")
Back to Journals » International Journal of Women's Health » Volume 17
Extremely High Systemic Immune Inflammation Levels Increase the Risk of All-Cause and Cardiovascular Mortality in Postmenopausal Women
Authors Wu F, Yang J, Liu Y, Zhang Y
Received 5 November 2024
Accepted for publication 11 May 2025
Published 20 May 2025 Volume 2025:17 Pages 1457—1468
DOI https://doi.org/10.2147/IJWH.S504664
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Fei Wu,1 Jiantong Yang,1 Yinchuan Liu,1 Yipei Zhang2
1Department of Gynecology, Jiangxi Maternal and Child Health Hospital, Nanchang, Jiangxi, 330006, People’s Republic of China; 2Department of Gynecology, Nanchang Hongdu Hospital of Traditional Chinese Medicine, Nanchang, Jiangxi, 330008, People’s Republic of China
Correspondence: Yipei Zhang, Department of Gynecology, Nanchang Hongdu Hospital of Traditional Chinese Medicine, Nanchang, Jiangxi, 330008, People’s Republic of China, Email [email protected]
Background: The systemic immune inflammation (SII) index provides a comprehensive assessment of inflammatory and immune status in patients with different diseases. However, it remains unclear whether the SII can be considered a valuable prognostic risk factor of all-cause mortality for postmenopausal women.
Methods: We analyzed data from 1882 postmenopausal women enrolled in the National Health and Nutrition Examination Survey (NHANES) from 1999 to 2018. The Systemic Immune-Inflammation Index (SII) was calculated using peripheral blood cell counts and categorized into quartiles. Multivariable Cox proportional hazards models and restricted cubic spline analyses were employed to assess the association between SII and mortality outcomes.
Results: Over a median follow-up period of 8 years, 13.5% individuals died, with 4% deaths attributed to CVD. Patients with extremely high SII levels experienced significantly higher all-cause and CVD mortality. Compared to the low SII group (Q1), the hazard ratio (HR) and 95% confidence interval (CI) for all-cause mortality risk were 0.96 (0.87, 1.07), 0.97 (0.88, 1.08), and 1.28 (1.16, 1.41) for Q2, Q3, and Q4, respectively. Similarly, the HR (95% CI) for CVD mortality in Q2, Q3, and Q4 were 1.02 (0.83, 1.24), 1.11 (0.92, 1.34), and 1.32 (1.10, 1.58), respectively. Including SII in addition to traditional risk factors resulted in a slight enhancement in mortality prediction capability.
Conclusion: Among postmenopausal women, extremely high SII levels were identified as an independent risk factor for all-cause and CVD mortality.
Keywords: systemic immune inflammation, mortality, postmenopausal women, women health, cardiovascular disease
Background
Postmenopausal women, defined as individuals who have completed menopause more than a year ago, generally range in age from 45 to 55 years.1 As the global population ages, the proportion of postmenopausal women has increased markedly.2 Current estimates suggest that nearly one billion women globally are in the postmenopausal phase.3 Significant hormonal changes, particularly the decline in estrogen levels, expose postmenopausal women to various health risks.4 Notably, the incidence of cardiovascular disease (CVD) in postmenopausal women is two to three times higher than in their premenopausal counterparts.5 This elevation is likely attributable to the diminished cardioprotective effects of estrogen following menopause, which leads to a rapid increase in CVD incidence.6 Moreover, postmenopausal women are at an elevated risk of developing osteoporosis, obesity, hypertension, diabetes, and other components of metabolic syndrome.7–9
Systemic immune inflammation is increasingly recognized as a pivotal pathological mechanism underlying a variety of chronic conditions, such as CVD, diabetes, and cancer.10–12 The excessive and persistent expression of inflammatory cytokines is strongly linked to a wide range of adverse health outcomes.13,14 Recently, the systemic immune-inflammation index (SII) has been introduced as an integrative measure for assessing the inflammatory and immune status of individuals.15 This index is derived from the counts of lymphocytes, neutrophils, and platelet. Neutrophils are indicative of the acute inflammatory response, lymphocytes represent immune regulation, and platelets are involved in inflammation and thrombosis.16,17 The combination of these three components provides a comprehensive measure of both immune suppression and inflammation, making SII a robust biomarker of systemic inflammation. Compared to other inflammatory scores, such as the “low-grade inflammation score”, the SII offers several advantages. It is relatively easy to calculate from routine complete blood counts (CBC), is non-invasive, and does not require specialized testing, making it feasible for large-scale epidemiological studies. Moreover, SII index has demonstrated its effectiveness as a prognostic tool for various inflammation-related diseases, encompassing cancer, inflammatory bowel disease, severe infections, and CVD.18–22 Although SII index has been studied in various contexts, there is limited evidence on the predictive value of SII specifically for cardiovascular and all-cause mortality in postmenopausal women, and whether extremely high levels of SII represent an independent risk factor compared to lower levels remains inadequately explored. Our study aims to address these gaps by investigating the association between SII and mortality outcomes in this specific population.
Postmenopausal women undergo significant hormonal shifts, primarily driven by a decline in estrogen levels, which results in physiological changes distinct from those observed in premenopausal women and men.23 Estrogen is known to play a pivotal role in regulating inflammation, lipid metabolism, and glucose homeostasis.24 Following menopause, the reduction in estrogen is associated with heightened systemic inflammation, as indicated by increased levels of markers such as C-reactive protein and the SII Index. This inflammatory burden contributes to an elevated risk of metabolic comorbidities, including obesity, metabolic syndrome, hypertension, diabetes, and CVD.25 The loss of estrogen’s cardioprotective effects further amplifies the susceptibility of postmenopausal women to cardiovascular conditions compared to their premenopausal counterparts.26 These factors collectively position postmenopausal women as a high-risk population, underscoring the need to investigate systemic inflammation and its health implications in this group. Recent studies have underscored the critical role of systemic inflammation in the pathogenesis of cardiovascular disease among postmenopausal women.27 Experts in the field have highlighted the urgent need for reliable prognostic markers to assess mortality risk in this vulnerable population.28 The SII has emerged as a promising tool for evaluating inflammatory status across various diseases, though its specific application in postmenopausal women remains underexplored.29
Therefore, this study aimed to investigate the association between SII levels and all-cause and CVD mortality in postmenopausal women, utilizing a US nationally representative cohort. The findings have the potential to extend the clinical value of the SII index and improve survival outcomes in the targeted populations.
Methods
Study Population
This study utilized data obtained from the National Health and Nutrition Examination Survey (NHANES), a comprehensive program administered by the Centers for Disease Control and Prevention (CDC) and the National Centers for Health Statistics (NCHS) in the United States. The NHANES survey aims to assess the health and nutritional status of the American population, adhering to the STROBE guidelines for documenting observational studies. Excluding individuals with incomplete data, the study population consisted of 1882 postmenopausal women and who participated in NHANES between 1999–2018. We utilized data from the NHANES cohort, which is a US nationally representative survey. From the total cohort, we only included postmenopausal women, which comprised 13.6% of the overall sample. Women were excluded if they were premenopausal, had incomplete data on menopausal status, or lacked other critical variables for analysis. Despite this selection, the study sample is still largely representative of postmenopausal women in the US, as the sampling weights provided by NHANES were applied to account for the complex survey design, ensuring generalizability to the broader population. The selection process of the study population is presented in Figure 1.
 |
Figure 1 Flow chart of study participants. Abbreviations: CVD, cardiovascular disease; NEUT, neutrophils; LYMPH, lymphocytes; PLT, platelets. |
Ethical Considerations
The NHANES protocol was approved by the National Center for Health Statistics Research Ethics Review Board, and all participants provided written informed consent. Our clinical study also received ethics approval from the Jiangxi Maternal and Child Health Hospital Ethics Committee (Approval No. EC-KY-202346).
Menopausal Status Definitions
Menopausal status was assessed using a self-reported reproductive health questionnaire. Women were considered postmenopausal if they reported not having had a menstrual period in the past 12 months and indicated either “hysterectomy” or “menopause/changes of life” as the reason. To minimize this potential bias, we excluded participants with incomplete or ambiguous responses regarding their menstrual history. Additionally, we employed the age criterion as a secondary check, verifying that participants were within the typical age range for menopause. The detailed questionnaire is available on the National Reproductive Health and Reproductive Health Action Plan website.30
Calculation of Systemic Immune-Inflammation Index
The complete blood count (CBC) was conducted in NHANES using the Coulter® DxH 800 analyzer and overseen by trained NHANES staff. Typically, the CBC includes measurements of red blood cell, white blood cell (WBC), and platelet (PLT). The SII is a calculated index that combines peripheral blood cell counts, specifically lymphocytes (LYMPH), neutrophils (NEUT), and PLTs, to assess the systemic immune and inflammatory response.29 The formula to calculate SII is as follows: SII = (Platelet count × Neutrophil count) / Lymphocyte count.
Mortality Ascertainment and Follow-up Calculation
This study utilized death data obtained from the death certificate records of the National Death Index, which were provided by the NCHS. The mortality files associated with these records were updated until December 31, 2019. Causes of death were determined using the International Classification of Diseases, 10th revision (ICD-10) codes. All-cause mortality encompassed deaths from cancer (C00-C97), CVD (I00-I09, I11, I13, I20-I51), cerebrovascular disease (I60-I69), respiratory disease (J10-J18, J40-J47), and other causes.
The follow-up time was calculated from the baseline assessment (start date) to either the occurrence of death (event) or the end of the study period (censoring date). Start Date: The start date was defined as the date of the initial NHANES interview and health assessment when the SII levels were measured. End Date: The end date was either the date of death (as determined by linkage to the National Death Index) or December 31, 2019, which was the cutoff for the most recent mortality data available. If a participant did not experience the event (death), they were censored at the end date of follow-up.
Ascertainment of Covariates
The study incorporated multiple covariates, comprising demographic information, medical history, and laboratory tests. The study collected demographic data through self-report NHANES questionnaires, which included essential variables such as age, racial/ethnic background (categorized as non-Hispanic White, Hispanic, non-Hispanic Black, or other), marital status, educational attainment, smoking and drinking habits. The calculation of the body mass index (BMI) involves dividing a person’s weight by the square of their height. The study utilized self-reported data to determine the physician-diagnosed conditions such as hypertension, diabetes, coronary heart disease, and heart failure, as well as the usage of glucose-lowering drugs, lipid-lowering drugs, and antihypertensive drugs. The levels of FBG were determined via a comprehensive analysis of blood samples. HbA1c levels were determined by analyzing whole blood samples using a Primus automated HPLC system (Primus I, CLC330 model). Blood lipids levels were were measured by analyzing fasting venous blood samples with a Hitachi 704 analyzer. Hemoglobin concentrations were determined by analyzing whole blood using a five-part differential complete blood count (Beckman Coulter MAXM analyzer). The measurement of C-reactive protein (CRP) is conducted using high-sensitivity assays performed on the Behring Nephelometer System. The eGFR was calculated using the simplified Modification of Diet in Renal Disease (MDRD) formula.31
Statistical Analysis
Data were analyzed using R version 4.0.2 and IBM SPSS version 23, accounting for NHANES’ complex survey design. The systemic immune-inflammation index (SII) was log-transformed due to its skewed distribution. Multivariable Cox proportional hazards models were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) for the association between SII quartiles and mortality outcomes, adjusting for confounders selected based on clinical relevance and univariate significance. The proportional hazards assumption was verified using Schoenfeld residuals. Kaplan-Meier curves were generated to visualize survival differences across SII quartiles, and restricted cubic splines were employed to assess linearity. Predictive performance was evaluated using C-statistics, integrated discrimination improvement (IDI), and net reclassification improvement (NRI). A two-tailed P-value <0.05 was considered statistically significant.
Results
A total of 18, 82 postmenopausal women with completed data were selected for analysis in this study. The weighted mean age of the participants was 69.7 ± 9.9 years. Among the participants, the median SII index was 486.5. When compared to the low SII group (Q1), those with extremely high SII levels (Q4) were older, and exhibited a higher proportion of non-Hispanic Whites, higher rates of heart failure, elevated levels of glucose, AST, NEUT, PLT, and CRP, as well as lower levels of HB, and LYMPH (P < 0.05) (Table 1).
 |
Table 1 Baseline Characteristics According to Quartiles of SII Levelsa |
During a median follow-up period of 8 years, 13.5% individuals died from any cause, and 4% individuals died specifically from CVD. The incidence of all-cause mortality in the Q1, Q2, Q3, and Q4 groups was 11.4%, 11.5%, 12.2%, and 19%, respectively, with a progressive increase observed across these groups (see Figure 2A, P for trend < 0.001). Similarly, the incidence of CVD mortality in the Q1, Q2, Q3, and Q4 groups was 3.2%, 3.4%, 3.7%, and 5.3%, respectively, demonstrating an upward trend across the four groups (refer to Figure 2B, P for trend < 0.001).
 |
Figure 2 The incidence of all-cause mortality (A) and CVD mortality (B) among the four groups. |
The SII index was transformed into its natural logarithm to create a continuous variable, revealing a non-linear association between the SII index and the risk of all-cause mortality (Figure 3A, P < 0.001 for nonlinearity). Table 2 presents a 22% increase in the risk of all-cause mortality per unit increase in the natural logarithm of the SII index (HR, 1.22; 95% CI, 1.14–1.29). After dividing the SII into quartiles and fully adjusting for confounders, it was found that patients in the Q4 group had a higher risk of all-cause mortality compared to those in the Q1 group (HR, 1.28; 95% CI, 1.16–1.41).
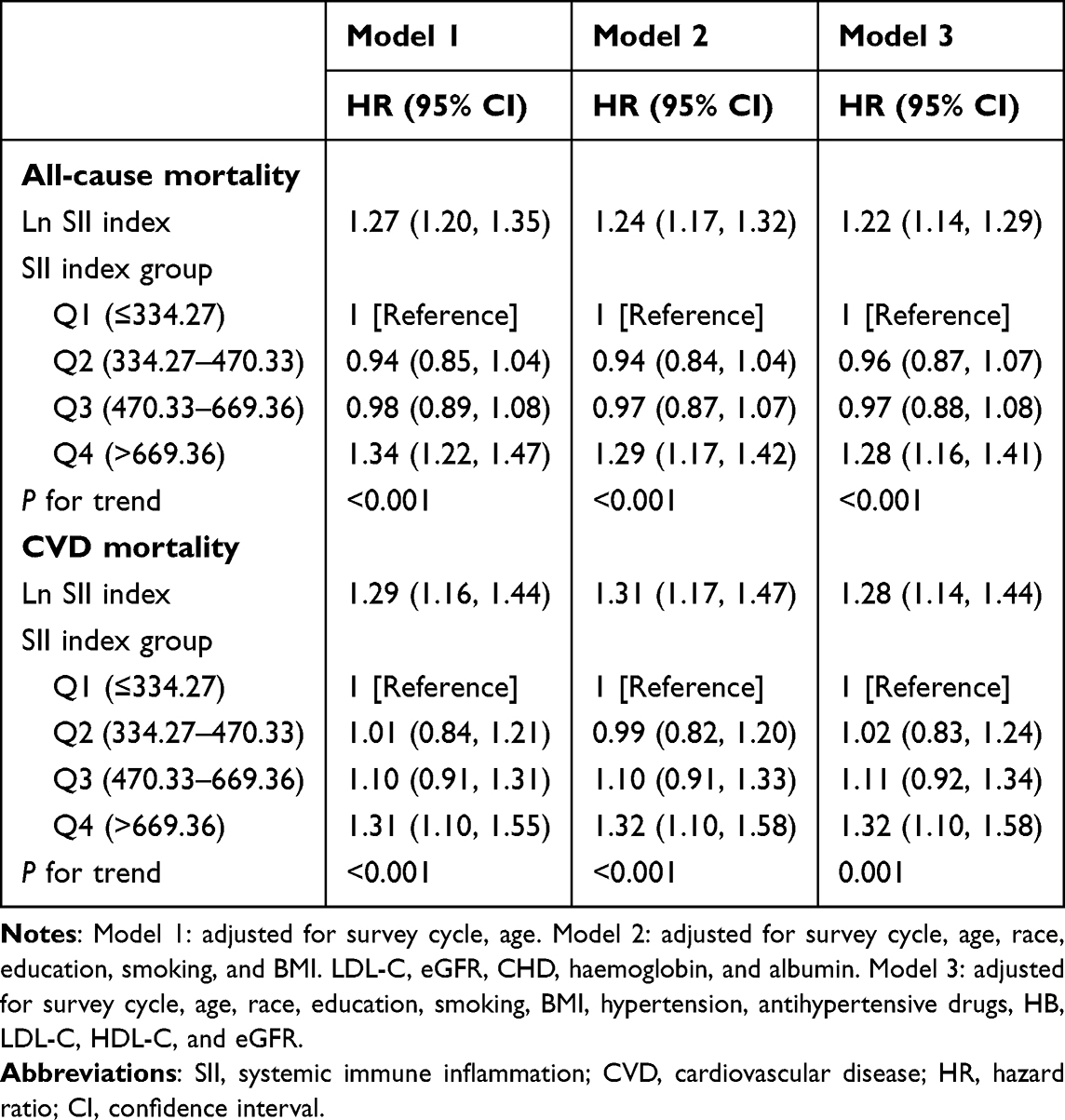 |
Table 2 Multivariable Cox Regression Analysis of the Association Between SII Levels and All-Cause and CVD Mortality |
 |
Figure 3 Restricted spline curve for the association between SII with all-cause (A) and CVD mortality (B). Adjusted for survey cycle, age, race, education, smoking, BMI, hypertension, antihypertensive drugs, HB, LDL-C, HDL-C, and eGFR. |
Table 2 demonstrates that elevated SII levels were associated with an increased risk of CVD mortality (HR, 1.28; 95% CI, 1.14–1.44). Likewise, the SII index was categorized into four quartiles, and individuals in Q4 exhibited the highest risk of CVD mortality (HR, 1.32; 95% CI, 1.10–1.58) when compared to the other groups. However, a linear relationship was found between SII and the risk of CVD mortality (Figure 3B, P = 0.126 for nonlinearity). Figure 4A illustrates the cumulative risk of all-cause mortality among the Q1, Q2, Q3, and Q4 groups, w ith the Q4 group exhibiting a significantly higher mortality risk compared to the other groups (Log-rank P < 0.001). The Kaplan-Meier curve indicated a comparable risk of CVD mortality in Q1, Q2, and Q3 groups, while the Q4 group exhibited a significantly higher risk of CVD mortality (Figure 4B, Log-rank P < 0.001).
 |
Figure 4 Kaplan-Meier curves according to quartiles of SII levels. Cumulative hazard of all-cause mortality for quartiles of SII (A), cumulative hazard of CVD mortality (B). |
Incremental Predictive Values of the SII Index
Table 3 presents the impact of incorporating SII alongside traditional risk factors on the predictive power for all-cause mortality and CVD mortality. SII was introduced as a continuous variable, and it was natural log-transformed (ln-transformed) to address its skewed distribution. The C-statistic for all-cause mortality increased from 0.811 (95% CI: 0.789–0.833) to 0.815 (95% CI: 0.792–0.837) after adding SII to the model, with a p-value of 0.21, indicating that the change was not statistically significant. Similarly, for CVD mortality, the C-statistic increased from 0.841 (95% CI: 0.812–0.870) to 0.845 (95% CI: 0.816–0.874), with a p-value of 0.27, suggesting no significant improvement in discrimination. Furthermore, the IDI and NRI values for all-cause mortality were 0.4% and 2.7%, for CVD mortality were 0.2% and −0.3%, respectively.
 |
Table 3 Improvements in Discrimination and Calibration for Mortality Risk Prediction by Adding SII to Traditional Risk Factors |
Discussion
The prospective cohort analysis using linked mortality data from NHANES to investigate the specific relationship between SII levels and all-cause and CVD mortality in postmenopausal women. The main findings of this study are as follows: 1) Although the incidence of death was similar across low, medium, and high SII levels, patients with extremely high SII levels experienced significantly higher rates of all-cause and CVD mortality. 2) SII levels exhibited a nonlinear association with all-cause mortality but showed a positive association with CVD mortality. 3) Increased risks of all-cause and CVD mortality were observed exclusively at extremely high SII levels. 4) The addition of SII to traditional risk factors did not significantly improve mortality risk prediction for either all-cause or CVD mortality, as indicated by the lack of significant change in C-statistics and other model performance metrics.
Previous studies have linked elevated SII with poorer survival in cancer populations, showing its association with increased all-cause mortality in gastric,32 urinary,33 and breast cancer patients.34 However, recent research highlights the importance of SII in non-cancer populations as well. In some NHANES-based studies, higher SII levels were significantly associated with increased all-cause mortality and CVD mortality in individuals with hyperuricemia,35 chronic kidney disease,36 diabetes,37 and rheumatoid arthritis.38 However, there is a paucity of research exploring the relationship between SII and mortality risk in postmenopausal women. Additionally, most prior studies used binary analyses to compare high vs low SII levels, rather than exploring a more detailed categorization of SII. Our study adds to the literature by examining SII across quartiles, which provides a more nuanced understanding of its relationship with mortality, particularly in postmenopausal women-a group uniquely at risk due to the effects of estrogen decline on inflammation and cardiovascular health. Our study found that extremely high SII levels are significantly associated with increased risks of all-cause mortality and cardiovascular mortality in postmenopausal women. This finding aligns with previous research, such as Yang et al reported a correlation between elevated SII levels and adverse outcomes in patients with coronary artery disease.18 Additionally, Zhong et al demonstrated in a systematic review of solid tumor patients that SII serves as a critical prognostic indicator.19 These studies reinforce the clinical utility of SII as a comprehensive tool for assessing inflammation and immune status, particularly in high-risk populations.
Postmenopausal women experience significant hormonal changes, primarily characterized by a reduction in estrogen levels, which contributes to several distinct physiological differences compared to the general population, including premenopausal women and men.23 Estrogen plays an essential role in modulating inflammation, lipid metabolism, and glucose homeostasis.24 Following menopause, the reduction in estrogen leads to increased systemic inflammation, as evidenced by elevated markers such as C-reactive protein and the SII index. Consequently, postmenopausal women generally have higher levels of systemic inflammation compared to their premenopausal counterparts and other populations. In addition, postmenopausal women are at an increased risk of developing metabolic comorbidities, including obesity, metabolic syndrome, hypertension, diabetes, and CVD.25 This elevated risk is largely attributable to changes in body composition, insulin resistance, and increased inflammatory response following menopause. The loss of estrogen’s cardioprotective effects also places postmenopausal women at a higher risk for cardiovascular conditions compared to premenopausal women.26 These factors collectively make postmenopausal women a particularly vulnerable group, underscoring the importance of studying systemic inflammation and its implications for health outcomes in this population.
In our analysis, we observed a non-linear relationship between SII levels and all-cause mortality. Specifically, while moderately elevated SII levels did not significantly increase mortality risk, individuals with extremely high SII levels experienced a marked rise in all-cause mortality. This non-linear association suggests that inflammation, as represented by SII, may need to surpass a certain threshold before significantly impacting overall mortality risk. In other words, a mild to moderate increase in inflammation might not be sufficient to substantially worsen health outcomes, whereas extremely high inflammation could trigger detrimental processes that lead to increased mortality. For CVD mortality, the association was positive and linear, indicating that increasing SII levels are directly associated with higher CVD mortality risk without a clear threshold effect. This finding suggests that inflammation has a more consistent impact on cardiovascular outcomes, possibly due to its role in the development and progression of atherosclerosis and other cardiovascular pathologies.27
Of note, we observed that the IDI for CVD mortality was 0.2%, whereas the NRI was −0.3%, indicating a slight negative impact on the reclassification of individuals’ CVD mortality risk when adding SII to the model. This finding suggests that incorporating SII alongside traditional risk factors may have led to some misclassification, thereby limiting its utility as an independent prognostic marker for CVD mortality in this population. It is possible that, while SII captures aspects of systemic inflammation, it may not adequately differentiate risk levels for CVD mortality, particularly in postmenopausal women with diverse cardiovascular risk profiles. This result emphasizes the need for further research to validate the prognostic value of SII and to explore whether additional markers or refined risk models might better classify CVD risk. Moreover, it underscores the importance of using SII as part of a more comprehensive risk assessment rather than relying on it as a standalone marker for CVD mortality.
The observation in our study can be attributed to several factors. This persistent inflammatory state can contribute to endothelial dysfunction, oxidative stress, and IR, all of which are associated with an increased risk of cardiovascular events and mortality.39 The presence of extremely high SII levels may further exacerbate the inflammatory process and accelerate the progression of atherosclerosis, leading to an increased risk of cardiovascular events and mortality.40,41 Increased levels of circulating pro-inflammatory cytokines and chemokines can promote platelet aggregation and thrombus formation, potentially leading to cardiovascular events, such as myocardial infarction or stroke.42 Persistent systemic inflammation, indicated by extremely high SII levels, can further impair glucose control in diabetic individuals. Inflammatory cytokines can disrupt insulin signaling pathways, leading to IR and poor glycemic control.43 This, in turn, can increase the risk of cardiovascular events and mortality. Chronic systemic inflammation, driven by extremely high SII levels, may contribute to multi-organ damage and dysfunction in diabetic individuals.44 Inflammation-mediated damage to vital organs, including the heart, kidneys, and blood vessels, can contribute to increased mortality risk.45 The cumulative effect of inflammation on multiple organ systems may exacerbate the overall disease burden and increase the risk of adverse outcomes.
The SII was calculated from platelet, neutrophil, and lymphocyte counts, reflects the body’s inflammatory and immune status. Inflammation plays a pivotal role in the development and progression of cardiovascular diseases.27 In postmenopausal women, the decline in estrogen levels heightens inflammatory responses, as evidenced by elevated markers such as C-reactive protein and SII.46,47 Estrogen modulates inflammation by inhibiting signaling pathways such as NF-κB and MAPK.24 Consequently, the loss of estrogen post-menopause may exacerbate inflammation via these pathways, increasing the risk of cardiovascular events and mortality. Moreover, extremely high SII levels may elevate mortality risk by promoting atherosclerosis, thrombosis, and endothelial dysfunction.40,41 For instance, interactions between neutrophils and platelets during inflammation facilitate thrombus formation and vascular damage.42 In postmenopausal women, inflammation is further linked to heightened risks of insulin resistance and metabolic syndrome, amplifying the burden of cardiovascular disease.43,44
Additionally, we found that incorporating SII into models alongside traditional risk factors (such as age, BMI, diabete, etc) slightly improved the predictive ability for both all-cause and CVD mortality, as reflected by a small increase in the C-statistic for both outcomes (from 0.811 to 0.815 for all-cause mortality, and from 0.841 to 0.845 for CVD mortality). The IDI further demonstrated modest gains in risk prediction when SII was added to the models. These findings suggest that while the SII can enhance mortality risk prediction beyond traditional factors, its additive value remains limited. One possible explanation is that traditional risk factors, such as age and pre-existing cardiovascular conditions, may already capture much of the risk in postmenopausal women, leaving limited room for additional improvements from inflammatory markers like SII.28 However, the association between extremely high SII levels and increased mortality risk suggests that SII could be useful for identifying a high-risk subset of patients who may not be fully captured by traditional risk factors alone. Further research is needed to explore whether SII could be integrated into clinical practice for more precise risk stratification, especially in populations with elevated inflammatory responses.
Although our results offer valuable insights, it is crucial to acknowledge various limitations when interpreting the findings. Firstly, although NHANES is a nationally representative cohort for the US, it may not fully capture the broader global population of postmenopausal women, especially those from different ethnic and socioeconomic backgrounds. Second, the measurement and calculation of SII may exhibit variations across studies, potentially leading to inconsistencies and impeding comparability among diverse research findings. Third, while SII serves as a convenient and accessible biomarker for systemic inflammation, it is limited in its scope as it only considers three blood components. To better understand the immune response and inflammation in postmenopausal women, additional biomarkers could be incorporated, including C-reactive protein,48 interleukin-6,49 tumor necrosis factor-alpha (TNF-α),50 and fibrinogen.51 Future studies may benefit from evaluating the combined prognostic value of SII alongside other inflammatory markers to improve risk stratification and prediction of adverse health outcomes. Fourth, this study may suffer from selection bias or attrition bias. Excluded participants or those lost to follow-up may exhibit distinct characteristics or experience varied health outcomes, thereby influencing the validity and generalizability of the findings. Fifth, We acknowledge that the levels of neutrophils and lymphocytes can indeed fluctuate over time due to acute conditions or temporary physiological changes. However, the SII, when measured in a stable, non-acute setting, can still provide valuable insights into an individual’s chronic inflammatory status.52 While a single SII measurement may not capture temporal fluctuations, it can serve as a useful proxy for chronic systemic inflammation, especially when measured in a non-acute phase. In our study, SII levels were measured during routine health assessments, which helped mitigate the effect of short-term variability and emphasized chronic inflammation. Finally, although our study considers known confounders during the analysis, it is important to recognize that complete elimination of residual confounding is not possible. These include dietary factors, physical activity, psychosocial stress, and hormone replacement therapy.53–56 Further research is warranted to enhance our understanding of the relationship between SII and mortality outcomes in this population. This should involve the implementation of randomized controlled trials and comprehensive studies that consider potential confounding factors.
Conclusion
In a sample of US postmenopausal women, a non-linear relationship existed between SII levels and the risk of all-cause mortality, as well as a positive association with the risk of CVD mortality. Significantly higher risks for all-cause and CVD mortality were observed only in individuals with extremely high SII levels. The identification of an increased mortality risk at extremely high SII levels highlights the potential for targeted therapeutic interventions to mitigate these adverse outcomes.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The NHANES protocol was approved by the National Center for Health Statistics Research Ethics Review Board, and all participants provided written informed consent. Additionally, our clinical study was reviewed and approved by the Ethics Committee of Jiangxi Maternal and Child Health Hospital (Approval No. EC-KY-202346).
Acknowledgments
The authors thank the participants of the NHANES databases.
Funding
No external funding received.
Disclosure
The authors declare no competing financial interests.
References
1. Pinkerton JV. Hormone therapy for postmenopausal women. N Engl J Med. 2020;382(5):446–455. doi:10.1056/NEJMcp1714787
2. Heer E, Harper A, Escandor N, Sung H, McCormack V, Fidler-Benaoudia MM. Global burden and trends in premenopausal and postmenopausal breast cancer: a population-based study. Lancet Glob Health. 2020;8(8):e1027–e1037. doi:10.1016/S2214-109X(20)30215-1
3. Lobo RA, Gompel A. Management of menopause: a view towards prevention. Lancet Diabetes Endocrinol. 2022;10(6):457–470. doi:10.1016/S2213-8587(21)00269-2
4. Hale GE, Burger H. Hormonal changes and biomarkers in late reproductive age, menopausal transition and menopause. Best Pract Res Clin Obstet Gynaecol. 2009;23(1):7–23. doi:10.1016/j.bpobgyn.2008.10.001
5. Van der Schouw Y. Incidence and mortality of cardiovascular disease in postmenopausal women world-wide and relevance for preventive strategies. Climacteric. 2009;12(sup1):1–5. doi:10.1080/13697130902896857
6. Iorga A, Cunningham CM, Moazeni S, Ruffenach G, Umar S, Eghbali M. The protective role of estrogen and estrogen receptors in cardiovascular disease and the controversial use of estrogen therapy. Biol Sex Differ. 2017;8:1–16. doi:10.1186/s13293-017-0152-8
7. Wong SK, Chin K-Y, Suhaimi FH, Ahmad F, Ima-Nirwana S. The relationship between metabolic syndrome and osteoporosis: a review. Nutrients. 2016;8(6):347. doi:10.3390/nu8060347
8. Ren J, Kelley RO. Cardiac health in women with metabolic syndrome: clinical aspects and pathophysiology. Obesity. 2009;17(6):1114–1123. doi:10.1038/oby.2009.8
9. Gaspard U. Hyperinsulinaemia, a key factor of the metabolic syndrome in postmenopausal women. Maturitas. 2009;62(4):362–365. doi:10.1016/j.maturitas.2008.11.026
10. Xiao S, Wang X, Zhang G, et al. Association of systemic immune inflammation index with estimated pulse wave velocity, atherogenic index of plasma, triglyceride-glucose index, and cardiovascular disease: a large cross-sectional study. Mediators Inflamm. 2023;2023:1966680. doi:10.1155/2023/1966680
11. Nie Y, Zhou H, Wang J, Kan H. Association between systemic immune-inflammation index and diabetes: a population-based study from the NHANES. Front Endocrinol. 2023;14:1245199. doi:10.3389/fendo.2023.1245199
12. Nøst TH, Alcala K, Urbarova I, et al. Systemic inflammation markers and cancer incidence in the UK Biobank. Eur J Epidemiol. 2021;36(8):841–848. doi:10.1007/s10654-021-00752-6
13. McCullough LE, Miller EE, Calderwood LE, et al. Maternal inflammatory diet and adverse pregnancy outcomes: circulating cytokines and genomic imprinting as potential regulators? Epigenetics. 2017;12(8):688–697. doi:10.1080/15592294.2017.1347241
14. Chen X, Zhang M, Zhou N, Zhou W, Qi H. Associations between genetically predicted concentrations of circulating inflammatory cytokines and the risk of ten pregnancy-related adverse outcomes: a two-sample Mendelian randomization study. Cytokine. 2024;180:156661. doi:10.1016/j.cyto.2024.156661
15. Zhao Y, Shao W, Zhu Q, et al. Association between systemic immune-inflammation index and metabolic syndrome and its components: results from the National Health and Nutrition Examination Survey 2011–2016. J Transl Med. 2023;21(1):691. doi:10.1186/s12967-023-04491-y
16. Scherlinger M, Richez C, Tsokos GC, Boilard E, Blanco P. The role of platelets in immune-mediated inflammatory diseases. Nat Rev Immunol. 2023;23(8):495–510. doi:10.1038/s41577-023-00834-4
17. Buonacera A, Stancanelli B, Colaci M, Malatino L. Neutrophil to lymphocyte ratio: an emerging marker of the relationships between the immune system and diseases. Int J Mol Sci. 2022;23(7):3636. doi:10.3390/ijms23073636
18. Yang YL, Wu CH, Hsu PF, et al. Systemic immune‐inflammation index (SII) predicted clinical outcome in patients with coronary artery disease. Eur J Clin Invest. 2020;50(5):e13230. doi:10.1111/eci.13230
19. Zhong J-H, Huang D-H, Chen Z-Y. Prognostic role of systemic immune-inflammation index in solid tumors: a systematic review and meta-analysis. Oncotarget. 2017;8(43):75381. doi:10.18632/oncotarget.18856
20. Ye Z, Hu T, Wang J, et al. Systemic immune-inflammation index as a potential biomarker of cardiovascular diseases: a systematic review and meta-analysis. Front cardiovasc med. 2022;9:933913. doi:10.3389/fcvm.2022.933913
21. Kocaaslan R, Dilli D, Çitli R. Diagnostic value of the systemic immune-inflammation index in newborns with urinary tract infection. Am J Perinatol. 2022;41(S 01):e719–e727. doi:10.1055/s-0042-1757353
22. Zhang Z, Chen Z. Higher systemic immune-inflammation index is associated with higher likelihood of peripheral arterial disease. Ann Vasc Surg. 2022;84:322–326. doi:10.1016/j.avsg.2021.12.011
23. Monteleone P, Mascagni G, Giannini A, Genazzani AR, Simoncini T. Symptoms of menopause—global prevalence, physiology and implications. Nat Rev Endocrinol. 2018;14(4):199–215. doi:10.1038/nrendo.2017.180
24. Straub RH. The complex role of estrogens in inflammation. Endocr Rev. 2007;28(5):521–574. doi:10.1210/er.2007-0001
25. Sinatora RV, Chagas EFB, Mattera FOP, et al. Relationship of inflammatory markers and metabolic syndrome in postmenopausal women. Metabolites. 2022;12(1):73. doi:10.3390/metabo12010073
26. Pérez-López FR, Chedraui P, Gilbert JJ, Pérez-Roncero G. Cardiovascular risk in menopausal women and prevalent related co-morbid conditions: facing the post-Women’s Health Initiative era. Fertil Sterility. 2009;92(4):1171–1186. doi:10.1016/j.fertnstert.2009.06.032
27. Raggi P, Genest J, Giles JT, et al. Role of inflammation in the pathogenesis of atherosclerosis and therapeutic interventions. Atherosclerosis. 2018;276:98–108. doi:10.1016/j.atherosclerosis.2018.07.014
28. De Kat A, Dam V, Onland-Moret N, Eijkemans M, Broekmans F, Van Der Schouw Y. Unraveling the associations of age and menopause with cardiovascular risk factors in a large population-based study. BMC Med. 2017;15:1–11. doi:10.1186/s12916-016-0759-3
29. Hu B, Yang X-R, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
30. Tang Y, Peng B, Liu J, Liu Z, Xia Y, Geng B. Systemic immune-inflammation index and bone mineral density in postmenopausal women: a cross-sectional study of the national health and nutrition examination survey (NHANES) 2007–2018. Front Immunol. 2022;13:975400. doi:10.3389/fimmu.2022.975400
31. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D; Group* MoDiRDS. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Ann Internal Med. 1999;130(6):461–470. doi:10.7326/0003-4819-130-6-199903160-00002
32. Wang K, Diao F, Ye Z, et al. Prognostic value of systemic immune-inflammation index in patients with gastric cancer. Chin J Cancer. 2017;36(1):75. doi:10.1186/s40880-017-0243-2
33. Huang Y, Gao Y, Wu Y, Lin H. Prognostic value of systemic immune-inflammation index in patients with urologic cancers: a meta-analysis. Cancer Cell Int. 2020;20:499. doi:10.1186/s12935-020-01590-4
34. Zhang Y, Sun Y, Zhang Q. Prognostic value of the systemic immune-inflammation index in patients with breast cancer: a meta-analysis. Cancer Cell Int. 2020;20:224. doi:10.1186/s12935-020-01308-6
35. Ren T, Zhou E, Wu J, Wang C, Yin Y. Systemic inflammation markers independently associated with increased mortality in individuals with hyperuricemia: results from the NHANES prospective cohort study. Immun Inflamm Dis. 2024;12(10):e70032. doi:10.1002/iid3.70032
36. Jia M, Yuan W, Chen Y, Wang Y, Shang L, Han S. Systemic immune inflammation index and all-cause mortality in chronic kidney disease: a prospective cohort study. Immun Inflamm Dis. 2024;12(9):e1358. doi:10.1002/iid3.1358
37. Chen X, Li A, Ma Q. Neutrophil-lymphocyte ratio and systemic immune-inflammation index as predictors of cardiovascular risk and mortality in prediabetes and diabetes: a population-based study. Inflammopharmacology. 2024;32(5):3213–3227.
38. Wang W, Yao W, Tang W, Li Y, Lv Q, Ding W. Nonlinear associations of systemic immune-inflammation index with all-cause and cardiovascular mortality in US adults with rheumatoid arthritis. Sci Rep. 2024;14(1):16639. doi:10.1038/s41598-024-67750-y
39. Cachofeiro V, Goicochea M, De Vinuesa SG, Oubiña P, Lahera V, Luño J. Oxidative stress and inflammation, a link between chronic kidney disease and cardiovascular disease: new strategies to prevent cardiovascular risk in chronic kidney disease. Kidney Int. 2008;74:S4–S9. doi:10.1038/ki.2008.516
40. D’Souza A, Hussain M, Howarth FC, Woods NM, Bidasee K, Singh J. Pathogenesis and pathophysiology of accelerated atherosclerosis in the diabetic heart. Mol Cell Biochem. 2009;331:89–116. doi:10.1007/s11010-009-0148-8
41. Gisterå A, Hansson GK. The immunology of atherosclerosis. Nat Rev Nephrol. 2017;13(6):368–380. doi:10.1038/nrneph.2017.51
42. Stark K, Massberg S. Interplay between inflammation and thrombosis in cardiovascular pathology. Nat Rev Cardiol. 2021;18(9):666–682. doi:10.1038/s41569-021-00552-1
43. Tilg H, Moschen AR. Inflammatory mechanisms in the regulation of insulin resistance. Mol Med. 2008;14:222–231. doi:10.2119/2007-00119.Tilg
44. Ruscitti P, Di Cola I, Di Muzio C, et al. Expanding the spectrum of the hyperferritinemic syndrome, from pathogenic mechanisms to clinical observations, and therapeutic implications. Autoimmunity Rev. 2022;21(7):103114. doi:10.1016/j.autrev.2022.103114
45. Saha S, Mahalanobish S, Dutta S, Sil PC. Mangiferin ameliorates collateral neuropathy in t BHP induced apoptotic nephropathy by inflammation mediated kidney to brain crosstalk. Food Funct. 2019;10(9):5981–5999. doi:10.1039/C9FO00329K
46. Gameiro CM, Romão F, Castelo-Branco C. Menopause and aging: changes in the immune system—a review. Maturitas. 2010;67(4):316–320. doi:10.1016/j.maturitas.2010.08.003
47. Ghosh M, Rodriguez-Garcia M, Wira CR. The immune system in menopause: pros and cons of hormone therapy. J Steroid Biochem Mol Biol. 2014;142:171–175. doi:10.1016/j.jsbmb.2013.09.003
48. Sproston NR, Ashworth JJ. Role of C-reactive protein at sites of inflammation and infection. Front Immunol. 2018;9:754. doi:10.3389/fimmu.2018.00754
49. Gabay C. Interleukin-6 and chronic inflammation. Arthritis Res Therapy. 2006;8:1–6. doi:10.1186/ar1917
50. Sinagra E, Perricone G, Romano C, Cottone M. Heart failure and anti tumor necrosis factor-alpha in systemic chronic inflammatory diseases. Eur J Internal Med. 2013;24(5):385–392. doi:10.1016/j.ejim.2012.12.015
51. Davalos D, Akassoglou K. Fibrinogen as a key regulator of inflammation in disease. In: Seminars in Immunopathology. Springer; 2012:43–62.
52. Huang Y-W, Yin X-S, Li Z-P. Association of the systemic immune-inflammation index (SII) and clinical outcomes in patients with stroke: a systematic review and meta-analysis. Front Immunol. 2022;13:1090305. doi:10.3389/fimmu.2022.1090305
53. Hart MJ, Torres SJ, McNaughton SA, Milte CM. Dietary patterns and associations with biomarkers of inflammation in adults: a systematic review of observational studies. Nutr J. 2021;20:1–14. doi:10.1186/s12937-021-00674-9
54. Hamer M, Stamatakis E. Physical activity and risk of cardiovascular disease events: inflammatory and metabolic mechanisms. Med Sci Sports Exercise. 2009;41(6):1206–1211. doi:10.1249/MSS.0b013e3181971247
55. Rohleder N. Stimulation of systemic low-grade inflammation by psychosocial stress. Psychosomatic Med. 2014;76(3):181–189. doi:10.1097/PSY.0000000000000049
56. Miller AP, Chen Y-F, Xing D, Feng W, Oparil S. Hormone replacement therapy and inflammation: interactions in cardiovascular disease. Hypertension. 2003;42(4):657–663. doi:10.1161/01.HYP.0000085560.02979.0C
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of Elevated Thyroid Stimulating Hormone with Atherosclerotic Cardiovascular Disease and Its Mortality in Elderly Community-Dwelling Chinese
Wang Y, Liu C, Liu L, Chen X, Wei L, Liu J, Peng S, Pi J, Zhang Q, Tomlinson B, Chan P, Zhang L, Fan H, Zheng L, Liu Z, Zhang Y
Clinical Interventions in Aging 2022, 17:1139-1150
Published Date: 2 August 2022
The Relationship Between the Neutrophil Percentage-to-Albumin Ratio and Rates of 28-Day Mortality in Atrial Fibrillation Patients 80 Years of Age or Older
Cai J, Li M, Wang W, Luo R, Zhang Z, Liu H
Journal of Inflammation Research 2023, 16:1629-1638
Published Date: 17 April 2023
The Relationship Between Fracture and Mortality in a Chinese Maintenance Hemodialysis Patients Cohort
Liu X, Liu Z, Niu Y, Zhang K, Zhang X, Yu C
Journal of Multidisciplinary Healthcare 2024, 17:2031-2038
Published Date: 1 May 2024
Prevalence and Risk Factors of Cardiovascular Disease in Rheumatoid Arthritis Patients: A Comparative Analysis of Real-World Data
Tekeoglu S
International Journal of General Medicine 2024, 17:5859-5868
Published Date: 6 December 2024
Predictors of Clinical Stability and Mortality in COPD: A Longitudinal Study
Loo WTW, Chew SY, Tan JHY, Soh RY, Koh MS, Lapperre TS, Tiew PY
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:2311-2324
Published Date: 7 July 2025