")
Back to Journals » Patient Preference and Adherence » Volume 19
Exploring the Real Mental Experience of Patients with Moyamoya Disease: A Qualitative Analysis
Authors Li M , Zhang W, Zhang N, Li S, Pan Z, Xiong X, Li Q, Wei J , Li H
Received 5 April 2025
Accepted for publication 3 July 2025
Published 7 July 2025 Volume 2025:19 Pages 1937—1950
DOI https://doi.org/10.2147/PPA.S527947
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Meng Li,1,* Wenling Zhang,2,* Ning Zhang,3 Shen Li,4 Zhongjie Pan,5 Xiaoyun Xiong,6 Qiong Li,3 Junfan Wei,7 Huawei Li1
1Nursing Department, The Third People’s Hospital of Henan Province, Zhengzhou, People’s Republic of China; 2Operation Department, Henan Provincial People’s Hospital, Zhengzhou, People’s Republic of China; 3School of Nursing Department, Xinxiang Medical University, Xinxiang, People’s Republic of China; 4School of Rehabilitation Department, Henan Vocational College of Tuina, Zhengzhou, People’s Republic of China; 5School of Medicine Department, Zhengzhou University of Industrial Technology, Zhengzhou, People’s Republic of China; 6Rehabilitation Medicine Department, The Third People’s Hospital of Henan Province, Zhengzhou, People’s Republic of China; 7Nursing Department, The Seventh Clinical College of Guangzhou University of Chinese Medicine, Shenzhen, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huawei Li, The Third People’s Hospital of Henan Province, 198 Funiu Road, Zhengzhou, Henan, People’s Republic of China, Tel +86 13937182631, Email [email protected] Junfan Wei, Guangzhou University of Chinese Medicine, No. 22,25 Yu’an 2nd Road, 30 District, Bao’an District, Shenzhen, People’s Republic of China, Tel +86 13253369959, Email [email protected]
Purpose: The objective of this study was to explore the real mental experiences of moyamoya disease patients.
Patients and Methods: A phenomenological research method was used, and participants were selected by purposive sampling from two tertiary care hospitals in Henan Province, China. Semi-structured in-depth interviews were conducted with 17 patients diagnosed as moyamoya disease face-to-face. Colaizzi’s method was used to analyze the collected data.
Results: Five major themes were identified through phenomenological analysis: (1) cognitive and emotional experiences, including fear, denial, and evolving self-perception; (2) psychological adjustment, featuring active coping strategies and reliance on social support; (3) impact on quality of life, including challenges in daily functioning and interpersonal relationships; (4) information needs and seeking, highlighting patients’ difficulties accessing and understanding health information; and (5) long-term care and support, encompassing extended rehabilitation needs, psychological counseling, and community and family involvement. These findings provide an in-depth account of the real mental experiences of patients with Moyamoya disease and reveal their psychological struggles, adaptive efforts, and care expectations.
Conclusion: This study reveals the complex psychological burden experienced by Chinese patients with moyamoya disease, including persistent emotional distress, evolving coping strategies with disease progression, and unsatisfied needs for social and informational support. These findings underscore the need to incorporate psychological care (eg, early screening, emotional counseling, and caregiver engagement) into routine moyamoya disease management.
Keywords: moyamoya disease, cognition, experience, life management, mental, MMD
Introduction
Moyamoya disease (MMD) is a rare cerebrovascular disorder first described by Suzuki and Takaku in 1969,1 which characterized by nonatherosclerotic narrowing of the arteries in the brain, often leading to ischemic or hemorrhagic stroke. While clinical attention has traditionally focused on its ischemic and hemorrhagic complications,1–3 emerging research emphasizes that MMD also has a profound psychological impact on patients.
Psychiatric and emotional disorders in patients with MMD are generalized rather than incidental. A growing body of research emphasizes the prevalence of mental health problems among patients with MMD. According to a large-scale analysis of hospitalized patients, about 39% of MMD patients suffered from psychiatric co-morbidities, including mood disorders, anxiety, and substance use disorders.4 In addition, a systematic review by Saccaro et al synthesized the results of more than 40 studies and emphasized that psychological distress (including mood disorders, anxiety, and emotional instability) frequently affects patients with MMD, sometimes in the absence of overt neurological symptoms.5 These findings challenge the view of MMD as a purely neurological disease and emphasize the necessity of considering MMD as a disease with complex biopsychosocial implications.6
However, most existing research relies on quantitative tools7–9 that, while valuable for epidemiologic insights, may fail to capture the subtle, authentic psychological experiences of patients. Surveys can determine levels of depression and anxiety, but they often miss how individuals cognitively and emotionally process the diagnosis, cope with uncertainty, or adjust their identities and relationships.10
This gap in the literature requires a qualitative approach rooted in psychological theory. Drawing on Lazarus and Folkman’s stress and coping framework,11 which conceptualizes stress as an interactive process between the individual and their environment. The aim of this study was to explore the real mental experiences of MMD patients. Such insight is essential for developing holistic and patient-centered care strategies, particularly in the realm of psychosocial support and mental health intervention.
Materials and Methods
Study Design and Recruiting
The research employed a descriptive qualitative design with a semi-structured interview approach to allow for the exploration of emerging themes during interviews. The participants were selected via purposive sampling and were drawn from two tertiary care hospitals in Henan Province. The study adhered to the Consolidated Criteria for Reporting Qualitative Research,12,13 see Supplementary Table 1 for details. The included patients were aged 18 years or older, could communicate in Mandarin, met the diagnostic criteria for MMD (International Classification of Diseases - 10 code 167.5) at least 6 months earlier14 and voluntarily participated in the research. We excluded patients with cognitive impairment, hearing impairment, primary psychiatric, or serious diseases, such as cancer, other neurological diseases or liver disease. The sample size was determined by data saturation.
Data Collection
Data collection occurred from January 2024 to April 2024, with interviews conducted individually in private rooms at the hospital’s outpatient department or separate spaces. We used a face-to-face interview format and participants signed informed consent forms. No one other than the participants and the researcher was present during the interview. Each interview lasted 30~60 minutes and was audio-recorded with participants’ consent. Open-ended questions encouraged participants to describe their experiences and adaptation processes following a MMD diagnosis. The researchers aimed to minimize their influence on responses by observing nonverbal cues and recording them postinterview. The research team comprised registered nurses or medical practitioner with qualitative research training who reviewed patients’ case histories to understand their conditions before conducting interviews. The interview guide was based on a review of available research and clinical experience of relevant experts. See Table 1 for details.
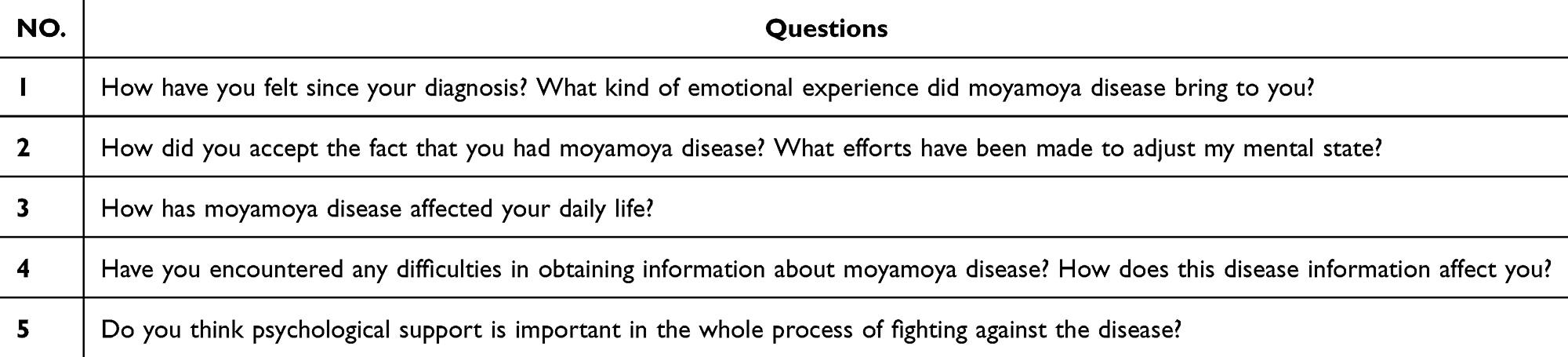 |
Table 1 Interview Guide |
Data Analysis and Rigor
We used the Colaizzi’s qualitative analysis procedure in this study,15 and we used NVivo 11.0 software to code and store the data. Each interview was professionally transcribed by reviewers. Then taking into account the overseas study experience and proficiency in English, the translation was translated from Chinese by M.L. and checked by J.W. The collected data were subjected to Colaizzi’s seven-step descriptive phenomenology process: (a) listening to the interviews and reading the transcripts for familiarization, (b) extracting significant statements related to experience with adult MMD patients, (c) deriving meaning from each significant statement, (d) categorizing all formulated meanings into thematic clusters, (e) integrating emergent themes into a comprehensive description, (f) identifying and describing the phenomena under analysis, (g) confirming findings with participants.16 Finally, the whole process was discussed, reviewed and revised by the whole research team.
To ensure the quality of the reported studies, all members of this research team were certified nurse practitioners, medical practitioners, or fellows. All members were at least master’s degree or have the title of associate director, and all were clinical medicine or nursing majors except Q.L. Q.L. completed the study of qualitative research under the guidance of M.L. and W.Z. He had never conducted qualitative research before, so all the work he participated in this study was carried out jointly with others and the quality of the work was strictly controlled. The other members of the research team have all studied qualitative research completely during their master’s studies. M.L., W.Z., J.W., Z.P., X.X. and H.L have all participated in qualitative research and published academic papers on qualitative research in the past. All study members were known to each other, and research team members maintained regular contact and feedback through meetings and telephone calls. The meeting is generally in the form of online meeting, and the software that provides technical support for the online meeting is “Tencent Meeting”. (https://meeting.tencent.com/)
Ensuring Quality of the Research Process and Product
Data analysis, team meetings, and participant validation were used to ensure rigor of this study. All interviews were conducted by four interviewers, Meng Li, Wenling Zhang, Dongsen Lv and Ning Zhang using semi-structured interview guidelines. They had rich experience in conducting semi-structured interviews, and their main research interests were chronic disease care and psychological care of patients. Participant statements were clarified during the interview, and data were recorded, transcribed verbatim, cross-checked, and returned to the participant for correction. Specifically, each transcript was encoded independently by Junfan Wei and Zhongjie Pan after cross-checking and discussion of the codes and topics; these two values were combined to determine the final transcript code. The codes were then grouped in accordance with similarities and differences, and the semantic content of the code was validated further. To enhance confirmability, an audit trail of coding revisions and memo writing was maintained throughout the analysis. To further ensure verifiability, we held frequent coding team meetings to discuss code usage, coding, refined definitions, and the translation, and any disagreements were resolved by the full group, see Supplementary Table 2 for examples of the coding strategy. Reliability was ensured by external research protocol review. To strengthen reflexivity, interviewers maintained reflective memos throughout the study to monitor how their prior clinical experience and assumptions might shape data interpretation. While all had expertise in chronic disease and patient communication, none had a treatment relationship with the participants to minimize role-based bias.
Ethic Consideration
This study followed the Declaration of Helsinki (and was approved by Ethics Committee of the Third People’s Hospital of Henan Province, ethics number: 2024-SZSYKY-003). All participants were informed of the purpose of the study and informed that participation in this study was voluntary and that they could withdraw at any time. All information about the patients was explained in detail as to what part of the information might be disclosed and what part of the information would not be disclosed. All patients participated in this study voluntarily. Written consent was received from participants prior to the commencement of data collection.
Results
None of the eligible subjects selected according to the inclusion and exclusion criteria refused to participate in the interview. We conducted three interviews with each participant, but the results of the first two were not included in the study, except for the third interview, which was directly related to the purpose of the study. The first two interviews serve as the basis for in-depth interviews to build a good trust and understanding with patients, so that patients can look inward more clearly to understand their current living state and further explore their true inner feelings. There were no data relevant to this study in the content and results of their interviews. Ultimately, 17 patients participated in this study. The patients included 8 men and 9 women with a mean age of 32.29 years (standard deviation = 5.89 years). The detailed demographic characteristics of all participants are presented in Table 2.
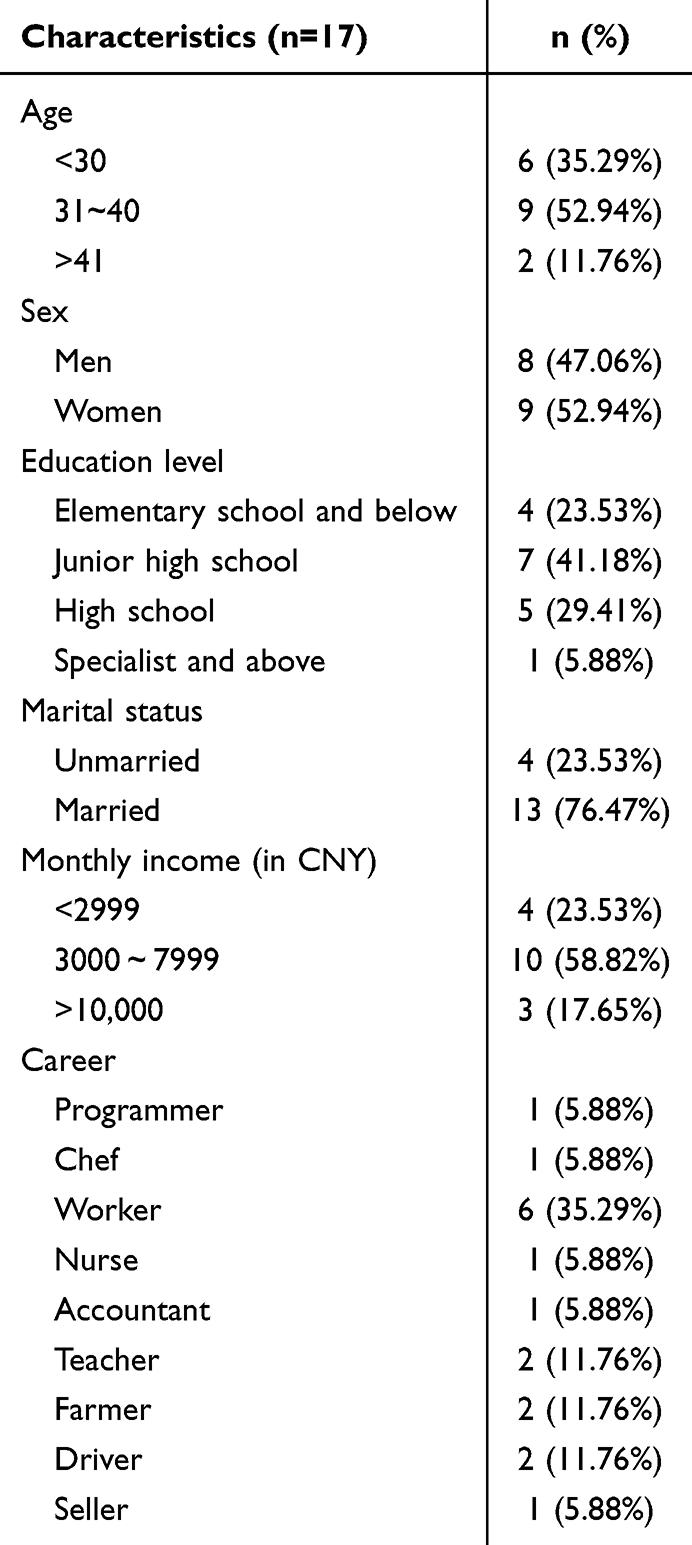 |
Table 2 Demographic Characteristics of the Participants |
From the interview data analysis, we summarized five themes: (1) cognitive and emotional experience, (2) process of psychological adjustment, (3) impact on quality of life, (4) information needs and seeking and (5) long-term care and support. The specific themes and sub-themes are shown in Table 3.
 |
Table 3 Themes and Subthemes |
Theme 1: Cognitive and Emotional Experience
Subtheme 1: Fear and Anxiety
Fear and anxiety were the most frequently reported emotional responses among participants. These reactions stemmed from the unpredictable nature of MMD, concerns over long-term prognosis, and fear of disability. Participants reported constant vigilance, existential worry, and emotional distress.
Whenever I think about my Moyamoya disease, I’m overwhelmed by fear and anxiety. I worry it might worsen, that there’s no cure, and that I could become a burden to my family. (N1)
I’m constantly anxious about when Moyamoya disease might strike. During attacks, I feel like I’m dying, and the pain and helplessness are unbearable. (N6)
Each time I see my doctor’s serious expression and hear bad news, extreme anxiety takes over. I do not know how to navigate this uncertain future. (N9)
I’m afraid of losing my intelligence and emotions, not recognizing my family, and jeopardizing my life, family, and career due to Moyamoya disease. (N11)
In the quiet of the night, my condition brings on feelings of loneliness and helplessness, leaving me anxious and uncertain about facing the future. (N17)
Formulated Meaning: Persistent fear is associated with the unpredictable course of MMD and its potential impact on identity, autonomy, and family roles.
Subtheme 2: Denial and Acceptance
Participants typically described an initial phase of denial following diagnosis, followed by a gradual process of emotional adaptation and acceptance. Denial is a short-term coping mechanism, while acceptance often occurs with the help of medical interventions and social support.
I cannot believe I have this rare Moyamoya disease; it must be a misdiagnosis. (N3)
I cannot accept this fact; how could this rare disease happen to me? (N4)
I do not want to face this disease; I hope it is just a dream, and everything will return to normal when I wake up. (N7)
I once had the rare Moyamoya disease, a severe cerebrovascular condition. Each time I had an episode, I felt a splitting headache, as if a smoky haze enveloped my brain. The doctor told me I needed immediate surgery, but I was deeply afraid. However, I knew that avoiding it was not an option. Therefore, I bravely underwent treatment and, with the doctor’s help, conquered the disease. Now, I feel completely recovered and have returned to a normal life. (N13)
Formulated Meaning: Clear implications: denial is the initial buffer against suffering, while acceptance comes from realistic contact with the disease and adaptive coping.
Subtheme 3: Altered Self-Perception
MMD significantly affected participants’ self-concept and mood. Some of them described their feelings of helplessness and alienation, while others reported shifts in their perceptions of life, identity and health.
Every time an episode strikes, it feels like an invisible force is choking me, making it impossible to breathe. (N1)
Even though doctors told me that this disease is very rare, thinking about it still makes me feel lonely and helpless. (N5)
I used to love life, sports, and creative work, but now I have to carefully maintain my health. I’m unsure if I can return to work normally like before. (N8)
Moyamoya disease has altered my life and changed my perspective, making me cherish each day even more. (N10)
I do not want this disease to define me; I’m just an ordinary person, a patient in need of care and understanding. (N15)
Formulated meaning: The illness experience reshapes self-image, ranging from perceived loss to post-traumatic growth, indicating identity re-evaluation.
Theme 2: Process of Psychological Adjustment
Subtheme 1: Coping Strategy
Participants employed a variety of coping strategies to manage their condition. These included adherence to medical treatment, maintaining a positive outlook, engaging in peer communication, and establishing self-monitoring routines. Such behaviors reflect a problem-focused and proactive coping style.
I will actively cooperate with the doctor’s treatment plan and not give up any opportunity for recovery. (N2)
I will maintain a positive mindset and not let this disease break my willpower. (N5)
I will undergo regular check-ups, closely monitor my physical condition, and prevent Moyamoya disease from relapsing. (N7)
I will communicate with fellow patients, share experiences, and support each other in overcoming this rare disease together. (N11)
I will cherish each day of life, and with a positive attitude, I will face the challenges and difficulties of the future. (N14)
Formulated Meaning: After experiencing the most intense emotional burdens, MMD patients often adopt positive coping styles such as adherence to treatment, emotional self-regulation, peer support, and future-oriented thinking for psychological adjustment.
Subtheme 2: Social Support
Social and interpersonal resources played a central role in the psychological adaptation of participants. Support came from family, friends, healthcare providers, and fellow patients. These interactions facilitated emotional stabilization, reduced isolation, and promoted motivation.
The companionship of my family, professional care from healthcare professionals, and encouragement from fellow patients all helped me regain the courage to live. This support allowed me to see a glimmer of hope amidst the pain and strengthened my determination to overcome the disease. I will cherish this strength, bravely move forward, and hope that more people can pay attention to and support rare disease patients, so we can collectively safeguard the power of life. (N6)
The companionship of family brings me warmth, the concern of friends gives me strength, and the professional support of the medical team fills me with confidence. Without their support, I could not imagine how I would face this rare MMD. These forces converge to become the source of my motivation to conquer the disease. (N14)
Formulated Meaning: Perceived social support enhances positive coping style and fosters psychological resilience of MMD patients during disease management.
Subtheme 3: Psychological Growth
In addition to basic coping styles, several participants described profound personal transformations as a result of their illness experience. This included increased emotional resilience, re-prioritization of life values, and deepened appreciation for relationships.
MMD has led me to reevaluate the meaning of life, and I have started to cherish each day more. (N9)
Although illness has subjected me to immense psychological stress, it has also taught me resilience and bravery. (N12)
Whenever I think about my rare condition, I still feel a hint of fear, but I know I cannot let fear control me. (N14)
The process of battling the disease has helped me better understand my inner self, and I have learned how to find hope amidst adversity. (N17)
My experience with MMD has made me more grateful and thankful for the support of my family and friends, as well as the care and treatment provided by doctors. (N18)
Formulated Meaning: A part of MMD patients experienced post-traumatic growth, demonstrating psychological growth characterized by meaning reconstruction, emotional maturity, and strengthened relational appreciation.
Theme 3: Impact on Quality of Life
Subtheme 1: Daily Function
Participants reported substantial disruptions in physical ability, routine activities, and emotional stability. While some expressed discouragement and helplessness, others engaged in cognitive reframing to sustain daily motivation and goal-oriented behavior.
MMD has made my life exceptionally challenging, but I will strive to overcome these difficulties and work toward a return to normalcy. (N4)
My rare MMD significantly impairs my daily life functions, making me feel very helpless and discouraged. (N7)
Despite my mobility limitations due to MMD, I always maintain a positive and optimistic outlook, believing that one day I can defeat this illness. (N11)
MMD has made me aware of the fragility and preciousness of life. I will cherish each day more and endeavor to make the most of every day. (N13)
Although my MMD has lowered my quality of life significantly, I will do my best to overcome the challenges and strive for a better life. (N16)
Formulated Meaning: MMD imposes diverse functional limitations that disrupt everyday life, prompting emotional distress. Nonetheless, participants demonstrate a range of adjustment efforts—balancing dependence and self-directed coping—to reestablish purpose and maintain quality of life.
Subtheme 2: Interpersonal Relationships
Participants described varied impacts of MMD on their social and family relationships. While many highlighted the emotional comfort and practical assistance offered by loved ones, others reported tension, miscommunication, and feelings of disconnection. Supportive relationships often became essential coping resources, whereas relational strain introduced additional psychological burdens.
MMD took away my ability to speak, but I have never felt alone. Friends communicate with me using pen and paper, and my family’s sign language makes me feel the warmth of life. (N2)
After each episode, I tend to forget things, but my wife patiently explains to me. Her love keeps the quality of my life high. (N4)
I lost sensation in the left half of my body due to Moyamoya disease, but my family has always been by my side, supporting and encouraging me. Their presence has helped me rediscover the meaning of life. (N6)
MMD has limited my mobility, but my children assist me with physical therapy and accompany me on walks every day. Our laughter is the most beautiful music. (N7)
Although my memory is not what it used to be, my friends regularly visit me and share bits of life with me. Their care makes me feel as warm as ever. (N11)
MMD has distanced me from my friends as they struggle to understand my condition, and I often feel isolated. Relationships with family have also become strained because they constantly worry about my health. However, every time I interact with doctors, they show endless patience and care, making me feel that I am not alone. I have also learned to communicate with the world in new ways, though it is challenging, and I am striving to make the most of each day. (N13)
Formulated Meaning: Social relationships can either buffer or compound the emotional challenges of MMD. The quality of support from close contacts significantly affects patients’ sense of connection, identity, and resilience.
Subtheme 3: Life Satisfaction
Despite the physical and psychological challenges of MMD, participants described varying degrees of life satisfaction. Many expressed gratitude, enhanced appreciation for health, and a redefinition of what constitutes a meaningful life.
Although I have rare MMD, every time I think about how many people care about me, my life is filled with hope and gratitude. I am content with life, and this illness has not defeated me. (N1)
After falling ill, I started to cherish every day, every breath, and every smile even more. Despite the difficulties in life, I never give up. I am satisfied with my life, and I believe the future will be better. (N5)
Falling ill made me realize that health is more important than anything else. Although there are some inconveniences in life, I always maintain an optimistic attitude. I believe that with faith and effort, one can lead a fulfilling and meaningful life. (N6)
Having this rare MMD has made me feel the fragility and unpredictability of life. However, it is this experience that has made me cherish and be grateful for every day even more. I am content with my current life, and I believe that every day is a gift from above. (N8)
Despite the challenges that the illness has brought to my life, the support of my family, the care of my friends, and the professional care from healthcare professionals have all made me feel incredibly warm. I am satisfied with my current life, and I will cherish every day and strive to make the most of it. (N11)
Formulated Meaning: Life satisfaction in the context of MMD is shaped by patients’ ability to reframe adversity, maintain social connection, and realign life priorities—resulting in existential growth despite ongoing limitations.
Theme 4: Information Needs and Seeking
Subtheme 1: Challenges in Accessing Reliable Information
Participants described considerable difficulty in locating trustworthy, disease-specific information about MMD. The rarity of the condition, combined with fragmented sources and misinformation online, heightened uncertainty and distress. Patients expressed a strong desire for centralized, authoritative educational resources and platforms for peer exchange.
After I fell ill, I was eager to learn about the causes and treatment methods for the rare MMD, but it was difficult to find authoritative and accurate information. I hope that doctors and healthcare institutions can provide more educational knowledge about rare diseases, allowing us patients to have a better understanding. (N6)
I had never heard of this rare MMD before I fell ill, and I felt very helpless and panicked once I was diagnosed. Later, I searched for some related information online, but it was overwhelming, and it was challenging to distinguish between what’s true and false. Having a professional platform or organization that provides us with accurate and comprehensive disease information would be immensely helpful for us patients. (N8)
After I fell ill, my family and friends helped me search for information about rare MMD, but it was challenging to find useful resources. I hope that more nonprofit organizations or social initiatives can pay attention to rare disease patients like us and provide targeted health information and psychological support. (N11)
Formulated Meaning: The lack of accessible, accurate, and centralized information in the daily disease management of patients with MMD leads to confusion and insecurity, emphasizing the need for supportive networks and communication platforms.
Subtheme 2: The Need for Understandable Disease-Related Explanations
Patients with MMD seek clarity on recurrence, causes, treatments, recovery, and complications. Clear explanations from healthcare professionals help alleviate worries and support informed decision-making. Effective communication between patients and healthcare providers is crucial for comprehensive understanding and management of the condition.
I have heard that this rare MMD is prone to recurrence; is that true? I’m genuinely worried. (N4)
I have some questions about the causes and treatment methods of this rare MMD; could you explain it to me again? (N9)
I have heard that the recovery period for this rare MMD is quite long, and I need to prepare mentally; is that true? I’m a bit scared. (N10)
Doctor, I’d like to know what complications are associated with this rare MMD. I want to understand them better for prevention purposes. (N12)
Formulated Meaning: Patients emphasized the need for healthcare providers to deliver information using simple language and repeat explanations when necessary. Such communication builds trust, reduces fear, and empowers patients to engage actively in managing their condition.
Subtheme 3: Psychological Impact of Information Acquisition
For many participants, initial exposure to information about MMD was distressing and disorienting. However, as their understanding deepened over time, information became a stabilizing force. Obtaining accurate and relevant information helped patients move from a fearful to a positive outlook, increased their resilience, motivated behavioral change, and enhanced their sense of mastery.
Upon learning that I had the rare MMD, I felt extremely shocked and helpless. I began to reevaluate my lifestyle and dietary habits, worrying about my future health. (N3)
When the doctor informed me about having the rare MMD, my initial feelings were fear and despair. However, as I delved deeper into understanding this condition, I gradually realized the importance of positive treatment and the right lifestyle choices for recovery. (N5)
After discovering I had the rare MMD, I started paying closer attention to my physical condition and mental well-being. I began to focus on maintaining a healthy diet and engaging in appropriate exercise while also learning how to cope with stress and anxiety. (N7)
Upon receiving the diagnosis of the rare MMD from my doctor, I began searching for relevant information and resources to understand the causes, symptoms, and treatment options for this condition. Through knowledge, I gradually overcame fear and insecurity, becoming more confident and determined. (N10)
Upon finding out that I had the rare MMD, I started cherishing every day of life even more. I learned how to balance work and life, placing greater importance on relationships with family and friends. Although the disease presented challenges, it also made me appreciate life and health more. (N12)
Formulated Meaning: As participants acquired worthy and comprehensible information, it transformed their initial anxiety into constructive coping. This knowledge not only enhanced emotional stability but also instilled a stronger sense of self-efficacy and readiness to make informed health choices.
Theme 5: Long-Term Care and Support
Subtheme 1: Long-Term Rehabilitation
Participants emphasized that recovery from MMD is not limited to short-term medical treatment or physical rehabilitation, but involves a gradual and enduring process of psychological and social adjustment. Many described rehabilitation as a prolonged, dynamic effort to regain both functional ability and emotional balance, sustained through ongoing self-motivation, emotional support, and encouragement from family, peers, and health providers.
Since being diagnosed with the rare MMD, I have been striving to adapt to the changes in my body for a long time. Throughout the recovery process, what I have felt the most need for is psychological support because the disease brings not only physical trauma but also mental stress. (N3)
I once fell into despair, unsure of what the future held. Because it takes a long time for the treatment to work. But it slowly starts to show some effects, I gradually realized that only by facing it positively could I overcome the disease. Now, I cherish each day more and strive to make the most of it. (N5)
Rehabilitation takes place over a long period. During the recovery process, I realized that I needed more care and companionship. My family’s support has been my greatest motivation; their encouragement and love have given me the confidence to conquer the disease. (N9)
During the recovery process, I encountered many patients like myself. We encourage and support each other, facing the disease together. This mutual support gives me warmth and the courage to conquer the disease. (N12)
Formulated Meaning: Recovery from MMD requires sustained physical, psychological, and social effort. Long-term rehabilitation is bolstered by ongoing encouragement, shared experience, and the integration of emotional care alongside physical healing.
Subtheme 2: Psychological Support
Participants described psychological intervention as a key enabler in adjusting to the emotional burden of MMD. It helped them recognize the mental health impact of their condition, develop effective emotional regulation strategies, and improve communication with family and peers. Beyond symptom relief, psychological support was seen as transformative—restoring confidence, reframing life priorities, and fostering resilience.
Psychological intervention is genuinely helpful; it has made me realize that my emotions are not baseless but influenced by the disease. I now have more confidence in facing my condition. (N2)
During the treatment process, psychological intervention taught me how to regulate my emotions, and I am no longer as prone to anxiety and depression as before. This has been very helpful in my recovery. (N5)
Through psychological intervention, I learned how to communicate better with family and friends. They now better understand my needs and emotions, which brings me warmth and comfort. (N7)
I used to feel like a burden, but now I know that through psychological intervention, I can better manage my emotions and no longer let the disease affect my quality of life and family relationships. (N10)
Psychological intervention has led me to reevaluate my worldview and values. I understand that health is the most important, and I must cherish each day and face life with a positive attitude. (N12)
Formulated Meaning: Psychological support enables emotional resilience, promotes adaptive interpersonal dynamics, and facilitates deeper acceptance and personal growth in the face of chronic illness.
Subtheme 3: Community and Family Support
Participants frequently highlighted the stabilizing role of community networks and family members. Their emotional and practical contributions not only supported daily living and rehabilitation but also reinforced a sense of belonging and collective strength in dealing with MMD.
The community has provided us, rare MMD patients, with a lot of help. They regularly organize health lectures and activities, allowing us to gain more knowledge about the disease and making us feel less alone. (N1)
Family is my strongest support. When my condition worsens, my family is always there by my side, giving me strength and courage. Without their support, I might not have been able to persist until now. (N3)
I am very grateful to my community and family. They have provided me with many resources and support, allowing me to become stronger and more optimistic in the face of the challenges posed by rare MMD. (N4)
Through participating in community rehabilitation training and the support of my family, I gradually overcame physical obstacles, rediscovered confidence and joy in life. (N11)
I believe that, through the joint efforts of the community and family, we can create a more friendly and supportive environment for MMD patients, helping them better cope with the disease, regain health, and happiness. (N13)
Formulated Meaning: Community and family involvement offers crucial practical assistance and emotional scaffolding that sustain patients through prolonged recovery. Their presence facilitates patients’ reintegration into society, strengthens their coping resources, and promotes continuity of care.
Discussion
This qualitative study provides new insights into the psychological experiences of people with MMD, particularly their emotional experiences as they go through their diagnosis, how they cope with emotional distress, psychological adjustment, and social adjustment. These findings are particularly important given the limited literature exploring MMD from a mental health perspective.
In the present study, patients report fear, recurrent anxiety, denial, and emotional vulnerability during the onset and progression of the MMD. While such profound emotional burdens are common in other chronic neurological diseases such as stroke and epilepsy, they appear to be particularly prominent in MMD patients. Recent studies have confirmed that patients with MMD bear a considerable emotional burden, with a proportion experiencing persistent psychological distress and developing clinical psychiatric into disorders. For example, Mansuri et al reported that nearly 39% of patients with MMD had psychiatric co-morbidities, mainly mood and anxiety disorders.4 In addition, Haas et al showed that patients with MMD exhibit significant neuropsychological impairment.17 What’s more, the pathophysiology of MMD - particularly chronic cerebral underperfusion - may also lead to broader somatic impairments, including cognitive decline, metabolic abnormalities, and fatigue.18 These somatic impairments, while often perceived as secondary, can exacerbate psychiatric symptoms such as depression, anxiety, and cognitive dysfunction.19 This underscores the need to view psychiatric comorbidities in MMD not merely as emotional reactions, but as neurovascularly mediated disorders with intertwined metabolic and somatic dimensions.5 Therefore, the psychological and mental health status of patients with MMD should be emphasized and assessed early, and healthcare professionals should consider it as a neurovascular-mediated disease to provide somatic-psychiatric integrated care.
During the process of acceptance and rehabilitation, many patients use coping strategies such as actively cooperating with treatment, seeking information, and building emotional resilience. These strategies are consistent with adaptive behaviors reported in chronic neurodegenerative diseases such as Parkinson’s disease. A recent focus group study described the transition of Parkinson’s patients through denial, emotional acknowledgement, and ultimately the adoption of proactive, task-oriented coping strategies to maintain autonomy and identity.20 In addition, comparative studies of Parkinson’s and epilepsy patients have found that proactive, problem-focused, and adherence-based strategies are common and associated with better psychosocial outcomes.21 These findings suggest that these adaptive patterns may be prevalent in the treatment of patients with progressive, indeterminate disorders, regardless of the specific diagnosis. This provides insights for healthcare professionals to facilitate this process by providing structured psychoeducational programs, teaching stress management techniques, and promoting self-monitoring tools that support autonomy and emotional regulation.
As patients gain a deeper understanding of the disease and come to term with it, they begin to employ various coping strategies, such as actively complying with treatment and seeking social support, to manage the stress caused by the disease. In this process, the support of family, friends, and medical teams proves to be crucial, providing emotional reliance and substantial assistance to patients and aiding in their psychological adaptation and growth. This finding is consistent with the findings of Kaitlyn Stoehr’s research.22 Common coping strategies included seeking information, establishing a medication routine to make dosage-related symptomatic variability more predictable, and finding tricks to manage individual symptoms. Social support and emotion-focused strategies, such as acceptance, faith, social comparison, perseverance, and positivity, are used to cope with the psychological impact of progressive illness.23 To enhance these effects, providers should consider counseling models that include caregivers and provide guidance to families on how to provide effective emotional and resource support to patients.
Social and family support was another central theme of our findings, which is consistent with the extensive literature in cancer and cardiovascular populations, where interpersonal relationships serve as an important buffer against psychological distress.24 In particular, positive support was associated with reduced anxiety and depression, while negative interactions heightened distress among both patients and their relatives. For patients with MMD, such a support system proved to be equally important - both practically and emotionally - providing not only useful help, but also comfort, as participant narratives indicate that “The companionship of my family.strengthened my determination to overcome the disease” (N14). Conversely, disruption of relationships was a recurring theme mentioned by patients during our interviews. Some patients described how their illness led to withdrawal from social roles, tension in family dynamics, or feelings of being misunderstood by peers. Similar correlates of impairment were seen in patients with epilepsy, stroke, and brain tumors, where chronic neurological impairment led to stigma, isolation, and altered family roles. This is poignantly reflected in the account of a patient with MMD: “MMD has alienated me from my friends. and strained my relationship with my family” (N13). Our study further reveals that despite this psychosocial stress, many patients demonstrate adaptive shifts, particularly through strengthening relationships with core caregivers. These connections may be protective factors, fostering resilience in chronic illness, a trend echoed in the broader chronic illness literature. This suggests that support groups-whether peer-led or professionally facilitated-can be introduced as part of an MMD recovery program to strengthen interpersonal connections and reduce isolation.
In addition, patients’ demand for clarity and accessibility of information is also outstanding. Reflecting broader trends in patient-centered medicine, that is, health literacy and access to information are directly related to psychological empowerment and treatment adherence.25 Lack of access to reliable knowledge is also associated with increased distress and decreased self-efficacy in rare patient populations,26 where health information is often fragmented or difficult to access, magnifying the psychological burden on patients. Therefore, we suggest that healthcare institutions develop patient-centered informational resources, including digital platforms and printed materials in accessible language, and ensure consistent follow-up education throughout the treatment process.
Finally, psychological interventions such as cognitive behavioral therapy (CBT), trauma-informed therapy, and structured family counseling have shown efficacy in a wide range of chronic illnesses such as cancer, depression, and neurovascular disease. For example, trauma-focused CBT has been widely used in home-based therapeutic settings to reduce psychological distress and promote emotional regulation.27 More broadly, CBT has shown robust benefits across a range of disorders by helping patients reframe negative thought patterns and build adaptive coping strategies that lead to improved quality of life.28 Incorporating such interventions into MMD care may significantly reduce psychological distress, improve emotional functioning, and enhance quality of life.
Strengths and Limitations
Our study has several strengths. First of all, this study is relatively innovative. As far as we know, this is the first qualitative study in mainland China to explore the real psychological experiences of patients with MMD (MMD). Adopting a phenomenological framework and drawing on Lazarus and Folkman’s stress coping theory, this study not only deepens the understanding of the psychological state of MMD patients, but also contributes theoretically by contextualizing the psychological experience associated with MMD through the cognitive-emotional regulation model. In addition, participants responded with a wide variety of responses, indicating a low incidence of bias. Moreover, because this qualitative study utilized the resources of a parallel study, it minimized the need for additional research time and funding. But at the same time, there were several limitations as well. First, our participant selection was limited to two tertiary care hospitals in Henan Province, China. This could restrict the representativeness of our sample, as the experiences and perceptions of MMD patients in different regions or healthcare settings may vary significantly. Second, while we conducted interviews with 17 patients, which yielded rich qualitative data, it is important to note that this sample size may not encompass the full spectrum of experiences among MMD patients. A larger sample size would enhance our ability to gain a more comprehensive understanding. Additionally, there is a potential risk of recall bias, as patients may not always recall specific details related to the onset of their disease, which could influence their responses.
Conclusion
This study reveals the complex psychological burden experienced by Chinese patients with MMD, including persistent emotional distress, evolving coping strategies with disease progression, and unsatisfied needs for social and informational support. These findings underscore the need to incorporate psychological care (eg, early screening, emotional counseling, and caregiver engagement) into routine MMD management. Future studies should include a larger geographic range of patients, while larger sample sizes may help further understanding, and multicenter studies and longitudinal qualitative designs may also enrich understanding of psychological trajectories over time.
Data Sharing Statement
Due to the sensitive nature of the questions asked in this study, survey respondents were assured raw data would remain confidential and would not be shared, so supporting data is not available.
Ethics Approval and Consent to Participate
This study followed the Declaration of Helsinki (and was approved by Ethics committee of the Third People’s Hospital of Henan Province, ethics number: 2024-SZSYKY-003). All participants were informed of the purpose of the study and provided written informed consent. This consent explicitly included the publication of anonymized responses and direct quotes.
Acknowledgments
We would like to thank all the patients, their families, and the providers who assisted with interviews for participation in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Gonzalez NR, Amin-Hanjani S, Bang OY, et al. Adult Moyamoya disease and syndrome: current perspectives and future directions: a scientific statement from the American heart association/American stroke association. Stroke. 2023;54(10):e465–e479. doi:10.1161/STR.0000000000000443
2. Ihara M, Yamamoto Y, Hattori Y, et al. Moyamoya disease: diagnosis and interventions. Lancet Neurol. 2022;21(8):747–758. doi:10.1016/S1474-4422(22)00165-X
3. Chiang CC, Shahid AH, Harriott AM, et al. Evaluation and treatment of headache associated with moyamoya disease - a narrative review. Cephalalgia. 2022;42(6):542–552. doi:10.1177/03331024211056250
4. Mansuri Z, Patel K, Trivedi C, et al. Burden of psychiatric disorders in Moyamoya disease: a national inpatient perspective from 2007-2014. Prim Care Companion CNS Disord. 2022;24(4). doi:10.4088/PCC.21m03157
5. Saccaro LF, Mallet C, Wullschleger A, Sabé M. Psychiatric manifestations in moyamoya disease: more than a puff of smoke? A systematic review and a case-reports meta-analysis. Front Psychiatry. 2024;15:1371763. doi:10.3389/fpsyt.2024.1371763
6. Desai R, Thakkar S, Patel HP, et al. Higher odds and rising trends in arrhythmia among young cannabis users with comorbid depression. Eur J Intern Med. 2020;80:24–28. doi:10.1016/j.ejim.2020.04.048
7. Yang YS, Ryu GW, Yeom I, Shim KW, Choi M. Stress and mood of adults with moyamoya disease: a cross-sectional study. Nurs Health Sci. 2020;22(3):795–802. doi:10.1111/nhs.12729
8. Kuroda S, Fujimura M, Takahashi J, et al. Diagnostic criteria for Moyamoya disease - 2021 revised version. Neurol Med Chir. 2022;62(7):307–312. doi:10.2176/jns-nmc.2022-0072
9. Ryu GW, Yang YS, Choi M, Shim KW. Lived experiences of adult patients with moyamoya disease: a qualitative case study. Jpn J Nurs Sci. 2020;17(3):e12332. doi:10.1111/jjns.12332
10. DeJean D, Giacomini M, Vanstone M, Brundisini F. Patient experiences of depression and anxiety with chronic disease: a systematic review and qualitative meta-synthesis. Ont Health Technol Assess Ser. 2013;13(16):1–33.
11. Nattiv A, Loucks AB, Manore MM, Sanborn CF, Sundgotborgen J, Warren MP. Stress, appraisal, and coping. Med Sci Sports Exercise. 2007;39(10):1867–1882. doi:10.1249/mss.0b013e318149f111
12. Shenton AK. Strategies for ensuring trustworthiness in qualitative research projects. Educ Inf. 2004;22(2):63–75. doi:10.3233/EFI-2004-22201
13. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
14. Asselman C, Hemelsoet D, Eggermont D, Dermaut B, Impens F. Moyamoya disease emerging as an immune-related angiopathy. Trends Mol Med. 2022;28(11):939–950. doi:10.1016/j.molmed.2022.08.009
15. Vignato J, Inman M, Patsais M, Conley V. Computer-assisted qualitative data analysis software, phenomenology, and Colaizzi’s method. West J Nurs Res. 2022;44(12):1117–1123. doi:10.1177/01939459211030335
16. Holloway I, Wheeler S. Qualitative research in nursing and healthcare. Br J Anaesth. 2010;84(5):552–555.
17. Haas P, Kittelberger BB, Hurth H, et al. Health-related quality of life and neuropsychological outcome after EC-IC bypass revascularization in adult patients with Moyamoya disease. Neurosurgery. 2024. doi:10.1227/neu.0000000000002813
18. Hao X, Tan C, Liu Z, et al. Research progress in unilateral moyamoya disease. Front Hum Neurosci. 2025;19:1503639. doi:10.3389/fnhum.2025.1503639
19. You J, Xia S. Association between the dietary inflammatory index and depressive symptoms in adults with metabolic syndrome: a cross-sectional study from the NHANES database. Front Nutr. 2025;12:1518551. doi:10.3389/fnut.2025.1518551
20. Daemen MMJ, De Bruijn-Heijligers B, Van Der Heijden C, et al. Navigating life with Parkinson’s disease: a focus group study on coping strategies and considerations for self-management support. J Adv Nurs. 2025;81(4):2003–2012. doi:10.1111/jan.16414
21. Krakow K, Haltenhof H, Bühler KE. Coping with Parkinson’s disease and refractory epilepsy. A comparative study. J Nerv Ment Dis. 1999;187(8):503–508. doi:10.1097/00005053-199908000-00007
22. Stoehr K, Pazira K, Bonnet K, Schlundt D, Charles D, Hacker M. Deep brain stimulation in early-stage Parkinson’s disease: patient experience after 11 years. Brain Sci. 2022;12(6):766. doi:10.3390/brainsci12060766
23. Bavik YL, Shaw JD, Wang XHF. Social support: multidisciplinary review, synthesis, and future agenda. Acad Manage Ann. 2020;14(2):726–758. doi:10.5465/annals.2016.0148
24. Hermann M, Goerling U, Hearing C, et al. Social support, depression and anxiety in cancer patient-relative dyads in early survivorship: an actor-partner interdependence modeling approach. Psychooncology. 2024;33(12):e70038. doi:10.1002/pon.70038
25. Mohiuddin AK. Low health literacy (LHL): a conniving opponent of patient treatment compliance. SIASAT. 2023;8(1):33–39. doi:10.33258/siasat.v8i1.141
26. Spring H. Health information, what happens when there isn’t any? Information literacy and the challenges for rare and orphan diseases. Health Info Libr J. 2014;31(3):243–246. doi:10.1111/hir.12068
27. Cohen JA, Mannarino AP. Trauma-focused cognitive behavior therapy for traumatized children and families. Child Adolesc Psychiatr Clin N Am. 2015;24(3):557–570. doi:10.1016/j.chc.2015.02.005
28. Dobkin DF, Allen LA, Menza M. Cognitive-behavioral therapy for depression in Parkinson’s disease: a pilot study. Mov Disord. 2010;22(7):946–952. doi:10.1002/mds.21455
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.