")
Back to Journals » Clinical Ophthalmology » Volume 18
Evaluation of Higher-Order Aberrations After the Smooth Incision Lenticular Keratomileusis (SILKTM) Procedure Using the ELITATM Femtosecond Platform for Correction of Myopic and Astigmatic Refractive Errors
Authors Chen L , Khamar P, Wang Y, Fu H, Shetty R
Received 23 April 2024
Accepted for publication 10 July 2024
Published 24 July 2024 Volume 2024:18 Pages 2155—2166
DOI https://doi.org/10.2147/OPTH.S466932
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Li Chen,1,* Pooja Khamar,2,* Ying Wang,3 Hong Fu,1 Rohit Shetty2
1Johnson & Johnson Surgical Vision, Inc., Milpitas, CA, USA; 2Narayana Nethralaya Eye Hospital, Bangalore, India; 3Johnson & Johnson Surgical Vision, Inc., Irvine, CA, USA
*These authors contributed equally to this work
Correspondence: Li Chen, Johnson & Johnson Surgical Vision, Inc., 510 Cottonwood Drive, Milpitas, CA, 95035, USA, Tel +1 408 273 4062, Email [email protected]
Purpose: To evaluate the changes of higher-order wavefront aberrations following the Smooth Incision Lenticular Keratomileusis (SILKTM) procedure for correction of myopic refractive errors with and without astigmatism, using the ELITATM Femtosecond Platform.
Methods: This prospective study included 24 eyes that underwent SILK procedure using one ELITA femtosecond laser system for the correction of myopic refractive errors with and without astigmatism. Preoperative and postoperative 1-day, 1-week, 1-month, 3-month, and 9-month eye exams were measured with a commercial wavefront aberrometer (iDESIGN® Refractive Studio, Johnson & Johnson Surgical Vision, Inc). Wavefront aberrations up to the 6th order Zernike coefficients, including coma Z(3, − 1) and Z(3, 1), spherical aberration Z(4, 1), and the wavefront error of all higher-order aberrations (HOAs RMS), were evaluated across a 6 mm pupil.
Results: The mean manifest refractive spherical equivalent changed from the preoperative refractions − 3.82 ± 1.26 D (range − 6.00 to − 2.25 D) to the postoperative refractions − 0.20 ± 0.15 D (range − 0.50 to 0.00 D) at the 9-month follow-up. Compared to baseline preoperative HOAs, the mean postoperative HOAs were significantly increased at the 1-day follow-up. On average, at the 9-month postoperative assessment the vertical coma Z(3, − 1) was − 0.054 ± 0.186 μm, horizontal coma Z(3, 1) was 0.016 ± 0.124 μm, spherical aberration Z(4, 0) was 0.046 ± 0.163 μm, and HOAs RMS was 0.363 ± 0.115 μm across a 6 mm pupil. There is no significant difference in the mean HOAs starting at 1-week follow-up for the horizontal coma (P = 0.346) and spherical aberration (P = 0.095).
Conclusions: The visual outcomes demonstrated that the SILK procedure for refractive lenticule extraction using ELITA femtosecond laser system is effective and predictable for the correction of myopic refractive errors with and without astigmatism. The ELITA femtosecond laser system induced minimal HOAs in surgical eyes following the SILK procedures. These results demonstrate fast corneal recovery starting at 1-week follow-up, and spherical aberration was not induced.
Keywords: wavefront aberrations, corneal refractive surgery, laser-assisted lenticule extraction, smooth incision lenticular keratomileusis
Introduction
Wavefront aberrations in the human eye can be classified as lower-order and higher-order aberrations (HOAs). Lower-order aberrations, comprising defocus and astigmatisms, correspond to the refractive sphere and cylinder errors in the human eye.1–4 Studies5,6 demonstrated that refractive sphere and cylinder errors dominate for nearly 90% of the wavefront aberrations in the population of normal eyes, with HOAs comprising the remaining 10%. Wavefront aberrations for small pupils are primarily influenced by refractive sphere and cylinder errors, making conventional correction such as spectacles, contact lenses, and laser vision correction effective for improving visual acuity.5–9 However, it has been observed that HOAs have a significant impact on the retinal image quality, especially in night vision with large pupils in normal eyes and in postoperative eyes after laser vision correction.7–9
Laser vision correction is a surgical procedure that uses a laser platform to reshape the cornea and correct the eye’s refractive sphere and cylinder errors, such as myopia, hyperopia, and astigmatism. Conventional correction through laser vision correction eliminates the need for spectacles and contact lenses thereby enhancing patients’ quality of life.10,11 Laser-assisted in-situ keratomileusis (LASIK), initially pioneered by Pallikaris et al in 1990,12 utilizes an excimer laser platform to reshape the corneal stroma after creating a flap through a microkeratome in earlier years13,14 or a femtosecond laser when the iFS® Advanced Femtosecond Laser (Johnson & Johnson Surgical Vision, Inc.) became available.15,16 An alternative method for laser vision correction is laser-assisted lenticule extraction (LALEX) procedure, which uses a femtosecond laser to create a lenticule within the corneal stroma and achieves refractive correction by extracting the lenticule through a small incision. Small incision lenticule extraction (SMILE), first performed by Sekundo and Blum in 2008 with Zeiss VisuMax500 femtosecond laser platform,17–22 has demonstrated comparable visual outcomes for conventional laser vision correction performed via a LASIK procedure.
Laser vision correction demands precise corneal tissue removal to achieve optimal visual outcomes. However, clinical observations indicate that HOAs, particularly coma and spherical aberration, tend to increase significantly after laser vision correction following a LASIK or SMILE procedure.23–30 These HOAs can result in symptoms such as halos, glare, and reduced contrast sensitivity, especially for night vision when pupils become larger due to low-light conditions.13,14
ELITA Femtosecond Platform is a new generation femtosecond (FS) laser platform developed for corneal refractive surgery by Johnson & Johnson Surgical Vision, Inc. (Milpitas CA, USA), which received CE Mark approval in March 2023 for SILK lenticule procedure and LASIK flap creation. The ELITA femtosecond laser system utilizes ultralow laser energy and a distinctive biconvex lenticule shape to perform a lenticule extraction SILK procedure for the correction of myopic refractive errors with and without astigmatism. In a clinical study involving 170 eyes, the visual outcomes at the 3-month refractive stability time point demonstrated that ELITA system is safe and effective for correcting myopic refractive errors with and without astigmatism.31 The purpose of this study is to investigate the changes of HOAs in surgical eyes following corneal lenticule extractions made by the SILK procedure using ELITA laser system.
Patients and Methods
Patients
This study was part of a prospective, single-arm, open-label clinical study31 conducted at one site in India (Narayana Nethralaya Eye Hospital, Bangalore) in accordance with the Declaration of Helsinki, ISO 14155:2011, and all other applicable laws and regulations. Human research ethics approval was obtained from the Narayana Nethralaya Ethics Committee (Bangalore, India) prior to beginning the study. The clinical study was registered on www.clinicaltrials.gov as NCT04200898. After written informed consent was obtained and confirmation that all eligibility criteria were met, the SILK procedure was performed by the same cornea-refractive surgeon who had previous experience with the SMILE procedure using VisuMax500 laser system.
A comprehensive preoperative evaluation was performed first by the surgeon for each patient to ensure that the patient was a suitable candidate for SILK procedure. Patients were required to be at least 18 years old and in good health to participate in the clinical study of the SILK procedure for laser vision correction. Inclusion criteria for eligible eyes included a myopic spherical equivalent (SE) refractive error of ≤−12.00 diopters (D) and astigmatism ≤−6.00 D, with at least 250 microns residual corneal stromal thickness after lenticule extraction. Additionally, patients were eligible to have uncorrected distance visual acuity (UCDVA) of 20/40 or worse, corrected distance visual acuity (CDVA) of 20/20 or better, and CDVA that is at least 2 lines better than UCDVA. Patients must also exhibit ≤0.75 D difference between cycloplegic and manifest refraction spheres, stable refractive error for at least 12 months, and have discontinued rigid contact lens wear for at least 4 weeks or soft contact lens wear for at least 2 weeks prior to surgery. Exclusion criteria for surgical eyes include corneal thickness less than 470 microns at the thinnest point, a history of prior intraocular or corneal surgery, corneal abnormalities, active ophthalmic diseases such as keratoconus, clinically significant dry eye syndrome, and evidence of glaucoma. Pupil size under mesopic lighting conditions was also assessed to evaluate the potential impact of postoperative complications such as halos and glare.
This study was part of the Phase II clinical study, which included refractive error range in the surgical eyes between −2.00 D and −6.00 D and astigmatism up to −1.00 D based on manifest refraction at optical infinity. Cyclotorsion correction after docking was available for astigmatism greater than −1. 00 D with SE limited to up to −6.00 D. It included 24 eyes that underwent a corneal refractive lenticule extraction SILK procedure for myopic correction at the Narayana Nethralaya Eye Institute, India. The SILK procedures were performed from April 6, 2021, to September 3, 2021, with preoperative and postoperative eye exams starting on March 27, 2021, and finishing on July 1, 2022.
Surgical Techniques
ELITATM Femtosecond Platform is a new generation of the commercial iFS® Advanced Femtosecond Laser (Johnson & Johnson Surgical Vision, Inc). This innovative FS laser platform is designed to conduct both the flap treatment for a LASIK procedure and the lenticule treatment for a LALEX procedure. It utilizes an ultralow energy per laser pulse (laser energy of 40–90 nJ) along with 1.0 µm focused spot size and tight spot spacing (mean spot spacing of 1.0 µm) for corneal tissue cuts. These features allow for the precise creation of corneal incisions with minimal tissue-bridges. For the SILK procedure, this advanced FS laser platform empowers surgeons to perform lenticule extraction procedure for myopic correction, with or without astigmatism, up to a maximum of −12.00 D sphere, and astigmatism correction up to −6.00 D, with the sum of sphere and cylinder between −1.00 D and −12.00 D using minus cylinder convention based on the manifest refraction at optical infinity.
The SILK procedure with the ELITA system uses a unique biconvex lenticule shape for myopic correction with or without astigmatism. The diagram in Figure 1 illustrates the cross-section of an applanated biconvex lenticule created by the ELITA system within the corneal stroma. The lenticule cutting procedure starts with the creation of the posterior lenticule surface incision, followed by an angled ring cut, an anterior lenticule surface incision, and finishes with the entry incision. The refractive correction is equally applied to both the anterior surface and posterior surface of the lenticule. Each lenticule is meticulously designed with an optical zone for refractive power correction and a transition zone to mitigate the edge effect generated by the ring cut. To prevent tissue tearing at the lenticule’s edge during extraction, a non-refractive flat ranging from 15 to 30 µm thickness is added in the center of the lenticule. The non-refractive flat consists of a layer with a consistent thickness, serving to enhance the mechanical properties of the lenticule.
 |
Figure 1 Biconvex lenticule incision for myopic correction with corneal cuts 1 for lenticule posterior surface, 2 for ring cut, 3 for anterior surface, and 4 for entry. |
Surgical Procedure
The corneal lenticule extraction with the ELITA system is akin to a SMILE procedure performed with the Zeiss VisuMax500 FS laser, which includes docking, femtosecond laser application, lenticule dissection, and extraction.
Prior to treating the eye, the treatment parameters were programmed on the FS laser platform, based on the required correction for manifest refractive errors (sphere and cylinder error) as well as the keratometry measurements (K1 and K2). Additionally, this new FS laser supports corneal markings to ensure proper lenticule centration and compensation for cyclotorsion. Corneal marking was performed before placing the suction ring on the surgical eye for docking. If lenticule treatment includes an astigmatism correction, the surgeon first created two peripheral marks with surgical ink on the nasal and temporal cornea. These nasal and temporal marks were aligned with the horizonal axis while the patient was in an upright position. Subsequently, the surgeon placed a central mark with the surgical ink at the pupil’s center while the eye was viewing a coaxial fixation target under a surgical microscope when the patient was at supine position on the surgical bed. Once docking was achieved under the ELITA system, the surgeon could align the lenticule treatment center with the central mark and adjust the lenticule axis to compensate for any cyclorotation of the surgical eye.
Data Analysis
Each eye underwent a preoperative eye exam, as well as a postoperative eye exam at 1-day, 1-week, 1-month, 3-month and 9-month after the lenticule extraction by the SILK procedure. During the eye exam, manifest refraction for UCDVA and the best corrected distance visual acuity (BCDVA) were conducted using a phoropter. Wavefront aberrations up to the 6th order Zernike polynomials were measured using a commercial iDESIGN® wavefront aberrometer (iDESIGN® Refractive Studio, Johnson & Johnson Surgical Vision, Inc). iDESIGN® Refractive Studio is a wavefront aberrometer, combined with a corneal topographer, which uses a Hartmann-Shark sensor to measure the whole eye’s wavefront aberrations at the pupil plane.
All wavefront measurements were conducted on each eye with a natural pupil while the eye was under mesopic light conditions (non-pharmacologically dilated). This study only included 24 eyes for which wavefront data were available with a pupil size equal to or larger than 6 mm at preoperative and postoperative iDesign wavefront measurements at 1-day, 1-week, 1-month, 3-month, and 9-month visits. Each wavefront measurement was then rescaled to a 6 mm pupil size for the analysis of HOAs. HOAs, such as comas, spherical aberration, and wavefront error of all higher-order aberrations (HOAs RMS) were analyzed based on a 6 mm pupil.
Statistical analyses were conducted using Microsoft Excel 2021 (Microsoft Corporation) to assess the changes of HOAs following SILK procedures in the 24 eyes. The data were analyzed using a paired study control method, where each eye’s preoperative HOAs were used as the control group to compare its postoperative HOAs at multiple time points. Student’s t-tests were performed to compare preoperative HOAs with postoperative HOAs at 1 day, 1 week, 1 month, 3 months, and 9 months. Differences were considered statistically significant when the p-value was less than 0.05.
Results
This prospective study included 24 eyes that underwent corneal lenticule extraction with the ELITA system and completed 9 months of follow-up. The mean age of patients was 22.6 ± 3.9 years, with 42% being women and 58% being men.
The ELITA system utilized ultralow laser energy per pulse, ranging from 58 nJ to 65 nJ, to create the lenticule’s posterior surface and anterior surface. Each lenticule treatment was configured with a 6 mm optical zone and 0.3 mm transition width. The anterior depth of the lenticule treatment was set as 110 μm, and a superior-entry incision width of 3 mm was set for extraction. A non-refraction flat, ranging from 15 μm to 30 μm thickness, was added to the center of each lenticule.
All lenticule cuts were successfully completed on the 24 surgical eyes using the ELITA system. There were no reported instances of suction loss throughout the entire study. In all cases, the lenticules were extracted successfully, with no or minimal additional dissection required.
Visual Outcomes at Postop 9-Month
Table 1 displays the mean manifest refractive errors of the 24 eyes measured both at the preoperative eye exams and at the 9-month postoperative eye exams. The mean manifest refractive SE of these 24 eyes changed from −3.82 to 1.26 D (range from −6.00 to −2.25 D) preoperatively to −0.20 ± 0.15 D (range from −0.50 to 0.00 D) at the 9-month postoperative assessments following the SILK procedures with the ELITA system. For all 24 eyes, the manifest refractions measured at postoperative 9-month visit were within ±0.50 D for manifest refraction sphere, manifest refraction cylinder, and manifest refraction SE.
 |
Table 1 Preoperative and 9-Month Postoperative Refractive Errors of the 24 Eyes |
Table 2 presents the visual outcomes for the UCDVA in the 24 eyes. It indicates that at the postoperative 9-month assessment, 63% of the surgical eyes achieved a UCDVA of 20/16 or better, while all 100% of the surgical eyes obtained a UCDVA of 20/20 or better.
 |
Table 2 Postoperative Uncorrected Distance Visual Acuity (UCDVA) of the 24 Eyes |
Figure 2 illustrates the comparison of BCDVA between the preoperative and the postoperative 9-month assessments, presented as a percentage of BCDVA for all eyes. It demonstrates that after lenticule extraction with the ELITA system, BCDVA increased by 37% for 20/16 and 4% for 20/20. More importantly, no patient experienced a loss of any visual acuity line at the 9-month postoperative evaluation. Specifically, at 9 months, no eye lost 1 line, 2 eyes gained 1 line, and 22 eyes (91.7%) had no change in BCDVA.
 |
Figure 2 Comparison of BCDVA between the preoperative and postoperative 9-month assessments. |
Figure 3 shows the linear regression analysis comparing the achieved manifest refractive SE correction at 9 months to the intended manifest refractive SE correction. With a regression line slope close to 1 (0.974) and a high R-squared value (0.9844), the scatter plot indicates that the achieved manifest refractive SE correction at the 9 months was on target in terms of magnitude. This demonstrates highly predictable visual outcomes following the SILK procedure using the ELITA system. All eyes (100%) achieved a visual outcome of manifest refractive SE within ±0.50 D.
 |
Figure 3 Intended vs achieved manifest refractive SE at postoperative 9-month assessment of the 24 surgical eyes (Solid lines showing range of ±0.50 D). |
Higher-Order Aberrations
Figure 4 displays the mean HOAs with a 6 mm pupil for the 24 eyes following lenticule extraction with the ELITA system. At 9 months, the average vertical coma Z(3, −1) was −0.054 ± 0.186 µm, horizontal coma Z(3, 1) was 0.016 ± 0.124 µm, the spherical aberration Z(4, 0) was 0.046 ± 0.163 µm, and the wavefront error of all higher-order aberrations HOAs RMS was 0.363 ± 0.115 µm with a 6 mm pupil. In comparison to the preoperative HOAs, the postoperative HOAs were significantly increased at the 1-day postoperative assessment (P = 0.015 for Z(3,-1); P = 0.001 for Z(4, 0); P = 0.000 for HOAs RMS) (as shown in Table 3). However, there was no significant difference in HOAs at 1-week, 1-month, 3-month and 9-month follow-up.
 |
Table 3 Statistical Changes of Postoperative HOAs at Each Time Points Compared to Preoperative HOAs from the 24 Eyes |
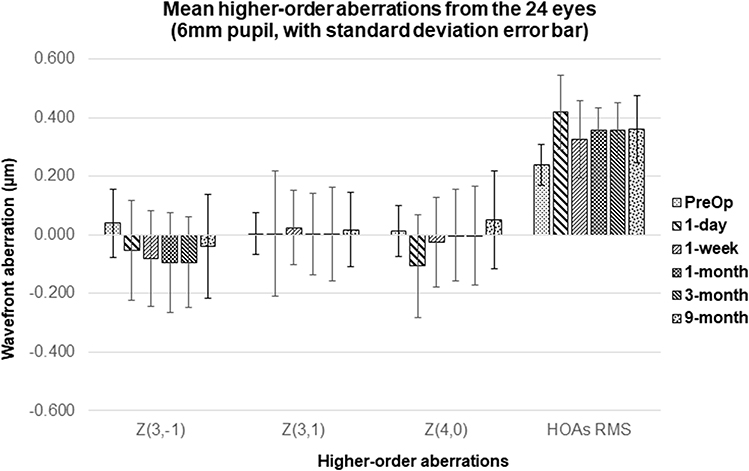 |
Figure 4 HOAs before and after corneal lenticule extractions. |
Table 3 presents the statistical differences in the HOAs between the preoperative and postoperative assessments in the 24 surgical eyes. When comparing the preoperative HOAs, it is notable that there were no significant changes observed for horizontal coma Z(3, 1) and spherical aberration Z(4, 0), starting at the 1-week postoperative HOAs evaluation. However, the observed increase of vertical coma Z(3, −1) in the postoperative eyes could potentially be attributed to the superior position of the entry cut and centration errors during the lenticule treatments.
Discussion
The application of FS laser technology in LALEX has progressed significantly over the past 15 years. Compared to the FS-LASIK procedure for refractive surgery, the entire LALEX procedure only needs one laser for correcting myopia with or without astigmatism. The LALEX procedure requires less corneal tissue removal and involves a smaller incision, making it safer for patients with thinner corneas. Additionally, the LALEX procedure performs better in correcting high myopia, as it better maintains corneal structural integrity and biomechanical stability.
The potential benefits of the LALEX procedure over LASIK also include no flap-related complications both intraoperatively and postoperatively, reducing the risk of flap wrinkles, displacement, and dry eye disease.25,32–34 Because the LALEX procedure involves a small incision of 2–4 mm, compared to the approximately 20 mm larger flap in LASIK, there is less damage to the corneal nerves, reducing the risk of postoperative dry eye. This makes the LALEX procedure suitable for patients who already have dry eye symptoms or concerns about developing dry eye.
This study was part of the phase II clinical study of the SILK procedure using the ELITA system, which included patients with mild to moderate myopia. It used a 6 mm large pupil to investigate the changes in HOAs in surgical eyes after the SILK procedure. Since all wavefront measurements were performed on each eye’s natural mesopic pupil, the sample size and wavefront data were limited by the availability of wavefront measurements obtained with a pupil size equal to or larger than 6 mm at all preoperative and postoperative visits. Because this study is a paired comparison of preoperative and postoperative aberrations in the same eyes, it allows for a smaller sample size due to the reduced variability of HOA measurements. The sample size of 24 eyes out of 170 used in this study is comparable to the 18 eyes out of 357 used for 6 mm pupil wavefront analysis in SMILE procedure submitted for FDA approval on October 4, 2018.35
In this study, all surgical eyes achieved a good visual outcome SE within ±0.50 D of emmetropia and no eyes experienced any loss of visual acuity line at 9-month follow-up. Therefore, lenticule extraction with SILK procedure using the ELITA system is safe and predictable for myopic correction.
Wavefront aberrations measured in surgical eyes can offer comprehensive optical information both before and after laser vision correction, and a method used to evaluate the treatment outcome of refractive surgery. HOAs were evaluated in this study using a 6 mm pupil size, which is larger than the 5 mm pupil size usually used in other HOAs studies28,29 to assess HOAs in surgical eyes after SMILE procedures. The results for a 6 mm pupil revealed low HOAs induced by the ELITA system in surgical eyes following the corneal lenticule extraction with SILK procedure. When compared to baseline preoperative HOAs, postoperative HOAs first increased at 1-day then subsequently stabilized starting at 1-week follow-up. This observation demonstrates a fast corneal wound healing response after the SILK procedure using the ELITA system for myopic correction.
The HOAs in surgical eyes after laser vision correction can vary with the preoperative eye exams, the laser technology and technique used in the refractive surgery, and the individual corneal healing response. Figure 5 compares the average HOAs with a 6 mm pupil at the preoperative eye exams and at the 3-month postoperative visit. It shows that small amounts of the 3rd order, 4th order and HOAs RMS, including coma, spherical aberration, trefoil, secondary astigmatism, and wavefront error all HOAs, are presented in a 6 mm pupil at the 3-month follow-up compared to baseline values. Compared to the postop 3-month HOAs after the SMILE procedure,30 lenticule treatment for mild to moderate myopia made by the SILK procedure induced fewer HOAs in the surgical eyes at the 3-month postoperative assessment.
 |
Figure 5 Postop 3-month HOAs in a 6 mm pupil after the SILK procedure using the ELITA system. |
We believe the minimal induction of HOAs, and the rapid corneal recovery observed after the lenticule extraction made by SILK procedure can be attributable to several factors of the ELITA system, including the use of a high-precision digital encoder guided scanning system that achieves sub-micron accuracy in thickness profile scanning,36 and the easy lenticule removal, which minimizes the unwanted deformation of corneal shape due to surgeon’s mechanical separation of the lenticule interfaces.37
It is well known that the quality of the corneal treatment surface is correlated directly with the surgical eye’s HOAs, which are critical for achieving an optimal vision correction. Studies have reported less induction of HOAs with the femtosecond laser than microkeratomes during LASIK.38,39 The quality of the corneal lenticular surface can be significantly impacted by some parameters of the FS laser, such as pulse repetition, pulse energy, focus spot size, and spot spacing. Research has demonstrated that the FS laser using lower energy pulse and tighter spot creates smoother corneal stromal beds, both in FS-LASIK flap procedures39 and lenticule extraction procedures.40 A recent study has also shown that the Clear procedure with Ziemer FEMTO LDV Z8, using lower FS energy and overlapping spot density, produced smoother lenticule surfaces for corneal lenticule extraction.41 Literature on SMILE procedures42–44 has indicated that patients treated with the VisuMax500 using lower energy settings and smaller spot spacing (laser energy of 125–135 nJ; spot spacing of 4.5 μm) achieved significantly smoother separations, faster visual recovery, and improved visual outcomes.
The SILK procedure using the ELITA system employs a unique biconvex lenticule shape for myopic correction. It utilizes symmetric lenticule posterior and anterior lenticule shape to minimize surface mismatch between the two lenticular interfaces following lenticule removal.31 Mismatched lenticule anterior and posterior surfaces can potentially lead to corneal folds and wrinkles in the lenticule interface, resulting in corneal HOAs and light scattering after lenticule removal. Considering that the biomechanical strength of the cornea decreases as a function of the corneal depth moving from anterior to posterior, the biconvex lenticule shape also offers superior corneal biomechanics compared to a plano-convex lenticule shape, as it requires less tissue cutting in the anterior stroma.
Various studies have observed significant increases in spherical aberration following laser vision correction.45–47 It is well known that there is an interaction between defocus and spherical aberration,48 and the induced spherical aberration after laser vision correction not only degrades retinal image quality but also impacts the subjective refraction of defocus. Several studies48–51 have proposed possible reasons for the induced spherical aberrations and have developed new treatment algorithms, including wavefront-optimized LASIK procedure and wavefront-guided LASIK procedure, aimed at reducing the spherical aberrations and HOAs in postoperative surgical eyes.
This study showed that spherical aberration was not induced after the lenticule extraction procedure with the ELITA system for myopic correction. This utilization of a flat patient interface for docking the surgical eye on the ELITA system eliminates the cosine effect and delivers uniform laser energy pulses across the entire treatment field of view. Additionally, the unique biconvex lenticule shape employed in lenticule extraction for myopic correction may lead to less corneal biomechanical response and epithelial remodeling, which contribute to the induced spherical aberration in surgical eyes after laser vision correction.52
Inappropriate centration during the surgical procedure may result in the misplacement of the treatment optical zone on the surgical eye, which can subsequently lead to an increase of HOAs, such as the increased vertical coma and wavefront error of all HOAs53–55 observed in this study. The current SILK procedure allows surgeons to adjust the treatment center after docking in two ways: either to the applanated pupil center or the applanated corneal central mark placed under a microscope before the lenticule treatment. However, using the applanated pupil center as the treatment center is not reliable for lenticule extraction due to either patient losing fixation during applanation from increased intraocular pressure or possible corneal displacement relative to the eye’s pupil caused by suction and docking process. In this study, the lenticule treatment center was manually adjusted by the surgeon to the central mark after docking. Nevertheless, the accuracy of manual centration depends on the experience and skill of the surgeons, which can result in centration errors caused by the misplacement of central mark under the microscope and the positioning of the treatment center on the ELITA system. The induced coma aberrations are expected to decrease when the auto-centration is available for the SILK procedure using the ELITA system.
Conclusions
This study has demonstrated that the SILK procedure using ELITA femtosecond laser system is efficient and predictable for the correction of myopic refractive errors with and without astigmatism. The changes in HOAs over a 9-month follow-up period following the SILK procedure were evaluated. One of the most distinctive feature settings in the SILK procedure compared to other lenticule extraction procedures is the utilization of ultralow laser energy pulses and an innovatively designed biconvex lenticule shape for myopic correction. In this study, the achieved visual outcomes were within ±0.50 D of emmetropia while inducing minimal HOAs in the surgical eyes after corneal lenticule extraction with SILK procedures using the ELITA system. Furthermore, rapid corneal recovery was demonstrated starting at the 1-week follow-up visit, and no spherical aberration was induced from the SILK procedures.
Data Sharing Statement
The authors do not intend to share individual deidentified participant data. A summarized report with endpoint data tables based on statistical planning and analysis may be requested directly from the corresponding author for consideration.
Acknowledgments
Li Chen and Pooja Khamar are co-first authors of this study. The authors would like to acknowledge Andrew Voorhees, Michal Laron, Carmen Jones, Priya Janakiraman, Brian Schwam, Luis Vargas, and Jesse Nelson for their assistance with this study.
Funding
This study was supported by Johnson & Johnson Surgical Vision, Inc., which participated in the design and conduct of the study.
Disclosure
L.C., Y. W., and H.F. are employees of Johnson & Johnson Surgical Vision, Inc. P.K. and R.S. perform research supported by Johnson & Johnson Surgical Vision, Inc. The authors report no other conflicts of interest in this work.
References
1. Liang J, Grimm B, Goelz S, Bille JF. Objective measurement of wave aberrations of the human eye with use of a Hartmann-Shack wave-front sensor. J Opt Soc Am A. 1994;11(7):1949–1957. doi:10.1364/JOSAA.11.001949
2. Liang J, Williams DR. Aberrations and retinal image quality of the normal human eye. J Opt Soc Am A. 1997;14(11):2873–2883. doi:10.1364/JOSAA.14.002873
3. Thibos LN, Applegate RA, Schwiegerling JT, Webb R. Standards for reporting optical aberrations of eyes. J Refract Surg. 2002;18(5):S652–S660. doi:10.3928/1081-597X-20020901-30
4. Salmon TO, Van de Pol C. Normal-eye Zernike coefficients and root-mean-square wavefront errors. J Cataract Refract Surg. 2006;32(12):2064–2074. doi:10.1016/j.jcrs.2006.07.022
5. Porter J, Guirao A, Cox I, Williams DR. Monochromatic aberrations of the human eye in a large population. J Opt Soc Am A. 2001;18(8):1793–1803. doi:10.1364/JOSAA.18.001793
6. Lombardo M, Lombardo G. Wave aberration of human eyes and new descriptors of image optical quality and visual performance. J Cataract Refract Surg. 2010;36(2):313–331. doi:10.1016/j.jcrs.2009.09.026
7. Yoon GY, Williams DR. Visual performance after correcting the monochromatic and chromatic aberrations of the eye. J Opt Soc Am A. 2002;19(2):266–275. doi:10.1364/JOSAA.19.000266
8. Wang L, Santaella RM, Booth M, Koch DD. Higher-order aberrations from the internal optics of the eye. J Cataract Refract Surg. 2005;31(8):1512–1519. doi:10.1016/j.jcrs.2004.01.048
9. Miller JM, Anwaruddin R, Straub J, Schwiegerling J. Higher order aberrations in normal, dilated, intraocular lens, and laser in situ keratomileusis corneas. J Refract Surg. 2002;18(5):S579–S583. doi:10.3928/1081-597X-20020901-16
10. Sugar A, Hood CT, Mian SI. Patient-reported outcomes following LASIK: quality of Life in the PROWL Studies. JAMA. 2017;317(2):204–205. doi:10.1001/jama.2016.19323
11. Ang M, Gatinel D, Reinstein DZ, Mertens E, Del Barrio JL A, Alió JL. Refractive surgery beyond 2020. Eye. 2021;35(2):362–382. doi:10.1038/s41433-020-1096-5
12. Pallikaris IG, Papatzanaki ME, Stathi EZ, Frenschock O, Georgiadis A. Laser in situ keratomileusis. Lasers Surg Med. 1990;10(5):463–468. doi:10.1002/lsm.1900100511
13. Knorz MC. Flap and interface complications in LASIK. Curr Opin Ophthalmol. 2002;13(4):242–245. doi:10.1097/00055735-200208000-00010
14. Ambrosio RJ, Wilson SE. Complications of laser in situ keratomileusis: etiology, prevention, and treatment. J Refract Surg. 2001;17(3):350–379. doi:10.3928/1081-597X-20010501-09
15. Lubatschowski H, Maatz G, Heisterkamp A, et al. Application of ultrashort laser pulses for intrastromal refractive surgery. Graefe’s Arch Clin Exp Ophthalmol. 2000;238(1):33–39. doi:10.1007/s004170050006
16. Ratkay-Traub I, Juhasz T, Horvath C, et al. Ultra-short pulse (femtosecond) laser surgery: initial use in LASIK flap creation. Ophthalmol Clin N Am. 2001;14:347–355.
17. Sekundo W, Kunert KS, Blum M. Small incision corneal refractive surgery using the small incision lenticule extraction (SMILE) procedure for the correction of myopia and myopic astigmatism: results of a 6-month prospective study. Br J Ophthalmol. 2011;95(3):335–339. doi:10.1136/bjo.2009.174284
18. Shah R, Shah S, Sengupta S. Results of small incision lenticule extraction: all-in-one femtosecond laser refractive surgery. J Cataract Refract Surg. 2011;37(1):127–137. doi:10.1016/j.jcrs.2010.07.033
19. Kamiya K, Shimizu K, Igarashi A, Kobashi H. Visual and refractive outcomes of femtosecond lenticule extraction and small incision lenticule extraction for myopia. Am J Ophthalmol. 2014;157(1):128–134. doi:10.1016/j.ajo.2013.08.011
20. Moshirfar M, McCaughey MV, Reinstein DZ, Shah R, Santiago-Caban L, Fenzl CR. Small-incision lenticule extraction. J Cataract Refract Surg. 2015;41(3):652–665. doi:10.1016/j.jcrs.2015.02.006
21. Reinstein DZ, Archer TJ, Carp GI. The Surgeon’s Guide to Small Incision Lenticule Extraction (SMILE). Thorofare, New Jersey: SLACK Incorporated; 2018.
22. Moshirfar M, Murri MS, Shah TJ, et al. Initial single-site surgical experience with SMILE: a comparison of results to FDA SMILE, and the earliest and latest generation of LASIK. Ophthalmol Ther. 2018;7(2):347–360. doi:10.1007/s40123-018-0137-7
23. Moreno-Barriuso E, Merayo Lloves J, Marcos S, et al. Ocular aberrations before and after myopic corneal refractive surgery: LASIK-induced changes measured with laser ray tracing. Invest Ophthalmol Vis Sci. 2001;42(6):1396–1403.
24. Mrochen M, Kaemmerer M, Mierdel P, Seiler T. Increased higher-order optical aberrations after laser refractive surgery; a problem of subclinical decentration. J Cataract Refract Surg. 2001;27(3):362–369. doi:10.1016/S0886-3350(00)00806-3
25. Waheed S, Chalita MR, Xu M, et al. Flap-induced and laser-induced ocular aberrations in a two-step LASIK procedure. J Refract Surg. 2004;21(4):346–352. doi:10.3928/1081-597X-20050701-08
26. Li X, Wang Y, Dou R. Aberration compensation between anterior and posterior corneal surfaces after Small incision lenticule extraction and Femtosecond laser-assisted laser in-situ keratomileusis. Ophthalmic Physiol Opt. 2015;35(5):540–551. doi:10.1111/opo.12226
27. Liu M, Chen Y, Wang D, et al. Clinical outcomes after SMILE and Femtosecond laser-assisted LASIK for myopia and myopic astigmatism: a prospective randomized comparative study. Cornea. 2016;35(2):210–216. doi:10.1097/ICO.0000000000000707
28. Chen X, Wang Y, Zhang J, Yang SN, Li X, Zhang L. Comparison of ocular higher-order aberrations after SMILE and Wavefront-guided Femtosecond LASIK for myopia. BMC Ophthalmol. 2017;17(1):42. doi:10.1186/s12886-017-0431-5
29. Hamilton DR, Chen AC, Khorrami R, Nutkiewicz M, Nejad M. Comparison of early visual outcomes after low-energy SMILE, high-energy SMILE, and LASIK for myopia and myopic astigmatism in the United States. J Cataract Refract Surg. 2021;47(1):18–26. doi:10.1097/j.jcrs.0000000000000368
30. Jin HY, Wan T, Wu F, Yao K. Comparison of visual results and higher-order aberrations after small incision lenticule extraction (SMILE): high myopia vs. mild to moderate myopia. BMC Ophthalmol. 2017;17(1):118. doi:10.1186/s12886-017-0507-2
31. Sachdev MS, Shetty R, Khamar P, et al. Safety and effectiveness of smooth incision lenticular keratomileusis (SILKTM) using the ELITA(TM) femtosecond laser system for correction of myopic and astigmatic refractive errors. Clin Ophthalmol. 2023;17:3761–3773. doi:10.2147/OPTH.S432459
32. Feng YF, Yu JG, Wang DD, et al. The effect of hinge location on corneal sensation and dry eye after LASIK: a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2013;251(1):357–366. doi:10.1007/s00417-012-2078-5
33. Xu Y, Yang Y. Dry eye after small incision lenticule extraction and LASIK for myopia. J Refract Surg. 2014;30(3):186–190. doi:10.3928/1081597X-20140219-02
34. Denoyer A, Landman E, Trinh L, et al. Dry eye disease after refractive surgery: comparative outcomes of small incision lenticule extraction versus LASIK. Ophthalmology. 2015;122(4):669–676. doi:10.1016/j.ophtha.2014.10.004
35. United States Food and Drug Administration. Summary of safety and effectiveness data (P150040/S003). Available from: https://www.accessdata.fda.gov/cdrh_docs/pdf15/p150040s003b.pdf.
36. Chen L, Bing L, Fu H. Evaluating the accuracy of refractive lenticule created by a new femtosecond laser in glass. Invest Ophthalmol Visual Sci. 2020;61(7):3592.
37. Minoguchi H, Rahaman R, Gao G, Umar A, Fu H. Assessment of corneal tissue interface quality for optimization of femtosecond laser SILK refractive surgery. Invest Ophthalmol Visual Sci. 2024;65:1065.
38. Sarayba MA, Ignacio TS, Binder PS, Tran DB. Comparative study of stromal bed quality by using mechanical, IntraLase femtosecond laser F15- and 30-kHz microkeratomes. Cornea. 2007;26(4):446–451. doi:10.1097/ICO.0b013e318033e7cc
39. Durrie DS, Kezirian GM. Femtosecond laser versus mechanical keratome flaps in wavefront-guided laser in situ keratomileusis: prospective contralateral eye study. J Cataract Refract Surg. 2005;31(1):120–126. doi:10.1016/j.jcrs.2004.09.046
40. Izquierdo L, Sossa D, Ben-Shaul O, Henriquez MA. Corneal lenticule extraction assisted by a low-energy femtosecond laser. J Cataract Refract Surg. 2020;46(9):1217–1221. doi:10.1097/j.jcrs.0000000000000236
41. Nanavaty MA, Naveed H, Ashena Z, Mukhija R. Ex-vivo study on the surface quality of corneal lenticule and stroma after low energy femtosecond laser lenticule extraction. Sci Rep. 2022;12(1):10034. doi:10.1038/s41598-022-13468-8
42. Ji YW, Kim M, Yong Kang DS, et al. Lower laser energy levels lead to better visual recovery after small incision lenticule extraction: prospective, randomized clinical trial. Am J Ophthalmol. 2017;179:159–170. doi:10.1016/j.ajo.2017.05.005
43. Ji YW, Kang DSY, Reinstein DZ, et al. Effect of lowering laser energy on the surface roughness of human corneal lenticules in small incision lenticule extraction. J Refract Surg. 2017;33(9):617–624. doi:10.3928/1081597X-20170620-02
44. Donate D, Thaeron R. Lower energy levels improve visual recovery in small incision lenticule extraction (SMILE). J Refract Surg. 2016;32(9):636–642. doi:10.3928/1081597X-20160602-01
45. Yoon G, Macrae S, Williams DR, Cox IG. Causes of spherical aberration induced by laser refractive surgery. J Cataract Refract Surg. 2005;31(1):127–135. doi:10.1016/j.jcrs.2004.10.046
46. Bottos KM, Leite MT, Aventura-Isidro M, et al. Corneal asphericity and spherical aberration after refractive surgery. J Cataract Refract Surg. 2011;37(6):1109–1115. doi:10.1016/j.jcrs.2010.12.058
47. Wu D, Wang Y, Zhang L, Wei S, Tang X. Corneal biomechanical effects: small-incision lenticule extraction versus femtosecond laser-assisted laser in situ keratomileusis. J Cataract Refract Surg. 2014;40(6):954–962. doi:10.1016/j.jcrs.2013.07.056
48. Chen L, Singer B, Guirao A, Porter J, Williams DR. Image metrics for predicting subjective image quality. Optom Vis Sci. 2005;82(5):358–369. doi:10.1097/01.OPX.0000162647.80768.7F
49. Mrochen M, Donitzky C, Wüllner C, et al. Wavefront-optimized ablation profiles: theoretical background. J Cataract Refract Surg. 2004;30(4):775–785. doi:10.1016/j.jcrs.2004.01.026
50. Schallhorn SC, Farjo AA, Huang D, et al. Wavefront-guided LASIK for the correction of primary myopia and astigmatism a report by the American Academy of Ophthalmology. Ophthalmology. 2008;115(7):1249–1261. doi:10.1016/j.ophtha.2008.04.010
51. Fabrikant A, Dai G, Chernyak D. Optimization of linear filtering model to predict post-LASIK corneal smoothing based on training data sets. Appl Math. 2013;4(12):1694–1701. doi:10.4236/am.2013.412230
52. Voorhees A, Fu H. Finite element comparison of biconvex and Plano-Convex lenticule designs for myopic correction. Invest Ophthalmol Visual Sci. 2024;65:1048.
53. He L, Liu A, Manche EE. Wavefront-guided versus wavefront-optimized laser in situ keratomileusis for patients with myopia: a prospective randomized contralateral eye study. Am J Ophthalmol. 2014;157(6):1170–1178. doi:10.1016/j.ajo.2014.02.037
54. Rozema JJ, Hastings GD, Jiménez-García M, Koppen C, Applegate RA. Influence of rigid lens decentration and rotation on visual image quality in normal and keratoconic eyes. Ophthalmic Physiol Opt. 2022;42(6):1204–1213. doi:10.1111/opo.13045
55. Miraftab M, Hashemi H, Aghamirsalim M, Fayyaz S, Asgari S. Matched comparison of corneal higher order aberrations induced by SMILE to femtosecond assisted LASIK and to PRK in correcting moderate and high myopia: 3.00mm vs. 6.00mm. BMC Ophthalmol. 2021;21(1):216. doi:10.1186/s12886-021-01987-3
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.