")
Back to Journals » Clinical Ophthalmology » Volume 18
Evaluation of Visual Outcomes, Postoperative Angle Alpha, and Angle Kappa After Implantation of Isofocal Intraocular Lenses
Authors Assaf AH , Samy H, Fawky N, Kamel MA
Received 15 May 2024
Accepted for publication 30 September 2024
Published 11 October 2024 Volume 2024:18 Pages 2879—2890
DOI https://doi.org/10.2147/OPTH.S478471
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Ahmed Hassan Assaf,1,2 Hams Samy,2 Noha Fawky,2 Menna Ahmed Kamel1
1Department of Ophthalmology, Ain Shams University, Cairo, Egypt; 2Watany Eye Hospital, Cairo, Egypt
Correspondence: Ahmed Hassan Assaf, Ain Shams University, Abbassia, Cairo, Egypt, Email [email protected]
Purpose: To evaluate the effect of angles kappa and alpha on the visual outcomes after implantation of isofocal intraocular lens (IOL) during cataract surgery.
Methods: This prospective study involved 66 eyes undergoing cataract surgery with Isopure IOLs. Exclusion criteria comprised irregular corneal astigmatism exceeding 1.0D, and ocular co-morbidities affecting visual outcomes post-surgery. Evaluation parameters included postoperative refraction, uncorrected and corrected-distance visual acuity (UDVA, CDVA), uncorrected intermediate visual acuity (UIVA), and distance-corrected intermediate visual acuity (DCIVA) at 80 cm. Additionally, postoperative angles alpha, kappa, and wavefront aberrations at a 3-mm pupil using ray tracing were assessed post-surgery at least 60 days later.
Results: Patients had a mean age of 64.48 ± 9.92 years. Mean postoperative manifest refraction spherical equivalent (MRSE) was − 0.21 ± 0.27 D. Mean UDVA and CDVA were LogMAR 0.06 ± 0.04 and 0.02 ± 0.06, respectively. Mean UIVA LogMAR 0.32 ± 0.08 while mean DCIVA was LogMAR 0.29 ± 0.08. Postoperative angles kappa and alpha were 0.39 ± 0.14 mm and 0.45 ± 0.15 mm, respectively. Mean postoperative ocular RMS higher-order aberrations (HOAs) 0.23 ± 0.08. Spherical aberration, coma, and trefoil averaged 0.05 ± 0.07, 0.12 ± 0.03, and 0.07 ± 0.03, respectively. No significant correlations were observed between postoperative angle kappa and alpha with UDVA, CDVA, or HOAs. A non-significant weak positive correlation was noted between angle kappa and UIVA/DCIVA, while no correlation was found between angle alpha and UIVA/DCIVA.
Conclusion: No substantial correlations were found between various postoperative angles kappa and alpha values and postoperative visual acuity metrics (UDVA, CDVA, UIVA, and DCIVA) or higher order ocular aberrations (including, spherical aberration, coma, and trefoil with a 3.0 mm diameter) in pseudophakic eyes implanted with isofocal intraocular lenses (IOLs).
Keywords: intraocular lens, cataract, optical quality, angle alpha, angle kappa
Introduction
Over the past decade, both new trifocal intraocular lenses (IOLs) and extended-depth-of-focus (EDOF) IOLs have been used trying to meet patients’ expectations for good unaided postoperative visual acuity at all distances (far, intermediate, and near), and many studies have been published achieving high patient satisfaction.1–3 A systematic review and Bayesian network meta-analysis of randomized clinical trials found that EDOF, bifocal, and trifocal IOLs provided better visual acuity than monofocal IOLs. Trifocal IOLs resulted in better uncorrected near visual acuity compared to EDOF IOLs, but no differences were found between EDOF and trifocal IOLs in uncorrected intermediate visual acuity.1 Similarly, another recent review noted that trifocal IOLs significantly improved near visual acuity compared to EDOF IOLs, with no notable differences in distance or intermediate visual acuity, halos, or glare. EDOF IOLs showed better corrected distance vision, while trifocal IOLs excelled in near vision. Both IOL types had similar outcomes for ocular aberration, contrast sensitivity, and patient satisfaction, with trifocal IOLs offering better quality of vision and increased spectacle independence.2 Another review found that trifocal IOLs showed no significant difference in uncorrected distance or near visual acuity in 1 year but did show more improvement in uncorrected intermediate visual acuity compared to bifocal IOLs. Contrast sensitivity results were inconsistent, and some studies found no significant differences in satisfaction or spectacle independence.3
The Isopure 1.2.3. IOL (PhysIOL s.a., Liège, Belgium, part of Beaver-Visitec International, Inc. [BVI], Waltham, USA) is a new aspherical, isofocal intraocular lens designed to improve intermediate vision without diminishing high-quality distance vision.4 Several clinical studies have reported good outcomes with this lens when implanted in patients with cataracts.5–12 Specifically, a large multicentric study with 183 eyes concluded that this new design provides excellent visual performance at distance and functional intermediate visions with an extended range of vision.10 Another randomized, single-masked study of bilateral isofocal or monofocal IOLs implanted in 127 patients concluded that both lenses offered excellent visual acuity and contrast sensitivity at distances with similar photic phenomena, but the isofocal model improved unaided intermediate visual performance.12 In vitro studies have also analyzed this lens using different metrics,13–16 and some found that the lens’ optical performance at −1 D was better than that of a monofocal IOL,14 while others concluded that it revealed a good balance between depth-of-focus (about 1.50 D) and optical quality under different conditions.15 The in vivo optical quality of the Isopure lens needs to be measured to fully characterize the optical performance of the lens when implanted.
Furthermore, Karhanová et al proposed measuring angle alpha and angle kappa preoperatively to reduce the postoperative risk for pronounced photic phenomena after implanting diffractive multifocal IOLs17. To the best of our knowledge, no in vivo studies have assessed the effect of angles kappa and alpha on the visual outcomes after implantation of the Isopure lens.
All the above studies examined the impact of preoperative angle kappa and alpha on visual outcomes. Given that both angle kappa and alpha can undergo changes following cataract surgery, with angle kappa showing more pronounced variability, we chose to focus exclusively on postoperative angle kappa and alpha in our investigation. To our knowledge, there are no in vivo studies that have investigated the influence of postoperative angle kappa and angle alpha on visual outcomes following Isopure lens implantation.
Therefore, the main aim of the current study is to analyze the postoperative visual outcomes of eyes implanted with Isopure IOLs by measuring the visual acuities for far and intermediate distances and ocular wavefront aberration in relation to postoperative angles kappa and alpha values.
Methods
Study Design and Patients
This was a single-center, prospective, nonrandomized, observational study conducted in Egypt. The study protocol was reviewed and approved by the Ethics Committee of Watany Eye Hospital (Cairo, Egypt) in accordance with the tenets of the Declaration of Helsinki. All patients provided written informed consent. The inclusion criteria were patients aged 45 years or older on the day of treatment who had received bilateral Isopure 1.2.3. IOL implants at least 60 days before the study visit. The exclusion criteria were regular corneal astigmatism of more than 1.0 D, irregular corneas, ocular comorbidities, intraoperative complications, and a postoperative absolute manifest spherical equivalent greater than 0.75 D.
Intraocular Lenses and Surgical Procedure
This prospective study of cataract interventions performed following a standard phacoemulsification technique included patients implanted with the Isopure 1.2.3. IOLs. The Isopure IOL is a glistening-free hydrophobic IOL with an ultraviolet and blue light filter and a 4-closed loops haptics platform (overall diameter = 11.0 mm). The material has a refractive index of 1.52, and the 6mm optic part is designed by polynomial technology to increase spherical aberrations that extend the depth of focus compared to monofocal IOLs. The IOL’s power ranged from +10.00 to +30.00 D (0.50 D steps for preloaded systems) and from +31.00 to +35.00 D (1.00 D steps for non-preloaded systems). All the surgical procedures were performed by the same expert surgeon (AA) using topical anesthesia with a 2.2mm incision at 135 degrees, and a 5–5.5 mm continuous capsulorhexis centered on the first Purkinje reflex. The Isopure IOL was implanted in the capsular bag using the dedicated injector system. OVD was washed below and above the IOL after implantation. The IOL centration was performed by the surgeon by positioning the first Purkinje reflex in the center of the IOL optic, based on their subjective judgment while viewing through the surgical microscope with the patient fixating on the microscope‘s light. This alignment was checked again just before concluding the surgery.
Outcome Measures, Analyses, and Sample Size
All patients underwent a complete ophthalmological examination at the preoperative baseline visit, recording monocular Snellen uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), distance corrected intermediate visual acuity (DCIVA), refraction, and optical biometry using the IOLMaster 700 (Carl Zeiss Meditec AG, Jena, Germany). We used the Barrett Universal II formula, and emmetropia was the refractive target in all cases. The following parameters were also measured at least 60 days after the implant surgery: refraction, UDVA, and CDVA. Total higher-order aberrations (HOAs), spherical aberration, coma, and trefoil were measured using iTrace ray-tracing aberrometer (Tracey Technologies, Houston, USA) through a fixed pupil diameter of 3.0 mm. The iTrace device combines a wavefront aberrometer and corneal topographer to obtain data on the eye’s optical properties. It can collect more than 700 raw data fields.18
Furthermore, we also measured Chord-Mu and Chord-Alpha in millimeters. With iTrace, angle alpha measurement assumes the limbus’s central alignment with the optical axis. The geometric center of the elliptical corneal limbus is determined; similarly, for angle kappa, the center of the pupil is determined. The visual axis is ascertained through direct measurement based on the patient’s fixation18–20 (Figure 1). iTrace represents measurements as Cord-Mu for Cord-Alpha for angle Kappa and Alpha, respectively. Measurements are expressed can be presented in cartesian values (X,Y) for statistical analysis or Radial values (R) and angles (A) for better clinical interpretation.
 |
Figure 1 Visual axis through direct measurement based on the patient’s fixation using the Itrace device. Red cross: first Purkinje reflex (proxy for the visual axis). Green cross: Pupillary center (line of sight). Magenta cross: center of the cornea (proxy for the optical axis. Angle Kappa (Chord Mu) and Angle Alpha are represented in green and blue colors, respectively, using either Cartesian values (X & (Y) or radial values (R), which include distance and angles (A). In the bottom right of the image, Angle Kappa Distance and Angle Kappa values are color-coded relative to average values for the age-group population. Yellow indicates slightly above normal, while red indicates above normal values. |
Multiple measurements were recorded for each eye, and the operator selected the three most consistent readings for further analysis. The iTrace software then averaged these selected readings. At least 2 months after surgery, postoperative measurements of Chord-Mu and Chord-Alpha were obtained using the iTrace aberrometer.
The descriptive analysis was summarized using the mean, standard deviation, and range for continuous variables, while all values were converted to a minus cylinder format for refractive outcomes. The sample size was calculated according to a previous study, which considered 22 patients.18 We took this figure as a minimum sample size but aimed to increase the number of subjects analyzed.
Results
In this study, a cohort of 33 consecutive patients (21 females) who underwent implantation of Isopure IOL contributed a total of 66 eyes for analysis. The patients had an average age of 64.48 ± 9.92 years (ranging from 47 years to 84 years). The surgical procedures were performed successfully without encountering complications, and no adverse events were noted during the subsequent follow-up period.
The mean axial length was 23.79± 0.88 (21.85 mm to 25.72mm), and the mean IOL power was 21.29 ± 2.15 (15.50D to 25.50 D). Additional demographic characteristics of the subjects are outlined in Table 1.
 |
Table 1 Demographic Characteristics of Participants Shown as Means, Standard Deviations (SD) and Ranges |
The mean postoperative MRSE was −0.21 ± 0.27 D (ranging from −0.75 to 0.38 D). 54.5% and 30.3% of the eyes exhibited MRSE within the range of −0.50 D to −0.14 D and −0.13 D to +0.13 D, respectively (Figure 2A). Notably, 93.94% of eyes achieved MRSE within ±0.50 D, while 100% fell within ±1.00 D. The mean postoperative refractive cylinder was −0.34 ± 0.19 D (ranging from 0 to −0.75 D) (Figure 2B).
 |
Figure 2 Distribution of postoperative spherical equivalent refraction (A) and refractive cylinder (B, negative value). |
Table 2 shows visual acuity outcomes at a distance of 3 meters and intermediate at 80 cm; the mean UDVA was LogMAR 0.06 ± 0.04 (0.00 to 0.15), while the mean CDVA LogMAR was 0.02 ± 0.06 (−0.10 to 0.10). The mean UIVA was LogMAR 0.32 ± 0.08 (0.15 to 0.50). The mean DCIVA was LogMAR 0.29 ± 0.08 (0.15 to 0.50). More than 95% of all eyes achieved UDVA and CDVA of 20/25, respectively; Figure 3. Regarding the intermediate visual acuity, Figure 4 shows the cumulative distribution of uncorrected and distance-corrected intermediate visual acuity.
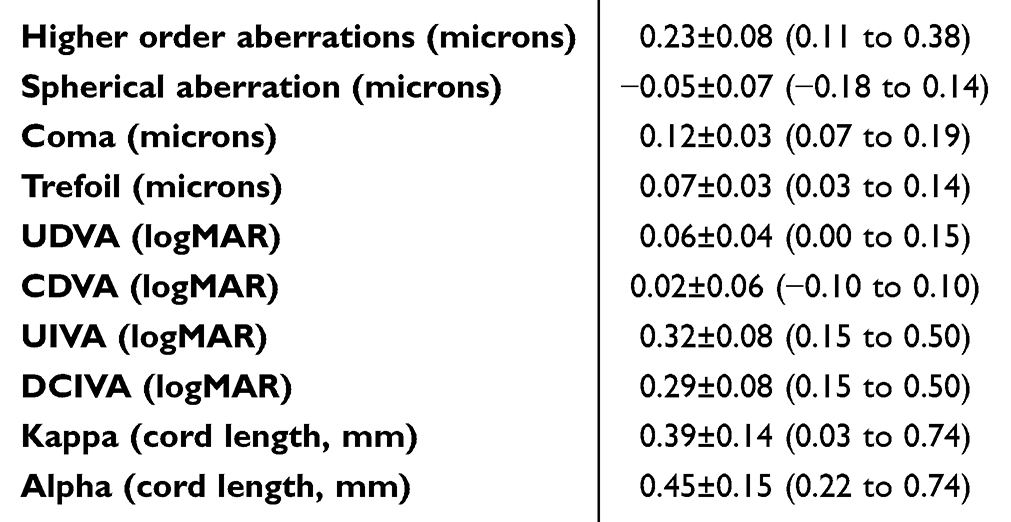 |
Table 2 Postoperative Wavefront Aberration, Visual Acuities, and Angles Alpha and Kappa Shown as Means, Standard Deviations and Ranges |
 |
Figure 3 Cumulative percentage of eyes for different degrees of uncorrected and distance-corrected visual acuity (20/x or better). |
 |
Figure 4 Cumulative percentage of eyes for different degrees of uncorrected and distance-corrected intermediate visual acuity (20/x or better). |
Mean CDVA was significantly better compared to UDVA (p < 0.001). Similarly, distance-corrected intermediate visual acuity (DCIVA) showed a significant enhancement over uncorrected intermediate visual acuity (UIVA) (p = 0.017).
Mean postoperative values of angles kappa and Alpha in cord lengths were 0.39 ± 0.14mm and 0.45 ± 0.15mm, respectively. Mean postoperative ocular RMS HOAs was 0.23 ± 0.08. Mean postoperative spherical aberration, coma, and trefoil were 0.05 ± 0.07, 0.12 ± 0.03, and 0.07 ± 0.03, respectively (Table 2).
Impact of Postoperative Angles Kappa and Alpha on Visual Acuities
There was no correlation between postoperative angle kappa and both postoperative UDVA and CDVA (R2 = 0.0003 and R2 = 0.0004, respectively). (Figure 5B and D). Similarly, there was no correlation between postoperative Chord-Alpha and both postoperative UDVA and CDVA (Figure 5A and C) (R2 = 0.0086 and R2 = 0.0061 respectively).
 |
Figure 5 Scatterplots showing the postoperative correlation between uncorrected distance visual acuity (UDVA) and corrected distance visual acuity (CDVA) with angles alpha and kappa. (A) UDVA vs angle alpha; (B) UDVA vs angle kappa; (C) CDVA vs angle alpha; (D) CDVA vs angle kappa. The continuous line plotted in each graph represents the line of best fit (equation and R2 values also indicated). |
Regarding intermediate visual acuity, there was a weak positive correlation between Chord-Mu and UIVA and DCIVA but did not reach statistical significance (Figure 6B and D) (R2 = 0.0032 and R2 = 0.0185 respectively). Chord-Alpha showed no correlation between UIVA and DCIVA (R2 = 0.0003 and R2 = 0.0008 respectively) (Figure 6A and C).
 |
Figure 6 Scatterplots showing the postoperative correlation between uncorrected intermediate visual acuity (UIVA) and distance-corrected intermediate visual acuity (DCIVA) with angles alpha and kappa. (A) UIVA vs angle alpha; (B) UIVA vs angle kappa; (C) DCIVA vs angle alpha; (D) DCIVA vs angle kappa. The continuous line plotted in each graph represents the line of best fit (equation and R2 values also indicated). |
Impact of Postoperative Angles Kappa and Alpha on HOAs
The study found no statistically significant correlation between Chord-Mu and Chord-Alpha with RMS HOAs, spherical aberration, coma, and trefoil, as indicated in Figure 7.
 |
Figure 7 Scatterplots showing the postoperative correlation between higher-order aberrations (HOAs), coma, spherical aberration (SA) and trefoil with angles alpha and kappa. (A) HOAs vs angle alpha; (B) HOAs vs angle kappa; (C) Coma vs angle alpha; (D) coma vs angle kappa; (E) SA vs angle alpha; (F) SA vs angle kappa; (G) trefoil vs angle alpha; (H) trefoil vs angle kappa. The continuous line plotted in each graph represents the line of best fit (equation and R2 values also indicated). |
Discussion
This study confirms the positive visual outcomes of the Isopure IOL, including solid visual acuity for distance and functional intermediate vision,6,9,10,12,14,21 irrespective of different values of Chord-Mu and Chord-Alpha.
With respect to the refractive target, 93.94% were within ±0.50 D, and 100% within ±1.0 D with a mean postoperative MRSE of −0.21 ± 0.27 D. These values agree with previous clinical studies: 95.7% of eyes within ±1.00 D and 73.2% within ±0.50 D, with a mean MRSE of −0.12 ± 0.42 D;10 and 99.23% of eyes within ±1.00 D and 84.62% within ±0.50 D, plus a mean MRSE of 0.06 ± 0.36 D.12
Isopure IOL, similar to other extended range of vision (ERV) lenses, formerly known as EDOF lenses, shows good tolerance to a residual refractive error with pupil diameters between 2.0 mm and 3.0 mm.5,11,22 Perez-Sanz et al noticed that visual outcomes of the Isopure decline by the presence of astigmatism with a pupil diameter of 4.5mm.11 Although the postoperative mean MRSE remains close to zero in this study, our findings indicate a statistically significant improvement of CDVA over UDVA. A similar trend was noted in the comparison between DCIVA and UIVA. This pattern can be attributed to a slightly larger MRSE compared to the previous studies. Therefore, in addition to the assessment of uncorrected visual acuities for distance and intermediate, we assessed the corrected distance visual acuity for both distances to rule out the influence of the remaining refractive error on the visual results.11,23
This study examined the effects of postoperative Chord-Mu and Chord-Alpha angles on distance and intermediate visual acuity with the Isopure Intraocular Lens (IOL). Drawing from our own clinical observations and existing literature, postoperative Chord-Mu tends to be substantially reduced from its preoperative measurements. In contrast, Chord-Alpha typically shows steady values before and after surgery.24,25 Furthermore, our primary goal was to assess the influence of Chord-Mu and Chord-Alpha on visual outcomes after implantation rather than their use as preoperative predictive indicators. Consequently, we chose to focus our assessment on the influence of the postoperative Chord-Mu and Chord-Alpha on visual outcomes after Isopure Isofocal IOL implantation.
The existing literature lacks information regarding the effects of Chord-Mu and Chord-Alpha on patients who have been implanted with Isopure IOL, which provides no reference points for reviewing our findings. To the best of our knowledge, our study is the first one to investigate the influence of Chord-Mu and Chord-Alpha on the visual outcomes after Isopure IOL implantation.
Concerning Chord-Mu, our findings revealed no correlation with postoperative corrected distance visual acuity. We observed a slight correlation between Chord-Mu and distance-corrected intermediate visual acuity (DCIVA); however, it did not achieve a level of statistical significance (Figure 6).
This outcome is consistent with earlier research that links angle kappa with visual results following multifocal intraocular lens (IOL) implantation.23,26–28 It contrasts with the conclusions of some other studies that view angle kappa as a risk factor for compromised visual outcomes after the implantation of multifocal IOLs.29,30
The average postoperative angle alpha was greater than the postoperative a Chord-Mu (Table 2), and it was anticipated that there would be a correlation between Chord-Alpha and both corrected distance visual acuity (CDVA) and distance-corrected intermediate visual acuity (DCIVA). However, similar to our observations with Chord-Mu, no correlation was found between Chord-Alpha and either distance and intermediate visual acuities. We observed that eyes with Chord-Alpha and Chord-Mu greater than 0.7mm cord length exhibited comparable CDVA and DCIVA to those eyes with smaller kappa and alpha angles, down to 0.3 mm cord length.
We theorize that the varying impacts of Chord-Mu and Chord-Alpha angles reported in previous studies may be due to the differences in the designs of the presbyopia correcting IOLs examined. It is important to note that the lenses in question were all diffractive optic IOLs, and the diameter of their inner rings could play a significant role in connecting the effect of Chord-Mu or Chord-Alpha with visual outcomes.23,26–31 The Isopure lens, in contrast, features neither rings nor zones on its optic surface, which renders it more resilient to functional decentration that could be induced by large Chord-Mu or Chord-Alpha. Based on this aspect, the Isopure lens appears to perform similarly to aspheric monofocal IOLs, as previously reported.32,33 Additionally, the polynomial technology with increased spherical aberrations with a balanced distribution of aberrations between the anterior and posterior surfaces of the lens causes placement of the aberrations close to the nodal point and enhances the lens’s resistance to decentration caused by larger angles of deviation.11,34,35 Nonetheless, future studies should still investigate the potential impact of angles kappa and alpha on visual performance in eyes with larger pupil diameters.
Within the scope of our study, no significant correlation was found between angles kappa and alpha, and higher-order aberrations. However, it is necessary to clarify that total higher-order aberrations (HOAs), spherical aberration, coma, and trefoil were measured using iTrace ray-tracing aberrometer (Tracey Technologies, Houston, USA) through a fixed pupil diameter of 3.0 mm, which is well below the standard diameter between 4.0 and 6.0 mm usually used in studies36,37 However, this finding still suggests that these parameters may have a negligible impact on the higher-order ocular aberrations associated with the Isopure 1.2.3 IOL. Consequently, our findings reinforce that angle kappa and angle alpha do not significantly influence visual acuity or higher-order aberrations in eyes with an aspheric, isofocal IOL (Isopure 1.2.3). On the other hand, to conclude that there is no correlation between different values of postoperative angles kappa and alpha and the visual outcomes of isofocal IOLs, other clinically significant visual variables should also be evaluated, like contrast sensitivity and the area under the curve (AUC) of the defocus curve, which were not considered in the present study.38
In this study, we did not assess the subjective visual quality through subjective contrast sensitivity curves. Instead, our focus was on evaluating the objective visual quality in vivo. Subjective outcomes can be influenced by individual patient personality traits and neural adaptation, which may introduce variability in the results.39,40
In this study, we analyzed the optical performance by assessing wavefront aberrations, and the results are shown in Table 2. The data revealed average ocular RMS HOAs of 0.23 ± 0.08µm, a modest degree of negative spherical aberration (−0.05 ± 0.07), and average coma and trefoil aberrations were 0.12 ± 0.03 and 0.07 ± 0.03, respectively. Bova and Vita6 employed a high-resolution pyramidal wavefront sensor-based aberrometer (Osiris, CSO, Florence, Italy) to study eyes implanted with Isopure IOLs, reporting total ocular aberrations with values of about 0.3 µm for HOAs, −0.05 µm for spherical aberration, 0.10 µm for trefoil, and 0.15 µm for coma at 3 mm pupil diameters. These results closely align with our cohort’s observations using ray-tracing technology.
When comparing their findings to those obtained from eyes implanted with the monofocal Tecnis PCB00 IOL, Bova and Vita observed similar optical aberrations at pupil sizes of 3.0 mm and 5.0 mm in both lens groups. They did, however, note a marginal increase in negative spherical aberration at the larger pupil size in comparison to the monofocal model. Nevertheless, the Isopure IOL did not exacerbate optical aberrations for the entire eye at either 3.0 mm or 5.0 mm, and no statistically significant difference was found between the two IOL groups in terms of spherical aberration (p = 0.22). The authors attributed this outcome to the IOL’s surface design, which incorporates negative pericentral spherical aberration. Optical bench testing demonstrated that the Isopure IOL produced a total negative spherical aberration of approximately −0.07 µm at a pupil diameter of 3.0 mm and a spatial frequency of 50 cycles/mm. This negative aberration is purposefully engineered to enhance the depth of focus, thereby improving intermediate vision following implantation.
Our study further examined the potential correlation between angles kappa and alpha and wavefront aberrations. As illustrated in Figure 7, we found no significant association between the magnitude of aberrations and Chord-Mu and Chord-Alpha.
We can deduce that no significant correlations were observed between different postoperative angles kappa and alpha values and postoperative visual acuity metrics (UDVA, CDVA, UIVA, and DCIVA). Furthermore, there is no correlation with the root mean square (RMS) values of ocular aberrations, encompassing higher-order aberrations, spherical aberration, coma, and trefoil with a 3.0 mm diameter, in pseudophakic eyes fitted with isofocal intraocular lenses (IOLs).
The study has several limitations that should be considered. First, the sample size was relatively small, and a larger number of patients would be beneficial to validate the results obtained in this study further. Additionally, no control group was included in this study. The primary objective was to investigate the impact of functional decentration on the visual outcomes specifically associated with this lens and to establish a cutoff value beyond which visual quality could be compromised. Another limitation is that higher-order aberrations were measured at a fixed pupil size of 3 mm for all eyes. Recent studies denoted pupil dependency of Isopure IOL with change in MTF and visual quality with a pupil size of 4.5mm.13,16 Hence, because various mesopic pupil sizes were noted among the eyes included, we opted to use a fixed pupil size to avoid introducing a confounding variable that could potentially influence the results. The main focus of this study remains the evaluation of the effect of functional decentration caused by Chord-Mu or Chord-Alpha on the visual outcomes of this lens.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cho JY, Won YK, Park J, et al. Visual Outcomes and Optical Quality of Accommodative, Multifocal, Extended Depth-of-Focus, and Monofocal Intraocular Lenses in Presbyopia-Correcting Cataract Surgery: a Systematic Review and Bayesian Network Meta-analysis. JAMA Ophthalmol. 2022;140(11):1045–1053. doi:10.1001/jamaophthalmol.2022.3667
2. Karam M, Alkhowaiter N, Alkhabbaz A, et al. Extended Depth of Focus Versus Trifocal for Intraocular Lens Implantation: an Updated Systematic Review and Meta-Analysis. Am J Ophthalmol. 2023;251:52–70. doi:10.1016/j.ajo.2023.01.024
3. Zamora-de La Cruz D, Bartlett J, Gutierrez M, Ng SM. Trifocal intraocular lenses versus bifocal intraocular lenses after cataract extraction among participants with presbyopia. Cochrane Database Syst Rev. 2023;1(1):CD012648. doi:10.1002/14651858.CD012648.pub3
4. Gutiérrez DF. Refractive multifocal intraocular lens with optimised optical quality in a range of focus and method to produce it. Patent EP2941222A1. 2013.
5. Stodulka P, Slovak M. Visual performance of a polynomial extended depth of focus intraocular lens. Open J Ophthalmol. 2021;11(03):214–228. doi:10.4236/ojoph.2021.113017
6. Bova A, Vita S. Clinical and Aberrometric Evaluation of a New Monofocal IOL with Intermediate Vision Improvement. J Ophthalmol. 2022;2022:4119698. doi:10.1155/2022/4119698
7. Perez-Sanz L, Charbel C, Poyales F, Garzon N. Influence of isofocal intraocular lenses on objective refraction based on autorefraction and aberrometry. Graefes Arch Clin Exp Ophthalmol. 2023;261(10):2863–2872. doi:10.1007/s00417-023-06102-4
8. Tomagova N, Elahi S, Vandekerckhove K. Clinical Outcomes of a New Non-Diffractive Extended Depth-of-Focus Intraocular Lens Targeted for Mini-Monovision. Clin Ophthalmol. 2023;17:981–990. doi:10.2147/OPTH.S405267
9. Lesieur G, Dupeyre P. A comparative evaluation of three extended depth of focus intraocular lenses. Eur J Ophthalmol. 2023;33(6):2106–2113. doi:10.1177/11206721231154818
10. Bernabeu-Arias G, Beckers S, Rincon-Rosales JL, Tana-Rivero P, Bilbao-Calabuig R. Visual Performance at Different Distances After Implantation of an Isofocal Optic Design Intraocular Lens. J Refract Surg. 2023;39(3):150–157. doi:10.3928/1081597X-20230124-02
11. Perez-Sanz L, Vega F, Azor-Moron JA, Cuellar F, Millan MS, Garzon N. Tolerance to residual astigmatism of an isofocal intraocular lens. Graefes Arch Clin Exp Ophthalmol. 2023;2023:1. doi:10.1007/s00417-023-06305-9
12. Ang RET, Stodulka P, Poyales F. Prospective Randomized Single-Masked Study of Bilateral Isofocal Optic-Design or Monofocal Intraocular Lenses. Clin Ophthalmol. 2023;17:2231–2242. doi:10.2147/OPTH.S425352
13. Azor JA, Vega F, Armengol J, Millan MS. Optical Assessment and Expected Visual Quality of Four Extended Range of Vision Intraocular Lenses. J Refract Surg. 2022;38(11):688–697. doi:10.3928/1081597X-20220926-01
14. Labuz G, Son HS, Naujokaitis T, Yildirim TM, Khoramnia R, Auffarth GU Laboratory Investigation of Preclinical Visual-Quality Metrics and Halo-Size in Enhanced Monofocal Intraocular Lenses. Ophthalmol Ther. 2021;10(4):1093–1104. doi:10.1007/s40123-021-00411-9
15. Lago CM, de Castro A, Benedi-Garcia C, Aissati S, Marcos S. Evaluating the effect of ocular aberrations on the simulated performance of a new refractive IOL design using adaptive optics. Biomed Opt Express. 2022;13(12):6682–6694. doi:10.1364/BOE.473573
16. Alarcon A, Canovas C, Koopman B, Pande MV, Koch DD, Piers P. Optical bench evaluation of the effect of pupil size in new generation monofocal intraocular lenses. BMC Ophthalmol. 2023;23(1):112. doi:10.1186/s12886-023-02839-y
17. Karhanová M, Pluháček F, Mlčák P, Vláčil O, Šín M and Marešová K. (2015). The importance of angle kappa evaluation for implantation of diffractive multifocal intra‐ocular lenses using pseudophakic eye model. Acta Ophthalmologica, 93(2), 10.1111/aos.12521
18. Technologies T iTrace 5.3.0 hiSW & Combo User Manual. 2014:66.
19. Mahr MA, Simpson MJ, Erie JC. Angle alpha orientation and magnitude distribution in a cataract surgery population. J Cataract Refract Surg. 2020;46(3):372–377. doi:10.1097/j.jcrs.0000000000000066
20. Mihaltz K, Vecsei-Marlovits PV. The impact of visual axis position on the optical quality after implantation of multifocal intraocular lenses with different asphericity values. Graefes Arch Clin Exp Ophthalmol. 2021;259(3):673–683. doi:10.1007/s00417-020-05052-5
21. Liu J, Dong Y, Wang Y. Efficacy and safety of extended depth of focus intraocular lenses in cataract surgery: a systematic review and meta-analysis. BMC Ophthalmol. 2019;19(1):198. doi:10.1186/s12886-019-1204-0
22. Bellucci R, Cargnoni M, Bellucci C. Clinical and aberrometric evaluation of a new extended depth-of-focus intraocular lens based on spherical aberration. J Cataract Refract Surg. 2019;45(7):919–926. doi:10.1016/j.jcrs.2019.02.023
23. Cervantes-Coste G, Tapia A, Corredor-Ortega C, et al. The Influence of Angle Alpha, Angle Kappa, and Optical Aberrations on Visual Outcomes after the Implantation of a High-Addition Trifocal IOL. J Clin Med. 2022;11(3):896. doi:10.3390/jcm11030896
24. Sandoval HP, Potvin R, Solomon KD. The Effects of Angle Kappa on Clinical Results and Patient-Reported Outcomes After Implantation of a Trifocal Intraocular Lens. Clin Ophthalmol. 2022;16:1321–1329. doi:10.2147/OPTH.S363536
25. Wang R, Long T, Gu X, Ma T. Changes in angle kappa and angle alpha before and after cataract surgery. J Cataract Refract Surg. 2020;46(3):365–371. doi:10.1097/j.jcrs.0000000000000063
26. Baenninger PB, Rinert J, Bachmann LM, et al. Distribution of preoperative angle alpha and angle kappa values in patients undergoing multifocal refractive lens surgery based on a positive contact lens test. Graefes Arch Clin Exp Ophthalmol. 2022;260(2):621–628. doi:10.1007/s00417-021-05403-w
27. Velasco-Barona C, Corredor-Ortega C, Mendez-Leon A, et al. Influence of Angle kappa and Higher-Order Aberrations on Visual Quality Employing Two Diffractive Trifocal IOLs. J Ophthalmol. 2019;2019:7018937. doi:10.1155/2019/7018937
28. Harrer A, Hirnschall N, Tabernero J, et al. Variability in angle kappa and its influence on higher-order aberrations in pseudophakic eyes. J Cataract Refract Surg. 2017;43(8):1015–1019. doi:10.1016/j.jcrs.2017.05.028
29. Fu Y, Kou J, Chen D, et al. Influence of angle kappa and angle alpha on visual quality after implantation of multifocal intraocular lenses. J Cataract Refract Surg. 2019;45(9):1258–1264. doi:10.1016/j.jcrs.2019.04.003
30. Garzon N, Garcia-Montero M, Lopez-Artero E, et al. Influence of angle kappa on visual and refractive outcomes after implantation of a diffractive trifocal intraocular lens. J Cataract Refract Surg. 2020;46(5):721–727. doi:10.1097/j.jcrs.0000000000000156
31. Prakash G, Prakash DR, Agarwal A, Kumar DA, Agarwal A, Jacob S. Predictive factor and kappa angle analysis for visual satisfactions in patients with multifocal IOL implantation. Eye. 2011;25(9):1187–1193. doi:10.1038/eye.2011.150
32. Bellucci R, Curatolo MC. A New Extended Depth of Focus Intraocular Lens Based on Spherical Aberration. J Refract Surg. 2017;33(6):389–394. doi:10.3928/1081597X-20170329-01
33. Tandogan T, Son HS, Choi CY, Knorz MC, Auffarth GU, Khoramnia R. Laboratory Evaluation of the Influence of Decentration and Pupil Size on the Optical Performance of a Monofocal, Bifocal, and Trifocal Intraocular Lens. J Refract Surg. 2017;33(12):808–812. doi:10.3928/1081597X-20171004-02
34. Benedi-Garcia C, Vinas M, Lago CM, et al. Optical and visual quality of real intraocular lenses physically projected on the patient’s eye. Biomed Opt Express. 2021;12(10):6360–6374. doi:10.1364/BOE.432578
35. Fernandez D, Barbero S, Dorronsoro C, Marcos S. Multifocal intraocular lens providing optimized through-focus performance. Opt Lett. 2013;38(24):5303–5306. doi:10.1364/OL.38.005303
36. AB-P FD, Gimenez G, Altemir I, Larrosa JM, Polo V, Pablo L. Optical aberrations in three different intraocular lens designs of a same platform. Saudi J Ophthalmol. 2021;35(2):126–130. doi:10.4103/1319-4534.337865
37. Steinmuller LN, Greve D, Rua Amaro D, Bertelmann E, Von sonnleithner C. Analysis of higher-order aberrations in relation to the clinical outcome of an enhanced monofocal IOL. Eur J Ophthalmol. 2023;33(6):2096–2105. doi:10.1177/11206721221134171
38. Fernandez J, Rodriguez-Vallejo M, Martinez J, Tauste A, Pinero DP. Biometric Factors Associated with the Visual Performance of a High Addition Multifocal Intraocular Lens. Curr Eye Res. 2018;43(8):998–1005. doi:10.1080/02713683.2018.1478981
39. Ntonti P, Bakirtzis M, Delibasis K, Seimenis I, Tsinopoulos I, Labiris G. Impact of personality on the decision process and on satisfaction rates in pseudophakic presbyopic correction. J Cataract Refract Surg. 2022;48(12):1433–1439. doi:10.1097/j.jcrs.0000000000001021
40. Yeu E, Cuozzo S. Matching the Patient to the Intraocular Lens: preoperative Considerations to Optimize Surgical Outcomes. Ophthalmology. 2021;128(11):e132–e141. doi:10.1016/j.ophtha.2020.08.025
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Refractive and Visual Outcomes of a Monofocal Non-Constant Aberration Aspheric Intraocular Lens
Hernández-Martínez A, Díaz-del-Rio MA, Ruiz-Santos M, Ruiz-Mesa R, Tañá-Rivero P
Clinical Ophthalmology 2022, 16:2521-2530
Published Date: 10 August 2022
The REVIVE Study: Long Term Outcomes of a Novel Non-Diffractive Extended Vision IOL versus Monofocal Control IOL
Shafer BM, McCabe C, Reiser H, Newsom TH, Berdahl J
Clinical Ophthalmology 2022, 16:3945-3950
Published Date: 28 November 2022
Long Term Clinical Outcomes of Hydrophilic and Hydrophobic Versions of a Trifocal IOL with the Same Optical Design
Ang RET
Clinical Ophthalmology 2023, 17:623-632
Published Date: 21 February 2023
Clinical Outcomes of a Monofocal, Optimized, Aspheric, Hydrophobic Acrylic Intraocular Lens Implant
García-Tomás B, Marín-Sánchez JM, García-Elskamp C, Alcon-Ruiz E, Montesinos-López L, García Martínez-Lozano B
Clinical Ophthalmology 2023, 17:3215-3224
Published Date: 27 October 2023
Extended Depth-of-Focus Intraocular Lens Implantation in Patients with Age-Related Macular Degeneration: A Pilot Study
Thananjeyan AL, Siu A, Jennings A, Bala C
Clinical Ophthalmology 2024, 18:451-458
Published Date: 13 February 2024