")
Back to Journals » Journal of Inflammation Research » Volume 18
Efficacy of Cooling Blankets and Cold Fluid Infusions in Classic Heatstroke Treatment: A Controlled Study in Rats
Authors Chen L , Liu C, Zhang Z , Zhang Y, Feng X
Received 31 December 2024
Accepted for publication 28 March 2025
Published 10 April 2025 Volume 2025:18 Pages 4979—4994
DOI https://doi.org/10.2147/JIR.S512014
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Tara Strutt
Lan Chen,1,* Chang Liu,1,* Zhaocai Zhang,2 Yuping Zhang,1 Xiuqin Feng1
1Nursing Department, The Second Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, Zhejiang, 310009, People’s Republic of China; 2Department of Critical Care Medicine, The Second Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, Zhejiang, 310009, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiuqin Feng, Nursing Department, The Second Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, Zhejiang Province, 310009, People’s Republic of China, Tel +8613757119151, Email [email protected]
Background: Rapid core temperature reduction is crucial for treating heatstroke. Clinical methods like cooling blankets and cold fluid infusions are common, but their specific effects are not well defined. This study evaluates these methods’ cooling effects and prognosis impact in classic heatstroke rats.
Methods: Sixty Sprague Dawley rats with classic heatstroke were divided into five groups: cooling blanket, cold fluid infusion, combination (combined cooling blanket and cold fluid infusion), natural cooling (control), and cold water immersion (positive control). Core temperature and mean arterial pressure were monitored. Blood samples were taken at 0.5 and 2 hours post-cooling for analysis. Half the rats underwent pathological evaluation and apoptosis analysis of heart and kidney tissues at 2 hours. The rest were observed for 24-hour survival.
Results: The combination group showed the fastest cooling within 10 minutes. Cooling blanket and cold fluid infusion groups had similar cooling rates. Heart and kidney function indicators and inflammatory cytokine levels were significantly lower in the combination and cold fluid infusion groups compared to the cooling blanket group. Pathological damage was highest in the cooling blanket group. Cooling rate negative correlated with organ function indicates and inflammation markers. No rats in the cooling groups died, while seven in the natural cooling group did.
Conclusion: Cooling methods differ in effectiveness and impact on inflammation and organ function. While cooling blankets demonstrate limited therapeutic efficacy and potential risks when used in isolation, rapid cold fluid infusion emerges as the preferred cooling modality by preserving cardiac structure and renal function while attenuating systemic inflammation. Early rapid cooling improves organ function and prognosis in classic heatstroke rats. Proper cooling methods are crucial for effective heatstroke management, reducing organ damage, and improving survival rates.
Plain Language Summary:Both cooling blankets and cold intravenous fluids help lower body temperature in heatstroke, but we are still learning how they differently affect the body.In animal studies, cold fluids given through veins worked better than just using cooling blankets - they protected both heart and kidneys from damage and reduced inflammation, even though both methods cooled the body equally fast.Using cold fluids together with cooling blankets cooled rats faster and more effectively, leading to less organ damage and fewer dangerous inflammation reactions.More research is needed to determine the best combination of cooling methods to help classic heatstroke patients recover better.
Keywords: heatstroke, cooling blanket, cold fluid infusion, cold water immersion, cooling rate, inflammation cytokine
Introduction
Heatstroke (HS) represents a life-threatening syndrome characterized by core body temperature exceeding 40°C coupled with central nervous system dysfunction. Classic heatstroke (CHS), predominantly affecting older adults with comorbidities during heatwaves, arises from passive exposure to hot-humid environments, characterized by disrupted thermoregulation due to an imbalance between heat production and dissipation.1 The severity of cellular and tissue damage in HS patients depends on the maximum temperature reached and the duration of hyperthermia.2 Rapid cooling to reduce core temperature can halt cellular damage, quickly reverse organ dysfunction, and improve patient outcomes.3 Clinical evidence indicates that achieving core temperature below 40.0°C within 30 minutes of symptom onset significantly reduces mortality and may prevent fatal outcomes.4,5 Our prior research further demonstrates that cooling rates during the initial 30-minute emergency treatment window exhibit significant correlations with both multi-organ dysfunction severity and in-hospital mortality rates.6 Therefore, implementing effective and convenient cooling measures to quickly restore core temperature is crucial for HS patients.7–9
Since the pathogenesis of HS does not involve a change in the hypothalamic set-point, antipyretics like aspirin and acetaminophen are ineffective in its treatment.10,11 Additionally, these medications can exacerbate coagulation disorders and liver damage in HS patients.9,11,12 Therefore, physical cooling remains the primary treatment method for HS patients. Effective cooling can be achieved through conduction (increasing the temperature gradient between the skin and surrounding objects), evaporation (increasing water vapor pressure), and convection (increasing air speed).8 Current research suggests that among traditional cooling methods, cold water immersion (CWI), which employs conductive cooling, has the fastest cooling rate and is often recommended as the primary on-site cooling measure for patients with exertional heatstroke (EHS).13,14 However, there is insufficient evidence to demonstrate the advantages of CWI for cooling patients with CHS. CWI has side effects such as shivering, peripheral vasoconstriction, and agitation, which can affect patient tolerance and may be associated with poor prognosis in elderly patients.15,16 Furthermore, CWI can interfere with other medical treatments, making it unsuitable for patients requiring active medical intervention, such as those with impaired consciousness, airway damage, circulatory failure, or convulsions.13,16 Other cooling measures, such as using ice packs for conductive cooling, tepid water sponge bathing for evaporative cooling, or fan-assisted convective cooling, are not sufficiently effective on their own and are typically used as part of combined cooling strategies.
Novel cooling methods, including the infusion of cold crystalloid fluids (4°C), the use of intravascular cooling catheters for internal cooling, and the use of cold air or water-circulating blankets for external cooling, have proven effective in inducing mild hypothermia and improving neurological outcomes in critically ill patients, particularly those with cardiac arrest.17 These methods, especially cold fluid infusion and cooling blankets (CB), are increasingly being applied in the treatment of HS due to their convenience. However, unlike the low perfusion state following cardiac arrest resuscitation, HS patients generally exhibit high blood flow and vasodilation to increase heat dissipation. Blood flow state is a crucial factor in body temperature regulation.18 Therefore, the effectiveness of these cooling methods in HS requires validation.8 To date, no controlled studies have explored and compared the impact of these cooling techniques on cooling time and outcomes in HS patients.
Rapid cooling constitutes the cornerstone of HS management, with method selection requiring careful consideration of implementation feasibility, thermal transfer efficiency, physiological tolerance, and ultimate clinical outcomes. The predominant reliance on rodent models in HS research stems from two critical factors: (1) inherent ethical and logistical constraints in conducting controlled human trials during acute emergencies, and (2) their unique capacity to replicate pathophysiological extremes unattainable in clinical settings. Rat models demonstrate particular translational value by recapitulating hallmark HS manifestations - including fulminant hyperthermia, systemic inflammatory cascades, and sequential multi-organ dysfunction - that mirror human pathophysiology, establishing them as a valuable translational platform for therapeutic evaluation.19 Under standardized protocols, thermal stress was induced through either: (i) precision-controlled environmental chambers maintaining 40–43°C with 60% relative humidity 20,21 or (ii) folded heating pad set at 43°C.22,23 This experimental framework incorporated continuous core temperature monitoring and arterial pressure monitoring, with validated diagnostic thresholds for CHS induction defined as core temperature >41.0–43.0°C20,23 concurrent with mean arterial pressure (MAP) reduction.22,24
This study aims to use CHS rats with CWI as the standard control to preliminarily explore the cooling effects of CB and cold fluid infusion and their differential impacts on organ function (including cardiac and renal function), providing a basis for subsequent clinical research. Based on existing studies, we hypothesize that the combined use of CB and cold fluid infusion will have a better cooling effect compared to either method alone.
Materials and Methods
Animal Preparation and Housing
Adult male Sprague-Dawley rats (350–400 g, Specific Pathogen Free) were housed individually at 20–25°C, 45–50% humidity, with a 12-hour light-dark cycle. They had free access to standard rodent feed and water. After a one-week acclimatization, experiments commenced. All protocols were conducted in compliance with the ARRIVE guidelines and approved by the Second Affiliated Hospital Zhejiang University School of Medicine (Approval ID: AIRB-2023-1677). Surviving rats were humanely euthanized using an overdose of sodium pentobarbital, adhering to ethical guidelines.
Surgical Procedures and Physiological Monitoring
Anesthesia and Preparation
Rats were anesthetized with an intraperitoneal injection of sodium pentobarbital at an initial dose of 40 mg/kg body weight to suppress corneal and pain reflexes such as those from tail clamping. Additional anesthesia was administered via intraperitoneal injection of sodium pentobarbital as necessary, tailored to each rat’s response, while avoiding the 10 minutes before and the 30 minutes after HS onset to prevent interference with vital sign monitoring. Anesthesia was maintained until blood was collected 2 hours after HS onset.
Cannulation and Monitoring
Under anesthesia, the right common carotid artery was cannulated using a 22G indwelling needle. This allowed for continuous monitoring of physiological variables and blood sample collection. The tail vein was cannulated for fluid administration. Core body temperature (Tc) was monitored at 10-minute intervals using a veterinary anal electronic thermometer (visual marker at 2.5 cm insertion depth). Continuous hemodynamic monitoring was achieved via a pressure transducer system (Chengdu Taimeng BL-420N) connected to the indwelling carotid arterial catheter, providing real-time measurement of MAP and heart rate (HR).
Induction of Classic Heatstroke
Post-cannulation, the rats were placed on a heating pad maintained at 43°C with circulating hot water to simulate heat stroke-inducing environmental conditions. HS onset was defined by two criteria: an increase in Tc to 42°C and a decrease in MAP by at least 10 mmHg. This dual-parameter approach provided a reliable identification of HS onset, typically occurring between 75 to 80 minutes of heat exposure. During heat exposure, rats exhibited physiological stress markers including increased respiratory rate, moistened oronasal regions, and visible perioral fluid droplets. Post-HS induction, body weight measurements were repeated, with thermal exposure-induced weight loss calculated as the difference from baseline values.
Sample Size Calculation
This study is a randomized controlled trial in which the cooling rate was used as the basis for sample size calculations. Based on preliminary experimental results, the cooling rate in the HS+WI group is approximately 5°C over 10 minutes with a standard deviation of 0.8. Assuming that a difference of 1°C in the cooling rate between any experimental group and the HS+WI group is considered significant, with a two-tailed significance level of α=0.05/6 and a power of 0.80, the required sample size for each group is calculated to be approximately 10. To ensure robustness, we have increased the sample size to 12 per group.
Experimental Groups and Cooling Methods
After successfully modeling HS, the rats were randomly divided into five groups using a random number table:
- HS with Natural Cooling (HS+C n=12): After modeling, rats were immediately removed from the heating pad and allowed to cool naturally at room temperature. This group served as the model control group to evaluate the effectiveness of the cooling measures.
- HS with Cold Water Immersion (HS+WI n=12): Immediately after modeling, the rats were immersed in 4°C cold water up to the neck for 5 minutes, then placed at room temperature. This group served as the positive control group to assess the cooling effects and impact on prognosis of different cooling methods.
- HS with Cooling Blanket (HS+CB n=12): The rats were placed supine on a custom-made 4°C CB for 10 minutes.
- HS with Cold Fluid Infusion (HS+LR n=12): Cold fluid at 4°C was administered via the tail vein, with a total volume of 4 mL per 100 g body weight, using a constant-rate infusion pump over 10 minutes. Previous studies by our team indicated that normal saline infusion could increase the risk of hypotension, acidosis, and renal damage in HS rats,25 so lactated Ringer’s solution was used in this study. To minimize the impact of environmental temperature on the cold fluid, 50 mL of fluid was drawn into a syringe wrapped with a cotton pad.
- HS with Combined Cooling (HS+CC n=12): Rats were cooled using both a CB for 10 minutes and 4°C cold fluid infusion for 10 minutes.
Preliminary experiments indicated that HS rats not receiving active cooling measures generally survived for more than 30 minutes at room temperature. Therefore, in this study, if rats in the cooling groups died within 30 minutes, they were excluded from the analysis, and additional rats were included in the same group. This approach was taken to ensure that early mortality was not due to the experimental cooling interventions. However, rats that died after 30 minutes were considered as having survived the critical period and were included in the final analysis.
Post-Cooling Monitoring and Analysis
Monitoring Protocol
Post-cooling Tc, MAP, and HR were monitored for up to 2 hours, and for surviving rats, Tc was monitored up to 6 hours post-cooling. Six rats from each group were selected for blood sample collection from the carotid artery cannula 0.5 hours post-cooling and were euthanized 2 hours post-cooling to collect heart and kidney tissues. The remaining six rats had blood samples collected at 2 hours post-cooling and were observed for survival until 24 hours post-cooling.
The experimental procedure overview can be referred to in Figure 1A.
 |
Figure 1 Experimental Procedures and Physiological Variables. (A) Overview of the experimental procedure. (B) Trend of Tc within 2 hours of cooling, with a detailed graph for the first 30 minutes. The HS+CC group exhibited the fastest cooling rate, while the HS+CB and HS+LR groups showed similar cooling rates. (C) Tc trend over 6 hours of cooling. The HS+LR group demonstrated the least subsequent cooling effect and had a low incidence of hypothermia. The HS+CC group experienced a rapid rebound to normal temperatures after early rapid cooling. (D) MAP trend within 2 hours of cooling, with a detailed graph for the first 30 minutes. The HS+LR group showed the smallest MAP drop following heatstroke onset, whereas the HS+WI group had the largest drop. The HS+LR and HS+CC groups exhibited the fastest MAP recovery, significantly higher than other groups at 20 minutes post-cooling. Abbreviations: Tc, core body temperature; MAP, mean arterial pressure. |
Analysis of Blood Samples for Organ Function and Inflammatory Markers
Arterial blood gases and electrolytes were analyzed immediately using an EDAN analyzer (Shenzhen Libang Precision Instrument Co. Ltd). Blood samples for prothrombin time (PT) and complete blood count (CBC) were processed within four hours. Other blood samples were centrifuged at 3000 rpm for 15 minutes to extract serum, which was then stored at −80°C for future analyses. Biochemical parameters such as PT, alanine aminotransferase (ALT), serum creatinine (Scr), and blood urea nitrogen (BUN) were measured using an automated biochemical analyzer (LWC400, Shenzhen Lanyun Medical Device Technology Co. Ltd). CBC was determined with a fully automated blood analyzer (Jiangxi Tekang Technology Co. Ltd). Serum levels of IL-6, TNF-α, neutrophil gelatinase-associated lipocalin (NGAL), cardiac troponin I (cTnI), and catecholamines were measured using specific ELISA kits (Wuhan Kelu Biotechnology Co. Ltd and Shanghai Fankew Industrial Co). following the manufacturers’ protocols.
Analysis of Tissue Samples for Organ Function and Inflammation
Tissue Sample Preparation
Kidney and heart tissues were rinsed, weighed, and homogenized in phosphate-buffered saline (PBS) to ensure complete disruption. The homogenates were centrifuged, and the supernatant was used for the analysis of inflammatory and damage markers.
Histological Examination
Tissue Preparation and Staining
Heart and kidney tissues were fixed, embedded in paraffin, and sectioned into 4-μm slices for histological examination. These sections were stained with hematoxylin and eosin (H&E) and examined under a microscope. A blinded semi-quantitative scoring method was used to assess organ damage.
Assessment of Cardiac Tissue Damage
Cardiac tissue damage was assessed semi-quantitatively based on Selcuk et al standards,26 examining 10 high-power fields per tissue sample. Scoring criteria included eosinophilic cytoplasm and nuclei, cytoplasmic vacuolation, congestion and hemorrhage in the interstitial small vessels, and infiltration of inflammatory cells in the interstitial space. Each field received up to 12 points, with higher scores indicating more severe damage.
Assessment of Renal Damage
Renal damage was evaluated using a scale for acute renal failure,27 examining 100 cortical tubules in at least 10 different areas per kidney. Scoring criteria included cell membrane blebs, loss of brush border, tubular epithelial flattening, cytoplasmic vacuolation, cell necrosis, tubular lumen obstruction, and interstitial edema. Each tubule was scored up to 10 points for a comprehensive assessment of renal damage.
Apoptosis Evaluation in Tissue Sections
Apoptosis in heart and kidney tissue sections was detected using a One-step TUNEL Assay Kit (HKI0011, Haoke). After fixation, embedding, sectioning, deparaffinization in xylene, and rehydration through a graded ethanol series, antigen retrieval was performed using an EDTA solution. The TUNEL reaction mixture was applied, sections incubated at 37°C, washed, and stained with DAPI for nuclear visualization. Sections were mounted and examined under a fluorescence microscope (Eclipse Ci-L, Nikon, Japan). Tissue images were captured at 10× magnification using SlideViewer microscope software. TUNEL staining was performed on heart and kidney specimens from four rats in each group. Apoptotic cells, identified by red fluorescence, were quantified in 10 randomly selected high-power fields and averaged by an observer who was blinded to the sample identities.
Outcomes
Due to the nature of the study, blinding of the intervention implementers was not feasible. However, the examiners and pathologists were blinded. Tc and MAP were measured using instruments.
Primary Outcomes
The primary outcomes of this study were the cooling effects of various cooling measures, which included:
- 10-minute Cooling Rate: This was calculated based on the Tc before cooling and the Tc at 10 minutes of cooling.
- Subsequent Cooling Effect: This was determined using the Tc at the end of cooling and the lowest Tc within 6 hours.
- Incidence of Hypothermia: Hypothermia was defined as a Tc below 33°C. The incidence of hypothermia at 2 hours and 6 hours was calculated for each group.
Secondary Outcomes
Secondary outcomes included MAP, cardiac and renal function indicators, inflammatory markers, histological evaluations, and mortality. Notably, five rats in the HS + C group died within 1 hour. For this group, only the 10-minute cooling rate and the trends of Tc, HR, and MAP within 30 minutes after cooling were calculated.
Statistical Analysis
Continuous variables were presented as mean ± standard deviation (SD). One-way analysis of variance (ANOVA) followed by Tukey’s honestly significant difference (HSD) post hoc test was applied for multi-group comparisons. Categorical variables were analyzed using Pearson’s chi-square test or Fisher’s exact test as appropriate, with post hoc pairwise comparisons adjusted by the Holm-Bonferroni method to maintain a family-wise error rate of α = 0.05. To evaluate differences in Tc, HR, and MAP trends between groups, a random effects model was used. A multivariate regression model assessed the relationship between the 10-minute cooling rate and organ function indicators, as well as inflammatory markers. Two models were established: an unadjusted model and an adjusted model that included the cooling method as a covariate to determine the independent effect of the cooling rate on outcomes. All statistical analyses were conducted using EmpowerStats (www.empowerstats.com) and GraphPad Prism 9.0.0. A P-value of less than 0.05 was considered statistically significant.
Results
Overall Situation and Mortality Rate
In the cooling groups, three rats died within 0.5 hours and were excluded from the study as per the research protocol; replacements were added to the corresponding groups. The mortality rate in the HS + C group was notably high. For this group, blood samples were collected and the rats were euthanized for organ sampling upon observing signs of imminent death rather than strictly adhering to the 0.5-hour and 2-hour time points. Specifically, seven rats in this group died: two died approximately 20 minutes after the onset of HS, three died after the 0.5-hour blood collection, and two died after the 2-hour blood collection. Consequently, the results from this group do not accurately reflect organ function and inflammation marker levels at each time point. This group serves only as a reference to evaluate the cooling effects of various measures within 30 minutes and the impact of active cooling on HS mortality. No rats in the other cooling groups died during the experiment.
Differences in Outcomes with Different Cooling Measures
Cooling Effects
As shown in Figure 1B, after leaving the heat source, Tc decreased rapidly in all groups, with the fastest rate occurring in the first 10 minutes. Upon ceasing active cooling measures, Tc continued to gradually decline, maintained a low level for a period, and then gradually increased. The HS + LR and HS + CC groups showed the fastest Tc rebound. Specifically, as presented in Table 1, the 10-minute cooling rate in each cooling group was significantly faster compared to the HS + C group (2.03 ± 0.82°C). The cooling rates in the HS + CB (4.32 ± 0.70°C) and HS + LR (4.27 ± 0.35°C) groups were slower than in the HS + WI group (4.99 ± 0.77°C), but the difference was not statistically significant, whereas the HS + CC group (6.70 ± 0.57°C) exhibited a significantly faster rate. The HS + LR group demonstrated a lower incidence and shorter duration of hypothermia at 2 and 6 hours compared to the HS + WI group (Figure 1C), with smaller subsequent cooling amplitude in the HS + LR and HS + CC groups.
 |
Table 1 Comparison of the Experimental Characteristics Between the Five Groups |
Map
After the onset of HS, MAP dropped sharply in all groups (Figure 1D). In the cooling groups, MAP reached its lowest point 5 minutes after cooling, with the HS + LR group having the highest MAP. Subsequently, MAP gradually increased, and 20 minutes post-cooling, the MAP in the HS + LR and HS + CC groups was higher than in the HS + WI and HS + CB groups (Table 1). The MAP in the HS + C group continued to decline, maintaining a lower level. These findings suggest that cooling with cold LR infusion or a combination of CB and cold LR infusion stabilizes circulatory function in HS rats.
Acid-Base Balance and Organ Function
As shown in Tables 1 and S1, the HS + CB (7.35 ± 0.06) and HS + CC (7.32 ± 0.05) groups exhibited lower pH levels at 0.5 hours post-cooling. The HS + CB group displayed signs of metabolic acidosis characterized by low base excess (BE), high lactate (LAC), and low bicarbonate (HCO3−), whereas the HS + CC group exhibited respiratory acidosis due to elevated partial pressure of carbon dioxide (PCO2). The HS + WI group exhibited significantly elevated renal function markers, including 0.5 hours Scr, BUN, and 2 hours NGAL levels, compared to both HS + LR and HS + CC groups. However, the HS + CB group had significantly higher Scr levels at 0.5 hours compared to other groups. Blood and myocardial tissue levels of cTnI were lower in the HS + LR and HS + CC groups, with significant differences in myocardial tissue cTnI. Catecholamine levels in blood and myocardial tissue were significantly lower in the HS + LR and HS + CC groups compared to the HS + WI group. No significant differences were found in ALT, platelets, and PT between groups. These results suggest that cooling with cold LR infusion or a combination of CB and cold LR infusion improves heart and kidney functions in HS rats.
Inflammatory Markers
White blood cell counts at 2 hours were lower in the HS + LR and HS + CC groups compared to the HS + WI group, with a significant difference observed in the HS + LR group. Levels of IL-6 and TNF-α in tissues and blood samples at 0.5 hours post-cooling were significantly lower in the HS + LR and HS + CC groups compared to the HS + WI and HS + CB groups. This indicates that the inflammatory responses in the HS + LR and HS + CC groups were milder than those in the other groups.
Histological Evaluation
Histopathological examination of heart tissue post-HS revealed partial degeneration and necrosis of myocardial cells, characterized by smaller nuclei, deeper staining, increased eosinophilia of the cytoplasm, vascular dilation, congestion in the myocardial interstitium, and inflammatory cell infiltration (Figure 2A). The HS + CB group exhibited the most severe lesions, with the highest pathological scores for myocardial damage (Figure 2C). Different degrees of damage were observed in the renal tissues of all groups of rats (Figure 2B). This included congestion in the capillary lumens of the glomeruli and renal tubules, infiltration of inflammatory cells, and degeneration and necrosis of the renal tubular epithelial cells. Among the cooling groups, the HS + CB group exhibited the most severe lesions, characterized by coagulative necrosis of the proximal convoluted tubules and a large number of red blood cells retained in the capillary lumens. The pathological score of the kidneys was significantly higher in the HS + CB group compared to the HS + LR and HS + CC groups (Figure 2C).
Figure 2 Continued. Figure 2 Histological Evaluation of Heart and Renal Tissue. (A) Cardiac histopathology with hematoxylin and eosin (H&E) staining. Scale bar = 50 µm. In the heart tissue of rats in the HS+C group, partial degeneration and necrosis of cardiomyocytes were observed, characterized by deeply stained nuclei, eosinophilic cytoplasm, and vacuolization in some cells (Red arrow). There was congestion in the myocardial stroma, with significant retention of red blood cells (Yellow arrow) and infiltration of inflammatory cells (Blue arrow). Similar findings were noted in the cooling groups, with the most severe lesions observed in the HS+CB group, while other groups exhibited relatively milder lesions. (B) Renal histopathology with H&E staining. Scale bar = 50 µm. Congestion was observed in the capillary lumens of the glomeruli, accompanied by infiltration of inflammatory cells (Red arrow). Tubular epithelial cells showed degeneration and necrosis, with cellular shedding (Blue arrow). Congestion was also noted in the interstitial blood vessels of the kidneys (Yellow arrow). Among the cooling groups, the HS+CB group exhibited the most severe lesions, characterized by coagulative necrosis of the proximal tubules, with visible tubular outlines but indistinct epithelial cell borders, nuclear disappearance, and cytoplasmic breakdown (Blue arrow). (C) Comparative cardiac and renal injury scoring. The HS+CB group had the highest pathological score in cardiac tissue, significantly different from the HS+LR group. The HS+CB group had the highest pathological score renal tissue, significantly different from the HS+LR and HS+CC groups. Data are presented as the mean ± SD. *P < 0.05, **P < 0.01, ***P < 0.001.

Apoptosis
Using the TUNEL assay to detect apoptosis, we observed significantly lower levels of apoptosis in the heart and kidney cells of the HS + LR and HS + CC groups compared to the HS + WI group (Figures 3). The HS + CB group had the highest apoptosis rate among the cooling groups, indicated by increased red fluorescence. This suggests that different cooling methods have varying impacts on cell death under heat stress conditions.
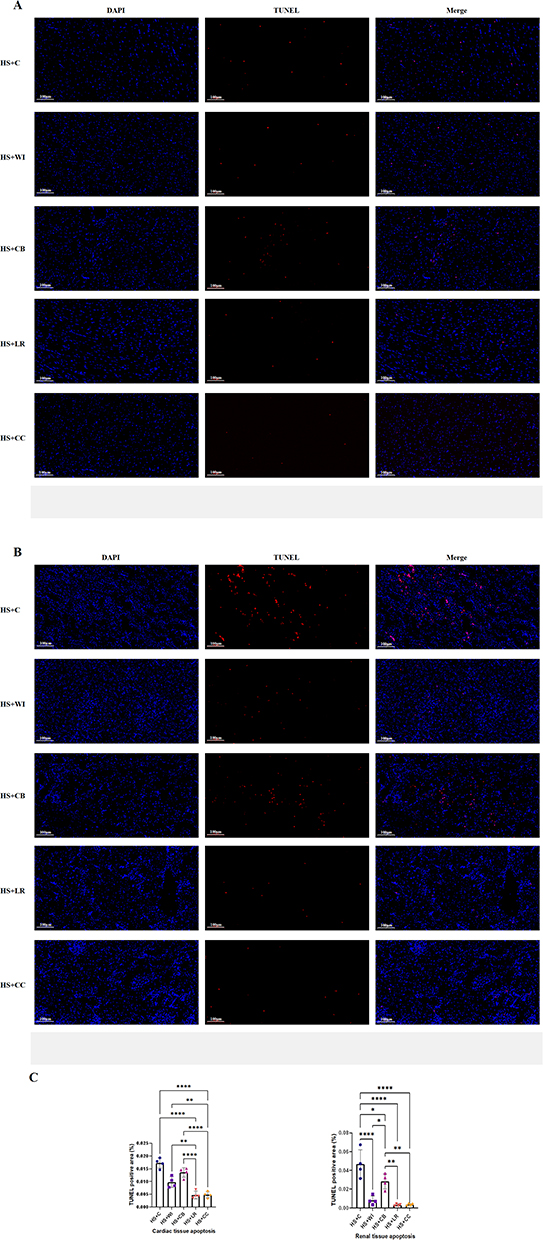 |
Figure 3 Cell Apoptosis of Heart and Renal Cortex Tissues Evaluated by TUNEL Staining. (A) Representative images of TUNEL-stained heart tissue sections. Scale bar = 100 µm. (B) Representative images of TUNEL-stained renal cortex tissue sections. Scale bar = 100 µm. (C) Statistical analysis of the TUNEL-positive area using ImageJ software. Data are presented as the mean ± SD. *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001. |
Impact of Cooling Rate on Outcomes
Univariate and multivariate logistic regression analyses evaluated the relationship between the 10-minute cooling rate and the incidence of hypothermia and test indicators. As shown in Table 2, the cooling rate significantly correlated with acid-base balance, organ function indicators, and inflammatory markers. Specifically, with the increase in cooling rate, levels of HCO3− and PCO2 significantly increased while lactate levels significantly decreased. Cardiac and renal function indicators such as Scr, NGAL, cTnI, and catecholamines, as well as inflammatory factors IL-6 and TNF-α, significantly decreased. After adjusting for cooling methods, the independent relationship between the cooling rate and these laboratory parameters (including blood gas analysis, organ function biomarkers, and inflammatory cytokines) remained statistically significant. Rapid cooling was significantly associated with the duration of hypothermia within 2 hours, but not at 6 hours. These results indicate that early rapid cooling improves heart and kidney functions and reduces inflammatory responses without causing prolonged hypothermia.
 |
Table 2 Logistic Regression of Cooling Rate for Laboratory Test Results in Rats With Heat Stroke |
Discussion
This study investigated the effects of clinical cooling methods—CB and cold fluid infusion—on cooling rate, organ function, and prognosis in CHS rats. Early rapid cooling significantly reduced the 24-hour mortality rate, improved cardiac and renal function, and reduced inflammation. Cold fluid infusion, alone or with CB, stabilized circulation and improved organ function better than CB alone. The combination of cold fluid infusion and CB achieved the fastest cooling rate.
The value of early rapid cooling in the treatment of HS has been widely recognized. In this study, the HS + C group, which did not receive active cooling measures, had a high mortality rate, with a 2-hour mortality rate of 58.3%. Pathological assessments showed more severe structural damage to the heart and kidneys and a higher rate of cell apoptosis. However, none of the groups that received active cooling measures had any deaths within 24 hours. Further analysis revealed a significant negative correlation between the 10-minute cooling rate and cardiac and renal function indicators, as well as inflammatory factor levels, and this relationship was independent of the type of cooling measure. This further confirms the crucial role of rapid cooling in the prognosis of HS. The pathophysiological mechanism of HS is complex, involving direct cellular damage caused by heat exposure and the resulting systemic inflammatory response, which plays a key role in multi-organ dysfunction.1,15 Rapid and active cooling after the onset of HS can not only quickly lower core temperature, halting heat toxicity to cells, but also improve prognosis by inhibiting the inflammatory response.
Due to factors such as blood redistribution, profuse sweating, and myocardial injury, HS patients often experience hypovolemic shock and circulatory failure. Clinical studies have found that deaths in HS patients often occur after hyperthermia and the associated circulatory failure.8 Therefore, in addition to rapid cooling, adequate fluid replacement to restore blood pressure and tissue perfusion is also crucial.28 Cold fluid infusion not only has a cooling effect but also serves to expand blood volume and replenish lost electrolytes, making it widely used clinically. This study found that MAP in each group dropped sharply after the onset of HS, but the HS + LR group experienced the smallest decline, and MAP in the HS + LR and HS + CC groups rebounded more quickly. Furthermore, the cardiac and renal function indicators in these two groups were significantly better than those in the HS + WI and HS + CB groups. This demonstrates that despite a cooling rate similar to that of CB, LR infusion is more beneficial for circulatory stability and organ function improvement, further illustrating the importance of volume resuscitation in the management of HS.
In addition to improving cardiac and renal function-related indicators, the HS + LR group also exhibited lower levels of inflammatory factors. We believe these effects are related not only to the improvement of tissue perfusion by volume resuscitation but also to the specific role of lactate components in the solution. Lactate is not only an important carbon source for cellular metabolism 2 but also a unique immunomodulatory molecule.29,30 Lactate can inhibit the synthesis and secretion of cytokines and chemokines in monocytes and macrophages induced by lipopolysaccharides,2 and it can regulate immune responses by downregulating the activation of the NLRP3 inflammasome and the production of IL-1β, thereby reducing the severity of acute inflammatory responses.31 Clinical studies have also shown that compared to saline, treatment using lactated Ringer’s solution for treating severe acute pancreatitis can significantly reduce systemic inflammation.9,32 The results of this study also indicate that the levels of inflammatory markers IL-6 and TNF-α in the myocardial tissue of rats with LR infusion (HS+LR, HS+CC) were significantly lower than in other groups. The levels of IL-6 and TNF-α are significantly correlated with the severity of hypotension and tissue damage in HS, further supporting the potential value of LR infusion in the treatment of HS.
Compared with the HS+LR group, the HS+CB group rats showed significantly more severe organ function and structural damage, which we believe is related not only to volume factors but also to the characteristics of surface cooling. Surface cooling, especially conductive cooling, requires establishing the maximum temperature gradient between the core and the skin to accelerate passive heat transfer from the core to the periphery.1 Therefore, a lower temperature of cold water or CB is needed to lower the surface temperature as much as possible. However, excessively low surface temperatures can cause peripheral vasoconstriction or shivering, thereby affecting the cooling effect and patient tolerance.33,34 Additionally, surface cooling can activate the sympathetic nervous system, increasing serum catecholamine levels, thereby exacerbating the burden on the circulatory system.35 Hence, although cold water immersion can achieve satisfactory cooling rates, it may be associated with patient intolerance and increased mortality. The results of this study also indicate that despite anesthetic drugs controlling the shivering response in rats, the cTnI and catecholamine concentrations in rats undergoing surface cooling alone (HS+WI, HS+CB) were significantly higher than in other groups, further indicating the potential impact of surface cooling on circulatory function. Moreover, shivering increases tissue oxygen consumption, which under conditions of insufficient tissue perfusion can induce metabolic acidosis.36 The insufficient cooling rate of CB necessitates prolonged cooling time to achieve better cooling effects. Prolonged local contact with cold sources exacerbates the adverse effects caused by excessively low surface temperatures, resulting in significant metabolic acidosis in the HS+CB group. The combination of slow cooling rate, insufficient tissue perfusion, and acidosis is likely to have contributed to severe structural and functional damage to the kidneys and heart in the HS+CB group.
The adverse effects caused by surface conductive cooling alone seem to be mitigated by the combined use of cold fluid infusion. The combined cooling group not only exhibited organ structural and functional indicators and inflammatory factor levels similar to the HS+LR group but also demonstrated the most optimal cooling rate. The protective effect of combined cooling on the organs of HS rats may be attributed to both rapid cooling and sufficient hydration, as these are key measures in the treatment of HS. The combined cooling group showed signs of respiratory acidosis 0.5 hours after cooling, which may be related to a decreased respiratory rate and reduced ventilation caused by rapid cooling. Since this study only collected specimens 2 hours after cooling, it was unable to assess the long-term effects of combined cooling on the body.
Rapid cooling may lead to hypothermia. This study found that compared to the cold fluid infusion groups, the two groups of rats subjected to surface cooling alone exhibited a more pronounced subsequent cooling effect, with a higher incidence and longer duration of hypothermia. External conductive cooling reduces core temperature by lowering the surface temperature. When cooling measures cease, the gradient between core temperature and surface temperature persists, resulting in a continued cooling effect and the occurrence of hypothermia. Cold fluid administered intravenously rapidly enters the central circulation, lowering the core temperature of tissues and organs. After stopping the infusion, the cold source dissipates and the body restores normal temperature through its thermoregulatory mechanisms. The combined cooling group’s body temperature dropped rapidly initially and then quickly returned to near-normal levels, possibly due to the restoration of hypothalamic thermoregulatory function from rapid cooling. This can also be validated by the faster temperature recovery in the cold water immersion group compared to the cooling blanket group.
Since this study only collected results within 2 hours after cooling, and hypothermia often occurs after 2 hours (as shown in the Figure 1C), this study cannot yet explore the impact of hypothermia on prognosis. However, studies suggest that hypothermia may increase the potential risk of adverse prognoses, such as arrhythmias and coagulopathies.15 Therefore, these results remind us to be vigilant about the subsequent cooling effects of cooling measures, especially surface cooling, to prevent hypothermia.
This study systematically evaluated the differences in cooling rate, inflammation markers, and organ structure and function between the commonly used clinical cooling methods of cold fluid infusion and CB in HS. To our knowledge, this is the first randomized controlled study to explore the utility of different cooling measures in HS rats. Active rapid cooling is the cornerstone of HS treatment; when implementing cooling measures, attention should not only be paid to the cooling rate but also to the relationship between cooling measures and prognosis. Therefore, the findings of this study provide important insights.
However, there are certain limitations to this study. This study focused on HS in rats. Although the HS response in rats is similar to that in humans, the larger surface area-to-body mass ratio in rats makes their core temperature more susceptible to environmental changes. Consequently, surface cooling methods such as CWI and CB may be more effective in rats. Furthermore, this investigation was designed within a hospital-based context focusing on clinically accessible cooling modalities including CB and cold fluid infusion. Notably, the study did not assess potential synergistic effects between CWI and concurrent cold intravenous fluid administration. Consequently, whether cold fluid infusion could attenuate certain adverse effects observed with CWI alone remains scientifically undetermined. Additionally, thermoregulation mechanisms in rats differ from those in humans, as rats are nearly incapable of cooling through evaporative heat loss from the trunk. However, the cooling methods employed in this study primarily relied on conductive mechanisms. Moreover, anesthesia can affect thermoregulation during the cooling process and suppress cardiovascular responses. Specifically, pentobarbital anesthesia may attenuate sympathetic-driven thermoregulatory responses and induce cardiovascular depression,37 potentially influencing cooling efficacy. The single intraperitoneal bolus administration further introduces variability in sustained anesthetic effects during prolonged experiments. Nonetheless, clinical guidelines recommend the use of benzodiazepines, propofol, or fentanyl to control agitation or shivering induced by cooling treatments.16 Therefore, anesthetized rats still exhibit significant similarities to clinical conditions. Additionally, this study is based on an anesthetized rat CHS model, and it remains uncertain whether the results can be generalized to EHS. EHS is more likely to cause severe renal impairment compared to CHS. Further research is needed to explore whether cold fluid infusion is more effective in mitigating EHS-induced renal impairment compared to CB alone. Further research should validate these findings in human clinical trials to clarify the value of different cooling measures in the management of HS patients, providing a basis for cooling measure choices and temperature management for clinical caregivers. Additionally, in-depth exploration of the relationship between hypothermia and prognosis will also promote further refinement of HS temperature management protocols.
Conclusion
Compared to the use of CB alone, early rapid infusion of cold fluid can improve the structure and function of the heart and kidneys in CHS rats and reduce the levels of inflammatory factors under similar cooling rates. Combining cold fluid infusion with CB can significantly accelerate the cooling rate, thereby reducing organ damage and inflammatory responses. These findings suggest that it is necessary to further study and evaluate the selection of cooling measures for HS patients to improve clinical outcomes in HS management.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study adhered to the principles outlined in GB/T 35892-20181 (General Guidelines for the Welfare of Laboratory Animals) to ensure the humane treatment of animals throughout the experiments. All protocols were approved by the Animal Ethics Committee of the Second Affiliated Hospital, Zhejiang University School of Medicine. This study was specifically approved by the Ethics and Welfare Committee of Animal Experimentation at the Second Affiliated Hospital, Zhejiang University School of Medicine (Approval ID: AIRB-2023-1677).
Acknowledgments
We thank Xiaoli Wei for the helpful professional support.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
All the authors declared no competing interests.
References
1. Bouchama A, Abuyassin B, Lehe C, et al. Classic and exertional heatstroke. Nat Rev Dis Primers. 2022;8:8. doi:10.1038/s41572-021-00334-6
2. Shapiro Y, Rosenthal T, Sohar E. Experimental heatstroke a model in dogs. Arch Intern Med. 1973;131:688–692. doi:10.1001/archinte.1973.00320110072010
3. Epstein Y, Yanovich R. Heatstroke. N Engl J Med. 2019;380:2449–2459. doi:10.1056/NEJMra1810762
4. Armstrong LE, Casa DJ, Millard-Stafford M, Moran DS, Pyne SW, Roberts WO. American college of sports medicine position stand. Exertional heat illness during training and competition. Med Sci Sports Exerc. 2007;39:556–572. doi:10.1249/MSS.0b013e31802fa199
5. Casa DJ, Armstrong LE, Kenny GP, O’Connor FG, Huggins RA. Exertional heat stroke: new concepts regarding cause and care. Curr Sports Med Rep. 2012;11:115–123. doi:10.1249/JSR.0b013e31825615cc
6. Chen L, Xu S, Yang X, Zhao J, Zhang Y, Feng X. Association between cooling temperature and outcomes of patients with heat stroke. Intern Emerg Med. 2023;18:1831–1842. doi:10.1007/s11739-023-03291-y
7. Bouchama A, Knochel JP. Heat stroke. N Engl J Med. 2002;346:1978–1988. doi:10.1056/NEJMra011089
8. Bouchama A, Dehbi M, Chaves-Carballo E. Cooling and hemodynamic management in heatstroke: practical recommendations. Crit Care. 2007;11:R54. doi:10.1186/cc5910
9. Heled Y, Rav-Acha M, Shani Y, Epstein Y, Moran DS. The “golden hour” for heatstroke treatment. Mil Med. 2004;169:184–186. doi:10.7205/milmed.169.3.184
10. Mayer S, Commichau C, Scarmeas N, Presciutti M, Bates J, Copeland D. Clinical trial of an air-circulating cooling blanket for fever control in critically ill neurologic patients. Neurology. 2001;56:292–298. doi:10.1212/wnl.56.3.292
11. Holtzclaw BJ. The febrile response in critical care: state of the science. Heart Lung. 1992;21:482–501.
12. Shapiro Y, Seidman DS. Field and clinical observations of exertional heat stroke patients. Med Sci Sports Exerc. 1990;22:6–14. doi:10.1249/00005768-199002000-00003
13. O’Connor FG, Casa DJ, Danzl DF, et al. Exertional heat illness in adolescents and adults: management and prevention. Available from: https://www.uptodate.com/contents/exertional-heat-illness-in-adolescents-and-adults-management-and-prevention. Accessed on April 7, 2025.
14. Casa DJ, McDermott BP, Lee EC, Yeargin SW, Armstrong LE, Maresh CM. Cold water immersion: the gold standard for exertional heatstroke treatment. Exerc Sport Sci Rev. 2007;35:141–149. doi:10.1097/jes.0b013e3180a02bec
15. Liu SY, Song JC, Mao HD, Zhao JB, Song Q. Expert consensus on the diagnosis and treatment of heat stroke in China. Mil Med Res. 2020;7:1. doi:10.1186/s40779-019-0229-2
16. Mechem CC, Danzl DF, Grayzel J. Severe nonexertional hyperthermia (classic heat stroke) in adults. Available from: https://www. uptodate.com/contents/severe-nonexertional-hyperthermia-classic-heat-stroke-in-adults. Accessed on April 7, 2025.
17. Bernard SA, Buist M. Induced hypothermia in critical care medicine: a review. Crit Care Med. 2003;31:2041–2051. doi:10.1097/01.CCM.0000069731.18472.61
18. Cramer MN, Gagnon D, Laitano O, Crandall CG. Human temperature regulation under heat stress in health, disease, and injury. Physiol Rev. 2022;102:1907–1989. doi:10.1152/physrev.00047.2021
19. Chang CK, Chang CP, Chiu WT, Lin MT. Prevention and repair of circulatory shock and cerebral ischemia/injury by various agents in experimental heatstroke. Curr Med Chem. 2006;13:3145–3154. doi:10.2174/092986706778742945
20. Wen Y, Huang M, Lin M, Lee C. Hypothermic retrograde jugular vein flush in heatstroke rats provides brain protection by maintaining cerebral blood flow but not by hemodilution. Crit Care Med. 2004;32:1391–1395. doi:10.1097/01.CCM.0000128568.99705.2A
21. Chen C, Hou C, Cheng K, Tian R, Chang C, Lin M. Activated protein C therapy in a rat heat stroke model. Crit Care Med. 2006;34:1960–1966. doi:10.1097/01.CCM.0000224231.01533.B1
22. Liu C, Cheng B, Lin M, Lin H. Small volume resuscitation in a rat model of heatstroke. Am J Med Sci. 2009;337:79. doi:10.1097/MAJ.0b013e31817da198
23. Cheng B, Chang C, Tsay Y, Wu T, Hsu C, Lin M. Body cooling causes normalization of cardiac protein expression and function in a rat heatstroke model. J Proteome Res. 2008;7:4935–4945. doi:10.1021/pr8000089
24. Wen Y, Huang M, Lin M, Lee C. Hypothermic retrograde jugular perfusion reduces brain damage in rats with heatstroke. Crit Care Med. 2003;31:2641–2645. doi:10.1097/01.CCM.0000094229.39473.C1
25. Chen L, Liu C, Zhang Z, Zhang Y, Feng X. Effects of normal saline versus lactated Ringer’s solution on organ function and inflammatory responses to heatstroke in rats. J Intensive Care. 2024;12:39. doi:10.1186/s40560-024-00746-y
26. Selcuk EB, Süngü M, Parlakpınar H, et al. Evaluation of the cardiovascular effects of varenicline in rats. Drug Des Devel Ther. 2015;9:5705–5717. doi:10.2147/DDDT.S92268
27. Paller MS, Hoidal JR, Ferris TF. Oxygen free radicals in ischemic acute renal failure in the rat. J Clin Invest. 1984;74:1156–1164. doi:10.1172/JCI111524
28. Leon LR, Bouchama A. Heat stroke. Compr Physiol. 2015;5:611–647. doi:10.1002/cphy.c140017
29. Certo M, Tsai C, Pucino V, Ho P, Mauro C. Lactate modulation of immune responses in inflammatory versus tumour microenvironments. Nat Rev Immunol. 2021;21:151–161. doi:10.1038/s41577-020-0406-2
30. Caslin HL, Abebayehu D, Pinette JA, Ryan JJ. Lactate is a metabolic mediator that shapes immune cell fate and function. Front Physiol. 2021;12: 688485.
31. Hoque R, Farooq A, Ghani A, Gorelick F, Mehal WZ. Lactate reduces organ injury in toll-like receptor- and inflammasome-mediated inflammation via GPR81-mediated suppression of innate immunity. Gastroenterology. 2014;146:1763–1774.
32. Wu BU, Hwang JQ, Gardner TH, et al. Lactated ringer’s solution reduces systemic inflammation compared with saline in patients with acute pancreatitis. Clin Gastroenterol Hepatol. 2011;9:710–717.e1. doi:10.1016/j.cgh.2011.04.026
33. Morgan SP. A comparison of three methods of managing fever in the neurologic patient. J Neurosci Nurs. 1990;22:19–24. doi:10.1097/01376517-199002000-00006
34. Talisman R, Lin JT, Soroff HS, Galanakis D. Gangrene of the back, buttocks, fingers, and toes caused by transient cold agglutinemia induced by a cooling blanket in a patient with sepsis. Surgery. 1998;123:592–595. doi:10.1067/msy.1998.85940
35. Axelrod P. External Cooling in the Management of Fever. Clin Infect Dis. 2000; 31:S224–S229.
36. Abou-Chebl A, DeGeorgia MA, Andrefsky JC, Krieger DW. Technical refinements and drawbacks of a surface cooling technique for the treatment of severe acute ischemic stroke. Neurocrit Care. 2004;1:131–143. doi:10.1385/NCC:1:2:131
37. Lin M. Effects of sodium pentobarbital on thermoregulatory responses in the rat. Neuropharmacology. 1981;20:693–698. doi:10.1016/0028-3908(81)90118-0
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.