")
Back to Journals » Clinical Ophthalmology » Volume 19
Factors Affecting Ray Trace LASIK Data Acquisition in Clinical Practice: Options for Addressing Accommodation
Authors Thananjeyan AL, Bala C
Received 24 February 2025
Accepted for publication 13 June 2025
Published 3 July 2025 Volume 2025:19 Pages 2079—2089
DOI https://doi.org/10.2147/OPTH.S524774
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Akshaya L Thananjeyan,1,2 Chandra Bala1
1PersonalEyes, Sydney, NSW, Australia; 2Emergency Department, Sydney Hand and Eye Hospital, Sydney, NSW, Australia
Correspondence: Chandra Bala, PersonalEyes, Sydney, NSW, Australia, Tel +61 88337111, Email [email protected]
Purpose: To assess factors affecting successful data acquisition for InnovEyes guided ray trace LASIK.
Setting: Single-site ophthalmology practice.
Design: Retrospective review.
Methods: A total of 1283 eyes with myopia and myopic astigmatism were assessed over 18-months for ray trace-based LASIK planning. Preoperative measurements were acquired using the InnovEyes Sightmap (Wavelight Plus, Alcon). Scan time per eye, number of scans, pupil size, calculated refraction and manifest spherical equivalent (SEQ) refraction were assessed. In a subset of eyes with significant accommodation, aberrometry-based refraction was adjusted prior to treatment, or cycloplegic measurement was used for treatment planning. In these subsets, 3-month post-operative refractive outcomes were analysed.
Results: Mean noncycloplegic scanning time (11.10± 14.11 minutes/eye to 8.10± 3.17 minutes/eye) and number of noncycloplegic scans per eye (6.28± 2.97 scans to 5.23± 2.12 scans) decreased over time. In nine eyes where the wavefront SEQ (4 mm) was less myopic (by 0.5D or more) than the manifest SEQ and no adjustment was made, all achieved uncorrected distance visual acuity (UDVA) of 20/20 or better. In 274 eyes (21.4%), wavefront SEQ (4mm) was more myopic (by > 0.5D) than manifest SEQ. Surgeon adjusted treatment in 95 eyes to within 0.5D of manifest SEQ resulted in 98% achieving UDVA of 20/20 or greater. In 23 eyes treated using cycloplegic wavefront data, 96% achieved UDVA of 20/20 or greater.
Conclusion: Use of the InnovEyes Sightmap system for ray trace LASIK is feasible in a clinical environment but demonstrates an operator learning curve. Accommodation during wavefront measurement can occur; this can be managed through surgeon adjustment of treatment or the use of cycloplegic wavefront data.
Keywords: laser in situ keratomileusis, ray trace, higher order aberration, accommodation
Introduction
Ray trace laser in situ keratomileusis (LASIK) has demonstrated safety and efficacy in the correction of myopia and myopic astigmatism, with no clinically significant increase in total ocular higher-order aberration (HOA) and a reduction in spherical aberration.1–5 This technology generates a personalised treatment pattern for each eye by constructing a virtual model (‘eyevatar’) based on comprehensive ocular measurements, including whole-eye aberrometry, anterior and posterior corneal tomography, axial length, and anterior chamber depth. These parameters are captured in a single session using the InnovEyes Sightmap system (Alcon Laboratories, Inc) which utilises Scheimpflug technology, interferometry, and Hartmann-Shack aberrometry. The model is then virtually treated to determine the optimal ablation pattern.
To date, there have been no published reports evaluating the integration of this technology into routine clinical practice. Practical factors such as operator learning curve, time required to acquire scans, and the number of scans necessary for treatment planning may impact its utility in busy refractive surgery settings. InnovEyes Sightmap measurements are obtained under scotopic conditions over a 6.5mm treatment zone to maximize wavefront data capture. However, this dark environment, in combination with patient-specific factors such as anxiety, can induce accommodation in some individuals potentially making the wavefront-derived spherical equivalent (SEQ) appear more myopic than the manifest SEQ. Treating a wavefront measurement that is artificially more myopic due to accommodation may lead to unintended hyperopic outcomes.
The present study evaluates the usability and data acquisition characteristics of the InnovEyes Sightmap in real-world refractive clinical practice over an 18-month period. In addition, we quantify the incidence and magnitude of accommodation observed during wavefront acquisition and explore two strategies for mitigating its impact: adjustment of the SEQ and the use of cycloplegic wavefront data.
Methods and Methods
Ethics
Ethics approval for this retrospective chart review was granted by an external ethics committee (Belberry Ltd; https://bellberry.com.au), and consent to use de-identified data was obtained from patients. This study adhered to the tenets of the Declaration of Helsinki.
Patients and Surgical Protocol
A retrospective chart review of sequential eyes with myopia and myopic astigmatism in adult patients undergoing ray trace LASIK over an 18-month period was conducted at a single ophthalmology private practice. Inclusion criteria as well as surgical protocol have been previously described.1,4 Myopic adults (18 years and older) with no coexisting ocular conditions or previous ocular surgery who underwent bilateral ray trace LASIK were included. All eyes targeted emmetropia, and no nomogram adjustments were made.
Patients were initially screened at a satellite clinic or at the surgery centre. Assessment at the satellite clinic involved a subjective refraction followed by a cycloplegic refraction (45 minutes after cyclopentolate 1% administration). On the day of surgery, another subjective refraction was performed along with an InnovEyes Sightmap assessment.
Patients who were initially screened at the laser surgery centre underwent a subjective refraction, followed by InnovEyes Sightmap assessment on the same day. They then underwent cycloplegic refraction (cyclopentolate 1%). If more than a 0.5D difference from manifest refraction was noted, then over the course of clinical use in some patients, a second cycloplegic InnovEyes Sightmap wavefront measurement was repeated.
Preoperative biometry (partial coherence interferometry), tomography (Scheimpflug principle), wavefront refraction, and whole-eye aberrometry (Hartmann-Shack) data were collected using the InnovEyes Sightmap (Alcon Laboratories, Inc). Ocular higher-order aberrations (HOAs) were measured under scotopic conditions with 3 lux of illumination (measured at the patient’s temple using a light meter). In patients who underwent ray trace LASIK treatment, preoperative data from the InnovEyes Sightmap were exported to the WaveNet Server (Alcon Laboratories, Inc.) and an excimer laser (EX500, Alcon Laboratories, Inc.), and a customized ablation profile was generated for each eye.
Outcome Measurements
The visual outcomes of 400 eyes (200 OD and 200 OS) of this cohort have been previously reported.1 However, the metrics on data acquisition in eyes undergoing noncycloplegic InnovEyes assessment are presented for the first time.
For each noncycloplegic eye assessment, time per InnovEyes Sightmap assessment (wavefront aberrometry, axial length and topography), number of wavefront aberrometry scans, noncycloplegic pupil size, and wavefront refraction were recorded. For each assessment, the InnovEyes Sightmap Overview page (Figure 1) was used to calculate the number of wavefront scans per eye and time duration. Time per assessment of each eye was calculated as the duration from the start of the 1st recorded wavefront aberrometry scan to last recorded topography scan done in one assessment for each eye. Only noncycloplegic assessment time was calculated. A quality assessment of each scan is done within the InnovEyes Sightmap. A green check representing adequate measurement appears next to each assessment as seen in Figure 1 if the following criteria are met: >80% of the points are acquired and no disturbances in the wavefront image exist, pupil diameter > 6mm; pupil ellipse < 6% and wavefront refraction is within 0.5D SEQ, 0.75D cylinder and 15 degree axis of subjective refraction. For topography, eyes must be aligned appropriately, and patients must not be blinking. Alignment must be less than 0.8 along the x, y, and z axis. Eyes must additionally be open wide enough to be able to register for cyclotorsion. The manufacturer recommended a minimum of four wavefront, two axial length and two topography scans; this recommendation was higher at the introduction of the technology.
 |
Figure 1 InnovEyes Sightmap Overview Map. Overview map example showing wavefront, axial length (A-scan), and tomography measurements with associated time stamps. |
A subgroup of eyes with a scotopic pupil size of ≥6mm was assessed to examine whether HOA was comparable before and after cycloplegia with 1% cyclopentolate. Ocular wavefront data was recorded according to the convention of the American National Standards Institute.6
A subset of eyes had a less myopic wavefront SEQ at 4mm than the manifest SEQ. These patients were treated without alteration of the ray trace treatment plan. The 3-month outcomes were assessed. A subset of eyes that displayed accommodation during InnovEyes Sightmap assessment was treated in one of two ways. Firstly, the treatment plan was manually adjusted such that the 4mm treated spherical equivalent was within 0.5D of the manifest spherical equivalent refraction. The 3-month post-operative refractive outcomes of this approach were assessed. Secondly, in a second subset of patients with accommodation, the cycloplegic wavefront was captured and used for planning treatment, ignoring the noncycloplegic wavefront measurement. The patient had their tomography, axial length and registration image for eye tracking captured prior to dilation. This was then followed by post-cycloplegic wavefront measurements. The 3-month post-operative refractive outcomes of this approach were assessed.
Statistical Analysis
Statistical analysis was performed using Microsoft Excel (Microsoft Office Excel; Microsoft) and IBM SPSS Statistics (Version 29). Descriptive statistics were reported as mean ± standard deviation (SD) and range for continuous variables (e.g., SEQ, pupil size, number of scans, time per scan) and as frequencies and percentages for categorical variables.
Normality of continuous variables and paired differences (e.g., noncycloplegic vs cycloplegic HOA, amount of accommodation between eyes of individual patients) was assessed using skewness, kurtosis, and visual inspection of histograms. If the differences were normally distributed, paired t-tests were applied. If normality was not met, the Wilcoxon signed-rank test was used. Statistical significance was set at p <0.05. Where comparisons involved both eyes from the same patient, intra-subject correlation was acknowledged and interpreted with caution.
Results
One thousand two hundred eighty three eyes (647 OD, 636 OS) were identified to have undergone InnovEyes Sightmap guided ray trace-LASIK (Wavelight+, Alcon) over an 18-month period. These eyes were further assessed for usability metrics in clinical practice.
The assessment of each eye involved 5.23±2.12 wavefront aberrometer scans and decreased from 6.28±2.97 over an 18-month period (Figure 2A). The time taken to measure all the wavefront, topography and a-scans for each eye was initially about 11.10±14.11 minutes/eye and reduced to 8.10±3.17 minutes/eye over 18 months (Figure 2B). There were periodic increases in scanning times depending on the introduction of new staff.
 |
Figure 2 InnovEyes Sightmap acquisition over an 18 month period (1283 eyes). (A) Mean number of non-cycloplegic wavefront scans per eye (error bars: SD) (B) Mean total time required to acquire wavefront, a-scan and tomography data per eye (error bars: SD) (C) Maximum noncycloplegic pupil size per eye. Abbreviation: SD, standard deviation. |
Mean noncycloplegic pupil size was 6.18±0.84mm (range: 3.16–8.70mm). Maximum pupil size per eye was ≥5mm in 96.4% of cases (Figure 2C). Despite scotopic conditions, 3.6% of eyes were not able to achieve a pupil size of ≥5mm without cycloplegia.
A non-cycloplegic scotopic pupil size of ≥6.5mm at InnovEyes Sightmap measurement, which is greater than the treatment optical zone, was noted in 47.1% of eyes. To assess whether cycloplegia (cyclopentolate 1%) impacts ocular HOA, a cohort of eyes (n=102, 58 patients) which achieved ≥ 6mm pupil size and underwent both noncycloplegic and cycloplegic wavefront measurements at the refractive surgery centre was examined. The mean noncycloplegic and cycloplegic pupil size per eye were 6.87±0.49mm (range: 6.03–8.07) and 8.07±0.53mm (range: 6.85–9.68), respectively. No significant difference was observed between noncycloplegic and cycloplegic RMS values (@6mm) for 3rd, 4th, 5th, and 6th order and total HOAs (Figure 3). On sub-analysis of each aberration (@6mm), there was no significant difference between the different aberrations except for a small but statistically significant difference in secondary coma, Z5−1 (0.00 ±0.02 before and −0.01 ±0.03 after cycloplegia, p=0.02) and secondary spherical aberration, Z6° (0.01 ±0.02 before and 0.00 ±0.02 after cycloplegia, p<0.001) at 6mm (Figure 4).
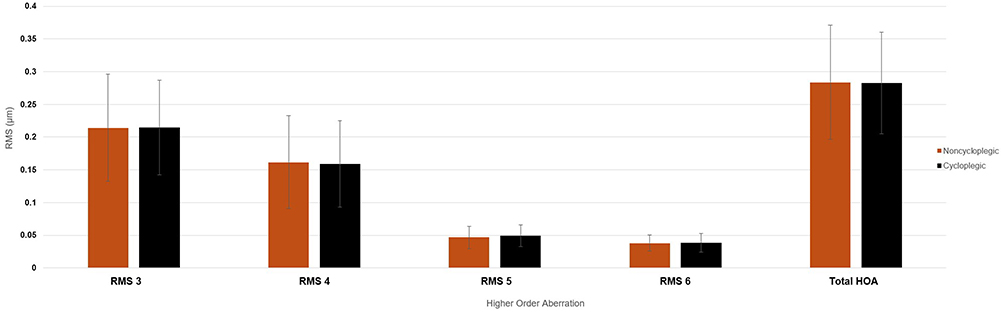 |
Figure 3 Comparison of higher order aberrations under noncycloplegic and cycloplegic conditions using InnovEyes Sightmap (102 eyes, 58 patients) (error bars: standard deviation). |
 |
Figure 4 Sub-analysis of ocular higher order aberration under noncycloplegic and cycloplegic conditions using InnovEyes Sightmap (102 eyes, 58 patients) (error bars: standard deviation). *=statistically significant (p<0.05). |
Accommodation During Wavefront Assessment
The average difference between manifest SEQ and wavefront SEQ refraction was 0.28±0.39D (range: −1.28 to 4.35). The wavefront SEQ (@4mm) was 0.5 D or less myopic than manifest SEQ in 1.0% of eyes (n=13) and >0.5D myopic in 21.4% of eyes (n=274) (Figure 5A). Accommodation from 0.50 to 0.74D and from 0.75D to 0.99D was seen in 12.8% and 5.2% of eyes, respectively. Accommodation of 1D or more was noted in 3.5% of eyes. When assessing both eyes of an individual patient, there is no significant difference between the eyes in the amount of accommodation (p=0.27; Figure 5B); however, in individual cases, there were large differences (OD 0.27±0.40D; range: −1.28–4.35 vs OS 0.29±0.39D; range: −0.81–3.68).
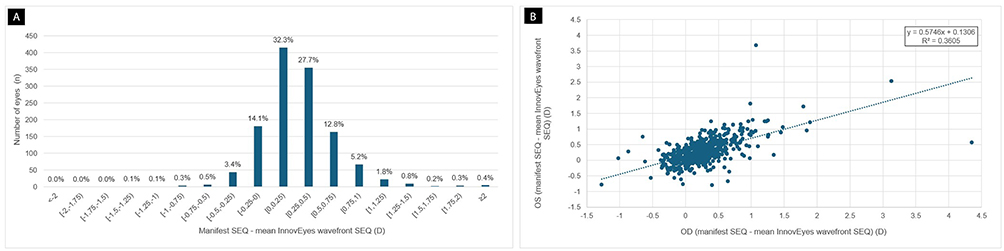 |
Figure 5 Manifest and wavefront spherical equivalent (SEQ). (A) Distribution of SEQ differences (manifest minus wavefront) (B) Inter-eye comparison of SEQ difference per patient (right - OD vs left - OS). |
Eyes with Less Myopic Wavefront SEQ Than Manifest SEQ
In eyes with wavefront SEQ (@4mm) less myopic than manifest SEQ by 0.5D or more (n=13), the wavefront-based treatment was applied without adjustment. In this group, nine eyes (8 patients, 4 OD and 5 OS) had post-operative follow-up available at 3 months (Figure 6A–D). All eyes achieved 20/20 or better vision, and 8/9 eyes achieved 20/16 or better (Figure 6A). In this small cohort, 2/9 eyes gained one or more lines of corrected distance visual acuity (CDVA) and no eyes lost Snellen lines of CDVA (Figure 6C).
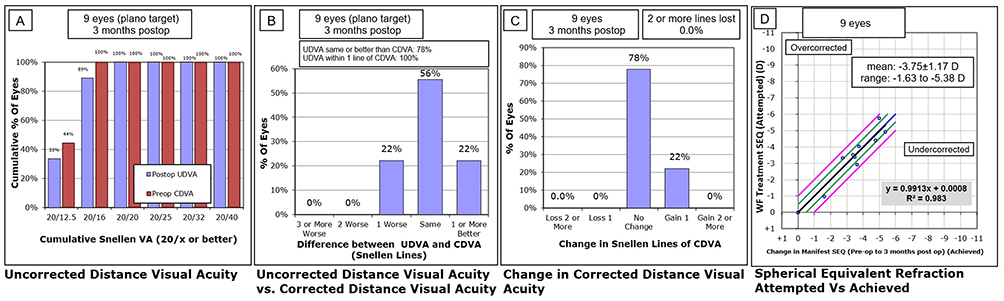 |
Figure 6 Three months post operative outcomes where wavefront SEQ was ≥0.5 D less myopic than manifest SEQ (unadjusted treatment) (9 eyes, 8 patients) (A) Cumulative postoperative UDVA vs preoperative CDVA. (B) Line difference between postoperative UDVA and preoperative CDVA. (C) Change between preoperative and postoperative CDVA. (D) Attempted vs achieved SEQ. Abbreviations: SEQ, spherical equivalent refraction; UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity; VA, visual acuity; D, dioptre, WF, wavefront. |
Eyes Demonstrating Accommodation
Eyes with more myopic wavefront SEQ than manifest refraction by >0.5D (274 eyes) due to accommodation were corrected depending on where they had their initial assessment. If the patient underwent cycloplegic refraction at a satellite practice, then they could not undergo cycloplegic assessment on the day of surgery. Post-operative outcomes of 23 eyes (one eye per patient) which underwent cycloplegic wavefront treatment and 95 eyes (one or both eyes per patient) which had surgeon adjusted treatment were further assessed. One hundred thirty-three eyes were excluded as the patients did not attend the 3-month follow-up.
Surgeon Adjustment of SEQ
Ninety-five eyes (39 OD, 56 OS, 74 patients) had their wavefront SEQ refraction (@ 4mm pupil) adjusted to within 0.5D of manifest SEQ. The spherical component was modified, without a standardised process advised by the manufacturer or adjustment based on a nomogram. At 3-months following surgery 98% of eyes achieved uncorrected distance visual acuity (UDVA) of 20/20 vision or better (Figure 7A). One-third (34%) of eyes gained one or more lines of UDVA when compared with preoperative CDVA (Figure 7B). No eyes lost two or more lines of CDVA (Figure 7C). After adjustment, 90.5% of eyes achieved within 0.5D of emmetropia (Figure 7D). If adjustment had not been made in this cohort, there would have been a potential overcorrection (shown in Figure 7E).
 |
Figure 7 Three month post operative refractive outcomes after surgeon adjustment for accommodation related instrument myopia (95 eyes, 74 patients). (A) Cumulative postoperative UDVA vs preoperative CDVA. (B) Line difference between postoperative UDVA and preoperative CDVA. (C) Change between preoperative and postoperative CDVA. (D) Attempted vs achieved SEQ (E) Pre-operative manifest SEQ vs uncorrected wavefront SEQ. Abbreviations: SEQ, spherical equivalent refraction; UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity; VA, visual acuity; D, dioptre, WF, wavefront. |
Cycloplegic Wavefront Based Treatment
A cohort of 46 eyes from 23 patients who were found to have accommodation during assessment underwent cycloplegic wavefront treatment. One eye from each patient was assessed post-operatively due to inter-eye correlation (12 OD and 11 OS) (Figure 8). Ninety-six percent achieved UDVA of 20/20 or greater. Two eyes gained one or more lines of UDVA compared to CDVA. No eyes lost two or more lines of CDVA. About 91.3% of eyes achieved within 0.5D of emmetropia.
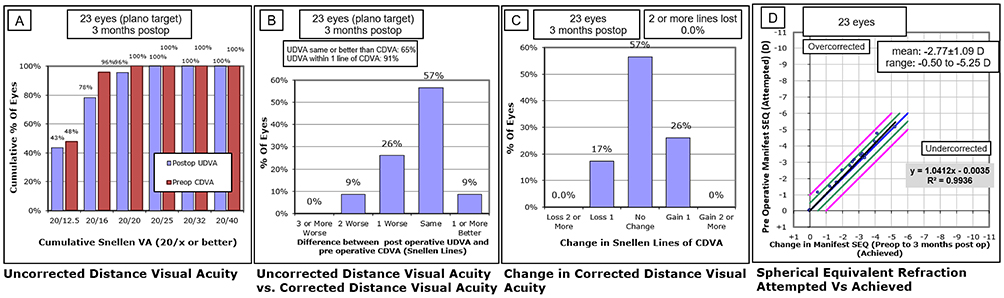 |
Figure 8 Three month post operative outcomes in eyes treated using cycloplegic wavefront data (23 eyes, 23 patients). (A) Cumulative postoperative UDVA vs preoperative CDVA. (B) Line difference between postoperative UDVA and preoperative CDVA. (C) Change between preoperative and postoperative CDVA. (D) Attempted vs achieved SEQ. Abbreviations: SEQ, spherical equivalent refraction; UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity; VA, visual acuity; D, dioptre, WF, wavefront. |
Discussion
This is the first study to report real-world usability and clinical considerations for InnovEyes Sightmap guided ray trace LASIK (Alcon) in a large cohort. While scan acquisition using this system is feasible in clinical practice, operator familiarity, accommodative variability and pupil size can significantly influence scan quality and subsequent treatment accuracy.
The adoption of new technology requires a change in workflow, the setup of the testing room and a change in the skills of operators. In the present study, a single device was set up, and initial scan acquisition time exceeded ten minutes per eye but improved to eight minutes with operator learning. This reduction was also aided by manufacturer-advised reduction in the number of required wavefront scans (four wavefront measurements) (Figure 2A). Periodic increases in acquisition time reflected staff turnover and training phases (Figure 2B), such as at months five and six. Once enough experience/familiarity was gained, the time to complete a set of scans reduced to 8.10±3.17 minutes/eye. This highlights the learning curve and importance of standardised staff training with the implementation of this technology.
The scans were undertaken in a darkroom to achieve a wide pupil for wavefront capture over a large diameter; however, this may exacerbate accommodation. In this relatively dark environment, staff play a role in aiding patient relaxation and reducing accommodation. Techniques used included asking the patient to look beyond the fixation target within the device and turning off automatic fogging. The patient was provided a target and asked to focus beyond the target. If they were still accommodating, manual fogging was undertaken. The target was moved away gradually to relax accommodation, while the patient was asked to maintain focus. All these techniques helped acquire scans with wavefront SEQ (@4mm) within 0.5D of manifest refraction in the majority of patients.
Scotopic pupil size in our study averaged 6.18±0.84mm (range: 3.16–8.70 mm), consistent with the prior literature (6.15–6.98mm and range from 3.20mm-9mm).7–10 Ninety-six percent of our cohort achieved a pupil size of 5mm or greater, the minimum requirement for a 6.5mm treatment zone. The ray trace algorithm in the device allows an extrapolation of wavefront data by a 1.5mm larger diameter than the measured diameter. However, despite utilising scotopic settings, some eyes were unable to dilate to appropriate levels for assessment. In these cases, pharmacologic dilation or non-ray trace LASIK may be more appropriate. It can be argued that if the pupil is not going to dilate in scotopic conditions, then there is limited value in treating HOA at a 6.5mm zone. The patient may get the same outcome as with a more traditional pattern of treatment. The alternate strategy is to capture a cycloplegic exam for treatment planning. In a subset of eyes with large noncycloplegic scotopic pupils (6mm or greater), cycloplegia did not significantly alter total, 3rd, 4th 5th, or 6th order ocular HOAs (Table 1, Figures 3 and 4), supporting previous studies.11,12
 |
Table 1 Preoperative Cycloplegic and Noncycloplegic Pupil Ocular Higher-Order Aberration |
Approximately 47% of eyes were able to achieve minimum pupil sizes of 6.5mm or greater during noncycloplegic assessment (Figure 2C). In those eyes where the pupil size is greater than the optical zone of 6.5mm, patients may experience postoperative symptoms of halos and glare, particularly in dim settings, and this is a known weakness irrespective of refractive surgery technique.13 This was not specifically examined in the present study. Symptoms of glare and halo have been reported to be higher in those with larger pupils in the early post-operative period.13 However, this reduces with time and post-operative recovery and pupil size is not significantly associated with visual performance.7 Future studies involving questionnaires would be beneficial to examine the influence of the 6.5mm optical zone treatment on patients with large scotopic pupils.
In the absence of accommodation, wavefront refraction is thought to be as accurate as manifest refraction. However, wavefront aberrometers have been reported to produce higher sphere, cylinder and SEQ values as compared to manifest values owing to accommodation.14,15 Accommodation during noncycloplegic wavefront measurement led to a more myopic SEQ in 21.4% of eyes (>0.5 D difference from manifest SEQ), a phenomenon consistent with instrument myopia. The mean difference is comparable to previous reports with wavefront analysers (0.3D).14 Interestingly, in 1% of eyes, the wavefront SEQ @4mm was lower than the manifest SEQ. It is possible that these patients were accommodating during this manifest refraction but do not accommodate all the time. Another possible explanation is that the wavefront refraction is a mathematical derivative of lower and higher-order components at 4mm and therefore is not to be considered an exact copy of manifest refraction. In the present study, this small cohort was treated without adjustment, and unaided vision of 20/20 was achieved in all eyes. This indirectly validates the wavefront measurement and ray trace algorithm, suggesting that perfect agreement between wavefront and manifest SEQ is not always necessary.
In the present study, the majority of accommodating eyes were between 0.5 and 0.74D (12.8%) and between 0.75 and 0.99D (5.2%). A small cohort could accommodate >1D (3.5%). There was no significant difference in the amount of accommodation between eyes; however, there were some patients with large differences which could potentially be due to anxiety during measurement (Figure 5). It is clear the amount of accommodation cannot be assumed to be the same between eyes of the individual for treatment planning. Due to these differences in accommodation between eyes, both eyes of patients were included in post-operative assessment.
If accommodation is not accounted for in treatment planning, significant overcorrection can occur. Figure 7E shows the potential for overcorrection by comparing the accommodated wavefront refraction SEQ and the manifest refraction SEQ. There would be three choices in these patients; keep repeating scans, utilise other traditional treatment patterns using the manifest refraction or adjust the wavefront refraction. In everyday practice, repeating scans leads to increase in patient anxiety, and therefore, two clinical approaches were used to mitigate accommodation-related overcorrection: adjusting the 4mm wavefront SEQ to within 0.5D of manifest refraction or using the cycloplegic wavefront.
In 95 eyes undergoing surgeon adjustment, the wavefront SEQ was adjusted to within 0.5D of manifest SEQ. 90.5% of eyes achieved a postoperative outcome within 0.5D of emmetropia and no eyes lost more than one line in CDVA. Figure 7D suggests that approximately 12 eyes were >0.5D over corrected and greater adjustment could have been made to improve the outcome. This adjustment is not a nomogram adjustment but an individual clinical decision.
The alternative approach to surgeon adjustment is to utilise cycloplegic wavefront data for treatment planning. This could only be done in patients who presented to the surgical centre for preoperative workup and were noted to accommodate despite operator assistance. In these patients, the iris registration image was acquired first followed by cycloplegic wavefront. Clinicians considering the use of cycloplegia may be concerned about the impact of cycloplegia on HOA. As previously discussed, this study showed no significant differences in 3rd, 4th, 5th, and 6th order RMS as well as total HOA at a 6mm optical zone between noncycloplegic and cycloplegic scans in a cohort of eyes, naturally achieving a pupil size of 6mm or greater. There does not appear to be a shift in spherical aberration, astigmatism or coma. This cohort was chosen as the wavefront was already available at the 6mm zone; therefore, a direct comparison between pre and post cycloplegia was possible. If cohort of eyes with small pupils were dilated for this comparison, there would be additional wavefront data once the pupil was dilated; therefore, there would never be any agreement. Recommendations against mydriatic use when the pupil size is greater than 6mm have been made for appropriate refractive error assessment.16 Furthermore, no benefit of pharmacological dilation in spherical accuracy has been reported in a cohort with pupil size greater than 6.3mm.17 The present data shows that dilation with cyclopentolate did not alter the HOAs in a clinically meaningful manner.
There are two concerns with using cycloplegic wavefront measurements. Firstly, the laser determines vertex position based on the pupil centre. In the ideal setting during ablation, the pupil size has to be within 20% of the pupil diameter of the registration image. This ensures the treatment is applied correctly at the corneal vertex. Dilating the pupil can change the pupil centre, and the laser may not be accurate in finding the vertex. In the present study, the registration image was taken prior to cycloplegia, and the cycloplegic wavefront measurements were completed thereafter. The second concern is that cyclopentolate would relax accommodation and post-operatively, if the patient has a basal tone of accommodation, this will appear as an undercorrection to the patient.
In 23 eyes undergoing cycloplegic wavefront-based treatment, 91.3% of eyes achieved a postoperative outcome within 0.5D of emmetropia and no eyes lost more than one line in CDVA. No eyes had an undercorrection (Figure 8D). However, these eyes may not have had a basal tone of accommodation. The cohorts are too small to determine which of the two techniques is superior (adjusting treatment SEQ or using cycloplegic wavefront); however, it is clear that both can be potentially clinically utilised.
Limitations of this study include being conducted at a single center, with a relatively short follow-up period and small sample sizes in key subgroups, particularly those involving cycloplegic wavefront treatment. The exclusion of eyes without 3-month follow-up introduces potential selection bias, which may affect the generalisability of the findings. Additionally, while this study highlights a learning curve associated with scan acquisition, it does not quantify the time required for individual operators to become proficient, which could be explored in future usability-focused research. Larger, prospective, and randomized studies are needed to validate these findings, particularly to assess postoperative outcomes and guide clinical practice. In patients with small scotopic pupils, the role of cycloplegic wavefront data warrants further investigation. Further studies will help guide best practices in the use of InnovEyes-guided ray trace LASIK and refine treatment planning for patients at risk of accommodation-induced refractive shifts.
Conclusions
InnovEyes Sightmap assessment and ray trace-guided LASIK are practical and implementable in real-world clinical practice. The integrated single-device platform enables efficient acquisition of all required preoperative data within seven to nine minutes per eye, with assessment time improving as operator experience increases. Accommodation during measurement is a recognised challenge but can be effectively managed either by surgeon-led adjustment of the treatment refraction or by modifying the acquisition process, including the use of cycloplegic wavefront measurements.
Funding
No funding was received for this study.
Disclosure
CB is a consultant for Alcon and J&J. CB also reports personal fees from Cambium Bio, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. He G, Bala C. Ray tracing guided myopic laser in situ keratomileusis - real world clinical outcomes. J Cataract Refract Surg. 2023;49:1140–1146. doi:10.1097/j.jcrs.0000000000001286
2. Kanellopoulos AJ. Initial outcomes with customized myopic LASIK, guided by automated ray tracing optimization: a novel technique. Clin Ophthalmol. 2020;14:3955–3963. doi:10.2147/OPTH.S280560
3. Kanellopoulos AJ, Maus M, Bala C, et al. International multicenter, myopic and myopic astigmatism femto LASIK, customized by automated ray-tracing ablation profile calculation: a postmarket study. Clin Ophthalmol. 2024;18:525–536. doi:10.2147/OPTH.S435581
4. Thananjeyan AL, Bala C. Higher-order aberrations following ray trace LASIK and the impact of eye movement on coma. Clin Ophthalmol. 2024;18(null):3389–3398. doi:10.2147/OPTH.S497131
5. Cummings AB, Kelly GE. Optical ray tracing-guided myopic laser in situ keratomileusis: 1-year clinical outcomes. Clin Ophthalmol. 2013;7:1181–1191. doi:10.2147/OPTH.S44720
6. American National Standard for Ophthalmics: methods for reporting optical aberrations of eyes. American National Standards Institute;2022.
7. Chan A, Manche EE. Effect of preoperative pupil size on quality of vision after wavefront-guided LASIK. Ophthalmology. 2011;118(4):736–741. doi:10.1016/j.ophtha.2010.07.030
8. Zhou Y, He X, Liu Z, et al. Agreement and repeatability of scotopic pupil size measurement with the 2WIN-S portable refractor in Chinese adults. Sci Rep. 2024;14(1):15650. doi:10.1038/s41598-024-66540-w
9. Chaidaroon W, Juwattanasomran W. Colvard pupillometer measurement of scotopic pupil diameter in emmetropes and myopes. Japanese J Ophthalmol. 2002;46(6):640–644. doi:10.1016/S0021-5155(02)00556-7
10. Colvard M. Preoperative measurement of scotopic pupil dilation using an office pupillometer. J Cataract Refract Surg. 1998;24(12):1594–1597. doi:10.1016/S0886-3350(98)80348-9
11. Kirwan C, O’Keefe M, Soeldner H. Higher-order aberrations in children. Am J Ophthalmol. 2006;141(1):67–70. doi:10.1016/j.ajo.2005.08.031
12. Awwad ST, El-Kateb M, McCulley JP. Comparative higher-order aberration measurement of the LADARWave and Visx WaveScan aberrometers at varying pupil sizes and after pharmacologic dilation and cycloplegia. J Cataract Refract Surg. 2006;32(2):203–214. doi:10.1016/j.jcrs.2005.08.058
13. Schallhorn SC, Kaupp SE, Tanzer DJ, Laurent J, Tidwell J, Bourque LB. Pupil size and quality of vision after LASIK. Ophthalmology. 2003;110(8):1606–1614. doi:10.1016/S0161-6420(03)00494-9
14. Cervino A, Hosking SL, Rai GK, Naroo SA, Gilmartin B. Wavefront analyzers induce instrument myopia. J Refract Surg. 2006;22(8):795–803. doi:10.3928/1081-597X-20061001-10
15. Refai A, Ismail AI, Ammar HG, EMJSMJ M. A comparative study between manifest, cycloplegic and wavefront refraction in myopia. Sohag Med J. 2018;22:9–16. doi:10.21608/smj.2018.31118
16. Giessler S, Hammer T, Duncker GIW. Aberrometry due dilated pupils--which mydriatic should be used? Klinische Monatsblatter fur Augenheilkunde. 2002;219(9):655–659. doi:10.1055/s-2002-35170
17. Subbaram MV, MacRae SM. Does dilated wavefront aberration measurement provide better postoperative outcome after custom LASIK? Ophthalmology. 2006;113(10):1813–1817. doi:10.1016/j.ophtha.2006.05.018
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.