")
Back to Journals » Risk Management and Healthcare Policy » Volume 18
Evaluating the Effectiveness of Spousal Testing Among Syphilis-Infected Pregnant Women in the Context of Mother-to-Child Transmission Elimination: A Multicenter Study in Southeastern China
Authors Xue X, Huang X, Liu G, Jiang X, Lin W, Chen Y, Huang C
Received 31 March 2025
Accepted for publication 7 July 2025
Published 12 July 2025 Volume 2025:18 Pages 2423—2433
DOI https://doi.org/10.2147/RMHP.S531584
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Xiaomeng Xue,1,2,* Xinxin Huang,3,* Guihua Liu,2 Xiumin Jiang,2 Wenzhao Lin,1,2 Yongfan Chen,1,2 Chengyu Huang1,2
1School of Nursing, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China; 2Nursing Department, Fujian Maternity and Child Health Hospital, College of Clinical Medicine for Obstetrics and Gynecology and Pediatrics, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China; 3The Ministry of Health, Fujian Maternity and Child Health Hospital, College of Clinical Medicine for Obstetrics and Gynecology and Pediatrics, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiumin Jiang, Nursing Department, Fujian Maternity and Child Health Hospital, College of Clinical Medicine for Obstetrics and Gynecology and Pediatrics, Fujian Medical University, No. 18. Daoshan Road, Fuzhou, Fujian, People’s Republic of China, Email [email protected]
Purpose: Syphilis during pregnancy poses significant risks to maternal and neonatal health. Spousal testing is crucial for preventing congenital syphilis transmission. This study assessed spousal testing rates among syphilis-positive pregnant women to guide public health interventions.
Methods: This multicenter effectiveness study was conducted in Southeast China, utilizing data from the Chinese HIV/AIDS, Syphilis, and Hepatitis B Prevention Information System between 2018 to 2024. Proportions were used to describe the sociodemographic characteristics of pregnant women with syphilis. Univariate and multivariate unconditional logistic regression models were used to analyze the factors associated with the testing status of spouses of pregnant women with syphilis.
Results: A total of 4,875 spouses were tested for syphilis. Older gestational age at the first prenatal visit (aOR = 1.014, 95% CI: 1.007– 1.022) and at delivery (aOR = 1.273, 95% CI: 1.011– 1.602) were associated with lower rates of spousal testing. Spouses of women reported in 2022– 2023 (aOR = 1.840, 95% CI: 1.465– 2.311) had a higher likelihood of being untested. Unmarried status (aOR = 1.181, 95% CI: 1.022– 1.364), junior high school education and below (aOR = 1.244, 95% CI: 1.121– 1.381), no history of infection (aOR = 2.281, 95% CI: 2.073– 2.510), and prenatal care in Grade II hospitals (aOR = 0.1.292, 95% CI: 1.140– 1.464) were risk factors for spousal testing.
Conclusion: From 2018 to 2024, the spousal testing rate was 60%, with a syphilis positivity rate of 14.7%. Data revealed multiple risk factors, such as a late first pregnancy test, advanced age, unmarried status, lower education level, no history of syphilis infection, and selection of prenatal care in Grade II hospitals as delivery facilities. Recommendations include establishing specialized clinics, post-test spousal counseling, and routine spousal testing.
Plain Language Summary: Syphilis is a worldwide epidemic infectious disease that poses a great threat to the health of newborns through sexual transmission and mother-to-child transmission. The incidence of syphilis is still high in China. Prevention of sexually transmitted infections is considered to be a key factor in the prevention of syphilis. The spouses of pregnant women with syphilis may act as vectors of infection, which increases the risk of syphilis infection in newborns. This study provides an in-depth analysis of the factors that affect the testing rate of the spouses of pregnant women with syphilis under the strategy of elimination of mother-to-child transmission (EMTCT) in Southeast China. The results revealed that the spousal testing rate increased from 2018 to 2024, whereas the syphilis positive rate among spouses was relatively high. The data revealed multiple risk factors, such as late first pregnancy test, advanced age, unmarried status, low education level, no previous history of syphilis infection, and selection of prenatal care in Grade II hospitals for delivery. This study validated the effectiveness of the EMTCT framework in reducing mother-to-child transmission of syphilis and highlighted the specific measures of the risk factors mentioned above in the future control of sexual and mother‒to-child transmission of syphilis.
Keywords: syphilis, pregnant woman, spousal testing, multicenter, influencing factors
Introduction
Syphilis is a sexually and vertically transmitted bacterial infection caused by the bacterium Treponema pallidum.1 According to World Health Organization (WHO) reports, new syphilis cases among adults aged 15–49 increased by over one million in 2022, reaching 8 million cases globally,2 and Chinese Center for Disease Control and Prevention (CDC) data revealed more than 460,000 new syphilis cases in China in 2020. Untreated syphilis in pregnancy leads to adverse outcomes among more than half of the women with active disease, including early fetal loss, stillbirth, prematurity, low birth weight, neonatal and infant death, and congenital disease among newborn babies.3 Surveillance data from China’s National Infectious Disease Monitoring System indicated a congenital syphilis incidence rate of 11.87 per 100,000 live births in 2019,4 imposing a substantial burden on both public healthcare systems and affected families.
In 2007, WHO launched the global strategy for the elimination of congenital syphilis, emphasizing that active screening and treatment of pregnant women and their partners could significantly reduce the incidence of congenital syphilis.5,6 WHO initiated the global Elimination of Mother-to-Child Transmission (EMTCT) program in 2007, aiming to comprehensively control and reduce the Mother-to-Child Transmission (MTCT) of HIV, syphilis, and hepatitis B virus to minimal levels. In 2022, WHO edited “Global health sector strategies on, respectively, HIV, viral hepatitis, and sexually transmitted infections for the period 2022–2030”, which emphasizes EMTCT as a critical strategic initiative to prevent and reduce childhood cases of HIV, syphilis, hepatitis B, and other diseases.7 By the end of 2024, twenty countries/regions had received WHO EMTCT certification. In 2010, China became the first country to integrate prevention strategies for MTCT of HIV, syphilis, and hepatitis B. This initiative achieved nationwide coverage of comprehensive testing services by 2015. Through sustained governmental efforts, including policy development, expanded free antenatal screening, standardized treatment protocols, and public education campaigns, China has achieved significant reductions in syphilis MTCT rates. In 2022, China implemented the “National Action Plan for the elimination of mother‒to‒child transmission of AIDS, syphilis and hepatitis B (2022–2025)”,8 marking a new phase in its EMTCT efforts.
Spouses of pregnant women infected with syphilis present potential transmission vectors with high syphilis seropositivity rates. When both partners are infected, the risk of neonatal syphilis infection increases substantially.9 Prompt treatment of seropositive partners helps prevent cross-infection, reduces the risk of maternal reinfection, and protects neonatal health. Consequently, partner notification and testing are critical components of syphilis control.10,11 The US CDC identified sexually transmitted infection (STI) prevention as a key strategy for syphilis control.12 However, studies indicate that approximately 70% of partners of syphilis-infected pregnant women in China remain untested,13 suggesting ongoing challenges in spousal testing rates. Therefore, this study aimed to investigate the prevalence and determinants of spousal testing among syphilis-seropositive pregnant women in Southeastern China with the ultimate goal of providing targeted interventions, optimizing clinical pathways, and interrupting intrafamilial transmission chains.
Methods
Study Design and Study Participants
This study was a population-based retrospective analysis. The study population comprised all syphilis-seropositive pregnant women who delivered in Fujian Province, China, between January 1, 2018, and June 15, 2024. Given the 100% coverage of universal free syphilis serological testing among pregnant women, this study comprehensively included all syphilis-positive pregnant women in the Fujian Province during this period. All medical records were uploaded to the China Information System for the prevention of HIV, syphilis, and hepatitis B.
Procedures
A standardized questionnaire was used to conduct face-to-face interviews with uniformly trained local medical staff and research participants, collecting data on sociodemographic characteristics, pregnancy-related issues, and spousal testing.
The study adhered to the Declaration of Helsinki (2024) and was approved by the Fujian Maternity and Child Health Hospital College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University. All participants signed an informed consent form.
The reported syphilis cases in pregnant women in China from 2018 to 2024 were downloaded from the Management Information System for HIV/AIDS, syphilis, and hepatitis B prevention. The case-selection process is illustrated in Figure 1.
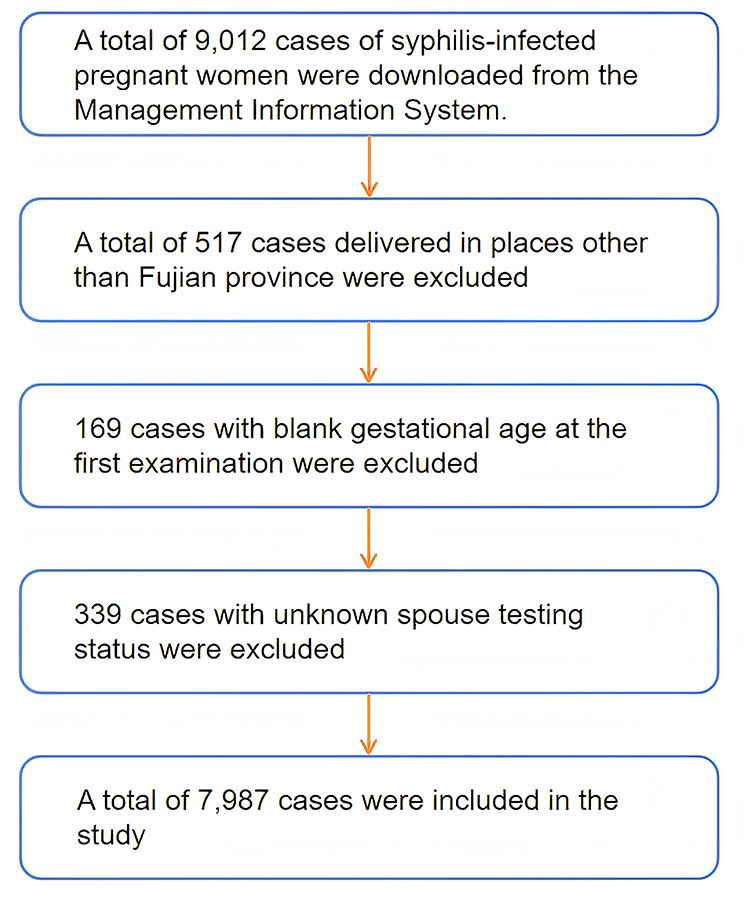 |
Figure 1 The case-selection process. |
Statistical Analysis
The sociodemographic characteristics of the study participants were described in terms of proportions. Univariate analysis and multivariate unconditional logistic models were used to determine the factors associated with the spousal testing status of pregnant women with syphilis. All variables were considered candidates for the multivariate model using the univariate chi-square test. Significant variables in the univariate chi-square test were included in the multivariate logistic regression analysis. Adjusted odds ratios (aORs) and 95% confidence intervals (95% CIs) were calculated using backward regression and multivariate unconditional logistic regression analyses (0 = tested, 1 = untested). All analyses were performed using SPSS version 26.0 (SPSS Inc., Chicago, IL, USA).
Results
Sociodemographic Characteristics
A total of 7987 participants were included in the study between January 1, 2018, and June 15, 2024. The spousal testing status for different delivery years is shown in Figure 2. The sociodemographic characteristics of the participants are provided in Table 1. Participants had a mean age of 29.82 years and a median age of 29 years. The test results were divided into 1744 unknown and 3131 clear results (positive and negative). Among the spouses of women with syphilis with clear test results, 460 (14.7%) were infected with syphilis.
 |
Table 1 Sociodemographic Characteristics of Pregnant Women with Syphilis Infection |
 |
Figure 2 The spousal testing status at different delivery years. |
Associations Between the Sociodemographic Characteristics of Pregnant Women with Syphilis and Detecting the Status of their Spouses
Among the marital statuses of pregnant women with syphilis, 6890 (86.20%) were married (first marriage/ remarriage), and 1097 (13.70%) were unmarried (unmarried/ cohabitation/ divorced/ widowed). Based on the Fujian Statistical Yearbook 2023 released by the Fujian Provincial Bureau of Statistics,14 this study classified the relevant data of urban and rural residents’ per capita disposable income in 2022 from high to low and divided them into three levels, respectively marked as “good” (Xiamen, Quanzhou, Fuzhou), “middle” (Zhangzhou, Putian, Longyan), and “poor” (Sanming, Ningde, Nanping). The grades of the hospital where the examination was performed were divided into grades III, II, I, and undetermined levels according to the Hospital Grading Management Standards.15 A total of 4875 (61%) spouses were tested, and 3112 (39%) were not tested. Table 2 summarizes whether the sociodemographic characteristics of pregnant women with syphilis were related to their spousal testing status. Age, nationality, occupation, marital status, education level, year of delivery, previous infection history, grade of hospital, and gestational age at first prenatal visit were related to the spousal testing status (P < 0.05). No significant associations were observed between spousal testing status and GDP per capita, gravidity, or parity (P > 0.05).
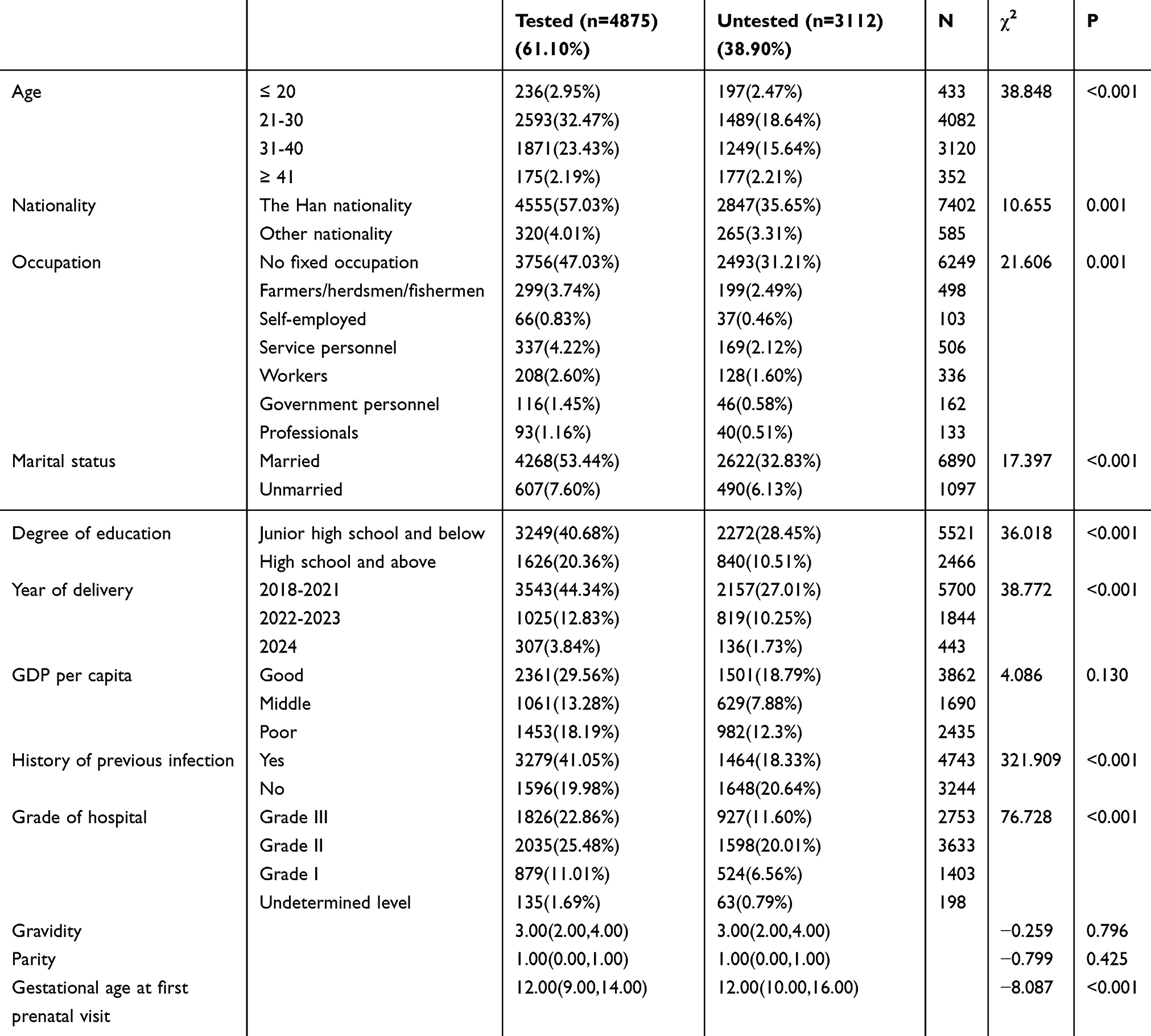 |
Table 2 Association Between Sociodemographic Characteristics and Pregnancy-Related Conditions with Spousal Testing Status |
Factors Influencing Spousal Testing of Syphilis
As the dependent variable (0 = tested, 1 = untested), the following independent variables were tested: the first prenatal examination, gestational age, gestational age at syphilis diagnosis, age, nationality, occupation, marital status, education level, year of delivery, history of previous infection, and hospital grade. Binary logistic regression analysis was performed using the backward likelihood ratio method (exclusion criteria: P = 0.15), and the results of the multivariate analysis are shown in Table 3. Nationality and occupation were not included in the equation. Initial gestational age, age, marital status, educational level, year of delivery, history of previous infection, and hospital grade were factors affecting the testing status of the spouse. For each 1-week increase in the gestational age at the first prenatal visit, the risk increased 1.014-fold (aOR = 1.014, 95% CI: 1.007–1.022; P < 0.05). Compared with pregnant women aged 31–40 years, those aged 21–30 years were associated with a lower risk, serving as a protective factor (aOR = 0.853, 95% CI: 0.772–0.944; P < 0.05), and the spouses of pregnant women aged 41 years or older had a greater risk, with a 1.273-fold increase (aOR = 1.273, 95% CI: 1.011–1.602; P < 0.05). Unmarried pregnant women had a 1.181-fold greater risk of their spouses remaining untested compared to married pregnant women (aOR = 1.181, 95% CI: 1.022–1.364; P < 0.05). Compared to pregnant women with an education level of high school or above, the risk of spousal non-testing was 1.244 times higher for those with an education level of junior high school or below (aOR = 1.244, 95% CI: 1.121–1.381; P < 0.05). Mothers in 2022–2023 had a 1.840-fold greater risk of having untested spouses compared to mothers in 2024 (aOR = 1.840, 95% CI: 1.465–2.311; P < 0.05). The risk of having an untested spouse was 2.281 times higher for pregnant women without a history of previous infection compared to those with a previous infection history (aOR = 2.281, 95% CI: 2.073–2.510; P < 0.05). Compared to pregnant women delivering in Grade I or lower hospitals, the risk of having an untested spouse was 1.292 times greater for those whose delivery hospital grade was Grade II (aOR = 1.292, 95% CI: 1.140–1.464; P < 0.05).
 |
Table 3 Binary Logistic Regression Analysis of Spousal Testing Status |
Discussion
This study analyzed the syphilis testing status of the spouses of 7987 syphilis-infected pregnant women who gave birth in Fujian Province from 2018 to 2024. Approximately 60% of the spouses underwent syphilis testing, and nearly 40% of the spouses did not. The testing rate of spouses of pregnant women with syphilis was higher than that in Wenzhou from 2016 to 2022 (45.45%).16 Fujian Province actively responded and formulated policies to reduce the rate of MTCT. In 2022, the government promulgated and implemented the “Outline for the Development of Women and Children (2021–2030) Implementation Plan for mother-to-child transmission of HIV, syphilis and hepatitis B (2023–2025)”, 17 which clarified general requirements, action objectives, strategic measures, and organizational support for elimination work. Data from contemporaneous studies in China indicate that the spousal testing program has yielded positive outcomes; however, opportunities for enhancement remain. This is still a key point in the implementation of MTCT of syphilis in Fujian Province.
Policy deficiencies have contributed significantly to the low spousal testing rates. Mobilizing partners of pregnant women with syphilis faces multiple challenges, including resource constraints, stigma, poor service quality, and out-of-pocket payment requirements.18 As obstetricians are not authorized to issue test orders for male partners, patients are required to independently arrange spousal testing upon returning home, a factor that may result in suboptimal compliance. Moreover, while serological testing for syphilis in pregnant women is free of charge, spousal testing is not, which may lead to poor compliance. Additionally, in the absence of sufficient social support, stigma may exacerbate psychological distress among partners of syphilis-positive pregnant women, potentially creating additional barriers to the promotion and implementation of EMTCT efforts.19,20 To improve spousal testing compliance, several hospitals in Fujian Province have introduced pilot programs incorporating two specific interventions: (i) granting obstetricians the authority to issue test orders for partners of syphilis-positive pregnant women to reduce procedural barriers and (ii) providing free testing for partners of syphilis-positive pregnant women. The effectiveness of this policy warrants confirmation through future follow-up.
This study revealed that later gestational age at the first prenatal examination was associated with a greater risk of lower spousal testing rates, aligning with findings reported by Zheng et al.21 Delayed syphilis diagnosis during pregnancy is associated with postponed follow-up care and reduced spousal testing rates. In 2010, the Chinese government launched the “National Free Preconception Health Examination Program”, which helped prevent and control syphilis MTCT.22 In this program, the government asked obstetricians to promote “early screening and early detection” before 12+6 weeks’ gestation. However, there are differences in the implementation of these policies in different cities. A few hospitals in underdeveloped areas have insufficient testing materials23 and laboratory testing personnel.24 Given the lack of testing training for medical staff,25 the doctors who conduct pregnancy tests do not issue a syphilis test report at the same time,26 and obstetricians who do not provide post-test consultation after a pregnant woman is found to be positive for syphilis may affect testing behavior of the spouse.26 Therefore, to improve the spousal testing rate, concerted efforts are needed to optimize preconception health initiatives, deliver targeted counseling during initial prenatal visits, and integrate routine syphilis testing into standardized first-trimester obstetric protocols. Healthcare systems should mandate universal syphilis screening during the first antenatal consultation while streamlining clinical workflows to ensure consistent implementation.
In this study, a lower risk of untested spouses was noted among women aged 21–30 years, while a higher risk was noted among women aged 41 years or older than among women aged 31–40 years. This finding aligns with the results of Tang et al,27 who reported that the spousal testing of syphilis-infected maternal sexual partners in the 36-year-old or older age group was low. This can be related to the challenges faced by pregnant women of advanced maternal age.28 The physiological and psychological status of older pregnant women has undergone certain changes. First, older multiparas may neglect pregnancy testing and pay insufficient attention to spousal testing because of “experience.” If it is their first pregnancy, older pregnant women may experience a sense of stigma due to their turbulent pregnancy experience,29 which makes them resistant to medical pregnancies and spousal testing. Studies have shown that the probability of the vertical transmission of syphilis increases with increasing maternal age.30 Therefore, if maternal age is further associated with syphilis infection, it poses a great threat to fetal health. Therefore, it is essential to provide enhanced humanistic and psychological care for older pregnant women, actively follow up on syphilis spousal testing, and offer individualized health counseling to pregnant women and their spouses as needed.
Spousal notification is an established component of STI control strategies and an integral part of maternal syphilis control and treatment.31 In this study, the risk of spouses not being tested was low in married women, similar to findings in Bolivia.32 We speculated that low spousal testing rates imply low spousal notification rates. Unmarried pregnant women are unwilling to inform their sexual partners because of their unstable relationships with their spouses, which negatively affects the subsequent treatment and transmission of syphilis. In a healthy marital relationship, there is usually knowledge exchange regarding disease prevention and treatment, and spouses may adopt each other’s lifestyles and attitudes,33 which is conducive to preventing transmission. Currently, there are few strategies for spousal notification of syphilis. Therefore, to improve the spousal testing rate for unmarried pregnant women with syphilis, more attention should be paid to protecting the privacy of pregnant women and their spouses. A comprehensive spousal notification policy should be established to ensure the physical safety and mental health of pregnant women while encouraging their spouses to undergo testing.
In this study, high school education or higher was identified as a protective factor among the spouses of pregnant women who were not tested. People with lower levels of education may know less about syphilis34 and have limited access to prevention and treatment.35 Therefore, to improve the spousal testing rate of pregnant women with low education levels, it is necessary to provide targeted publicity forms and content to encourage spouses to cooperate with testing. Moreover, the decision-making power of women in marital relationships is primarily influenced by their economic status.36 In China, women with a lower economic status tend to have lower educational attainment.37 Consequently, women with less education may be less effective at motivating their spouses to participate in partner testing. Few studies have examined the relationship between the household decision-making power of women and partner testing, making this an important area for future research.
This study observed a high rate of spousal testing for pregnant women who delivered in 2024. We used the time of the national action plan issued by the Chinese government to eliminate mother-to-child syphilis transmission as the time node for this study. The Chinese government initiated a pilot project in September 2017 to eliminate MTCT of syphilis in certain provinces. The rate of spousal testing from 2022 to 2023 decreased, which is considered to be related to the impact of the global COVID-19 pandemic at that time. The COVID-19 pandemic has been reported to affect the availability and timely access to healthcare for sexually transmitted diseases (STDs) for people with syphilis and their sexual partners.38 According to the available data up to June 2024 in this study, the spousal testing rate is back on track and steadily increasing.
In this study, we reported that women without a previous infection were at a high risk of having an untested spouse. This factor has been disputed by other researchers. Dou et al39 reported the same results as those in the current study, whereas Zheng et al21 reported the opposite effect. This can be explained by the fact that this study and Dou et al used populations in the southeastern or eastern regions of China as research objects, which have certain similarities and comparability in demographic characteristics and geographical features. However, Zheng et al studied pregnant women infected with syphilis in Yunnan Province. Given Yunnan Province’s adjacency to a country with a high syphilis prevalence, observed differences in study conclusions or population characteristics should be considered. We believe that pregnant women without syphilis infection before pregnancy are less likely to receive syphilis health education and that their attention and vigilance are not high. However, the current study revealed that previously infected pregnant women were more willing to urge their spouses to undergo testing.
This study contributes novel data by reporting the positive rate among spouses of syphilis-infected pregnant women who completed testing. Among the 3131 spouses of pregnant women with syphilis infection, 460 (14.70%) were positive, which was lower than the 21.36% reported by Zhang et al9 and the 19.7% reported by HuiXia Ji.40 This may be related to the overall low incidence of syphilis in Fujian Province and the positive effect of the policy response. The positive rate of syphilis tests in the general population in China is only 0.33%.41 Syphilis-positive rates are markedly higher in spouses of infected pregnant women than in the general population, highlighting their elevated risk of infection. This can be explained by the fact that syphilis is an STD with a long incubation period, hidden symptoms of infection, and is easily confused with other diseases.42 When the infection status of the spouse is unknown, the mother and fetus will be exposed to greater risks,43 the risk of syphilis in the newborn will increase.44 Moreover, untreated syphilis-positive spouses will elevate the probability of repeated prenatal reinfection among pregnant women. Therefore, future health education can provide warnings based on data and typical cases to help expectant parents understand the harm caused by syphilis in newborns, clarify the necessity of active treatment, and promote positive maternal spousal testing behavior.
This study uniquely identifies the effect of delivery hospital grade on the rate of spousal testing. Compared to Grade I and lower hospitals, prenatal care in Grade II hospitals was a risk factor for spousal testing. Implementation of the EMTCT policy for syphilis requires funds as well as medical and human resources. With the support of sufficient resources, the awareness of pregnancy management among medical staff, health education levels of service providers, and compliance of the families of pregnant women with medical staff will increase. Although there are few studies on the effect of the level of delivery hospitals on the rate of spousal testing, this can be explained by patients’ choice of medical institutions. The National Medical Service Situation from January to August 2023 reported that the number of medical visits increased by 8.7% in Grade III hospitals and 9.0% in Grade I hospitals,45 which can be explained by the results of this study. Grade III hospitals have sufficient medical resources, whereas Grade I and lower-grade hospitals have lower family income requirements. Therefore, more pregnant women are willing to choose Grade III hospitals and Grade I or below hospitals. The number of patients receiving prenatal care in Grade II hospitals has decreased, and their attention to medical staff training and the path specification of spousal testing has decreased.
Limitation
As this was a retrospective study, we were unable to collect data on the economic income of pregnant women, which limited further exploration of how income and household decision-making power of women influence spousal testing. Future research will explore this topic further by incorporating culturally relevant analyses of patriarchal structures. Additionally, as policies allowing obstetricians to prescribe spousal testing and provide free spousal testing are currently being piloted in select regions, our team will analyze changes in spousal testing rates before and after policy implementation once more comprehensive data become available.
Conclusion
This study provides an in-depth analysis of the factors affecting the testing rate of the spouses of pregnant women with syphilis under the strategy of elimination of EMTCT in Southeast China. This study revealed that the rate of spousal testing was approximately 60% from 2018 to 2024 and that the positive rate of syphilis testing among spouses was as high as 14.7%. The data revealed multiple risk factors such as a late first pregnancy test, advanced age, unmarried status, lower education level, no previous history of syphilis infection, and selection of prenatal care in Grade II hospitals as delivery facilities. At the same time, this study verified the effectiveness of the EMTCT framework’s policies in reducing the MTCT of syphilis. To address these risk factors, hospitals should establish specialized care clinics, provide joint counseling for spouses after testing, and offer laboratory test orders to spouses of infected individuals in obstetric departments. Hospitals with sufficient resources may consider offering free testing services for spouses to improve testing rates. Healthcare providers should deliver targeted health education to high-risk populations with low spousal testing rates, utilize cautionary case studies, and, when necessary, assign dedicated volunteers for follow-up and encourage spousal testing. Secondary hospitals should optimize post-test counseling procedures and pathways while enhancing the health education skills of healthcare workers.
Data Sharing Statement
The data that support the findings of this study are available from the Management Information System for HIV/AIDS, syphilis, and hepatitis B prevention but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data is however available from the authors Xiaomeng Xue and Xinxin Huang upon reasonable request and with permission of the Management Information System for HIV/AIDS, syphilis, and hepatitis B prevention.
Ethics Approval and Informed Consent
The study adhered to the Declaration of Helsinki and was approved by Fujian Maternity and Child Health Hospital College of Clinical Medicine for Obstetrics and Gynecology and Pediatrics, and all participants in this study signed an informed consent form.
Acknowledgments
We would like to thank Editage (www.editage.cn) for English language editing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Peeling RW, Mabey D, Chen XS, Garcia PJ. Syphilis. Lancet. 2023;402(10398):336–346. doi:10.1016/S0140-6736(22)02348-0
2. World Health Organization. Implementing the Global Health Sector Strategies on HIV, Viral Hepatitis and Sexually Transmitted Infections, 2022–2030. Geneva: World Health Organization; 2022.
3. Ingall D, Sánchez PJ. Syphilis. In: Remington JS, Klein JO, editors. Infectious Diseases of the Fetus and Newborn Infant.
4. Chen XS, Cao NX, Wang QQ, et al. Prevention and control of syphilis in China:10-year’s national program and its achievements. Chin J Aids STD. 2022;28(9):1001–1004.
5. World Health Organization. Global Guidance on Criteria and Processes for Validation: Elimination of Mother-to Child Transmission of HIV and Syphilis. Geneva: World Health Organization; 2017.
6. Hossain M, Broutet N, Hawkes S. The elimination of congenital syphilis: a comparison of the proposed World Health Organization action plan for the elimination of congenital syphilis with existing national maternal and congenital syphilis policies. Sex Transm Dis. 2007;34(7 Suppl):S22–S30.
7. World Health Organization. Global Health Sector Strategies on, Respectively, HIV, Viral Hepatitis and Sexually Transmitted Infections for the Period 2022-2030. Geneva: World Health Organization; 2022.
8. National Health Commission of the People’s Republic of China. Eliminate mother-to-child transmission of AIDS, syphilis and hepatitis B action plan (2022-2025). Available from: http://www.nhc.gov.cn/fys/s3581/202212/afe6bc9626be45a0b25bee93f01fef10.shtml.
9. Zhang XH, Chen YM, Sun Y, Qiu LQ, Chen DQ. Differences in maternal characteristics and pregnancy outcomes between syphilitic women with and without partner coinfection. BMC Pregnancy Childbirth. 2019;19(1):439. doi:10.1186/s12884-019-2569-z
10. Konje ET, Magoma MTN, Hatfield J, Kuhn S, Sauve RS, Dewey DM. Missed opportunities in antenatal care for improving the health of pregnant women and newborns in Geita district, Northwest Tanzania. BMC Pregnancy Childbirth. 2018;18(1):394. doi:10.1186/s12884-018-2014-8
11. Dalle J, Baumgarten VZ, Ramos MC, et al. Maternal syphilis and accomplishing sexual partner treatment: still a huge gap. Int J STD AIDS. 2017;28(9):876–880. doi:10.1177/0956462416678710
12. CDC. Sexually transmitted diseases treatment guidelines, 2010. MMWR. 2010;59:RR–12.
13. Dou L, Wang X, Wang F, et al. Epidemic profile of maternal syphilis in China in 2013. Biomed Res Int. 2016;2016:9194805. doi:10.1155/2016/9194805
14. Fujian Provincial Bureau of Statistics. Fujian Statistical Yearbook. Beijing: China Statistics Press; 2023.
15. Notice of the general office of the ministry of health on issuing the “detailed rules for the implementation of the evaluation standards for tertiary general hospitals (2011 edition)”. Available from: http://www.nhc.gov.cn/cms-search/xxgk/getManuscriptXxgk.htm?id=0404f9cd71764ab29b2365e069cfbf2d.
16. Chen H, Hu Z, Xiang O. Analysis of the effectiveness of preventing mother to child transmission of syphilis in Wenzhou City from 2016 to 2022. Chin J Public Health Manage. 2024;40(1):
17. Health Commission of the Fujian Province. Fujian province has carried out comprehensive efforts to eliminate mother-to-child transmission of AIDS, syphilis and hepatitis B. Available from: https://wjw.fujian.gov.cn/xxgk/fgwj/zcjd/bmzcjd/202310/t20231026_6285660.htm.
18. World Health Organization. Sexually transmitted infections (STIs). Available from: https://www.who.int/news-room/fact-sheets/detail/sexually-transmitted-infections-(stis). (2024)
19. Brittain K, Mellins CA, Phillips T, et al. Social support, stigma and antenatal depression among HIV-infected pregnant women in South Africa. AIDS Behav. 2017;21(1):274–282. doi:10.1007/s10461-016-1389-7
20. Qin S, Tan Y, Lu B, Cheng Y, Nong Y. Survey and analysis for impact factors of psychological distress in HIV-infected pregnant women who continue pregnancy. J Matern Fetal Neonatal Med. 2019;32(19):3160–3167. doi:10.1080/14767058.2018.1459550
21. Zheng M, Qi SF, Li Y, Zheng JR, Guo GP. Analysis on syphilis screening among 4036 puerperas with syphilis and their spouses and its influencing factors in Yunnan Province. Soft Sci Health. 2019;33(8):91–94.
22. The State Council The People’s Republic of China. Health and family planning commission: national free preconception eugenics program to achieve full coverage of rural areas. Available from: https://www.gov.cn/xinwen/2014-04/18/content_2662381.htm.
23. Munkhuu B, Liabsuetrakul T, Chongsuvivatwong V, Geater A, Janchiv R. Antenatal care providers’ practices and opinions on the services of antenatal syphilis screening in Ulaanbaatar, Mongolia. Southeast Asian J Trop Med Public Health. 2006;37(5):975–982.
24. Baker C, Limato R, Tumbelaka P, et al. Antenatal testing for anaemia, HIV and syphilis in Indonesia-a health systems analysis of low coverage. BMC Pregnancy Childbirth. 2020;20(1):326. doi:10.1186/s12884-020-02993-x
25. Pakki IB, Kuntoro SRD, Purnomo W. The Influence of posyandu cadres’ training to ward the predisposing factors of Provider Initiated Testing and Counseling (PITC) of HIV services for the pregnant women and its utilization on Samarinda Municipality, Indonesia. Indian J Public Health Res Dev. 2020;11(3):2028–2033.
26. Dinh TH, Detels R, Nguyen MA. Factors associated with declining HIV testing and failure to return for results among pregnant women in Vietnam. AIDS. 2005;19(11):1234–1236. doi:10.1097/01.aids.0000176228.09474.59
27. Tang LY, Mou HZ, Gao S, et al. Syphilis testing analysis among partners of syphilis infected pregnant women in Guangdong province in 2013. Chin J Women Child Health. 2017;8(2):1–5,10.
28. Dongarwar D, Tahseen D, Aliyu MH, Salihu HM. Pregnancy outcomes among Asian Americans of advanced maternal age, 1992-2018. J Obstet Gynaecol Res. 2021;47(6):2117–2125. doi:10.1111/jog.14790
29. Goldenberg RL, Thompson C. The infectious origins of stillbirth. Am J Obstet Gynecol. 2003;189(3):861–873. doi:10.1067/s0002-9378(03)00470-8
30. Mak S, Thomas A. Steps for conducting a scoping review. J Grad Med Educ. 2022;14(5):565–567. doi:10.4300/JGME-D-22-00621.1
31. Koenig LJ, Moore J. Women, violence, and HIV: a critical evaluation with implications for HIV services. Matern Child Health J. 2000;4(2):103–109. doi:10.1023/a:1009570204401
32. Díaz-Olavarrieta C, García SG, Feldman BS, et al. Maternal syphilis and intimate partner violence in Bolivia: a gender-based analysis of implications for partner notification and universal screening. Sex Transm Dis. 2007;34(7 Suppl):S42–S46. doi:10.1097/01.olq.0000261725.79965.af
33. Monden CW, de Graaf ND, Kraaykamp G. How important are parents and partners for smoking cessation in adulthood? An event history analysis. Prev Med. 2003;36(2):197–203.
34. Ying L, Shaokai T, Xingdong Y, et al. Awareness and knowledge of syphilis among different populations in Guangzhou, Guangdong Province, China. Sex Health. 2013;10(3):282–283. doi:10.1071/SH12181
35. Kane MA, Bloch EM, Bruhn R, Kaidarova Z, Murphy EL. Demographic determinants of syphilis seroprevalence among U.S. blood donors. BMC Infect Dis. 2015;15:63.
36. Gupta I, Roy A. What really empowers women? Taking another look at economic empowerment. J Soc Econ Dev. 2023;25:17–31.
37. Chao F, Jie D. From human capital to national knowledge capital:the impact of academic education and cognitive skills on labor wage income. Chongqing High Educ Res. 2025;13(1):32–44.
38. Pagaoa M, Grey J, Torrone E, et al. Trends in nationally notifiable sexually transmitted disease case reports during the US COVID-19 pandemic, January to December 2020. Sex Transm Dis. 2021;48(10):798–804. doi:10.1097/OLQ.0000000000001506
39. Dou LX, Wang XY, Wang Q, et al. Uptake of syphilis testing among spouses/ partners of syphilis infected pregnant women. Chin J Women Child Health. 2015;6(6):21–2429.
40. Ji HX. Clinical analysis of couples with syphilis. Chin J Dermatology. 2000;(01):51–52.
41. Yang XY, Chen DY, Wang HX, et al. Epidemiological trends of five sexually transmitted infections in China. Chinese J Evidence-Based Med. 2022;22(07):778–784.
42. Peeling RW, Hook EW. The pathogenesis of syphilis: the great mimicker, revisited. J Pathol. 2006;208(2):224–232. doi:10.1002/path.1903
43. Li Z, Wang Q, Qiao Y, Wang X, Jin X, Wang A. Incidence and associated predictors of adverse pregnancy outcomes of maternal syphilis in China, 2016-19: a cox regression analysis. BJOG. 2021;128(6):994–1002. doi:10.1111/1471-0528.16554
44. DiOrio D, Kroeger K, Ross A. Social vulnerability in congenital syphilis case mothers: qualitative assessment of cases in Indiana, 2014-2016. Sex Transm Dis. 2018;45(7):447–451. doi:10.1097/OLQ.0000000000000783
45. Statistical Information Center. National medical services from January to August 2023. Available from: http://www.nhc.gov.cn/mohwsbwstjxxzx/s7967/202401/d6fd0c655fc04e0585ce143e014adc1a.shtml. (2024)
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.