")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Facilitator and Barrier to Health Information System Use from Health Professionals Perspective: A Scoping Review
Authors Yuliasih N, Khoiry QA , Alfian SD , Suwantika AA , Abdulah R
Received 1 January 2025
Accepted for publication 18 June 2025
Published 7 July 2025 Volume 2025:18 Pages 3901—3920
DOI https://doi.org/10.2147/JMDH.S515295
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Pavani Rangachari
Nur Yuliasih,1 Qisty A Khoiry,1 Sofa D Alfian,1– 3 Auliya A Suwantika,1– 3 Rizky Abdulah1,2
1Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jatinangor, Indonesia; 2Drug Utilization and Pharmacoepidemiology Research Group, Center of Excellence for Pharmaceutical Care Innovation, Universitas Padjadjaran, Jatinangor, Indonesia; 3Center for Health Technology Assessment, Universitas Padjadjaran, Jatinangor, Indonesia
Correspondence: Sofa D Alfian, Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jl. Raya Jatinangor, KM 21, Jatinangor, Sumedang, Indonesia, Tel/Fax +62-022-7796200, Email [email protected]
Objective: This study aimed to present factors that potentially influenced system use by identifying facilitator or barrier to acceptance from the perspective of healthcare professionals.
Methods: A scoping review was used in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines. The literature search was conducted on two electronic databases, Scopus and MEDLINE through PubMed, limiting the publication timeframe from January 2013 to December 2023. Moreover, a developed search strategy was used based on keywords and MeSH terms derived from the Population, Concept, and Context (PCC) components. The inclusion criteria were studies that discussed information system in healthcare, incorporated healthcare professionals who directly engaged with health information system (HIS), conducted within healthcare settings, identified facilitator or barrier to the use of information system in healthcare, and were available in full-text English. Barrier and facilitator were considered as factors impeding and promoting HIS use, respectively. The scoping review adopted a thematic analysis.
Results: The results showed that a total of 79 studies met the inclusion criteria and were included in this review. A total of 16 distinct facilitators and 16 barriers were identified, which were then grouped into four categories, comprising colleague and social support, organizational, individual, as well as technological and technical contexts. The most frequently mentioned facilitator was usefulness and simplification of daily tasks, while the predominant barrier was lack of technical support.
Conclusion: The systematic mapping of facilitator and barrier provided a foundation for policymakers and healthcare professionals in decision-making processes to enhance acceptance HIS.
Keywords: health information system, health professionals, facilitator, barrier, electronic health record
Introduction
Effective communication is significantly important in the present healthcare landscape, as inadequacy may lead to conflicts among healthcare providers.1 The implementation of health information system (HIS) enhances community welfare by improving quality health services, the performance of health professionals, and reducing potential treatment errors.2 Due to the intrinsic connection with communication processes, the effective use of HIS necessitates healthcare professionals communicating effectively through system, understanding updates and protocols, as well as providing feedback on experiences.3–5 In the past era of paper records, data has become difficult to interpret, illegible, lost, or incomplete, resulting in limited analysis and insights.6 HIS is a structured framework that integrates data collection, processing, and reporting to support decision-making, enhance service quality, ensure patient safety, control healthcare financing, improve the overall effectiveness and efficiency of health services.7–9 The digitization of healthcare data has significantly transformed the responsibilities and tasks of health professionals, leading to increased engagement in technical roles.10 In principle, good health services require the support of HIS infrastructure.11 Information system is a fundamental enabler of knowledge management for health services.12
Various types of HIS widely used in healthcare settings include Electronic Medical Record (EMR), Computerized Physician Order Electronic (CPOE), management, immunization information, institutional information, disease management, clinical documentation, and health information exchange networks.2,13 The benefits of these HIS, such as improved care coordination14 and enhanced decision-making,15 are heavily reliant on effective communication facilitated by systems and the communication surrounding use. However, practical use entails both benefits and challenges. The benefits comprise increased efficiency, improved care coordination, and enhanced decision-making.16,17 Previous systematic reviews showed that all seven quantitative studies focusing on process evaluation signified patient satisfaction with the use of digital health technology in pharmaceutical care delivered by pharmacists.18 It is important to acknowledge and tackle associated challenges, such as the privacy and security of patient data. Resistance to change among healthcare professionals can also hinder the use and integration of HIS technology into existing workflows.10,16
A comprehensive understanding of facilitator and barrier in HIS is essential. This provides benefits, such as enhancing clinical outcomes, streamlining care coordination, optimizing practice efficiencies, and effectively monitoring data over time.19 On the other hand, awareness of barrier allows organizations to proactively address and mitigate the factors. Digital health technology interventions have proved effective, but the impact on clinical outcomes varies, signifying the need for personalized feedback to ensure consistent and beneficial effects.20 Important factors affecting system acceptance by users include attitudes, behavioral control, transition costs, service coordination, information management, and the ability to track healthcare outcomes, all of which are facilitator.21 Meanwhile, financial issues, resistance to change, and IT problems during implementation were commonly mentioned as barrier to the use of Electronic Health Records (EHR) and Health Information Exchanges (HIE).22
Understanding the multifaceted challenges associated with HIS implementation is crucial for overall success. Although these challenges include significant barrier encountered by patients in adopting and effectively using systems, concerns regarding the privacy and security of health information,23 limitations in access to patient portals24 as well as other digital health interfaces, the perspectives of healthcare professionals are equally critical. Health professionals are the primary users and implementers of HIS in daily practice.25 Acceptance, effective use, and identification of facilitator and barrier directly impact the successful integration of HIS into clinical workflows,26,27 ultimately affecting patient care and safety.19,28
Barrier and facilitator related to HIS use, as well as the impact on the on-user engagement and satisfaction need to be discussed. Understanding the broader context in which the system is implemented is essential while developing strategies to overcome challenges. Previous systematic reviews have focused only on a single country,29 a specific region,30 or emphasized the exploration of acceptance theory.31 A review from the perspective of healthcare professionals regarding facilitator and barrier, without being limited to a specific region, is needed. In general, scoping reviews are designed to map key concepts and examine studies in an area to provide an overview of the extent and nature of the current literature.32–34 Therefore, this scoping review aimed to provide thematic summary information on facilitator or barrier to HIS use from the perspective of healthcare professionals, making the scoping review methodology well-suited to explore the available evidence without imposing strict inclusion criteria.
Method
The review follows the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines35 (Supplementary Material 1):
Information Sources and Search Strategy
The literature search for this scoping review was conducted on two electronic databases including Scopus, a comprehensive multidisciplinary database with scientific, technical, medical, and social sciences literature as well as MEDLINE through PubMed, a premier source for biomedical and health-related studies. These two databases were selected to provide broad and focused coverage of the relevant literature. To minimize potential bias in the search strategy, several steps were taken. Firstly, the PCC (Population, Concept, Context) framework was applied to define the scope of the search, ensuring that all relevant facets of the study question were considered. The participants (P) consisted of healthcare professionals including, but not limited to, physicians, nurses, pharmacists, and allied health staff, who use HIS. The concept (C) focused on facilitator and barrier affecting the adoption and use. The context (C) comprises various healthcare settings, including hospitals, clinics, community health centers, and other relevant environments where these systems are implemented.
Secondly, the search strategy was developed by translating the PCC components into relevant keywords and MeSH terms. For example, ‘healthcare professionals’ and related terms were used to represent the Population, ‘acceptance and barrier’ represented the Concept, while “hospital”, “clinic”, and ‘community health’ represented the Context, with ‘health information systems’ as the primary topic of focus.
Thirdly, the search terms were combined using Boolean operators (AND, OR) to refine the search and retrieve the most relevant studies. The combination strategies were carefully considered to capture the most relevant studies and minimize irrelevant studies. The full strategy using a combination of medical subject heading terms and text words is presented in Table 1. A scoping review methodology was selected due to the broad and heterogeneous nature of the study question. Given the wide range of HIS, technologies, and healthcare settings, a scoping review allowed effective mapping of the existing evidence and identifying key concepts, rather than focusing on a specific intervention or outcome, as in a systematic review. This approach was suitable for exploring the overall landscape of facilitator and barrier in the field.33
 |
Table 1 Literature Search Strategy |
Eligibility Criteria
To minimize potential bias in the selection of studies for this scoping review, clear and objective eligibility criteria were established in line with the PCC framework. The scoping review included original observational or experimental that met the following criteria:
- Healthcare professionals directly engaged with HIS, including but not limited to physicians, nurses, midwives, pharmacists. This criterion ensured that the perspectives and experiences captured are from individuals who directly interact with HIS in professional roles, providing relevant insights into facilitator and barrier.
- Focused on the assessment of HIS, defined as an integrated and interoperable system designed to manage healthcare data, including various functions namely collecting, storing, managing, and transmitting data of patients, operational management of hospitals, and supporting healthcare policy decision.36 This provides a clear and consistent definition of the core concept under investigation, ensuring that the included literature focuses on comprehensive HIS rather than isolated technologies or systems with limited functionality.
- Identify facilitator or barrier to HIS use by healthcare professionals.37 This criterion directly addresses the question of the scoping review, ensuring that the included studies provide data relevant to understanding the factors influencing HIS use.
- Studies conducted within healthcare setting (eg, hospitals, clinics, community health centers). This ensures that the results are relevant to real-world healthcare environments where HIS is implemented and used, enhancing the applicability of the review results to practice.
- Availability of full text in English. Limiting inclusion to English language studies allows for a comprehensive understanding and accurate synthesis of the evidence, mitigating potential misinterpretations due to translation limitations.
- Published between 2013 and 2023. This timeframe was selected to capture the contemporary landscape of HIS adoption and use. The starting year of 2013 was selected to focus on more recent developments and challenges in the field, considering the rapid evolution of health information technology in the past decade. The end year of 2023 ensures the inclusion of the most up-to-date studies available at the time of the search.
Exclusions criteria comprised:
- Studies lacking full-text availability. The exclusion of these studies ensures that a thorough assessment of the methodology and results can be conducted, as crucial information may be missing from abstracts or other limited-access formats.
- Conference proceedings, letters, editorials, commentaries, posters, reviews, and presentations. These publication types generally provide preliminary results, opinions, or summaries rather than in-depth analyses of original study. Focusing on original observational or experimental studies ensures a more robust and detailed evidence base for the scoping review.
- Studies focusing on mobile phone devices. While mobile health (mHealth) is relevant, the focus of this review is on integrated and interoperable HIS. Excluding studies solely on individual mobile phone applications helps to maintain the scope on more comprehensive healthcare data management systems.
Study Selection
Relevant studies identified through title and abstract screening were independently evaluated by two authors (NY, QAK). Subsequently, a thorough evaluation of the full-text versions was independently conducted against the eligibility criteria. This dual review further minimized the risk of selection bias by ensuring that the final inclusion of studies was based on a consistent and agreed-upon application of the criteria. In cases of disagreements that could not be resolved, the other three authors (SDA, AAS, and RA) were available to act as adjudicators. Consensus was adopted for final resolution in all cases of disagreement. This multi-reviewer approach with a clear mechanism for resolving conflicts reduced the potential for subjective bias in the final selection of studies.
Extraction and Management Data
The data extraction process was primarily undertaken by NY and QAK, while SDA checked and verified the data extraction process. This independent verification step further minimized the risk of extraction errors, ensuring the accuracy and completeness of the extracted data. Any discrepancies or doubts identified during this verification process were discussed and resolved through consensus among all three authors. Data were extracted using predefined extraction tables and manually recorded in Microsoft Excel 2010. The use of predefined tables ensured that all relevant data points were systematically collected across all included studies, reducing the potential for information bias due to inconsistent extraction. The characteristics of each extracted article included general information (author, year of publication, study location), objectives, type of HIS, methods (study design, population, sample size, data collection methods), key results (facilitator and barrier), and funding.
Data Analysis and Synthesis
Based on the heterogeneity of the data concerning population, type of HIS examined, and methodological approaches, a qualitative narrative synthesis was undertaken to address the broad study question of this scoping review. The primary method of data analysis included a thematic content analysis of the extracted facilitator and barrier to HIS adoption and use by two authors (NY and QAK) independently. In this process, each extracted facilitator and barrier was subjected to content analysis through the coding of relevant keywords. The process allowed for cross-verification of emerging themes and reduced the risk of individual bias influencing the categorization of results. Disagreements in coding or theme assignment were resolved through discussion and consensus among the two primary authors. Following the independent coding, the identified keywords were categorized into four themes based on previous studies.30,38 These categories provided facilitator and barrier of HIS for understanding the key contextual domains, including colleague and social context, organizational, individual, as well as technological and technical. Colleague and social context were defined as the role of co-workers and leaders who have a good understanding and knowledge of digital system in creating a shared awareness to motivate users toward increasing acceptance and intention to adopt technology in the workplace.39 Organizational context refers to readiness of policymakers in preparing infrastructure and resources (finance and human resources with the potential to master information technology).40 Individual context is defined as capacity in the implementation of system, including experience, age, attitudes and behavior towards technology, ability to be trained/learned, intention to use, perceptions, expectations of system, knowledge, and awareness of system/technology.41 Technological context of the study was described as the capacity and availability of information technology with technical support to increase acceptance and use of the system.17 Additionally, each facilitator and barrier was analyzed through the lens of the 2023 World Bank classification settings, annually updated by July 1 based on Gross National Income (GNI) per capita from the preceding calendar year.42 The specific GNI per capita thresholds for each income group served as crucial benchmarks. These include low-income country (LIC), lower middle-income country (LMIC), upper middle-income country (UMIC), and high-income country (HIC), with GNI per capita of $1135 or less in 2022, between $1136 to $4465, $4466 to $13,845, and $13,846 or more, respectively.
Quality Assessment
QAK conducted the evaluation of included studies to determine methodological quality assessment, with additional independent verification performed by SDA. Any discrepancies between the reviewers (QAK and SDA) were resolved through consensus. This step ensured that judgments were not solely reliant on a single individual interpretation, thereby reducing the risk of subjective bias. The quality assessment process for the included studies was based on the method adopted. Studies using qualitative method were assessed using JBI Critical Appraisal Checklist for Qualitative Research.43 Similarly, those that applied the cross-sectional method were subjected to the JBI Critical Appraisal Checklist for Cross-Sectional Research.44 Studies using mixed method were assessed using the Mixed Methods Appraisal Tool.45 These checklists incorporate specific criteria designed to evaluate various aspects of study quality, thereby minimizing bias arising from a lack of clear assessment criteria. Studies scoring higher than 70%, between 50% and 70%, and less than 50%, were categorized as high, medium quality, and low quality, respectively. The pre-defined categorization of quality scores (high, medium, and low) based on established thresholds provided a consistent and transparent approach to interpreting the assessment results, reducing potential bias in the overall quality rating of the included studies.
Result
Study Selection
The PRISMA flowchart showing the literature selection steps is presented in Figure 1. A comprehensive search across Scopus and MEDLINE through PubMeddatabases resulted in 676 references potentially meeting the inclusion criteria. Following a selection process, comprising duplicate removal as well as titles and abstracts evaluation, 148 studies were reviewed for full-text eligibility assessment. Finally, 79 that met the inclusion criteria were included in the review.
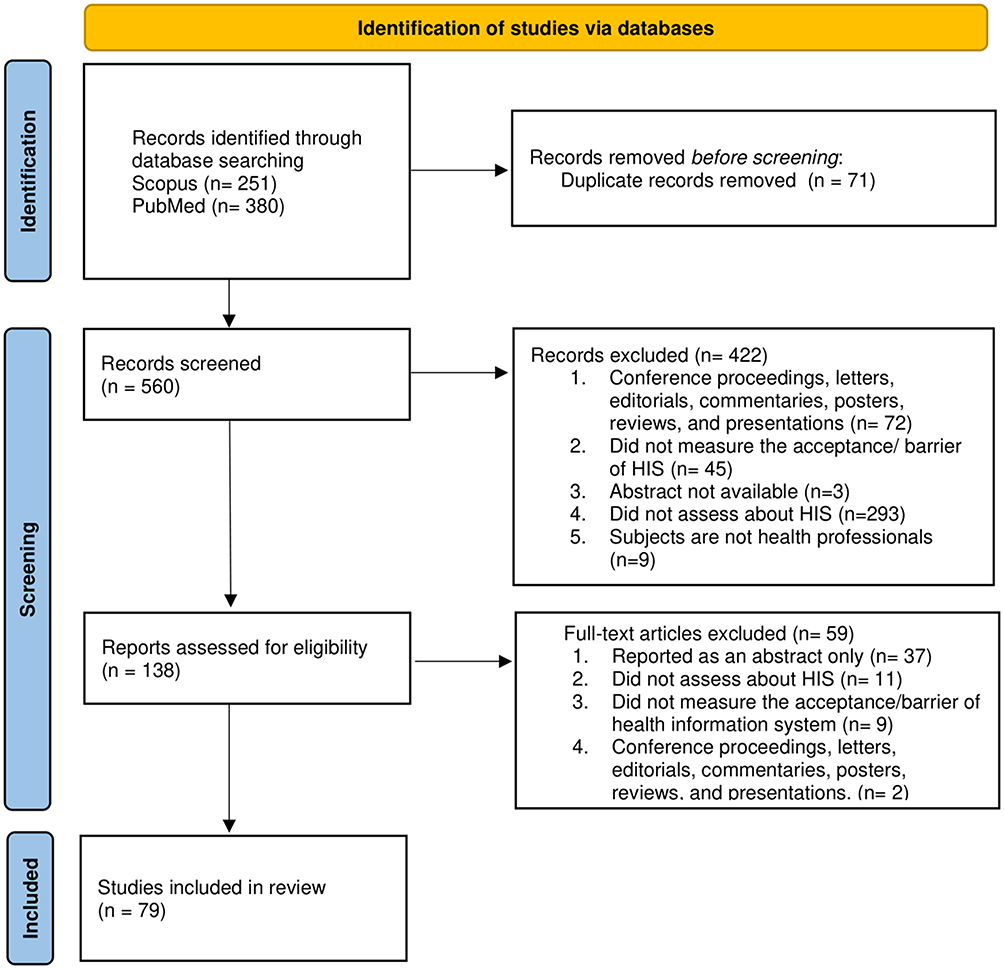 |
Figure 1 PRISMA Flowchart of Study Selection Process. Adapted from Page M J et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; n71 10.1136/bmj.n71. Creative Commons.46 |
Study Characteristic
Table 2 shows the characteristics of the studies included in the analysis. The majority (14 studies, 17.7%) were conducted in the United States of America21,47–59 and in 2015.55,57,60–71 In terms of data collection, 48 studies used cross-sectional study design,8,21,47,50,52–55,60–62,64–66,71–104 18 used qualitative,48,49,51,56,59,63,67,68,105–114 and 13 used mixed methods,57,58,69,70,115–123 respectively. The study with the largest number of participants at 6443 was by Vitari et al.91 The most commonly used type of HIS was electronic health records.1–9,21,47–53,55,60,61,64–68,72,74,75,77,78,82,86,88–93,96,100,102,103,106–109,111,115,118,119 Physicians47,51–53,56–58,60,61,63,69,70,82,83,86,87,89,90,92,100,101,112,114,117–119,122 and nurses8,50,55,64,66,67,71,74,75,78,79,94,95,97,98,105,106,108 were the 2 healthcare professionals commonly selected as subjects for investigations (Supplementary Material 2).
 |
Table 2 Studies Characteristics |
Main Result
The review explored facilitator and barrier across various contextual perspectives (Supplementary Material 3). Organizational context showed facilitating conditions regarding HIS use as the most frequent facilitator, as shown by the results from 11 studies. HIC and LMIC were the focus of the most discussions (4 studies each), as presented in Figure 2. However, the lack of consensus responsibility was identified as a significant barrier, with results from 13 studies outlining the impact. HIC had the highest number of discussions, while no LMIC addressed the issue. From an individual context perspective, positive behavior and attitude were outlined as the primary facilitator for HIS use, according to the results from 27 studies. Negative perception was identified to be a prominent barrier, as signified by 10 studies. In the technological context, the usefulness and daily task-simplifying of HIS were identified as the most substantial facilitator, with evidence from 22 studies supporting this observation. Conversely, the lack of technical support was identified as a significant barrier, with 19 studies identifying the impact. In the social context, support from experienced friends was identified as an influential facilitator, judging by the results from 11 studies. Lack of leadership role was recognized to be a significant barrier, based on evidence from 12 studies.
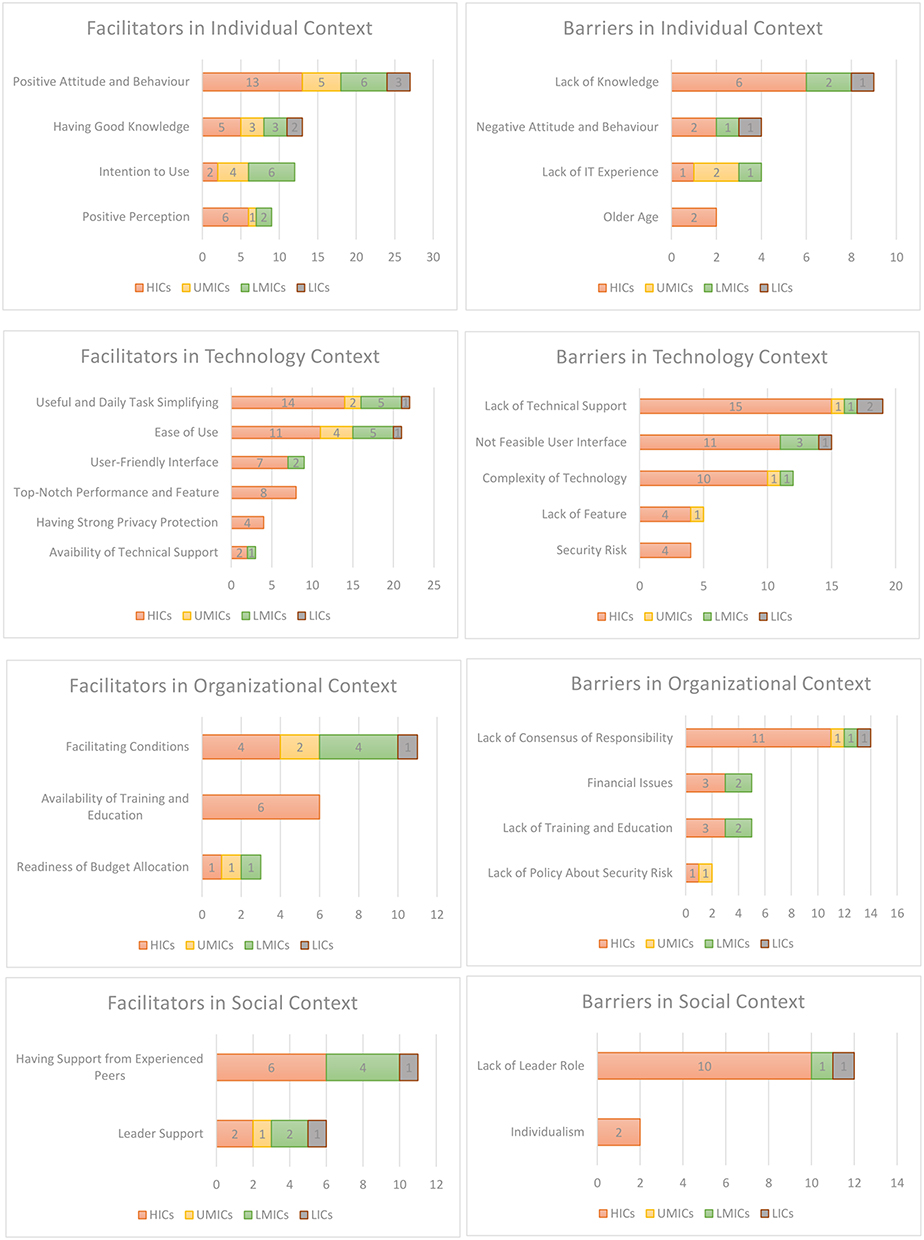 |
Figure 2 Facilitator and Barrier of Utilization of HIS. |
Quality Assessment
A quality assessment was conducted, and the results showed that there were no low-quality identified in the qualitative and mixed-method studies (Supplementary Material 4). Among the qualitative studies, 13 and 5 were categorized under high and moderate quality, respectively. Similarly, in the mixed method, 11 and 2 were classified under high and moderate quality. Regarding the cross-sectional studies, the majority of 36 studies were determined to be of high quality, with 9 classified under moderate quality. Meanwhile, only 2 studies were considered to be of low quality, as both lacked clear descriptions of inclusion criteria, subject and setting explanations, standard criteria for the measured conditions, and details of the statistical analysis adopted.
Discussion
This review outlined the multifaceted nature of facilitator and barrier toward the implementation and use of information system and technology by healthcare professionals, ranging from individual, technological, organizational, and social contexts. This classification provided a comprehensive understanding of the diverse factors. By organizing these facilitator and barrier into specific categories, a deeper insight into the multifaceted nature of the challenges and opportunities associated with HIS use was acquired.
Individual Context
In LIC, the identified facilitator in individual contexts was limited to positive attitude and behavior,68,93,103 alongside possessing good IT knowledge.93,103 A positive attitude and behavior, comprise maintaining an optimistic outlook on life, expecting improvement and success, as well as viewing the bright side of challenging situations.124 HIC, UMIC, and LMIC recognized a broader spectrum of facilitator in individual contexts, including previous IT experience, positive attitude and behavior, intention to use, positive perception, and good knowledge. Studies showed that subjects with a positive perception of HIS usefulness, often due to good IT knowledge or experience, tend to have a more positive attitude towards the application in work, perceiving it as facilitator rather than barrier.125 Furthermore, the intention to use HIS significantly strengthened this relationship, specifically when users believe in the positive impact towards HIS.125 This implies that the effective adoption of HIS could be significantly improved by training initiatives to enhance health workers confidence in using system and by clearly communicating the benefits to increase motivation.
The most prevalent barrier in the individual context across HIC, UMIC, LMIC, and LIC was negative perception towards the use of new technology in the implementation of HIS. Barrier in individual contexts was nearly the same in all categories of countries, signifying a shared struggle in addressing barrier toward HIS implementation. To overcome negative perceptions, there is a need to actively acquire positive information and experiences. This enables healthcare professionals to effectively handle the inevitable challenges faced in demanding healthcare settings.126 Negative perceptions often arise from a natural tendency to focus more on negative information. Consciously combating this bias by identifying positive aspects can be instrumental in reshaping perceptions.127 However, lack of IT experience was not mentioned as barrier in LIC, which can be attributed to limited exposure to complex system and a greater emphasis on addressing resource constraints.128 A combination of technological enhancements, capacity-building activities, and data quality assessment with a feedback system has proven to be effective in enhancing IT experience.129
Evidence increasingly shows the challenges arising from a lack of human-centered design in HIS, directly impacting performance in healthcare settings. For example, inadequate HIS planning, lack of training for professionals, and inadequate preparation for unplanned system disruptions can all lead to compromised healthcare quality and increased risks to patient safety.130 Additionally, studies show systemic issues within HIS that can be partly attributed to a lack of proper consideration for human capabilities and limitations during the design and implementation stages.131,132 To optimize performance and ensure patient safety, a complete understanding of the cognitive, physical, and organizational dimensions of healthcare professionals interaction with these technologies must be achieved through user usability testing.133
Technology Context
The most prominent facilitator across diverse economic settings was the ability to be useful and simplify daily tasks. This suggests that regardless of the economic context, health professionals value technology known to demonstrably ease workload, streamline routines, and ultimately improve efficiency in daily operations. This is consistent with the understanding that the core value proposition of HIS lies in the ability to optimize workflows and reduce administrative burdens.134 Similarly, ease of use and a user-friendly interface were mentioned, showing that when technology is easy to navigate, it reduces resistance towards change and enhances user satisfaction, ultimately contributing to better integration and utilization.
Emphasis on top-notch performance and having strong security protection was predominantly articulated by HIC only. The pursuit of top-notch performance was in line with the importance of ensuring seamless and efficient functioning of HIS technology, thereby optimizing healthcare delivery and administrative processes.135 The emphasis on these aspects was driven by the crucial need to maintain the highest levels of data privacy and security, particularly due to the sensitive nature of healthcare information.136 This signified that HIC was proactive in recognizing the security risk threat to technology use and having good awareness of the potential threats posed by security vulnerabilities. The vulnerability to security breaches, data theft, and unauthorized access presents a universal challenge transcending economic distinctions.137,138
The fact that LMIC and LIC specifically mentioned “Availability of Technical Support” as facilitator, but not “Top-Notch Performance” or “Strong Security”, suggests HIS adoption is likely in an early stage where basic functionality and support are the main needs. Therefore, both may not be focused on the more complex demands of strong security and high-level performance that become more critical with advanced HIS integration. HIC did not cite “Availability of Technical Support” as facilitator, probably due to the perception as a bare minimum. Reliable technical support is a given and not a key driver for HIS use, likely focused on more advanced features of the technology. Although HIC may have greater resources for addressing security risks, it is essential for UMIC, LMIC, and LIC to also prioritize strong security measures to safeguard sensitive health information.136 Acknowledging and addressing this shared concern present the commitment to mitigating risks and promoting a secure environment for health information management.139 In the modern world, a diverse set of technologies including the Internet of Things, blockchain, mobile health apps, cloud platforms, and integrated forms, are being leveraged to strengthen the security and privacy of healthcare information.140
The predominant barrier often cited is the lack of technical issues. However, the nature of technical issues experienced by LIC and LMIC differs significantly from those encountered by HIC and UMIC. LIC and LMIC frequently face perceived technical problems such as poor internet access leading to slow system performance, inadequate computer infrastructure limiting efficient HIS use, and unreliable power supply leading to data loss due to lack of automatic saving.93,103 However, HIC and UMIC encounter minor technical issues, such as frequent and disruptive bubble messages, the absence of a “help” button for immediate assistance with technical problems, and other relatively minor technical matters.57,110,113,116,119
The complexity of technology, lack of essential features, and non-feasible user interface collectively pose significant barrier to effective HIS use. The intricate nature of modern technology often results in HIS platforms being overly complex, making it challenging for effective navigation and use by healthcare professionals.141 Additionally, the absence of crucial features in system hinders the ability to meet the diverse needs of healthcare providers and organizations, leading to suboptimal functionality.142 The presence of a non-feasible user interface further elevates the usability issues, diminishing user experience and making it arduous for individuals to interact with the system.143,144 These barrier significantly impede the integration and effective HIS use in healthcare technology landscape, thereby impacting the delivery of quality patient care and the overall efficiency of healthcare processes.
Technology barrier in HIS is a direct consequence and deeply intertwined with human performance.145 The capacity of healthcare professionals to work efficiently and effectively is directly limited by poorly designed HIS that often ignore human-centered design principles.146 Systems with technical problems, difficult-to-use interfaces, or unreliable performance led to increased mental effort, a higher risk of errors, and interruptions in established clinical workflows.147 The mismatch between health IT design and how humans think and work reduces productivity while also endangering patient safety.130 The frustration and mental overload caused by poorly designed or difficult technology can result in workarounds, lower user satisfaction, and the failure to realize the intended benefits of HIS.148 This emphasizes the critical importance of putting human-centered design principles first in the development and implementation of HIS to maximize both system effectiveness and human performance in healthcare.
Organizational Context
Facilitating conditions appear as a relevant facilitator across all income levels. These conditions comprised a range of crucial elements such as conducive policy frameworks,60,62,80,82,96,121 robust infrastructure,53,64,72,73,78,79,82,90,98,104,115,149 and proficient human resources,110,112 collectively creating a conducive environment. The prevalence of mentions across diverse income levels presented the universal recognition of the crucial role played by facilitating conditions in driving the effective use of technology.150,151 Since each country aims to improve healthcare system, recognizing facilitating conditions remains a key factor.
Availability of training and education was recognized as a crucial facilitator for successful HIS use, particularly in HIC.72,102,109,110,112,114 In well-resourced settings such as HIC, organizations are likely to invest more in comprehensive training programs to ensure proper system adoption and maximize the benefits of HIS. This facilitator being predominantly conveyed reflected an effort to prioritize continuous learning and skill development in leveraging technological advancements in healthcare system.152 The implementation of new technology, such as HIS, requires comprehensive training for effective use, supporting the growth of both the individual and the organization.153 Therefore, training plays a crucial role in enhancing individual skills as well as driving organizational growth and success. The training programs are crucial for ensuring the desired outcomes of implementation are defined and measured.154
HIC, UMIC, and LMIC recognized the importance of substantial budget allocations for the implementation and sustainability of HIS. This collective awareness is grounded in the understanding that adequate financial resources are essential for the successful deployment and long-term viability of HIS in healthcare system.155 LIC did not consistently elaborate the availability of budgetary allocations as facilitator. This disparity can be attributed to several factors, including limited financial resources, competing healthcare priorities, challenges in budget transparency and allocation, as well as a lack of comprehensive strategic planning.156 In LIC, the perception that budget availability is not facilitator might point to it being a more fundamental limitation requiring urgent attention to be addressed. The infrequent mention of budget availability suggests that while financial commitment is essential for HIS implementation, it is likely that having a budget is considered a basic necessity rather than a frequently recognized positive facilitator.
HIC mentioned financial issues as barrier, while LICs did not, suggesting the need for closer examination. This discrepancy in acknowledgment may be attributed to the varying financial,157,158 resources availability, and educational landscapes between the two categories of countries.159 In HIC, financial constraints might relate to the high costs of implementing and maintaining sophisticated, integrated HIS, including advanced security features, interoperability solutions, and continuous upgrades.160 These countries might face budgetary competition for cutting-edge technologies and encounter challenges in justifying the return on investment for complex HIS implementations.161 On the other hand, LIC might focus on the more fundamental matters that need to be in place before money problems for specific HIS including no electricity or internet, not enough trained people, or no existing systems. In these situations, not having significant money for investment in HIS might be assumed and not specifically pointed out as barrier.162
The lack of consensus regarding responsibility was the most commonly cited barrier to effective HIS use across diverse healthcare landscapes. The absence of clearly defined roles and responsibilities results in an impaired collaboration between practitioners,49,51,67 diminished trust in information from other healthcare providers,48,51,56,61,71,99,108,109,111,112,123 and uncertainty surrounding documentation duties.78,93,109 These challenges arise due to ambiguous accountability, with practitioners uncertain of who is responsible for key tasks such as result follow-up, order entry, and record updates.127,163 Irrespective of income status, all countries struggle with this barrier, experiencing limited information flow, disjointed care, and compromised patient outcomes due to nebulous governance in health information management.164 Therefore, responsibility consensus should be established as a universal priority to facilitate optimal HIS use.
Awareness regarding the lack of policy on risk security is predominantly evident in HIC120 and UMIC,122 while it should logically be a universal concern across all countries, regardless of income level.165 The relative silence from LIC might not necessarily show the absence of such risks, but rather a potential lack of resources, expertise, or prioritization in identifying and articulating these concerns.166 Since HIC and UMIC show an absence of robust risk security policies, there is a need for a more concentrated effort to address this critical aspect of HIS implementation.165 This necessitates the development and dissemination of best practices, the provision of technical assistance, and fostering international collaboration to establish universal standards and guidelines for HIS risk security policy.
The adoption of HIS is significantly influenced by the basic contrasts in policy and funding structures between high-income and low-income settings. HIC often benefits from substantial public and private investment in digital infrastructure, coupled with supportive national policies that mandate or incentivize HIS implementation, promote interoperability, and ensure data security.167 This conducive environment fosters widespread adoption and sophisticated system development. Conversely, LICs frequently face significant hurdles due to limited financial resources, fragmented or non-existent national digital health strategies, and competing priorities for healthcare spending.156 Consequently, HIS adoption in these settings is often piecemeal, underfunded, and struggles with infrastructural limitations and a lack of cohesive policy frameworks, leading to a digital divide in healthcare capabilities.
Social Context
Support from peers and the influential role of leadership were widely acknowledged as key facilitator in effective HIS use. The crucial role of peer networks includes sharing best practices, knowledge exchange, and mutual encouragement, all of which contributed to successful implementation.168 These results are in line with social learning theory, positing that individuals learn and adopt new behaviors by observing and interacting with others within social network.169 Furthermore, effective leadership plays a crucial role in championing technological advancements, fostering a culture of innovation, and garnering support for change initiatives.170 With social support being strongly emphasized, it appears that efforts focused on enabling peer learning and mentorship programs could be particularly impactful in advancing successful HIS adoption, specifically in settings facing resource limitations.171
The absence of effective leadership and an environment characterized by individualism presented significant barrier to successful HIS use in healthcare settings. Inadequate leadership could hinder the development and implementation of cohesive strategies for integration, leading to fragmented efforts and a lack of organizational buy-in.172,173 A leader's absence or lack of engagement can cause healthcare workers to feel unsure, resist change, and not commit to new HIS, obstructing the implementation. Meanwhile, a leader who models autonomy, accountability, teamwork, and patient-focused improvement can prevent these barrier.174 HIC often identified individualism to be a prominent barrier, as the emphasis on self-reliance and autonomy may impede the collective efforts required for comprehensive implementation and use.175 Addressing these barrier necessitates effective leadership to drive cohesive strategies and a shift towards a collaborative culture that prioritizes the collective benefit of HIS in healthcare system.176 This result implies that addressing systemic issues related to leadership and organizational culture may be more critical than focusing solely on individual attitudes when seeking to promote effective HIS implementation.
Public Health Implication
Comparing successful and failed HIS adoptions provides valuable insights, allowing the identification of key facilitator and barrier by studying instances of significant improvements and critical shortcomings in healthcare delivery and efficiency. For example, successful implementations often show strong leadership support, comprehensive user training, robust technical infrastructure, and a user-centered design approach consistent with existing workflows. Conversely, unsuccessful cases show barrier such as inadequate stakeholder engagement, insufficient funding, poor system usability, lack of interoperability, and resistance to change. Understanding these differentiating factors offers valuable lessons for policymakers, healthcare administrators, and implementers aiming to maximize successful HIS adoption and avoid common mistakes.
Facilitator identified in this scoping review show key elements supporting successful HIS implementation, ultimately improving patient care through better information access and decision-making. These facilitator will enhance healthcare system efficiency through streamlined workflows and resource management. Equally, barrier underscore the challenges requiring attention for effective adoption and the realization of these benefits. This review of facilitator and barrier provides a foundation for informed decision-making by policymakers and healthcare professionals to enhance HIS acceptance.
The adoption of HIS is significantly shaped by overarching policy landscapes. Facilitator and barrier identified in this review offer valuable insights for policymakers aiming to optimize HIS adoption and effectiveness.177 This understanding can contribute to targeted interventions and policies that address barrier and leverage facilitator to optimize information system use in healthcare, ultimately leading to improved delivery, better patient outcomes, and a positive impact on public health. To reduce resistance and foster greater acceptance, policymakers should prioritize early and continuous engagement of healthcare professionals,178 invest in comprehensive training and support,179 clearly articulate the benefits of HIS for patient care and workflow efficiency,180 establish and enforce stringent data security and privacy policies,181 adopt a user-centered design approach,130 as well as establish robust communication channels for feedback.178 Drawing upon global best practices, policymakers should also consider investing in interoperable infrastructure, establishing clear national standards (including for data security and privacy), prioritizing user participation in system design, ensuring adequate and sustainable funding, as well as promoting collaboration across healthcare organizations.179 By strategically addressing these areas with a strong emphasis on data security and privacy, policymakers can create an enabling environment for successful HIS adoption, contributing to a more efficient, patient-centered, and secure healthcare system.
Strength, Limitation, and Future Study
A key strength of this study lies in the approach, which allows for a broad mapping of the landscape, capturing a diverse range of factors influencing HIS adoption and use as perceived by health professionals. The review helps to inform policymakers of the factors that facilitate or hinder the use of information system or technology by healthcare professionals. Facilitating factors or barrier to the use of information system or information technology have been presented. However, this study also presents a limitation including the literature search conducted using terms that may not have comprised all publications in the databases, no further contact existed with the authors of the papers to validate the content analysis of the review, grey literature was excluded, no risk of bias assessment was performed, results were presented descriptively, and only English language studies were included. Although this scoping review primarily focused on facilitator and barrier to the use of core HIS functionalities from the perspective of daily healthcare professional interaction, the growing influence of Artificial Intelligence (AI) and broader digital health trends on the evolution of these systems must be acknowledged. Studies suggest that AI capacity to revolutionize clinical decision-making and improve health outcomes has potential applications in healthcare,182 presenting significant implications for future HIS design and implementation. By leveraging AI as a preferred method for handling big data in healthcare, analytical algorithms can enhance EHRs through big data analytics, enabling healthcare providers to deliver better clinical services by filtering and categorizing large datasets for enhanced data interpretation.183,184 Future studies should explore how the integration of AI-powered tools and the broader digital health ecosystem impacts facilitator and barrier identified in this review. Moreover, the long-term impact of specific HIS functionalities on measurable patient outcomes should be explored as well as economic evaluation as a basis for information technology system development policy. Understanding these factors remains crucial for stakeholders implicated in the design, implementation, and maintenance of HIS.
Conclusion
In conclusion, these results underscore the critical need for targeted interventions that enhance technical support, address user resistance, and streamline HIS training programs to ensure widespread adoption. Future studies should investigate both the economic evaluation of HIS implementations and long-term impacts on healthcare efficiency and patient outcomes, alongside an exploration of the evolving influence of AI and the broader digital health ecosystem on HIS adoption.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funds were provided to the current work.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Sinskey JL, Chang JM, Shibata GS, Infosino AJ, Rouine-Rapp K. Applying conflict management strategies to the pediatric operating room. Anesth Analg. 2019;129(4):1109–1117. doi:10.1213/ANE.0000000000003991
2. Popescu C, EL-Chaarani H, EL-Abiad Z, Gigauri I. Implementation of health information systems to improve patient identification. Int J Environ Res Public Health. 2022;19(22):15236. doi:10.3390/ijerph192215236
3. Kreps GL. Online information and communication systems to enhance health outcomes through communication convergence: online health information and communication Systems. Hum Commun Res. 2017;43(4):518–530. doi:10.1111/hcre.12117
4. Colicchio TK, Facelli JC, Del Fiol G, Scammon DL, Bowes WA, Narus SP. Health information technology adoption: understanding research protocols and outcome measurements for IT interventions in health care. J Biomed Inform. 2016;63:33–44. doi:10.1016/j.jbi.2016.07.018
5. Ross J, Stevenson F, Lau R, Murray E. Factors that influence the implementation of e-health: a systematic review of systematic reviews (an update). Implement Sci. 2016;11(1):146. doi:10.1186/s13012-016-0510-7
6. Popa-Velea O, Purcărea VL. Issues of therapeutic communication relevant for improving quality of care. J Med Life. 2014;7 Spec No. 4(Spec Iss 4):39–45.
7. Bagherian H, Sattari M. Health information system in developing countries: a review on the challenges and causes of success and failure. Med J Islam Repub Iran. 2022. doi:10.47176/mjiri.36.111
8. Barzekar H, Ebrahimzadeh F, Luo J, Karami M, Robati Z, Goodarzi P. Adoption of hospital information system among nurses: a technology acceptance model approach. Acta Inform Medica. 2019;27(5):305–310. doi:10.5455/aim.2019.27.305-310
9. Jeyakumar T, McClure S, Lowe M, et al. An education framework for effective implementation of a health information system: scoping review. J Med Internet Res. 2021;23(2):e24691. doi:10.2196/24691
10. Stanfill MH, Marc DT. Health information management: implications of artificial intelligence on healthcare data and information management. Yearb Med Inform. 2019;28(01):056–064. doi:10.1055/s-0039-1677913
11. Haux R. Health Information Systems: past, Present, Future – revisited. In: Mantas J, Hasman A, Haux R editors. Studies in Health Technology and Informatics. IOS Press;2022:108–134. doi:10.3233/SHTI220945
12. Epizitone A, Moyane SP, Agbehadji IE. A systematic literature review of health information systems for healthcare. Healthcare. 2023;11(7):959. doi:10.3390/healthcare11070959
13. Bassi J, Lau F. Measuring value for money: a scoping review on economic evaluation of health information systems. J Am Med Inform Assoc. 2013;20(4):792–801. doi:10.1136/amiajnl-2012-001422
14. David Bates W. Health information technology and care coordination: the next big opportunity for informatics? Yearb Med Inform. 2015;24(01):11–14. doi:10.15265/IY-2015-020
15. Barker W, Chang W, Everson J, et al. The evolution of health information technology for enhanced patient-centric care in the United States: data-driven descriptive study. J Med Internet Res. 2024;26:e59791. doi:10.2196/59791
16. Kisekka V, Giboney JS. The effectiveness of health care information technologies: evaluation of trust, security beliefs, and privacy as determinants of health care outcomes. J Med Internet Res. 2018;20(4):e107. doi:10.2196/jmir.9014
17. Nielsen P, Sahay S. A critical review of the role of technology and context in digital health research. Digit Health. 2022;8. doi:10.1177/20552076221109554
18. Alfian SD, Insani WN, Puspitasari IM, Wawruch M, Abdulah R. Effectiveness and process evaluation of using digital health technologies in pharmaceutical care in low- and middle-income countries: a systematic review of quantitative and qualitative studies. Telemed E-Health. 2023;29(9):1289–1303. doi:10.1089/tmj.2022.0406
19. Alotaibi YK, Federico F. The impact of health information technology on patient safety. Saudi Med J. 2017;38(12):1173–1180. doi:10.15537/smj.2017.12.20631
20. Ridho A, Alfian SD, Van Boven JFM, et al. Digital health technologies to improve medication adherence and treatment outcomes in patients with tuberculosis: systematic review of randomized controlled trials. J Med Internet Res. 2022;24(2):e33062. doi:10.2196/33062
21. Darby AB, Su Y, Reynolds RB, Madlock-Brown C. A survey-based study of pharmacist acceptance and resistance to health information technology. Perspect Health Inf Manag. 2019;16(Spring):1a. doi:10.1016/j.ijmedinf.2015.03.004
22. Williams KS, Shah GH, Leider J, Gupta A. Overcoming barriers to experience benefits: a qualitative analysis of electronic health records and health information exchange implementation in local health departments. EGEMs Gener Evid Methods Improve Patient Outcomes. 2017;5(1):18. doi:10.5334/egems.216
23. Luna R, Rhine E, Myhra M, Sullivan R, Kruse CS. Cyber threats to health information systems: a systematic review. Technol Health Care. 2016;24(1):1–9. doi:10.3233/THC-151102
24. Tan SSL, Goonawardene N. Internet health information seeking and the patient-physician relationship: a systematic review. J Med Internet Res. 2017;19(1):e9. doi:10.2196/jmir.5729
25. Alolayyan MN, Alyahya MS, Alalawin AH, Shoukat A, Nusairat FT. Health information technology and hospital performance the role of health information quality in teaching hospitals. Heliyon. 2020;6(10):e05040. doi:10.1016/j.heliyon.2020.e05040
26. Mazlan EM, Bath PA. Impact of health informatics implementation on clinical workflow: a review. 2012.
27. Bowens FM, Frye PA, Jones WA. Health information technology: integration of clinical workflow into meaningful use of electronic health records.
28. Bates DW, Singh H. Two decades since to err is human: an assessment of progress and emerging priorities in patient safety. Health Aff. 2018;37(11):1736–1743. doi:10.1377/hlthaff.2018.0738
29. Walle AD, Demsash AW, Adem JB, et al. Exploring facilitators and barriers of the sustainable acceptance of e-health system solutions in Ethiopia: a systematic review. PLoS One. 2023;18(8):e0287991. doi:10.1371/journal.pone.0287991
30. Stamatian F. Barriers in the implementa- tion of health information systems: a scoping review. 2013.
31. AlQudah AA, Al-Emran M, Shaalan K. Technology acceptance in healthcare: a systematic review. Appl Sci. 2021;11(22):10537. doi:10.3390/app112210537
32. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
33. Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18(1):143. doi:10.1186/s12874-018-0611-x
34. Munn Z, Pollock D, Khalil H, et al. What are scoping reviews? Providing a formal definition of scoping reviews as a type of evidence synthesis. JBI Evid Synth. 2022;20(4):950–952. doi:10.11124/JBIES-21-00483
35. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
36. D’Agostino M, Marti M, Otero P, et al. Toward a holistic definition for information systems for health in the age of digital interdependence. Rev Panam Salud Pública. 2021;45:1. doi:10.26633/RPSP.2021.143
37. Sitorus HM, Govindaraju R, Wiratmadja II, Sudirman I. Technology adoption: an interaction perspective. IOP Conf Ser Mater Sci Eng. 2016;114:12080. doi:10.1088/1757-899X/114/1/012080
38. Khalifa M. Barriers to health information systems and electronic medical records implementation. a field study of Saudi Arabian hospitals. Procedia Comput Sci. 2013;21:335–342. doi:10.1016/j.procs.2013.09.044
39. Litchfield I, Bentham L, Hill A, McManus RJ, Lilford R, Greenfield S. The impact of status and social context on health service co-design: an example from a collaborative improvement initiative in UK primary care. BMC Med Res Methodol. 2018;18(1):136. doi:10.1186/s12874-018-0608-5
40. Kabukye JK, De Keizer N, Cornet R. Assessment of organizational readiness to implement an electronic health record system in a low-resource settings cancer hospital: a cross-sectional survey. PLoS One. 2020;15(6):e0234711. doi:10.1371/journal.pone.0234711
41. Xiao WS. The Role of collectivism–individualism in attitudes toward compliance and psychological responses during the COVID-19 pandemic. Front Psychol. 2021;12:600826. doi:10.3389/fpsyg.2021.600826
42. World Bank. World Bank Country Classification 2023.; 2023. Available from: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups.
43. Lockwood C, Munn Z, Porritt K. Qualitative research synthesis: methodological guidance for systematic reviewers utilizing meta-aggregation. Int J Evid Based Healthc. 2015;13(3):179–187. doi:10.1097/XEB.0000000000000062
44. Joanna Briggs Institute. The Joanna Briggs Institute critical appraisal tools for use in JBI systematic reviews: checklist for analytical cross sectional studies. 2017. Available from: https://jbi.global/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Analytical_Cross_Sectional_Studies2017_0.pdf.
45. Hong QN, Pluye P, Fabregues S, et al. Mixed Methods Appraisal Tool (MMAT), Version 2018. Registration of Copyright (#1148552). Industry Canada; 2014:39–45.
46. Page M J et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ, n71 10.1136/bmj.n71
47. Yoo S, Lim K, Jung SY, et al. Examining the adoption and implementation of behavioral electronic health records by healthcare professionals based on the clinical adoption framework. BMC Med Inform Decis Mak. 2022;22(1). doi:10.1186/s12911-022-01959-7
48. Dillon E, Chuang J, Gupta A, et al. Provider perspectives on advance care planning documentation in the electronic health record: the experience of primary care providers and specialists using advance health-care directives and physician orders for life-sustaining treatment. Am J Hosp Palliat Med. 2017;34(10):918–924. doi:10.1177/1049909117693578
49. Bardach SH, Real K, Bardach DR. Perspectives of healthcare practitioners: an exploration of interprofessional communication using electronic medical records. J Interprof Care. 2017;31(3):300–306. doi:10.1080/13561820.2016.1269312
50. Holden RJ, Asan O, Wozniak EM, Flynn KE, Scanlon MC. Nurses’ perceptions, acceptance, and use of a novel in-room pediatric ICU technology: testing an expanded technology acceptance model. BMC Med Inform Decis Mak. 2016;16(1):1–10. doi:10.1186/s12911-016-0388-y
51. Quinn M, Forman J, Harrod M, et al. Electronic health records, communication, and data sharing: challenges and opportunities for improving the diagnostic process. Diagnosis. 2019;6(3):241–248. doi:10.1515/dx-2018-0036
52. Khairat S, Burke G, Archambault H, Schwartz T, Larson J, Ratwani R. Focus section on health IT usability: perceived burden of EHRs on physicians at different stages of their career. Appl Clin Inform. 2018;9(2):336–347. doi:10.1055/s-0038-1648222
53. Bush RA, Kuelbs C, Ryu J, Jiang W, Chiang G. Structured data entry in the electronic medical record: perspectives of pediatric specialty physicians and surgeons. J Med Syst. 2017;41(5):75. doi:10.1007/s10916-017-0716-5
54. Held AD, Woodall LJ, Hertig JB. Pharmacists’ familiarity, utilization, and beliefs about health information exchange: a survey of pharmacists in an Indiana pharmacy organization. J Am Pharm Assoc. 2014;54(6):625–629. doi:10.1331/JAPhA.2014.14080
55. Gartrell K, Trinkoff AM, Storr CL, Wilson ML, Gurses AP. Testing the electronic personal health record acceptance model by nurses for managing their own health: a cross-sectional survey. Appl Clin Inform. 2015;6(2):224–247. doi:10.4338/ACI-2014-11-RA-0107
56. Thorn SA, Carter MA, Bailey JE. Emergency physicians’ perspectives on their use of health information exchange. Ann Emerg Med. 2014;63(3):329–337. doi:10.1016/j.annemergmed.2013.09.024
57. Kamal AH, Kavalieratos D, Bull J, Stinson CS, Nicolla J, Abernethy AP. Usability and acceptability of the QDACT-PC, an electronic point-of-care system for standardized quality monitoring in palliative care. J Pain Symptom Manage. 2015;50(5):615–621. doi:10.1016/j.jpainsymman.2015.05.013
58. Muslin IS, Vardaman JM, Cornell PT. Fostering acceptance of computerized physician order entry: insights from an implementation study. Health Care Manag. 2014;33(2):165–171. doi:10.1097/HCM.0000000000000011
59. Liu X, Barreto EF, Dong Y, et al. Discrepancy between perceptions and acceptance of clinical decision support Systems: implementation of artificial intelligence for vancomycin dosing. BMC Med Inform Decis Mak. 2023;23(1):157. doi:10.1186/s12911-023-02254-9
60. Abdekhoda M, Gohari M, Ahmadi M, Noruzi A. The effects of organizational contextual factors on physicians’ attitude toward adoption of electronic medical records. J Biomed Inform. 2015;53:174–179. doi:10.1016/j.jbi.2014.10.008
61. Wang JY, Ho HY, Chen JD, Chai S, Tai CJ, Chen YF. Attitudes toward inter-hospital electronic patient record exchange: discrepancies among physicians, medical record staff, and patients. BMC Health Serv Res. 2015;15(1):264. doi:10.1186/s12913-015-0896-y
62. Ologeanu-Taddei R, Morquin D, Domingo H, Bourret R. Understanding the acceptance factors of an Hospital Information System: evidence from a French University Hospital. AMIA Annu Symp Proc AMIA Symp. 2015;2015:1001–1007.
63. Lugtenberg M, Weenink JW, van der Weijden T, Westert GP, Kool RB. Implementation of multiple-domain covering computerized decision support systems in primary care: a focus group study on perceived barriers. BMC Med Inform Decis Mak. 2015;15:82. doi:10.1186/s12911-015-0205-z
64. Maillet É, Mathieu L, Sicotte C. Modeling factors explaining the acceptance, actual use and satisfaction of nurses using an electronic patient record in acute care settings: an extension of the UTAUT. Int J Med Inf. 2015;84(1):36–47. doi:10.1016/j.ijmedinf.2014.09.004
65. Alazzam MB, Basari ASH, Sibghatullah AS, Doheir M, Enaizan OMA, Mamra AHK. EHRS acceptance in Jordan hospitals by UTAUT2 model: preliminary result. J Theor Appl Inf Technol. 2015;78(3):473–482.
66. El Mahalli A. Adoption and barriers to adoption of electronic health records by nurses in three governmental hospitals in Eastern Province, Saudi Arabia. Perspect Health Inf Manag. 2015;12:1f.
67. Gonzalez Z, Recondo F, Sommer J, et al. Nurses’ expectations and perceptions of a redesigned electronic health record. Stud Health Technol Inform. 2015;210:374–378.
68. Landis-Lewis Z, Manjomo R, Gadabu OJ, et al. Barriers to using eHealth data for clinical performance feedback in Malawi: a case study. Int J Med Inf. 2015;84(10):868–875. doi:10.1016/j.ijmedinf.2015.07.003
69. Chow A, Lye DCB, Arah OA. Psychosocial determinants of physicians’ acceptance of recommendations by antibiotic computerised decision support systems: a mixed methods study. Int J Antimicrob Agents. 2015;45(3):295–304. doi:10.1016/j.ijantimicag.2014.10.009
70. Helldén A, Al-Aieshy F, Bastholm-Rahmner P, et al. Development of a computerised decisions support system for renal risk drugs targeting primary healthcare. BMJ Open. 2015;5(7):e006775. doi:10.1136/bmjopen-2014-006775
71. Lin HC. The impact of national cultural differences on nurses’ acceptance of hospital information systems. CIN - Comput Inform Nurs. 2015;33(6):265–272. doi:10.1097/CIN.0000000000000152
72. Luyten J, Marneffe W. Examining the acceptance of an integrated electronic health records system: insights from a repeated cross-sectional design. Int J Med Inf. 2021;150. doi:10.1016/j.ijmedinf.2021.104450
73. Iskandar YHP, Subramaniam G, Majid MIA, Ariff AM, Rao GKL. Predicting healthcare professionals’ intention to use poison information system in a Malaysian public hospital. Health Inf Sci Syst. 2020;8(1). doi:10.1007/s13755-019-0094-0
74. Saare MA, Mahdi AA, Lashari SA, Sari SA, Hamid NA. Measuring prevailing practices of healthcare professional on electronic health record through the lens of Iraq. Bull Electr Eng Inform. 2021;10(2):970–977. doi:10.11591/eei.v10i2.2408
75. Tubaishat A. Perceived usefulness and perceived ease of use of electronic health records among nurses: application of technology acceptance model. Inform Health Soc Care. 2018;43(4):379–389. doi:10.1080/17538157.2017.1363761
76. Ljubicic V, Ketikidis PH, Lazuras L. Drivers of intentions to use healthcare information systems among health and care professionals. Health Informatics J. 2020;26(1):56–71. doi:10.1177/1460458218813629
77. Abdekhoda M, Dehnad A, Zarei J. Determinant factors in applying electronic medical records in healthcare. East Mediterr Health J. 2019;25(1):24–33. doi:10.26719/emhj.18.007
78. Al-Rawajfah O, Tubaishat A. Barriers and facilitators to using electronic healthcare records in Jordanian hospitals from the nurses’ perspective: a national survey. Inform Health Soc Care. 2019;44(1):1–11. doi:10.1080/17538157.2017.1353998
79. Zhou LL, Owusu-Marfo J, Asante Antwi H, Antwi MO, Kachie ADT, Ampon-Wireko S. assessment of the social influence and facilitating conditions that support nurses’ adoption of hospital electronic information management systems (HEIMS) in Ghana using the unified theory of acceptance and use of technology (UTAUT) model. BMC Med Inform Decis Mak. 2019;19(1). doi:10.1186/s12911-019-0956-z
80. Iskandar YHP, Ariff AM, Gilbert L. Investigating emergency department healthcare professionals’ intention to use the poison information system. Malays J Med Health Sci. 2022;18(2):129–135.
81. Boadu RO, Lamptey MA, Boadu KAO, Adzakpah G, Mensah NK. Healthcare providers’ intention to use technology to attend to clients in Cape Coast Teaching Hospital, Ghana. BioMed Res Int. 2021;2021. doi:10.1155/2021/5547544.
82. Hossain A, Quaresma R, Rahman H. Investigating factors influencing the physicians’ adoption of electronic health record (EHR) in healthcare system of Bangladesh: an empirical study. Int J Inf Manag. 2019;44:76–87. doi:10.1016/j.ijinfomgt.2018.09.016
83. Abdekhoda M, Salih KM. Determinant factors in applying picture archiving and communication systems (PACS) in healthcare. Perspect Health Inf Manag. 2017;14(Summer):1c.
84. Nadri H, Rahimi B, Afshar HL, Samadbeik M, Garavand A. Factors affecting acceptance of hospital information systems based on extended technology acceptance model: a case study in three paraclinical departments. Appl Clin Inform. 2018;9(2):238–247. doi:10.1055/s-0038-1641595
85. Lin IC, Lin C, Hsu CL, Roan J, Yeh JS, Cheng YH. The usage behavior and intention stability of nurses: an empirical study of a nursing information system. J Nurs Res. 2016;24(1):48–57. doi:10.1097/jnr.0000000000000103
86. Baysari MT, Dort BAV, Zheng WY, et al. Prescribers’ reported acceptance and use of drug-drug interaction alerts: an Australian survey. Health Informatics J. 2022;28(2):146045822211006. doi:10.1177/14604582221100678
87. Chuang CH, Li YF, Kuo LC, Yang MC, Kao LT. Factors influencing the use of health information exchange by physicians—using the national health insurance PharmaCloud system in Taiwan. Int J Environ Res Public Health. 2021;18(16):8415. doi:10.3390/ijerph18168415
88. De Benedictis A, Lettieri E, Gastaldi L, Masella C, Urgu A, Tartaglini D. Electronic medical records implementation in hospital: an empirical investigation of individual and organizational determinants. PLoS One. 2020;15(6):e0234108. doi:10.1371/journal.pone.0234108
89. Alsohime F, Temsah MH, Al-Eyadhy A, et al. Satisfaction and perceived usefulness with newly-implemented Electronic Health Records System among pediatricians at a university hospital. Comput Methods Programs Biomed. 2019;169:51–57. doi:10.1016/j.cmpb.2018.12.026
90. Hwang HG, Dutta B, Chang H-C. The differing effect of gender and clinical specialty on physicians’ intention to use electronic medical record. Methods Inf Med. 2019;58(S 02):e58–e71. doi:10.1055/s-0039-1695718
91. Vitari C, Ologeanu-Taddei R. The intention to use an electronic health record and its antecedents among three different categories of clinical staff. BMC Health Serv Res. 2018;18(1):194. doi:10.1186/s12913-018-3022-0
92. Abdekhoda M, Ahmadi M, Dehnad A, Noruzi A, Gohari M. Applying electronic medical records in health care: physicians’ perspective. Appl Clin Inform. 2016;07(02):341–354. doi:10.4338/ACI-2015-11-RA-0165
93. Biruk S, Yilma T, Andualem M, Tilahun B. Health Professionals’ readiness to implement electronic medical record system at three hospitals in Ethiopia: a cross sectional study. BMC Med Inform Decis Mak. 2014;14(1):115. doi:10.1186/s12911-014-0115-5
94. Vollmer AM, Prokosch HU, Evans S, Kuttler K. Evaluation of acceptance of nursing information system in a German and American Hospital. Stud Health Technol Inform. 2016;225:118–122.
95. Ifinedo P. The moderating effects of demographic and individual characteristics on nurses’ acceptance of information systems: a Canadian study. Int J Med Inf. 2016;87:27–35. doi:10.1016/j.ijmedinf.2015.12.012
96. Struik MHL, Koster F, Schuit AJ, Nugteren R, Veldwijk J, Lambooij MS. The preferences of users of electronic medical records in hospitals: quantifying the relative importance of barriers and facilitators of an innovation. Implement Sci. 2014;9(1). doi:10.1186/1748-5908-9-69
97. Hsu HH, Wu YH. Investigation of the effects of a nursing information system by using the technology acceptance model. CIN - Comput Inform Nurs. 2017;35(6):315–322. doi:10.1097/CIN.0000000000000313
98. Sharifian R, Askarian F, Nematolahi M, Farhadi P. Factors influencing nurses’ acceptance of hospital information systems in Iran: application of the Unified Theory of Acceptance and Use of Technology. Health Inf Manag J. 2014;43(3):23–28. doi:10.12826/18333575.2014.0001.Sharifian
99. Hadji B, Martin G, Dupuis I, Campoy E, Degoulet P. 14 Years longitudinal evaluation of clinical information systems acceptance: the HEGP case. Int J Med Inf. 2016;86:20–29. doi:10.1016/j.ijmedinf.2015.11.016
100. Sayyah Gilani M, Iranmanesh M, Nikbin D, Zailani S. EMR continuance usage intention of healthcare professionals. Inform Health Soc Care. 2017;42(2):153–165. doi:10.3109/17538157.2016.1160245
101. Albahar F, Abu-Farha RK, Alshogran OY, Alhamad H, Curtis CE, Marriott JF. Healthcare professionals’ perceptions, barriers, and facilitators towards adopting computerised clinical decision support systems in antimicrobial stewardship in Jordanian hospitals. Healthcare. 2023;11(6):836. doi:10.3390/healthcare11060836
102. Feely K, Edbrooke L, Bower W, et al. Allied health professionals’ experiences and lessons learned in response to a big bang electronic medical record implementation: a prospective observational study. Int J Med Inf. 2023;176:105094. doi:10.1016/j.ijmedinf.2023.105094
103. Walle AD, Ferede TA, Baykemagn ND, et al. Predicting healthcare professionals’ acceptance towards electronic personal health record systems in a resource-limited setting: using modified technology acceptance model. BMJ Health Care Inform Online. 2023;30(1):e100707. doi:10.1136/bmjhci-2022-100707
104. Seliaman ME, Albahly MS. The reasons for physicians and pharmacists’ acceptance of clinical support systems in Saudi Arabia. Int J Environ Res Public Health. 2023;20(4):3132. doi:10.3390/ijerph20043132
105. Heidarizadeh K, Rassouli M, Manoochehri H, Zagheri Tafreshi M, Kashef Ghorbanpour R. Nurses’ perception of challenges in the use of an electronic nursing documentation system. CIN - Comput Inform Nurs. 2017;35(11):599–605. doi:10.1097/CIN.0000000000000358
106. De leeuw JA, Woltjer H, Kool RB. Identification of factors influencing the adoption of health information technology by nurses who are digitally lagging: in-depth interview study. J Med Internet Res. 2020;22(8). doi:10.2196/15630
107. Geeven IPAC, Jessurun NT, Wasylewicz ATM, et al. Barriers and facilitators for systematically registering adverse drug reactions in electronic health records: a qualitative study with Dutch healthcare professionals. Expert Opin Drug Saf. 2022;21(5):699–706. doi:10.1080/14740338.2022.2020756
108. Njane A, Jedwab R, Calvo R, et al. Perioperative Nurses’ Perceptions Pre-Implementation of an Electronic Medical Record System. In: editors, Honey M, Ronquillo C, Lee TT, Westbrooke L. Studies in Health Technology and Informatics. IOS Press; 2021:522–527. doi:10.3233/SHTI210787
109. Janssen A, Donnelly C, Elder E, Pathmanathan N, Shaw T. Electronic medical record implementation in tertiary care: factors influencing adoption of an electronic medical record in a cancer centre. BMC Health Serv Res. 2021;21(1):23. doi:10.1186/s12913-020-06015-6
110. Scantlebury A, Sheard L, watt I, Cairns P, Wright J, Adamson J. Exploring the implementation of an electronic record into a maternity unit: a qualitative study using Normalisation Process Theory. BMC Med Inform Decis Mak. 2017;17(1):1–10. doi:10.1186/s12911-016-0406-0
111. Malm-Nicolaisen K, Fagerlund AJ, Pedersen R. How Do Users of Modern EHR Perceive the Usability, User Resistance and Productivity Five Years or More After Implementation? In: Otero P, Scott P, Martin SZ, Huesing E editors. Studies in Health Technology and Informatics. IOS Press;2022:829–833. doi:10.3233/SHTI220195
112. Centemero NS, Rechel B. Barriers and facilitators to a health information exchange system between general practitioners and hospitals: a qualitative study in Southern Switzerland. Swiss Med Wkly. 2021;151(41–42):w30063. doi:10.4414/smw.2021.w30063
113. Koskela T, Sandström S, Mäkinen J, Liira H. User perspectives on an electronic decision-support tool performing comprehensive medication reviews - a focus group study with physicians and nurses. BMC Med Inform Decis Mak. 2016;16:6. doi:10.1186/s12911-016-0245-z
114. Huang Z, George MM, Tan YR, et al. Are physicians ready for precision antibiotic prescribing? A qualitative analysis of the acceptance of artificial intelligence-enabled clinical decision support systems in India and Singapore. J Glob Antimicrob Resist. 2023;35:76–85. doi:10.1016/j.jgar.2023.08.016
115. Ahmed MH, Bogale AD, Tilahun B, et al. Intention to use electronic medical record and its predictors among health care providers at referral hospitals, north-West Ethiopia, 2019: using unified theory of acceptance and use technology 2(UTAUT2) model. BMC Med Inform Decis Mak. 2020;20(1). doi:10.1186/s12911-020-01222-x
116. Marcilly R, Colliaux J, Robert L, et al. Improving the usability and usefulness of computerized decision support systems for medication review by clinical pharmacists: a convergent, parallel evaluation. Res Soc Adm Pharm. 2023;19(1):144–154. doi:10.1016/j.sapharm.2022.08.012
117. Askari M, JLYY T, Aarnoutse MF, Meulendijk M. Perceived effectiveness of clinical pathway software: a before-after study in the Netherlands. Int J Med Inf. 2020;135. doi:10.1016/j.ijmedinf.2019.104052
118. Paré G, Raymond L, De guinea AO, et al. Barriers to organizational adoption of EMR systems in family physician practices: a mixed-methods study in Canada. Int J Med Inf. 2014;83(8):548–558. doi:10.1016/j.ijmedinf.2014.06.003
119. Van Biesen W, Van Cauwenberge D, Decruyenaere J, Leune T, Sterckx S. An exploration of expectations and perceptions of practicing physicians on the implementation of computerized clinical decision support systems using a Qsort approach. BMC Med Inform Decis Mak. 2022;22(1). doi:10.1186/s12911-022-01933-3
120. Fung EWT, Au-Yeung GTF, Tsoi LM, et al. Pharmacists’ perceptions of the benefits and challenges of electronic product information system implementation in Hong Kong: mixed-method study. J Med Internet Res. 2020;22(11):e20765. doi:10.2196/20765
121. Handayani PW, Hidayanto AN, Pinem AA, Hapsari IC, Sandhyaduhita PI, Budi I. Acceptance model of a Hospital Information System. Int J Med Inf. 2017;99:11–28. doi:10.1016/j.ijmedinf.2016.12.004
122. Aumpanseang V, Suthiwartnarueput K, Pornchaiwiseskul P. Determinants affecting the health information sharing management and practice for patient referral in Thailand: the perceptions of patients and healthcare professionals. Perspect Health Inf Manag. 2022;19(4):1b.
123. Shamba D, Day LT, Zaman SB, et al. Barriers and enablers to routine register data collection for newborns and mothers: EN-BIRTH multi-country validation study. BMC Pregnancy Childbirth. 2021;21:21. doi:10.1186/s12884-020-03517-3
124. White M, Bryson A. Positive employee attitudes: how much human resource management do you need? Hum Relat. 2013;66(3):385–406. doi:10.1177/0018726712465096
125. Pan X. Technology acceptance, technological self-efficacy, and attitude toward technology-based self-directed learning: learning motivation as a mediator. Front Psychol. 2020;11:564294. doi:10.3389/fpsyg.2020.564294
126. Matheson C, Robertson HD, Elliott AM, Iversen L, Murchie P. Resilience of primary healthcare professionals working in challenging environments: a focus group study. Br J Gen Pract. 2016;66(648):e507–e515. doi:10.3399/bjgp16X685285
127. Kim S, Bochatay N, Relyea-Chew A, et al. Individual, interpersonal, and organisational factors of healthcare conflict: a scoping review. J Interprof Care. 2017;31(3):282–290. doi:10.1080/13561820.2016.1272558
128. Hoxha K, Hung YW, Irwin BR, Grépin KA. Understanding the challenges associated with the use of data from routine health information systems in low- and middle-income countries: a systematic review. Health Inf Manag J. 2022;51(3):135–148. doi:10.1177/1833358320928729
129. Lemma S, Janson A, Lå P, Wickremasinghe D, Källestål C. Improving quality and use of routine health information system data in low- and middle-income countries: a scoping review. PLoS One. 2020;15(10):e0239683. doi:10.1371/journal.pone.0239683
130. Jabin MSR. Operational disruption in healthcare associated with software functionality issue due to software security patching: a case report. Front Digit Health. 2024;6:1367431. doi:10.3389/fdgth.2024.1367431
131. Rahman Jabin MS, Steen M, Wepa D, Bergman P. Assessing the healthcare quality issues for digital incident reporting in Sweden: incident reports analysis. Digit Health. 2023;9:20552076231174307. doi:10.1177/20552076231174307
132. Pan D, Nilsson E, Rahman Jabin MS. A review of incidents related to health information technology in Swedish healthcare to characterise system issues as a basis for improvement in clinical practice. Health Informatics J. 2024;30(3):14604582241270742. doi:10.1177/14604582241270742
133. Alfian SD, Sania JA, Aini DQ, et al. Evaluation of usability and user feedback to guide telepharmacy application development in Indonesia: a mixed-methods study. BMC Med Inform Decis Mak. 2024;24(1):130. doi:10.1186/s12911-024-02494-3
134. Wang Y, Kung L, Byrd TA. Big data analytics: understanding its capabilities and potential benefits for healthcare organizations. Technol Forecast Soc Change. 2018;126:3–13. doi:10.1016/j.techfore.2015.12.019
135. Sheikh A, Anderson M, Albala S, et al. Health information technology and digital innovation for national learning health and care systems. Lancet Digit Health. 2021;3(6):e383–e396. doi:10.1016/S2589-7500(21)00005-4
136. Price WN, Cohen IG. Privacy in the age of medical big data. Nat Med. 2019;25(1):37–43. doi:10.1038/s41591-018-0272-7
137. Abouelmehdi K, Beni-Hessane A, Khaloufi H. Big healthcare data: preserving security and privacy. J Big Data. 2018;5(1):1. doi:10.1186/s40537-017-0110-7
138. Jain P, Gyanchandani M, Khare N. Big data privacy: a technological perspective and review. J Big Data. 2016;3(1):25. doi:10.1186/s40537-016-0059-y
139. Dinh-Le C, Chuang R, Chokshi S, Mann D. Wearable health technology and electronic health record integration: scoping review and future directions. JMIR MHealth UHealth. 2019;7(9):e12861. doi:10.2196/12861
140. Shojaei P, Vlahu-Gjorgievska E, Chow YW. Security and privacy of technologies in health information systems: a systematic literature review. Computers. 2024;13(2):41. doi:10.3390/computers13020041
141. Sittig DF, Singh H. A new socio-technical model for studying health information technology in complex adaptive healthcare systems. 2015.
142. Tummers J, Tekinerdogan B, Tobi H, Catal C, Schalk B. Obstacles and features of health information systems: a systematic literature review. Comput Biol Med. 2021;137:104785. doi:10.1016/j.compbiomed.2021.104785
143. Sumarlin R. The review of user experience and user interface design of hospital information system to improve health care service. Proc Int Conf Business Eco Soc Sci Human. 2018. doi:10.2991/icobest-18.2018.39
144. Bitan Y, Patterson ES. Unique challenges in user interface design for medical devices that use predictive algorithms. Proc Int Symp Hum Factors Ergon Health Care. 2020;9(1):265–266. doi:10.1177/2327857920091004
145. Hottes AK, Foran C, Lee M, Blumenthal MS. Technological Approaches to Human Performance Enhancement. RAND Corporation; 2021. doi:10.7249/RRA1482-2
146. Van Velsen L, Ludden G, Grünloh C. The limitations of user-and human-centered design in an eHealth context and how to move beyond them. J Med Internet Res. 2022;24(10):e37341. doi:10.2196/37341
147. Shan Y, Shang J, Yan Y, Ye X. Workflow interruption and nurses’ mental workload in electronic health record tasks: an observational study. BMC Nurs. 2023;22(1):63. doi:10.1186/s12912-023-01209-9
148. Yusof MM, Takeda T, Shimai Y, Mihara N, Matsumura Y. Evaluating health information systems-related errors using the human, organization, process, technology-fit (HOPT-fit) framework. Health Informatics J. 2024;30(2):14604582241252763. doi:10.1177/14604582241252763
149. Ali SM, Burhanuddin MA, Yaseen AT, et al. E-Health technological barriers faced by Iraqi healthcare institutions. Intell Data Anal. 2023;27:115–135. doi:10.3233/IDA-237438
150. Kamarozaman Z, Razak FZA. The role of facilitating condition in enhancing user’s continuance intention. J Phys Conf Ser. 2021;1793(1):12022. doi:10.1088/1742-6596/1793/1/012022
151. Rumangkit S, Surjandy, Billman A. 2023. The Effect of Performance Expectancy, Facilitating Condition, Effort Expectancy, and Perceived Easy to Use on Intention to using Media Support Learning Based On Unified Theory of Acceptance and Use of Technology (UTAUT). Mursitama TN, Noerlina, Utama DN. In: Abrori SA, editor. E3S Web Conf. Vol. 426. 02004. doi:10.1051/e3sconf/202342602004
152. Qureshi Z. Technology, growth, and inequality: changing dynamics in the digital era. 2021.
153. Farias JS, Resende MM. Impact of Training on the implementation of a new electronic system and acceptance of new technologies in a federal institution of higher education. Rev Adm UFSM. 2020;13(4):773–791. doi:10.5902/1983465932624
154. Barnett S, Jones SC, Caton T, Iverson D, Bennett S, Robinson L. Implementing a virtual community of practice for family physician training: a mixed-methods case study. J Med Internet Res. 2014;16(3):e83. doi:10.2196/jmir.3083
155. Cylus J, Papanicolas I, Smith P, eds.. Health System Efficiency: How to Make Measurement Matter for Policy and Management. WHO Regional Office for Europe; 2016.
156. Wiseman V, Mitton C, Doyle‐Waters MM, et al. Using economic evidence to set healthcare priorities in low‐income and lower‐middle‐income countries: a systematic review of methodological frameworks. Health Econ. 2016;25(S1):140–161. doi:10.1002/hec.3299
157. Peters DH, Garg A, Bloom G, Walker DG, Brieger WR, Hafizur Rahman M. Poverty and access to health care in developing countries. Ann N Y Acad Sci. 2008;1136(1):161–171. doi:10.1196/annals.1425.011
158. Papanicolas I, Woskie LR, Jha AK. Health care spending in the United States and other high-income countries. JAMA. 2018;319(10):1024. doi:10.1001/jama.2018.1150
159. Perry HB, Zulliger R, Rogers MM. Community health workers in low-, middle-, and high-income countries: an overview of their history, recent evolution, and current effectiveness. Annu Rev Public Health. 2014;35(1):399–421. doi:10.1146/annurev-publhealth-032013-182354
160. Hanson K, Brikci N, Erlangga D, et al. The lancet global health commission on financing primary health care: putting people at the centre. Lancet Glob Health. 2022;10(5):e715–e772. doi:10.1016/S2214-109X(22)00005-5
161. Verily AA, Adams L, Barrett M, et al. The promise of digital health: then, now, and the future. NAM Perspect. 2022;6(22). doi:10.31478/202206e
162. Merchant R, Torous J, Rodriguez-Villa E, Naslund JA. Digital technology for management of severe mental disorders in low-income and middle-income countries. Curr Opin Psychiatry. 2020;33(5):501–507. doi:10.1097/YCO.0000000000000626
163. Hansen S, Baroody AJ. Electronic health records and the logics of care: complementarity and conflict in the U.S. healthcare system. Inf Syst Res. 2020;31(1):57–75. doi:10.1287/isre.2019.0875
164. Murphy AR, Reddy MC. Ambiguous Accountability: the Challenges of Identifying and Managing Patient-Related Information Problems in Collaborative Patient-Care Teams. In:
165. Soomro ZA, Shah MH, Ahmed J. Information security management needs more holistic approach: a literature review. Int J Inf Manag. 2016;36(2):215–225. doi:10.1016/j.ijinfomgt.2015.11.009
166. Essue BM, Kapiriri L. Priority setting for health system strengthening in low income countries. A qualitative case study illustrating the complexities. Health Syst. 2021;10(3):222–237. doi:10.1080/20476965.2020.1758596
167. Siddiqi S, Mataria A, Rouleau KD, Iqbal M, eds. Transforming Health Systems: confronting Challenges, Seizing Opportunities. In: Making Health Systems Work in Low and Middle Income Countries: Textbook for Public Health Practitioners. Cambridge University Press; 2022:225–593. https://www.cambridge.org/core/product/047CE795800CE3822AF85E2F067EE74B.
168. Holden RJ. Social and personal normative influences on healthcare professionals to use information technology: towards a more robust social ergonomics. Theor Issues Ergon Sci. 2012;13(5):546–569. doi:10.1080/1463922X.2010.549249
169. Akers RL, Jennings WG. Social Learning Theory. In: Piquero AR, editor. The Handbook of Criminological Theory.
170. Laukka E, Huhtakangas M, Heponiemi T, Kanste O. Identifying the roles of healthcare leaders in HIT implementation: a scoping review of the quantitative and qualitative evidence. Int J Environ Res Public Health. 2020;17(8):2865. doi:10.3390/ijerph17082865
171. Murrell AJ, Blake-Beard S, Porter DM. The importance of peer mentoring, identity work and holding environments: a study of African American leadership development. Int J Environ Res Public Health. 2021;18(9):4920. doi:10.3390/ijerph18094920
172. Sfantou D, Laliotis A, Patelarou A, Sifaki- Pistolla D, Matalliotakis M, Patelarou E. Importance of leadership style towards quality of care measures in healthcare settings: a systematic review. Healthcare. 2017;5(4):73. doi:10.3390/healthcare5040073
173. Zajac S, Woods A, Tannenbaum S, Salas E, Holladay CL. Overcoming challenges to teamwork in healthcare: a team effectiveness framework and evidence-based guidance. Front Commun. 2021;6:606445. doi:10.3389/fcomm.2021.606445
174. Van Diggele C, Burgess A, Roberts C, Mellis C. Leadership in healthcare education. BMC Med Educ. 2020;20(S2):456. doi:10.1186/s12909-020-02288-x
175. Raphael D, Curry-Stevens A, Bryant T. Barriers to addressing the social determinants of health: insights from the Canadian experience. Health Policy. 2008;88(2–3):222–235. doi:10.1016/j.healthpol.2008.03.015
176. Bigland C, Evans D, Bolden R, Rae M. Systems leadership in practice: thematic insights from three public health case studies. BMC Public Health. 2020;20(1):1735. doi:10.1186/s12889-020-09641-1
177. Abu-Odah H, Molassiotis A, Liu JYW. Gathering policymakers’ perspectives as an essential step in planning and implementing palliative care services at a national level: an example from a resource-limited country. BMC Palliat Care. 2022;21(1):43. doi:10.1186/s12904-022-00936-1
178. Ștefan AM, Rusu NR, Ovreiu E, Ciuc M. Empowering healthcare: a comprehensive guide to implementing a robust medical information system—components, benefits, objectives, evaluation criteria, and seamless deployment strategies. Appl Syst Innov. 2024;7(3):51. doi:10.3390/asi7030051
179. World Health Organization. Strategy for Optimizing National Routine Health Information Systems: Strengthening Routine Health Information Systems to Deliver Primary Health Care and Universal Health Coverage.
180. Bates DW, Heitmueller A, Kakad M, Saria S. Why policymakers should care about “big data” in healthcare. Health Policy Technol. 2018;7(2):211–216. doi:10.1016/j.hlpt.2018.04.006
181. McGraw D, Mandl KD. Privacy protections to encourage use of health-relevant digital data in a learning health system. Npj Digit Med. 2021;4(1):2. doi:10.1038/s41746-020-00362-8
182. Reddy S. Generative AI in healthcare: an implementation science informed translational path on application, integration and governance. Implement Sci. 2024;19(1):27. doi:10.1186/s13012-024-01357-9
183. Al Kuwaiti A, Nazer K, Al-Reedy A, et al. A review of the role of artificial intelligence in healthcare. J Pers Med. 2023;13(6):951. doi:10.3390/jpm13060951
184. Secinaro S, Calandra D, Secinaro A, Muthurangu V, Biancone P. The role of artificial intelligence in healthcare: a structured literature review. BMC Med Inform Decis Mak. 2021;21(1):125. doi:10.1186/s12911-021-01488-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Facilitators and Barriers of Integrated Care for Older Adults with Multimorbidity: A Descriptive Qualitative Study
Wu J, Xue E, Huang S, Fu Y, Chen D, Shao J, Zhang H, Tang L, Ye Z
Clinical Interventions in Aging 2023, 18:1973-1983
Published Date: 29 November 2023
Barriers and Facilitators of Early Palliative Care in the Trajectory of People Living with Chronic Condition: A Mini Review Using Socio-ecological Framework to Inform Public Health Strategy
Haroen H, Maulana S, Harlasgunawan AR, Rahmawati S, Riansyah A, Musthofa F, Pardosi JF
Journal of Multidisciplinary Healthcare 2024, 17:4189-4197
Published Date: 29 August 2024