage ratio of the lengths of the vertical and horizontal sides on both the affected and healthy sides using the Hess chart. This method serves as an objective tool for assessing preoperative diplopia and orbital fracture severity.9 The HAR% measurement was employed to evaluate the effects of orbital steroid injection treatment.
Systemic Data Analysis
The thyroid panel assay comprised free triiodothyronine, free tetraiodothyronine, and thyroid-stimulating, thyrotropin receptor, thyroglobulin, and thyroid peroxidase antibodies. Comprehensive metabolic panel assessments included the white blood cell count, neutrophil count, and C-reactive protein, total bilirubin, aspartate aminotransferase, alanine aminotransferase, γ-glutamyl transpeptidase, creatinine, and glucose levels.
Statistical Analysis
Data analysis was conducted using SPSS Statistics Ver. 27 (IBM Corp., Armonk, NY, USA), with comparisons performed using the Wilcoxon signed-rank test.
Results
Ophthalmic Manifestations
The initial CAS (SD) averaged 4.22(1.29) and significantly decreased to 2.20(1.10) (P<0.001) at 4 weeks post-injection. The mean MRD1 measurement (SD) decreased from 4.25(1.67) mm to 3.53(1.55) mm (P<0.001) over the same period, while the MRD2 remained unchanged post-injection. We noted reductions in the maximum coronal area of the extraocular muscles, including the superior rectus (30.9%), inferior rectus (36.2%), medial rectus (21.1%), lateral rectus (26.9%), and inferior oblique (23.3%) (all P<0.001) (Figure 2). The mean HAR% (SD) was initially 94.42(4.45) % and increased to 98.94(6.26) % (P=0.014) after 4 weeks. No significant variations were observed in the IOP or the extent of proptosis (Table 1).
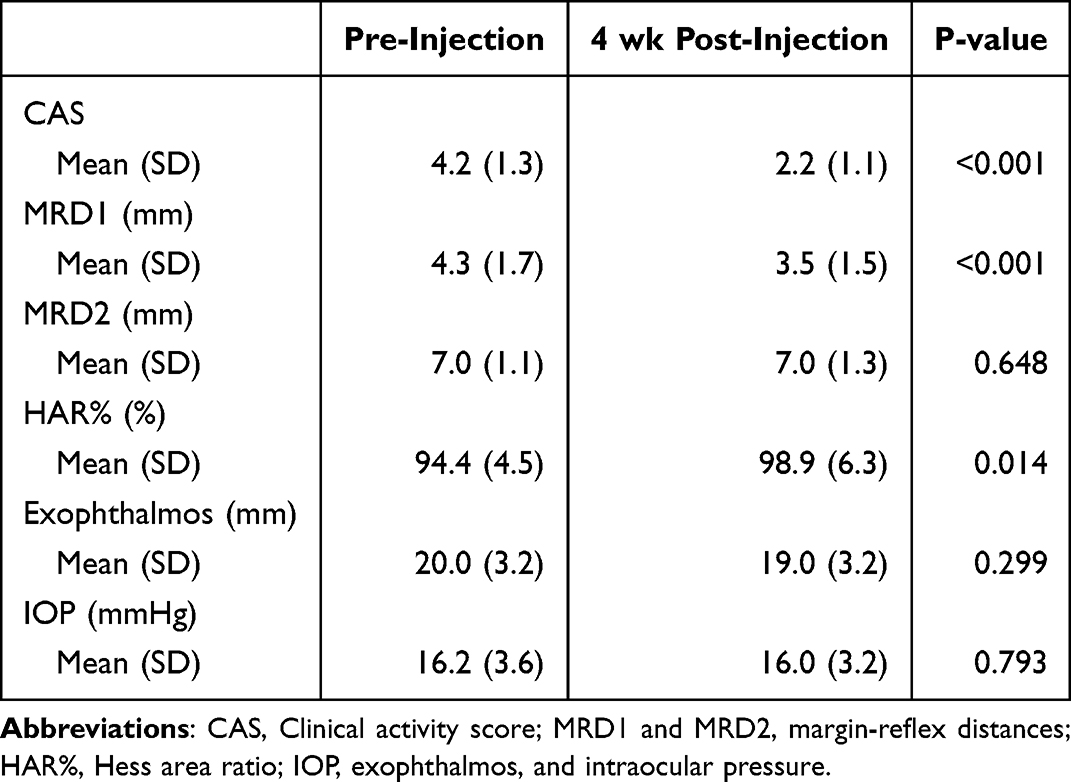 |
Table 1 Changes of Ophthalmic Parameters Before and 4 Weeks After a Single Deep Orbital Injection of 40 Mg of Triamcinolone Acetonide |
 |
Figure 2 Changes of cross-sectional area of extraocular muscles before and 4 weeks after a single deep orbital injection of 40 mg of triamcinolone acetonide. Abbreviations: IR, inferior rectus; SR, superior rectus; IO, inferior oblique; MR, medial rectus; and LR, lateral rectus muscles. |
Systemic Manifestations
At 2 weeks after the injection, increases in white blood cell and neutrophil counts were observed (P=0.017, P=0.021), followed by subsequent decreases by week 4 (P=0.011, P=0.008). Importantly, no exacerbation of hepatic enzyme levels, glucose, or creatinine was observed (Table 2). Several indices within the thyroid panel were affected, with distinct decreases observed in free triiodothyronine (P<0.04), thyroid-stimulating antibody (P<0.02), thyrotropin receptor antibody (P<0.01), and thyroid peroxidase antibody, and the thyroglobulin antibody level gradually decreased within 4 weeks post-injection (Table 3). Serum and urinary cortisol levels temporarily decreased after 2 weeks (P<0.001, P<0.001) and then increased after 4 weeks compared with the 2-week levels (P=0.027, P=0.050). Adverse effects included menstrual irregularities (5/28,17.8%), internal hemorrhage (5/28, 17.8%), acne (2/28, 7.1%), insomnia (2/28, 7.1%), and leg cramps (1/28, 3.6%).
 |
Table 2 Changes of Serum Laboratory Data Before and 4 Weeks After a Single Deep Orbital Injection of 40 Mg of Triamcinolone Acetonide |
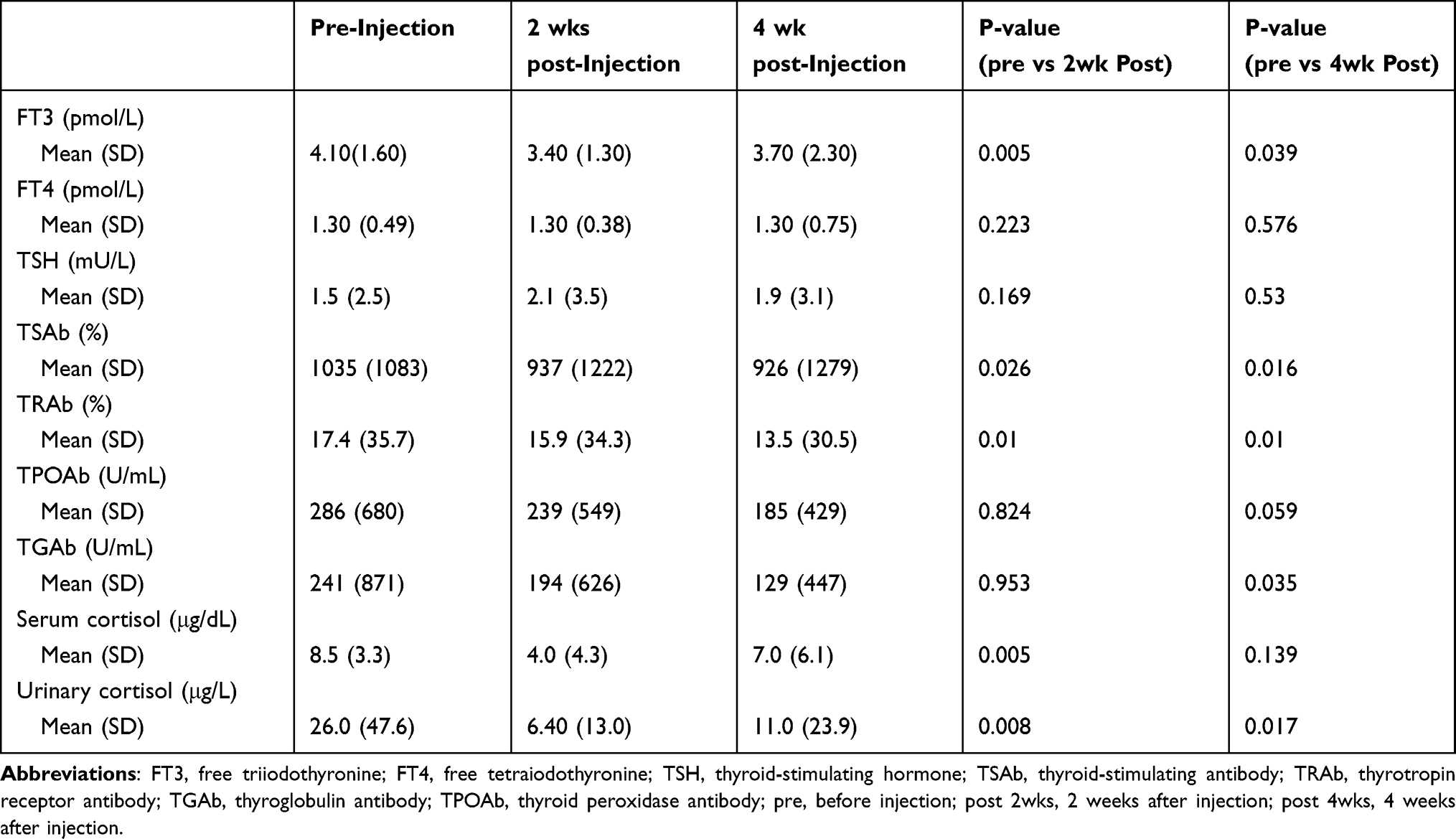 |
Table 3 Changes of Thyroid Panel and Cortisol Level Before and 4 Weeks After a Single Deep Orbital Injection of 40 Mg of Triamcinolone Acetonide |
Discussion
The present study introduces a promising therapeutic approach for TED management through a single deep orbital injection of 40 mg of triamcinolone acetonide. This intervention significantly improved the inflammatory activity of TED, including upper eyelid retraction and extraocular muscle swelling, while exhibiting minimal adverse ocular and systemic effects.
Deep orbital injection, as an emerging technique, allows for the direct administration of steroids to the posterior aspect of the orbital globe, bypassing the orbital septum.7,8,10–12 Our results align with previous reports, demonstrating that the injection of triamcinolone has a substantial anti-inflammatory effect on the extraocular muscles and levator muscles of the upper eyelids. This study includes differences in the studied populations (East Asian vs Caucasian) and variations in methodology (frequency, injection area, and steroid agents) compared with previous reports; nevertheless, our study substantiates the concept that a single orbital corticosteroid injection can attenuate TED activity.13
One concern associated with local administration of steroid agents around the eye is the potential adverse effect on IOP. Previous research has explored the mechanisms underlying corticosteroid-induced ocular hypertension, which is often linked to changes in gene expression in the trabecular meshwork.14 The absence of elevated IOP in our study could be attributed to corticosteroid administration in the posterior segment, potentially minimizing direct effects on the endothelium of Schlemm’s canal. Deep orbital injection delivers corticosteroids closer to the inflamed orbital tissue and farther from Schlemm’s canal, resulting in less of an increase in IOP (0%–16.7%)7,8,11,12,15 than that produced with pre-aponeurotic or sub-Tenon injection (4%–31%).16–20 However, the deep orbital injection technique must be approached with caution because of reported complications such as globe perforation, vessel occlusion, and toxic neuropathy, although our study did not encounter such issues.7,8
In addition to its ophthalmic effects, we vigilantly monitored potential systemic effects of orbital corticosteroid injections. While intravenous methylprednisolone pulse therapy has been associated with acute and severe liver damage and metabolic disorders,21–25 our study observed minimal hepatic, glycemic, and renal impacts by a single local injection. However, serum and urinary cortisol levels displayed temporary decreases, suggesting a mild depression in endogenous cortisol production. Ebner et al also reported blood and urinary cortisol levels after multiple orbital injections, with only urinary cortisol showing a difference between week 0 and week 10 after injection.7 Our study provides a more detailed understanding of the influence of a single injection, indicating that cortisol can be systemically absorbed for up to 2 weeks, with levels tending to rebound to normal within 4 weeks, particularly in blood. This finding suggests that monthly local injections can limit systemic adverse effects. Moreover, Alkawas et al compared the clinical effects of multiple deep orbital injections with oral steroid administration and concluded that orbital injection is effective and safe in mitigating the systemic adverse effects of steroids, further supporting the safety and efficacy of deep orbital injection.12
An additional contribution of our study compared with previous reports is the decrease in antibodies related to TED activity, signifying the suppression of systemic autoimmune responses by local injection.26–34 This finding suggests that the orbital steroid agents may be absorbed into the bloodstream to some extent, implying that local injection can impact TED activity not only locally but also systemically. In other words, the systemic impact is limited, indicating that adverse systemic effects resulting from local injection are within an acceptable range.
Several limitations warrant consideration. Our study focused on a single initial administration, lacking data on multiple administrations in clinical settings and long-term follow-up. Consequently, the effects and side effects of multiple injections remain unexplored. Future research should also investigate dose-dependent side effects and conduct comparative analyses of various steroid injection administration methods to provide a comprehensive understanding of their safety and efficacy.
Conclusions
In summary, our study robustly demonstrates the favorable effects of a single deep orbital corticosteroid administration for TED treatment without inducing substantial local or systemic adverse effects. Improvements in local and systemic assessments, TED-related antibody levels, and orbital muscle dimensions underscore the effectiveness of this intervention in modulating TED activity. While our study has limitations, including a limited patient cohort and a lack of iterative treatments, comprehensive validation will necessitate an expanded and iteratively treated patient series in the future.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
This study was approved by the Ethical Committee of the Oculofacial Clinic Group (Registration ID: 2023072801).
Informed Consent
Written informed consent was obtained from the patients for participation in this study and for the publication of this case report and the accompanying images.
Acknowledgments
We thank Lisa Kreiner, PhD, from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Author Contributions
TK and MM conceived the idea of the study. TK supervised the conduct of this study. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bartalena L, Kahaly GJ, Baldeschi L, et al. EUGOGO. The 2021 European Group on Graves’ orbitopathy (EUGOGO) clinical practice guidelines for the medical management of graves’ orbitopathy. Eur J Endocrinol. 2021;185(4):G43–G67. doi:10.1530/EJE-21-0479
2. Wang Y, Smith TJ. Current concepts in the molecular pathogenesis of thyroid associated ophthalmopathy. Invest Ophthalmol Vis Sci. 2014;55(3):1735–1748. doi:10.1167/iovs.14-14002
3. Kendall-Taylor P, Crombie AL, Stephenson AM, Hardwick M, Hall K. Intravenous methylprednisolone in the treatment of graves’ ophthalmopathy. BMJ. 1988;297(6663):1574–1578. doi:10.1136/bmj.297.6663.1574
4. Hiromatsu Y, Tanaka K, Sato M, et al. Intravenous methylprednisolone pulse therapy for graves’ ophthalmopathy. Endocr J. 1993;40(1):63–72. doi:10.1507/endocrj.40.63
5. Gebertt S. Depot-methylprednisolone for subconjunctival and retrobulbar injections. Lancet. 1961;278(7198):344–345. doi:10.1016/S0140-6736(61)90636-5
6. Garber MI. Methylprednisolone in the treatment of exophthalmos. Lancet. 1966;287(7444):958–960. doi:10.1016/S0140-6736(66)90954-8
7. Ebner R, Devoto MH, Weil D, et al. Treatment of thyroid associated ophthalmopathy with periocular injections of triamcinolone. Br J Ophthalmol. 2004;88(11):1380–1386. doi:10.1136/bjo.2004.046193
8. Bagheri A, Abbaszadeh M, Yazdani S, et al. Intraorbital steroid injection for active thyroid ophthalmopathy. JOVR. 2020;15(1):69–77. doi:10.18502/jovr.v15i1.5948
9. Yamanaka Y, Watanabe A, Rajak SN, Nakayama T, Sotozono C. Correlation between surgical timing and postoperative ocular motility in orbital blowout fractures. Graefes Arch Clin Exp Ophthalmol. 2022;260(1):319–325. doi:10.1007/s00417-021-05327-5
10. Goldberg RA. Orbital steroid injections. Br J Ophthalmol. 2004;88(11):1359–1360. doi:10.1136/bjo.2004.051755
11. Bordaberry M, Marques DL, Pereira-Lima JC, Marcon IM, Schmid H. Repeated peribulbar injections of triamcinolone acetonide: a successful and safe treatment for moderate to severe graves’ ophthalmopathy. Acta Ophthalmol. 2009;87(1):58–64. doi:10.1111/j.1755-3768.2008.01171.x
12. Alkawas AA, Hussein AM, Shahien EA. Orbital steroid injection versus oral steroid therapy in management of thyroid-related ophthalmopathy. Clin Exp Ophthalmol. 2010;38(7):692–697. doi:10.1111/j.1442-9071.2010.02332.x
13. Hiromatsu Y, Kojima K, Ishihara N, et al. Role of magnetic resonance imaging in thyroid-associated ophthalmopathy: its predictive value for therapeutic outcome of immunosuppressive therapy. Thyroid. 1992;2(4):299–305. doi:10.1089/thy.1992.2.299
14. Clark AF. Basic sciences in clinical glaucoma; steroids, ocular hypertension, and glaucoma. J Glaucoma. 1995;4(5):354–369. doi:10.1097/00061198-199510000-00010
15. Hirooka K, Shiraga F, Tanaka S, Baba T, Mandai H. Risk factors for elevated intraocular pressure after trans-tenon retrobulbar injections of triamcinolone. Jpn J Ophthalmol. 2006;50(3):235–238. doi:10.1007/s10384-005-0306-9
16. Xu D, Liu Y, Xu H, Li H. Repeated triamcinolone acetonide injection in the treatment of upper-lid retraction in patients with thyroid-associated ophthalmopathy. Can J Ophthalmol. 2012;47(1):34–41. doi:10.1016/j.jcjo.2011.12.005
17. Lee SJ, Rim TH, Jang SY, et al. Treatment of upper eyelid retraction related to thyroid-associated ophthalmopathy using subconjunctival triamcinolone injections. Graefes Arch Clin Exp Ophthalmol. 2013;251(1):261–270. doi:10.1007/s00417-012-2153-y
18. Lee JM, Lee H, Park M, et al. Subconjunctival injection of triamcinolone for the treatment of upper lid retraction associated with thyroid eye disease. J Craniofac Surg. 2012;23(6):1755–1758. doi:10.1097/SCS.0b013e3182646043
19. Hamed-Azzam S, Mukari A, Feldman I, et al. Fornix triamcinolone injection for thyroid orbitopathy. Graefes Arch Clin Exp Ophthalmol. 2015;253(5):811–816. doi:10.1007/s00417-015-2957-7
20. Chew EY, Glassman AR, Beck RW, et al. Ocular side effects associated with peribulbar injections of triamcinolone acetonide for diabetic macular edema. Retina. 2011;31(2):284–289. doi:10.1097/IAE.0b013e3181f049a8
21. Le Moli R, Baldeschi L, Saeed P, Regensburg N, Mourits MP, Wiersinga WM. Determinants of liver damage associated with intravenous methylprednisolone pulse therapy in graves’ ophthalmopathy. Thyroid. 2007;17(4):357–362. doi:10.1089/thy.2006.0267
22. Liu D, Ahmet A, Ward L, et al. A practical guide to the monitoring and management of the complications of corticosteroid therapy. Allergy Asthma Clin Immunol. 2013;9(1):30. doi:10.1186/1710-1492-9-30
23. Weissel M, Hauff W. Fatal liver failure after high-dose glucocorticoid pulse therapy in a patient with severe thyroid eye disease. Thyroid. 2000;10(6):521. doi:10.1089/thy.2000.10.11
24. Marinó M, Morabito E, Brunetto MR, Bartalena L, Pinchera A, Marocci C. Acute and severe liver damage associated with intravenous glucocorticoid pulse therapy in patients with graves’ ophthalmopathy. Thyroid. 2004;14(5):403–406. doi:10.1089/10507250477419327631
25. Farrell GC. Drugs and steatohepatitis. Semin Liver Dis. 2002;22(02):185–194. doi:10.1055/s-2002-30106
26. Bahn RS. Graves’ ophthalmopathy. N Engl J Med. 2010;362(8):726–738. doi:10.1056/NEJMra0905750
27. Rapoport B, McLachlan SM. The thyrotropin receptor in graves’ disease. Thyroid. 2007;17(10):911–922. PubMed: 17822379. doi:10.1089/thy.2007.0170
28. Khoo DH, Eng PH, Ho SC, et al. Graves’ ophthalmopathy in the absence of elevated free thyroxine and triiodothyronine levels: prevalence, natural history, and thyrotropin receptor antibody levels. Thyroid. 2000;10(12):1093–1100. PubMed: 11201855. doi:10.1089/thy.2000.10.1093
29. Eckstein AK, Lösch C, Glowacka D, et al. Euthyroid and primarily hypothyroid patients develop milder and significantly more asymmetrical graves’ ophthalmopathy. Br J Ophthalmol. 2009;93(8):1052–1056. PubMed: 19221109. doi:10.1136/bjo.2007.137265
30. Gerding MN, van der Meer JW, Broenink M, Bakker O, Wiersinga WM, Prummel MF. Association of thyrotrophin receptor antibodies with the clinical features of graves’ ophthalmopathy. Clin Endocrinol. 2000;52(3):267–271. PubMed: 10718823. doi:10.1046/j.1365-2265.2000.00959.x
31. Eckstein AK, Plicht M, Lax H, et al. Thyrotropin receptor autoantibodies are independent risk factors for Graves’ ophthalmopathy and help to predict severity and outcome of the disease. J Clin Endocrinol Metab. 2006;91(9):3464–3470. PubMed: 16835285. doi:10.1210/jc.2005-2813
32. Morris JC, Hay ID, Nelson RE, Jiang NS. Clinical utility of thyrotropin-receptor antibody assays: comparison of radioreceptor and bioassay methods. Mayo Clin Proc. 1988;63(7):707–717. PubMed: 2898572. doi:10.1016/S0025-6196(12)65533-5
33. Kotwal A, Stan M. Thyrotropin receptor antibodies-an overview. Ophthalmic Plast Reconstr Surg. 2018;34(4S):S20–S27. doi:10.1097/IOP.0000000000001052
34. Vargas-Uricoechea H, Nogueira JP, Pinzon-Fernandez MV, Schwarzstein D. The usefulness of thyroid antibodies in the diagnostic approach to autoimmune thyroid disease. Antibodies. 2023;12(3):48. doi:10.3390/antib12030048
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.