")
Back to Journals » Journal of Inflammation Research » Volume 17
Examining the Long-Term Prognostic Significance of Serum sST2: Influence of Myocardial Infarction History and Subgroup Level Standardization
Authors Guan XQ, Guan L, Cheng G, Sun ZJ, Wang CH
Received 12 June 2024
Accepted for publication 15 October 2024
Published 25 October 2024 Volume 2024:17 Pages 7733—7744
DOI https://doi.org/10.2147/JIR.S482475
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Xue-Qing Guan, Lin Guan, Gong Cheng, Zhi-Jun Sun, Chuan-He Wang
Department of Cardiology, Shengjing Hospital of China Medical University, Shenyang, 110021, People’s Republic of China
Correspondence: Zhi-Jun Sun; Chuan-He Wang, Department of Cardiology, Shengjing Hospital of China Medical University, Shenyang, 110021, People’s Republic of China, Tel/Fax +86 18940251218 ; Tel/Fax +86 18940252598, Email [email protected]; [email protected]
Aim: In this study, the predictive value of soluble growth stimulation expressed gene 2 protein (sST2) for long-term clinical outcomes in patients with acute heart failure (AHF) is assessed. In addition, the influence of a history of myocardial infarction on the levels of sST2 in patients with HF, as well as its impact on outcome events, is explored. We also aim to establish a specific standard for sST2 levels in this subgroup.
Methods: We conducted an ambispective cohort study involving hospitalized patients with AHF, measuring their sST2 levels and following their progress over three years. The primary endpoint was major adverse cardiovascular events (MACEs), encompassing heart failure readmission and all-cause mortality over three years. Cox regression analysis was used to evaluate the prognostic significance of sST2 levels, along with a subgroup analysis using propensity score matching (PSM) to adjust for confounding variables. Receiver operating characteristic (ROC) curve analysis was utilized to determine the optimal sST2 threshold using Youden’s J statistics, and a sensitivity analysis included Kaplan–Meier survival curves.
Results: The study included 149 patients with a median age of 68 years, of whom 57% were male. Both univariate and multivariate Cox regression analyses confirmed sST2 as an independent predictor of MACEs. Post-PSM analysis, 124 samples were grouped by MI history ROC curve analysis revealed an area under the curve of 0.726 for predicting MACEs in patients with MI, demonstrating a significant predictive value for sST2 levels above 34 ng/mL, which correlated with increased readmission and mortality rates. In contrast, sST2 levels in patients without MI history showed no significant predictive relevance.
Conclusion: sST2 has significant long-term predictive value for clinical outcomes in patients with AHF, particularly for those with a prior MI history, indicating a need for heightened clinical attention and thorough follow-up to mitigate long-term adverse cardiovascular outcomes.
Keywords: Acute heart failure, myocardial infarction, soluble growth-stimulated expression gene 2, ventricular remodeling
Introduction
Heart failure (HF) represents a complex clinical syndrome arising from diverse etiologies, including myocardial infarction (MI), characterized by pathological alterations in cardiac structure and/or function. These alterations disrupt ventricular function, leading to symptoms such as dyspnea, fatigue, and fluid retention, which may manifest as pulmonary and systemic congestion, along with peripheral edema.1
HF remains a leading cause of cardiovascular morbidity and mortality worldwide.2–4 Notably, in China, the prevalence of HF is approximately 1.1%, with an incidence rate of 275 per 100,000 person-years, contributing to three million new cases annually.5 The number of HF cases diagnosed has risen with advances in diagnostic techniques, underscoring the importance of enhancing clinical treatment strategies.
Ventricular remodeling (VR) involves cardiac adjustments in response to mechanical stress, neurohormonal factors, and genetic influences following cardiac injury, playing a pivotal role in HF progression.6,7 Various clinical tools, including echocardiography, cardiac magnetic resonance imaging, and serum biomarkers of fibrosis, facilitate the assessment of VR, thereby informing therapeutic decisions.8
Soluble growth stimulation expressed gene 2 protein (sST2), a subtype of the ST2 protein linked to inflammation, myocardial hypertrophy, and interstitial fibrosis,9,10 serves as a significant prognostic marker in stable HF patients. Although sST2 cannot be used as an independent biomarker for HF diagnosis, its combined use with N-terminal pro-B-type Natriuretic Peptide (NT-proBNP) enhances diagnostic precision.11,12 The diagnostic utility of sST2 is further highlighted by its stability across different ages and renal function levels, proving beneficial in specific patient cohorts.13,14 Notably, sST2 levels escalate post-MI, surpassing NT-proBNP in detecting early maladaptive cardiac remodeling15 and demonstrating prolonged predictive value for ventricular remodeling up to one year post-MI.16
Given the robust link between sST2 levels and ventricular remodeling, understanding the influence of post-MI fibrosis on sST2 levels in patients with HF is essential. This understanding prompts consideration of whether distinct sST2 level benchmarks are required for patients with HF and a MI history. Our study focuses on patients experiencing their initial HF readmission post-MI compared to those with HF but no MI history, aiming to elucidate the impact of MI on sST2 levels through comprehensive data analysis and comparison.
Methods
Study Population
Patients admitted to Shengjing Hospital, affiliated with China Medical University, from May 2017 to December 2018 for acute heart failure (AHF) were enrolled in this study. The study adhered to the ethical standards of the 2013 amendment of the 1975 Declaration of Helsinki and received approval from the hospital’s ethics committee (Ethics Approval Number: 2023PS1307K). The criteria for inclusion and exclusion were aligned with the European Guidelines for Heart Failure,17 detailed below:
Inclusion Criteria
1) Patients classified within New York Heart Association (NYHA) functional classes II to IV, displaying typical symptoms of HF, including dyspnea, orthopnea, paroxysmal nocturnal dyspnea, reduced exercise tolerance, fatigue, prolonged recovery after physical activity, and ankle edema.
2) Elevated levels of NT-proBNP (≥ 300 pg/mL).
3) Echocardiographic confirmation of any of the following:
- Impaired systolic function.
- Impaired diastolic function.
- Left ventricular hypertrophy.
- Left atrial enlargement.
4) Requirement for intravenous diuretics or vasodilators.
Exclusion Criteria
1) Patients presenting with symptomatic hypotension, defined by a systolic blood pressure ≤ 90 mmHg, or those with unmanageable hypertension with readings ≥ 180/100 mmHg.
2) Patients suffering from severe co-morbid conditions, including liver failure, malignant tumors, hematological disorders, or uremia.
3) Patients with incomplete clinical records.
4) Patients actively participating in other clinical trials.
Study Protocol and Data Collection
During the patient selection phase, the following data was collected:
1) Basic demographic information, including age, gender, and body mass index (BMI).
2) History of comorbidities, such as hypertension, diabetes, coronary heart disease, atrial fibrillation, cerebral infarction, and myocardial infarction.
3) Laboratory parameters at admission, specifically NT-proBNP and sST2.
4) Echocardiographic evaluations, including measurements of left atrial diameter (LAD) and left ventricular ejection fraction (LVEF).
5) Medication regimen at discharge, encompassing angiotensin-converting enzyme inhibitors (ACEIs), angiotensin II receptor blockers (ARBs), angiotensin receptor-neprilysin inhibitors (ARNIs), beta-blockers, and mineralocorticoid receptor antagonists (MRAs).
The initial data were collected from a review of medical records and patient interviews, with eligible patients monitored subsequently at intervals of 3 months, 6 months, 1 year, and 3 years post-discharge. All-cause readmissions and survival rates were recorded at each follow-up.
Laboratory and Ultrasound Investigations
1) Serum sST2 measurement: Serum samples from patients were analyzed for sST2 using an enzyme-linked immunosorbent assay (ELISA) with the Presage ST2 assay kit (Critical Diagnostics, San Diego, CA, USA).
2) Other laboratory results: The results of the routine hospitalization examinations conducted during the study subjects’ admission period were utilized. The procedure was as follows: Firstly, the medical staff, adhering to aseptic techniques, collected peripheral venous blood from patients (who had fasted for more than 8 hours prior to blood collection). Then, the blood samples were immediately stored in a low-temperature environment and centrifuged and aliquoted according to standard protocols. After that, the blood samples were transported at low temperatures to the relevant laboratories in the hospital’s clinical testing department within the stipulated time frame. Finally, the tests were completed in standard laboratories, including measurements of NT-proBNP, complete blood count, total cholesterol, triglycerides, blood ions, fasting blood glucose, glycated hemoglobin, and serum uric acid levels.
3) Echocardiographic assessment: Evaluations of LAD and LVEF were performed at admission using a Philips IE33/EPIQ7C ultrasound system. Ejection fraction was calculated using Simpson’s biplane method, defined as the ratio of the difference between end-diastolic volume (EDV) and end-systolic volume (ESV) to EDV.
Primary Endpoints
The primary outcome assessed was the occurrence of major adverse cardiovascular events (MACEs) over a three-year period following discharge. MACEs were defined according to the ACC/AHA/HFSA Heart Failure Management Guidelines as HF rehospitalization and/or all-cause mortality within three years post-discharge.18
Statistical Analysis
Continuous variables adhering to a normal distribution were presented as means and standard deviations, while those not normally distributed were summarized using medians and interquartile ranges. Categorical variables were expressed in both counts and percentages. To evaluate differences in baseline characteristics across varying patient outcomes, independent sample t-tests were utilized for normally distributed continuous variables, Mann–Whitney U-tests for non-normally distributed variables, and chi-squared or Fisher’s exact tests for categorical variables.
sST2 levels were incorporated as a continuous variable in both univariate and multivariate Cox regression analyses to determine their prognostic significance on clinical outcomes. A 1:1 propensity score matching (PSM) was implemented to compare patients with and without a history of MI, using a caliper width of 0.02 to ensure precise matching.
After matching, reassessment of baseline characteristics and outcomes between subgroups was performed. The optimal cut-off values for sST2, specific to each endpoint in both subgroups, were established using Youden’s J statistic method and receiver operating characteristic (ROC) curves. Based on these thresholds, patients were categorized into subgroups for a sensitivity analysis involving Kaplan–Meier (KM) survival curves to validate the association between elevated sST2 levels and clinical outcomes.
All statistical analyses were conducted using IBM SPSS Statistics (version 27.0.1.0, 2021) and R software (version 4.3.0). A p-value less than 0.05 was deemed to indicate statistical significance.
Results
Study Population and Outcomes
The initial cohort included 255 patients, of which 79 were lost to follow-up over a three-year period. After excluding cases with incomplete data and removing outliers, the final dataset for statistical analysis comprised 149 patients. The median age of this group was 68 years, with women representing 43% of the population. Seventy patients had a history of MI, while 79 had no prior MI. Within the first year, 62 patients (41.6%) were readmitted due to HF, 27 patients (18.1%) died, and a total of 70 patients (47%) met the criteria for MACEs. By the end of the three-year follow-up, 85 patients (57%) had been readmitted, 50 patients (33.6%) had died, and 92 cases (61.7%) were classified as having experienced MACEs (Figure 1).
 |
Figure 1 Clinical status at follow-up. Abbreviations: MACE, major adverse cardiovascular events. |
Analysis of patient profiles based on three-year outcomes revealed that those who underwent HF readmission or died were typically older (median age 70 years vs 64 years), had a lower BMI (24 vs 25), and presented with higher initial levels of NT-proBNP (4310 pg/mL vs 1916 pg/mL) and sST2 (36 ng/mL vs 28 ng/mL). These patients generally showed lower LVEF values, indicating compromised cardiac function. In contrast, no significant differences were noted in other demographic or clinical variables such as gender, smoking history, presence of hypertension, diabetes, coronary heart disease, atrial fibrillation, cerebral infarction history, left atrial size measured by echocardiography, or discharge medication regimen (Table 1).
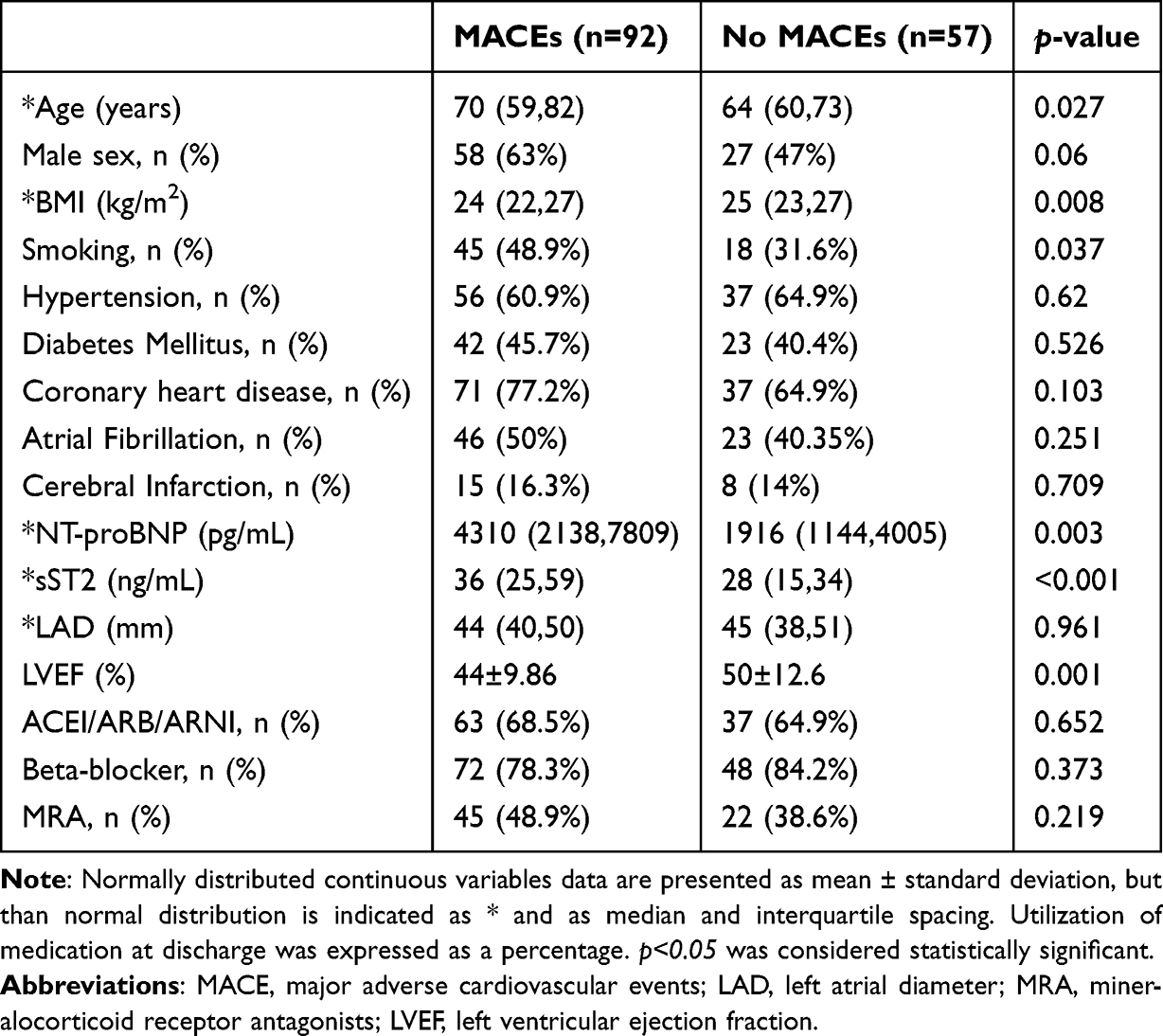 |
Table 1 Comparison of Characters Between Different 3-Year Primary Outcomes |
Survival Analysis
The sST2 was included in the COX proportional regression model as a continuous variable, with 3-year MACE events, 3-year heart failure readmission and 3-year death as outcome analysis, and the results are shown in Table 2. In the univariate analysis, sST2 for 3-year MACE events, 3-year HF readmission and 3-year deaths were statistically significant at p <0.001 level with HR of 1.015,1.016 and 1.017, respectively. In addition, NT-proBNP> 3165 pg/mL, age> 68 years, BMI, were statistically significant in the 3-year MACE analysis (p <0.05), EF value in the univariate analysis of 3-year MACE event and 3-year heart failure readmission as outcome, but not in the outcome of 3-year death events. According to the results of univariate analysis and population characteristics, age, BMI, EF value, and NT-proBNP were selected for multivariate Cox proportional risk model analysis. The results showed that both sST 2 and NT-proBNP> 3165 pg/mL were independent risk factors for 3-year MACE events and 3-year heart failure readmission, and for sST 2 and NT-proBNP> 3165 pg / mL and age> 68 years for 3 years mortality (Table 2).
 |
Table 2 Univariate and Multivariate Cox Regression Analyses for Primary Outcomes |
Baseline Characteristics in Matched Cohort
To mitigate baseline variability between subgroups, PSM was utilized, creating a matched cohort based on MI history. This resulted in a balanced selection of 124 patients. Post-matching analysis highlighted significant differences in the prevalence of coronary heart disease (p < 0.001) and atrial fibrillation (p = 0.007). However, sST2 levels did not show significant differences between the groups (Table 3).
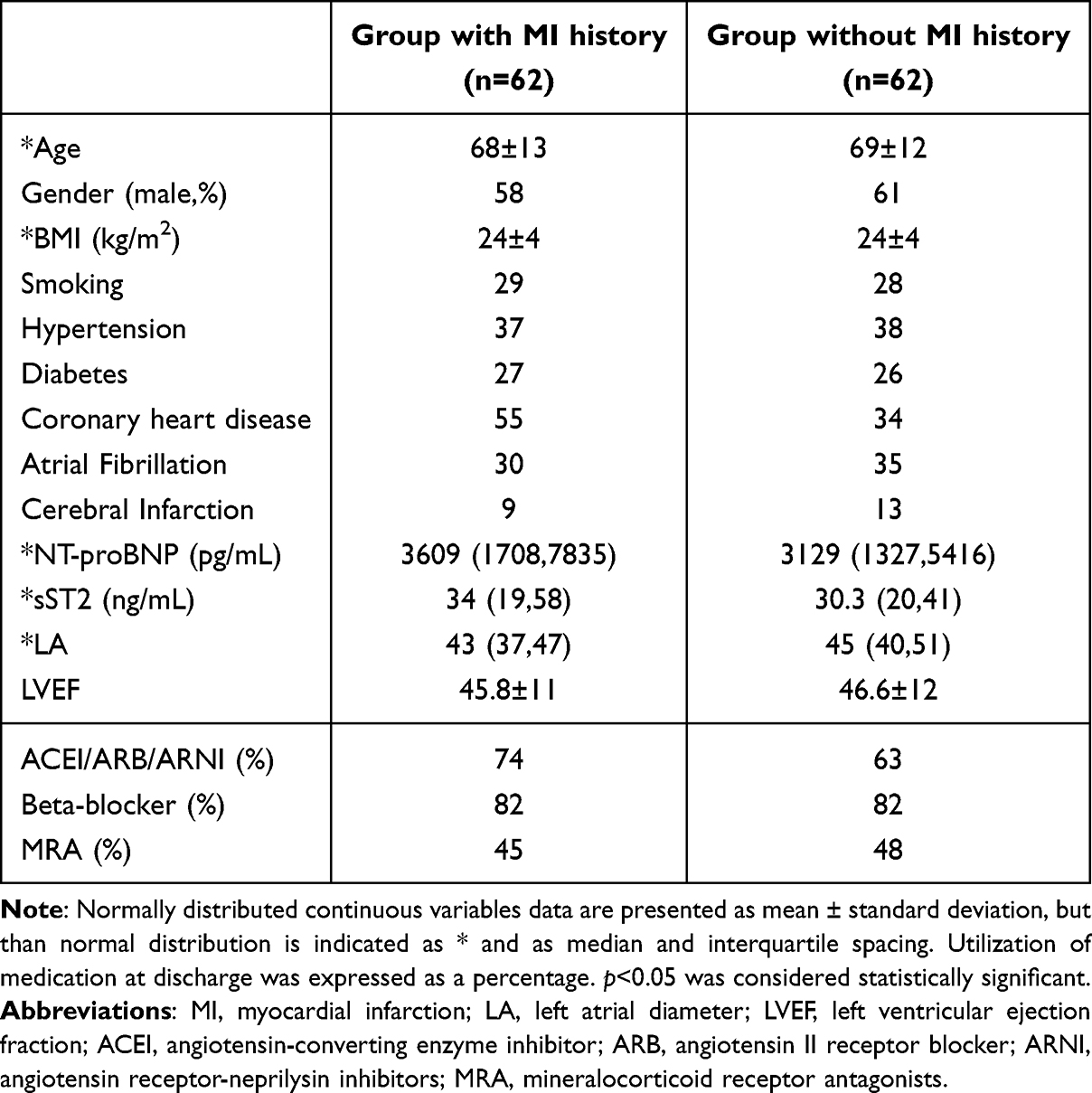 |
Table 3 Basic Characters Between Matched Groups |
ROC Analysis and Cut-Offs
The diagnostic potential of sST2 for predicting 3-year MACEs was further evaluated through ROC curve analysis. In the subgroup with a history of MI, the AUC for sST2 was 0.746, indicating good predictive value, while in the subgroup without MI history, the AUC was 0.643. Similar trends were observed for 3-year HF readmission, with AUCs of 0.748 for the MI history subgroup and 0.684 for the no MI history subgroup. For 3-year mortality, AUCs in both groups were below 0.7. Using Youden’s J statistic, the optimal cutoff value of sST2 for predicting 3-year HF readmission and 3-year MACEs was established at 34 ng/mL (Figures 2A-2C).
 |
Figure 2 Receiver operating curves for 3-year MACEs, 3-year HF readmission, 3-year death (A) ROC curve for 3-year MACEs. (B) ROC curve for 3-year HF readmission. (C) ROC curve for 3-year death. The red line is the group with a history of MI (MI=1), and the blue line is the group without a history of MI (MI=0). Abbreviations: MACE, major adverse cardiovascular events; HF, heart failure; MI, myocardial infarction. |
Sensitivity Analysis
To verify the robustness of our findings, a sensitivity analysis was performed within the established subgroups to examine if the differences in outcomes related to sST2 levels were consistent. This analysis revealed that within the subgroup of individuals with a history of MI, those with sST2 levels greater than 34 ng/mL faced a significantly higher risk of experiencing 3-year MACEs (p < 0.001), 3-year HF readmission (p = 0.011), and 3-year mortality (p < 0.001). In contrast, in the subgroup without a history of MI, although a higher sST2 level was associated with an increased tendency for 3-year HF readmission (p = 0.018), there were no statistically significant differences concerning 3-year MACEs and 3-year mortality. (Figures 3A and 3B).
 |
Figure 3 Outcomes of MI and NMI groups at 3 years (A) Outcomes of MI. (B) Outcomes of NMI. Abbreviations: MI, myocardial infarction; NMI, no myocardial infarction; HF, heart failure. |
Further analysis using KM survival curves for these subgroups highlighted that, for patients with a history of MI, elevated sST2 levels (> 34 ng/mL) correlated with a poorer long-term prognosis post-MI (p = 0.00048). However, for patients without a history of MI, the differences in long-term outcomes were not as marked (p = 0.15), suggesting a variable impact of sST2 based on prior MI history (Figures 4A and 4B).
 |
Figure 4 KM curve for surviving analyses in subgroups(A) KM curve for 3-year events in patients with a history of MI. The difference in the risk of MACEs between the two groups with a history of MI is shown. (B) KM curve for 3-year events in patients without a history of MI. The difference in the risk of MACEs between the two groups with no history of MI is shown. Abbreviations: MI, myocardial infarction; KM, Kaplan–Meier; MACE, major adverse cardiovascular events. |
Discussion
Initially recognized for its role in suppressing tumor growth in 1989,19 the relevance of sST2 has significantly expanded, particularly due to its cardioprotective properties mediated by the ligand interleukin-33 (IL-33). IL-33 is known to inhibit myocyte hypertrophy and fibrosis.20,21 While the combined use of sST2 and NT-proBNP has been shown to improve diagnostic accuracy for HF, sST2 alone does not serve as an independent diagnostic marker.12,22 This limitation is partly due to the overlapping and confounding presence of circulating sST2 levels in patients with HF or inflammatory conditions.23
The clinical utility of sST2 in HF has been significantly advanced by numerous clinical studies over the years.24 sST2 has been established as a potent predictor of adverse clinical events in AHF.10,13,25 A 2016 meta-analysis encompassing 7 clinical trials with over 6,372 participants confirmed the prognostic value of sST2 in predicting poor outcomes in patients with chronic HF.26 In summary, the role of sST2 in the prognosis of chronic heart failure is widely supported, but there is not similarly strong evidence for its prognostic role in acute heart failure. Our study was designed to explore the long-term prognostic significance of sST2 in patients with AHF, addressing a gap in previous research, which primarily focused on shorter observation periods of one year or less. Our study extended the follow-up duration to three years, tracking HF readmissions and all-cause mortality. The Cox survival analysis, which included 149 patients, identified sST2 as an independent risk factor for prognostic events in both univariate and multivariate contexts, underscoring its potential for long-term predictive value in AHF. The findings notably confirmed the statistical significance of sST2 in predicting HF readmissions within a three-year period, with a p-value of less than 0.001.
In addition, it is well-documented that sST2 levels increase following MI and exhibit long-term prognostic significance in these individuals. Consistent with clinical observations, patients displaying elevated sST2 levels post-MI appeared more susceptible to subsequent HF events.15,16,27
However, there is insufficient clinical evidence to indicate whether patients with heart failure will exhibit higher ST2 levels due to a history of myocardial infarction, and whether ST2 plays a more unique role in this specific patient population. Given the absence of prior studies directly addressing this issue, we engaged in detailed subgroup analyses. We categorized patients with HF according to their history of MI to explore the predictive capabilities of sST2 across different HF scenarios. Patients were categorized based on MI history, employing 1:1 PSM to ensure comparable baseline characteristics across groups. Ultimately, 124 samples were analyzed.
Although median sST2 levels were 34 ng/mL and 30 ng/mL in the respective groups, no statistically significant difference in levels between these groups was detected. However, subsequent ROC curve analysis indicated that sST2 provided superior predictive value for 3-year MACEs in the group with a history of MI (AUC = 0.746), reinforcing our hypothesis and affirming the prognostic utility of sST2 in this demographic. The ROC analysis for 3-year HF readmission mirrored this trend (AUC = 0.748). While analyzing 3-year mortality, ROC curves also showed higher AUC values in the MI history group compared to those without, although both were below 0.7. The limited sample size may influence these findings, particularly concerning statistical significance related to all-cause mortality.
These findings corroborate the hypothesized predictive role of sST2 in HF outcomes following MI. To ensure the reliability of our conclusions, further subgroup analyses were conducted. Employing the Youden’s index, the optimal cutoff value for sST2 was established at 34 ng/mL. Patients exceeding this threshold exhibited higher rates of readmission and mortality, substantiating the initial results and emphasizing the predictive importance of elevated sST2 levels in this patient cohort.
However, several limitations warrant acknowledgment in the context of this study. Firstly, the sample size was relatively small compared to previous studies. To address this, we utilized 1:1 PSM to ensure balanced data groups and conducted additional subgroup analyses to enhance the stability and credibility of our results.
Another limitation is the sole measurement of sST2 levels at baseline, without subsequent assessments during the follow-up period. Despite this, previous studies have demonstrated that baseline sST2 levels retain their prognostic value.13,28
Due to the limited sample size, it was challenging to further classify patients with HF based on different etiologies. As HF can result from various causes, each potentially promoting myocardial fibrosis through distinct pathways,29–31 future research should consider examining subgroups such as patients with atrial fibrillation complicated by HF.
Additionally, the impact of emerging HF therapies, particularly orally administered medications that may influence sST2 levels by preventing ventricular fibrosis or enhancing ventricular remodeling, presents another concern for future studies.32,33 For example, SGLT2 inhibitors are now recognized as a critical component in managing HF and could affect future research outcomes in this area.34,35
Conclusion
We prolonged the predictive value for the prognosis of patients with AHF over a three-year period. The findings also highlight that the diagnostic utility of sST2 varies significantly among different HF patient groups, particularly demonstrating greater value in patients with a history of MI. This underscores the importance of considering prognostic differences among patient groups when monitoring sST2 levels in clinical practice. Specifically, for patients with a history of MI and elevated sST2 levels above 34 ng/mL, heightened attention to medication management and follow-up is advised to mitigate the risk of long-term adverse cardiovascular events.
Abbreviations
sST2, Soluble growth stimulation expressed gene 2 protein; PSM, propensity score matching; ROC, receiver-operating characteristics curve; KM curve: Kaplan-Meier curve; MI, myocardial infarction; AHF, acute heart failure; HF, heart failure; NT-proBNP, N-terminal pro-B-type natriuretic peptide; BMI, body mass index; LAD, left atrial diameter; LVEF, left ventricular ejection fraction; MRA, mineralocorticoid receptor antagonist; SD, standard deviation; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin (II) receptor blocker; ARNI, angiotensin receptor-neprilysin inhibitor; AUC, area under the receiver operating characteristics curves; ESC, European Society of Cardiology; SGLT2i, sodium-glucose transport protein 2 inhibitor.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of the Shengjing Hospital of China Medical University(Approval number:2019PS598K). The study was conducted in accordance with the requirement stipulated in the 2013 revision of the 1975 Declaration of Helsinki. The Ethics Committee exempted the requirement of written informed consent: This study is a observational retrospective study. It only collects the patient’s clinical data, does not interfere with the patient’s treatment plan, and will not bring risks to the patient’s physiology. The researchers confirm that patients’ information will not be disclosed unless it is de-identified, in order to maintain confidentiality and personal privacy.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflict of interest, which should be reported in the paper.
References
1. McDonagh TA, Metra M, Adamo M, et al. Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2024;26:5–17. doi:10.1002/ejhf.3024
2. Wang H, Chai K, Du M, et al. Prevalence and Incidence of Heart Failure Among Urban Patients in China: a National Population-Based Analysis. Circ Heart Fail. 2021;14:e008406. doi:10.1161/circheartfailure.121.008406
3. Yu Y, Liu J, Zhang L, et al. Perceived Economic Burden, Mortality, and Health Status in Patients With Heart Failure. JAMA Network Open. 2024;7:e241420. doi:10.1001/jamanetworkopen.2024.1420
4. Peng L, Ma L, Jiang QQ, et al. The mechanism of Panax notoginseng in the treatment of heart failure based on biological analysis. World J Tradit Chin Med. 2022;8:530–538.
5. Cai A, Zheng C, Qiu J, et al. Prevalence of heart failure stages in the general population and implications for heart failure prevention: reports from the China Hypertension Survey 2012-15. Eur J Prev Cardiol. 2023;30:1391–1400. doi:10.1093/eurjpc/zwad223
6. Frantz S, Hundertmark MJ, Schulz-Menger J, Bengel FM, Bauersachs J. Left ventricular remodelling post-myocardial infarction: pathophysiology, imaging, and novel therapies. Eur Heart J. 2022;43:2549–2561. doi:10.1093/eurheartj/ehac223
7. Karam S, Margaria JP, Bourcier A, et al. Cardiac Overexpression of PDE4B Blunts β-Adrenergic Response and Maladaptive Remodeling in Heart Failure. Circulation. 2020;142:161–174. doi:10.1161/circulationaha.119.042573
8. López B, Ravassa S, Moreno MU, et al. Diffuse myocardial fibrosis: mechanisms, diagnosis and therapeutic approaches. Nat Rev Cardiol. 2021;18:479–498. doi:10.1038/s41569-020-00504-1
9. Kuehn BM. Biomarkers May Help Stratify Patient Heart Failure Risk, Guide Treatment. Circulation. 2020;141:399–400. doi:10.1161/CIRCULATIONAHA.119.045477
10. Aimo A, Januzzi JL, Bayes-Genis A, et al. Clinical and Prognostic Significance of sST2 in Heart Failure: JACC Review Topic of the Week. J American Coll Cardiol. 2019;74:2193–2203. doi:10.1016/j.jacc.2019.08.1039
11. Ky B, French B, McCloskey K, et al. High-sensitivity ST2 for prediction of adverse outcomes in chronic heart failure. Circ Heart Fail. 2011;4:180–187. doi:10.1161/circheartfailure.110.958223
12. Vergaro G, Gentile F, Aimo A, et al. Circulating levels and prognostic cut-offs of sST2, hs-cTnT, and NT-proBNP in women vs. men with chronic heart failure. ESC Heart Failure. 2022;9:2084–2095. doi:10.1002/ehf2.13883
13. Emdin M, Aimo A, Vergaro G, et al. sST2 Predicts Outcome in Chronic Heart Failure Beyond NT-proBNP and High-Sensitivity Troponin T. J American Coll Cardiol. 2018;72:2309–2320. doi:10.1016/j.jacc.2018.08.2165
14. Aimo A, Januzzi JL, Vergaro G, et al. Circulating levels and prognostic value of soluble ST2 in heart failure are less influenced by age than N-terminal pro-B-type natriuretic peptide and high-sensitivity troponin T. European J Heart Fail. 2020;22:2078–2088. doi:10.1002/ejhf.1701
15. Gruzdeva O, Dyleva Y, Uchasova E, et al. Biological markers and cardiac remodelling following the myocardial infarction. Aging. 2019;11:3523–3535. doi:10.18632/aging.101994
16. Bière L, Garcia G, Guillou S, et al. ST2 as a predictor of late ventricular remodeling after myocardial infarction. Int J Cardiol. 2018;259:40–42. doi:10.1016/j.ijcard.2018.02.058
17. McDonagh TA, Metra M, Adamo M, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42:3599–3726. doi:10.1093/eurheartj/ehab368
18. Yancy CW, Jessup M, Bozkurt B, et al. ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J American Coll Cardiol. 2017;70:776–803. doi:10.1016/j.jacc.2017.04.025
19. Tominaga S. A putative protein of a growth specific cDNA from BALB/c-3T3 cells is highly similar to the extracellular portion of mouse interleukin 1 receptor. FEBS Lett. 1989;258(301–304). doi:10.1016/0014-5793
20. Schmitz J, Owyang A, Oldham E, et al. IL-33, an interleukin-1-like cytokine that signals via the IL-1 receptor-related protein ST2 and induces T helper type 2-associated cytokines. Immunity. 2005;23:479–490. doi:10.1016/j.immuni.2005.09.015
21. Garbern JC, Williams J, Kristl AC, et al. Dysregulation of IL-33/ST2 signaling and myocardial periarteriolar fibrosis. J Mol Cell Cardiol. 2019;128:179–186. doi:10.1016/j.yjmcc.2019.01.018
22. Heidenreich PA, Bozkurt B, Aguilar D, et al. AHA/ACC/HFSA Guideline for the Management of Heart Failure: executive Summary: a Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145:e876–e894. doi:10.1161/CIR.0000000000001062
23. Januzzi JL Jr, Peacock WF, Maisel AS, et al. Measurement of the interleukin family member ST2 in patients with acute dyspnea: results from the PRIDE (Pro-Brain Natriuretic Peptide Investigation of Dyspnea in the Emergency Department) study. J Am Coll Cardiol. 2007;50:607–613. doi:10.1016/j.jacc.2007.05.014
24. Zeng Z, Hong XY, Li Y, et al. Serum-soluble ST2 as a novel biomarker reflecting inflammatory status and illness severity in patients with COVID-19. Biomarker Med. 2020;14:1619–1629. doi:10.2217/bmm-2020-0410
25. Rørth R, Jhund PS, Kristensen SL, et al. The prognostic value of troponin T and N-terminal pro B-type natriuretic peptide, alone and in combination, in heart failure patients with and without diabetes. Eur J Heart Fail. 2019;21:40–49. doi:10.1002/ejhf.1359
26. Aimo A, Vergaro G, Passino C, et al. Prognostic Value of Soluble Suppression of Tumorigenicity-2 in Chronic Heart Failure: a Meta-Analysis. JACC Heart Fail. 2017;5:280–286. doi:10.1016/j.jchf.2016.09.010
27. Wang YP, Wang JH, Wang XL, et al. Roles of ST2, IL-33 and BNP in predicting major adverse cardiovascular events in acute myocardial infarction after percutaneous coronary intervention. J Cell Mol Med. 2017;21:2677–2684. doi:10.1111/jcmm.13183
28. Morrow DA, Velazquez EJ, DeVore AD, et al. Cardiovascular biomarkers in patients with acute decompensated heart failure randomized to sacubitril-valsartan or enalapril in the PIONEER-HF trial. Eur Heart J. 2019;40:3345–3352. doi:10.1093/eurheartj/ehz240
29. Künzel SR, Hoffmann M, Weber S, et al. Diminished PLK2 Induces Cardiac Fibrosis and Promotes Atrial Fibrillation. Circ Res. 2021;129:804–820. doi:10.1161/circresaha.121.319425
30. Pucci A, Aimo A, Musetti V, et al. Amyloid Deposits and Fibrosis on Left Ventricular Endomyocardial Biopsy Correlate With Extracellular Volume in Cardiac Amyloidosis. J Am Heart Assoc. 2021;10:e020358. doi:10.1161/jaha.120.020358
31. Moreira LM, Takawale A, Hulsurkar M, et al. Paracrine signalling by cardiac calcitonin controls atrial fibrogenesis and arrhythmia. Nature. 2020;587:460–465. doi:10.1038/s41586-020-2890-8
32. Jiao T, Wang Y, Lin X, et al. Axitinib targets cardiac fibrosis in pressure overload-induced heart failure through VEGFA-KDR pathway. Front Med Lausanne. 2023;10(1256156). doi:10.3389/fmed.2023.1256156
33. Cunningham JW, Claggett BL, O’Meara E, et al. Effect of Sacubitril/Valsartan on Biomarkers of Extracellular Matrix Regulation in Patients With HFpEF. J Am Coll Cardiol. 2020;76:503–514. doi:10.1016/j.jacc.2020.05.072
34. Lee H-C, Shiou Y-L, Jhuo S-J, et al. The sodium-glucose co-transporter 2 inhibitor empagliflozin attenuates cardiac fibrosis and improves ventricular hemodynamics in hypertensive heart failure rats. Cardiovas Diabet. 2019;18(45). doi:10.1186/s12933-019-0849-6
35. Vijay A, Astbury S, Panayiotis L, et al. Dietary Interventions Reduce Traditional and Novel Cardiovascular Risk Markers by Altering the Gut Microbiome and Their Metabolites. Front Cardiovasc Med. 2021;8(691564). doi:10.3389/fcvm.2021.691564
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.