")
Back to Journals » Clinical Ophthalmology » Volume 19
Epidemiology, Tear Film, and Meibomian Gland Dysfunction in Facial Palsy: A Comparative Analysis
Authors Guerrero-de Ferran C, Bastán-Fabián D , del Castillo-Morales A , Rivera-Alvarado IJ , Valdez García JE
Received 29 July 2024
Accepted for publication 26 November 2024
Published 8 January 2025 Volume 2025:19 Pages 93—100
DOI https://doi.org/10.2147/OPTH.S481124
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Caroline Guerrero-de Ferran, Daniel Bastán-Fabián, Alfredo del Castillo-Morales, I Jocelyn Rivera-Alvarado, Jorge E Valdez García
School of Medicine, Tecnologico de Monterrey, Monterrey, NL, México
Correspondence: Jorge E Valdez García, School of Medicine, Tecnologico de Monterrey, Av. Ignacio Morones Prieto 3000, Colonia Los Doctores, Monterrey, NL, CP 64710, México, Tel +52 81 88 88 05 51, Email [email protected]
Purpose: To compare the meibographies and dry eye parameters of paretic vs non-paretic sides of patients with a facial palsy diagnosis.
Patients and Methods: Twenty patients with unilateral facial palsy were recruited and the severity of the disease was staged using the House-Brackmann scale. A comprehensive dry eye evaluation was performed using the Oculus 5M Keratograph. A Pearson correlation coefficient was performed to determine correlation strength between House-Brackmann score and Meibomian gland atrophy. Meibographies were analyzed via ImageJ software to determine the affected area, and they were compared to the observer manual score. Cohen’s Kappa coefficient was calculated to compare agreement between manual and ImageJ meibography scoring.
Results: Tear breakup time was reduced in the affected side (p = 0.21), tear meniscus height was much greater in the non-affected side (p = 0.02). Finally, Meibomian gland alterations were more evident in the affected side, with upper Meibomian glands having a loss of 29.55 ± 13.31% (p = 0.03) and lower glands presenting a loss of 44.44 ± 16.9% (p =< 0.001). Pearson correlation coefficient between House-Brackmann score and Meibomian gland atrophy was 0.841 (p < 0.001 [95% CI: 0.64– 0.94]). Cohen’s kappa coefficient was 0.643 (p < 0.001).
Conclusion: A clear difference in Meibomian gland and tear film dynamics can be observed in paretic vs non-paretic sides. A greater House-Brackmann score was correlated with a greater Meibomian gland atrophy area. A strong positive correlation is seen between the House-Brackmann score and Meibomian gland atrophy. Software-based analysis also showed a greater glandular area loss when compared to clinician’s analysis. The level of agreement was moderate, so disparities are observed, especially in grade 2 Meibomian gland dropout where the least level of agreement was seen in cross tabulation. This study further incentivizes multimodal patient evaluation, which has been a growing area of interest in healthcare.
Keywords: Meibomian gland dysfunction, facial palsy, meibography, dry eye disease, orbicularis oculi
Introduction
Facial palsy (FP) is the most common cranial neuropathy in clinical practice, with an annual incidence of 30–40 cases per 100,000 people.1–3 If left untreated, it can result in long-term physical and psychological sequelae with a marked decrease in quality of life.4 Diagnosis is eminently clinical by means of the House-Brackmann scale, which consists of 6 stages of increasing severity; the Sunnybrook scale is also employed and is considered a more comprehensive scale due to its more ophthalmologic-driven grading scheme.4 There are many etiologies, with idiopathic (also known as Bell’s palsy), congenital, traumatic, infectious, and neoplastic origins. Bell’s palsy is, by far, the most frequent cause of FP.4–6
Dry eye disease (DED) affects approximately 100 million people worldwide but there is a massive number of undiagnosed patients.7 DED and Meibomian gland dysfunction (MGD) are current areas of interest in ophthalmology with an upward trend in research. In 2007, the Tear Film and Ocular Surface Society (TFOS) presented an initiative called the Dry Eye Workshop (TFOS: DEWS).8 They defined DED as a multifactorial disease, characterized by the loss of tear film (TF) homeostasis manifested by ocular surface symptoms, where TF instability and hyperosmolarity, ocular surface inflammation and damage, as well as neurosensory abnormalities play a fundamental role.9 MGD is considered the most important cause of DED since the majority of patients have been found to present some degree of this ailment.10,11
Regarding the eye and orbit, FP causes upper and lower eyelid dysfunction due to orbicularis oculi impairment, resulting in an inability to completely close the eyelids in most cases and an increase in ocular surface damage due to exposure to air, foreign bodies, and pathogens. Likewise, TF dynamics are altered due to an uneven distribution of tears in the ocular surface and their drainage through the lacrimal puncta, increased evaporation due to increased width of the palpebral fissure, and MGD.3,12 MGD due to FP is an interesting phenomenon, in which the lipid layer of the tear film is diminished due to Meibomian gland stasis and atrophy secondary to exposure. These glands are surrounded by Riolan’s muscle, a subdivision of striated muscle, separate from the pretarsal orbicularis oculi muscle.13,14 This muscle aids in glandular drainage and its weakness ultimately leads to obstruction and atrophy of the Meibomian glands.2,14–16
The importance of MGD in DED lies in the multi-layer nature of TF. Meibomian glands secrete the lipid component of the tears, which contribute to increased lubrication, surface wettability, and tear breakup time (TBUT).2,8,10,16–23 This lipid layer also helps in tear distribution in an evenly manner, as well as preventing tear spillage from the palpebral margins and sealing the eyelids during sleep.8,15 MGD is diagnosed based on a myriad of clinical features, such as conjunctival blood vessel ingurgitation, foamy tear film, Meibomian gland ostial dilation and increased viscosity of their secretions, and corneal epithelial damage secondary to TF instability.14,21,24,25 Studies such as TBUT, corneal staining, Schirmer’s test, and meibography are of great assistance during consultation.6,14,26–31
A novel tool in DED diagnosis is the JENVIS Dry Eye Report, which consists of a battery of tests such as tear meniscus height (TMH), TBUT, Dry Eye Questionnaire (DEQ), Infrared non-contact meibography, conjunctivochalasis, and conjunctival hyperemia measured by an Oculus 5M Keratograph (®K5 M; Oculus GmbH, Wetzlar, Germany).11–15 It is important to note that the meiboscore included in the 5M Keratograph meibographer is prone to over and/or underestimation by the user, so software analysis of the Meibomian glandular area is a promising tool in aiding classification by reducing inter- and intra-observer variation. These devices and software aides are part of an ever-increasing trend in multimodal patient evaluation, which offers better patient outcomes, both in clinical aspects and in patient satisfaction/education indicators.
The aim of this study was to compare the tear film parameters, percentage of Meibomian glandular atrophy, and conjunctival hyperemia of patients’ paretic versus non-paretic hemifaces by means of the 5M Keratograph. Furthermore, a comparison between the degree of glandular area loss granted manually and by the ImageJ software (Research Services Branch, National Institute of Mental Health, Bethesda, Maryland, USA) was also performed to determine the difference between manual vs automated grading of glandular dropout.
Materials and Methods
This study was approved by the Comité de Ética en Investigación (CEI) and Comité de Investigación (CI) of the Zambrano-Hellion, Hospital ethics committee in February 2020 according to the Helsinki declaration under the registration number: P000302-CDLPPFU. Informed consent was obtained from all participants. An observational, cross-sectional, and comparative pilot study was performed. Twenty patients with an FP diagnosis were selected, all of which were referred to our institution from two urban third-level healthcare centers. Inclusion criteria consisted of patients over the age of 18 with a unilateral FP diagnosis of any etiology (Bell’s, congenital, vascular, cranioencephalic trauma, neoplastic or infectious). Exclusion criteria included any history of eyelid surgery and/or facial trauma.
Disease staging was done using the House-Brackmann scale, DED evaluation was performed by a different researcher, and it consisted of the Ocular Surface Disease Index (OSDI) score (translated to Spanish), tear meniscus height (TMH), TBUT, infrared meibography, and conjunctival hyperemia analysis using an Oculus 5M Keratograph (®K5 M; Oculus GmbH, Wetzlar, Germany). Meibographies were classified by the meiboscore scale, where grade 0 represents no loss whatsoever, grade 1 represents <33% of glandular area loss, grade 2 represents 33–66% area loss, and grade 3 represents >66% area loss. These were later analyzed using ImageJ software (Research Services Branch, National Institute of Mental Health, Bethesda, Maryland, USA) to determine the percentage of glandular area loss.
The sample calculation was done using a formula that considers the population proportion in an infinite population, in this case, the Mexican population of 126 million people. A confidence level of 85% was included, as well as a population proportion of 0.02 (based on a FP prevalence of 2–3 per 10,000 people), a margin of error of 5%, which yielded a sample size of 17 patients. An infinite population in this study reflects a sample size of <5% of the total population.
Descriptive statistics were reported, namely the sex and age of the recruited patients, as well as the etiology of their FP. Central dispersion measurements such as mean and range for descriptive statistics, and the mean and standard deviation for the dry eye parameters were also included. Normality of data was assessed via the Kolmogorov–Smirnov. A comparative analysis was performed using the t-student test for the evaluation of paretic vs non-paretic sides. A p value of less than 0.05 was considered statistically significant. A Pearson correlation coefficient was performed to determine the strength of the correlation between the House-Brackmann scale and the degree of Meibomian gland atrophy. Finally, a Cohen’s kappa coefficient was calculated to determine the level of agreement between manual meibography scoring and software assisted meibography scoring.
Results
In our study, 20 patients were recruited, of which 11 patients (55%) were female, the mean age of diagnosis was 57.80 ± 18.28 years (range of 22–80 years), and the evolution time of the disease was 67.05 ± 156.8 months (range of 3–720 months). Disease etiology was Bell’s palsy in 10 patients (50%), the rest of the etiologies are summarized in Table 1. In terms of laterality, the most affected side was the left hemiface in 13 patients (65%). Disease severity was predominantly grade IV on the House-Brackmann scale (8 patients, 40%) and the rest being reported in Figure 1. All the patients were currently under topical therapy with sodium hyaluronate as per needed and 18 had already undergone facial exercise therapy.
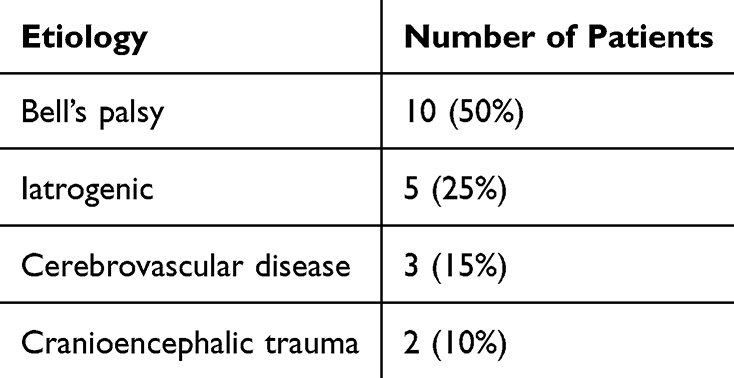 |
Table 1 Facial Palsy Etiologies |
 |
Figure 1 Severity distribution of Facial Palsy, measured by HB scale. A Pie Chart describing the percentage of patients with different HB score. |
TF comparative analysis demonstrated a statistically significant difference (p = 0.02) in TMH when comparing paretic vs non-paretic sides, with an increased TMH in the paretic hemiface. Another finding was the difference in TBUT, where the paretic side presented a diminished TBUT compared to the non-paretic side, but it was not statistically significant (p = 0.21). Conjunctival hyperemia was more evident in the affected side and was statistically significant (p = 0.02) and OSDI questionnaire reported a mean score of 64.947 ± 19.79, which reflected a severe grade of dry eye symptomatology. These findings are summarized in Table 2.
 |
Table 2 Comparison Analysis of Paretic vs Non-Paretic Sides |
The Pearson correlation analysis yielded a correlation coefficient of 0.841 (p < 0.001 [95% CI: 0.64–0.94]) between House-Brackmann scale and Meibomian gland dropout. Meibography analysis using ImageJ software yielded statistically significant results when comparing upper and lower Meibomian gland area percentage loss, especially in the lower eyelid. Cohen’s kappa coefficient was 0.643 and was statistically significant (p < 0.001).
Discussion
Our study describes the changes in TF dynamics and MGD in patients with unilateral FP and highlights the differences when comparing the affected vs unaffected sides. The epidemiology reported in our sample reflects the study by Tavares-Brito et al,32 where 920 patients with FP were evaluated, and most of them were females with Bell’s palsy as the most common etiology.32 However, certain differences such as age of presentation and evolution time of the disease were observed, with both being greater in our study, although with a much smaller sample size. This could be explained by geographic and cultural differences, since patients in Mexico tend to forgo medical counsel well into advanced disease, this creating a great disparity in presentation and prognosis.
When assessing DED by the 5M Keratograph JENVIS Dry Eye Report, we noticed a lack of research in the literature, but our findings reflect other results from studies by Wan et al2 and Altin Ekin et al,33 where TBUT was decreased in the affected side when compared with the unaffected side. The lack of statistical significance can be explained by a small sample size due to the timeframe in which this study was performed (COVID-19 pandemic). An interesting finding in our study was the increased TMH in the paretic side since we could not find other studies reporting the same result. The differences in TMH between sides could be due to the loss of muscular tone and increased laxity of the lower eyelid, thus increasing TMH at the expense of a greater palpebral fissure height.
Another crucial factor that cannot be overlooked in glandular dynamics is the orbicularis oculi function, specifically Riolan’s muscle. This muscle contributes to Meibomian gland drainage during blinking, thus integrating the lipid layer component into the tear film.8 The importance of this layer lies in its ability to diminish the surface tension of the tear film, thus preventing tear “spillage” over the palpebral margin. In addition to this, the lipid component helps in preventing evaporation of tears and improves lubrication and distribution over the eyeball.34–37 Thus, when the paretic hemiface tries to blink, Riolan’s muscle cannot contract properly, leading to improper drainage of Meibomian glands. It was unexpected for patients to have a greater TMH since tear spillage would be greater in a diminished lipid content, but reflex tearing could also be an explanation for this, and future studies could look into tear osmolarity.
Furthermore, there is very little research on infrared meibographies in patients with FP. This study contributes to the structural and qualitative analysis of these glands. The difference in upper and lower glandular loss area when comparing the paretic vs non-paretic side was evident, as well as statistically significant (p=0.0374, and p < 0.001, respectively). The correlation analysis yielded a strong positive correlation between House-Brackmann score and the Meibography glandular dropout score. This is because a higher HB score entails a greater degree of FP and, as a result, a greater degree of glandular atrophy due to exposure. However, due to the small sample, a great degree of uncertainty about the strength of the correlation is present. Further studies with greater sample sizes are warranted to clarify this finding.
Although other factors, such as hormones, environmental insults such as air pollution, geographical relative humidity, and Demodex folliculorum infestation contribute to MGD, this difference between healthy and affected sides may be explained by the FP itself. The disease mechanism consists of glandular obstruction, exposure, and eventual atrophy due to incomplete blinking and Riolan’s muscle dysfunction.8,15 Most of the patients in the study presented with a grade IV on the House Brackmann scale, which corresponds to incomplete blinking, and the effects of this are in accordance with previous findings.38 Although there are different MGD staging scales, evaluator experience plays an important role in detecting the percentage of glandular atrophy. In Figure 2, we present a female patient with right-sided FP; if the Meiboscore proposed by Arita et al39 is used, a grade of 1 and 0 can be established in the right and left upper eyelids, respectively. However, using ImageJ software, we determined both as grade 1, thus demonstrating a clear difference between human and computer evaluation. Cohen’s kappa yielded a moderate level of agreement between manual and software-assisted meibography scoring and was statistically significant. This fact highlights the potential implementation of image analysis software in the classification of MGD, especially in grade 2 meibographies where the least level of agreement was seen in crosstabulation.
 |
Figure 2 Upper eyelid meibographies of a 38-year-old female patient with right-sided facial palsy. Area of glandular loss analysis was made with ImageJ. (A) Upper right eyelid. (B) Upper left eyelid. (C) Upper right eyelid with 27% loss of glandular area as estimated by ImageJ. (D) Upper left eyelid with 15% loss of glandular area as estimated by ImageJ. |
The degree to which the glands are affected also appears to be different depending on the vertical axis, with the lower lids being more affected when comparing them to their upper counterpart. In Figure 3, a male patient presented a greater loss in the paretic side, but it was even more evident in the lower glands, where 50% loss was observed while the upper glands presented a loss of 28%. This may be explained by the increased laxity of the eyelid and the consequent exposure of the glands to environmental factors.
 |
Figure 3 Lower eyelid meibographies of a 76-year-old male patient with right-sided facial palsy. Area of glandular loss analysis was made with ImageJ. (A) Upper right eyelid with 33% loss of glandular area. (B) Upper left eyelid with 28% loss of glandular area. (C) Lower right eyelid with 50% loss of glandular area. (D) Left lower eyelid with 28% loss of glandular area. |
This study can expand its horizons even further, such as evaluating disease progression with different treatment modalities. Likewise, lipid interferometry could prove to be an important tool for evaluating the TF lipid layer in these patients. A limitation in our study was the small sample size, but it stands to reason that an even greater sample could improve the statistical power of the study. Another limitation was the use of the House Brackmann scale as the main grading of severity for facial palsy. Even though it is a mostly subjective tool, it was included because it is the most widely used grading scale for facial palsy, it is fast and relatively easy to do. The CADS and Sunnybrook scales would have been better options for grading FP but, due to hospital policy, patients were not evaluated by these means. The CADS and Sunnybrook scales offer several objective measures of periocular facial nerve function, and they will be surely utilized in future research projects.40
Conclusion
In summary, patients with a FP diagnosis should be evaluated thoroughly with a complete DED workup and should be treated accordingly. It is crucial to evaluate the tear film in these patients, as well as the Meibomian glands, because of all the implications in quality of life that FP can entail, including the issues associated with DED. There is still much to be investigated from the Meibomian glands in patients with FP, from their structural changes to their functional alterations, the former can be evaluated with infrared meibography as in our study, while the latter can be investigated via tear lipid interferometry.
Some practical implications of this study include the importance of correctly evaluating FP patients due to the TF alterations that arise from ocular exposure, as well as the implementation of image processing software to standardize the percentage of glandular atrophy when evaluating patients not only with an FP diagnosis but as a tool in improving patient care and outcomes in all DED patients. Overall, this study further incentivizes multimodal patient evaluation, which has been a growing area of interest in healthcare.
Acknowledgments
The abstract for this paper was presented at the 2023 ARVO Conference in New Orleans, Louisiana, as a poster presentation. The poster’s abstract was published in the IOVS abstract journal and can be consulted in the following link: Facial Palsy and the Ocular Surface: Epidemiology, Tear Film, and Meibomian gland alteration analysis. | IOVS | ARVO Journals. Likewise, this paper has also been uploaded as a preprint in medRxiv.org and can be found in the following link: https://www.medrxiv.org/content/10.1101/2023.07.24.23293013v1
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gilchrist JM. Seventh cranial neuropathy. Semin Neurol. 2009;29(1):5–13. PMID: 19214928. doi:10.1055/s-0028-1124018
2. Zhao H, Wu SN, Cheng Z, et al. Mean tear-film lipid layer thickness and video display terminal time as risk factors for abnormal blinking in children. Front Med. 2021;8:785901. PMID: 34938751; PMCID: PMC8687116. doi:10.3389/fmed.2021.785901
3. Bergeron CM, Moe KS. The evaluation and treatment of upper eyelid paralysis. Facial Plast Surg. 2008;24(2):220–230. PMID: 18470834. doi:10.1055/s-2008-1075838
4. Kanerva M, Jonsson L, Berg T, et al. Sunnybrook and House-Brackmann systems in 5397 facial gradings. Otolaryngol Head Neck Surg. 2011;144(4):570–574. PMID: 21493237. doi:10.1177/0194599810397497
5. Chang YS, Choi JE, Kim SW, et al. Prevalence and associated factors of facial palsy and lifestyle characteristics: data from the Korean National Health and Nutrition Examination Survey 2010–2012. BMJ Open. 2016;6(11):e012628. PMID: 28157670; PMCID: PMC5128953. doi:10.1136/bmjopen-2016-012628
6. Melvin TAN, Limb CJ. Overview of facial paralysis: current concepts. Facial Plast Surg. 2008;24(2):155–163. doi:10.1055/s-2008-1075830
7. Shah CT, Blount AL, Nguyen EV, Hassan AS. Cranial nerve seven palsy and its influence on meibomian gland function. Ophthalmic Plast Reconstr Surg. 2012;28(3):166–168. PMID: 22327637. doi:10.1097/IOP.0b013e31823f2f82
8. Arita R, Kawashima M, Ito M, et al. Clinical safety and efficacy of vitamin D3 analog ointment for treatment of obstructive meibomian gland dysfunction. BMC Ophthalmol. 2017;17(1):84. PMID: 28592257; PMCID: PMC5463421. doi:10.1186/s12886-017-0482-7
9. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II definition and classification report. Ocular Surf. 2017;15(3):276–283. PMID: 28736335. doi:10.1016/j.jtos.2017.05.008
10. Nichols KK. The international workshop on meibomian gland dysfunction: introduction. Invest Ophthalmol Vis Sci. 2011;52(4):1917–1921. PMID: 21450912; PMCID: PMC3072156. doi:10.1167/iovs.10-6997
11. Rico-Del-Viejo L, Benítez-Del-Castillo JM, Gómez-Sanz FJ, et al. The influence of meibomian gland loss on ocular surface clinical parameters. Cont Lens Anterior Eye. 2019;42(5):562–568. PMID: 30981662. doi:10.1016/j.clae.2019.04.004
12. Chu EA, Byrne PJ. Treatment considerations in facial paralysis. Facial Plast Surg. 2008;24(2):164–169. PMID: 18470827. doi:10.1055/s-2008-1075831
13. Lipham WJ, Tawfik HA, Dutton JJ. A histologic analysis and three-dimensional reconstruction of the muscle of Riolan. Ophthalmic Plast Reconstr Surg. 2002;18(2):93–98. PMID: 11897949. doi:10.1097/00002341-200203000-00002
14. Call CB, Wise RJ, Hansen MR, et al. In vivo examination of meibomian gland morphology in patients with facial nerve palsy using infrared meibography. Ophthalmic Plast Reconstr Surg. 2012;28(6):396–400. PMID: 22836800. doi:10.1097/IOP.0b013e3182611641
15. Nelson JD, Shimazaki J, Benitez-del-Castillo JM, et al. The international workshop on meibomian gland dysfunction: report of the definition and classification subcommittee. Invest Ophthalmol Vis Sci. 2011;52(4):1930–1937. PMID: 21450914; PMCID: PMC3072158. doi:10.1167/iovs.10-6997b
16. Takahashi Y, Kakizaki H. Meibomian gland dysfunction in cranial nerve VII palsy. Ophthalmic Plast Reconstr Surg. 2015;31(3):179–181. PMID: 25098447. doi:10.1097/IOP.0000000000000235
17. Takahashi Y, Watanabe A, Matsuda H, et al. Anatomy of secretory glands in the eyelid and conjunctiva: a photographic review. Ophthalmic Plast Reconstr Surg. 2013;29(3):215–219. PMID: 23381567. doi:10.1097/IOP.0b013e3182833dee
18. Chhadva P, Goldhardt R, Galor A. Meibomian gland disease: the role of gland dysfunction in dry eye disease. Ophthalmology. 2017;124(11S):S20–S26. PMID: 29055358; PMCID: PMC5685175. doi:10.1016/j.ophtha.2017.05.031
19. Foulks GN, Bron AJ. Meibomian gland dysfunction: a clinical scheme for description, diagnosis, classification, and grading. Ocul Surf. 2003;1(3):107–126. PMID: 17075643. doi:10.1016/s1542-0124(12)70139-8
20. Obata H. Anatomy and histopathology of the human lacrimal gland. Cornea. 2006;25(10 Suppl 1):S82–9. PMID: 17001201. doi:10.1097/01.ico.0000247220.18295.d3
21. Arita R, Fukuoka S, Morishige N. New insights into the morphology and function of meibomian glands. Exp Eye Res. 2017;163:64–71. PMID: 28950939. doi:10.1016/j.exer.2017.06.010
22. Tomlinson A, Bron AJ, Korb DR, et al. The international workshop on meibomian gland dysfunction: report of the diagnosis subcommittee. Invest Ophthalmol Vis Sci. 2011;52(4):2006–2049. PMID: 21450918; PMCID: PMC3072162. doi:10.1167/iovs.10-6997f
23. Mathers WD. Ocular evaporation in meibomian gland dysfunction and dry eye. Ophthalmology. 1993;100(3):347–351. PMID: 8460004. doi:10.1016/s0161-6420(93)31643-x
24. Garza-Leon M, Ramos-Betancourt N, Beltrán-Diaz de la Vega F, et al. Meibography. A new technology for the evaluation of Meibomian glands. Revista Mexicana de Oftalmologia. 2017;91(4):165–171. doi:10.1016/j.mexoft.2016.04.007
25. Wong S, Srinivasan S, Murphy PJ, et al. Comparison of meibomian gland dropout using two infrared imaging devices. Cont Lens Anterior Eye. 2019;42(3):311–317. PMID: 30413376. doi:10.1016/j.clae.2018.10.014
26. Robin JB, Jester JV, Nobe J, et al. In vivo transillumination biomicroscopy and photography of meibomian gland dysfunction. A clinical study. Ophthalmology. 1985;92(10):1423–1426. PMID: 4069605. doi:10.1016/s0161-6420(85)33848-4
27. Wise RJ, Sobel RK, Allen RC. Meibography: a review of techniques and technologies. Saudi J Ophthalmol. 2012;26(4):349–356. doi:10.1016/j.sjopt.2012.08.007
28. Pult H, Riede-Pult BH. Non-contact meibography: keep it simple but effective. Cont Lens Anterior Eye. 2012;35(2):77–80. PMID: 21885325. doi:10.1016/j.clae.2011.08.003
29. Pult H, Nichols JJ. A review of meibography. Optom Vis Sci. 2012;89(5):E760–9. PMID: 22488268. doi:10.1097/OPX.0b013e3182512ac1
30. Nichols JJ, Berntsen DA, Mitchell GL, et al. An assessment of grading scales for meibography images. Cornea. 2005;24(4):382–388. PMID: 15829792. doi:10.1097/01.ico.0000148291.38076.59
31. Pflugfelder SC, Tseng SC, Sanabria O, et al. Evaluation of subjective assessments and objective diagnostic tests for diagnosing tear-film disorders known to cause ocular irritation. Cornea. 1998;17(1):38–56. PMID: 9436879. doi:10.1097/00003226-199801000-00007
32. Tavares-Brito J, van Veen MM, Dusseldorp JR, et al. Facial palsy-specific quality of life in 920 patients: correlation with clinician-graded severity and predicting factors. Laryngoscope. 2019;129(1):100–104. PMID: 30208215. doi:10.1002/lary.27481
33. Ekın MA, Ugurlu SK, Imre SS, et al. The role of meibomian gland dysfunction on the development of dry eye disease in patients with facial nerve palsy. Arq Bras Oftalmol. 2021;85(2):128–135. PMID: 34431896. doi:10.5935/0004-2749.20220021
34. Knop E, Knop N, Millar T, et al. The international workshop on meibomian gland dysfunction: report of the subcommittee on anatomy, physiology, and pathophysiology of the meibomian gland. Invest Ophthalmol Vis Sci. 2011;52(4):1938–1978. PMID: 21450915; PMCID: PMC3072159. doi:10.1167/iovs.10-6997c
35. Kojima T, Dogru M, Kawashima M, et al. Advances in the diagnosis and treatment of dry eye. Prog Retin Eye Res. 2020;78:100842. PMID: 32004729. doi:10.1016/j.preteyeres.2020.100842
36. Chan TCY, Chow SSW, Wan KHN, et al. Update on the association between dry eye disease and meibomian gland dysfunction. Hong Kong Med J. 2019;25(1):38–47. PMID: 30713149. doi:10.12809/hkmj187331
37. Willcox MDP, Argüeso P, Georgiev GA, et al. TFOS DEWS II tear film report. Ocul Surf. 2017;15(3):366–403. PMID: 28736338; PMCID: PMC6035753. doi:10.1016/j.jtos.2017.03.006
38. Wan T, Jin X, Lin L, Xu Y, Zhao Y. Incomplete blinking may attribute to the development of meibomian gland dysfunction. Curr Eye Res. 2015;41(2):179–185. doi:10.3109/02713683.2015.1007211
39. Arita R, Minoura I, Morishige N, et al. Development of definitive and reliable grading scales for meibomian gland dysfunction. Am J Ophthalmol. 2016;169:125–137. doi:10.1016/j.ajo.2016.06.025
40. Malhotra R, Ziahosseini K, Litwin A, Nduka C, El-Shammah N. CADS grading scale: towards better grading of ophthalmic involvement in facial nerve paralysis. Br J Ophthalmol. 2015;100(6):866–870. doi:10.1136/bjophthalmol-2015-307167
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Autologous Platelet‐Rich Plasma Drops for Evaporative Dry Eye Disease from Meibomian Gland Dysfunction: A Pilot Study
Murtaza F, Toameh D, Chiu HH, Tam ES, Somani S
Clinical Ophthalmology 2022, 16:2199-2208
Published Date: 6 July 2022
Pulsed Light Therapy in the Management of Dry Eye Disease: Current Perspectives
Barbosa Ribeiro B, Marta A, Ponces Ramalhão J, Marques JH, Barbosa I
Clinical Ophthalmology 2022, 16:3883-3893
Published Date: 24 November 2022
Prevalence of Dry Eye Disease Among Individuals Scheduled for Cataract Surgery in a Norwegian Cataract Clinic
Graae Jensen P, Gundersen M, Nilsen C, Gundersen KG, Potvin R, Gazerani P, Chen X, Utheim TP, Utheim ØA
Clinical Ophthalmology 2023, 17:1233-1243
Published Date: 27 April 2023
A Randomized, Controlled Trial Comparing Tearcare® and Cyclosporine Ophthalmic Emulsion for the Treatment of Dry Eye Disease (SAHARA)
Ayres BD, Bloomenstein MR, Loh J, Chester T, Saenz B, Echegoyen J, Kannarr SR, Perez VL, Rodriguez TC, Dickerson Jr JE
Clinical Ophthalmology 2023, 17:3925-3940
Published Date: 18 December 2023
Evaluation of Perfluorohexyloctane Eyedrops in Habitual Contact Lens Wearers
Geffen DI, Pennell G
Clinical Ophthalmology 2024, 18:3179-3183
Published Date: 7 November 2024