")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Efficacy of Cooling Blankets for Early Temperature Management in Heat Stroke Patients: A Multicenter Retrospective Cohort Study
Authors Chen L , Jin D, Gong Z, Lu L, Zhao J, Xu S, Yang X, Zhang Y, Feng X
Received 13 February 2025
Accepted for publication 4 May 2025
Published 9 May 2025 Volume 2025:18 Pages 2629—2639
DOI https://doi.org/10.2147/JMDH.S522541
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Lan Chen,1,* Dingping Jin,1,* Zhumei Gong,2 Liyun Lu,3 Junlu Zhao,4 Shuying Xu,5 Xiaoling Yang,6 Yuping Zhang,1 Xiuqin Feng1
1Nursing Department, The Second Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 2Emergency Department, Yiwu Central Hospital, Yiwu, Zhejiang Province, People’s Republic of China; 3Emergency Department, Jinhua People’s Hospital, Jinhua, Zhejiang Province, People’s Republic of China; 4Emergency Department, Affiliated Jinhua Hospital, Zhejiang University School of Medicine, Jinhua Municipal Central Hospital, Jinhua, Zhejiang Province, People’s Republic of China; 5Emergency Department, Dongyang People’s Hospital, Dongyang, Zhejiang Province, People’s Republic of China; 6Emergency Department, Lanxi People’s Hospital, Lanxi, Zhejiang Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiuqin Feng, Nursing Department, The Second Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, People’s Republic of China, Email [email protected]
Objective: Water circulation cooling blankets are commonly used in heat stroke management, but their efficacy and safety remain insufficiently studied. This study aimed to assess the cooling effect of the cooling blanket within the first 24 hours after emergency department admission in patients with heat stroke.
Methods: Retrospective data were collected from six hospitals. The primary outcomes included body temperature at 0.5 and 2 hours post-treatment and changes in temperature during these intervals. The cooling effect was assessed using logistic regression, generalized additive mixed models, and genetic and propensity score matching. Test effectiveness was evaluated based on the non-inferiority test formula.
Results: A total of 191 patients were included, with 84 (44.0%) receiving cooling with the blanket. The mean cooling duration was 2 hours. Body temperatures at 0.5 hours were 39.80 ± 0.96 °C in the cooling blanket group versus 39.26 ± 0.94 °C in the non-cooling blanket group. At 2 hours, temperatures were 38.08 ± 1.00 °C and 37.84 ± 0.96 °C, respectively. No significant differences were found in body temperature at 0.5 hours (β, − 0.19 [95% CI, − 0.50, 0.12]; P = 0.242) or 2 hours (β, − 0.24 [95% CI, − 0.57, 0.09]; P = 0.161) between the cooling blanket and non-cooling blanket groups. Similarly, no significant differences in temperature changes at 0.5 or 2 hours were observed. After adjusting for propensity scores, no differences in temperature were found in the matching cohort. The non-inferiority criterion was met, with effectiveness scores of 1.000 at 0.5 hours and 0.998 at 2 hours.
Conclusion: The cooling blanket demonstrated no significant temperature reduction advantage compared to the non-cooling blanket group. High-quality randomized controlled trials remain necessary to further evaluate its therapeutic role in heat stroke management.
Keywords: cooling blanket, cooling effect, heat stroke, generalised additive mixed model, genetic matching
Introductions
Heat stroke (HS) is a life-threatening condition characterized by a core body temperature exceeding 40 °C, accompanied by central nervous system dysfunction and multi-organ damage.1 The degree of cellular and tissue damage in HS patients is directly related to the peak temperature and duration of hyperthermia.2,3 Rapid cooling of the core body temperature can prevent cellular injury, reverse organ dysfunction, and improve patient outcomes.1,4,5 Therefore, effective and timely cooling strategies are critical to preventing irreversible damage and reducing mortality in HS patients.6–8
Cooling techniques for HS can be broadly classified into internal and external methods. Internal cooling, such as intravascular cooling or renal replacement therapy, requires specialized equipment and expertise. It carries risks such as bloodstream infections, venous thromboembolism, and edema, limiting its immediate applicability in the management of HS.9–11 Antipyretic agents, such as aspirin and acetaminophen, are ineffective in HS due to the underlying mechanisms of fever,12,13 and may exacerbate coagulopathy and liver injury.5,8,13 As a result, external cooling methods are preferred in clinical practice.
External cooling techniques include evaporation, conduction, convection, and radiation.12 A water circulation cooling blanket (CB) utilizes conduction to regulate the cooling rate and target temperature by adjusting the blanket and body temperature settings. The maximum temperature gradient between the blanket and the patient accelerates passive heat transfer.1,14 A blanket temperature of 4 °C is recommended when using it in HS patients.15 However, when the skin temperature falls below 30 °C, cutaneous vasoconstriction and shivering may occur, potentially reducing cooling efficiency, increasing oxygen consumption, and inducing metabolic acidosis.16,17
CB have demonstrated efficacy in inducing mild hypothermia and improving neurological outcomes in critically ill patients.18 However, despite their widespread use, few studies have investigated the effectiveness of CB in early temperature management for HS patients. The effectiveness of CB specifically in managing HS remains insufficiently studied.19 This study aims to compare the cooling effects of the CB and non-CB methods during the first 24 hours post-admission to the emergency department (ED) through a non-inferiority study design. We hypothesize that the CB may not significantly improve cooling outcomes in HS patients. Since this was a retrospective study, baseline characteristics between the CB and non-CB groups were not balanced. Therefore, we employed genetic matching combined with propensity score matching to balance the observed covariates between the two groups.
Methods
Study Design and Participants
The multicentre study protocol was approved by the Ethics Committee of the Second Affiliated Hospital of Zhejiang University School of Medicine (approval 2022–0913), and it conforms to the provisions of the Declaration of Helsinki. This retrospective cohort study was carried out across six tertiary care hospitals over two summer seasons, spanning from January 1, 2021, to September 30, 2022, and has been detailed in our prior researches.20,21 The requirement for informed consent was waived because the data were anonymous, and the STROBE guidelines for cohort studies were applied.
Only adult patients with HS who were admitted to the ED were enrolled. According to the expert consensus in China,15 HS was defined as cases subjected to high-intensity exercise or exposed to high temperature and high humidity environments, with at least one of the following clinical presentations: 1) core temperature above 40 °C; 2) functional impairment of the central nervous system; 3) functional impairment of multiple organs (≥ 2); and 4) severe coagulopathy or disseminated intravascular coagulation (DIC).
Exclusion criteria for this study included patients transferred from another hospital with body temperature <39.5 °C, those who required immediate cardiopulmonary resuscitation or had other serious diseases, such as severe trauma or massive cerebral haemorrhage, those who were discharged from the ED within 4 h, and those with unavailable outcomes.
Data Collection
We extracted clinical data, including demographic variables, symptoms and signs at presentation, HS type, underlying comorbidities, vital signs, Glasgow Coma Scale score, and in-hospital mortality. The main laboratory indicators of organ function obtained at ED admission were collected, including neutrophils, platelets, creatinine, alanine aminotransferase, troponin I, prothrombin time (PT), pH, partial pressure of carbon dioxide (PCO2), and base excess (BE).
We carefully reviewed all patient orders and nursing records to extract information on CB use, including the time it was started and ended, the setting temperature of the blanket, and the target body temperature. Information on other cooling techniques was also collected, such as evaporation, cold pack, iced gastric lavage, iced bladder lavage, intravenous injection of cold saline, and use of nonsteroidal drugs. Additionally, the use of a lytic cocktail was confirmed. We also focused on information on shivering during cooling in the nursing record sheet. Since all participating EDs were equipped with standardized air-conditioning systems maintaining ambient temperatures at 20–24 °C and relative humidity at 55–65%, we did not investigate the potential influence of outdoor atmospheric conditions on cooling efficacy.
Outcomes
The primary outcome of this study was body temperature at 0.5 and 2 h, as well as changes in temperature between these time points. In the six hospitals included in this study, patient body temperature was measured using infrared ear thermometry. Therefore, the intervals for temperature measurement and recording were inconsistent. In this study, body temperature at 0.5 h and 2 h refers to readings obtained 25−35 min and 100−140 min after ED admission, respectively. The 0.5 h and 2 h temperature reduction were calculated based on the initial temperature at admission to ED and the temperature at 0.5 h and 2 h, respectively. The lowest temperature within 24 hours was also obtained from electronic medical records.
Statistical Analysis
Baseline characteristics, laboratory results, cooling methods, and patient outcomes were summarized using descriptive statistics. Continuous variables were presented as mean ± standard deviation for normally distributed data (compared with Student’s t-test) or median (interquartile range) for non-normally distributed data (compared with the Mann–Whitney U-test). Categorical variables were reported as numbers (percentages) and analyzed using the chi-squared test or Fisher’s exact test, as appropriate.
To evaluate the cooling effect of CB, we used regression analysis to compare body temperatures at 0.5 and 2 hours between the CB and non-CB groups. Results were presented as β coefficients with 95% confidence intervals (CIs). Patients who did not receive CB within 0.5 hours were classified as part of the non-CB group for the 0.5-hour analysis, and similarly, those who received CB cooling after 2 hours were included in the non-CB group for the 2-hour analysis. Adjusted models accounted for hospital site, baseline characteristics, HS type, and cooling methods. Additionally, initial body temperature at admission was included as a covariate since subsequent body temperatures were strongly influenced by admission values. Furthermore, we performed comprehensive sensitivity analyses stratified by both age categories (<65≦65, >65 years) and HS classification to evaluate the robustness of our findings across clinically relevant subgroups.
To further explore body temperature trends within the first 2 and 24 hours after admission, a generalized additive mixed model (GAMM) was applied. GAMM is well-suited for longitudinal data analysis due to its flexibility in modeling time-dependent effects, ability to handle missing data, and adaptability to unbalanced and unevenly spaced time points.22
The baseline data revealed an imbalance between the CB and non-CB groups, with the CB group presenting more severe conditions. To adjust for confounders and achieve covariate balance, genetic matching based on estimated propensity scores was applied. Hospital site, cooling methods, baseline characteristics, admission vital signs, and laboratory results were included as covariates to calculate propensity scores for each patient. A 1:1 repeated genetic matching algorithm was used to balance both covariates and propensity scores between the two groups. Genetic matching, a robust multivariate method, employs an evolutionary search algorithm to determine optimal covariate weights and does not solely rely on propensity scores, though incorporating them significantly enhances its performance.23 After matching, logistic regression was conducted to assess differences in outcomes, with propensity scores included as covariates in adjusted models.
To evaluate the effectiveness of temperature differences between the two groups, a non-inferiority test was performed. In this cohort, the CB group showed mean temperature reductions of 1.11 °C at 0.5 hours and 2.83 °C at 2 hours. Based on the principle that non-inferiority margins should preserve at least 50% of the control group’s therapeutic effect and considering the critical requirement for rapid cooling in HS patients, the non-inferiority margin was conservatively defined as the temperature in the non-CB group not exceeding that of the CB group by more than 0.5 °C at both 0.5-hour and 2-hour timepoints, representing 45% of the CB group’s 0.5-hour cooling effect and 18% of its 2-hour effect while meeting clinical needs for early rapid temperature management. This margin was selected to ensure both statistical rigor and clinical relevance in evaluating cooling efficacy between the two treatment approaches.
All statistical analyses were performed using EmpowerStats (www.empowerstats.com) and R (version 3.5.1, www.r-project.org). Statistical significance was set at a two-tailed P-value < 0.05.
Results
Demographic and Clinical Characteristics of HS Patients
Initially, 338 patients were recruited; 191 patients remained after applying the exclusion criteria (Figure 1). Table 1 shows the median age, 66.24 ± 14.96 years, and 76 (39.79%) were women. Overall, 80 (41.88%) patients exhibited classic HS (CHS) and 111 (58.12%) exertional HS (EHS). Hypertension (26.18%) was the most common comorbidity, followed by mental disorders (14.14%), diabetes (7.85%), and chronic heart disease (7.85%). The median body temperature and Glasgow Coma Scale score at admission were 40.76 ± 0.79 °C and 8.26 ± 4.11, respectively. In this study, 24 patients (12.57%) experienced in-hospital mortality.
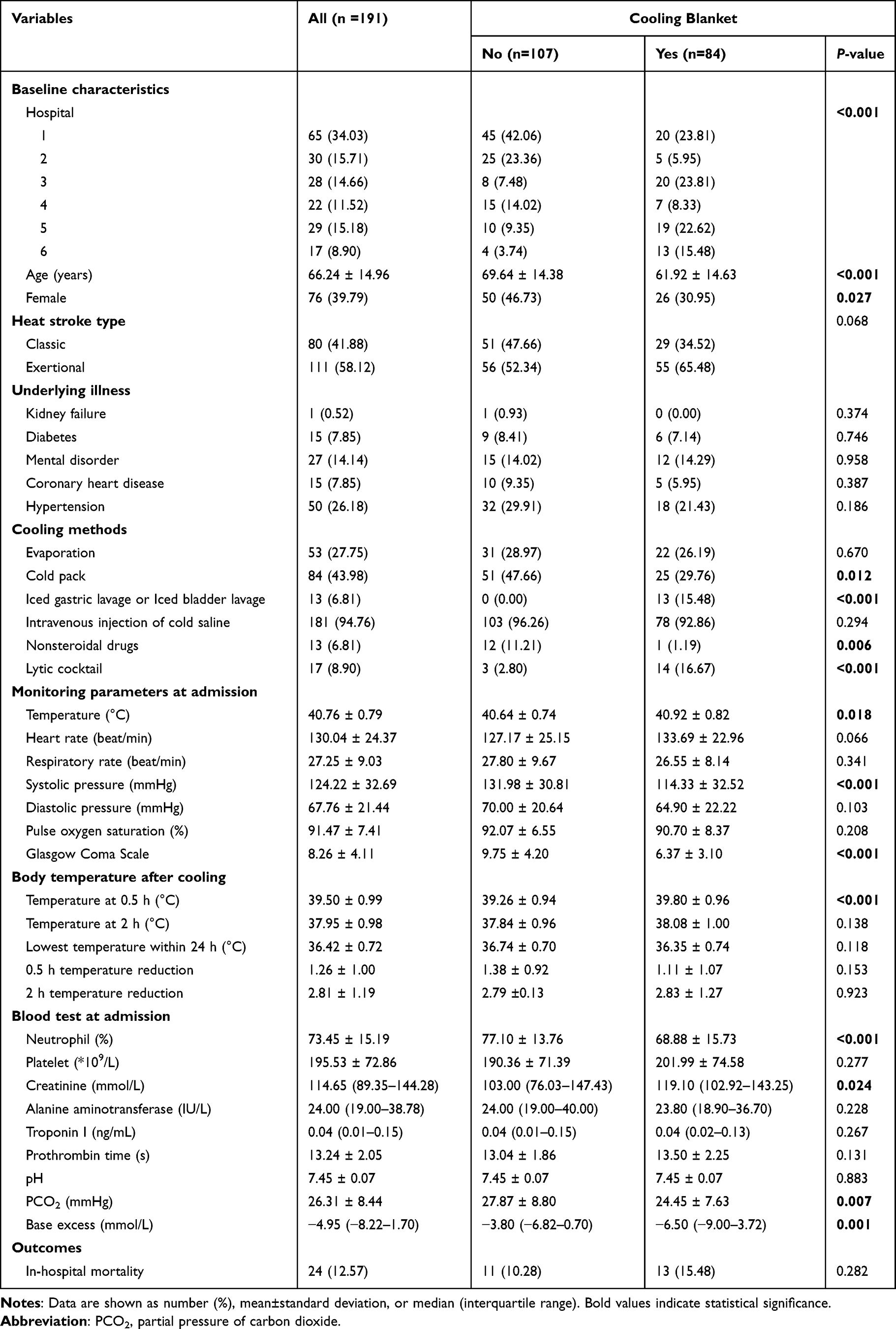 |
Table 1 Patient Baseline Characteristics, Cooling Methods and Main Outcomes |
 |
Figure 1 Flow chart. Initially, 338 patients were recruited; 191 patients remained after applying the exclusion criteria. Abbreviations: ED, emergency department; HS, heat stroke. |
Cooling Methods
Among the cooling methods, 94.76% of patients received cold fluid infusion. Cold packs were used by 84 patients (43.98%). Other methods include evaporation (27.75%) and ice-cold gastric and bladder lavages (6.81%). Nonsteroidal drugs were administered to 13 patients (6.81%), although they were not recommended. A lytic cocktail comprising chlorpromazine, promazine, and meperidine was used in 17 (8.90%) patients to achieve vasodilation and suppress shivering.24
Combined with other cooling techniques, 84 patients (44.0%) were cooled using CB. There were 61 (80.26%) patients who underwent CB cooling within 0.5 h, 12 (15.79%) between 0.5 h and 2 h, and three (3.95%) patients after 2 h. Eleven patients had no record of CB discontinuation. The longest time of CB cooling was 31 h, and the lowest body temperature at stopping CB was 35.6 °C. The mean CB time was 2.00 (1.30−3.25) h. CB use differed significantly among hospitals. Compared to the non-CB group, the CB group was younger and had a higher initial body temperature, lower systolic pressure, and lower Glasgow Coma Scale scores (P <0.05). Furthermore, the CB group had a lower neutrophil count, PCO2, and BE and higher creatinine levels (P <0.05). In total, 29 patients had records of shivering, among whom 18 manifested this symptom: 15 with CB cooling.
Cooling Effect
The cooling effect of CB in the ED at 0.5 h and 2 h was revealed by univariate and multivariate regression (Table 2). There was no difference in body temperature at 0.5 h between the non-CB and CB groups in univariate analysis (β, 0.19 [95% CI, −0.12, 0.49]; P = 0.230). In the multivariate model, the difference between these two groups was also insignificant (β, −0.19 [95% CI, −0.50, 0.12]; P = 0.242). This phenomenon existed in the 0.5 h temperature reduction (β, 0.19 [95% CI, −0.12, 0.50]; P = 0.242), the body temperature at 2 h (β, −0.24 [95% CI, −0.57, 0.09]; P = 0.161), and 2 h temperature reduction (β, 0.24 [95% CI, −0.09, 0.57]; P = 0.161). Notably, subgroup analyses demonstrated consistent cooling rates between CB and non-CB groups across different age strata and HS types (exertional vs classic), with no statistically significant differences observed (Table S1).
 |
Table 2 The Difference in Body Temperature After Cooling Between the Cooling Blanket Group and Non-Cooling Blanket Group |
GAMM (Table S2) showed that the body temperature within the first 2 and 24 h significantly decreased with time across all patients and subgroups. No significant difference was observed in the cooling rate within the first 2 h between the non-CB and CB groups (β, −0.06 [95% CI, −0.24, 0.18]; P= 0.4981) (Figure 2A). However, following the initial rapid cooling phase, the body temperature of the CB group dropped and was maintained at a lower temperature (β, −0.02 [95% CI, −0.04, −0.01]; P = 0.005) (Figure 2B).
 |
Figure 2 Association between body temperature within 2 h and 24 h and CB using the GAMM. (A) Temperature trends during first 2 hours. Body temperature decreased rapidly in both groups. Key observations: - No statistically significant differences were observed in temperature reduction between the two groups at either the 0.5-hour or 2-hour time points (all P > 0.05). - The impact of body temperature within the first 2 h was not significantly affected by the CB type (P for interaction = 0.498). (B) 24-hour temperature trajectories. Non-CB group: Temperature reached its lowest point at 5–10 hours, with slight rebound and stabilization thereafter. CB group: Temperature showed a sustained, slow decline, with the maximum intergroup difference at 15 hours and persistently lower temperatures at 24 hours. Key findings: - The impact of body temperature within the first 24 h was significantly affected by the CB type (P for interaction = 0.005). - The body temperature within the first 24 h decreased by 0.02°C (95% CI: −0.01–-0.04) every hour in the CB group compared to that in the non-CB group. X-axis: Time after cooling initiation (hours). Y-axis: Body temperature (°C). Abbreviations: GAMM, generalized additive mixed model; CI, confidence interval. |
Propensity score and genetic matching were used to determine the optimal balance between the CB and non-CB groups. In total, 150 pairs were matched. Table S3 shows the baseline clinical, laboratory characteristics, and cooling methods of the matched cohorts. Apart from hospital, gender, platelet, and iced gastric lavage or iced bladder lavage, all other confounders were similar in the matched cohort. Logistic regression analysis was performed to assess cooling effect of CB. In univariate analysis, no significant difference was observed in the body temperature at 0.5 h (β, 0.25 [95% CI, −0.08, 0.58]; P = 0.145) and 2 h (β, −0.10 [95% CI, −0.44, 0.23]; P = 0.553) between the non-CB and CB groups (Table 3). After adjusting for propensity-score, this phenomenon existed.
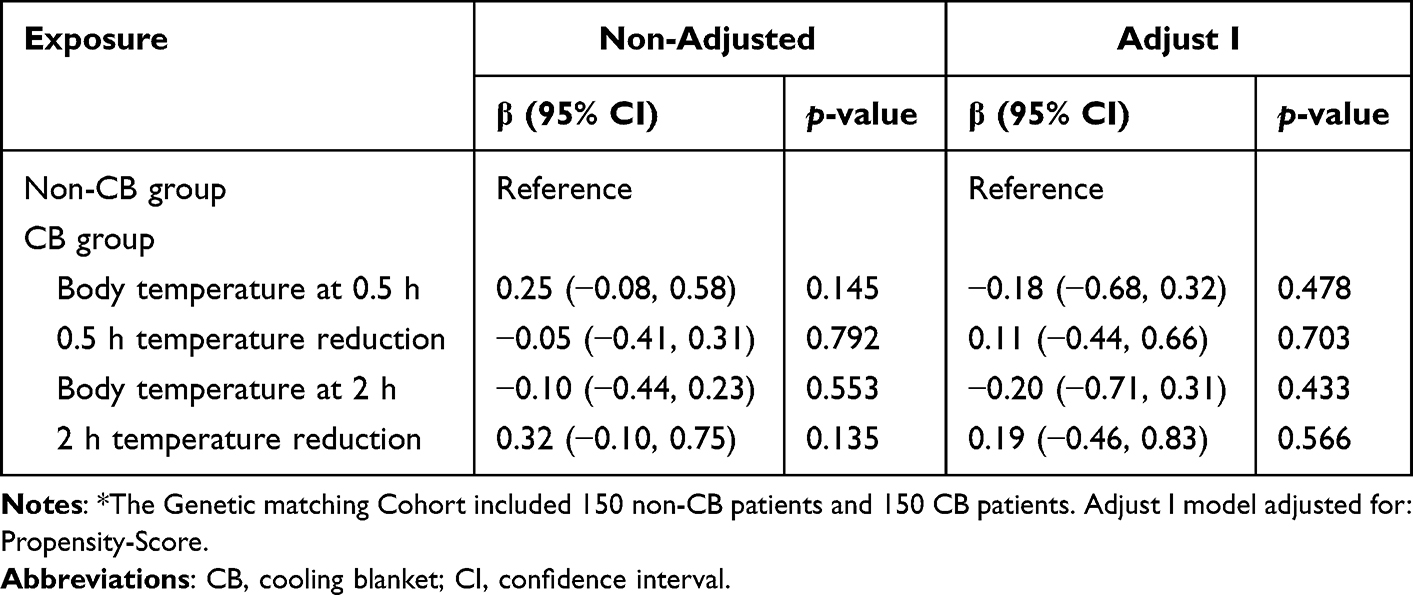 |
Table 3 Logistic Regression of Cooling Blanket with Outcomes in the Genetic Matching Cohort* |
Based on the non-inferiority test formula, the effectiveness of the test was evaluated. The non-inferiority criterion was met, with effectiveness scores of 1.000 at 0.5 hours and 0.998 at 2 hours, based on the criterion that the non-blanket group’s temperature should not exceed 0.5°C higher than the blanket group.
Discussion
In this retrospective multicenter study of HS patients, no statistically significant difference in body temperature at 0.5 and 2 hours was observed between the CB and non-CB groups. However, following the initial rapid cooling phase, body temperatures in the CB group remained consistently lower. Even after genetic matching, CB use did not demonstrate a significant advantage over non-CB methods. These findings suggest that while CB may contribute to sustained cooling—such as their role in inducing hypothermia and improving neurological outcomes in critically ill patients18 —their effectiveness in achieving rapid early cooling for HS warrants further investigation.
Although cold-water immersion is widely regarded as the preferred cooling method for EHS,25 its use may hinder critical medical interventions, such as monitoring, fluid administration, and resuscitation. Consequently, it may be unsuitable for patients with urgent medical needs, such as impaired consciousness, airway compromise, seizures, or hemodynamic instability.26 Furthermore, in CHS, cold-water immersion often induces severe shivering and agitation, which are linked to higher mortality rates.7,26 Currently, no conclusive evidence supports the superiority of any specific cooling method for the early management of heat stroke in emergency settings. Instead, the choice of cooling technique often depends on factors such as the patient’s condition, equipment availability, and staff familiarity with the chosen method.7
In ED, cooling techniques are often combined to achieve optimal results.16 Rapid infusion of 4 °C saline, whether prehospital or in the ED, is a convenient and effective cooling method.5,19 Besides facilitating heat dissipation, cold-saline infusion helps restore blood pressure and tissue perfusion, promoting hemodynamic stability. Consequently, it is frequently included in comprehensive treatment strategies, particularly for EHS patients who present with dehydration.27 In our study, cold-saline infusion was the most commonly employed cooling method, with no other in vivo cooling techniques used in this cohort.
While applying ice packs to areas such as the axilla, neck, and groin is simple, its cooling effect is often minimal or even negligible.19,28 Spraying the body with cold water while simultaneously fanning to enhance evaporative heat loss is a non-invasive, effective, and well-tolerated approach.1 Conversely, gastric and bladder lavage, though capable of reducing body temperature, are labor-intensive for nursing staff and associated with complications such as gastric distension and aspiration risk,17 limiting their practicality in clinical settings.
The CB was the most commonly used external cooling method in our cohort. However, no statistically significant difference was observed in the body temperature within the first 2 h between the non-CB and CB groups. The results were unchanged both in the GAMM and in matched cohort. This may possibly be due to delay in the start time of the device, poor contact between the CB surface and the skin, and shivering.
Patients with HS mostly explode during heatwaves, causing great personnel and resource pressure in the ED.1 Caregivers often choose easier measures such as cold fluid infusion and ice packs to cool their patients first. Using a CB often requires staff cooperation, especially when placing a cold blanket on the patient’s back. On reviewing the nursing record sheet to obtain information on CB, we found that about 20% of patients in the CB group were not commenced within 0.5 h. Even for those with a CB record within 0.5 h, the timing of true CB initiation was also uncertain. After the CB starts, time is required for the blanket temperature to drop to the set target. Only after that can the maximum possible temperature gradient between the patient and the blanket surface be established14 and have a cooling effect. Therefore, the benefits of using CB may be offset by the time required to start devices.1 Additionally, delayed CB use may be related to the availability of equipment and staff familiarity with it.7
Poor contact between the CB and the skin may also contribute to its limited cooling effectiveness.29 To optimize cooling, Hoedemaekers et al9 applied two CBs—one under and one over the patient—along with a smaller blanket under the head. In contrast, in our cohort, only a single blanket was placed under the back, accompanied by a cold cap encircling the head. Additionally, healthcare workers often place a sheet between the blanket and the skin to prevent skin damage, although corresponding notes were not observed in the nursing care records. To avoid contamination from the patient’s excrement, cotton pads are sometimes placed under the buttocks, further reducing the blanket’s contact area. Another challenge arises from the frequent need to reposition patients for cleaning, as diarrhea is a common symptom in HS patients and often persists until cooling is complete.1 These factors collectively hinder the consistent application of CBs, reducing their potential efficacy as an external cooling method.
When using conductive cooling methods, it is essential to establish the largest possible temperature gradient between the body core and skin.1,30 To achieve rapid cooling, a lower blanket temperature must be set. However, cold signals from the skin stimulate the dorsomedial portion of the posterior hypothalamus—the primary motor center for shivering—activating anterior motor neurons. This leads to increased skeletal muscle tone, heightened sensitivity of the spindle stretch reflex, and subsequent convulsions or shivering.14,31 During cooling with a CB, the incidence of shivering has been reported to range from 57% to 100%.31–33 In our cohort, 29 patients had records of shivering, with 18 displaying the symptom: 15 were cooled using a CB, while the other three used ice packs or evaporative cooling methods. Shivering not only generates additional body heat, counteracting the reduction of core temperature,17,33 but it also causes significant discomfort and reduces patient tolerance for cooling interventions.31,34 Moreover, vasoconstriction triggered by the activation of cold receptors in the skin can further impede effective cooling.14
In addition to being no more effective than other cooling techniques, CB treatment is associated with greater temperature fluctuations and more frequent rebound hypothermia episodes.30 The large temperature gradient between the core and peripheral body regions created by CB use may increase the risk of overcooling.35 In our cohort, patients in the CB group experienced lower body temperatures for prolonged periods (within 24 hours). In some cases, CB cooling was not discontinued until hypothermia had occurred. This may be due to heavy workload pressures that hinder regular temperature assessments after initial rapid cooling or a lack of staff awareness regarding hypothermia prevention. We attempted to identify the optimal body temperature for stopping CB cooling; however, only 73 patients who used CB had documented cooling cessation times and corresponding body temperatures. While the precise definition of hypothermia and its adverse effects in HS patients remain unclear,4 it is evident that proper guidelines are needed to titrate cooling effectively and maintain body temperature within an optimal range.36
To the best of our knowledge, this is the first study to evaluate the cooling effect of CB using real-world data. Given the more severe baseline conditions observed in the CB group, we utilized a genetic matching-incorporated propensity score to adjust for unbalanced confounders. Genetic matching offers superior covariate balance and is more robust compared to commonly used alternative propensity score methods.37 Although this study was not conducted as a randomized controlled trial, we believe its findings offer valuable insights into the cooling efficacy of CB in facilitating rapid early cooling for HS.
Despite its strengths, this study has several limitations. First, while based on real-world data and supported by genetic matching, unmeasured or unobserved confounders may still exist. Second, data on CB temperature settings and the incidence of shivering were limited, preventing a precise evaluation of the relationship between CB use, blanket temperature, and shivering. Third, body temperature in this study was measured using infrared ear thermometers, which might differ slightly from core body temperature. In the CB group, the temperature might have been lower than the core temperature during the cooling period due to the use of the cold cap. However, this potential discrepancy likely increased the reliability of our results by reducing the risk of overestimation. Finally, the absence of standardized protocols for CB use in HS patients at the study hospitals may have impacted its efficacy. Optimizing CB application timing, defining target cessation temperatures, and ensuring consistent and adequate skin contact could improve cooling efficiency and reduce adverse outcomes.
Conclusions
In summary, no significant difference in body temperature was observed between the non-CB and CB groups at 0.5 h and 2 h. However, following the initial rapid cooling phase, the body temperature in the CB group remained consistently lower. Considering the challenges associated with CB use and its observed cooling effects, future high-quality randomized controlled trials—including both clinical and animal studies—should investigate standardized CB protocols to comprehensively evaluate cooling efficacy, determine optimal treatment duration and discontinuation thresholds, and clarify CB’s role in early HS temperature management. Such studies would provide evidence-based guidance for EDs selecting cooling strategies.
Abbreviations
HS, heat stroke; CB, cooling blanket; ED, emergency department; DIC, disseminated intravascular coagulation; PT, prothrombin time; PCO2, partial pressure of carbon dioxide; BE, base excess; CIs, confidence intervals; GAMM, generalised additive mixed model; CHS, classic heat stroke; EHS, exertional heat stroke.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the Second Affiliated Hospital of Zhejiang University School of Medicine (approval 2022-0913). The requirement for informed consent was waived because the data were anonymous.
Acknowledgments
Lan Chen and Dingping Jin are co-first authors for this study.
Funding
This study was funded by Research Fund of Zhejiang Provincial Health Commission.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Bouchama A, Abuyassin B, Lehe C, et al. Classic and exertional heatstroke. Nat Rev Dis Primers. 2022;8(1):8. doi:10.1038/s41572-021-00334-6
2. Bynum GD, Pandolf KB, Schuette WH, et al. Induced hyperthermia in sedated humans and the concept of critical thermal maximum. Am J Physiol. 1978;235(5):R228–36. doi:10.1152/ajpregu.1978.235.5.R228
3. Buckley IK. A light and electron microscopic study of thermally injured cultured cells. Lab Invest. 1972;26(2):201–209.
4. Laitano O, Leon LR, Roberts WO, Sawka MN. Controversies in exertional heat stroke diagnosis, prevention, and treatment. J Appl Physiol. 2019;127(5):1338–1348. doi:10.1152/japplphysiol.00452.2019
5. Shapiro Y, Seidman DS. Field and clinical observations of exertional heat stroke patients. Med Sci Sport Exer. 1990;22(1):6–14.
6. Bouchama A, Knochel JP. Heat stroke. New Engl J Med. 2002;346(25):1978–1988. doi:10.1056/NEJMra011089
7. Bouchama A, Dehbi M, Chaves-Carballo E. Cooling and hemodynamic management in heatstroke: practical recommendations. CRIT CARE. 2007;11(3):R54. doi:10.1186/cc5910
8. Heled Y, Rav-Acha M, Shani Y, Epstein Y, Moran DS. The “golden hour” for heatstroke treatment. Mil Med. 2004;169(3):184–186. doi:10.7205/milmed.169.3.184
9. Hoedemaekers CW, Ezzahti M, Gerritsen A, van der Hoeven JG. Comparison of cooling methods to induce and maintain normo- and hypothermia in intensive care unit patients: a prospective intervention study. Crit Care. 2007;11(4):R91. doi:10.1186/cc6104
10. Sonder P, Janssens GN, Beishuizen A, et al. Efficacy of different cooling technologies for therapeutic temperature management: a prospective intervention study. Resuscitation. 2018;124:14–20. doi:10.1016/j.resuscitation.2017.12.026
11. Wang X, Moy BT, Hiendlmayr BJ, Krainski F, Duvall WL, Fernandez AB. Intravascular Cooling Catheter-Related Venous Thromboembolism After Hypothermia: a Case Report and Review of the Literature. Ther Hypothermia Tem. 2018;8(2):117–120.
12. Mayer S, Commichau C, Scarmeas N, Presciutti M, Bates J, Copeland D. Clinical trial of an air-circulating cooling blanket for fever control in critically ill neurologic patients. Neurology. 2001;56(3):292–298. doi:10.1212/wnl.56.3.292
13. Holtzclaw BJ. The febrile response in critical care: state of the science. Heart Lung. 1992;21(5):482–501.
14. Talisman R, Lin JT, Soroff HS, Galanakis D. Gangrene of the back, buttocks, fingers, and toes caused by transient cold agglutinemia induced by a cooling blanket in a patient with sepsis. Surgery. 1998;123(5):592–595. doi:10.1067/msy.1998.85940
15. Liu SY, Song JC, Mao HD, Zhao JB, Song Q. Expert consensus on the diagnosis and treatment of heat stroke in China. Military Med Res. 2020;7(1):1.
16. Leon LR, Bouchama A. Heat stroke. Compr Physiol. 2015;5(2):611–647. doi:10.1002/cphy.c140017
17. Abou-Chebl A, DeGeorgia MA, Andrefsky JC, Krieger DW. Technical refinements and drawbacks of a surface cooling technique for the treatment of severe acute ischemic stroke. Neurocrit Care. 2004;1(2):131–143. doi:10.1385/NCC:1:2:131
18. Bernard SA, Buist M. Induced hypothermia in critical care medicine: a review. Crit Care Med. 2003;31(7):2041–2051. doi:10.1097/01.CCM.0000069731.18472.61
19. Gaudio FG, Grissom CK. Cooling Methods in Heat Stroke. J Emerg Med. 2016;50(4):607–616. doi:10.1016/j.jemermed.2015.09.014
20. Chen L, Lu L, Fang Y, et al. Glasgow Coma Scale on admission as predictor of neurological sequelae at discharge and acute respiratory failure in patients with heatstroke. Postgrad Med J. 2023;99(1178):1237–1245. doi:10.1093/postmj/qgad071
21. Chen L, Zhao J, Lu L, et al. Association between normal saline infusion volume in the emergency department and acute kidney injury in heat stroke patients: a multicenter retrospective study. Renal Failure. 2024;46(1):1.
22. Gueorguieva R, Krystal JH. Move over ANOVA: progress in analyzing repeated-measures data and its reflection in papers published in the Archives of General Psychiatry. Arch Gen Psychiatry. 2004;61(3):310–317. doi:10.1001/archpsyc.61.3.310
23. Alexis D, Jasjeet SS. Genetic matching for estimating causal effects: a general multivariate matching method for achieving balance in observational studies. Rev Econ Stat. 2013;95(3):1.
24. Dundee JW, Clarke RS. Pharmacology of Hypothermia. Int Anesthesiol Clin. 1964;2:857–872. doi:10.1097/00004311-196408000-00013
25. O’Connor FG, Casa DJ, Danzl DF, et al. Exertional Heat Illness in Adolescents and Adults: Management and Prevention. 2023. (Accessed February 2024).
26. Mechem CC, Danzl DF, Grayzel J. Severe Nonexertional Hyperthermia (Classic Heat Stroke) in Adults. 2024. (Accessed February 2024).
27. Lipman GS, Gaudio FG, Eifling KP, Ellis MA, Otten EM, Grissom CK. Wilderness Medical Society Clinical Practice Guidelines for the Prevention and Treatment of Heat Illness:. 2019 Update. Wild Environ Med. 2019;30(4):S33–46.
28. Kielblock AJ, Van Rensburg JP, Franz RM. Body cooling as a method for reducing hyperthermia. An evaluation of techniques. Samj S Afr Med J. 1986;69(6):378–380.
29. Mayer SA, Kowalski RG, Presciutti M, et al. Clinical trial of a novel surface cooling system for fever control in neurocritical care patients. Crit Care Med. 2004;32(12):2508–2515. doi:10.1097/01.ccm.0000147441.39670.37
30. O’Donnell J, Axelrod P, Fisher C, Lorber B. Use and effectiveness of hypothermia blankets for febrile patients in the intensive care unit. Clin Infect Dis. 1997;24(6):1208–1213. doi:10.1086/513660
31. Morgan SP. A comparison of three methods of managing fever in the neurologic patient. J Neurosci Nurs. 1990;22(1):19–24. doi:10.1097/01376517-199002000-00006
32. Abbey J, Andrews C, Avigliano K, et al. A pilot study: the control of shivering during hypothermia by a clinical nursing measure. J Neurosurg Nurs. 1973;5(2):78–88. doi:10.1097/01376517-197312000-00007
33. Shah NG, Cowan MJ, Pickering E, et al. Nonpharmacologic approach to minimizing shivering during surface cooling: a proof of principle study. J Crit Care. 2012;27(6):741–746.
34. Manthous CA, Hall JB, Olson D, et al. Effect of cooling on oxygen consumption in febrile critically ill patients. Am J Resp Crit Care. 1995;151(1):10–14.
35. Rajek A, Greif R, Sessler DI, Baumgardner J, Laciny S, Bastanmehr H. Core cooling by central venous infusion of ice-cold (4°C and 20°C) fluid: isolation of core and peripheral thermal compartments. Anesthesiology. 2000;93(3):629–637. doi:10.1097/00000542-200009000-00010
36. Merchant RM, Abella BS, Peberdy MA, Soar J, Ong ME, Schmidt GA, et al. Therapeutic hypothermia after cardiac arrest: unintentional overcooling is common using ice packs and conventional cooling blankets. Crit Care Med. 2006;34(12 Suppl). doi:10.1097/01.CCM.0000246016.28679.36
37. Radice R, Ramsahai R, Grieve R, Kreif N, Sadique Z, Sekhon JS. Evaluating treatment effectiveness in patient subgroups: a comparison of propensity score methods with an automated matching approach. Int J Biostat. 2012;8(1):14. doi:10.1515/1557-4679.1382
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.