")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Empowering Stoma Care: Enhancing Knowledge, Confidence, and Support Through Collaborative Approaches Between Doctors and Parental Communities for Children with Stomas
Authors Gaol LML , Saraswati LQ, Gultom GS, Anita M, Firmansyah Y, Setiawan FV, Wijaya BA
Received 14 January 2025
Accepted for publication 13 July 2025
Published 17 July 2025 Volume 2025:18 Pages 4089—4098
DOI https://doi.org/10.2147/JMDH.S517481
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Leecarlo Millano Lumban Gaol,1– 3 Lavenia Quinta Saraswati,2 Grace Shintauli Gultom,2 Melian Anita,1,3 Yohanes Firmansyah,4 Fiona Valencia Setiawan,4 Bryan Anna Wijaya4
1Faculty of Medicine, Padjadjaran University, Bandung, Indonesia; 2Department of Surgery, Pediatric Surgery Division, Tarakan General Hospital, Jakarta, Indonesia; 3Faculty of Medicine, Krida Wacana Christian University, Jakarta, Indonesia; 4Faculty of Medicine, Tarumanagara University, Jakarta, Indonesia
Correspondence: Leecarlo Millano Lumban Gaol, Faculty of Medicine, Padjadjaran University, Raya Bandung Sumedang Street No. 21, Bandung, West Java, 45360, Indonesia, Email [email protected]
Introduction: Effective postoperative care is pivotal, and parents play a vital role in managing complications and outcomes. Despite their importance, parents often struggle with the complexities of stoma care. Managing pediatric stomas necessitates a collaborative effort between healthcare professionals and community support, forming a multidisciplinary team that empowers parents with the knowledge and confidence required for effective stoma management.
Purpose and Objectives: This study assesses the impact of collaborative efforts between doctors and community support systems on children’s quality of stoma care.
Methods: A cross-sectional study involving 224 participants evaluated the influence of stoma support communities in Jakarta. The study used a validated 11-question questionnaire to measure community impact and stoma care knowledge.
Results: Spearman Correlation analysis indicated significant relationships between doctor-patient communication and factors such as the stoma’s condition (r:0.285, p< 0.001), knowledge (r:0.417, p< 0.001), support in stoma care (r:0.458, p< 0.001), self-confidence (r:0.440, p< 0.001), support systems (r:0.407, p< 0.001), and ease of access to care (r:0.357, p< 0.001). Multivariate analysis highlighted that the quality of doctor-patient communication significantly affects stoma condition, support systems, self-confidence, and access to care (p< 0.025). ROC prediction analysis showed that effective doctor-patient communication through Komunitas Stoma Pada Anak Jakarta (KOSPAJA) significantly enhances support and self-confidence in stoma care (A> 0.70).
Conclusion: The collaboration between doctors and community support significantly enhances parents’ knowledge, confidence, and support in managing their child’s stoma, leading to improved care quality and reduced complication rates.
Keywords: children, doctor, parental community, stoma, stoma care
Introduction
Stoma or ostomy originates from the Latin word ostium, meaning “opening” or “mouth.” The intestinal stoma is the most common surgical procedure among the various stomas.1 A stoma is commonly established in the small intestine (ileostomy) and large intestine (colostomy) to facilitate bowel evacuation.2 Surgical openings were created on the anterior abdomen from the urinary tract or the bowel to create intestinal stomas. Depending on their type, it is defined as end stomas and loop or double-barreled stomas. The choice of stomas depends on the specific medical situation.3 Creating an intestinal stoma is a life-saving procedure, frequently performed and crucial in managing congenital and acquired gastrointestinal diseases.2 Creating a stoma includes diverting fecal output, decompressing the intestines, protecting anastomotic sites, or a combination of these procedures. Unlike adults, pediatric stomas are temporary and serve as an initial procedure to address congenital disorders in children.4 Conditions necessitating stoma creation in children for survival include Anorectal Malformation (ARM), Hirschsprung’s Disease, Jejunoileal Atresia, Intussusception, perforated Necrotizing Enterocolitis (NEC), Trauma, and Intestinal tumor.2,4 The number of stomas used in the United States ranges from 750,000 to 1 million. An estimated 15,000 new ostomies are created each year. A stoma may be created as a colostomy or an ileostomy, either planned or as an emergency procedure. The Michigan Surgical Quality population-based study included 4250 patients. 37% had elective ostomy cases, and 55% had emergency ones.5
Stoma formation can help patients return to a healthy life and prolong their lives. However, this may cause patients living with a stoma to face both social and psychological challenges. Social problems include decreased working activities, less participation in social activities, worsening in partner relationships, avoidance of traveling, and reduced contact with relatives. Individuals with a stoma, such as low self-esteem, depression, changes in body image, anxiety, and stagnation, may experience psychological issues. Physical problems are often the common focus of healthcare professionals, and they mostly neglect the psychological aspects. Building a community for stoma users to experience understanding, care, and shared experiences is essential for the continuous care of patients with stomas.6 Caring for a child with a stoma requires more intensive attention due to the anxiety and fear experienced by both the child and the parents. Preparedness for stoma creation is crucial in enhancing the child’s quality of life. The care of a child with a stoma involves a multidisciplinary team that can guide the family to feel more confident in managing the child’s stoma condition.7 The recovery process for a child with a stoma depends not only on perioperative and operative conditions but also on effective family care. Research indicates that parents’ ability to provide postoperative care can reduce complication rates and contribute to positive outcomes. Parents, as the primary caregivers, when the child leaves the hospital, may encounter challenges in stoma care due to a lack of knowledge and training from medical professionals, resulting from a short hospital stay.8
Methods
Place and Ethical Clearance of Research
This research was conducted at Tarakan General Hospital, West Java, and has received ethical approval from the ethics committee at Tarakan General Hospital (No.051/KEPK/RSUDT/2024).
Research Design
This cross-sectional study, conducted in August 2024 at Tarakan Regional Hospital, Jakarta, involved 224 research respondents.
Sample and Sampling Method
This study’s sample consisted of parents who were members of Komunitas Stoma Pada Anak Jakarta (KOSPAJA) and had children with a history of stoma care or installation. The sampling method was total sampling, or all parents were invited to participate. The recruitment process followed a standardized protocol: all eligible parents were invited to participate in the study through an official communication distributed by the KOSPAJA administrators.
The invitation included a brief explanation of the study objectives, ethical considerations, and questionnaire instructions. Participants who agreed to participate were provided with a structured self-administered questionnaire, which they completed voluntarily. The questionnaire was distributed electronically via a secure link during scheduled community gatherings. Responses were collected anonymously to ensure confidentiality. This standardized approach ensured participant engagement and data collection consistency across the study sample.
Exclusion Criteria
The exclusion criteria in this study were parents who had difficulty speaking Indonesian or refused to participate.
Data Collection Methods
The questionnaire outline in the study is as follows:
- Since when did you join the KOSPAJA group?
- Reasons for creating a stoma
- Stoma Condition
- The community plays a vital role in increasing knowledge about stomas
- Receiving Support and Assistance in Caring for a Stoma
- Have a friend to share the condition of a child with a stoma
- Feeling more confident in caring for a child with a stoma
- Get additional knowledge from experts
- Ease of obtaining stoma supplies
- Regular Consultations
- The Ways to Interact with Doctors
Questions 1–3 are only for personal and medical reasons for stoma research respondents. Questions numbers 4–11 are based on opinions and are responded to using a Likert scale of 1 (Strongly Disagree) and 5 (Strongly Agree).
Pilot Testing
This questionnaire was conducted as a preliminary study involving 20 research respondents outside the KOSPAJA community. The validity testing method used the Pearson Product-Moment test and reliability testing using Cronbach’s Alpha (margin: 0.6). The entire questionnaire, totaling 11 questions, had a Cronbach’s Alpha value > 0.8.
Consent
This study was conducted offline after obtaining parental consent. It was piloted on twenty parents whose children had stomas. Parents who consented to participate in the study were asked to complete a questionnaire. They were also asked to sign an integrity pledge stating that they would not discuss the answers in this study with anyone else and would not refer to external sources while completing the questionnaire. Each parent was contacted in advance via email, and written consent was sent to their email for approval.
Data Management
Data were entered into Microsoft Excel and analyzed using IBM SPSS Version 21 for Windows, Armonk, NY. They were presented as descriptive statistics and analyzed, and free-text comments were collected.
Demographic characteristics of respondents were tabulated. Median stoma perception scores were calculated based on respondents’ level of agreement with eight statements. The statements were rated on the following scale: strongly disagree = 1, disagree = 2, neutral = 3, agree = 4, and strongly agree = 5. Median scores were compared among subgroups of respondents based on demographic characteristics and background. Other responses were analyzed descriptively. Respondents’ perceptions of the role of the community, support in stoma care, and confidence in caring for a child with a stoma were assessed by their level of agreement with the statements.
Respondents’ perceptions regarding the importance of community support, consultation with a physician, and ease of obtaining stoma supplies were also recorded based on responses to the Likert scale. Further analysis was conducted if more than 20% of the respondents selected “agree” or “strongly agree” to a particular question. The training period in stoma competency and interactions with physicians were also recorded. Free text comments are invited to provide additional insights.
Data Analysis
Data were analyzed using descriptive methods, receiver operating characteristic (ROC) curve, and Spearman correlation analysis. This study involved 11 questions, with questions 1–3 focusing on the personal and medical reasons behind stoma installation. Questions 4–9 measured respondents’ perceptions of the role of the community, support received, and confidence in caring for children with a stoma using a Likert scale. Questions 10 and 11 evaluated the relationship between doctors and patients using a Likert scale, where a scale of 1 indicates the best doctor-patient relationship.
Qualitative data from questions 1–3 were presented in proportions to describe the general reasons for stoma installation. For questions 4–9, data were analyzed by comparing the median scores of respondents’ perceptions of various aspects of support and confidence in stoma care. This analysis provides an overview of how the community and external support play a role in improving parents’ ability to care for their children.
Furthermore, ROC analysis was used to evaluate the doctor-patient variables (questions 10 and 11) as a reference line in determining the relationship quality between doctors and parents. The ROC curve allows researchers to evaluate the sensitivity and specificity of the doctor-patient relationship score. The Area Under the Curve (AUC) is calculated as a measure of the predictive accuracy of the independent variable being tested.
The interpretation of the AUC value in this context is as follows:
- An AUC of 0.5 indicates that the model is no better than a random guess predicting the outcome, suggesting a non-significant doctor-patient relationship.
- An AUC between 0.7 and 0.8 indicates moderate performance, indicating that the doctor-patient relationship is starting to play a role in determining stoma care outcomes.
- An AUC between 0.8 and 0.9 indicates excellent performance, indicating that the doctor-patient relationship strongly and significantly influences parental support and confidence.
- An AUC above 0.9 indicates excellent performance, and the doctor-patient relationship is a key factor in determining stoma care.
Result
This study revealed that among the 224 members of the Stoma Community for Children in Jakarta, 64.3% were male and 35.7% were female. Most members (61.6%) had been part of the community for less than a year, 22.8% had been involved for one to three years, and 15.6% for over three years. Regarding stoma conditions in children, 84.8% had closed stomas, whereas 15.2% still had open stomas. Most respondents (84.8%) emphasized the importance of regular doctor consultations, and 92.9% preferred face-to-face interactions at outpatient clinics over messaging (7.1%) (Table 1).
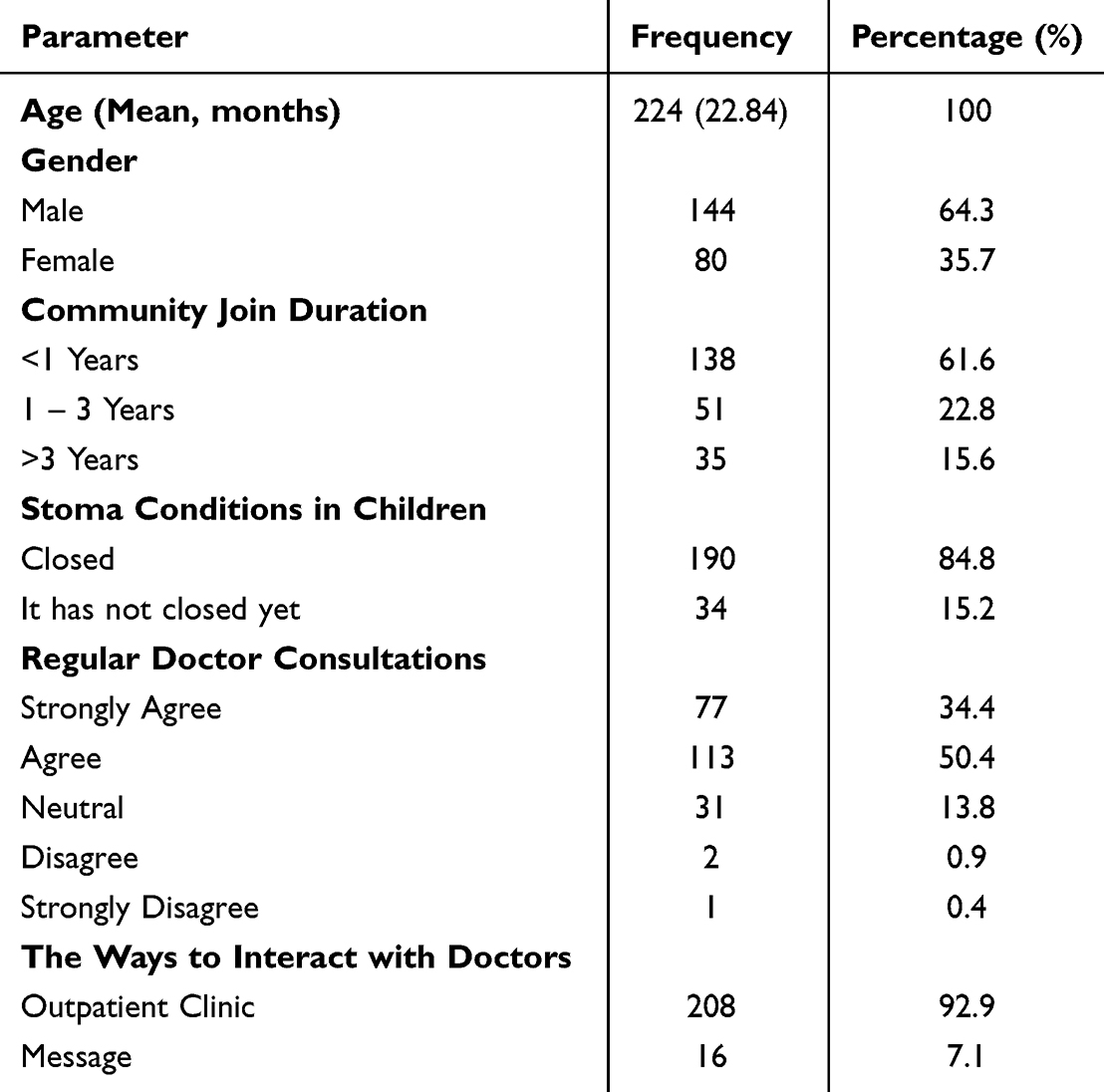 |
Table 1 Characteristics of the Stoma Community for Children in Jakarta |
This study revealed that in the Stoma Community for Children in Jakarta, Hirschsprung’s disease was the leading cause of stoma creation, accounting for 50% of cases. Anorectal malformation (ARM) closely followed, contributing to 30.3% of stoma cases. Intestinal atresia was the third most common cause, representing 16.9% of cases (Figure 1).
 |
Figure 1 Underlying Disease Leading to Stoma Creation in the Stoma Community for Children in Jakarta. |
This study underscored the pivotal role of parental communities in enhancing stoma empowerment. Most respondents valued gaining additional knowledge from experts, with 85.2% agreeing. Furthermore, 75.9% reported increased confidence in managing stoma care as a result of expert advice, and 84.4% appreciated the support and assistance they received. The findings also indicated that 82.6% found it beneficial to have peers with whom they could exchange information about stoma conditions, while 82.2% noted that stoma supplies were readily accessible. The results highlighted how community support and accessible resources significantly improved stoma management and empowerment (Table 2).
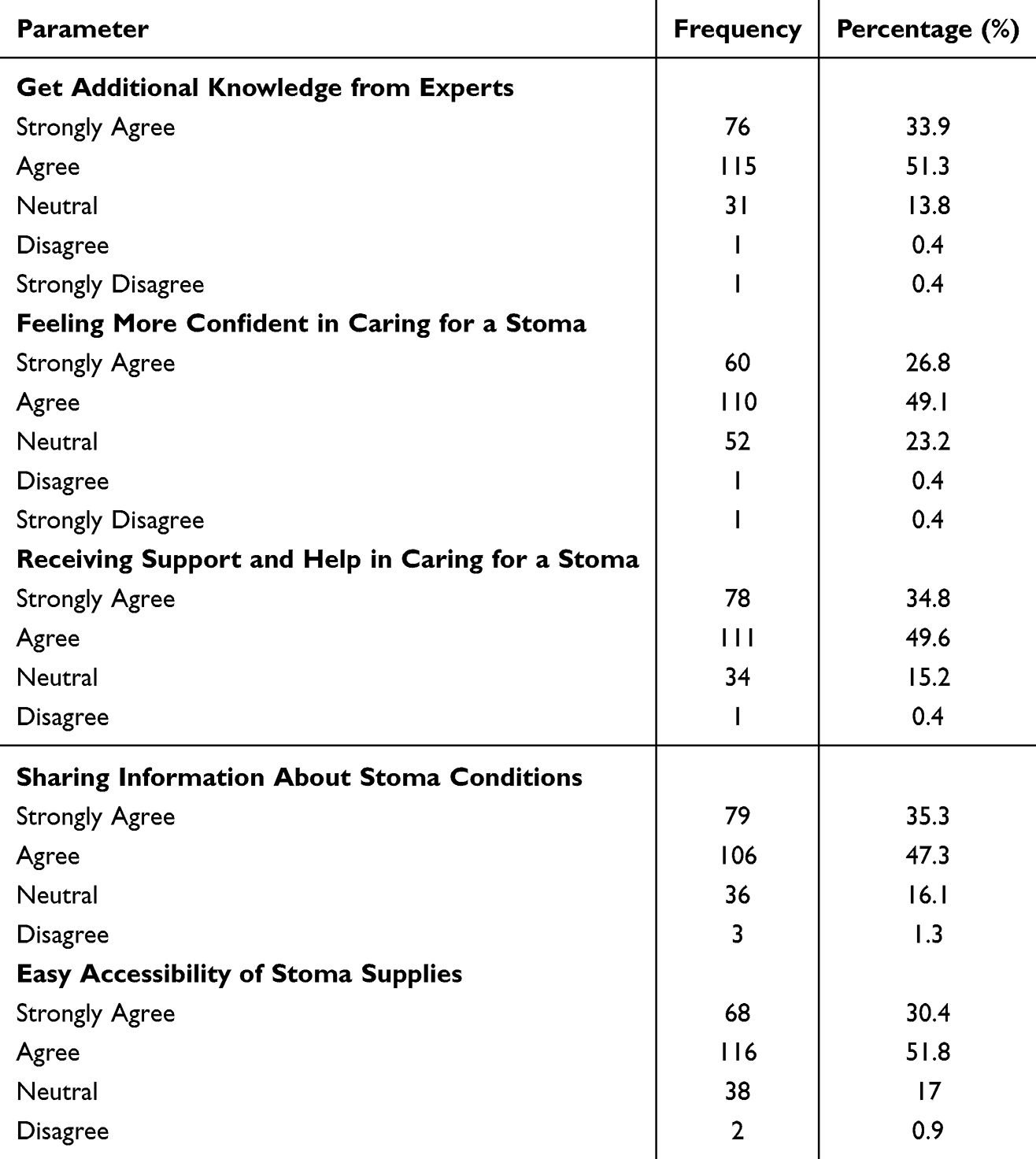 |
Table 2 The Role of Parental Communities on Stoma Empowerment |
Multivariate analysis further highlighted that the collaborative approaches between doctors and parental communities significantly affected stoma condition, support systems, self-confidence, and access to care (p < 0.025). ROC prediction analysis indicated that, as assessed by KOSPAJA, doctor-patient communication was a robust predictor of support and assistance as well as self-confidence in stoma care, with an area under the curve (AUC) exceeding 0.70 (Figure 2 and Table 3).
 |
Table 3 Area Under the Curve of Collaborative Approaches Between Doctors and Parental Communities |
 |
Figure 2 Receiver Operating Characteristic (ROC) Curve of Collaborative Approaches Between Doctors and Parental Communities. |
Spearman Correlation analysis demonstrated significant relationships between collaborative approaches by doctors and parental communities and several key variables: reason for a stoma (r = 0.280, p < 0.001), stoma condition (r = 0.285, p < 0.001), stoma knowledge in the community (r = 0.417, p < 0.001), support and assistance in stoma care (r = 0.458, p < 0.001), self-confidence (r = 0.440, p < 0.001), support system (r = 0.407, p < 0.001), special knowledge (r = 0.357, p < 0.001), and ease of access to care (r = 0.471, p < 0.001) (Table 4).
 |
Table 4 Spearman Correlation Analysis of Collaborative Approaches Between Doctors and Parental Communities |
Discussion
Living with a stoma can essentially influence the quality of life (QoL), affecting them physically, mentally, and socially. Physically, children with a stoma frequently confront challenges such as overseeing stoma care, managing skin irritation, and adapting to changes in physical abilities. These physical issues can lead to inconvenience and require continuous therapeutic consideration, which can disturb their daily activities and routines.9 Mentally, the nearness of a stoma can lead to sentiments of uneasiness, sadness, and a diminished sense of self-esteem in children. They may battle with body image issues and feel self-conscious about their appearance, which can be incredibly challenging over a long time.10 Getting support from family, companions, and healthcare specialists is noteworthy in changing how children investigate these social challenges.11 Socially, the effect of a stoma amplifies to include family, companions, and classmates. Children may find engaging in social activities, attending school regularly, or participating in sports challenging due to concerns around stoma management and potential injuries.12
Some studies have indicated that ostomy patients encounter numerous issues post-stoma creation, primarily due to insufficient knowledge, inadequate pre-operative preparation, and suboptimal postoperative management. Notably, 73% of ostomy patients report skin-related problems. Effective stoma education is crucial for achieving proficiency in management and minimizing complications. Early intervention in stoma care management significantly enhances quality of life and reduces the incidence of complications.13
Providing holistic support, children can better adapt to their new reality and achieve a higher quality of life.14 Living with a stoma requires long-term adjustment and complex treatment, essentially affecting patients’ QoL. According to the British Diary of Nursing, stoma surgery is an invasive procedure that influences the standard of living not fairly quickly post-operation, but throughout the patient’s life. The changes in substantial capacities, body image, and individual care needs require continuous adjustment and can disturb social, emotional, and work-related life perspectives.15
Parents play a crucial role in the healing process and care of stomas. When caring for stomas, families must gain knowledge and develop various skills.16 They require assistance to alleviate the caregiving load. Enhanced preparation and support for the responsibilities they undertake are essential. The psychological impact on the whole family should be a key consideration in the preparation and support given to parents. Utilizing resources from trauma-informed care literature can help families manage challenging procedures and emergencies at home.17
Stoma patients’ ability to care for themselves is significantly enhanced by community assistance, including peer networks and specialized stoma care. Based on the British Journal of Nursing Research, those with community assistance and structured instruction could adjust to their surroundings more skillfully and lead better lives.18 Parents and children face the dual challenge of adapting to the stoma and managing stoma care. Children’s responses will vary depending on their age and developmental stage. Therefore, when establishing a therapeutic relationship with parents and children, it is essential to consider numerous factors to choose strategies that best fit the child’s and family’s unique circumstances. Typically, children in their first two years are wary of unfamiliar faces and tend not to trust strangers. Therefore, building a strong rapport with the parents is crucial, allowing the child to see this trust before any physical care is administered. Engaging in play and gentle physical contact can help form a positive relationship with the child beyond invasive procedures.19
Statutory services aim to assist parents in fulfilling their responsibilities, including coordinating care and navigating the system.20 However, the practical implementation of this mandate is challenging. Recognizing the potential benefits of greater integration between healthcare services, various care models for children with medical complexities are currently being evaluated in Canada and the United States, emphasizing the importance of healthcare coordination.21,22
Accessible and high-quality training is essential for parents to feel at ease when leaving their child in the care of others, whether paid carers, family members, or respite services. Increased access to respite care, peer support, and financial aid has been shown to reduce the burden on families. Reductions in services supporting families, such as respite care, can lead to acute problems and higher costs in the long term when families struggle to cope.23 Community paediatricians and palliative care often play a significant role in care coordination, while charitable funds support nurses coordinating care, daily emotional and practical support, and parent/carer training. However, there is a need for the expansion of these services.24,25
Communities play a crucial role in assisting families in navigating the challenges of stoma care. They offer vital resources that can significantly enhance the experience for these families and provide immediate assistance. This support encompasses emotional and practical needs and includes valuable training and information that make the caregiving process more manageable. Community care addresses the most basic human needs, both emotional and practical. Local support groups serve as a lifeline for families dealing with the emotional challenges of stoma care. These groups provide parents and caregivers with a safe space to connect with others who can relate to their situation. They can share their experiences, exchange advice, and find support, comfort, and encouragement in these environments.
Training and education are fundamental in effectively supporting families and caregivers managing stoma care. Educating parents of children with stomas can significantly boost their understanding of care through a family-centred approach, empowering them to manage and prevent potential side effects more effectively.26,27 Support from community health care services on proper stoma care techniques, the use of medical devices, and strategies for handling everyday challenges associated with stoma management benefits the patient’s life and families. Participating in these programs gives them valuable knowledge and skills that enhance their confidence and competence in caregiving. Overall, communities play a crucial role in assisting families in navigating the complexities of stoma care by providing the necessary tools, knowledge, and support that help to increase people’s quality of life.12,26,27
This study has several limitations that should be considered when interpreting the findings. One key limitation is the absence of comparative data on complication rates between patients who received comprehensive parental and community support and those who did not. This restricts our ability to evaluate the potential influence of social support systems on clinical outcomes. Additionally, most participants (85%) had already undergone stoma closure during data collection. This may have introduced recall bias, as participants may not have accurately remembered the details of their stoma-related experiences. Furthermore, the emotional and physical distance from their period of living with a stoma may have affected the way they perceived and reported their experiences, potentially influencing the study results.
Conclusion
Collaboration between healthcare professionals and community support networks is vital in enhancing parents’ understanding and confidence in managing their child’s stoma. By combining medical expertise with community resources, parents gain crucial knowledge and hands-on guidance, which improves their ability to deliver effective care. This integrated approach helps parents navigate the complexities of stoma management and provides essential emotional and practical support. Consequently, this partnership results in higher-quality care, fewer complications, and better outcomes for children with stomas. This holistic support system ensures that families are well-equipped to handle the challenges of stoma care.
Acknowledgments
This study has been presented as a self-funded presentation. The authors thank the Tarakan General Hospital for their permission to conduct this research ethically.
Ethical Declaration
This study complied with the ethical standards outlined in the Declaration of Helsinki. The research protocols were reviewed and approved by the appropriate institutional ethics committee, ensuring the protection of the respondents’ rights, safety, and well-being throughout the study. Respondents were informed of their rights, including the right to provide informed consent, the right to withdraw at any time without penalty, and the right to ask questions and receive clear information about the study. Confidentiality was strictly maintained, with no identifying information used or disclosed at any stage of the research process. All respondents were treated with respect and dignity, and measures were taken to minimize any potential risk or harm associated with participation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mulita F, Lotfollahzadeh S. Intestinal Stoma. 2024. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22873030.
2. Rashed N, Khalifa M, Zein El Dein N, Omar T. Stoma care for children having colostomy in Menoufia University Hospital. Menoufia Nurs J. 2020;5(1):47–53. doi:10.21608/menj.2020.123794
3. Saunders RN, Hemingway D. Intestinal stomas. Surgery. 2008;26(8):347–351. doi:10.1016/j.mpsur.2008.05.011
4. Massenga A, Chibwae A, Nuri AA, et al. Indications for and complications of intestinal stomas in the children and adults at a tertiary care hospital in a resource-limited setting: a Tanzanian experience. BMC Gastroenterol. 2019;19(1):157. doi:10.1186/s12876-019-1070-5
5. Davis BR, Valente MA, Goldberg JE, Lightner AL, Feingold DL, Paquette IM. The American Society of Colon and Rectal Surgeons clinical practice guidelines for ostomy surgery. Dis Colon Rectum. 2022;65(10):1173–1190. doi:10.1097/DCR.0000000000002498
6. Ayaz‐Alkaya S. Overview of psychosocial problems in individuals with stoma: a review of literature. Int Wound J. 2019;16(1):243–249. doi:10.1111/iwj.13018
7. Maia EMB, Assis GM. Perception of the parents of children with intestinal stoma regarding the nursing orientations. ESTIMA Braz J Enterostomal Ther. 2019. doi:10.30886/estima.v17.663_IN
8. Gao X, Huang K, Cui X, Zhou C. WeChat‐assisted health education improves care ability, reduces care burden and improves quality of life of parents of infants after enterostomy. J Paediatr Child Health. 2021;57(7):1067–1071. doi:10.1111/jpc.15399
9. Goodman W, Downing A, Allsop M, et al. Quality of life profiles and their association with clinical and demographic characteristics and physical activity in people with a stoma: a latent profile analysis. Qual Life Res. 2022;31:1–10. doi:10.1007/s11136-022-03102-5
10. Polidano K, Chew-Graham C, Farmer A, Saunders B. Access to psychological support for young people following stoma surgery: exploring patients’ and clinicians’ perspectives. Qual Health Res. 2020;31(3):535–549. doi:10.1177/1049732320972338
11. Danielsen AK, Rosenberg J. Health related quality of life may increase when patients with a stoma attend patient education—a case-control study. PLoS One. 2014;9:e90354. doi:10.1371/journal.pone.0090354
12. Stavropoulou A, Vlamakis D, Kaba E, et al. “Living with a Stoma”: exploring the lived experience of patients with permanent colostomy. Int J Environ Res Public Health. 2021;18:8512. doi:10.3390/ijerph18168512
13. Alenezi A, Mansour E. Impact of stoma care education in minimizing the incidence of stoma skin complications. Bahrain Med Bull. 2016;38:151–153. doi:10.12816/0047489
14. Hollinworth H, Howlett S, Tallett J, et al. Professional holistic care of the person with a stoma: online learning. Br J Nurs. 2004;13:1268–1275. doi:10.12968/bjon.2004.13.21.17115
15. Black P, Notter J. Psychological issues affecting patients living with a stoma. Br J Nurs. 2021;30:S20–S32. doi:10.12968/bjon.2021.30.6.S20
16. Hinton L, Armstrong N. ‘They don’t know themselves, so how can they tell us?’: parents navigating uncertainty at the frontiers of neonatal surgery. Sociol Health Illn. 2020;42(S1):51–68. doi:10.1111/1467-9566.13073
17. Marsac ML, Kassam-Adams N, Hildenbrand AK, et al. Implementing a trauma-informed approach in pediatric health care networks. JAMA Pediatr. 2016;170(1):70. doi:10.1001/jamapediatrics.2015.2206
18. Liu Y, Wang L, Zhu L. The impact of stoma management education on the self-care abilities of individuals with an intestinal stoma. Gastrointestinal Nurs. 2023;21:S14–S21. doi:10.12968/gasn.2023.21.Sup4.S14
19. Forest-Lalande L. Best practice guidelines for ostomy care in neonates, children, and adolescents: an executive summary. J Wound Ostomy Cont Nurs. 2023;50:381–385. doi:10.1097/WON.0000000000001001
20. Aidoo E, Rajapakse D. End of life care for infants, children and young people with life-limiting conditions: planning and management: the NICE guideline 2016. Arch Dis Child Educ Pract Ed. 2018;103(6):edpract–2017–312767. doi:10.1136/archdischild-2017-312767
21. Altman L, Zurynski Y, Breen C, Hoffmann T, Woolfenden S. A qualitative study of health care providers’ perceptions and experiences of working together to care for children with medical complexity (CMC). BMC Health Serv Res. 2018;18(1):70. doi:10.1186/s12913-018-2857-8
22. Breen C, Altman L, Ging J, Deverell M, Woolfenden S, Zurynski Y. Significant reductions in tertiary hospital encounters and less travel for families after implementation of Paediatric Care Coordination in Australia. BMC Health Serv Res. 2018;18(1):751. doi:10.1186/s12913-018-3553-4
23. Sartore GM, Pourliakas A, Lagioia V. Peer support interventions for parents and carers of children with complex needs. Cochrane Database Syst Rev. 2021;2021(12). doi:10.1002/14651858.CD010618.pub2
24. Sobotka SA, Lynch E, Quinn MT, Awadalla SS, Agrawal RK, Peek ME. Unmet respite needs of children with medical technology dependence. Clin Pediatr. 2019;58(11–12):1175–1186. doi:10.1177/0009922819870251
25. Edelstein H, Schippke J, Sheffe S, Kingsnorth S. Children with medical complexity: a scoping review of interventions to support caregiver stress. Child Care Health Dev. 2017;43(3):323–333. doi:10.1111/cch.12430
26. Hakim A, Palizban E, Ahmadi Angali K. The effect of family-centered empowerment model on the Level of parents’ knowledge of children with ostomy. J Pediatr Nurs. 2015;1(4):22–31.
27. Golpazir-Sorkheh A, Ghaderi T, Mahmoudi S, Moradi K, Jalali A. Family-centered interventions and quality of life of clients with ostomy. Nurs Res Pract. 2022;2022(1):1–9. doi:10.1155/2022/9426560
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.