")
Back to Journals » Journal of Inflammation Research » Volume 17
Elevated Serum HMGB1 Levels and Their Association with Recurrence of Acute Ischaemic Stroke
Authors Shen L, Yang J, Zhu Z, Li W, Cui J, Gu L
Received 8 May 2024
Accepted for publication 21 September 2024
Published 30 September 2024 Volume 2024:17 Pages 6887—6894
DOI https://doi.org/10.2147/JIR.S477415
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Liping Shen, Jiangsheng Yang, Zufu Zhu, Weizhang Li, Junyou Cui, Lingyun Gu
Department of Neurology, Jiangyin Hospital Affiliated to Nantong University, Jiangyin, Jiangsu, People’s Republic of China
Correspondence: Lingyun Gu, Department of Neurology, Jiangyin Hospital Affiliated to Nantong University, 163 Shoushan Road, Jiangyin, Jiangsu, 214400, People’s Republic of China, Tel/Fax +86 13915313817, Email [email protected]
Purpose: The study aimed to investigate the correlation between baseline serum levels of high mobility group box 1 (HMGB1) and the recurrence of acute ischemic stroke (AIS).
Patients and Methods: A total of 544 AIS patients were enrolled and followed up monthly. Serum HMGB1 levels were measured using enzyme-linked immunosorbent assay (ELISA). The primary endpoint was the first recurrence of AIS.
Results: During a median follow-up period of 43 months, 62 of the 544 AIS patients experienced a recurrence. Both HMGB1 levels and national institute of health stroke scale (NIHSS) scores were significantly higher in the recurrence group compared to the no-recurrence group (p< 0.05). According to the receiver operating characteristic curve analysis, the combination (0.855, 95% CI: 0.800– 0.911) of HMGB1 (0.745, 95% CI: 0.663– 0.826) and NIHSS (0.822, 95% CI: 0.758– 0.886) had a higher value for predicting AIS recurrence than either of them (p< 0.05). Kaplan-Meier analyses demonstrated that the cumulative survival without AIS recurrence was significantly lower in patients in the high HMGB1 level group than in the low HMGB1 level group (p< 0.05). The multifactorial Cox analyses indicated that elevated baseline serum HMGB1 levels (HR: 7.489, 95% CI:4.383– 12.795) were a highly effective predictor of recurrence in AIS.
Conclusion: Elevated baseline serum HMGB1 levels were found to be a highly effective predictor of recurrence in AIS.
Keywords: high mobility group box 1, acute ischemic stroke, recurrence
Introduction
The Global Burden of Disease Study 2019 showed a significant increase in annual stroke incidence and deaths from 1990 to 2019.1 Stroke is the leading cause of death in China, with the overall prevalence, morbidity, and mortality of stroke among adults aged 40 years and older estimated to be 2.6%, 505.2/100,000 person-years, and 343.4/100,000 person-years in 2020, respectively.2 Acute ischemic stroke (AIS), which accounts for more than 86.9% of stroke, has a high recurrence rate, with 3.6% and 5.6% recurrence rates at 3 months and 12 months, respectively.3 Epidemiological findings suggest that the 1-year risk of recurrence of AIS is 7–13%, and its 10-year risk of recurrence approaches 40%.4,5 A number of biomarkers have been found to predict recurrence of AIS, such as cyclophilin A, cystatin C, lipoprotein-associated phospholipase A2, and homocysteine.6–9 However, some biomarkers have certain limitations in clinical application or controversial results in some studies. Therefore, accurate prediction of recurrence of AIS remains challenging.
The occurrence of AIS induces inflammatory responses and oxidative stress, which directly or indirectly result in neuronal cell damage or death, thereby further exacerbating the condition.10–12 In addition, it has been found that inflammatory responses and oxidative stress stimulate the release of high mobility group box 1 (HMGB1) from damaged or necrotic cells.13,14 HMGB1 normally acts as a damage-associated molecular pattern molecule in the extracellular space, modulating the inflammatory response and oxidative stress through different pathways.14,15 HMGB1 released after AIS was found to play a crucial role in both the early pathological damage process and the late promotion of brain tissue repair and remodeling.16
A systematic review and meta-analysis including 28 studies found that patients with AIS exhibit elevated plasma HMGB1 levels, which are positively correlated with disease severity and infarct volume.17 Furthermore, a study involving 132 patients with AIS after intravenous thrombolysis found that plasma HMGB1 levels peak 6 hours after thrombolytic therapy and were associated with a poor prognosis at 3 months.18 Elevated baseline plasma HMGB1 levels were also an independent predictor of poor prognosis at 1 year after AIS.19,20 These findings strongly support the importance of monitoring baseline HMGB1 levels in patients with AIS, especially for the assessment of disease severity and prognosis.
Genetic analysis and follow-up of 871 patients with AIS revealed that HMGB1 polymorphisms were significantly associated with a high risk of ischemic stroke, in particular the HMGB1 rs1412125 polymorphism, which may be a new genetic biomarker and potential target for detection of susceptibility and recurrence of ischemic stroke.21 However, there are relatively few studies of baseline serum HMGB1 levels and AIS on a more long-term basis, and whether they are associated with ischemic stroke recurrence. Therefore, this study investigated the correlation between baseline serum HMGB1 levels and AIS recurrence through a long-term study in patients with AIS.
Material and Methods
Study Population
The study was a prospective study. A total of 544 patients with AIS treated at Jiangyin People’s Hospital from January 2020 to September 2020 were included in this study. The study was approved by the Ethics Committee of Jiangyin People’s Hospital (approval number: 2020009) in accordance with the Declaration of Helsinki. All enrolled patients met the definition of Chinese AIS diagnostic and therapeutic guidelines, were given medication according to the guidelines, and signed a written informed consent before enrolment.22 Patients will be excluded if they present with the following diseases: recurrent ischemic stroke or cerebral haemorrhage with neurodegenerative diseases such as Parkinson’s disease, Alzheimer’s disease or vascular dementia, transient ischemic attack, haematological diseases, autoimmune diseases, co-infections, inability to follow up.
Clinical and Laboratory Assessments
All enrolled patients underwent a neurological physical examination by a specialist with extensive clinical experience, and a detailed history of current and past medical conditions, particularly any previous history of hypertension, diabetes mellitus, or atrial fibrillation, was taken and recorded. Elbow venous blood was drawn from fasting enrolled patients on the second day of hospitalisation.
A portion of the blood samples were sent to the central laboratory for the measurement of low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C) using Roche e602 modules, as in our previously published article.23 A portion of the blood sample was centrifuged at 3000r/min for 15 minutes and the upper serum layer was extracted into an Eppendorf tube. Then the Eppendorf tubes were frozen at −80°C for examination. Serum HMGB1 levels were measured by human ELISA kit (Elabscience, China) according to the instruction. The level of HMGB1 was calculated by reading the absorbance at 450 nm with a spectrophotometer.
Follow-Up
After patients were discharged from the hospital, they were followed up with regular monthly outpatient interviews or telephone interviews with patients’ families. The study was followed until the end of December 2023, with a median follow-up time of 43 months (interquartile range, 39–45 months). The endpoint event in this study was out-of-hospital recurrent AIS. A total of 62 enrolled patients with recurrent AIS were recorded in this study (Figure 1).
 |
Figure 1 Flow chart of the study. AIS, acute ischemic stroke. |
Statistical Analysis
The statistical analysis was conducted using the SPSS 25.0 statistical package. Quantitative variables were presented as means ± standard deviations and compared using Student’s t-test. Categorical variables were presented as absolute numbers (percentages) and compared using the chi-square test and Mann–Whitney-Wilcoxon test. The receiver operating characteristic curve (ROC) was used to determine the best cut-off value for each variable to predict recurrence of AIS. Kaplan-Meier survival curves were used to conduct survival analysis which were then compared using the Log rank test. To analyze the relationships between HMGB1 levels and AIS recurrence, univariate and multivariate Cox proportional hazards models were employed, calculating hazard ratios (HRs) and 95% confidence intervals (CIs). All variables that reached statistical significance in univariate Cox analysis were included in the multivariate Cox analysis. A p value<0.05 was considered statistically significant (two-tailed).
Results
The Comparison of Baseline Clinical Data
During the follow-up interval with a median time of 43 months, 62 recurrences were recorded in 544 patients with AIS. Patients were divided into an AIS recurrence group and a no AIS recurrence group based on whether or not they had recurrence of AIS. The comparison of baseline clinical data between these two groups was detailed in Table 1. The prevalence of hypertension, diabetes mellitus and atrial fibrillation was significantly higher in the AIS recurrence group than in the no AIS recurrence group (p<0.05). LDL-C levels, HMGB1 levels and national institute of health stroke scale (NIHSS) were significantly higher in the AIS recurrence group than in the no-AIS recurrence group, while HDL-C levels were lower than in the no-AIS recurrence group (p<0.05). There was no statistical difference in gender and age between the two groups.
 |
Table 1 The Demographic and Baseline Clinical Characteristics of the Patients |
Assessment of the Predictive Value of AIS Recurrence
Serum HMGB1 levels and NIHSS used to assess the severity of AIS were used for ROC curve analysis (Figure 2). Based on ROC curve analysis, HMGB1 was a significant predictor of AIS recurrence with an area under curve (AUC) of 0.745 (95% CI: 0.663–0.826). The AUC of NIHSS for predicting AIS recurrence was 0.822 (95% CI: 0.758–0.886). The combined HMGB1 and NIHSS had an AUC of 0.855 (95% CI: 0.800–0.911) for predicting AIS recurrence, which has a higher predictive value than either factor (p<0.05).
 |
Figure 2 Receiver operating characteristic curve for predicting AIS recurrence. Receiver operating characteristic curves were used to determine the area under the curve for each variable and z-test comparisons were performed. Abbreviations: AIS, acute ischemic stroke; HMGB1, high mobility group protein box 1; NIHSS, National Institute of Health stroke scale. |
Survival Analysis of Factors Affecting AIS Recurrence
The optimal cut-off value for HMGB1 (13.62µg/L) was then calculated by the Jordon’s index, based on which the patients were divided into a high HMGB1 level group and a low HMGB1 level group for survival analysis. Kaplan-Meier analysis revealed a significant difference between the cumulative survival rates without AIS recurrence between the two groups (Figure 3). The cumulative survival free of AIS recurrence was significantly lower in patients in the high HMGB1 level group than in the low HMGB1 level group (p<0.05).
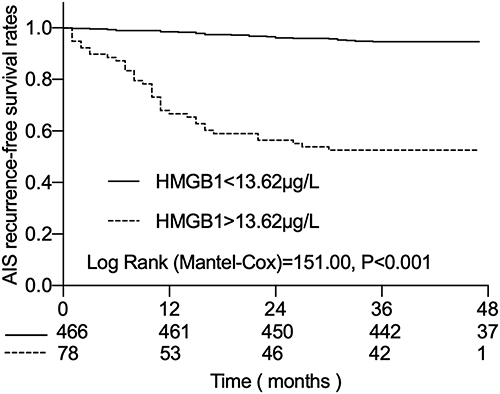 |
Figure 3 Kaplan-Meier curves showing the probability of no recurrence in patients with AIS at different HMGB1 levels. Kaplan-Meier survival curves were used to conduct survival analysis which were then compared using the Log rank test. Abbreviations: AIS, acute ischemic stroke; HMGB1, high mobility group protein box 1. |
The univariate Cox analysis found that elevated baseline serum HMGB1 levels were as much a predictor of AIS recurrence as a history of previous hypertension, diabetes mellitus, and atrial fibrillation, as well as elevated LDL-C levels and high NIHSS (Table 2). Subsequent multifactorial cox analyses of statistically different metrics in the univariate cox found that elevated baseline HMGB1 (HR:7.489, 95% CI:4.383–12.795) and LDL-C (HR:2.433, 95% CI:1.435–4.124) levels and high NIHSS (HR:7.904, 95% CI:4.508–13.858), and a history of atrial fibrillation (HR:2.383, 95% CI:1.384–4.103) remained predictive factors for recurrence of AIS.
 |
Table 2 Univariate and Multivariate COX Analysis for Recurrence of AIS |
Discussion
Previous studies have found that plasma HMGB1 levels are significantly higher and positively correlated with NIHSS in patients with AIS.18,24 Another study found HMGB1 to be the best biomarker for diagnosing and predicting AIS severity.25 This is similar to our study. In the present study, serum HMGB1 levels were found to be significantly elevated in AIS recurrence. HMGB1 had the same value as NIHSS in predicting AIS recurrence. The predictive value of HMGB1 was even greater when combined with NIHSS. HMGB1 was similar to LDL-C, NIHSS, and history of atrial fibrillation as predictors of AIS recurrence.
In AIS patients, large amounts of HMGB1 are secreted by ischemic brain tissue and released extracellularly to promote an inflammatory response to exacerbate brain damage, and large amounts of HMGB1 can also be detected in ischemic brain tissue in the chronic phase.26,27 Elevated HMGB1 can further activate platelets and induce thrombosis, exacerbating brain tissue injury.28
The release of HMGB1 from ischemic brain tissue may be the main reason for the elevation of HMGB1 after ischemia.29 Moreover, it remains elevated during the subacute phase, making it a time-sensitive marker of brain injury and recovery.30 Factors responsive to systemic inflammatory responses such as CRP, IL-6 and TNF-a have been found to be associated with long-term prognosis and recurrent events in AIS.31,32 However, the temporal dynamics and specificity of HMGB1 provide additional prognostic value, which makes HMGB1 a more relevant predictor of AIS recurrence.
Methods commonly used as clinical treatments for AIS such as intravenous thrombolysis and endovascular thrombectomy affect HMGB1 levels. Although intravenous thrombolysis can initiate reperfusion, it may also lead to HMGB1 release caused by reperfusion injury, elevating HMGB1 levels.18 In contrast, patients with successful reperfusion via thrombectomy typically exhibit lower HMGB1 levels.33 However, in cases of incomplete reperfusion, HMGB1 levels may remain elevated, indicating continued tissue damage.
HMGB1 is not only a prognostic marker for AIS, but is also considered an important therapeutic target.30 In a rat model of cerebral ischemia-reperfusion, HMGB1 was massively translocated to the cytoplasm and its plasma level was significantly elevated, whereas inhibition of HMGB1 reduced the volume of cerebral infarcts and ameliorated neurological deficits.34 In addition, inhibition of HMGB1 effectively attenuated neuroinflammation, reduced infarct volume, and promoted motor function recovery.35 In a rat model of ischemic stroke, HMGB1 inhibitor significantly reduced mortality, attenuated cerebral hemorrhage, brain swelling, blood-brain barrier injury and neuronal apoptosis, and improved the prognosis of neurological function.36 A large number of studies have found that some clinically used drugs such as atorvastatin, berberine, minocycline and diosgenin can inhibit the expression and transport of HMGB1, thereby suppressing inflammation, reducing neuronal damage, decreasing infarct size and improving neurological function.37–40
This study has a few limitations. Firstly, it was a single-centre study. Case ascertainment was carried out in only one hospital, which may have introduced some selection bias. Secondly, serum HMGB1 levels were only measured at admission, not at the time of the patient’s AIS relapse, which did not allow for a before and after control study. In addition, this study only investigated the relationship between serum HMGB1 levels and AIS recurrence. However, the association between elevated serum HMGB1 levels and poor functional prognosis and death in AIS was not investigated, as previous studies have shown that elevated HMGB1 levels were associated with poor prognosis in patients with AIS.41,42 Therefore, large, multi-centre, long-term clinical trials are needed to confirm the association between HMGB1 and AIS recurrence.
Conclusion
In the present study, we found that AIS relapsers had higher serum HMGB1 levels. Elevated serum HMGB1 levels at baseline had a high predictive value for AIS recurrence, which was even higher when combined with NIHSS. HMGB1 along with multiple factors LDL-C, NIHSS, and history of atrial fibrillation were predictors of AIS recurrence. This study provides a foundation for the clinical application of serum HMGB1 levels in AIS management, particularly in risk stratification, early warning, individualized treatment, and prognosis. Future studies could focus on validating the effectiveness of HMGB1 as a predictive biomarker, particularly a diagnostic tool combining HMGB1 with other established predictors, and exploring its applicability in different patient populations.
Data Sharing Statement
The data from this study are available on request from the corresponding author. The data are not publicly available due to privacy and ethical restrictions.
Ethics Approval and Informed Consent
The study was approved by the Ethics Committee of Jiangyin People’s Hospital (approval number: 2020009) in accordance with the Declaration of Helsinki. All enrolled patients signed a written informed consent before enrolment.
Funding
This research was funded by the development fund of Affiliated Hospital of Xuzhou Medical University (grant no. XYFY2021029), Medical Research Program of Jiangsu Provincial Health and Wellness Commission (grant no. Z2021042).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Collaborators GBDS. Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):795–820. doi:10.1016/S1474-4422(21)00252-0
2. Tu WJ, Zhao Z, Yin P, et al. Estimated Burden of Stroke in China in 2020. JAMA Network Open. 2023;6(3):e231455. doi:10.1001/jamanetworkopen.2023.1455
3. Tu WJ, Wang LD, Special Writing Group of China Stroke Surveillance R. China stroke surveillance report 2021. Mil Med Res. 2023;10(1):33. doi:10.1186/s40779-023-00463-x
4. Bejot Y, Daubail B, Giroud M. Epidemiology of stroke and transient ischemic attacks: current knowledge and perspectives. Rev Neurol. 2016;172(1):59–68. doi:10.1016/j.neurol.2015.07.013
5. Mohan KM, Crichton SL, Grieve AP, et al. Frequency and predictors for the risk of stroke recurrence up to 10 years after stroke: the South London Stroke Register. J Neurol Neurosurg Psych. 2009;80(9):1012–1018. doi:10.1136/jnnp.2008.170456
6. Chang CS, Kuo CL, Huang CS, et al. Association of cyclophilin A level and pulse pressure in predicting recurrence of cerebral infarction. Kaohsiung J Med Sci. 2020;36(2):122–128. doi:10.1002/kjm2.12143
7. Zeng Q, Lin K, Yao M, et al. Significant correlation between cystatin C, cerebral infarction, and potential biomarker for increased risk of stroke. Curr Neurovasc Res. 2015;12(1):40–46. doi:10.2174/1567202612666150102150941
8. Wei L, Ke Z, Zhao Y, et al. The elevated lipoprotein-associated phospholipase A2 activity is associated with the occurrence and recurrence of acute cerebral infarction. Neuroreport. 2017;28(6):325–330. doi:10.1097/WNR.0000000000000765
9. Anniwaer J, Liu MZ, Xue KD, et al. Homocysteine might increase the risk of recurrence in patients presenting with primary cerebral infarction. Int J Neurosci. 2019;129(7):654–659. doi:10.1080/00207454.2018.1517762
10. Qin C, Yang S, Chu YH, et al. Signaling pathways involved in ischemic stroke: molecular mechanisms and therapeutic interventions. Signal Transduct Target Ther. 2022;7(1):215. doi:10.1038/s41392-022-01064-1
11. Ren X, Hu H, Farooqi I, et al. Blood substitution therapy rescues the brain of mice from ischemic damage. Nat Commun. 2020;11(1):4078. doi:10.1038/s41467-020-17930-x
12. Hu X, Wu D, He X, et al. circGSK3beta promotes metastasis in esophageal squamous cell carcinoma by augmenting beta-catenin signaling. Mol Canc. 2019;18(1):160. doi:10.1186/s12943-019-1095-y
13. Xue J, Suarez JS, Minaai M, et al. HMGB1 as a therapeutic target in disease. J Cell Physiol. 2021;236(5):3406–3419. doi:10.1002/jcp.30125
14. Chen R, Kang R, Tang D. The mechanism of HMGB1 secretion and release. Exp Mol Med. 2022;54(2):91–102. doi:10.1038/s12276-022-00736-w
15. Yu Y, Tang D, Kang R. Oxidative stress-mediated HMGB1 biology. Front Physiol. 2015;6:93. doi:10.3389/fphys.2015.00093
16. Gao B, Wang S, Li J, et al. HMGB1, angel or devil, in ischemic stroke. Brain Behav. 2023;13(5):e2987. doi:10.1002/brb3.2987
17. Le K, Mo S, Lu X, et al. Association of circulating blood HMGB1 levels with ischemic stroke: a systematic review and meta-analysis. Neurol Res. 2018;40(11):907–916. doi:10.1080/01616412.2018.1497254
18. Wang J, Jiang Y, Zeng D, et al. Prognostic value of plasma HMGB1 in ischemic stroke patients with cerebral ischemia-reperfusion injury after intravenous thrombolysis. J Stroke Cerebrovasc Dis. 2020;29(9):105055. doi:10.1016/j.jstrokecerebrovasdis.2020.105055
19. Tsukagawa T, Katsumata R, Fujita M, et al. Elevated Serum High-Mobility Group Box-1 Protein Level Is Associated with Poor Functional Outcome in Ischemic Stroke. J Stroke Cerebrovasc Dis. 2017;26(10):2404–2411. doi:10.1016/j.jstrokecerebrovasdis.2017.05.033
20. Huang JM, Hu J, Chen N, et al. Relationship between plasma high-mobility group box-1 levels and clinical outcomes of ischemic stroke. J Crit Care. 2013;28(5):792–797. doi:10.1016/j.jcrc.2012.10.003
21. Qiu L, Li L, He Z, et al. Association between HMGB1 genetic variants and ischemic stroke susceptibility, onset age, and recurrence risk among Chinese Han individuals. Am J Transl Res. 2023;15(5):3326–3341.
22. Chinese Society of Neurology CSS. Chinese guidelines for diagnosis and treatment of acute ischemic stroke 2018. Chin J Neurol. 2018;51(9):666–682. doi:10.3760/cma.j.issn.1006-7876.2018.09.004
23. Gu L, Jiang W, Jiang W, et al. Elevated serum FGF21 levels predict heart failure during hospitalization of STEMI patients after emergency percutaneous coronary intervention. PeerJ. 2023:11:e14855. doi:10.7717/peerj.14855
24. Zhou P, Li YQ, Li WD, et al. Changes in serum high mobility group box-1 protein and high-sensitivity C-reactive protein in patients with acute cerebral infarction and their clinical significance. Zhongguo Wei Zhong Bing Ji Jiu Yi Xue. 2012;24(5):265–268. doi:10.3760/cma.j.issn.1003-0603.2012.05.003
25. Keshk WA, Zineldeen DH, El-Heneedy YA, et al. Thrombomodulin, alarmin signaling, and copeptin: cross-talk between obesity and acute ischemic stroke initiation and severity in Egyptians. Neurol Sci. 2018;39(6):1093–1104. doi:10.1007/s10072-018-3396-0
26. Umahara T, Uchihara T, Hirokawa K, et al. Time-dependent and lesion-dependent HMGB1-selective localization in brains of patients with cerebrovascular diseases. Histol Histopathol. 2018;33(2):215–222. doi:10.14670/HH-11-914
27. Kim JB, Sig Choi J, Yu YM, et al. HMGB1, a novel cytokine-like mediator linking acute neuronal death and delayed neuroinflammation in the postischemic brain. J Neurosci. 2006;26(24):6413–6421. doi:10.1523/JNEUROSCI.3815-05.2006
28. Kim SW, Lee JK. Role of HMGB1 in the Interplay between NETosis and Thrombosis in Ischemic Stroke: a Review. Cells. 2020;9(8). doi:10.3390/cells9081794
29. Dyer MR, Chen Q, Haldeman S, et al. Deep vein thrombosis in mice is regulated by platelet HMGB1 through release of neutrophil-extracellular traps and DNA. Sci Rep. 2018;8(1):2068. doi:10.1038/s41598-018-20479-x
30. Li J, Wang Z, Li J, et al. HMGB1: a New Target for Ischemic Stroke and Hemorrhagic Transformation. Transl Stroke Res. 2024. doi:10.1007/s12975-024-01258-5
31. VanGilder RL, Davidov DM, Stinehart KR, et al. C-reactive protein and long-term ischemic stroke prognosis. J Clin Neurosci. 2014;21(4):547–553. doi:10.1016/j.jocn.2013.06.015
32. Ma F, Li L, Xu L, et al. The relationship between systemic inflammation index, systemic immune-inflammatory index, and inflammatory prognostic index and 90-day outcomes in acute ischemic stroke patients treated with intravenous thrombolysis. J Neuroinflammation. 2023;20(1):220. doi:10.1186/s12974-023-02890-y
33. Liu KL, He J, Zang YJ. Clinical effect of intravascular interventional therapy in the treatment of acute ischemic stroke and its influence on cognitive function, cerebral hemodynamics and inflammatory factors. Pak J Med Sci. 2022;38(5):1143–1149. doi:10.12669/pjms.38.5.5255
34. Wang J, Han D, Sun M, et al. A Combination of Remote Ischemic Perconditioning and Cerebral Ischemic Postconditioning Inhibits Autophagy to Attenuate Plasma HMGB1 and Induce Neuroprotection Against Stroke in Rat. J Mol Neurosci. 2016;58(4):424–431. doi:10.1007/s12031-016-0724-9
35. Jin L, Zhu Z, Hong L, et al. ROS-responsive 18beta-glycyrrhetic acid-conjugated polymeric nanoparticles mediate neuroprotection in ischemic stroke through HMGB1 inhibition and microglia polarization regulation. Bioact Mater. 2023;19:38–49. doi:10.1016/j.bioactmat.2022.03.040
36. Chen H, Guan B, Wang B, et al. Glycyrrhizin Prevents Hemorrhagic Transformation and Improves Neurological Outcome in Ischemic Stroke with Delayed Thrombolysis Through Targeting Peroxynitrite-Mediated HMGB1 Signaling. Transl Stroke Res. 2020;11(5):967–982. doi:10.1007/s12975-019-00772-1
37. Wang L, Zhang X, Liu L, et al. Atorvastatin protects rat brains against permanent focal ischemia and downregulates HMGB1, HMGB1 receptors (RAGE and TLR4), NF-kappaB expression. Neurosci Lett. 2010;471(3):152–156. doi:10.1016/j.neulet.2010.01.030
38. Zhu JR, Lu HD, Guo C, et al. Berberine attenuates ischemia-reperfusion injury through inhibiting HMGB1 release and NF-kappaB nuclear translocation. Acta Pharmacol Sin. 2018;39(11):1706–1715. doi:10.1038/s41401-018-0160-1
39. Hayakawa K, Mishima K, Nozako M, et al. Delayed treatment with minocycline ameliorates neurologic impairment through activated microglia expressing a high-mobility group box1-inhibiting mechanism. Stroke. 2008;39(3):951–958. doi:10.1161/STROKEAHA.107.495820
40. Zhu S, Tang S, Su F. Dioscin inhibits ischemic stroke‑induced inflammation through inhibition of the TLR4/MyD88/NF‑kappaB signaling pathway in a rat model. Mol Med Rep. 2018;17(1):660–666. doi:10.3892/mmr.2017.7900
41. Chu XH, Hu HY, Godje ISG, et al. Elevated HMGB1 and sRAGE levels in cerebrospinal fluid of aneurysmal subarachnoid hemorrhage patients. J Stroke Cerebrovasc Dis. 2023;32(5):107061. doi:10.1016/j.jstrokecerebrovasdis.2023.107061
42. Sapojnikova N, Kartvelishvili T, Asatiani N, et al. Correlation between MMP-9 and extracellular cytokine HMGB1 in prediction of human ischemic stroke outcome. Biochim Biophys Acta. 2014;1842(9):1379–1384. doi:10.1016/j.bbadis.2014.04.031
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.