")
Back to Journals » Clinical Ophthalmology » Volume 18
Evolution of Workload Associated with Anti-VEGF Treatments for AMD, DME, RVO and mCNV in Hospital District of Southwest Finland
Authors Heloterä H, Viita AM, Laine J
Received 24 May 2024
Accepted for publication 20 November 2024
Published 8 December 2024 Volume 2024:18 Pages 3645—3655
DOI https://doi.org/10.2147/OPTH.S479816
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hanna Heloterä,1,2 Anna-Mari Viita,1 Juha Laine1,3
1Roche Oy, Espoo, Finland; 2Department of Ophthalmology, University of Eastern Finland, Kuopio, Finland; 3InFLAMES Flagship, University of Turku, Turku, Finland
Correspondence: Juha Laine, Roche Oy, Finland, Email [email protected]
Background: The prevalence of vision-threatening diseases, such as age-related macular degeneration (AMD) and diabetic macular edema (DME), is likely to increase in developed countries owing to an aging population, rising life expectancy, and unfavorable lifestyle changes. Increases in the burden of vision-threatening diseases pose a challenge to the healthcare system. After the emergence of intravitreal anti-VEGF inhibitors, treatment options for neovascular AMD (nAMD), DME, retinal vein occlusion (RVO) and myopic choroidal neovascularization (myopic CNV) have increased. As this change in treatment practices has occurred over the last two decades, it is important to demonstrate changes in patient numbers and administered treatments to provide solutions for handling the workload and productivity in ophthalmology departments. In addition, the registry data landscape has evolved in Finland in recent years. Thus, understanding the possibilities and limitations of ophthalmology registries and patient information systems is required.
Methods: This study involved the secondary use of retrospectively registered data from the data warehouse of the Hospital District of Southwest Finland. Our goal was to explore how the workload of ophthalmology departments caused by intravitreal injections has evolved from 2015 to 2022.
Results: The ophthalmology department workload increased significantly during our observation period as the total number of patients receiving intravitreal treatments for nAMD, DME, RVO, and myopic CNV increased 199.6% from 2015 to 2021. In addition, the total number of administered anti-VEGF injections increased during our observation period, but the increase rate began to subside (2019– 2020: increase 23.7%, 2020– 2021: increase 10.3%, 2021– 2022: increase 6.7%).
Conclusion: Supporting the utilization of registry data is essential in evidence-based discussions evolving workload in healthcare. However, it is important to understand the limitations and the quality of the registries. Our study contributes to better understanding the Finnish registry perspective, and it demonstrates the increase in workload in ophthalmology departments caused by intravitreal injections.
Keywords: retina, treatment burden, aging, diabetes
Introduction
The prevalence of vision-threatening diseases such as glaucoma, cataract, age-related macular degeneration (AMD), and diabetic retinopathy (DR) is likely to increase in developed countries due to aging population, rising of life expectancy, and unfavorable lifestyle changes such as unhealthy eating habits, and lack of physical activity.1–4 In Finland it is projected that the number of people over 65 years of age will increase by 15.6% over the next 20 years, and by 20.9% during the next 30 years (https://stat.fi/tilasto/vaenn). The increased burden of vision-threatening diseases will pose a significant burden on the healthcare system, as well as on individuals suffering from disabling eye diseases. After the emergence of intravitreal anti-VEGF inhibitors, treatment options for certain retinal vascular diseases have increased. These treatment options which can slow down the disease progression can provide patients more time with better vision, but it will also lead to increased numbers of patients treated in ophthalmology departments, and raise the need for more efficient resource allocation. As this change in treatment practices has occurred over the last two decades, it is important to be able to produce evidence of the changed resource needs of ophthalmology clinics.5–7 At the time of study initiation, aflibercept, the most commonly used on-label product for ophthalmic vasculature-related conditions had the following indications: neovascular age-related macular edema (nAMD), diabetic macular edema (DME), retinal vein occlusion (RVO), and myopic choroidal neovascularization (myopic CNV). The study will focus on these indications.
In 2020 in Finland in the age group of +65 years the majority (70.1%) of new cases of visual impairment were due to AMD, 1.5% were due to DR, and 2.9% were due to retinal vascular occlusion. In the age group–18-64 years, 4.3% of new visual impairments are due to DR.8 Interestingly, Purola et al recently reported stagnation in the incidence and prevalence of visual impairment due to AMD in Finland from 2010. The authors suggested that recent treatment options have reduced the amount of visual impairment caused by nAMD.9 It has also been reported that the incidence rates of visual impairment due to DR in Finland have been declining and shifting to older ages in the 2000s and the 2010s, regardless of the increasing prevalence of diabetes. In addition to the emergence of intravitreal treatment, this result may reflect improvements in the care of patients with underlying diabetes.10
The Finnish national guidelines recommend the use of intravitreal anti-VEGF therapies for the treatment of nAMD. Currently recommended therapies include bevacizumab, ranibizumab, and aflibercept, administered at fixed, pro re nata (PRN), or treat-and-extend (T&E) intervals. This guideline recommends the use of bevacizumab as a first-line treatment which will be continued as long as a treatment response is observed.11 A decision to switch to another therapy is based on physicians’ evaluation of treatment response, and any changes in visual acuity, as well as swelling or fluid observed in the optical coherence tomography.11 In addition to bevacizumab, aflibercept has also been widely used in Finland, especially after bevacizumab has clinically failed, while treatment with ranibizumab has remained marginal.12 Two other treatment options, brolucizumab and faricimab have been approved for use after the publications of these guidelines.13–16 This study does not include these treatment options as they had not yet been in clinical use during the analysis period. Treatment options for DME and RVO include corticosteroids (intravitreal and implants) in addition to the anti-VEGF therapy.5,6
This study aims to identify patient numbers associated with intravitreal injections in the Hospital District of Southwest Finland and to study the usefulness of ophthalmology registry data, and patient information systems as reliable data sources. In addition, our goal was to demonstrate how patient numbers and treatment patterns have evolved between 2015–2021. Thus, the aim was to demonstrate how the workload (number of intravitreal treatments provided per year) of ophthalmology departments in the hospital district of Southwest Finland evolved during the observation period.
Materials and Methods
This study was based on retrospective registered data from the data warehouse of the Hospital District of Southwest Finland (HDSF). Auria Clinical Informatics (ACI) is a part of hospital operations and operates in connection with the Turku University Hospital District (currently The Wellbeing Services County of Southwest Finland, WSCSF), Satasairaala, and Vaasa Central Hospital, but our data included only data from the Turku University Hospital District. This study was conducted with permission from the Hospital District of Western Finland (permit no. T55_2022_SP-3168743), and the Act on the Secondary Use of Health and Social Data (Finland’s Ministry of Justice 552/2019). Therefore, the requirement for informed consent from patients was waived. Descriptive statistical analyses were performed using R 4.0.3, 4.2.2, SPSS 27 and Microsoft Excel. We did not apply imputation to the missing values. Data was stored and analyzed in Findata’s (the Finnish Social and Health Data Permit Authority) secured processing environment, KAPSELI, and the anonymity of the output tables and figures was confirmed by Findata.
The study focused on patients receiving and initiating intravitreal anti-VEGF treatment (ranibizumab, aflibercept, or bevacizumab) for wAMD (ICD-10 h35.31), DME (ICD-10 h36.01), RVO (ICD-10 h34.8), or myopic CNV (ICD-10 h44.2), during each year from to 2015–2022. The data search process was divided into two parts. First-wave data for the years 2015–2021 was collected from the Oberon database (Figure 1). Oberon is an operational management system and part of the Uranus patient information system delivered by the CGI at the Turku University Hospital. In that analysis, anti-VEGF data for the years 2019–2021 was complemented by data from the ophthalmology quality registry provided by BCB Medical. However, we observed that laterality information in the Oberon database was incomplete; thus, a second data search was performed using BCB data only for the years 2019–2022. Only patient and injection numbers were analyzed using the BCB registry data. Patients who initiated treatment each year were analyzed separately as incident cohorts by diagnosis (wAMD, DME, RVO, and myopic CNV) and the first anti-VEGF agent received. Incident patients were defined as those who had not received treatment within the years prior to the first anti-VEGF administration within the study period. Data from 2014 were also used to construct the first incident cohort in 2015. Annual incident cohorts were recorded between 2015 and 2021.
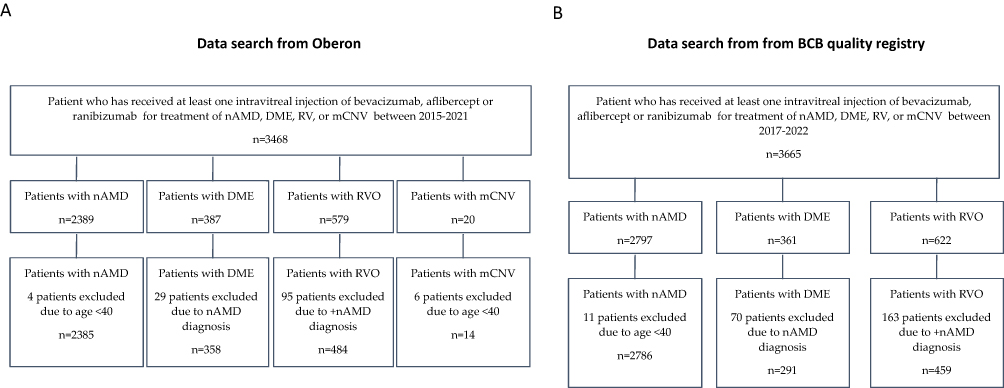 |
Figure 1 Patient distribution. (A) Patient distribution between therapeutic areas in data search made from Oberon for the years 2015–2021. Data was supplemented with anti-VEGF data from the BCB registry for the years 2019–2021. (B) Patient distribution between therapeutic areas in data search made from the BCB quality registry for the years 2019–2022. |
The workload was analyzed by recording individual intravitreal treatment (IVT) visits that were detected by procedure codes CKD05 and CKW99, as well as by analyzing visits that were related to individual treatments (bevacizumab, ATC code L01XC07; aflibercept, ATC code S01LA05; ranibizumab, ATC code S01LA04) based on the date of administration. The S01LA08 code can also be used for intravitreal bevacizumab injections, but it was not included in the data for the analysis period. As bevacizumab is considered a low-cost treatment in ophthalmology, it has not been recorded in prescription information; however, it was possible to collect bevacizumab data from the quality registry for the years 2018–2021. Before 1.5.2018 CKW99 was used in WSCSF for intravitreal anti-VEGF injections and CKD05 was used for intravitreal corticosteroid implants (Ozurdex, Iluvien). After 1.5.2018 CKD05 was used in the WSCSF for intravitreal anti-VEGF injections and CKW99 for intravitreal corticosteroid implants.
Study Population and Data Search Waves
Patients who received at least one intravitreal injection of bevacizumab, aflibercept, or ranibizumab for the treatment of DME (ICD-10 h36.01), nAMD (ICD-10 h35.31), RVO (ICD-10 h34.8), or mCNV (ICD-10 h44.2) between 2015–2022 were included in this study. The patients were divided into the previously mentioned analysis groups based on the date of their first diagnosis. Patients with DME, RVO, or mCNV at any point were diagnosed with H35.31 (nAMD) diagnosis were excluded from the DME, RVO, and mCNV analyses due to the more aggressive type of nAMD (Figure 1).
The data search was conducted in two waves. In the first wave patient data were collected from the Oberon database for the years 2015–2021. These analyses included 358 DME, 2389 nAMD, 484 RVO, and 14 myopic CNV patients (Figure 1A). Only patients who had received at least one injection of bevacizumab, ranibizumab, or aflibercept were included, but some patients with previously mentioned diagnoses who had not received any anti-VEGF treatment or received only corticosteroids or laser treatments were excluded. Based on these exclusion criteria, 29 patients were excluded from DME analyses, 95 patients were excluded from RVO analyses, and six patients were excluded from myopic CNV analyses. Four patients were excluded from the nAMD analyses due to their age (<40 years). These were either patients with diabetes, those with considered recording errors, or patients who may have had retinal changes requiring intravitreal treatment, while no better code was available.
The observation was, however, that laterality data in the Oberon database were incomplete; thus, a second wave of data search was performed using the quality registry for the years 2019–2022. The data analysis was limited and focused on the number of patients and injections. The analysis included 361 DME patients, 2797 nAMD patients, and 622 RVO patients (Figure 1B). No mCNV recordings were recorded in this study. Due to additional nAMD diagnoses, 70 patients were excluded from the DME analyses and 163 patients were excluded from the RVO analyses. Eleven patients were excluded from the nAMD analyses due to age (<40 years).
Results
Study Population
Based on Oberon data, median age at the time of first anti-VEGF injection ie at the time of entry for our analysis, was 57 years for type 1 diabetic DME patients (SD 14.4 years, RANGE 25–90 years, IQR: Q1-Q3 45–66 years), 67 years for type 2 diabetic patients with DME (SD 9.6 years, RANGE 40–93 years, IQR: Q1-Q3 61–74 years), 81 years for nAMD patients (SD 8.3 years, RANGE 45–101 years, IRQ: Q1-Q3 74–86 years), 75 years for RVO patients (SD 10.6, RANGE 24–96, IQR: Q1-Q3 68–81 years) and 65 years for myopic CNV patients (SD 14.5 years, RANGE 41–93 years, IQR: Q1-Q3 53–72 years). Based on gender distribution, 37.3 % of DME, 64.4 % of nAMD, 55.4 % of RVO and 71.4 % of myopic CNV patients were females. Patients with type 1 diabetes were identified from a pool of patients with DME using the ICD-10 code E10. It was observed that some patients had both E10 and E11 codes; however in those cases the patients were treated as type I patients. In our analyses, 39.1% of DME patients had type 1 diabetes, and 60.9% of patients had type 2 diabetes.
Newly Diagnosed Patients and New Patients Starting Intravitreal Treatment During 2015-2021
The number of incident patients per year, and the number of new patients starting anti-VEGF therapy per year are shown in Figure 1. The number of incident patients is shown for the years 2015–2021, whereas the number of new patients starting anti-VEGF treatment is shown only for the years 2019–2022. The years 2015–2018 were excluded from this analysis because of changes in recording practices and registries during the observational period, which affects the quality of anti-VEGF data for the said period. In addition, we used the first anti-VEGF date as the baseline value to identify the patients for our analyses. Patients who did not receive any anti-VEGF therapy during the observation period were excluded from the analyses.
In total, the annual number of new patients for all diagnoses of interest varied between 255 and 458 for the years 2015–2021 (Table 1), whereas the total number of new patients starting anti-VEGF treatment (DME, nAMD, RVO, and myopic CNV) varied from 489 to 572 in the years 2019–2021. The highest number of patients was in the nAMD group. Interestingly, the number of newly diagnosed DME patients remained approximately the same during the time period of 2015–2020, but an 73.8% increase was observed in the number of AMD patients (n=191, 2015; n=332, 2021), along with an 188.5% increase in RVO patients (2015 n=26, 2021, n=75). The number of patients with myopic CNV remained low throughout the observational period.
 |
Table 1 New Diagnosed Patients and Patients Starting Anti-VEGF Treatment |
Workload for a Clinic
To explore the workload for a clinic in terms of administration capacity caused by IVT (CKD05) visits for DME, nAMD, RVO, and myopic CNV, we analyzed the total number of IVT- and anti-VEGF- treated patients for the years 2015–2022 from the Oberon database, and the years 2019–2022 from the BCB Ophthalmology Quality Registry (Table 2). Additionally, we calculated the total number of IVT visits during the same period (Figure 2 and Table 3).
 |
Table 2 Number of IVT and Anti-VEGF-Treated Patients for the Years 2015–2022 |
 |
Table 3 Number of IVT Visits for the Years 2015–2021 in DME, nAMD, RVO and Myopic CNV. If a Patient Has Received Treatment for Both Eyes on the Same Visit, This Visit is Counted as One Visit in This Analysis |
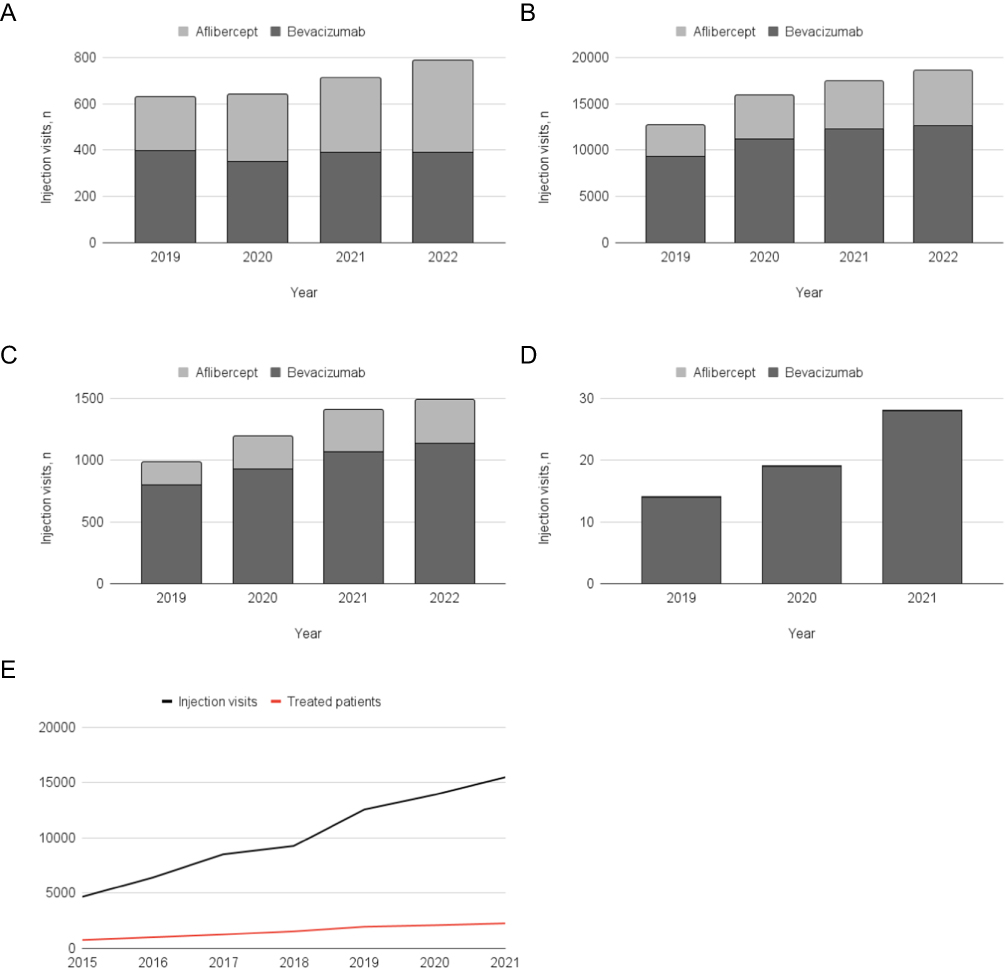 |
Figure 2 Number of IVT anti-VEGF injections or IVT injection visits per year (2015–2022) in DME, nAMD, RVO and myopic CNV. Ranibizumab injections are not shown in A-D due to low injection numbers. (A) Distribution of administered bevacizumab and aflibercept injections per year DME (B) Distribution of administered bevacizumab and aflibercept injections per year in nAMD (C) Distribution of administered bevacizumab and aflibercept injections per year in RVO (D) Distribution of administered bevacizumab and aflibercept injections per year in Myopic CNV. (E) Visual timeline for evolution of intravitreal treatments and patient numbers. Data for (B-D) obtained from the quality registry. Data for (A), (E) and (F) obtained from Oberon. Abbreviations: DME, diabetic macular edema; nAMD, neovascular age related macular degeneration; RVO, retinal vein occlusion; myopic CNV, myopic choroidal neovascularization; IVT, intravitreal treatment. |
For all diseases included in the analysis, both the total number of treated patients and the total number of treatment visits increased over the entire observational period. Based on the Oberon data, the total yearly number of IVT-treated patients for all diagnoses of interest increased 199.6% from 759 patients in 2015 to 2274 patients in 2021 (Table 2A). The number of IVT-treated patients increased by 198.5%, 176.8%, and 470.4% for DME, nAMD and RVO, respectively, from 2015 to 2021. Interestingly, the number of exact patients varied between the Oberon and quality registries, possibly as a consequence of the variance in recording practices (Table 2A and B).
Moreover, based on Oberon data, the total number of IVT visits per year (including DME, nAMD, RVO, and myopic CNV) increased by 232.5% from 2015 to 2021 (4661 vs 15499, Table 3). The number of IVT visits increased by 192.6%, 210.4%, and 654.3% for DME, nAMD, and RVO, respectively, from 2015 to 2021.
The total number of treatment visits reflects the total resources required for IVT treatment per year. If a patient received treatment for both eyes during the same visit, the visit was recorded as one visit in this analysis (based on the Oberon data). We were able to obtain laterality information from the quality registry. Thus, the years data for 2019–2022 shows the total number of administered injections (Figure 2A-D). In 2022, 31.1% of DME patients, 26.4% of nAMD patients, and 4.6% of RVO patients received treatment in both eyes. The total number of administered anti-VEGF injections increased during the observation period, but the rate of increase began to subside (2019–2020 increase: 23.7%, 2020–2021 increase: 10.3%, 2021–2022 increase: 6.7%). Myopic CNV was not recorded in the quality registry. Thus, quality registry analyses were lacking.
Figure 2 represents the share of bevacizumab and aflibercept among the total anti-VEGF treatments for the years 2019–2021. Ranibizumab is not shown in this figure as its use remained marginal during the entire observational period. Ranibizumab usage was only observed in nAMD, 16 injections being the highest number of injections in 2016, and zero injections being the lowest number of injections in 2021. In total, 56 ranibizumab injections were administered between 2015–2021, accounting for 0.3% of all registered injection visits (data from the Oberon search). For the years 2019–2022 bevacizumab was the most commonly used treatment for all diseases of interest, followed by aflibercept (Figure 2B-E). For example, in 2021, bevacizumab injections accounted for 55.2% of DME, 70.7% of nAMD, 76.3% of RVO, and 100% of myopic CNV from all anti-VEGF injections (DME, nAMD, and the RVO number from the quality registry and mCNV from the Oberon analysis, Figure 2), whereas aflibercept had a share of 44.8% in DME, 29.3% in nAMD, and 23.7% in RVO from all anti-VEGF injection visits during the same year.
Discussion
Since the emergence of intravitreal anti-VEGF treatment, the number of treatment options for retinal vascular diseases has dramatically improved. These new treatment options have led to an accumulation of new patients in ophthalmology departments (ie, an increased demand). New treatment options may delay disease progression, and provide patients more active days with improved vision. In contrast, receiving treatment may require frequent visits to the ophthalmology department which may cause inconvenience to patients and their caregiver(s) in the form of increased time commitment and travel costs. Thus, to better understand workload from the perspective of ophthalmology departments, we need data to demonstrate how patient numbers and administered IVTs have evolved in recent years. Therefore, our study aims to investigate the workload of ophthalmology departments caused by intravitreal treatments provided for DME, nAMD, RVO, and myopic CNV in The Wellbeing Services County of Southwest Finland. Approximately 486000 people (8.5% of the Finnish population) live in WSCSF. Described data represents the treatment practices of the WSCSF and generalization to the rest of Finland should, therefore, be made with caution. For example in the treatment of nAMD both treat and extend (T& E) and pro re nata (PRN) regimens are used in Finland. As WSCSF uses treat and extend (T& E) regiment, the results reflect more likely workload of the clinics, which use the same approach. However, it is considered that general trends in increased workload apply also outside of WSCSF.
In this study we analyzed data for diseases with aflibercept as the indicated therapy at the time of study initiation. Aflibercept is currently the most commonly used on-label product in Finland and therefore it was used as a reference. In our analyses it was observed that the number of patients, and the total number of administered intravitreal injections increased considerably during the observational period. For example, the total number of patients receiving intravitreal treatment for nAMD, DME, RVO, and myopic CNV increased 199.6% from 2015 to 2021, and the total number of IVT visits increased by 232.5% during the same period. An increase in the number of patients with nAMD and RVO may have occurred because of the aging population. However, in the beginning of the observational period an increase in treatment options may also have been driving the diagnosis. In addition it should be noted that the analyses included only patients who had received at least one anti-VEGF injection. Patients who received only corticosteroids are not included in the analyses. Based on first-hand comments by the head of the ophthalmology department at the Turku University Hospital, resources at the clinic have not followed this development. Regardless of the extensive efforts in patient journey optimization, increasing IVT treatment visits have resulted in longer wait times for patients with other ophthalmological conditions. As the patient numbers continue to increase, evidence-based discussions on resources become essential. It is crucial that both the facilities and the human resources are planned for the increasing demand, or alternatively there is a need to find more ways to optimize the patient journey, or otherwise decrease the workload associated with anti-VEGF injections. For example, more durable treatment options resulting with fewer IVT visits could play a role in finding solutions in terms of productivity improvements. Currently the decisions about treatment interval modifications are guided by optical coherence tomography (OCT) images analyzed by physicians. An example of future resource savings is the implementation of artificial intelligence based image analysis, and home OCT. Resource prioritization is another topic that may come under scrutiny in the coming years. An example of the prioritization would be identifying which treatment option would bring the longest possible treatment interval for each patient, and whether there is a time point when a treatment will no longer provide enough benefit for the patient and should be discontinued. To perform evidence based prioritization of resources, accurate data regarding workload, treatment results, and markers guiding personalized treatment approaches are essential.
To support evidence-based decision-making, patient records should be accurate. Nationally standardized recording practices would be beneficial. Our study reveals that retrospective registry data do have many possibilities but also limitations, as the recording of patient data has not been planned to serve studies. The WSCSF has tried to overcome this limitation by introducing an ophthalmology quality registry to its systems starting in mid-2018. Currently any data from a quality registry must be requested separately. Owing to these limitations in real-world data there may be some gaps, for example due to changes in information systems or recording practices. Ophthalmology provides an especially good example of how accurate recording is needed, as each patient has two eyes that may have different medication requirements. In our experience it is important to study and discuss these data gaps to better understand the output of national-level analyses. In addition, despite the observations being from a single country, the findings may also guide critical viewpoints for real-world data projects outside of Finland. For example, as bevacizumab is considered a low-cost treatment in ophthalmology, its use has not been recorded in the WSCSF in prescription information, but yet it is possible to collect bevacizumab data from the quality registry for 2018–2021. As bevacizumab is widely used in Finland, the lack of bevacizumab data would highly underestimate anti-VEGF usage in the previous years. Furthermore, the registry data is always only as good as the recorded input. The Oberon patient information system does not require recording the diagnosis at each treatment visit. This may create the possibility of an error as an old diagnosis may be carried over from previous visits if a new diagnosis is not recorded. Hints of this occurrence were observed as different results of new patients starting treatment were calculated based on diagnosis or anti-VEGF treatment. For nAMD in particular, treatment is usually initiated within a few days after diagnosis. Therefore in nAMD these numbers should closely resemble each other. In addition, the number of new RVO patients appeared to be slightly lower during the first few years. To better understand these site-specific limitations in recording practices, we would encourage involving the treating physician from the respective centers in the data analysis to effectively recognize the gaps and limitations. Our data search criteria also creates additional limitations for this study as only patients who had received anti-VEGF treatments are included. Thus our criteria will exclude patients who may have been treated only with corticosteroids. However, in the majority of cases anti-VEGF treatment is initiated before corticosteroids and the number of patients receiving only corticosteroids during their treatment journey is considered marginal.
In ophthalmology registry studies lies a specific challenge as patients may receive treatment in both eyes. To separate treatments per eye, attention should be paid to this issue during data recording, and data systems should be planned to respond to this need. Based on the quality registry during 2022, 31.1% of DME patients, 26.4% of nAMD patients, and 4.6% of RVO patients received treatment in both eyes. Based on literature, an average 12.2% of nAMD patients develop bilateral disease during the first year of follow-up, and 26.8% develop nAMD in their fellow eyes in a 4 year follow up.17 During our analysis, we found laterality information to be a limitation of the data received from Oberon, as lateral information was missing from many injection-related dates. For this reason, we decided to perform a second data request, where data collection was performed from a quality registry, and medication information was linked with laterality information. Due to this challenge, it is important to clearly report in registry studies how results were obtained to facilitate further interpretation of the results, for example when calculating costs related to healthcare resource utilization.
Intravitreal anti-VEGF treatments are also administered outside the studied indications (off-label). Therefore the true total patient numbers and provided intravitreal treatment numbers in ophthalmology departments are slightly higher. In addition, our data search criteria may have led to an underestimation of the number of patients in certain diagnostic groups. For example, mCNV may be easily misdiagnosed as nAMD initially. Therefore these patients may have been included in the nAMD patient pool instead of the mCNV group. However, from all indications, patients with nAMD clearly represent the largest patient group, and the changes in this patient group are especially relevant when discussing resources. Currently, nAMD is one of the most common causes of irreversible blindness among the elderly in developed countries.4 Unfortunately, the number of AMD patients is expected to increase in the future due to the aging population. It has been projected that by 2040 approximately 288 million individuals globally will suffer from AMD.1,18 Therefore, attention should be paid to this patient group in Finland as the population is aging.
Understanding the possibilities and limitations of registry data is becoming even more important now as data lakes in Finland are evolving, and registry research in Finland has been boosted by the implementation of the separate Act on the Secondary Use of Health and Social Data as well as the foundation of Findata. In Finland university hospitals have collaborated in creating an IT system (ACES-RWM) to automate and evaluate ophthalmic care.19 The future will show if this system responds to this need, and if recording practices and information systems can be aligned in Finland for the area of ophthalmology.
As registry data can be a powerful tool to support knowledge-based management, actions that generate information for registries should be well planned. Current registries are planned to serve patient care, but also data generation should be considered in each user level. Based on the challenges met in the study we consider the key takeaway being the observation that to support registry data analysis also the data input should be planned to support that goal. Systems should be planned to minimize variation created by recording practices of individual users. It would be also useful for the secondary data to be taken into consideration when planning patient information systems. It is also of importance to highlight that patient information system users should recognise the importance of accurate recording practices.
Conclusions
In the future the number of patients with retinal vascular diseases is expected to increase due to the aging population and changes in lifestyle-related issues. Therefore the use of registries in creating an evidence-based understanding of evolving patient numbers is critical. Further, it is critical to explore the possibilities and limitations of registries. Our study led to a heightened understanding of the Finnish registry landscape and demonstrated an increased workload by intravitreal injections in ophthalmology departments. Confidently these data will facilitate discussions about changing resource needs in ophthalmology departments and registry studies in the future.
Abbreviations
DME, diabetic macular edema; nAMD, neovascular age-related macular degeneration; RVO, retinal vein occlusion; myopic CNV, myopic choroidal neovascularization; IVT, intravitreal; VEGF, vascular endothelial growth factor; HDSF, Hospital District of Southwest Finland; ACI, Auria Clinical Informatics; WSCF, Wellbeing Services County of Southwest Finland.
Ethics Approval and Informed Consent
This study was conducted with permission from the Hospital District of Western Finland (permit no. T55_2022_SP-3 168743), and the Act on the Secondary Use of Health and Social Data (Finland’s Ministry of Justice 552/2019). Therefore, informed consent was not obtained from all the patients.
Acknowledgments
We thank Vesa Aaltonen and Minna Kumpula for their clarification of treatment and recording practices in the WSCSF. We also thank Susanna Moliski for the language review.
Funding
Study was funded by Roche Oy.
Disclosure
Authors are employees of Roche Oy. The authors report no other conflicts of interest in this work.
References
1. Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014;2(2):e106–16. doi:10.1016/S2214-109X(13)70145-1
2. Zhou B, Lu Y, Hajifathalian K, Collaboration NCDRF. Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4.4 million participants. Lancet. 2016;387(10027):1513–1530. doi:10.1016/S0140-6736(16)00618-8
3. Collaboration NCDRF. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet. 2017;390(10113):2627–2642.
4. Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990-2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221–e34. doi:10.1016/S2214-109X(17)30393-5
5. Schmidt-Erfurth U, Garcia-Arumi J, Bandello F, et al. Guidelines for the management of diabetic macular edema by the European Society of Retina Specialists (EURETINA). Ophthalmologica. 2017;237(4):185–222. doi:10.1159/000458539
6. Schmidt-Erfurth U, Garcia-Arumi J, Gerendas BS, et al. Guidelines for the management of retinal vein occlusion by the European Society of Retina Specialists (EURETINA). Ophthalmologica. 2019;242(3):123–162. doi:10.1159/000502041
7. Flaxel CJ, Adelman RA, Bailey ST, et al. Age-related macular degeneration preferred practice pattern(R). Ophthalmology. 2020;127(1):P1–P65. doi:10.1016/j.ophtha.2019.09.024
8. Ojamo M, Tolkkinen L, Kaarniranta K, Uusitalo H, Ojamo M, Tuuminen R. The Finnish register of visual impairment: annual statistics 2020. Acta ophthalmologica. 2020;98(5):472–476. doi:10.1111/aos.14376
9. Purola P, Kaarniranta K, Ojamo M, Gissler M, Uusitalo H. Visual impairment due to age-related macular degeneration during 40 years in Finland and the impact of novel therapies. Acta Ophthalmol. 2022;101(1):57–64.
10. Purola PKM, Ojamo MUI, Gissler M, Uusitalo HMT. Changes in visual impairment due to diabetic retinopathy during 1980-2019 based on nationwide register data. Diabetes Care. 2022;45(9):2020–2027. doi:10.2337/dc21-2369
11. Tuuminen R, Uusitalo-Jarvinen H, Aaltonen V, et al. The Finnish national guideline for diagnosis, treatment and follow-up of patients with wet age-related macular degeneration. Acta Ophthalmol. 2017;95(A105 Suppl):1–9. doi:10.1111/aos.13501
12. Karesvuo P, Hakkala L, Kaarniranta K, Uusitalo H, Ojamo M, Tuuminen R. Correlation between the rate of intravitreal injections, use of aflibercept as a second-line treatment and visual impairment for wet AMD in Finland. Acta Ophthalmol. 2020;98(5):472–476.
13. Dugel PU, Koh A, Ogura Y, et al. HAWK and HARRIER: Phase 3, multicenter, randomized, double-masked trials of brolucizumab for neovascular age-related macular degeneration. Ophthalmology. 2020;127(1):72–84. doi:10.1016/j.ophtha.2019.04.017
14. Brown DM, Emanuelli A, Bandello F, et al. KESTREL and KITE: 52-week results from two phase iii pivotal trials of brolucizumab for diabetic macular edema. Am J Ophthalmol. 2022;238:157–172. doi:10.1016/j.ajo.2022.01.004
15. Heier JS, Khanani AM, Quezada Ruiz C, et al. Efficacy, durability, and safety of intravitreal faricimab up to every 16 weeks for neovascular age-related macular degeneration (TENAYA and LUCERNE): two randomised, double-masked, phase 3, non-inferiority trials. Lancet. 2022;399(10326):729–740. doi:10.1016/S0140-6736(22)00010-1
16. Wykoff CC, Abreu F, Adamis AP, et al. Efficacy, durability, and safety of intravitreal faricimab with extended dosing up to every 16 weeks in patients with diabetic macular oedema (YOSEMITE and RHINE): two randomised, double-masked, phase 3 trials. Lancet. 2022;399(10326):741–755. doi:10.1016/S0140-6736(22)00018-6
17. Wong TY, Chakravarthy U, Klein R, et al. The natural history and prognosis of neovascular age-related macular degeneration: a systematic review of the literature and meta-analysis. Ophthalmology. 2008;115(1):116–126. doi:10.1016/j.ophtha.2007.03.008
18. Li JQ, Welchowski T, Schmid M, Mauschitz MM, Holz FG, Finger RP. Prevalence and incidence of age-related macular degeneration in Europe: a systematic review and meta-analysis. Br J Ophthalmol. 2020;104(8):1077–1084. doi:10.1136/bjophthalmol-2019-314422
19. Tuulonen A, Kataja M, Aaltonen V, et al. A comprehensive model for measuring real-life cost-effectiveness in eyecare: automation in care and evaluation of system (aces-rwm). Acta Ophthalmol. 2022;100(3):e833–e40. doi:10.1111/aos.14959
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.