")
Back to Journals » Clinical Ophthalmology » Volume 18
Factors Affecting Outcomes of Stereoacuity in Partially Refractive Accommodative Esotropia with Motor Success Treated by Preoperative Prism Correction and Surgery
Authors Yagasaki T , Yokoyama Y , Yagasaki A , Hozumi K, Ichikawa S
Received 24 March 2024
Accepted for publication 15 August 2024
Published 21 August 2024 Volume 2024:18 Pages 2327—2335
DOI https://doi.org/10.2147/OPTH.S470504
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Teiji Yagasaki,1,2 Yoshimi Yokoyama,2 Ayaka Yagasaki,1,2 Kenta Hozumi,2 Sho Ichikawa2,3
1Yagasaki Eye Clinic, Ichinomiya, Aichi, Japan; 2Department of Ophthalmology, Japan Community Health Care Organization Chukyo Hospital, Nagoya, Aichi, Japan; 3Chukyo Eye Clinic, Nagoya, Aichi, Japan
Correspondence: Teiji Yagasaki, Email [email protected]
Purpose: Favorable stereoacuity does not develop in all patients with partially refractive accommodative esotropia (PRAET) successfully aligned, and there have been few previous reports on the factors influencing stereoacuity outcomes in patients with PRAET treated with prismatic correction (PPC) and/or surgery. This study aimed to analyze factors affecting stereoacuity outcomes in patients of PRAET treated with PPC and surgery.
Study Design: Retrospective study.
Methods: Sixty-six patients with alignment within 10 prism diopters at final visit with PPC and surgery were included. According to the final stereoacuity, patients were grouped into the fine group (≤ 60 arcsec (“)), the coarse group (60 “<, 3000” ≤), and absent stereoacuity group. Preoperative patient characteristics were compared among three groups using analysis of variance. Comparison of final stereoacuity among three groups based on age at onset (very early: ≤ 6 months; early: > 6 months, ≤ 2 years; late: > 2 years) was carried out with the Kruskal–Wallis test.
Results: There were no differences in ages at initial PPC, at surgery, at final visit, durations of misalignment, of PPC, or after surgery; however, significant differences in ages at onset and initial visit were found. Age at onset in the absent group was significantly earlier than those of the fine and the coarse groups (p < 0.001 and p < 0.001, respectively). Moreover, of the 25 patients with age at onset > 2 years, 18 patients (72%) showed fine or coarse stereoacuity (p < 0.001).
Conclusion: Although stereoacuity outcomes in patients with early onset were poor despite of the finally successful alignments obtained with PPC and surgery, fine stereoacuity and coarse stereoacuity were obtained in 24% and 44% of patients with age at onset > 2 years.
Keywords: partially refractive accommodative esotropia, prism correction, stereoacuity, critical period, surgery
Introduction
Partially refractive accommodative esotropia (PRAET) responds only partially to full cycloplegic hyperopic correction, and any residual nonaccommodative component exceeding 8–10 prism diopters (PD) is managed with prismatic correction and/or surgery to develop stereopsis and binocularity. Although successful ocular realignment is achieved with prismatic correction and/or surgery, favorable stereoacuity does not develop in all patients with PRAET.1–8
Factors influencing the outcome of stereoacuity have been adequately analyzed for infantile and fully refractive accommodative esotropia. The association between infantile esotropia, better stereoacuity outcomes, earlier age at surgery, and shorter duration of constant misalignment has been clarified.9–11 For fully accommodative esotropia, an earlier age of onset and dawdling provision of fully hyperopic correction are thought to be poor outcomes of stereoacuity.12–18 However, there have been few reports on the factors influencing stereoacuity outcomes in patients with PRAET treated with prismatic correction and/or surgery. Iordanous et al reported that age of onset appeared to be the most important factor affecting postoperative stereoacuity in patients with PRAET from a comparison between 22 patients who achieved stereoacuity of 100 seconds of arc (“) or better and 33 patients with stereoacuity worse than 100”.2 However, their study excluded patients in which stereoacuity could not develop. Mohan and Sharma also reported that the median onset age in PRAET patients with stereoacuity was 1.50 years, which was significantly younger than 2.75 years in those with no stereopsis (p < 0.049).3 However, they did not compare patients with fine and coarse stereoacuity. Reports by Arnoldi and Kurup et al pointed out that postoperative alignment in patients with PRAET might influence the outcomes of stereoacuity, with no descriptions relating to the age at onset.1,4 Therefore, the critical period for stereoacuity development in patients undergoing PRAET remains unclear. This study aimed to analyze the preoperative factors influencing the outcomes of stereoacuity in patients with PRAET upon maintaining favorable alignment when treated with PPC and surgery.
Subjects and Methods
This study was approved by the Institutional Review Board of the Japan Community Health Care Organization, Chukyo Hospital (approval no. 2010032). All study and data collection protocols conformed to local laws, and informed consent was obtained from all the parents or guardians of the patients. All the medical procedures complied with the principles of the Declaration of Helsinki.
The medical records of 107 children diagnosed with PRAET who were treated at our institution between 2000 and 2021 were retrospectively reviewed. Patients who were diagnosed with PRAET with favorable alignment (within 10Δ of orthotropia) during the entire course of treatment with PA and surgery and were followed up for at least 6 months postoperatively were included in the study. Patients with deteriorated fully refractive accommodative esotropia before the initial visit were also included. Exclusion criteria were as follows: history of strabismus surgery, amblyopia, use of bifocals with a high accommodative convergence/accommodation (AC/A) ratio, extraocular muscle palsy, any vertical strabismus, overaction of oblique muscle, developmental delay, preterm birth (gestational age ≤37 weeks), Down’s syndrome, or neurologic or ocular abnormalities including nystagmus. Patients who took more than 1 month to wear glasses and/or Fresnel prisms while awake were also excluded. Finally, 66 patients were included in this study.
At the initial visit, atropine sulfate 1% was prescribed to all children, and cycloplegic refraction was routinely performed with a comprehensive evaluation within a week of the initial visit. After full hyperopic or hyperopic astigmatic correction, a diagnosis of PRAET was established if the residual esodeviation for distance and near with glasses exceeded 10Δ despite a reduction in esotropia of at least 10Δ for distance and near. As a routine examination, cycloplegic refraction was repeated at intervals of six months to one year for glass correction. Best-corrected visual acuity was measured using the Landolt C test in older children, and the Teller test or Cardiff acuity cards in infants and younger children. Bilateral amblyopia was defined as decreased bilateral visual acuity, with the better-seeing eye possessing a decimal visual acuity of 0.5 or worse in older children, and a decreased bilateral grating acuity below that of normal development in infants. Unilateral amblyopia was also defined as a difference of two or more Landolt C-lines or a difference of two or more octaves in the grating acuity between the best-corrected visual acuity values of the two eyes. The angle of deviation was primarily assessed using alternate prism and cover test (APCT). The Krimsky and Hirschberg methods were not applied to avoid angle inaccuracies.19 For patients who were too young for distance testing, measurements were performed only near. Each patient underwent at least three measurements performed by one of the authors over several weeks until reliable measurements were achieved.
Soon after establishing the diagnosis of PRAET, each patient was given PPC using a Fresnel prism (FP) mounted base-out on spectacles, almost equally divided over the left and right eyes to maintain deviation within the range from orthophoria to 10Δ for residual esotropia at distance. Patients undergoing PPC were followed up for at least 6 months once they showed stable esotropia (defined as prism non-builders); if alignment with PPC exceeded 10Δ for esotropia or any exotropia at distance developed, as detected using the APCT, the prisms were changed to maintain the range from orthophoria to 10Δ of residual esotropia at distance.
Surgery was indicated if the binocular response at distance with the Bagolini striated lenses test was positive20,21 or if three repeated stable alignments were present from orthophoria to 10Δ of residual esotropia at distance after the final prism change. All patients underwent unilateral or bilateral medial rectus recession. Postoperative follow-ups were initially performed at 1, 2, 4, and 8 weeks, with the patients subsequently observed every 3–6 months, on average, until the final examination. A postoperative angle within 10Δ of orthophoria was considered indicative of favorable alignment.
Stereoacuity was measured using the Original Stereo Fly Test or Randot Stereotest (Stereo Optical, Chicago, IL, USA). All patients were grouped into the fine group (F) (≤60 arcsec (”); 7 patients), the coarse group (C) (60” <, 3000” ≤; 21 patients), and the absent group (A) (38 patients).
The following parameters were collected for statistical assessment: age at onset (constant phase), age at initial visit, age at initial PPC, age at surgery, age at final visit, duration of PPC, duration after surgery, total duration after initial visit, cycloplegic refractive error (spherical equivalent) at the initial visit and final visit, angle at near and distance fixation without glasses at initial visit and surgery, and angle at near and distance fixation with glasses at final visit. Age at onset was confirmed both by the first observation of a constant ocular misalignment by either parents or guardians and by evidence of these changes in previous photographs. Moreover, all patients were divided into three groups based on the age at onset: very early (≤6 months; 20 patients), early (>6 months, ≤2 years; 25 patients), and late-onset (>2 years; 21 patients).
Statistical analyses were performed using Microsoft Excel for Mac version 16 (Microsoft Corp., Redmond, WA, USA) and Prism 8 for macOS (GraphPad Software, Boston, MA, USA). Data collected from the three groups (F, C, and A) were statistically compared using one-way ANOVA and the Tukey–Kramer test. Comparisons of stereopsis outcomes among the three groups based on the age of onset were also performed using the Kruskal–Wallis test. The correlation between logarithmic stereoacuity and the age at onset (months) was also analyzed. Two-tailed p-values of <0.05 were considered statistically significant.
Results
A total of 66 patients, including 32 boys and 34 girls, were grouped into the F, C, and A groups with seven, 21, and 38 participants, respectively. Table 1 shows a comparison of the characteristics between the three groups. Mean ages at onset were 3.45 ± 0.75 years, 2.82 ± 2.05 years, and 1.08 ± 1.13 years in groups F, C, and A, respectively, showing significant differences (F versus C: p = 0.584, F versus A: p < 0.001, and C versus A: P < 0.001). The comparison of stereopsis outcomes among the three groups based on age at onset was significantly positive (p < 0.001) (Table 2). At final visit, fine stereoacuity was not found in 15 very early patients and 26 early patients and coarse stereoacuity was found in only 2 very early patients (13%) and 8 early patients (31%). In comparison, fine stereoacuity and coarse stereoacuity were found in 7 patients (28%) and 11 patients (44%) of 25 patients with late onset. Moreover, a significant positive correlation was found between logarithmic stereoacuity and age at onset (R = 0.590, p < 0.001) (Figure 1). From those results, it may be very hard to obtain fine stereoacuity (≤60”) for patients with age at onset ≤2 years. Especially, stereoacuity outcomes in patients of PRAET with age of very early onset ≤6 months were poor, even if final alignments were successfully obtained with PPC and surgery.
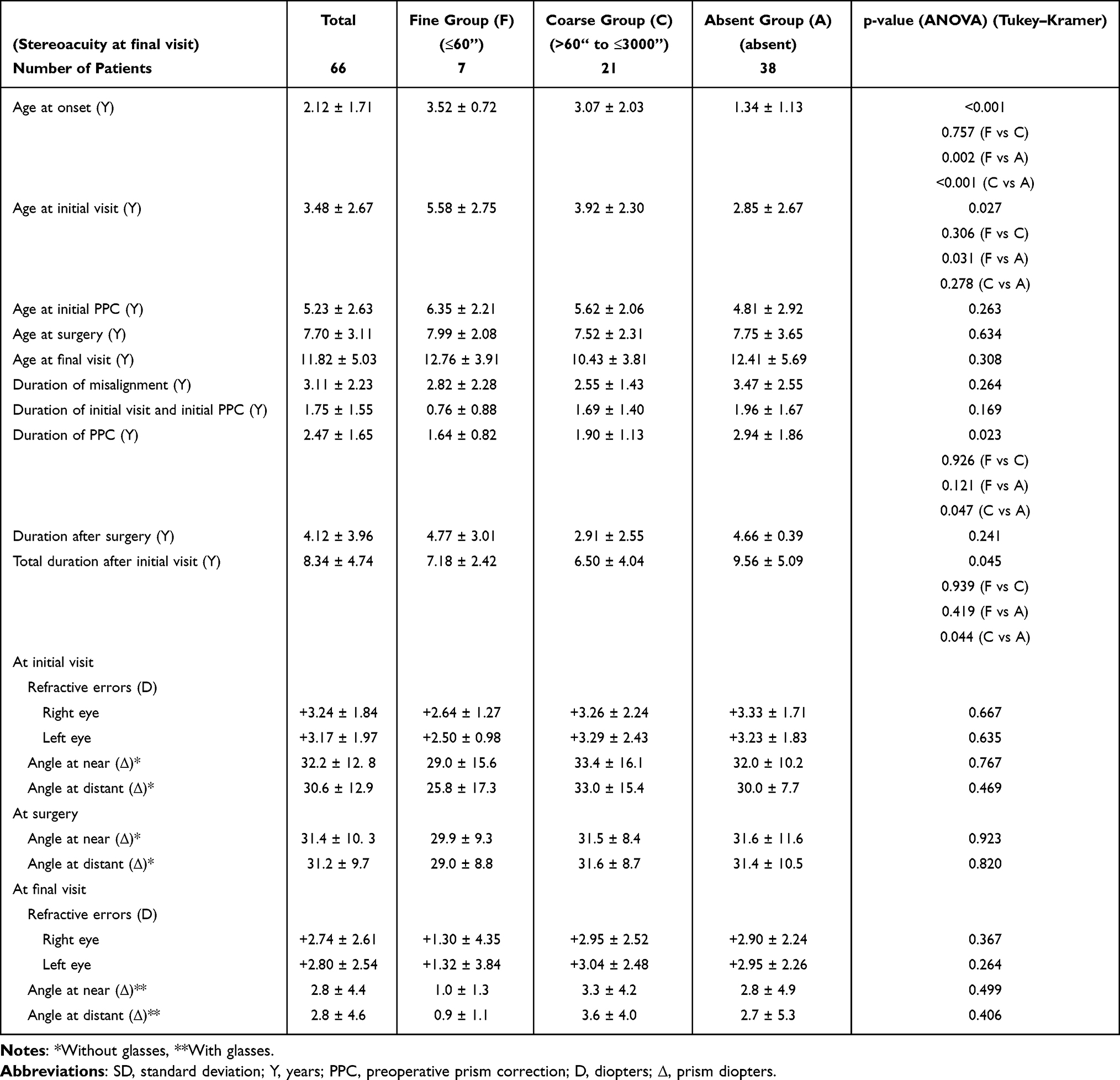 |
Table 1 Characteristics of Patients with Partially Refractive Accommodative Esotropia (Mean ± SD) |
 |
Table 2 Comparison of Stereopsis Outcomes Among Three Groups Based on Age at Onset (%) |
 |
Figure 1 Correlation between stereoacuity and age of onset. A significant positive correlation between logarithmic stereoacuity and age at onset was found. |
Mean age at the initial visit was 5.58 ± 2.67 years, 3.92 ± 2.30 years, and 2.85 ± 2.67 years in groups F, C, and A, respectively, showing significant differences (F versus C: p = 0.306, F versus A: p = 0.031, and C versus A: p = 0.278). However, no differences were found among the 3 groups in terms of age at the initial PPC, duration of the initial visit and the initial PPC, age at surgery, and age at the final visit. No significant positive correlation was found between logarithmic stereoacuity and misalignment duration (R = 0.063, p = 0.618) (Figure 2). Comparisons of the duration of misalignment and the total duration after the initial visit between the three groups also showed no differences. However, the duration of PPC and total duration after the initial visit in group A were significantly longer than those in group C (2.94 ± 1.86 years vs 1.90 ± 1.13 years; p = 0.047, 9.56 ± 5.09 years vs 6.50 ± 4.04 years; p = 0.044). These results proved that poorer stereoacuity outcomes in patients with PRAET were not influenced by age at initial PPC, age at surgery, duration of PPC, or total duration after the initial visit.
 |
Figure 2 Correlation between stereoacuity and duration of misalignment. No significant positive correlation was found between logarithmic stereoacuity and misalignment duration (R=0.063, p=0.618). |
No differences were found between the three groups in cycloplegic refractive error at the initial and final visits, angle at near and distance fixation without glasses at the initial visit and surgery, or angle at near and distance fixation with glasses at the final visit.
Discussion
Stereoacuity develops abruptly from three to four months of age, proceeds rapidly during the first year of life, and improves to 80% of the normal mature value by two years of age.10,16 During the early critical period, early onset strabismus may lead to an unfavorable prognosis for stereoacuity, even if ocular realignment is achieved with surgery or delayed glasses. It has been well documented that several factors, including age at onset, age at surgery, and duration of misalignment, have a great influence on the outcomes of stereoacuity in patients with infantile esotropia9–11 and fully refractive accommodative esotropia.12–18 However, few studies have investigated the factors affecting the outcomes of stereoacuity in patients undergoing PRAET.
Of the 108 patients in report by Arnoldi,1 40 patients (37%) had surgical success defined as a tropia within 8Δ of orthotropia, 21 patients (19%) had residual esotropia, and 47 patients (44%) had consecutive exotropia at the final visit. Although good stereopsis of at least 400 seconds of arc was found only in 14% and 13% of patients with residual esotropia and consecutive exotropia, respectively, 35% of surgically successful patients showed good stereopsis (p < 0.05, chi-square test). Furthermore, Kurup et al pointed out that postoperative alignment in patients with PRAET may influence outcomes of stereoacuity.4 However, all patients included in this study maintained their alignment within 10 prism diopters with PPC and surgery until the final visit. Therefore, the outcome of stereoacuity in this study might not have been influenced by controlling alignment during PRAET.
Some investigators have suggested an association between the age at the onset of strabismus and the stereoacuity outcome in surgically aligned patients with PRAET.2,3,5,7,8 Iordanous et al reported that the mean onset age of constant esodeviation between 24 patients showing between stereoacuity ≤100” was 31.8 ± 12.9 months, which was significantly older than 23.8 ± 10.0 months in 33 patients not achieving stereoacuity ≤100” (p = 0.012), and concluded that the age of onset beyond 30–36 months in patients with PRAET was associated with better postoperative stereoacuity. On the contrary, they also compared the effects of the duration of misalignment and the age at the surgery on the outcome of stereoacuity ≤100” in patients with PRAET but, unlike our results, they found statistical significance in those values. However, they excluded patients not achieving stereoacuity at all after surgery from their study,2 which may place limitations on the true association between the outcome of stereoacuity, duration of misalignment, and age at surgery in patients with PRAET.
Mohan and Sharma also reported that only 8 (18%) of 47 patients with PRAET had stereoacuity (60–120”) postoperatively and that the median age at onset of strabismus was 2.75 years in patients who achieved stereoacuity, which was significantly older than in those who did not, whose age was 1.5 years (P = 0.049).3 However, they measured stereoacuity with the TNO Stereo Tests containing only 4 ranges of 60′′, 120′′, 240′′, and 480′′. In the TNO Stereo Test, anaglyph red/green glasses are used to present two different images to both eyes. However, it has been known that the red/green format can introduce artifacts in binocular vision testing.22–24 Zhang et al investigated the mechanism of poorer stereoacuity using TNO Stereo Tests compared with stereo thresholds using anaglyph black/white glasses.25 Therefore, it is difficult to reliably compare stereoacuity between TNO Stereo Tests and other tests using different step ranges. In addition, coarse stereoacuity in patients with PRAET may be attributed to the absence of stereoacuity in the TNO Stereo Tests.
Recently, a significant association between the age at the onset of strabismus and the outcome of stereoacuity in surgically aligned patients with PRAET has been reported in Japan.5,8
Of the 35 patients reported by Suzuki et al, the mean age at onset of strabismus in 16 patients achieving measurable stereoacuity ≤3000” with Stereo Fly Test was 30.4 ± 13.0 months, which was significantly older than the 19 patients achieving no stereoacuity, who were of a mean age of 14.7 ± 9.4 months. They also reported that patients with an earlier age at the initial visit showed poorer stereoacuity outcomes.5 Those findings are almost the same as the results in our report. In their report, the age at surgery was another factor that affected the outcome of stereoacuity. However, in other reports, including ours, age at surgery did not have a significant effect on the stereoacuity.2–4 We strictly decided surgical timing to be a positive binocular response at distance with the Bagolini striated lenses test or three repeated stable alignments from orthophoria to 10Δ of residual esotropia at distance after the final prism change. Giaschi et al revealed that stereoacuity in the coarse range is mature at four years of age,26 and fine stereoacuity is still immature at five years of age, reaching adult levels between six and nine years of age.27 Moreover, some studies have revealed a delay in the development of the parvocellular pathway associated with fine stereoacuity during the first two years of life.28,29 Therefore, controlling alignments from orthophoria to 10Δ of residual esotropia are essential in keeping normative developments of coarse and fine stereoacuity before surgery, especially during the first two years of life from our study and report by Nishikawa et al.8
In our study, the overall rate of measurable stereopsis at the final visit was 42% (28 patients) with a significant difference between patients with age at onset of ≤2 years old (24%) and with age at onset of >2 years old (72%). Although patients with age at onset of >2 years completely retained their alignment from orthophoria to 10Δ of residual esotropia with PPC and surgery, their outcome of stereoacuity was far from ideal. As mentioned previously, stereoacuity develops abruptly from three to four months of age, proceeds rapidly during the first year of life, and improves to 80% of the normal mature value by two years of age.15,16 During the early critical period, early onset strabismus may lead to an unfavorable prognosis for stereoacuity, even if ocular realignment is achieved using glasses, PPC, or delayed surgery. In infantile esotropia, a shorter duration of misalignment and surgery before the age of 6–8 months is recommended for favorable stereopsis.9–11 Similarly, in cases of PRAET with onset within two years of age, a similar policy is required for favorable stereoacuity. A prompt initial visit soon after onset may be key to initiating ocular realignment with glasses, PPC, or surgery without delay. We advocate prompt consultation for early onset PRAET, realignment with glasses, PPC, and surgery.
This study has some limitations. In our study, the age of onset was mainly determined based on the subjective recall of parents or guardians. Physicians were unable to determine whether these children truly experienced a constant misalignment or if the misalignment was intermittent before their first visit. Moreover, it was difficult to determine when refractive accommodative esotropia corrected to <10 PD with full correction worsened over time and became PRAET. Nevertheless, younger age at onset is strongly associated with a favorable prognosis for stereoacuity and prompt initiation of ocular realignment in patients with PRAET.
Conclusion
According to the final stereoacuity, 66 patients of PRAET successfully aligned (<10 PD) with PPC and surgery were grouped into the fine group, the coarse group, and absent stereoacuity group to analyze factors affecting stereoacuity outcomes. No differences in ages at initial PPC, at surgery, at final visit, durations of misalignment, of PPC, or after surgery were found. However, significant differences in ages at onset and initial visit among three groups were found. Fine stereoacuity was not found in 15 very early patients and 26 early patients and coarse stereoacuity was found in only 2 very early patients (13%) and 8 early patients (31%). Age at onset in the absent group was significantly earlier than those of the fine and the coarse groups. Of the 25 patients with age at onset >2 years, 18 patients (72%) showed fine or coarse stereoacuity. Although stereoacuity outcomes in patients with early onset were poor despite of the finally successful alignments, fine stereoacuity and coarse stereoacuity were obtained in 24% and 44% of patients with age at onset >2 years.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author [TY], upon reasonable request.
Acknowledgments
We would like to thank Editage for English language editing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any grants or funding.
Disclosure
The authors declare that we have no conflicts of interest in this study.
References
1. Arnoldi K. Long-term surgical outcome of partially accommodative esotropia. Am Orthopt J. 2002;52:75–84. doi:10.3368/aoj.52.1.75
2. Iordanous Y, Mao A, Makar I. Preoperative factors affecting stereopsis after surgical alignment of acquired partially accommodative esotropia. Strabismus. 2015;23(4):151–158. doi:10.3109/09273972.2015.1099708
3. Mohan K, Sharma SK. Long-term motor and sensory outcomes after surgery for the nonaccommodative component of partially refractive accommodative esotropia. J AAPOS. 2018;22(5):356–360. doi:10.1016/j.jaapos.2018.06.006
4. Kurup SP, Barto HW, Myung G, Mets MB. Stereoacuity outcomes following surgical correction of the nonaccommodative component in partially accommodative esotropia. J AAPOS. 2018;22(2):92–96. doi:10.1016/j.jaapos.2017.12.003
5. Suzuki Y, Mitsukawa T, Hama Y, Tomita A, Yamada M. Preoperative factors affecting outcome after surgery of partially accommodative esotropia. J Jpn Ophthalmol Soc. 2020;124(12):987–994.
6. Jang Y, Lee HJ, Jung JH, Kim SJ. Effect of prism adaptation in patients with partially accommodative esotropia: clinical findings and surgical outcomes. Graefes Arch Clin Exp Ophthalmol. 2021;259(1):223–229. doi:10.1007/s00417-020-04902-6
7. Kim DH, Yang HK, Hwang JM. Long-term surgical outcomes of preoperative prism adaptation in patients with partially accommodative esotropia. Eye (Lond). 2021;35(4):1165–1170. doi:10.1038/s41433-020-1086-7
8. Nishikawa N, Kinouchi R, Kawaguchi Y, Fushitsu R. A retrospective evaluation of partially accommodative esotropia using preoperative prism adaptation test: surgical outcomes and investigation of prognostic factors. J Jpn Ophthalmol Soc. 2023;127(7):680–688.
9. Ing MR, Okino LM. Outcome study of stereopsis in relation to duration of misalignment in congenital esotropia. J AAPOS. 2002;6(1):3–8. doi:10.1067/mpa.2002.120172
10. Birch EE, Wang J. Stereoacuity outcomes following treatment of infantile and accommodative esotropia. Optom Vis Sci. 2009;86(6):647–652. doi:10.1097/OPX.0b013e3181a6168d
11. Yagasaki T, Yokoyama Y, Tsukui M. Relationship between stereopsis outcome and timing of surgical alignment in infantile esotropia. J AAPOS. 2020;24(2):
12. Baker JD, Parks MM. Early-onset accommodative esotropia. Am J Ophthalmol. 1980;90(1):11–18. doi:10.1016/s0002-9394(14)75070-6
13. Wilson ME, Bluestein EC, Parks MM. Binocularity in accommodative esotropia. J Pediatr Ophthalmol Strabismus. 1993;30(4):233–236. doi:10.3928/0191-3913-19930701-04
14. Mulvihill A, MacCann A, Flitcroft I, O’Keefe M. Outcome in refractive accommodative esotropia. Br J Ophthalmol. 2000;84(7):746–749. doi:10.1136/bjo.84.7.746
15. Fawcett S, Leffler J, Birch EE. Factors influencing stereoacuity in accommodative esotropia. J AAPOS. 2000;4(1):15–20. doi:10.1016/s1091-8531(00)90006-5
16. Fawcett SL, Birch EE. Risk factors for abnormal binocular vision after successful alignment of accommodative esotropia. J AAPOS. 2003;7(4):256–262. doi:10.1016/s1091-8531(03)00111-3
17. Berk AT, Koçak N, Ellidokuz H. Treatment outcomes in refractive accommodative esotropia. J AAPOS. 2004;8(4):384–388. doi:10.1016/j.jaapos.2004.02.001
18. Matsuo T, Yamane T, Fujiwara H, Ohtsuki H, Watanabe Y. Predictive factors for long-term outcome of stereoacuity in Japanese patients with pure accommodative esotropia. Strabismus. 2005;13(2):79–84. doi:10.1080/09273970590935084
19. Choi RY, Kushner BJ. The accuracy of experienced strabismologists using the Hirschberg and Krimsky tests. Ophthalmology. 1998;105(7):1301–1306. doi:10.1016/S0161-6420(98)97037-3
20. Kushner BJ, Morton GV. Postoperative binocularity in adults with longstanding strabismus. Ophthalmology. 1992;99(3):316–319. doi:10.1016/s0161-6420(92)31970-0
21. Murray AD, Orpen J, Calcutt C. Changes in the functional binocular status of older children and adults with previously untreated infantile esotropia following late surgical realignment. J AAPOS. 2007;11(2):125–130. doi:10.1016/j.jaapos.2006.10.016
22. Simons K, Elhatton K. Artifacts in fusion and stereopsis testing based on red/green dichoptic image separation. J Pediatr Ophthalmol Strabismus. 1994;31(5):290–297. doi:10.3928/0191-3913-19940901-05
23. Simons K. A comparison of the Frisby, Random-Dot E, TNO, and Randot circles stereotests in screening and office use. Arch Ophthalmol. 1981;99(3):446–452. doi:10.1001/archopht.1981.03930010448011
24. Larson WL. Effect of TNO red-green glasses on local stereoacuity. Am J Optom Physiol Opt. 1988;65(12):946–950. doi:10.1097/00006324-198812000-00005
25. Zhang Y, Meng B, Wu H. Evaluating the mechanism by which the TNO Stereo Test overestimates stereo thresholds. J Ophthalmol. 2021;18(2021):6665638.
26. Giaschi D, Narasimhan S, Solski A, Harrison E, Wilcox LM. On the typical development of stereopsis: fine and coarse processing. Vis Res. 2013;30(89):65–71. doi:10.1016/j.visres.2013.07.011
27. Blake R, Wilson H. Binocular vision. Vis Res. 2011;51(7):754–770. doi:10.1016/j.visres.2010.10.009
28. Hammarrenger B, Leporé F, Lippé S, Labrosse M, Guillemot JP, Roy MS. Magnocellular and parvocellular developmental course in infants during the first year of life. Doc Ophthalmol. 2003;107(3):225–233. doi:10.1023/b:doop.0000005331.66114.05
29. Dobkins KR, Anderson CM, Lia B. Infant temporal contrast sensitivity functions (tCSFs) mature earlier for luminance than for chromatic stimuli: evidence for precocious magnocellular development? Vis Res. 1999;39(19):3223–3239. doi:10.1016/s0042-6989(99)00020-6
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.