")
Back to Journals » Psoriasis: Targets and Therapy » Volume 15
Epidemiology and Health Care of Generalized Pustular Psoriasis in Germany – Methodology and Outcomes of Claims Data Analysis
Authors Hagenström K , Müller K, Ben-Anaya N, Augustin M
Received 20 March 2025
Accepted for publication 25 June 2025
Published 15 July 2025 Volume 2025:15 Pages 273—283
DOI https://doi.org/10.2147/PTT.S529515
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Tina Bhutani
Kristina Hagenström, Katharina Müller, Nesrine Ben-Anaya, Matthias Augustin
Institute for Health Services Research in Dermatology and Nursing (IVDP), University Medical Center Hamburg-Eppendorf (UKE), Hamburg, Germany
Correspondence: Kristina Hagenström, Institute for Health Services Research in Dermatology and Nursing (IVDP), University Medical Center Hamburg-Eppendorf (UKE), Martinistraße 52, Hamburg, 20246, Germany, Tel +49 40 741059513, Fax +49 40 74105534, Email [email protected]
Purpose: Epidemiological and health care data on generalized pustular psoriasis (GPP) show large differences in literature. This study assessed GPP epidemiology, comorbidities and health care in Germany.
Patients and Methods: Nationwide population-related German claims data were analyzed using different case definitions for internal validation.
Results: In 2019, the prevalence of GPP in Germany in adults ranged from 8 to 39 and incidence from 1 to 15 persons per 100,000. Prevalence was higher in women and increased with age. Thirty-three percent had at least one other psoriatic ICD-10 code. People with GPP had significantly more skin diseases as well as cardiovascular and mental diseases than persons without psoriasis/GPP. The average annual drug costs per capita were € 2050 and were highest in those receiving biologicals (€ 15,524). Marked differences in treatment by specialist were observed.
Conclusion: Acknowledging that the observed frequency or costs associated with GPP may be underestimated due to a few inherent limitations is important. Differences in GPP coding behavior and diagnostic accuracy may contribute to variations in epidemiology. The high disease burden is reflected by high annual costs and by significant comorbidity.
Plain Language Summary: Generalized pustular psoriasis (GPP) is a severe form of psoriasis that causes painful, pus-filled blisters on the skin. Our study, conducted in Germany, aimed to explore how common GPP is, what other health problems people with GPP experience, and how they are treated. We analyzed health insurance data from across the country, using various methods to ensure our findings were accurate.
We found that GPP is a rare condition compared to other types of psoriasis, affecting between 8 and 39 adults per 100,000 people in Germany in 2019. The number of people with GPP varied, with new cases ranging from 1 to 15 per 100,000 people. GPP was more common in women and increased with age. In addition, about a third of people with GPP also had other types of psoriasis. People with GPP had more skin diseases, heart problems, and mental health problems than people without psoriasis. The average annual cost of treating GPP was € 2050 per person, but this amount could be as high as € 15,524 for those receiving advanced treatments known as biologics. We also saw significant differences in how GPP is treated depending on which specialist was involved.
In conclusion, our study highlights that GPP is a costly condition with a high burden of additional health problems. Variations in how GPP is diagnosed and coded might explain differences in reported prevalence and costs. Improving diagnostic accuracy and treatment approaches could lead to better care and reduced expenses for patients.
Keywords: prevalence, incidence, frequency of illness, statutory health insurance data, validation
Introduction
Generalized pustular psoriasis (GPP) is a rare chronic inflammatory, very burdensome and potentially life-threatening disease. GPP shares some signs and symptoms with psoriasis vulgaris but is now a distinct disease that requires accurate diagnosis and specific treatment approaches.1 GPP is characterized by eruptions of sterile pustules on erythematous ground which mostly affect the non-acral skin,2 and by occurrence of acute flares with often severe systemic symptoms. In many cases, the flares require hospitalization.3 The frequency and duration of GPP flares differ widely among patients.3
To date, there is little and contradicting literature on the epidemiology of the disease in the general population. In published data, GPP annual prevalence varies between 0.18 and 46 per 100,000 persons4–8 and incidences between 0.06 and 0.8 per 100,000 persons.4,6 Sex differences manifest with a greater disease incidence in women compared to men, and GPP typically afflicts individuals aged between the fourth and sixth decade of life.3,4,6,9 Furthermore, little is known about the comorbidities of people with GPP. Publications suggest that between 30 and 70% also have a history of or concomitant psoriasis vulgaris.4,9
Adequate medical care for people with GPP is crucial, but robust data on patient care in Germany and evidence-based guidelines are still lacking. Such health care data are essential to develop effective and efficient health care strategies since patients with GPP require intensive outpatient and frequently inpatient treatment,10,11 resulting in higher drug costs and longer hospital stays compared to psoriasis vulgaris.11,12
Due to limited literature on this rare disease, new population-based epidemiology data as well as data on health care are of great importance for understanding the disease burden of GPP in Germany, particularly for appropriate health care planning. A related pending question is the internal validation of GPP diagnoses in claims data which might give a clue to a better understanding of the differences in published literature.
The objective of the current study was to analyze epidemiology of GPP, comorbidities and health care in Germany based on claims data. To do so, different methodological approaches were used and differences explained.
Materials and Methods
Study Design, Data Source and Study Population
This is a retrospective claims data analysis based on a representative anonymized 40% sample of a large nationwide statutory health insurance (SH) (N = 2,885,984; 56.8% women, average age 49.1 years) of all persons who were insured for at least one day between 01/01/2016 and 12/31/2020. The study population consists of insured persons who were at least 18 years old. Depending on the research question, different insurance periods were observed.
Case Definitions
In order to obtain the most valid prevalence of GPP, three distinct case definitions were applied (Table 1). To calculate GPP incidence, the case definitions were extended to include a diagnosis-free period of eight quarters before the incidence quarter. The results were validated by sensitivity analysis with a diagnosis-free period of at least 12 quarters.
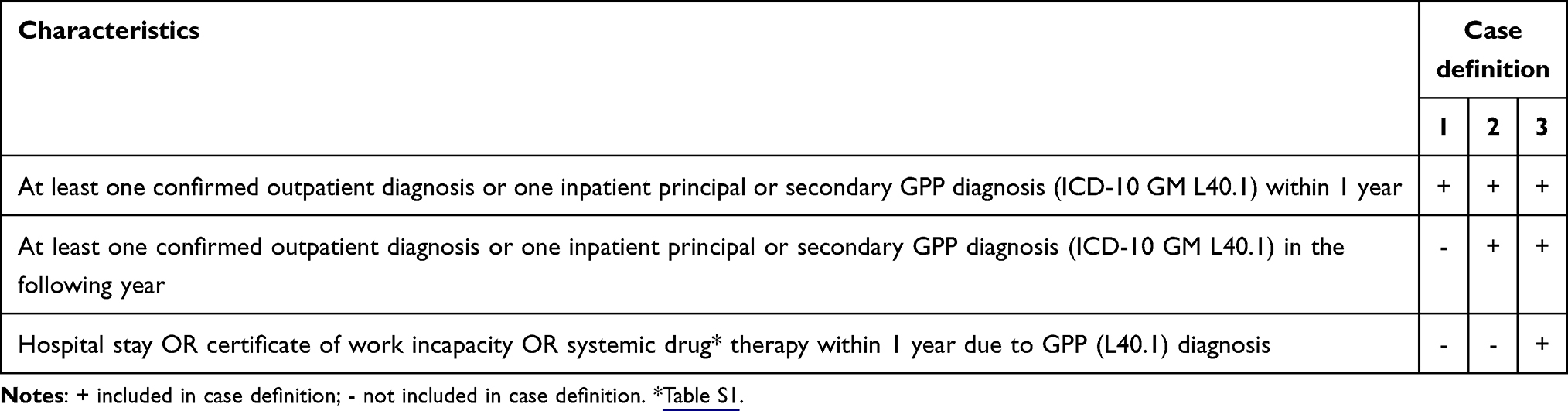 |
Table 1 Case Definitions to Determine the Prevalence of Generalized Pustular Psoriasis (GPP) |
Differential Diagnosis and Comorbidities
Miscoding of persons with a diagnosis of GPP was accounted for as follows: a) any psoriasis diagnoses (L40) among prevalent GPP in 2019 (cross-diagnoses) and b) other dermatological diseases among prevalent GPP in 2019 without a GPP diagnosis in 2018 (differential diagnoses) (Table S1). Comorbidity related to GPP to be investigated based on the literature (Table S2). Insured persons with differential diagnosis or comorbidities were included if they had at least one other main or secondary relevant diagnosis in an outpatient or inpatient setting in the GPP prevalence year 2019. Comorbidities of GPP were compared to two comparison groups, persons with psoriasis but without GPP and persons without any psoriasis diagnosis (L40).
Outpatient Care
Drug prescriptions were analyzed based on case definition 1 (Table S3). Prescribers were classified into:13 general practitioner (01–03), dermatologist (21), pediatrician (34−47), internist (23−30, 32−33), rheumatologist (12,31). For the analysis of long-term medication, at least one relevant prescription per quarter had to be available for all four quarters of a year. In addition, phototherapy (Fee schedule item, EBM Number 30430, 30,431, 10,350)13 was evaluated. In order to determine the course of drug treatment, insured persons with incident GPP in 2018 were followed up for eight quarters. The first observation quarter does not correspond to the prescription quarter.
Statistics
Epidemiology estimates are expressed per 100,000 persons. Direct standardization by age and sex was performed using the German population on 31 December of the respective year. Relative frequencies (in per cent) were calculated for categorical variables. When comparing comorbidities, the relative risk (RR) of people with GPP compared with controls was calculated and reported with the corresponding 95% confidence intervals. For the calculation of the relative risk for each comorbidity, the controls were first compared with respect to their mean age. Drug costs were considered as gross amounts without deduction of VAT and manufacturer rebates (payer perspective). Analyses were calculated using SAS version 9.4 German (SAS Institute, Cary, NC, USA).
Results
Epidemiology
In 2019, the prevalence of GPP ranged from 8 to 39 per 100,000 adults and the incidence from 1 to 15 per 100,000 adults. Extrapolated to Germany, between 5805 and 28,529 adults would likely have received a diagnosis of GPP, with incident cases estimated at 992 and 10,820 persons (Table S4). About 1.5% of prevalent persons were hospitalized due to GPP (average hospital days 17.2 days, SD: 14.02, min-max: 3–92 days) and 32.6% had at least one inpatient stay, a certificate of incapacity for work or relevant systemic medication. Different case definitions of incidence rate showed no differences. Prevalence and incidence remained stable throughout the period from 2016 to 2020. Irrespective of the case definition, the prevalence and incidence of GPP was lower in men than in women and peaked in the 60 to under 80 age group before declining in older age groups (Figure 1 - case definition 1; Figure S1 - case definition 2).
 |
Figure 1 Standardized annual prevalence and incidence rates of insured persons coded with ICD-10-L40.1 generalized pustular psoriasis (GPP) per 100.000, sex and age in 2019 (definition 1: N=875). |
Cross- and Differential Diagnosis
Cross-diagnosis showed that almost two-thirds of GPP prevalent persons had at least one other psoriasis diagnosis (case definition 1). Another skin condition (differential diagnosis) was coded in 58.2% of people with GPP (case definition 1). Psoriasis vulgaris was most commonly diagnosed as a cross or differential diagnosis (Table S5).
Comorbidity
In contrast to persons with other codings of psoriasis, those with GPP had significant differences in five conditions (Table 2). When comparing people with GPP and without any psoriasis diagnosis, people with GPP showed a significantly higher RR of skin diseases as well as cardiovascular and mental diseases. No differences in the frequency of comorbidities were found related to the case definitions.
 |
Table 2 Comorbidity of Generalized Pustular Psoriasis (GPP) in 2019: Relative Risks in Insured Persons with GPP vs Those with Psoriasis but Not GPP (Comparison Group A; N=64,047) and vs Individuals Without Psoriasis (Comparison Group B; N=2,008,03) |
Outpatient Care
Of the people with GPP, 68.1% received at least one relevant drug prescription. Of all systemic prescriptions, systemic glucocorticosteroids were prescribed most frequently (56.4%), followed by methotrexate (25.4%) (Table 3). In the group of biologics, adalimumab (6.8%) followed by secukinumab (6.3%) was prescribed most frequently.
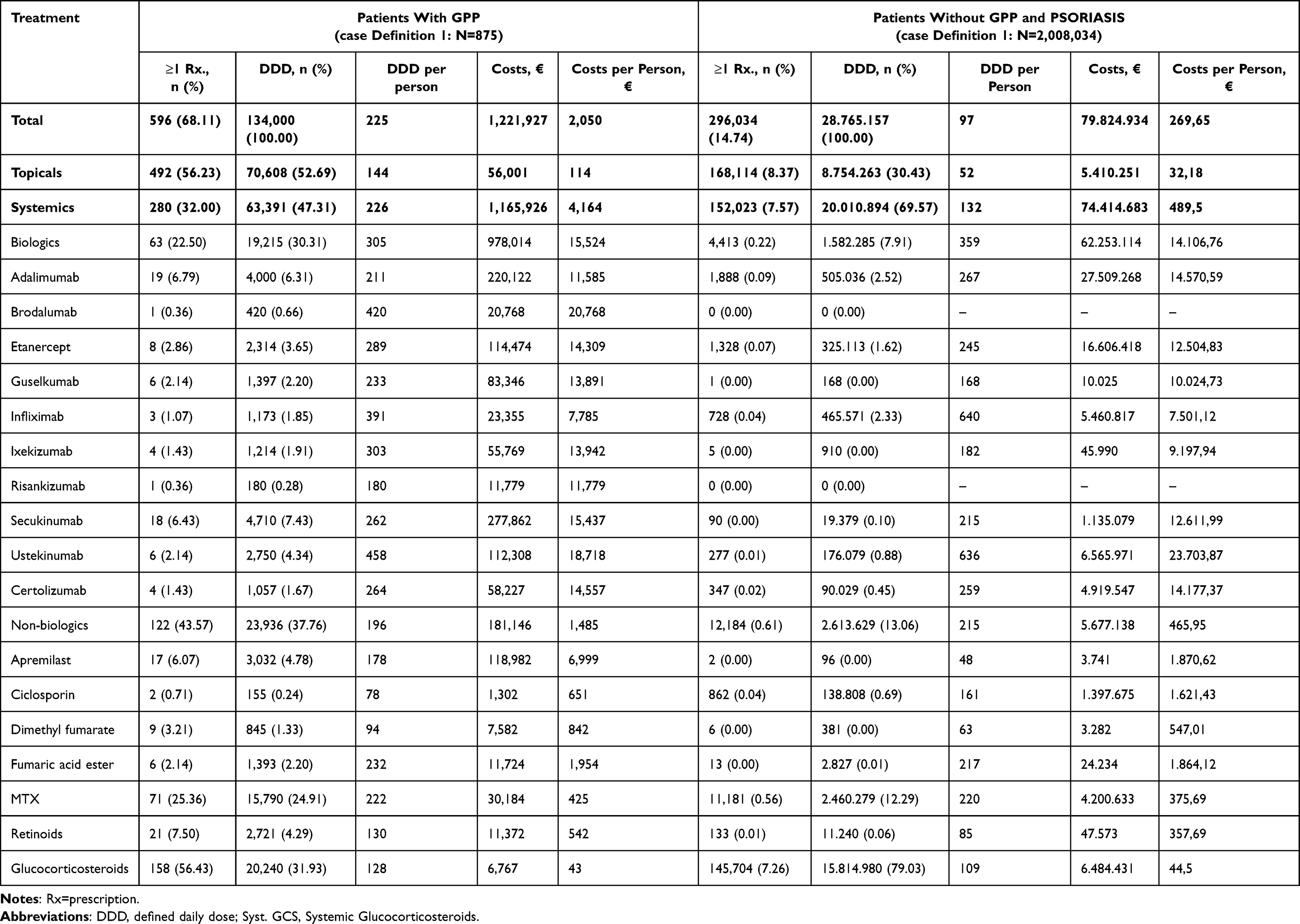 |
Table 3 Prescriptions and Defined Daily Doses (DDD) of Systemic Treatments in Patients with Generalized Pustular Psoriasis (GPP) and Without GPP and Psoriasis in 2019 |
The average total annual cost of drugs in the cohort observed was €1,22 million (€2050 per person). Total annual costs of persons receiving biologics were €978,014 (€15,524 per person) compared to €181,146 (€1485 per person) for non-biologic systemic treatments.
About 12.7% of persons with GPP received long-term drug therapy. Most of these were topical preparations (49.9%), followed by systemic conventional drugs (28.0%) and biologics (21.9%). About 3.2% of insured persons with GPP received phototherapy (Table 3).
About 50.7% of all drugs were prescribed by dermatologists, 28.1% by general practitioners, 9.5% by rheumatologists and 1.2% by internists. Biologics were prescribed mainly by dermatologists and rheumatologists (Figure 2). Systemic glucocorticosteroids were prescribed more often by general practitioners, whereas dimethyl fumarate and retinoids were mainly prescribed by dermatologists.
 |
Figure 2 Shares of daily drug doses (DDD) related to drugs prescribed for generalized pustular psoriasis (GPP) by specialist groups in 2019 (N=875). |
The drug treatments for incident persons with GPP were prescribed by a dermatologist or general practitioner in the vast majority of cases. While the proportion of persons treated by dermatologists decreased steadily over time (to 42.31% in the last quarter of observation), the proportion of persons treated by general practitioners or rheumatologists increased (Figure 3).
 |
Figure 3 Share of medical specialties being the first prescribers of drugs for incident people with generalized pustular psoriasis (GPP) in 2018 (N=334). |
Discussion
The objective of the current large-scale claims data analysis was to gain robust data on the prevalence, incidence and health care of GPP in Germany. The methodology followed previous studies showing good internal and external validity in chronic inflammatory skin diseases.14,15 Our data suggest that there are large variations in prevalence data depending on the methods of data work-up. The prevalence of GPP in countries, such as Korea (12 per 100,000)5,8 and the United States (14 per 100,000),5,8 was comparable to the observed prevalence in this study. The prevalence of GPP was lower with 1.5 per 100,000 in Sweden,4,6 0.18 per 100,000 in France,6 and 0.7 per 100,000 in Brazil.7 Differences between countries may be due to differences in study design, case definitions, coding habits, population structure and health care systems. A published German claims data study using the same selection criteria as case definition 1 described a similarly high GPP crude prevalence of 45 per 100,000.16 The incidence of GPP was 0.06 per 100,000 in France in 20016 and 0.8 per 100,000 in Sweden in 2015,4 compared with 1 and 15 per 100,000 in our study. The studies differed in the selection of incident cases according to the diagnosis-free period prior to GPP diagnosis. The French study did not include information on diagnosis-free time6 and Löfvendahl et al4 defined diagnosis-free time as ten years. Against this background, it can be assumed that the chosen diagnosis-free time of up to 3 years is too short for an accurate estimation which most likely resulted in overestimated incidences. However, the most important determinant of the high rate of GPP codings in Germany most probably is overcoding of false GPP cases. Further validation studies based on statutory health insurance (SHI) data with a longer diagnosis-free period should be sought.
The findings align with the existing literature, which indicates that GPP occurs less frequently in men than in women.3,4,6 The highest prevalence was observed in the age group 70 to under 80 across all case definitions. In other studies, the highest prevalences were observed in younger age groups, such as those between 40 to 60 or 60 to under 70 years old.3,4,6,9,17,18 Such differences are not unexpected and are likely due to the differing underlying populations, which differ significantly not only in size but also in their age structures, making them difficult to compare.
The utilization of diagnostic data from hospitals indicates that the available data (1.5% hospitalized for GPP extrapolated to 425 cases) is comparable with the hospital cases of the federal government’s health monitoring (GBE) (with 395 inpatient GPP cases in 2019).19 It can be postulated that all inpatient stays were associated with an acute GPP episode, ie flare, given that 1.5% of all inpatient stays lasted at least three days. In the study by Zema et al,10 the proportion of GPP persons experiencing a flare was found to be higher at 18%. The study also found that 36% were treated as inpatients and 53% as outpatients. When a certificate of incapacity for work due to GPP and systemic medicines is also taken into account, the proportion rises to 32.6%. Nevertheless, the proportion is likely to be overestimated when considering systemic therapies, as these therapies are also used for moderate or less severe GPP.
Concomitant psoriasis vulgaris occurred in 38.2% of persons with GPP, compared to the literature with 43% and 50%.4,9,20 RR for concomitant diseases reveals GPP is associated with significantly higher rates of skin diseases and cerebrovascular diseases compared to psoriasis but no GPP. In addition to genetic factors, a higher degree of systemic inflammation in GPP may be important. Ichthyosis, pemphigus, viral skin infections, impetigo and dermatitis are comorbidities that are raised as potential differential diagnoses for GPP. However, the SHI data do not permit to assure whether these are true comorbidities or misdiagnoses.
In the current cohort, topical therapy plays the greatest role in drug supply for persons coded with GPP. A reason may be frequent association (or confounding) with psoriasis vulgaris. Systemic drugs frequently used in the treatment of GPP include acitretin, ciclosporin, methotrexate and infliximab.10,21,22 General practitioners are distinguished by a very high utilization of systemic glucocorticosteroids. The relatively high proportion of dermatologists (56%) indicates a high demand for highly qualified specialist dermatological care for persons with GPP. A small proportion of persons with GPP received continuous drug therapy, which most probably results from the predominant interval-like occurrence of GPP (flares) and the fact that no suitable regimens for recurrence prevention had yet been developed in the observation period. With respect to treatment costs, the costs of outpatient medication often represent the largest share. A primary study determined higher drug costs of €4324 per persons with psoriasis per year than our present study (€2050).23 However, in the primary study medication use was collected for the last three months and then extrapolated to a full year, which may lead to overestimates. Furthermore, biologics are associated with higher costs compared to conventional systemic therapies,24,25 as this study also shows.
Strengths and Limitations
The fundamental strength of this analysis is the extensive data set on SHI, which offers valuable insights into the population coverage of SHI, since it covers around 90% of the German population.26 However, it is important to consider the limitations of the data and the methodology employed when interpreting the results. For instance, the demographic profiles of the various health insurance funds exhibit notable differences.27 To minimize these discrepancies, epidemiology rates were standardized. Furthermore, a study on psoriasis demonstrated that the epidemiological findings of the DAK-G data can be extrapolated without limitation to the SHI population, provided that they are standardized.14 As GPP can also present as an episodic disease, it is also possible that insured persons do not visit their physician annually, which may result in an underestimation of true prevalences and an overestimation of incidences.4 In addition, topical emollients are over-the-counter drugs not covered by SHI. This may result in an underestimation of the drug costs. Since OTC drugs are cheap, they, however, do not lead to marked changes in the drug costs for severe skin diseases.
Conclusion
According to the claims data, GPP is a rare but highly relevant disease. Determining the specific diagnosis of GPP is not trivial, and epidemiologic rates vary widely. In Germany, a marked overuse of the coding for GPP needs to be assumed since the wide case definition exceeds all international data by far. Further studies are needed to assess the extent and reason of incorrect coding in the claims data. This would also allow to control the reliability and validity of the results. The study data highlight the high disease burden of comorbidities in persons with GPP. GPP is now regarded as a distinct entity from psoriasis vulgaris. It requires diagnosis-specific management and an evidence-based guideline which is currently lacking. Patients with GPP have a high need for qualified, explicitly dermatological care. In treatment, there are differences between specialties. To fill the remaining knowledge gaps, primary health care studies, particularly well-established patient registries, are needed, and international collaboration and data exchange are key.
Data Sharing Statement
The datasets generated for the claims data cohort are not available as the use of claims data is restricted to defined people.
Ethics Approval and Informed Consent
The study was conducted according to national guidelines for the use of administrative databases.28,29 According to those guidelines, no approval of an ethical committee or patient consent was required.
Acknowledgments
We would like to thank DAK-G for their cooperation and for providing the data and to Claudia Garbe for her scientific support and assistance.
The project was financially supported by Boehringer Ingelheim Pharma (BI) GmbH & Co. KG. This was an independent, investigator-initiated study supported by BI. BI had no role in the design, analysis or interpretation of the results in this study. BI was given the opportunity to review the manuscript for medical and scientific accuracy, as well as intellectual property considerations. We acknowledge the financial support from the Open Access Publication Fund of UKE - Universitätsklinikum Hamburg-Eppendorf and DFG – German Research Foundation.
Funding
The project was financially supported by the company Boehringer Ingelheim Pharma GmbH & Co. KG.
Disclosure
Dr. Kristina Hagenström and Katharina Müller declare no conflicts of interest in this work. Dr. Nesrine Ben-Anaya has served as consultant/paid speaker for AbbVie, Almirall Incyte, Lilly and Pfizer. Prof. Matthias Augustin has served as a consultant, lecturer, researcher, and/or has received research grants from companies manufacturing drugs for chronic skin diseases, including AbbVie, Almirall, Amgen, Biogen, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Centocor, Eli Lilly, Galderma, Hexal, Incyte, Janssen, LEO, Medac, MSD, Mylan B.V., Novartis, Pfizer, Sandoz and UCB.
References
1. Zheng M, Jullien D, Eyerich K. The prevalence and disease characteristics of generalized Pustular Psoriasis. Am J Clin Dermatol. 2022;23(Suppl 1):5–12. doi:10.1007/s40257-021-00664-x
2. Wolf P, Ceovic R, Conrad C, et al. Characteristics and management of generalized pustular psoriasis (GPP): experience from the Central and Eastern Europe (CEE) GPP expert network. J Eur Acad Dermatol Venereol. 2024;38(8):1531–1542. doi:10.1111/jdv.19808
3. Kharawala S, Golembesky AK, Bohn RL, Esser D. The clinical, humanistic, and economic burden of generalized pustular psoriasis: a structured review. Expert Rev Clin Immunol. 2020;16(3):239–252. doi:10.1080/1744666X.2019.1708193
4. Löfvendahl S, Norlin JM, Schmitt-Egenolf M. Prevalence and incidence of generalized pustular psoriasis in Sweden: a population-based register study. Br J Dermatol. 2022;186(6):970–976. doi:10.1111/bjd.20966
5. Lee JY, Kang S, Park JS, Jo SJ. Prevalence of Psoriasis in Korea: a population-based epidemiological study using the Korean national health insurance database. Ann Dermatol. 2017;29(6):761–767. doi:10.5021/ad.2017.29.6.761
6. Augey F, Renaudier P, Nicolas J-F. Generalized pustular psoriasis (Zumbusch): a French epidemiological survey. Eur J Dermatol. 2006;16(6):669–673.
7. Duarte GV, Esteves de Carvalho AV, Romiti R, et al. Generalized pustular psoriasis in Brazil: a public claims database study. JAAD Int. 2022;6:61–67. doi:10.1016/j.jdin.2021.12.001
8. Kam O, Osborne S, George SE, et al. Prevalence of generalized pustular psoriasis in the United States using the all of us research database. J Eur Acad Dermatol Venereol. 2024;38(6):e536–e537. doi:10.1111/jdv.19749
9. Twelves S, Mostafa A, Dand N, et al. Clinical and genetic differences between pustular psoriasis subtypes. J Allergy Clin Immunol. 2019;143(3):1021–1026. doi:10.1016/j.jaci.2018.06.038
10. Zema CL, Valdecantos WC, Weiss J, et al. Understanding flares in patients with generalized Pustular Psoriasis documented in US electronic health records. JAMA Dermatol. 2022;158(10):1142–1148. doi:10.1001/jamadermatol.2022.3142
11. Morita A, Kotowsky N, Gao R, et al. Patient characteristics and burden of disease in Japanese patients with generalized pustular psoriasis: results from the medical data vision claims database. J Dermatol. 2021;48(10):1463–1473. doi:10.1111/1346-8138.16022
12. Hanna ML, Singer D, Valdecantos WC. Economic burden of generalized pustular psoriasis and palmoplantar pustulosis in the United States. Curr Med Res Opin. 2021;37(5):735–742. doi:10.1080/03007995.2021.1894108
13. National Association of Statutory Health Insurance Physicians [Kassenärztliche Bundesvereinigung]. Key tables [Schlüsseltabellen] [WWW document]. 2024. Available from: https://www.kbv.de/media/sp/Arztnummern_Richtlinie.pdf.
14. Hagenström K, Müller K, Garbe C, Augustin M. Prevalence of psoriasis and psoriatic arthritis in Germany - analysis of claims data. J Dtsch Dermatol Ges. 2024;22(1):45–54. doi:10.1111/ddg.15269
15. Hagenström K, Sauer K, Mohr N, et al. Prevalence and medications of atopic dermatitis in Germany: claims data analysis. Clin Epidemiol. 2021;13:593–602. doi:10.2147/CLEP.S315888
16. Schäfer I, Rustenbach SJ, Radtke M, et al. Epidemiologie der Psoriasis in Deutschland--Auswertung von Sekundärdaten einer gesetzlichen Krankenversicherung. Gesundheitswesen. 2011;73(5):308–313. doi:10.1055/s-0030-1252022
17. Jin H, Cho -H-H, Kim W-J, et al. Clinical features and course of generalized pustular psoriasis in Korea. J Dermatol. 2015;42(7):674–678. doi:10.1111/1346-8138.12863
18. Zelickson BD, Muller SA. Generalized pustular psoriasis. A review of 63 cases. Arch Dermatol. 1991;127(9):1339–1345. doi:10.1001/archderm.1991.01680080075005
19. Federal health reporting [Gesundheitsberichterstattung des Bundes]. Hospital cases per 100,000 inhabitants by age [WWW document]. 2024. Available from: https://www-genesis.destatis.de/genesis//online?operation=table&code=23131-0001&bypass=true&levelindex=1&levelid=1722584332956#abreadcrumb.
20. Kromer C, Loewe E, Schaarschmidt M-L, et al. Drug survival in the treatment of generalized pustular psoriasis: a retrospective multicenter study. Dermatol Ther. 2021;34(2):e14814. doi:10.1111/dth.14814
21. Robinson A, van Voorhees AS, Hsu S, et al. Treatment of pustular psoriasis: from the medical board of the national Psoriasis foundation. J Am Acad Dermatol. 2012;67(2):279–288. doi:10.1016/j.jaad.2011.01.032
22. Reich K, Augustin M, Gerdes S, et al. Generalized pustular psoriasis: overview of the status quo and results of a panel discussion. J Dtsch Dermatol Ges. 2022;20(6):753–771.
23. Jungen D, Augustin M, Langenbruch A, et al. Cost-of-illness of psoriasis - results of a German cross-sectional study. J Eur Acad Dermatol Venereol. 2018;32(1):174–180. doi:10.1111/jdv.14543
24. Fonia A, Jackson K, Lereun C, et al. A retrospective cohort study of the impact of biologic therapy initiation on medical resource use and costs in patients with moderate to severe psoriasis. Br J Dermatol. 2010;163(4):807–816. doi:10.1111/j.1365-2133.2010.09944.x
25. Le Moigne M, Sommet A, Lapeyre-Mestre M, et al. Healthcare cost impact of biological drugs compared with traditional systemic treatments in psoriasis: a cohort analysis in the French insurance database. J Eur Acad Dermatol Venereol. 2014;28(9):1235–1244. doi:10.1111/jdv.12318
26. Swart E. Health care utilization research using secondary data. In: Janssen C, Swart E, von Lengerke T, editors. Health Care Utilization in Germany. New York, NY: Springer; 2014:63–86.
27. Hoffmann F, Icks A. Unterschiede in der Versichertenstruktur von Krankenkassen und deren Auswirkungen für die Versorgungsforschung: Ergebnisse des Bertelsmann-Gesundheitsmonitors. Gesundheitswesen. 2012;74(5):291–297. doi:10.1055/s-0031-1275711
28. Hoffmann W, Latza U, Baumeister SE, et al. Guidelines and recommendations for ensuring Good Epidemiological Practice (GEP): a guideline developed by the German Society for Epidemiology. Eur J Epidemiol. 2019;34(3):301–317. doi:10.1007/s10654-019-00500-x
29. Swart E, Schmitt J. STandardized Reporting Of Secondary data Analyses (STROSA)—Vorschlag für ein Berichtsformat für Sekundärdatenanalysen. Z Evid Fortbild Qual Gesundhwes. 2014;108(8–9):511–516. doi:10.1016/j.zefq.2014.08.022
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Epidemiological Characteristics of Chronic Viral Hepatitis in Kazakhstan: Data from Unified Nationwide Electronic Healthcare System 2014–2019
Ashimkhanova A, Syssoyev D, Gusmanov A, Yesmembetov K, Yespotayeva A, Abbay A, Nurpeissova A, Sarria-Santamera A, Gaipov A
Infection and Drug Resistance 2022, 15:3333-3346
Published Date: 27 June 2022
Assessment of the Prevalence and Incidence of COVID-19 in Saudi Arabia
Alyahyawi HE, Alharbi RA, Alatawi SK, Ahmed WAM, Almalki SSR
Journal of Multidisciplinary Healthcare 2023, 16:227-236
Published Date: 24 January 2023
Association of Triglyceride Glucose Index with Prevalence and Incidence of Diabetic Retinopathy in a Singaporean Population
Neelam K, Aung KCY, Ang K, Tavintharan S, Sum CF, Lim SC
Clinical Ophthalmology 2023, 17:445-454
Published Date: 2 February 2023
Use of Linked Nordic Registries for Population Studies in Hematologic Cancers: The Case of Multiple Myeloma
Abildgaard N, Freilich J, Anttila P, Bent-Ennakhil N, Ma Y, Lassenius M, Ørstavik S, Toppila I, Waage A, Turesson I, Hansson M
Clinical Epidemiology 2023, 15:987-999
Published Date: 18 September 2023
Type 2 Diabetes, the Epidemic: Trends in Prevalence and Incidence, 2004-2020
Overbeek JA, Nijpels G, Swart KMA, Blom MT, Elders PJM, Herings RMC
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1503-1509
Published Date: 28 March 2024