")
Back to Journals » Journal of Inflammation Research » Volume 17
Evaluating Inflammatory Bowel Disease-Related Quality of Life Using an Interpretable Machine Learning Approach: A Multicenter Study in China
Authors Zhen J, Liu C, Zhang J, Liao F, Xie H, Tan C, An P, Liu Z, Jiang C, Shi J, Wu K, Dong W
Received 3 April 2024
Accepted for publication 30 July 2024
Published 9 August 2024 Volume 2024:17 Pages 5271—5283
DOI https://doi.org/10.2147/JIR.S470197
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Junhai Zhen,1 Chuan Liu,2 Jixiang Zhang,2 Fei Liao,2 Huabing Xie,1 Cheng Tan,2 Ping An,2 Zhongchun Liu,3 Changqing Jiang,4 Jie Shi,5 Kaichun Wu,6 Weiguo Dong2
1Department of General Practice, Renmin Hospital of Wuhan University, Wuhan, Hubei Province, 430060, People’s Republic of China; 2Department of Gastroenterology, Renmin Hospital of Wuhan University, Wuhan, Hubei Province, 430060, People’s Republic of China; 3Department of Psychiatry, Renmin Hospital of Wuhan University, Wuhan, 430060, People’s Republic of China; 4Department of Clinical Psychology, Beijing Anding Hospital, Capital Medical University, Beijing, 100088, People’s Republic of China; 5Department of Medical Psychology, Chinese People’s Liberation Army Rocket Army Characteristic Medical Center, Beijing, 100032, People’s Republic of China; 6Department of Gastroenterology, Xijing Hospital, Air Force Medical University, Xi’an, 710032, People’s Republic of China
Correspondence: Kaichun Wu, Department of Gastroenterology, Xijing Hospital, Air Force Medical University, Xi’an, 710032, People’s Republic of China, Tel/Fax +8629-84771600, Email [email protected] Weiguo Dong, Department of Gastroenterology, Renmin Hospital of Wuhan University, 99 Zhangzhidong Road, Wuhan, Hubei Province, 430060, People’s Republic of China, Tel/Fax +8627-88041911, Email [email protected]
Purpose: Impaired quality of life (QOL) is common in patients with inflammatory bowel disease (IBD). A tool to more quickly identify IBD patients at high risk of impaired QOL improves opportunities for earlier intervention and improves long-term prognosis. The purpose of this study was to use a machine learning (ML) approach to develop risk stratification models for evaluating IBD-related QOL impairments.
Patients and Methods: An online questionnaire was used to collect clinical data on 2478 IBD patients from 42 hospitals distributed across 22 provinces in China from September 2021 to May 2022. Eight ML models used to predict the risk of IBD-related QOL impairments were developed and validated. Model performance was evaluated using a set of indexes and the best ML model was explained using a Local Interpretable Model-Agnostic Explanations (LIME) algorithm.
Results: The support vector machine (SVM) classifier algorithm-based model outperformed other ML models with an area under the receiver operating characteristic curve (AUC) and an accuracy of 0.80 and 0.71, respectively. The feature importance calculated by the SVM classifier algorithm revealed that glucocorticoid use, anxiety, abdominal pain, sleep disorders, and more severe disease contributed to a higher risk of impaired QOL, while longer disease course and the use of biological agents and immunosuppressants were associated with a lower risk.
Conclusion: An ML approach for assessing IBD-related QOL impairments is feasible and effective. This mechanism is a promising tool for gastroenterologists to identify IBD patients at high risk of impaired QOL.
Keywords: clinical research, artificial intelligence, model development, clinical decision support system
Introduction
Inflammatory bowel disease (IBD) refers to a group of chronic, relapsing inflammatory disorders of the intestinal tract that includes ulcerative colitis (UC) and Crohn’s disease (CD).1 Millions of people suffer from IBD, and the incidence of these conditions has rapidly increased in recent years. As a result, IBD has become a global public health problem that imposes a heavy burden on both patients and society.2,3 While great advances have been made in understanding IBD pathogenesis and developing effective therapeutic options, patients often still require lifelong regular medical follow-up, pharmacological treatment, and even surgery, which can have a substantial negative impact on quality of life (QOL).4,5
Treatment responsiveness and clinical relapse have been the primary treatment endpoints considered during IBD management. More recently, mucosal healing and the normalization of particular novel biomarkers have been used to evaluate treatment efficacy. Patient-reported outcomes (PRO) have also been proposed and widely accepted as therapeutic targets. In 2015, the Selecting Therapeutic Targets in IBD (STRIDE) program first recommended QOL as a PRO,6,7 citing growing concern about IBD-associated QOL impairments. Several research studies have indicated that the occurrence of IBD-related QOL impairments can be complicated by multiple factors, including disease severity, the use of relevant treatment, and IBD-related symptoms.8 Thus, their timely detection could inform early intervention strategies and improve long-term prognosis. While several IBD-specific QOL scores have been established, including the IBD Questionnaire 32 (IBDQ-32), IBDQ-36, Crohn’s, and UC Questionnaire (CUCQ),9 most have multiple evaluation items that may not be suitable for all gastroenterology clinics. In addition, most gastroenterologists have not taken professional QOL assessment courses, and an ideal method to assess the risk of QOL impairments among IBD patients remains lacking. Therefore, there is an urgent need for an effective and easy-to-use tool to help gastroenterologists promptly detect and manage IBD-related QOL impairments.
Over the past few years, artificial intelligence (AI) technology has been rapidly applied in the medical field. The main branch of AI, machine learning (ML), is highly effective at recognizing complicated relationships between variables and outcomes and several studies have verified that AI models can reliably evaluate various diseases.10–12 However, no research has been conducted to evaluate the risk of IBD-related QOL impairments using ML algorithms. The current multicenter study used routine, easily accessible IBD patient data to develop AI assessment models of IBD-related QOL impairments.
Material and Methods
Data Source and Study Subjects
IBD patients were enrolled between September 2021 and May 2022 from 42 hospitals distributed across 22 provinces in China. All included patients received an online questionnaire. Ethics approval of this study was granted by the institutional review board of Renmin Hospital of Wuhan University (approval number: WDRY2022-K150), and all participants signed the informed consent. This study was also conducted in compliance with ethical principles of the Declaration of Helsinki. Patients were included in the study if (1) their IBD was diagnosed according to the 2018 Chinese Society of Gastroenterology’s consensus on the diagnosis and treatment of IBD,13 (2) they were aged ≥18 years, (3) they were able to understand the survey content, accepted the survey, and were willing to receive physician management and psychological investigations, with good medication compliance, and had (4) complete clinical data. Patients were excluded if they had (1) a previous history of mental illness such as depression and schizophrenia, (2) other diseases that seriously affect QOL, or (3) undetermined colitis.
Data Collection and Outcome Definition
This study used an online questionnaire to collect IBD patient data, including demographic characteristics (age, sex), disease activity or severity (remission, mild activity period, moderate activity period, and severe activity period; as classified in the latest IBD management consensus),13 disease course (<2 years, 2–5 years, >5 years), outpatient diagnosis (UC or CD), symptoms (diarrhoea, hematochezia, abdominal pain, systemic inflammatory symptoms, extraintestinal symptoms, complication manifestations), and prior therapies (5-aminosalicylic acid, glucocorticoids, immunosuppressants, biological agents, surgery). Potential psychological disorders (depression, anxiety, and sleep quality) were also systematically evaluated using three scales: (1) The Patient Health Questionnaire-9 (PHQ-9), an effective depression screening scale with high sensitivity14,15 that consists of nine questions with scores ranging from 0 to 3 for each question, and summed scores ranging from 0 to 27. Summed scores of 0–4, 5–9, 10–14, and 15–27 indicate no depression, mild depression, moderate depression, and severe depression, respectively.16 Since scores ≥10 are usually used to indicate the diagnostic status of depression,17,18 10 was used as the cut-off value in the current study. (2) Generalized Anxiety Disorder-7 (GAD-7), one of the most validated and widely used tools for assessing anxiety worldwide, has seven items that each range from 0 to 3, with total scores ranging from 0 to 21. Summed scores of 0–4, 5–9, 10–14, and 15–21 indicate no anxiety, mild anxiety, moderate anxiety, and severe anxiety, respectively.19 Based on the results of prior studies,17,20 10 was also used as the cut-off value for this scale. (3) The Pittsburgh Sleep Quality Index (PSQI) is a questionnaire that is widely used by clinicians to assess several domains of sleep, including sleepiness, insomnia symptoms, and the use of sleeping pills, in the past month. It consists of seven dimensions with summed scores ranging from 0 to 21. Summed scores of 0–5, 6–10, 11–15, and 16–21 indicate good sleep quality, moderate sleep quality, poor sleep quality, and very poor sleep quality,21 respectively. Patients with summed sleep scores of 0–6 were defined as having no impaired sleep quality, while those with scores >6 had impaired sleep quality.
The primary outcome selected to establish AI models was IBD-related QOL. An IBD questionnaire (IBD-Q) designed by Guyatt et al22 was used to evaluate the QOL of IBD patients. This scale is a common tool that is shown to be valid and reliable in assessing IBD patient QOL. It consists of 32 items with four main aspects (intestinal symptoms, systemic symptoms, emotional domains, and social domains). Each item ranges from 1 to 7, and the summed scores range from 32 to 224, with a higher score representing a better QOL.23 In this study, patients with summed QOL scores ≥169 were defined as having normal QOL, while those with scores <169 had impaired QOL.
Data Preprocessing and Feature (Variable) Selection
There were no missing values, outliers, or extreme values in the raw data, indicating that this data was of high quality. Categorical features such as sex, outpatient diagnosis, symptoms, psychological disorders, and prior therapies were preprocessed using one-hot encoding. The continuous numerical feature, age, was handled using the min-max method [where new value = (original value - min)/ (max - min)] to reduce the influence of dimension and guarantee comparability between different features. Since only 37.7% of enrolled IBD patients were characterized as having impaired QOL (see the distribution of samples in Supplementary Figure 1), this could lead to imbalanced data and a strong bias towards patients with normal QOL. Resampling was widely used to process the imbalanced data, and the Borderline synthetic minority oversampling technique (Borderline-SMOTE) was used to mitigate the imbalance distribution effect.24 The data were also randomly split into a training dataset (80%) for model establishment purposes and a testing dataset (20%) for evaluating the tuned AI models (internal validation).
Features can have different values, with some being redundant or irrelevant while others are critical. Thus, a feature selection step was used to reduce complexity while enhancing the efficiency of the AI models. First, features with a single category ratio of >90% were removed. Then, Spearman correlation analysis was used to assess the correlation between features, and only one of the features with a high correlation (absolute value of the correlation coefficient >0.5) was retained. A heatmap was also used to visualize the correlations between features. Support Vector Machine-Recursive Feature Elimination (SVM-RFE) was then used to select the final candidate features that were shown to optimize the performance of the classifiers.25,26 SVM-RFE uses backward sequential selection to rank the importance of features, and each time, the deleted features minimized the change range of the leave-one-out error bound based on SVM compared to removing the other features.
Establishment and Evaluation of the AI Model
Several widely used supervised ML algorithms, including Random Forest (RF), K-Nearest Neighbor (KNN), Support vector classifier (SVC), eXtreme Gradient Boosting (XGBoost), Categorical boosting (CatBoost), Multilayer Perceptron (MLP), stacking ensemble model and soft voting ensemble-based model, were used to establish the AI model. The KNN model, one of the most commonly used and simplest classifiers, is realized by determining the similarity or distance between the tested and the training cases.27 SVC is a well-known algorithm that completes the classification task by establishing the decision boundaries that maximize the margin.28 RF, XgBoost, CatBoost, Stacking, and the soft voting classifier are all ensemble ML algorithms that have been intensively explored in the medical field. MLP is one of the most frequently used feedforward artificial neural network (ANN) algorithms. In addition to input and output layers, hidden layers are also required for the standard architecture of an MLP model.29,30 The stacking and soft voting models used in this study contained all of these models (RF, KNN, SVC, XgBoost, CatBoost, and MLP).
Grid search combined with 10-fold cross-validation (CV) was used to identify the best hyperparameters for each model. The training dataset was divided into 10 parts, and the AI models were trained in nine parts while the remaining one part was used to get the classification performance index (accuracy). After 10 iterations, 10 accuracy values and their average were generated. The processes outlined above were used on all the hyperparameter combinations and the best hyperparameter combination was used to develop and test the corresponding AI models (Supplementary Figure 2).
The performance of each AI model was assessed in the testing dataset. AUC (area under the curve), accuracy ( ), sensitivity (recall)
), sensitivity (recall)  , specificity
, specificity  , precision
, precision , and F1 scores (
, and F1 scores ( ) were calculated, respectively, where TP, FP, TN, FN represent the number of true positives, false positives, true negatives and false negatives, respectively. The calibration curve and isotonic regression were used to evaluate the calibration of the AI models. The Brier score [score (Y, P) = 1/n *
) were calculated, respectively, where TP, FP, TN, FN represent the number of true positives, false positives, true negatives and false negatives, respectively. The calibration curve and isotonic regression were used to evaluate the calibration of the AI models. The Brier score [score (Y, P) = 1/n *  (P: probability of model prediction; Y: actual probability of occurrence; n: number of predicted events)] was also determined to quantitatively evaluate the calibration. Lower Brier scores represented better model calibration. This study was also assessed by applying the International Journal of Medical Informatics (IJMEDI) checklist to evaluate the quality of ML in the medical field (Supplementary Table 1).31
(P: probability of model prediction; Y: actual probability of occurrence; n: number of predicted events)] was also determined to quantitatively evaluate the calibration. Lower Brier scores represented better model calibration. This study was also assessed by applying the International Journal of Medical Informatics (IJMEDI) checklist to evaluate the quality of ML in the medical field (Supplementary Table 1).31
Feature Importance and AI Model Interpretations
To determine which feature contributed most to the development of the AI models, a bar chart of feature importance was created based on the best AI model using the visualization python package, “Yellowbrick”. The Local Interpretable Model-Agnostic Explanations (LIME) algorithm was used to explain how the AI model made a classification decision for an IBD patient.32 A flowchart of how the AI models were built to predict IBD-related QOL is shown in Figure 1.
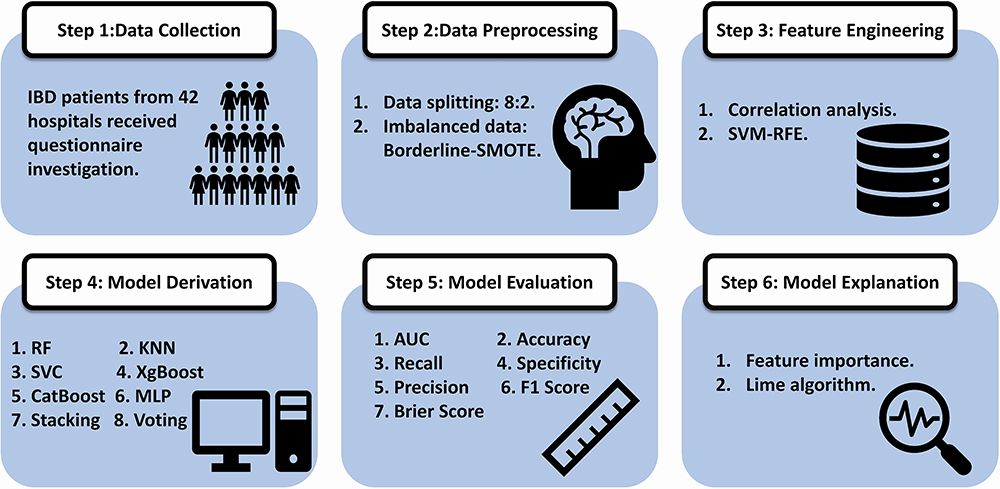 |
Figure 1 Flowchart of building the AI models in predicting IBD related QOL. This study consists of six critical steps, including data collection, data preprocessing, feature engineering, model derivation, model evaluation and model explanation. Abbreviations: Borderline-SMOTE, Borderline synthetic minority oversampling technique; SVM-RFE, Support Vector Machine-Recursive Feature Elimination; RF, Random Forest; KNN, K-Nearest Neighbor; SVC, Support vector classifier; XgBoost, eXtreme Gradient Boosting; CatBoost, Categorical boosting; MLP, Multilayer Perceptron; AUC, area under the curve of ROC; Lime, Local Interpretable Model-Agnostic Explanations. |
Software and Statistical Analysis
Data processing, feature selection, statistical analysis, development, evaluation, and interpretation of the AI models were all conducted using Python software, version 3.9.12. The packages used in this study included “Pandas”, “NumPy”, “Scikit-learn”, “Matplotlib”, and “SciPy”. The continuous feature was expressed as the mean ± standard deviation (mean ± SD) and compared using the Student’s t-test. Categorical features were expressed as percentages and compared using Pearson’s Chi-square or Fisher’s exact tests. All statistical analyses were 2-tailed and a P value <0.05 was considered statistically significant.
Results
Patient Characteristics
The enrollment flow chart of the IBD patients included in this study is shown in Supplementary Figure 3. A total of 2843 potential patients were initially enrolled, of whom 365 met the exclusion criteria and were excluded: 154 refused to be investigated, 60 had incomplete clinical data, 71 were <18 years of age, 11 had a history of mental illness (eight with depression, three with schizophrenia), eight had diseases that seriously impact QOL, and 61 had undetermined colitis. The remaining 2478 IBD patients (1371 with UC and 1107 with CD) met the inclusion criteria and were included in the study, of whom 1982 and 496 patients were allocated to the training and testing datasets, respectively. The baseline characteristics of the IBD patients are presented in Table 1 and Supplementary Table 2. Of the enrolled patients, 933 and 1545 had impaired and normal QOL, respectively. The overall baseline characteristics of the patients in the training and testing datasets were similar, with 746 (37.64%) patients having impaired QOL in the training dataset and 187 (37.70%) having impaired QOL in the testing dataset (Table 1). The mean age of patients with impaired and normal QOL was 38.66 and 37.54 years, respectively and 41.69% and 35.08% were men, respectively (Supplementary Table 2).
 |
Table 1 Baseline Characteristics of the Enrolled IBD Patients in Training and Testing Dataset |
Feature Selection
A total of 17 features were selected after removing three features (systemic inflammatory symptoms, extraintestinal symptoms, and complication manifestations) with a single category ratio of >90%. Correlation analysis was then conducted and another three features (5-ASA, outpatient diagnosis, and depression) were also deleted due to their high correlation with other features (Figure 2A). SVM-RFE with 10-fold cross-validation was also used to obtain the final features. A total of eight vital features (severity, glucocorticoids, anxiety, sleep disorders, abdominal pain, immunosuppressant use, biological agent use, and course of disease) remained. The association between the screening accuracy and the number of features at each split according to the SVM-REF algorithm is shown in Figure 2B.
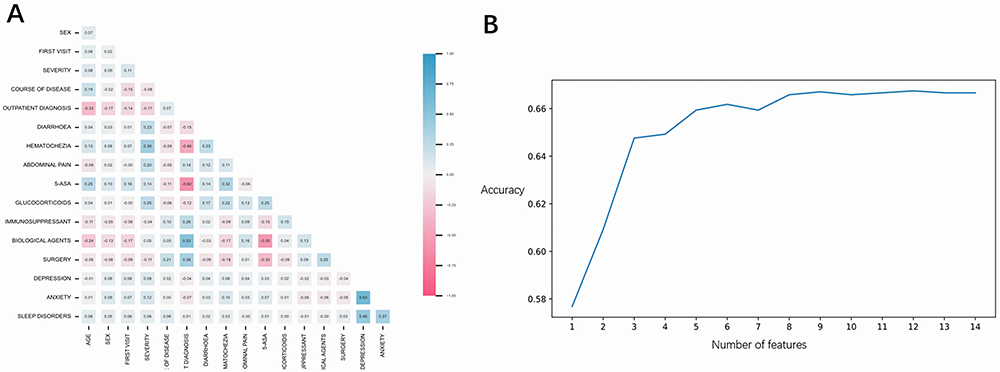 |
Figure 2 (A) The heatmap of all the features correlation. The red and blue color stand for the negative and positive correlations between two features, respectively, high correlation was defined as the absolute value of the correlation coefficient > 0.5, Three features (5-ASA, Outpatient diagnosis, and Depression) were deleted for high correlation with other features. (B) SVM-RFE algorithm with 10-fold cross-validation (CV) was applied to get the final features, and a total of 8 vital features (Severity, Glucocorticoids, Anxiety, Sleep disorders, Abdominal pain, Immunosuppressant, Biological agents, and Course of disease) remained, the Y-axis represents screening accuracy and the X-axis represents number of features at each split based on the SVM-REF algorithm. Abbreviations: 5-ASA, 5-aminosalicylic acid. |
AI Model Performance
Eight AI models were developed to evaluate the QOL of IBD patients, of which the strongest hyperparameters are shown in Supplementary Table 3. In the internal validation (testing datasets), the best-performing model was SVC with an AUC and an accuracy of 0.80 and 0.71, respectively, higher than those of the other models (AUC: RF, 0.77; KNN, 0.72; XGBoost, 0.75; CatBoost, 0.72; MLP, 0.74; Stacking, 0.73; and Voting, 0.77; Accuracy: RF, 0.68; KNN, 0.66; XGBoost, 0.68; CatBoost, 0.66; MLP, 0.69; Stacking, 0.68; Voting, 0.68) (Table 2 and Figure 3A). Other performance indexes, including sensitivity (recall), specificity, precision, and F1 score are shown in Table 2. The SVC model was well-calibrated with a lower Brier score (0.19) than the other AI models (Table 2 and Figure 4A–H).
 |
Table 2 Comparison the Parameters of Models for Prediction of IBD Related Quality of Life in the Internal Validation (Testing Datasets) |
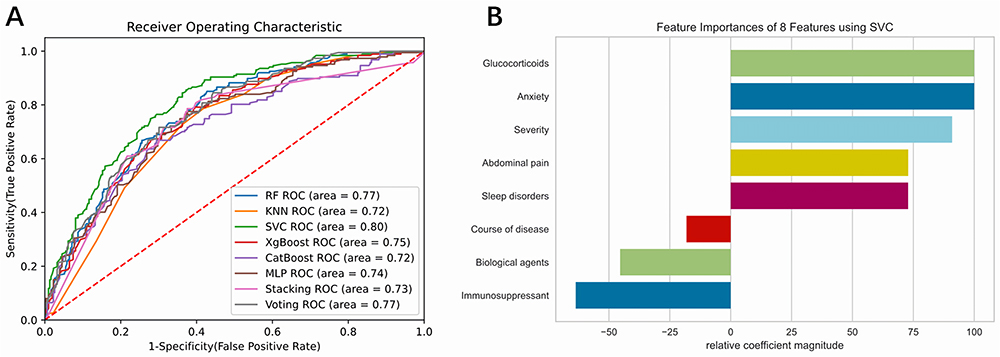 |
Figure 3 (A) The AUC of the ROC curve for each AI model in the evaluation of IBD related impaired QOL. (B) Bar chart of feature importance based on the SVC algorithm. The python package called “Yellowbrick” was used to determine the importance of each feature, as a whole, the use of glucocorticoids, the presence of anxiety, abdominal pain, sleep disorders and more severe diseases all contributed to a higher risk of impaired QOL. While the longer course of disease, the use of biological agents and immunosuppressants were associated with the lower risk. Abbreviations: RF, Random Forest; KNN, K-Nearest Neighbor; SVC, Support vector classifier; XgBoost, eXtreme Gradient Boosting; CatBoost, Categorical boosting; MLP, Multilayer Perceptron. |
 |
Figure 4 The calibration curve and isotonic regression to evaluate the calibration of the AI models. (A) calibration curve and isotonic regression of RF algorithm model; (B) calibration curve and isotonic regression of KNN algorithm model; (C): calibration curve and isotonic regression of SVC algorithm model; (D) calibration curve and isotonic regression of XgBoost algorithm model; (E) calibration curve and isotonic regression of CatBoost algorithm model; (F): calibration curve and isotonic regression of MLP algorithm model; (G) calibration curve and isotonic regression of Stacking algorithm model; (H) calibration curve and isotonic regression of Voting algorithm model. |
Feature Importance and AI Model Interpretation
The feature importance of the SVC algorithm was shown in Figure 3B. The use of glucocorticoids and the presence of anxiety, abdominal pain, sleep disorders, and more severe disease all contributed to a higher risk of impaired QOL. Meanwhile, a longer disease course and the use of biological agents and immunosuppressants were associated with a lower risk. To demonstrate the clinical utility and translational impact of the AI model in actual clinical settings, two patients with normal and impaired QOL who were correctly classified by the SVC algorithm were also assessed. The LIME technique found that a patient with a probability of 0.75 is likely to have normal QOL. This example was correctly evaluated using the following conditions: disease remission, no glucocorticoid use, no anxiety, no sleep disorders, no abdominal pain, and the use of biological agents. Meanwhile, a short course of disease (<2 years) and no immunosuppressant use had an incorrect effect on the final classification results (Figure 5A). The LIME technique also found that a randomly chosen patient with impaired QOL had a 0.62 probability of having QOL impairment. This patient was correctly evaluated using the following conditions: severe disease, sleep disorders, and no immunosuppressant treatment. Meanwhile, the absence of anxiety and abdominal pain, no glucocorticoid use, the use of biological agents, and a longer disease course (>5 years) had an incorrect effect on the final classification results (Figure 5B).
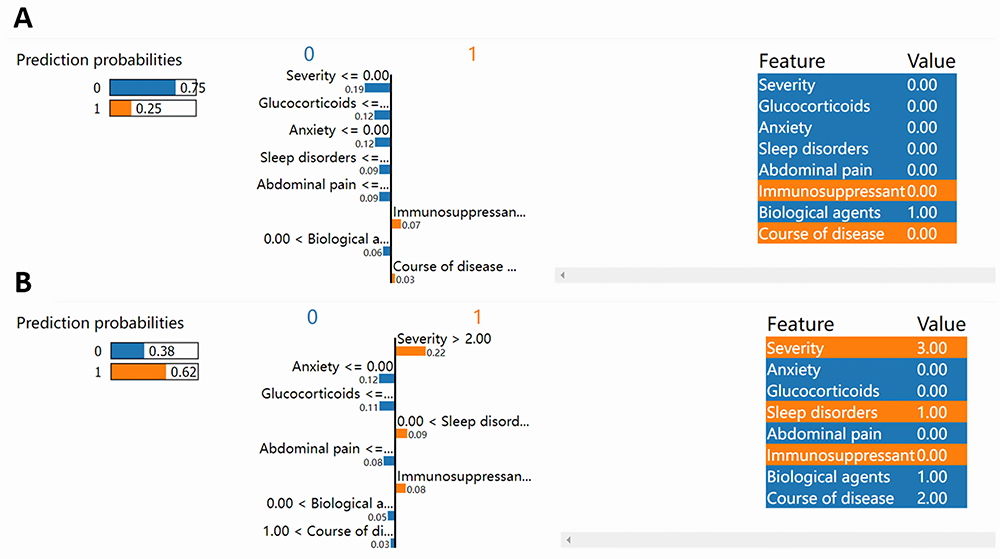 |
Figure 5 SVC algorithm model interpretation based on Lime technique in the evaluation of IBD patients without or with impaired QOL. (A) an IBD patients with normal QOL, the Lime technique indicates this patient has the probability of 0.75 with normal QOL, this example is correctly evaluated mainly through the following conditions: the remission status of IBD, without the use of glucocorticoids, without anxiety, sleep disorders, and abdominal pain, the use of biological agents, while, short course of disease (less than 2 years), and without use of immunosuppressant had an incorrect effect on the final classification results. (B) another IBD patients with impaired QOL, Lime technique indicates this patient has the probability of 0.62 with impaired QOL. This patient is correctly evaluated mainly through the following conditions: the disease is at severe activity period, with sleep disorders, and no immunosuppressant treatment, while without anxiety, abdominal pain, and glucocorticoids use, with biological agents use, and longer course of disease (over 5 years) had an incorrect effect on the final classification results. |
Discussion
This multicenter study established and validated a set of commonly used AI models to assess the risk of IBD-related QOL impairments. To our knowledge, this is the first study to stratify the risk of QOL impairments using an interpretable ML approach. AI models were also shown to effectively assess the risk of QOL impairments among IBD patients. The AI algorithms can give the probability of high risk and low risk of QOL impairment. Low risk indicates a low risk of QOL impairment, while high risk indicates a high possibility of QOL impairment, when the probability of high risk is higher than that of low risk, the patient is judged as high risk of QOL impairment; otherwise, the patient is judged as low risk of QOL impairment. Of the ones used in this study, the SVC model had the best classification performance. By using eight routinely accessible IBD patients’ features (severity, glucocorticoids, anxiety, sleep disorders, abdominal pain, immunosuppressant use, biological agent use, and course of disease), gastroenterologists can use the SVC based model to detect IBD patients who are potentially at risk for impaired QOL, this in turn can detect early if they are suffering from impaired QOL and help them with in time intervention. The societal and economic implications of IBD highlight the importance of assessing the impaired QOL experienced by IBD patients. This evaluation is crucial not only from a clinical standpoint but also in terms of public health and economic considerations.33
Given the importance of normalizing the QOL of IBD patients, its use as an endpoint for IBD treatment is likely to increase.6 Identifying predictors of QOL impairments in IBD patients will inform appropriate evaluation and management strategies. Recent studies have assessed independent predictors of IBD-related QOL impairments, including disease severity,34 psychological distress,35 symptoms,36 and various therapeutic approaches.37 The current study differed from previous studies through the use of ML feature selection methods to identify predictors of IBD-related QOL impairments. Of the 20 features explored, disease severity, glucocorticoid use, anxiety, sleep disorders, abdominal pain, immunosuppressant use, biological agent use, and disease course were defined as the eight most vital predictors. Of these, the use of glucocorticoids and anxiety were the two most important risk factors, followed by more severe disease, abdominal pain, and sleep disorders.
Glucocorticoids work through a variety of mechanisms and signaling pathways to reduce IBD-related inflammation,38,39 and are often recommended for the treatment of IBD patients with moderate to severe disease.40 Interestingly, the current study showed that glucocorticoid use was one of the most important risk factors for impaired QOL, a finding consistent with prior studies.41,42 There are some possible explanations for this observation. First, the use of glucocorticoids may be a surrogate indicator for IBD severity since they are typically used to treat IBD patients in the active phase of the disease. Second, glucocorticoid treatment exposes IBD patients to several glucocorticoid-related side effects including low bone density,43 neuropsychiatric disorders,44 and serious infections.45 One large-scale study found that at least one adverse event will occur in 80–90% of IBD patients during a conventional glucocorticoid treatment course.46 A large retrospective cohort study conducted by Lewis et al47 identified higher mortality among IBD patients who had received prolonged glucocorticoid therapy, potentially due to their increased rates of major adverse cardiovascular events and hip fractures. However, to consider the impact of glucocorticoid treatment on IBD patient QOL, rational use dimensions such as treatment dose, course of treatment, and method of administration must also be considered since they can affect treatment efficacy and glucocorticoid-related side effects, further impacting QOL. Subgroup analysis based on these glucocorticoid treatment conditions was not performed by either the current or prior studies. Thus, additional studies are needed to clarify the influence of such factors on IBD patient QOL.
This study also found that biological agent use, immunosuppressant use, and a longer disease course were associated with improved QOL. The first two factors were shown to improve IBD patient QOL in previous studies,41,48 however, evidence on the impact of disease course has been relatively ambiguous. Some studies found the QOL improved over time,49–51 while others did not.52,53 Our recently published multicenter prospective cross-sectional study identified disease course as an independent factor that influences IBD patient disease knowledge. A longer disease course correlated positively with patient knowledge about their condition.54 IBD patients with high disease-related knowledge tend to use more adaptive coping strategies55 and have better medication adherence,56 which may contribute to a higher QOL and improved outcomes. This may explain why a longer disease course was associated with a better QOL in the current study.
A few studies have constructed models to evaluate the risk of IBD-related QOL impairments, primarily relying on conventional logistic regression (LR). Our recently published study used the same data as the current study to construct an LR model to predict QOL by gender. The AUC of the male and female prediction models were 0.771 and 0.770, respectively.57 AI algorithms can be used to explore the complicated relationships between features and target outcomes and provide a novel approach to individualized risk assessment. While no prior study developed AI models to assess the risk of impaired QOL among IBD patients, the current study found that the SVC algorithm achieved an AUC of 0.80, indicating that this model was better at predicting QOL impairments than the conventional LR model we had used previously. These findings indicate that a model based on the SVC algorithm may help to evaluate IBD-related QOL impairments with good classification performance, this might be attributed to the SVC’s superior ability in uncovering complex relationships between key features in this study and label (IBD-related QOL),28 which was also confirmed by the former medical researches.58,59
The current study has some limitations. First, some features, such as psychological interventions,60 parental stress,61 and health information gathering from the internet,62 were not accounted for in the AI models. These features may also influence IBD QOL and potentially impact model performance. Second, while data of IBD patient were obtained from 42 hospitals distributed across 22 provinces in China, only 2478 IBD patients were finally enrolled in the study. This may be because IBD is not yet common in China.13 Due to the lack of relevant data sources, we also did not validate the AI models in the external validation dataset, including those from other countries or racial groups. However, the rigorous methodology used in the current study ensured that the AI models were stable and practical. Third, subgroup analysis by diagnosis (UC and CD) was not performed given the small sample size, limiting assessment of QOL among patients with different IBD types. Fourth, Due to the lack of time-related information in the questionnaire survey (partly because large proportion of IBD patients have difficulty recalling the relevant time information accurately), this study did not further conduct the meaningful analyses like KM-plot or COX regression models. Finally, although we found the good performance of SVC based model in identifying impaired QOL among IBD patients, for the complexity of clinical practice, further evaluation might also be needed to determine the risk and benefits of deploying the model in real-world scenarios. This would require the design of clinical trials for comprehensive evaluation.
In the future, additional researches should be conducted to further optimize the ML model’s performance to improve the evaluation accuracy of impaired QOL among IBD patients. The introduction of other important features such as psychological interventions, parental stress, and health information gathering from the internet can be considered to further improve the ML model’s performance. Besides, it might also be the good idea to apply other novel methods like deep learning methods, which might perform better, therefore potentially improve the accuracy and stability of the AI model. What’s more, we found eight features that play critical role in evaluating impaired QOL among IBD patients, this might provide clues for effective prevention and intervention strategies related to impaired QOL in IBD patients, so the effects of these strategies can be evaluated by conducting intervention trials in the future.
Conclusion
This study developed and validated novel IBD-related QOL impairment risk assessment models using an interpretable ML approach. The SVC algorithm-based AI model had the best discriminating power, suggesting that it could be used to evaluate QOL impairments using routine and easily accessible IBD patient data and AI. Research on other groups of IBD patients, as well as the combination of other relevant features, is required to further validate and improve the performance and practicality of QOL assessment models.
Abbreviation
5-ASA, 5-aminosalicylic acid; AI, artificial intelligence; AUC, area under the curve of ROC; CatBoost, Categorical boosting; CD, Crohn’s disease; CV, cross-validation; IBD, Inflammatory Bowel Disease; KNN, K-Nearest Neighbor; Lime, Local Interpretable Model-Agnostic Explanations; ML, machine learning; MLP, Multilayer Perceptron; QOL, Quality of life; RF, Random Forest; ROC, receiver operating characteristic; SVC, Support vector classifier; SVM-RFE, Support Vector Machine-Recursive Feature Elimination; UC, Ulcerative colitis; XgBoost, eXtreme Gradient Boosting.
Data Sharing Statement
The data underlying this article will be shared on reasonable request to the corresponding author.
Ethical Statement
The ethics approval of this study was granted by the institutional review board of Renmin Hospital of Wuhan University (approve number: WDRY2022-K150).
Acknowledgments
The authors would like to thank 42 participating institutions and associated IBD physicians for their help in this study, which are listed below (in no particular order): Renmin Hospital of Wuhan University, Xijing Hospital, Air Force Medical University, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College (Hong Lyv), the Second Affiliated Hospital of Xi’an Jiaotong University (Fenrong Chen, Sumei Sha), Peking University First Hospital (Tian Yuling), Peking University Third Hospital (Jun Li), Beijing Friendship Hospital, Capital Medical University (Ye Zong, Haiying Zhao), Ruijin Hospital, Shanghai Jiaotong University School of Medicine (Tianyu Zhang), First Affiliated Hospital of Sun Yat-sen University (Baili Chen, Ren Mao, Yao He, Shenghong Zhang), General Hospital, Tianjin Medical University (Hailong Cao, Shuai Su, Wenyao Dong, Lili Yang), Second Hospital of Hebei Medical University (Qian Liu, Rongrong Zhan), Sir Run-Run Shaw Hospital, Zhejiang University School of Medicine (Jing Liu), the First Affiliated Hospital of Wenzhou Medical University (Xiangrong Chen, Xiaowei Chen, Lingyan Shi), the Affiliated Hospital of Medical School of Ningbo University (Jinfeng Wen), Jiangsu Province Hospital, the First Affiliated Hospital of Nanjing Medical University (Jingjing Ma), Jiangsu Province Hospital of Chinese Medicine (Lei Zhu), General Hospital of Eastern Theater Command of Chinese People’s Liberation Army (Juan Wei), the Second Affiliated Hospital of Soochow University (Han Xu), Shengjing Hospital of China Medical University (Nan Nan, Feng Tian), the First Affiliated Hospital of Dalian Medical University (Xiuli Chen, Jingwei Mao), Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (Liangru Zhu), Zhongnan Hospital of Wuhan University (Mei Ye), Xiangya Hospital of Central South University (Shuijiao Chen), the Second Xiangya Hospital of Central South University (Hanyu Wang), Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China (Xue Yang, Yinghui Zhang), the First Affiliated Hospital of Anhui Medical University (Juan Wu), Qilu Hospital, Shandong University (Xiaoqing Jia), the Affiliated Hospital of Qingdao University (Xueli Ding, Jing Guo, Ailing Liu), the First Hospital of Jilin University (Haibo Sun, Jing Zhan), the First Affiliated Hospital of Kunming Medical University (Yating Qi), General Hospital of Ningxia Medical University (Shaoqi Yang, Ting Ye), the Second Affiliated Hospital of Zhengzhou University (Sumin Wang, Dandan Wang), the First Affiliated Hospital of Guangxi Medical University (Xiaoping Lyu, Junhua Fan, Shiquan Li), Chongqing General Hospital (Chongqing Hospital, University of Chinese Academy of Sciences) (Lingya Xiang), the First Affiliated Hospital of Xinjiang Medical University (Ping Yao, Hongliang Gao), the Second Affiliated Hospital of Harbin Medical University (Wanying Li), the First Affiliated Hospital of the University of Science and Technology of China, Anhui Provincial Hospital (Xuemei Xu), Daping Hospital, Army Medical University (Zhuqing Qiu), Affiliated Hangzhou First People’s Hospital, Zhejiang University School of Medicine (Wen Lyu), the Affiliated Hospital of Southwest Medical University (Xiaolin Zhong), General Hospital of Southern Theater Command of People’s Liberation Army (Ang Li, Xiangqiang Liu, Yanchun Ma), Suzhou Municipal Hospital (North District), Nanjing Medical University Affiliated Suzhou Hospital (Zhi Pang). Besides, The authors would like to thank editors and the anonymous reviewers for their valuable comments and suggestions to improve the quality of the paper.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by The National Natural Science Foundation of China (No. 82170549).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nakase H, Uchino M, Shinzaki S, et al. Evidence-based clinical practice guidelines for inflammatory bowel disease 2020. J Gastroenterol. 2021;56(6):489–526. doi:10.1007/s00535-021-01784-1
2. Park KT, Ehrlich OG, Allen JI, et al. The Cost of Inflammatory Bowel Disease: An Initiative From the Crohn’s & Colitis Foundation. Inflamm Bowel Dis. 2020;26(1):1–10. doi:10.1093/ibd/izz104
3. Zhao M, Gönczi L, Lakatos PL, Burisch J. The Burden of Inflammatory Bowel Disease in Europe in 2020. J Crohns Colitis. 2021;15(9):1573–1587. doi:10.1093/ecco-jcc/jjab029
4. Knowles SR, Graff LA, Wilding H, Hewitt C, Keefer L, Mikocka-Walus A. Quality of Life in Inflammatory Bowel Disease: a Systematic Review and Meta-analyses-Part I. Inflamm Bowel Dis. 2018;24(4):742–751. doi:10.1093/ibd/izx100
5. Knowles SR, Keefer L, Wilding H, Hewitt C, Graff LA, Mikocka-Walus A. Quality of Life in Inflammatory Bowel Disease: a Systematic Review and Meta-analyses-Part II. Inflamm Bowel Dis. 2018;24(5):966–976. doi:10.1093/ibd/izy015
6. Calviño-Suárez C, Ferreiro-Iglesias R, Bastón-Rey I, Barreiro-de Acosta M. Role of Quality of Life as Endpoint for Inflammatory Bowel Disease Treatment. Int J Environ Res Public Health. 2021;18(13). doi:10.3390/ijerph18137159
7. Peyrin-Biroulet L, Sandborn W, Sands BE, et al. Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE): determining Therapeutic Goals for Treat-to-Target. Am J Gastroenterol. 2015;110(9):1324–1338. doi:10.1038/ajg.2015.233
8. Benchimol EI, Bernstein CN, Bitton A, et al. The Impact of Inflammatory Bowel Disease in Canada 2018: a Scientific Report from the Canadian Gastro-Intestinal Epidemiology Consortium to Crohn’s and Colitis Canada. J Can Assoc Gastroent. 2019;2(Suppl 1):S1–s5. doi:10.1093/jcag/gwy052
9. Chen XL, Zhong LH, Wen Y, et al. Inflammatory bowel disease-specific health-related quality of life instruments: a systematic review of measurement properties. Health Qual Life Outcomes. 2017;15(1):177. doi:10.1186/s12955-017-0753-2
10. Pan Y, Zhang L, Zhang R, et al. Screening and diagnosis of colorectal cancer and advanced adenoma by Bionic Glycome method and machine learning. Am J Cancer Res. 2021;11(6):3002–3020.
11. Li T, Huang H, Zhang S, et al. Predictive models based on machine learning for bone metastasis in patients with diagnosed colorectal cancer. Front Public Health. 2022;10:984750. doi:10.3389/fpubh.2022.984750
12. Da Rio L, Spadaccini M, Parigi TL, et al. Artificial intelligence and inflammatory bowel disease: where are we going? World J Gastroenterol. 2023;29(3):508–520. doi:10.3748/wjg.v29.i3.508
13. Inflammatory Bowel Disease Group, Chinese Society of Gastroenterology, Chinese Medical Association. Chinese consensus on diagnosis and treatment in inflammatory bowel disease (2018, Beijing). J Dig Dis. 2021;22(6):298–317. doi:10.1111/1751-2980.12994
14. Turner A, Hambridge J, White J, et al. Depression screening in stroke: a comparison of alternative measures with the structured diagnostic interview for the diagnostic and statistical manual of mental disorders, fourth edition (major depressive episode) as criterion standard. Stroke. 2012;43(4):1000–1005. doi:10.1161/strokeaha.111.643296
15. Meader N, Moe-Byrne T, Llewellyn A, Mitchell AJ. Screening for poststroke major depression: a meta-analysis of diagnostic validity studies. J Neurol Neurosurg Psych. 2014;85(2):198–206. doi:10.1136/jnnp-2012-304194
16. Dajpratham P, Pukrittayakamee P, Atsariyasing W, Wannarit K, Boonhong J, Pongpirul K. The validity and reliability of the PHQ-9 in screening for post-stroke depression. BMC Psych. 2020;20(1):291. doi:10.1186/s12888-020-02699-6
17. Swaminathan A, Fan D, Borichevsky GM, et al. The disease severity index for inflammatory bowel disease is associated with psychological symptoms and quality of life, and predicts a more complicated disease course. Aliment Pharmacol Ther. 2022;56(4):664–674. doi:10.1111/apt.17058
18. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
19. Mughal AY, Devadas J, Ardman E, Levis B, Go VF, Gaynes BN. A systematic review of validated screening tools for anxiety disorders and PTSD in low to middle income countries. BMC Psychiatry. 2020;20(1):338. doi:10.1186/s12888-020-02753-3
20. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
21. Dietch JR, Taylor DJ, Sethi K, Kelly K, Bramoweth AD, Roane BM. Psychometric Evaluation of the PSQI in U.S. College Students. J Clin Sleep Med. 2016;12(8):1121–1129. doi:10.5664/jcsm.6050
22. Guyatt G, Mitchell A, Irvine EJ, et al. A new measure of health status for clinical trials in inflammatory bowel disease. Gastroenterology. 1989;96(3):804–810.
23. Yarlas A, Maher S, Bayliss M, et al. The Inflammatory Bowel Disease Questionnaire in Randomized Controlled Trials of Treatment for Ulcerative Colitis: systematic Review and Meta-Analysis. J Patient Cent Res Rev. 2020;7(2):189–205. doi:10.17294/2330-0698.1722
24. Han W, Huang Z, Li S, Jia Y. Distribution-Sensitive Unbalanced Data Oversampling Method for Medical Diagnosis. J Med Syst. 2019;43(2):39. doi:10.1007/s10916-018-1154-8
25. Xia J, Sun L, Xu S, et al. A Model Using Support Vector Machines Recursive Feature Elimination (SVM-RFE) Algorithm to Classify Whether COPD Patients Have Been Continuously Managed According to GOLD Guidelines. Int J Chron Obstruct Pulmon Dis. 2020;15:2779–2786. doi:10.2147/copd.S271237
26. Li F, Zhao C, Xia Z, Wang Y, Zhou X, Li GZ. Computer-assisted lip diagnosis on Traditional Chinese Medicine using multi-class support vector machines. BMC Compl Altern Med. 2012;12:127. doi:10.1186/1472-6882-12-127
27. Abu Alfeilat HA, Hassanat ABA, Lasassmeh O, et al. Effects of Distance Measure Choice on K-Nearest Neighbor Classifier Performance: a Review. Big Data. 2019;7(4):221–248. doi:10.1089/big.2018.0175
28. Gupta A, Kahali B. Machine learning-based cognitive impairment classification with optimal combination of neuropsychological tests. Alzheimers Dement. 2020;6(1):e12049. doi:10.1002/trc2.12049
29. Majidzadeh Gorjani O, Byrtus R, Dohnal J, Bilik P, Koziorek J, Martinek R. Human Activity Classification Using Multilayer Perceptron. Sensors. 2021;21(18). doi:10.3390/s21186207
30. Tseng YJ, Wang YC, Hsueh PC, Wu CC. Development and validation of machine learning-based risk prediction models of oral squamous cell carcinoma using salivary autoantibody biomarkers. BMC Oral Health. 2022;22(1):534. doi:10.1186/s12903-022-02607-2
31. Cabitza F, Campagner A. The need to separate the wheat from the chaff in medical informatics: introducing a comprehensive checklist for the (self)-assessment of medical AI studies. Int J Med Inform. 2021;153:104510. doi:10.1016/j.ijmedinf.2021.104510
32. Tasin I, Nabil TU, Islam S, Khan R. Diabetes prediction using machine learning and explainable AI techniques. Healthc Technol Lett. 2023;10(1–2):1–10. doi:10.1049/htl2.12039
33. Park J, Jeong GH, Song M, et al. The global, regional, and national burden of inflammatory bowel diseases, 1990-2019: a systematic analysis for the global burden of disease study 2019. Dig Liver Dis. 2023;55(10):1352–1359. doi:10.1016/j.dld.2023.04.003
34. Pizzi LT, Weston CM, Goldfarb NI, et al. Impact of chronic conditions on quality of life in patients with inflammatory bowel disease. Inflamm Bowel Dis. 2006;12(1):47–52. doi:10.1097/01.mib.0000191670.04605.e7
35. Iglesias-Rey M, Barreiro-de Acosta M, Caamaño-Isorna F, et al. Psychological factors are associated with changes in the health-related quality of life in inflammatory bowel disease. Inflamm Bowel Dis. 2014;20(1):92–102. doi:10.1097/01.MIB.0000436955.78220.bc
36. Nagy B, Laczkóné Majer R. Specific quality of life factors in patients with inflammatory bowel disease. Orv Hetil. 153(38):1511–1519. doi:10.1556/oh.2012.29369
37. Xu J, Lin H, Feng X, Tang M, Shen J, Ran Z. Different therapeutic approaches on quality of life in patients with inflammatory bowel disease. BMC Gastroenterol. 2014;14:199. doi:10.1186/s12876-014-0199-5
38. Riccardi L, Mazzon E, Bruscoli S, et al. Peroxisome proliferator-activated receptor-alpha modulates the anti-inflammatory effect of glucocorticoids in a model of inflammatory bowel disease in mice. Shock. 2009;31(3):308–316. doi:10.1097/SHK.0b013e31818339e7
39. Fischer A, Gluth M, Weege F, et al. Glucocorticoids regulate barrier function and claudin expression in intestinal epithelial cells via MKP-1. Am J Physiol Gastroint Liver Physiol. 2014;306(3):G218–28. doi:10.1152/ajpgi.00095.2013
40. Domènech E. Inflammatory bowel disease: current therapeutic options. Digestion. 2006;73(Suppl 1):67–76. doi:10.1159/000089781
41. Rivera Sequeiros A, Gil García E, Chillόn Martinez R. N800 Statistical comparison of predictors of quality of life in inflammatory bowel disease. J Crohn’s Colitis. 2017;11(1):S491–S491. doi:10.1093/ecco-jcc/jjx002.924
42. Bernklev T, Jahnsen J, Schulz T, et al. Course of disease, drug treatment and health-related quality of life in patients with inflammatory bowel disease 5 years after initial diagnosis. Eur J Gastroenterol Hepatol. 2005;17(10):1037–1045. doi:10.1097/00042737-200510000-00006
43. Even Dar R, Mazor Y, Karban A, Ish-Shalom S, Segal E. Risk Factors for Low Bone Density in Inflammatory Bowel Disease: Use of Glucocorticoids, Low Body Mass Index, and Smoking. Dig Dis. 2019;37(4):284–290. doi:10.1159/000496935
44. Ali S, Paul S, Yakkali S, et al. Glucocorticoids-Induced Neuropsychiatric Disorders in Patients With Inflammatory Bowel Disease: a Systematic Review. Cureus. 2022;14(9):e28981. doi:10.7759/cureus.28981
45. Brassard P, Bitton A, Suissa A, Sinyavskaya L, Patenaude V, Suissa S. Oral corticosteroids and the risk of serious infections in patients with elderly-onset inflammatory bowel diseases. Am J Gastroenterol. 2014;109(11):1795–1802. doi:10.1038/ajg.2014.313
46. Curtis JR, Westfall AO, Allison J, et al. Population-based assessment of adverse events associated with long-term glucocorticoid use. Arthritis Rheum. 2006;55(3):420–426. doi:10.1002/art.21984
47. Lewis JD, Scott FI, Brensinger CM, et al. Increased Mortality Rates With Prolonged Corticosteroid Therapy When Compared With Antitumor Necrosis Factor-α-Directed Therapy for Inflammatory Bowel Disease. Am J Gastroenterol. 2018;113(3):405–417. doi:10.1038/ajg.2017.479
48. Feagan BG, Reinisch W, Rutgeerts P, et al. The effects of infliximab therapy on health-related quality of life in ulcerative colitis patients. Am J Gastroenterol Apr. 2007;102(4):794–802. doi:10.1111/j.1572-0241.2007.01094.x
49. Greenley RN, Kunz JH, Schurman JV, Swanson E. Abdominal pain and health related quality of life in pediatric inflammatory bowel disease. J Pediatr Psychol. 2013;38(1):63–71. doi:10.1093/jpepsy/jss097
50. Burisch J, Weimers P, Pedersen N, et al. Health-related quality of life improves during one year of medical and surgical treatment in a European population-based inception cohort of patients with inflammatory bowel disease--An ECCO-EpiCom study. J Crohns Colitis. 2014;8(9):1030–1042. doi:10.1016/j.crohns.2014.01.028
51. Blondel-Kucharski F, Chircop C, Marquis P, et al. Health-related quality of life in Crohn’s disease: a prospective longitudinal study in 231 patients. Am J Gastroenterol. 2001;96(10):2915–2920. doi:10.1111/j.1572-0241.2001.4681_b.x
52. Haapamäki J, Roine RP, Sintonen H, Kolho KL. Health-related quality of life in paediatric patients with inflammatory bowel disease related to disease activity. J Paediatr Child Health. 2011;47(11):832–837. doi:10.1111/j.1440-1754.2011.02034.x
53. Huppertz-Hauss G, Lie Høivik M, Jelsness-Jørgensen LP, et al. Health-related Quality of Life in Patients with Inflammatory Bowel Disease 20 Years After Diagnosis: results from the IBSEN Study. Inflamm Bowel Dis. 2016;22(7):1679–1687. doi:10.1097/mib.0000000000000806
54. Xie H, Zhang J, Liu C, Yang B, Dong W. Development and validation of a questionnaire to test Chinese patients’ knowledge of inflammatory bowel disease. Sci Rep. 2023;13(1):7061. doi:10.1038/s41598-023-34286-6
55. Moradkhani A, Kerwin L, Dudley-Brown S, Tabibian JH. Disease-specific knowledge, coping, and adherence in patients with inflammatory bowel disease. Dig Dis Sci. 2011;56(10):2972–2977. doi:10.1007/s10620-011-1714-y
56. Jimmy B, Jose J. Patient medication adherence: measures in daily practice. Oman Med J. 2011;26(3):155–159. doi:10.5001/omj.2011.38
57. Liu C, Zhang J, Chen M, et al. Gender Differences in Psychological Symptoms and Quality of Life in Patients with Inflammatory Bowel Disease in China: a Multicenter Study. J Clin Med. 2023;12(5). doi:10.3390/jcm12051791
58. Hamzeh O, Alkhateeb A, Zheng JZ, et al. A Hierarchical Machine Learning Model to Discover Gleason Grade-Specific Biomarkers in Prostate Cancer. Diagnostics. 2019;9(4). doi:10.3390/diagnostics9040219
59. Alghanim F, Al-Hurani I, Qattous H, et al. Machine Learning Model for Multiomics Biomarkers Identification for Menopause Status in Breast Cancer. Algorithms. 2024;17(1):13.
60. Mussell M, Böcker U, Nagel N, Olbrich R, Singer MV. Reducing psychological distress in patients with inflammatory bowel disease by cognitive-behavioural treatment: exploratory study of effectiveness. Scand J Gastroenterol. 2003;38(7):755–762. doi:10.1080/00365520310003110
61. Jelenova D, Prasko J, Ociskova M, et al. Quality of life and parental styles assessed by adolescents suffering from inflammatory bowel diseases and their parents. Neuropsychiatr Dis Treat. 2016;12:665–672. doi:10.2147/ndt.S104260
62. Niv G, Bar josef S, Ben Bassat O, et al. Quality of life and uncertainty in Crohn’s disease. Qual Life Res. 2017;26(6):1609–1616. doi:10.1007/s11136-017-1509-5
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.