")
Back to Journals » Infection and Drug Resistance » Volume 18
Five-Year Prospective Follow-Up of Patients with Hepatitis C Virus Infection Treated with Direct-Acting Antiviral Agents
Authors Zhang Y, Xia H, Fan L, Jiang L, Yang B, Wang F
Received 28 August 2024
Accepted for publication 11 January 2025
Published 24 January 2025 Volume 2025:18 Pages 455—471
DOI https://doi.org/10.2147/IDR.S487414
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor M. Mora-Montes
Yaping Zhang,1,2,* Huan Xia,3,* Luchang Fan,1 Lu Jiang,4 Bin Yang,2 Fengmei Wang4,5
1The Third Central Clinical College of Tianjin Medical University, Tianjin Medical University, Tianjin, 300170, People’s Republic of China; 2Tianjin Key Laboratory of Extracorporeal Life Support for Critical Diseases, Institute of Hepatobiliary Disease, Nankai University Affiliated Third Central Hospital, Tianjin, 300072, People’s Republic of China; 3Department of Infectious Diseases, Tianjin Second People’s Hospital, Tianjin, 300192, People’s Republic of China; 4Department of Hepatology and Gastroenterology, Tianjin First Central Hospital, Tianjin, 300192, People’s Republic of China; 5Tianjin Key Laboratory of Molecular Diagnosis and Treatment of Liver Cancer, Tianjin First Central Hospitial, Tianjin, 300192, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fengmei Wang; Bin Yang, Email [email protected]; [email protected]
Purpose: The research intended to present prospective data on the long-term prognosis of individuals with hepatitis C virus (HCV) infection who received direct-acting antiviral agent (DAA) treatment.
Patients and Methods: Patients who received DAA treatment at Tianjin Third Central Hospital and Tianjin Second People’s Hospital were prospectively enrolled and subsequently underwent a longitudinal follow-up. This research monitored occurrences of virological relapse, hepatocellular carcinoma (HCC), mortality, and liver disease progression. The annualized incidence rates (AIRs), cumulative incidence rates of adverse events and risk factors were investigated. Changes in liver stiffness measurement (LSM), aspartate aminotransferase-to-platelet ratio index (APRI) score, fibrosis-4 (FIB-4) index, as well as the albumin-bilirubin (ALBI) scores were also documented.
Results: A total of 862 individuals were followed up for 4.86 (P25, P75; 4.48, 5.48) years. The proportion of all participants with undetectable HCV-RNA exceeded 98% at all follow-up time points. Patients experienced virological relapse, HCC, death and disease progression with a cumulative AIRs of 1.03% (95% confidence interval [CI] 0.6– 1.5), 1.76% (95% CI 1.2– 2.3), 1.51% (95% CI 1.0– 2.0), and 5.81% (95% CI 4.8– 6.8), respectively. Cirrhotic patients were at a heightened risk of virological relapse (adjusted hazard ratio [aHR] 3.20, 95% CI 1.59– 9.75; p = 0.016), HCC (aHR 6.57, 95% CI 2.66– 16.28; p < 0.0001), and unfavorable prognosis (aHR 6.93, 95% CI 2.56– 18.74; p < 0.0001). Additionally, patients with diabetes faced an elevated risk of HCC (aHR 2.33, 95% CI 1.05– 5.15; p = 0.038) and poor prognosis (aHR 2.72, 95% CI 1.13– 6.55; p = 0.026). Furthermore, liver stiffness measurement (LSM) exhibited a significant decrease compared to baseline. Additionally, patients in the cirrhosis group showed reductions in APRI score, FIB-4 index and ALBI score to different degrees.
Conclusion: Cirrhotic patients exhibited increased susceptibility to virological relapse, HCC, unfavorable prognosis, and liver disease progression following DAA treatment. Consequently, it is imperative to implement a rigorous monitoring protocol for all cirrhotic patients after DAA treatment.
Keywords: chronic hepatitis C, cirrhosis, direct-acting antiviral agents, sustained virologic response, follow-up
Introduction
Chronic hepatitis C virus (HCV) infection has historically been a prominent contributor to developing hepatocellular carcinoma (HCC) and liver-related mortality, a trend that shifted to introduce direct-acting antivirals (DAAs) to China.1 And DAAs’ advent has significantly transformed the management of HCV infection, yielding a notable sustained virologic response (SVR) in individuals suffering from advanced liver disease, irrespective of genotype or previous treatment experience.
During the era of DAAs, real-world SVR rates within Asian populations varied from 85% to nearly 100%, influenced by factors such as HCV genotype, cirrhosis status, and history of prior HCC.2 The elimination of HCV has been documented to halt the advancement of cirrhosis or even reverse early-stage cirrhosis, which is a notable contributing cause to HCC. As a result, this helps delay advancement of liver disease to its terminal stage, prevents liver-related fatalities, and diminishes the likelihood of developing HCC.3,4 Nonetheless, the cessation of viral clearance post liver disease progression may prove challenging, particularly in individuals with advanced cirrhosis. While successfully treated patients experience sustained virologic responses and enhanced liver function, they continue to face a risk to develop HCC with extended follow-up after DAA treatment. Existing studies have indicated that achieving SVR diminishes the likelihood of hepatic decompensation and HCC, leading to improved survival outcomes.5–7Even with the increasing successful treatment of HCV cases using DAAs in recent years, the occurrence of HCC remains high in cirrhotic patients.8 Regrettably, the adoption of DAA treatment in China still lags. The absence of real-world, prospective, long-term follow-up data, particularly towards cirrhotic patients, has restricted our comprehension of HCV treatment and its effectiveness.
This study was designed to provide prospective data on the long-term prognosis of HCV-infected patients treated with DAAs who achieve SVR. The incidence of virological relapse, de novo hepatocellular carcinoma (HCC), death and progression of liver disease were all monitored. The annualized incidence rates (AIRs) and accumulative incidence rates of adverse events were analyzed, and risk factors were studied. Changes in liver stiffness measurement (LSM), aspartate aminotransferase-to-platelet ratio index (APRI) score, fibrosis-4 (FIB-4) index, and albumin-bilirubin (ALBI) scores were also recorded during the follow-up period. Our study has strong implications for the long-term prognosis of cirrhotic patients with HCV infection treated with DAAs.
Material and Methods
Study Design and Population
This multi-centred and observational cohort study included consecutive adult individuals (aged over 18 years) diagnosed with chronic HCV infection as well as undergoing treatment with DAAs from March 2018 to December 2019 within Tianjin Third Central Hospital and Tianjin Second People’s Hospital. Chronic HCV infection was defined as serum HCV RNA detected by the COBAS TaqMan HCV kit for more than 6 months.
The presence of liver cirrhosis was confirmed through the following criteria: (1) liver biopsy; (2) LSM (>12.5 kPa) or transient elastography [>1.8 m/s for ultrasound (US) and >7 kPa for Magnetic Resonance Imaging (MRI)]; (3) liver imaging examinations indicating cirrhosis-related features; (4) platelet count <120; (5) clinical manifestations (ascites, varices, encephalopathy). The exclusion criteria comprised: (1) co-infection with Hepatitis B virus (HBV) or Human Immunodeficiency Virus (HIV); (2) voluntary withdrawal from treatment for reasons unrelated to medication; (3) treatment duration of fewer than 12 weeks; (4) missing data; (5) dropout from follow-up; as well as (6) prior use of DAA treatment.9
These APRI score, FIB-4 index, as well as the ALBI score are derived from the standard laboratory parameters available. Elevated APRI, FIB-4 index, and/or ALBI scores within a patient before the clinical diagnosis of cirrhosis may suggest advanced liver fibrosis, but this may not be recognized until the patient experiences complications associated with cirrhosis, such as hepatic decompensation or HCC. The calculation methods were consistent to previously described protocols.10–12
In the study, patients received DAA treatment for either 12 or 24 weeks. Clinical, laboratory, and virological parameters were evaluated at baseline, EOT, and at 1-year to 5-year follow-up intervals after treatment completion. Hepatitis C virus RNA levels were determined, and the detection ranged from 15 up to 6.9*107 IU/mL. This observational study was approved by the Ethics Committee of Tianjin Third Central Hospital and Tianjin Second People’s Hospital. Tianjin Third Central Hospital is the leading review board (Ethics Batch No. IRB2018-03-01). Informed consent was obtained from all patients prior to study initiation. This study was conducted in full compliance with the Declaration of Helsinki.
Study Endpoints
The main objective in the research was to evaluate the long-term prognosis, which encompassed cumulative occurrence of HCC, progression of liver disease, HCV relapse, and mortality. Liver stiffness was monitored annually through the transient elastography or APRI score. An increase in LSM from less than 12.4 kPa to greater than 12.4 kPa or an increase in APRI score from less than 2.0 to greater than 2.0 was considered indicative of “elevated liver stiffness”.13 The progression of liver disease refers primarily to increase in liver stiffness or development of decompensated complications such as ascites, variceal bleeding, hepatic encephalopathy, or jaundice in our study. This secondary endpoint focused on comparing the long-term outcomes among patients with cirrhosis and those without cirrhosis. Regular monitoring of HCC was conducted in all patients pre-DAA and post-DAA treatment, with a diagnosis from HCC adhering to international guidelines.14 During the follow-up duration, occurrences of de novo HCC or mortality from any cause were documented for all patients until the conclusion of this study. Detection of HCC was conducted through annual follow-up assessments and review of primary medical records. The follow-up period concluded upon the diagnosis of HCC, patient death, or detection of positive HCV RNA. Data collection continued until March 31, 2024.
Statistical Analysis
Baseline characteristic comparisons among cirrhotic with non-cirrhotic patients were conducted through SPSS 25.0. The data were presented in percentages and analyzed through either the chi-square test or Fisher’s exact test. Furthermore, comparisons between normally and non-normally distributed data were conducted through Mann–Whitney U-test. Calculate the annual incidence rate of adverse events (per 1000 person years [PY]) under the assumption of Poisson distribution. In order to compare the annual incidence rate of events during follow-up among different subgroups and across years post-SVR during the follow-up period, two-factor analysis of variance and Tukey post analysis were used. Survival analysis was conducted using R software, using survival packages for hypothesis testing of proportional hazards and survival regression modeling. Kaplan Meier method was used to assess the cumulative incidence rate of HCC, and log rank test was used to analyze the subgroup differences. We apply univariate and multivariate Cox proportional hazards regression models to evaluate the impact of various factors on the risk of virological recurrence, HCC, and mortality. When the p-value was less than 0.05, it had statistical significance.
Results
Baseline Characteristics of Patients
Out of the initial 1274 subjects, 369 individuals had incomplete data or did not achieve SVR12, 9 patients had concurrent HBV infection, 4 had co-infection with HIV, and 30 had less than a 1-year follow-up period. Ultimately, 862 individuals successfully completed the long-term follow-up (Figure 1). Within the study, 862 patients satisfied the inclusion criteria. In the baseline cohort, cirrhosis was identified in 302 patients (35.0%). The demographic as well as the baseline clinical characteristics of cirrhotic and non-cirrhotic patients were presented in Table 1.
 |
Table 1 Baseline Characteristics of Patients Available for Evaluation After 5 Year Following EOT |
 |
Figure 1 The flowchart of patients’ recruitment. |
All patients were categorized into either cirrhotic or non-cirrhotic, with 302 patients (35.0%) identified as having cirrhosis (Table 1). There was no statistically significant difference in the distribution of the two groups of males (41.7% vs 43.8%, P = 0.566). The cirrhotic individuals were notably older than non-cirrhotic patients (60.5 vs 56.0, P < 0.0001). The proportion of patients with liver cirrhosis who have a history of HCC is significantly higher than that of non-cirrhotic patients (10.6% vs 0.9%, P < 0.0001). Additionally, the proportion of treatment-naïve patients was substantially lower among cirrhotic patients than those non-cirrhotic patients (89.7% vs 94.3%, P < 0.0001). In addition, serological indices, comorbidity, APRI scores, FIB-4 index, ALBI scores, genotypes, treatment regimens for DAAs, and treatment duration of the patients in both groups are also presented in Table 1.
The LSM levels were markedly higher in cirrhotic patients compared to non-cirrhotic patients (median: 18.6 vs 8.1). Additionally, significant differences were observed among cirrhotic with non-cirrhotic patients, as presented in Table 1. The levels and normalization rate of indicators related to liver and kidney function for all participants after DAA treatment improved to a large degree at EOT and at 1 up to 5 years following treatment compared with baseline, which were displayed in Table S1.
Results of Follow-Up of Patients After DAA Treatment
The median follow-up time for the entire study cohort was 4.86 years, with a follow-up time of 4.48 years for the 25th percentile and 5.48 years for the 75th percentile. The maximum post-End of Treatment (EOT) follow-up period extended to 6.23 years. Furthermore, the follow-up status of the patients up to the end of March 2024 was illustrated in Table 2, with 851 patients completing 1-year follow-up, 410 patients completing 2-year follow-up, 336 patients completing 3-year follow-up, 257 patients completing 4-year follow-up, and 193 patients completing 5-year follow-up. During long-term surveillance, 21 patients experienced virological relapse, resulting in an accumulated incidence rate of 1.03% (95% CI 0.6–1.5). Additionally, 36 participants developed HCC with an accumulated incidence rate of 1.76% (95% CI 1.2–2.3), while 31 patients did not survive, leading to an accumulated incidence rate of 1.51% (95% CI 1.0–2.0). Furthermore, 119 patients exhibited progression of liver disease, reflecting an accumulated incidence rate of 5.81% (95% CI 4.8–6.8). The accumulated incidence rates of other complications, including ascites, encephalopathy, upper gastrointestinal bleeding, anemia, thrombocytopenia, agranulocytosis, hypersplenism, hypoproteinemia, and portal vein tumor thrombosis, were 1.95% (95% CI 1.4–2.6), 0.98% (95% CI 0.6–1.4), 0.68% (95% CI 0.3–1.0), 1.32% (95% CI 0.8–1.8), 1.37% (95% CI 0.9–1.9), 0.64% (95% CI 0.3–1.0), 1.03% (95% CI 0.6–1.5), 2.00% (95% CI 1.4–2.6), and 0.68% (95% CI 0.3–1.0), respectively (Table 2). The overall and HCV-related mortality were 3.64% (15.1/1000 person-years) and 2.11% (8.8/1000 person-years), respectively (Table 2). On average, deaths occurred approximately 2.60 years after the EOT. Among the deceased, 18 patients (5.96%) passed away due to liver-related causes, with 3 (0.99%) from liver decompensation and 15 (4.97%) from HCC. Additionally, 13 patients (2.32%) succumbed to non-liver related causes, including congestive heart failure, cerebral infarction, renal carcinoma, lung carcinoma, silicosis, and aplastic anemia. The incidence rates of HCC, disease progression, and HCV relapse were notably higher in cirrhotic patients (P < 0.01). Furthermore, both overall and HCV-related mortality rates were markedly elevated within cirrhotic patients (P < 0.0001) (Table S2).
 |
Table 2 The Annualized Incidence Rates (AIRs) of Adverse Events in Patients Under Long-Term Surveillance After SVR |
Baseline Risk Factors and Cumulative Incidence for Virological Relapse
The percentages of patients who cannot detect HCV RNA were 100% (862/862), 98.7% (840/851), 98.7% (405/410), 99.4% (334/336), 99.2% (255/257), and 99.5% (192/193) at the EOT, 1-, 2-, 3-, 4-, and 5-year post-treatment, respectively. Among the patients, 21 cases of virological relapse occurred during the surveillance period. The incidence rate of virological relapse was 12.9 per 1000 person-years during the first year after treatment, showing a gradual decrease over time. The cumulative incidence of virological relapse in the 5 years after achieving SVR was 1.03% (95% CI 0.6–1.5). It was worth noting that the incidence of virological recurrence within a cirrhosis group was higher than that in a non-cirrhosis group (1.61%,95% CI 0.8–2.4 vs 0.60%, 95% CI 0.2–1.0, P = 0.001) (Table S2). In a univariable analysis, factors related to treatment failure included being treatment-naïve for DAA treatment (HR 3.31, 95% CI 1.11–9.83), having prior HCC (HR 4.26, 95% CI 1.25–14.48), and presenting with liver cirrhosis at baseline (HR 3.94, 95% CI 1.59–9.75). Conversely, gender, age, BMI, elevated AFP levels, HCV viral load, alcohol abuse, hypertension, coronary heart disease, fatty liver, diabetes, APRI score, FIB-4 index, as well as ALBI score showed no significant associations with virological relapse. In the multivariable analysis, liver cirrhosis at baseline remained significantly associated with treatment failure (adjusted HR 3.20, 95% CI 1.24–8.25). However, being treatment-naïve for DAAs or having a previous history of HCC were not identified to be risk factors for treatment failure within this cohort (adjusted HR 2.51, 95% CI 0.83–7.56 and adjusted HR 2.38, 95% CI 0.67–8.50) (Table 3). The cumulative hazards of virological relapse were analyzed based on various baseline factors. Patients with cirrhosis, prior treatment experience, and a history of HCC exhibited significantly higher cumulative hazards of virological relapse (Figure 2).
 |
Table 3 Univariate and Multivariate COX Regression Analysis of Different Predictors Variables of Virological Relapse After DAA Treatment |
 |
Figure 2 Cumulative risk analysis of (A) cirrhosis; (B) Treatment-naïve; (C) prior HCC with virologic relapse (Log rank test). |
Baseline Risk Factors and Cumulative Incidence for HCC
Thirty-six cases of de novo HCC were identified after achieving SVR at either 12 or 24 weeks post-treatment. The incidence rate of HCC was 12.9 per 1000 person years in the first year, increased to 31.7 per 1000 person years in the second year, and decreased to 23.8 per 1000 person years in the third year. The occurrence of HCC stayed consistent in patients without cirrhosis from 0.1 to 3.5 per 1000 person-years. In contrast, patients with underlying cirrhosis exhibited a notably elevated annual incidence rate, peaking at 69.5 per 1000 person-years two years after achieving SVR. The difference was statistically significant (P < 0.0001) (Table S2).
In the analysis using univariate and multivariate Cox regression models for assessing baseline factors related to the development of HCC post-DAA treatment, several significant findings emerged. In univariate analysis, increased risks of HCC were linked to age ≥60 years, prior treatment experience, presence of cirrhosis, alcohol abuse, hypertension, coronary heart disease, diabetes, and an ALBI score > −2.60. Notably, the presence of cirrhosis emerged as the most potential predictor of HCC after DAA treatment, with a hazard ratio of 8.43 (95% CI 3.26–21.83, P < 0.0001). Subsequent multivariate analysis further explored the independent impact of these baseline factors on developing HCC. In multivariate analysis incorporating significant variables within univariate analysis (P < 0.05), baseline liver cirrhosis, alcohol abuse, and diabetes were recognized to be autonomous factors contributing to the risk of HCC. Specifically, liver cirrhosis at baseline (adjusted HR 6.57, 95% CI 2.66–16.28), alcohol abuse (adjusted HR 4.71, 95% CI 2.07–10.70), and diabetes (adjusted HR 2.33, 95% CI 1.05–5.15) were related to an increased risk of HCC. Conversely, age, treatment-naïve status, hypertension, coronary heart disease, and ALBI score were not found to be autonomous factors for HCC in this cohort (Table 4). Furthermore, the HCC’s cumulative hazard analysis based on different baseline factors revealed that patients with cirrhosis, decompensated cirrhosis, age ≥60, treatment experience, hypertension, coronary heart disease, diabetes, alcohol abuse, and ALBI score ≥-2.60 had significantly higher cumulative hazards of HCC (Figure 3).
 |
Table 4 Univariate and Multivariate COX Regression Analysis of Different Predictors Variables of Cases of HCC After DAA Treatment |
 |
Figure 3 Cumulative probability of HCC according to (A) cirrhosis; (B) compensated cirrhosis (C) age; (D) treatment-naïve; (E) hypertension; (F) Coronary heart disease; (G) diabetes; (H) alcohol abuse and (I) AIBI score (Log rank test). |
Baseline Risk Factors and Cumulative Incidence for Mortality
Over the course of the 5-year monitoring period, 31 cases of all-cause death were recorded, resulting in a cumulative incidence of all-cause mortality of 1.51%. In univariate analysis, factors related to patients’ survival included being male, age ≥60, baseline liver cirrhosis, alcohol abuse, hypertension, diabetes, presence of nephropathy, and ALBI score. In this study cohort, factors such as BMI index, treatment-naïve status, elevated AFP levels, HCV RNA viral load, coronary heart disease, fatty liver, APRI score, and the FIB-4 index were not related to patients’ mortality within univariate analysis. However, in multivariable analysis, baseline liver cirrhosis and diabetes were identified as factors markedly related to patients’ mortality. Specifically, baseline liver cirrhosis (adjusted HR 6.93, 95% CI 2.56–18.74) and diabetes (adjusted HR 2.72, 95% CI 1.13–6.55) were associated with a heightened risk of mortality. On the other hand, factors such as gender, age, alcohol abuse, hypertension, presence of nephropathy, and ALBI score were not identified to be independent risk causes for mortality within this cohort (Table 5). Significantly higher cumulative hazards of death were observed in patients suffering from cirrhosis, decompensated cirrhosis, baseline HCC, HCC, age ≥60, male gender, virological relapse, alcohol use, hypertension, diabetes, and nephropathy. These factors were related to an increased risk of mortality within the study cohort (Figure 4).
 |
Table 5 Univariate and Multivariate COX Regression Analysis of Different Predictors Variables of Death After DAA Treatment |
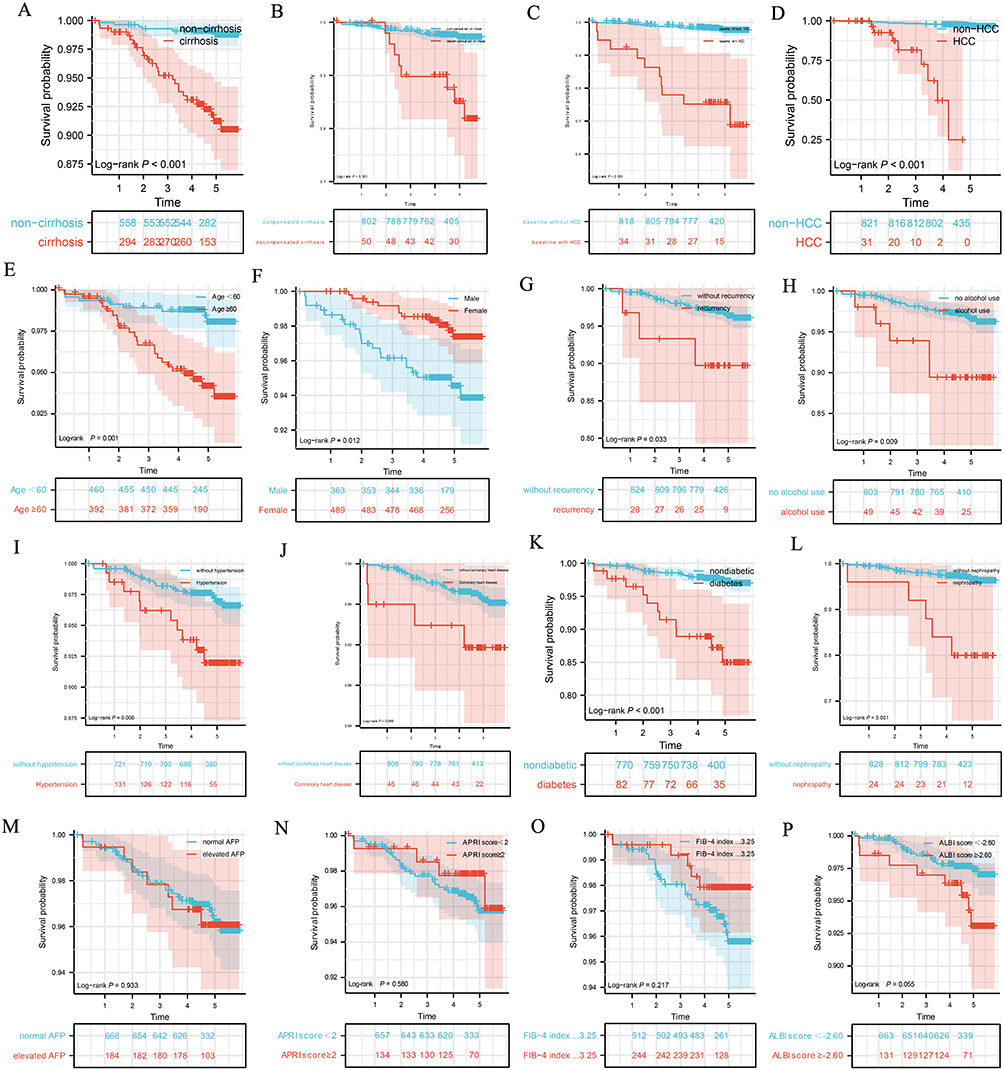 |
Figure 4 Survival analysis of different subgroups (A–P) of patients after DAA treatment. (A) cirrhosis; (B) decompensated cirrhosis; (C) baseline with HCC; (D) HCC; (E) age; (F) gender; (G) virologocial recurrence; (H) alcohol abuse; (I) hypertension; (J) coronary disease; (K) diabetes; (L) nephropathy; (M) AFP; (N) APRI score; (O) FIB-4 index; (P) ALBI score. |
Changes of Liver Stiffness Measurement After DAA Treatment
Our study revealed a notable decrease in LSM at EOT as well as 1, 2, 3, 4, and 5 years of follow-up within cirrhosis patients (all P < 0.01). Additionally, LSM values demonstrated a notable decrease at EOT and throughout a follow-up period in non-cirrhosis patients (all P < 0.001) (Figure 5).
 |
Figure 5 Liver stiffness measurement value at baseline, EOT, 1yFU, 2yFU, 3yFU, 4yFU and 5yFU of (A) cirrhosis patients and (B) non-cirrhosis patients (*, P<0.05; **, P<0.01, ****, P<0.0001). Abbreviations: LSM, liver stiffness measurement; EOT, end of treatment; 1yFU,1-year follow-up; 2yFU, 2-year follow-up; 3yFU, 3-year follow-up; 4yFU, 4-year follow-up; 5yFU, 5-year follow-up. |
Changes of APRI Score, FIB-4 Index and ALBI Score Over Time
Changes in the APRI score, FIB-4 index, and ALBI score were assessed over various time points. We found a notable decrease in APRI score levels at the EOT and at 1, 2, 3, 4, and 5 years of follow-up than baseline in both cirrhosis and non-cirrhosis groups (all P < 0.0001). Specifically, FIB-4 index levels decreased markedly at EOT, 1yFU, and 2yFU in cirrhosis patients (all P < 0.0001), while non-cirrhosis patients had no significant changes (P > 0.05). The ALBI score in cirrhosis patients showed a significant decrease at 1yFU, 2yFU, and 3yFU (P < 0.0001, P < 0.01, and P < 0.05, respectively) but showed no significant changes at 4yFU and 5yFU (P > 0.05). Furthermore, a substantial decrease within the ALBI score was observed during 1-year follow-up within the non-cirrhosis group (P < 0.001) (Table S3 and Figure 6). Furthermore, our evaluation of their long-term impact on the risks of virological relapse, HCC, and mortality did not identify them as independent causes contributing to developing these outcomes (Tables 3–5; Figure 3 and 4).
 |
Figure 6 (A) APRI score, (B) FIB-4 index and the (C) ALBI score at Baseline, EOT, 1yFU, 2yFU, 3yFU, 4yFU and 5yFU (*, P<0.05; **, P<0.01; ***, P<0.001; ****, P<0.0001). |
Discussion
Recently, the landscape of antiviral therapy for HCV infection has shifted from interferon (IFN)-based regimens to interferon-free DAAs. Nevertheless, prospective data on the long-term outcomes in real-world settings are sparse and intricate. To our understanding, our study represents the most extensive follow-up period, multi-center prospective study of patients in China following SVR achieved through DAA treatment. Our extensive follow-up study commenced with patients who achieved sustained virologic response. Following the availability of effective DAA regimens in China in 2017, we prospectively recruited individuals who received DAA treatment.
With the widespread utilization of DAAs, achieving SVR is nearly universal among HCV-infected individuals following antiviral treatment. Nevertheless, viral eradication may not always equate to a complete cure for the disease, as patients remain susceptible to disease progression. Numerous investigations have demonstrated that achieving SVR at 12 or 24 weeks is linked to enhanced clinical results, such as mitigating fibrosis progression and lowering the risk of HCC.15–18 Despite achieving SVR, there remains a residual risk of liver disease progression, underscoring the crucial significance of ongoing patient surveillance. As outlined by Wang S. and colleagues, diligent surveillance and prompt diagnosis play a pivotal role in enhancing cancer cure rates by enabling timely and appropriate follow-up interventions.19 Given the impracticality of monitoring all patients who have achieved a virologic cure, it is imperative to pinpoint individuals at elevated risk for viral reactivation, HCC, and mortality. This task is further complicated by the dynamic nature of HCC risk, which evolves over time with changes in patients’ age and fibrosis status. While several studies have investigated factors predisposing virologically cured patients to short-term HCC risk, there is a scarcity of research focusing on the long-term risks of viral reactivation, HCC development, and overall prognosis.20–22 In this study, we examined the enduring risks of virological relapse, HHC, and overall prognosis by leveraging various baseline markers that could be monitored regularly during the follow-up period. Our goal was to pinpoint high-risk individuals necessitating vigilant surveillance. Consistent with prior research findings, it was noted that the occurrence of HCV virological relapse following successful SVR was infrequent.23 In our investigation, 21 individuals encountered a virological relapse, resulting in a cumulative incidence of 1.03% at the 5-year mark post SVR achievement. Notably, the cirrhosis cohort exhibited a higher incidence of virological relapse than non-cirrhosis group. Through multivariate analysis, we confirmed the presence of cirrhosis independently rised risk of HCV reappearance. Furthermore, subgroup analysis through Log rank test revealed that patients with cirrhosis, those with prior treatment experience, and individuals with a history of HCC displayed a significantly elevated hazard of virological relapse. Patients, experienced virological relapse, were more inclined to have liver cirrhosis at the baseline assessment in comparison to those without cirrhosis.
Successful elimination of HCV through antiviral therapy diminishes, though does not eradicate, the likelihood of developing HCC. Studies have indicated that the AIR of HCC in individuals possessing both HCV infection and cirrhosis ranges from 1.5% to 8%.24,25 The remarkable success rates of SVR attained through novel DAA combination therapy offer promising prospects for a substantial decrease in the occurrence of liver cancer, particularly among individuals with cirrhosis.22,26 However, research conducted in Europe and North America has demonstrated that DAA therapy has minimal impact on HCC’s incidence. In fact, certain studies have suggested a potential elevated risk associated with DAA treatment.27,28 In our analysis, factors such as baseline liver cirrhosis, diabetes, and daily alcohol consumption of ≥25 grams were found to be significantly related to the onset of HCC. Notably, diabetes has become an independent risk factor in developing HCC, and its risk is twice that of non-diabetic individuals. As anticipated, the presence of baseline liver cirrhosis was firmly linked to an elevated HCC risk. Furthermore, alcohol abuse emerged as another potential risk factor for HCC. Subgroup analysis using Log rank tests indicated that patients with cirrhosis, particularly those with decompensated cirrhosis, aged 60 and above, prior treatment experience, hypertension, coronary heart disease, diabetes, alcohol misuse, and an ALBI score of ≥−2.60 exhibited a heightened cumulative hazard of HCC.
Studies have indicated that undergoing DAA therapy and attaining SVR are linked to enhanced overall survival rates among patients with HCV, and even in individuals with HCC.29–31 Achieving SVR has been demonstrated to be correlated to a decreased risk of liver-related mortality and overall mortality rates.32,33 In our assessment of the extended survival outcomes after DAA treatment, we observed that patients with cirrhosis, decompensated cirrhosis, baseline HCC, HCC, aged over 60, male gender, virological relapse, alcohol consumption, hypertension, diabetes, and nephropathy exhibited a notably elevated cumulative hazard of all-cause mortality. Furthermore, the multivariable analysis underscored that baseline liver cirrhosis and diabetes stood out as independent factors influencing patients’ survival and overall prognosis. Our findings indicate a reduced overall and liver-related mortality rate among patients cohort following a successful achievement of SVR through DAA treatment. This suggests a positive prognosis for these individuals.7,32,34 Data from epidemiological studies in the United States revealed a decline in mortality attributed to HCV infection following the implementation of DAA therapies.35 There have been previous reports on the association among HCV infection with diabetes.36,37 Our study findings revealed that diabetes was pinpointed to be an independent risk factor in developing HCC and was associated with an unfavorable prognosis. Therefore, individuals with HCV, particularly those with cirrhosis and diabetes mellitus, should undergo vigilant monitoring.
Research conducted on interferon therapies has shown that a considerable proportion of patients with HCV may experience regression to liver fibrosis upon achieving SVR.38 Furthermore, recent research has presented evidence of liver stiffness improvement following the administration of novel DAA treatment.39–41 These studies have highlighted a reduction in liver stiffness across all fibrosis stages. In our extended surveillance, we noted a substantial decrease in LSM at EOT and at 1-year to 5-year follow-up in all patients. These findings suggest that DAA therapy holds an important state in enhancing liver biochemical parameters and reversing liver fibrosis. This is a good guide to the treatment of patients with hepatitis C cirrhosis.
Research has indicated a strong relationship among non-invasive markers of fibrosis, with severity of liver fibrosis and the potentially advancement of HCC.42–45 The APRI and FIB-4 scores have proven to be effective tools in detecting fibrosis and are widely accepted in clinical practice guidelines. Additionally, the ALBI score emerges as a valuable and cost-efficient approach for risk assessment and personalized monitoring of HCC in cirrhotic patients with a background of prior HCV infection through DAA treatment.44 During the five-year follow-up period, we assessed the changes in APRI score, FIB-4 index, and ALBI score over time. Our findings revealed a notable reduction in APRI scores at EOT as well as the 1-year until up to 5-year follow-ups compared to baseline levels. In cirrhotic patients, the FIB-4 index exhibited a notable decrease at EOT, 1-year, and 2-year follow-up, whereas non-cirrhotic patients showed no significant changes within FIB-4 index levels. Additionally, the ALBI score significantly decreased in cirrhotic patients at 1 to 3-year follow-up, with no significant changes at 4-year and 5-year follow-up. Notably, a marked reduction within ALBI score was also observed at the 1-year follow-up in the non-cirrhotic group. In our initial univariate analysis, individuals with an ALBI score greater than −2.60 exhibited an increased risk of developing HCC and mortality. However, upon conducting a multivariate analysis, an ALBI score exceeding −2.60 was not identified as an independent risk factor for HCC or survival. It is essential to further validate the prognostic significance of the APRI score, FIB-4 index, and ALBI score with extended follow-up within our study cohort.
Our study’s notable strengths lie in the enrollment of a substantial population from two medical centres and the extensive prospective long-term follow-up period after DAAs’ introduction into China in 2017. Furthermore, our study design was prospective over the long term, encompassing a study cohort comprising both cirrhotic and non-cirrhotic patients. However, there are certain limitations. First, excluding patients with a history of HBV co-infection and HCV patients with a history of HIV co-infection may lead to underestimating the potential benefits of DAAs. Second, there may still be some unobservable variables affecting our results. We attempted to mitigate this by thoughtfully selecting variables that we believed could be pertinent to the outcomes of our study.
Conclusion
Despite achieving SVR, there remains a persistent risk of virological relapse, HCC, HCV-related mortality and liver-related complications even after the successful post-treatment 5-year follow-up period. Hence, it is imperative to implement a rigorous surveillance protocol for all cirrhotic patients undergoing treatment with DAAs, and extended follow-up is essential for evaluating the long-term risk of disease progression, particularly within individuals possessing liver cirrhosis.
Abbreviations
BMI, Body mass index; HCV, Hepatitis C virus; SD, standard deviation; WBC, White blood cell; Hb, Hemoglobin; PLT, Platelet; ALT, Alanine aminotransferase; AST, Aspartate aminotransferase; ALP, Alkaline phosphatase; GGT, Glutamyl transpeptidase; ALB, Albumin; GLOB, Globulin; Tbil, total bilirubin; Cr, creatinine; UA, uric acid; AFP, Alpha-fetoprotein; HCC, Hepatocellular carcinoma; LSM, liver stiffness measurement; APRI, Aspartate aminotransferase-to-platelet ratio index; FIB-4, Fibrosis-4; ALBI, Albumin-bilirubin; DAAs, Direct-acting antiviral agents; SOF, Sofosbuvir; RBV, Ribavirin; VEL, velpatasvir; OBV, ombitasvir; PTV, paritaprevir; r, ritonavir; DSV, dasabuvir; ASV, asunaprevir; DCV, Daclatasvir; EBR/GZR, Elbasvir/Grazoprevir.
Acknowledgments
The authors thank all the participants enrolled in this study and the researchers involved in the study design, recruitment of patients, treatment, data collection and patient follow-up. This work was sponsored by Tianjin Key Medical Discipline (Specialty) Construction Project (Grant No. TJYXZDXK-034A), and the Tianjin Health Research Project (Grant No. TJWJ2022XK027).
Disclosure
The authors declare no conflict of interest in this work.
References
1. Easterbrook P, Luhmann N, Newman M, Walsh N, Lesi O, Doherty M. New WHO guidance for country validation of viral hepatitis B and C elimination. Lancet Gastroenterol Hepatol. 2021;6(10):778–780. doi:10.1016/S2468-1253(21)00267-3
2. Huang CF, Iio E, Jun DW, et al. Direct-acting antivirals in East Asian hepatitis C patients: real-world experience from the REAL-C Consortium. Hepatol Int. 2019;13(5):587–598. doi:10.1007/s12072-019-09974-z
3. Bruno S, Stroffolini T, Colombo M, et al. Sustained virological response to interferon-alpha is associated with improved outcome in HCV-related cirrhosis: a retrospective study. Hepatology. 2007;45(3):579–587. doi:10.1002/hep.21492
4. Innes H, McDonald S, Hayes P, et al. Mortality in hepatitis C patients who achieve a sustained viral response compared to the general population. J Hepatol. 2017;66(1):19–27. doi:10.1016/j.jhep.2016.08.004
5. Carrat F, Fontaine H, Dorival C, et al. Clinical outcomes in patients with chronic hepatitis C after direct-acting antiviral treatment: a prospective cohort study. Lancet. 2019;393(10179):1453–1464. doi:10.1016/S0140-6736(18)32111-1
6. Calvaruso V, Craxì A. Hepatic benefits of HCV cure. J Hepatol. 2020;73(6):1548–1556. doi:10.1016/j.jhep.2020.08.006
7. van der Meer AJ, Berenguer M. Reversion of disease manifestations after HCV eradication. J Hepatol. 2016;65(1 Suppl):S95–s108. doi:10.1016/j.jhep.2016.07.039
8. Robert Jr SB. The Possible Association Between DAA Treatment for HCV Infection and HCC Recurrence. Gastroenterology & hepatology. 2016;12(12):776–779.
9. Kim SK, Fujii T, Kim SR, et al. Hepatitis B Virus Treatment and Hepatocellular Carcinoma: controversies and Approaches to Consensus. Liver Cancer. 2022;11(6):497–510. doi:10.1159/000525518
10. Wai CT, Greenson JK, Fontana RJ, et al. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology. 2003;38(2):518–526. doi:10.1053/jhep.2003.50346
11. Vallet-Pichard A, Mallet V, Nalpas B, et al. FIB-4: an inexpensive and accurate marker of fibrosis in HCV infection. comparison with liver biopsy and fibrotest. Hepatology. 2007;46(1):32–36. doi:10.1002/hep.21669
12. Johnson PJ, Berhane S, Kagebayashi C, et al. Assessment of liver function in patients with hepatocellular carcinoma: a new evidence-based approach-the ALBI grade. J Clin Oncol. 2015;33(6):550–558. doi:10.1200/JCO.2014.57.9151
13. H You, FS Wang, T Li, et al. Guideline for the prevention and treatment of hepatitis C (2022 version)]. Chin J Hepatol. 2022;30(12):1332–1348. doi:10.3760/cma.j.cn501113-20221220-00605
14. Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358–380. doi:10.1002/hep.29086
15. Rockey DC, Friedman SL. Fibrosis Regression After Eradication of Hepatitis C Virus: from Bench to Bedside. Gastroenterology. 2021;160(5):1502–1520.e1501. doi:10.1053/j.gastro.2020.09.065
16. Ioannou GN, Feld JJ. What Are the Benefits of a Sustained Virologic Response to Direct-Acting Antiviral Therapy for Hepatitis C Virus Infection? Gastroenterology. 2019;156(2):446–460.e442. doi:10.1053/j.gastro.2018.10.033
17. Singal AG, Rich NE, Mehta N, et al. Direct-Acting Antiviral Therapy for Hepatitis C Virus Infection Is Associated With Increased Survival in Patients With a History of Hepatocellular Carcinoma. Gastroenterology. 2019;157(5):1253–1263.e1252. doi:10.1053/j.gastro.2019.07.040
18. Ioannou GN, Green PK, Berry K. HCV eradication induced by direct-acting antiviral agents reduces the risk of hepatocellular carcinoma. J Hepatol. 2017;68:25–32.
19. Wang S, Liu Y, Feng Y, et al. A Review on Curability of Cancers: more Efforts for Novel Therapeutic Options Are Needed. Cancers. 2019;11(11):1782. doi:10.3390/cancers11111782
20. Mücke MM, Mücke VT, Peiffer KH, et al. Absence of HBV Reactivation in Patients With Resolved HBV Infection Following DAA Therapy for Hepatitis C: a 1-Year Follow-up Study. Open Forum Infectious Diseases. 2019;6(1):ofy340. doi:10.1093/ofid/ofy340
21. Soliman H, Ziada D, Hamisa M, et al. The Effect of HCV Eradication after Direct-Acting Antiviral Agents on Hepatic Steatosis: a Prospective Observational Study. Endocrine, Metabolic & Immune Disorders Drug Targets. 2022;22(1):100–107. doi:10.2174/1871530321666210125125500
22. Kanwal F, Kramer JR, Asch SM, Cao Y, Li L, El-Serag HB. Long-Term Risk of Hepatocellular Carcinoma in HCV Patients Treated With Direct Acting Antiviral Agents. Hepatology. 2020;71(1):44–55. doi:10.1002/hep.30823
23. Formann E, Steindl-Munda P, Hofer H, et al. Long-term follow-up of chronic hepatitis C patients with sustained virological response to various forms of interferon-based anti-viral therapy. Alimentary Pharmacology & Therapeutics. 2006;23(4):507–511. doi:10.1111/j.1365-2036.2006.02785.x
24. Blach S, Zeuzem S, Manns M. Global prevalence and genotype distribution of hepatitis C virus infection in 2015: a modelling study. The lancet Gastroenterology & Hepatology. 2017;2(3):161–176. doi:10.1016/S2468-1253(16)30181-9
25. Lok AS, Seeff LB, Morgan TR, et al. Incidence of hepatocellular carcinoma and associated risk factors in hepatitis C-related advanced liver disease. Gastroenterology. 2009;136(1):138–148. doi:10.1053/j.gastro.2008.09.014
26. JM Pawlotsky, F Negro, A Aghemo, et al. EASL recommendations on treatment of hepatitis C: final update of the series. J Hepatol. 2020;73(5):1170–1218. doi:10.1016/j.jhep.2020.08.018
27. Reig M, Mariño Z, Perelló C, et al. Unexpected high rate of early tumor recurrence in patients with HCV-related HCC undergoing interferon-free therapy. J Hepatol. 2016;65(4):719–726. doi:10.1016/j.jhep.2016.04.008
28. Lai CL, Yuen MF. Prevention of hepatitis B virus-related hepatocellular carcinoma with antiviral therapy. Hepatology. 2013;57(1):399–408. doi:10.1002/hep.25937
29. Tahata Y, Hikita H, Mochida S, et al. Liver-related events after direct-acting antiviral therapy in patients with hepatitis C virus-associated cirrhosis. Journal of Gastroenterology. 2022;57(2):120–132. doi:10.1007/s00535-021-01845-5
30. Kamp WM, Sellers CM, Stein S, Lim JK, Kim HS. Impact of Direct Acting Antivirals on Survival in Patients with Chronic Hepatitis C and Hepatocellular Carcinoma. Scientific Reports. 2019;9(1):17081. doi:10.1038/s41598-019-53051-2
31. Jiang X, Song HJ, Chang CY, Wilson DL, Lo-Ciganic WH, Park H. Impact of Direct-acting Antivirals on Hepatocellular Carcinoma and Mortality Among Medicaid Beneficiaries With Hepatitis C. Medical Care. 2023;61(8):505–513. doi:10.1097/MLR.0000000000001870
32. van der Meer AJ, Feld JJ, Hofer H, et al. Risk of cirrhosis-related complications in patients with advanced fibrosis following hepatitis C virus eradication. J Hepatol. 2017;66(3):485–493. doi:10.1016/j.jhep.2016.10.017
33. Morgan RL, Baack B, Smith BD, Yartel A, Pitasi M, Falck-Ytter Y. Eradication of hepatitis C virus infection and the development of hepatocellular carcinoma: a meta-analysis of observational studies. Annals of Internal Medicine. 2013;158(5 Pt 1):329–337. doi:10.7326/0003-4819-158-5-201303050-00005
34. Nahon P, Bourcier V, Layese R, et al. Eradication of Hepatitis C Virus Infection in Patients With Cirrhosis Reduces Risk of Liver and Non-Liver Complications. Gastroenterology. 2017;152(1):142–156.e142. doi:10.1053/j.gastro.2016.09.009
35. Kim D, Li AA, Gadiparthi C, et al. Changing Trends in Etiology-Based Annual Mortality From Chronic Liver Disease, From 2007 Through 2016. Gastroenterology. 2018;155(4):1154–1163.e1153. doi:10.1053/j.gastro.2018.07.008
36. Negro F. Facts and fictions of HCV and comorbidities: steatosis, diabetes mellitus, and cardiovascular diseases. J Hepatol. 2014;61(1 Suppl):S69–78. doi:10.1016/j.jhep.2014.08.003
37. Ding Y, Li G, Zhou Z, Deng T. Molecular mechanisms underlying hepatitis C virus infection-related diabetes. Metabolism: Clinical and Experimental. 2021;121:154802. doi:10.1016/j.metabol.2021.154802
38. Shiratori Y, Imazeki F, Moriyama M, et al. Histologic improvement of fibrosis in patients with hepatitis C who have sustained response to interferon therapy. Annals of Internal Medicine. 2000;132(7):517–524. doi:10.7326/0003-4819-132-7-200004040-00002
39. Bachofner JA, Valli PV, Kröger A, et al. Direct antiviral agent treatment of chronic hepatitis C results in rapid regression of transient elastography and fibrosis markers fibrosis-4 score and aspartate aminotransferase-platelet ratio index. Liver International: Official Journal of the International Association for the Study of the Liver. 2017;37(3):369–376. doi:10.1111/liv.13256
40. Tachi Y, Hirai T, Kojima Y, et al. Liver stiffness reduction correlates with histological characteristics of hepatitis C patients with sustained virological response. Liver International: Official Journal of the International Association for the Study of the Liver. 2018;38(1):59–67. doi:10.1111/liv.13486
41. Ogasawara N, Kobayashi M, Akuta N, et al. Serial changes in liver stiffness and controlled attenuation parameter following direct-acting antiviral therapy against hepatitis C virus genotype 1b. J Med Virol. 2018;90(2):313–319. doi:10.1002/jmv.24950
42. Toyoda H, Kumada T, Tada T, et al. Differences in the impact of prognostic factors for hepatocellular carcinoma over time. Cancer Science. 2017;108(12):2438–2444. doi:10.1111/cas.13406
43. Morandi A, Risaliti M, Montori M, Buccianti S, Bartolini I, Moraldi L. Predicting Post-Hepatectomy Liver Failure in HCC Patients: a Review of Liver Function Assessment Based on Laboratory Tests Scores. Medicina (Kaunas, Lithuania). 2023;59(6). doi:10.3390/medicina59061099
44. Caviglia GP, Troshina G, Santaniello U, et al. Long-Term Hepatocellular Carcinoma Development and Predictive Ability of Non-Invasive Scoring Systems in Patients with HCV-Related Cirrhosis Treated with Direct-Acting Antivirals. Cancers. 2022;14(3):828. doi:10.3390/cancers14030828
45. Ioannou GN, Beste LA, Green PK, et al. Increased Risk for Hepatocellular Carcinoma Persists Up to 10 Years After HCV Eradication in Patients With Baseline Cirrhosis or High FIB-4 Scores. Gastroenterology. 2019;157(5):1264–1278.e1264. doi:10.1053/j.gastro.2019.07.033
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Repeated Measurement of FIB-4 to Predict Long-Term Risk of HCC Development Up to 10 Years After SVR

Zou Y, Yue M, Jia L, Wang Y, Chen H, Wang Y, Zhang M, Feng Y, Yu R, Yang S, Huang P
Journal of Hepatocellular Carcinoma 2022, 9:1433-1443
Published Date: 30 December 2022