")
Back to Journals » Research and Reports in Urology » Volume 17
Fresh Frozen Cadavers as a Novel Training Model for Percutaneous Nephrolithotomy (PCNL)
Authors Mantica G, Chierigo F , Tailly T, Spies PV, Du Plessis DE , Dotta F, Oppel C, Oyibo EU , De Klerk C , Gqoli LVZ, Drocchi G , Delport JE, Marais R , Van Heerden H, Osman MR, Padayachee WP, Ferro M, Terrone C, Van der Merwe A
Received 31 December 2024
Accepted for publication 7 May 2025
Published 17 May 2025 Volume 2025:17 Pages 167—173
DOI https://doi.org/10.2147/RRU.S515072
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Panagiotis J Vlachostergios
Guglielmo Mantica,1 Francesco Chierigo,2 Thomas Tailly,3 Petrus Venter Spies,4 Danelo Estienne Du Plessis,4 Federico Dotta,5 Cleve Oppel,6 Emmanuel Ugbede Oyibo,6 Cecelia De Klerk,4 Lonwabo Viwe Zuko Gqoli,7 Giovanni Drocchi,1 Johannes Eduard Delport,4 Ruzaan Marais,4 Hesma Van Heerden,4 Mohammed Riaz Osman,8 Winston PR Padayachee,9 Matteo Ferro,2 Carlo Terrone,1 André Van der Merwe4
1Department of Surgical and Diagnostic Integrated Sciences (DISC), University of Genova, Genova, Italy; 2Department of Urology, ASST Santi Paolo E Carlo, Milan, Italy; 3Department of Urology, University Hospital Ghent, Ghent, Belgium; 4Department of Surgery, Division of Urology, Faculty of Medicine and Health Sciences, Tygerberg Hospital, Stellenbosch University, Cape Town, South Africa; 5Department of Urology, Galliera Hospital, Genova, Italy; 6Department of Urology, Groote Schuur Hospital, University of Cape Town, Cape Town, South Africa; 7Department of Urology, Nelson Mandela University, Port Elizabeth, South Africa; 8JMH City Hospital, Durban, South Africa; 9Department of Urology, University of Witwatersrand, Johannesburg, South Africa
Correspondence: Guglielmo Mantica, Department of Surgical and Diagnostic Integrated Sciences (DISC), University of Genova, Genova, Italy, Email [email protected]
Introduction: This study aimed to evaluate fresh-frozen cadavers (FFC) as a novel model for percutaneous nephrolithotomy (PCNL) training, focusing on ultrasound-guided supine PCNL.
Methods: Sixteen urologists participated in a 2-day course at a tertiary center to assess the utility of an FFC model for ultrasound-guided supine PCNL. After the procedure, the participants completed a 24-question evaluation of the FFC model using a 5-point Likert scale. The questionnaire assessed tissue quality, US imaging, procedural steps, overall experience compared to live patient procedures, and suitability of the model for both basic and advanced supine PCNL training.
Results: The tactile sensation, skin stiffness, and distensibility of the calyces resembled real-life scenarios as the cadavers thawed. Similarly, US quality was worse in frozen cadavers and improved after irrigation with the collection system. Valdivia-Galdakao positioning is considered more difficult than in real life, because of rigor mortis.
Conclusion: FFC demonstrated robust content validity as a training model for PCNL. The model provides a realistic and effective training experience, offering a promising tool for developing critical surgical skills, while minimizing radiation exposure and procedural risks.
Keywords: fresh frozen cadavers, percutaneous nephrolithotomy, trainingmodel, ultrasound, guided, simulator
Introduction
Renal stones are considered one of the most common urinary tract diseases, affecting 5%–10% of the global population, with an increasing prevalence worldwide.1 Among the surgical treatment options, extracorporeal shockwave lithotripsy, percutaneous nephrolithotomy (PCNL), ureteroscopy (URS), and retrograde intrarenal surgery (RIRS) are the most commonly performed procedures.2 According to the guidelines of the European Association of Urology (EAU) and the American Urological Association (AUA), PCNL is the preferred treatment for renal stones > 2 cm, and an optional approach for stones between 1 and 2 cm.3,4
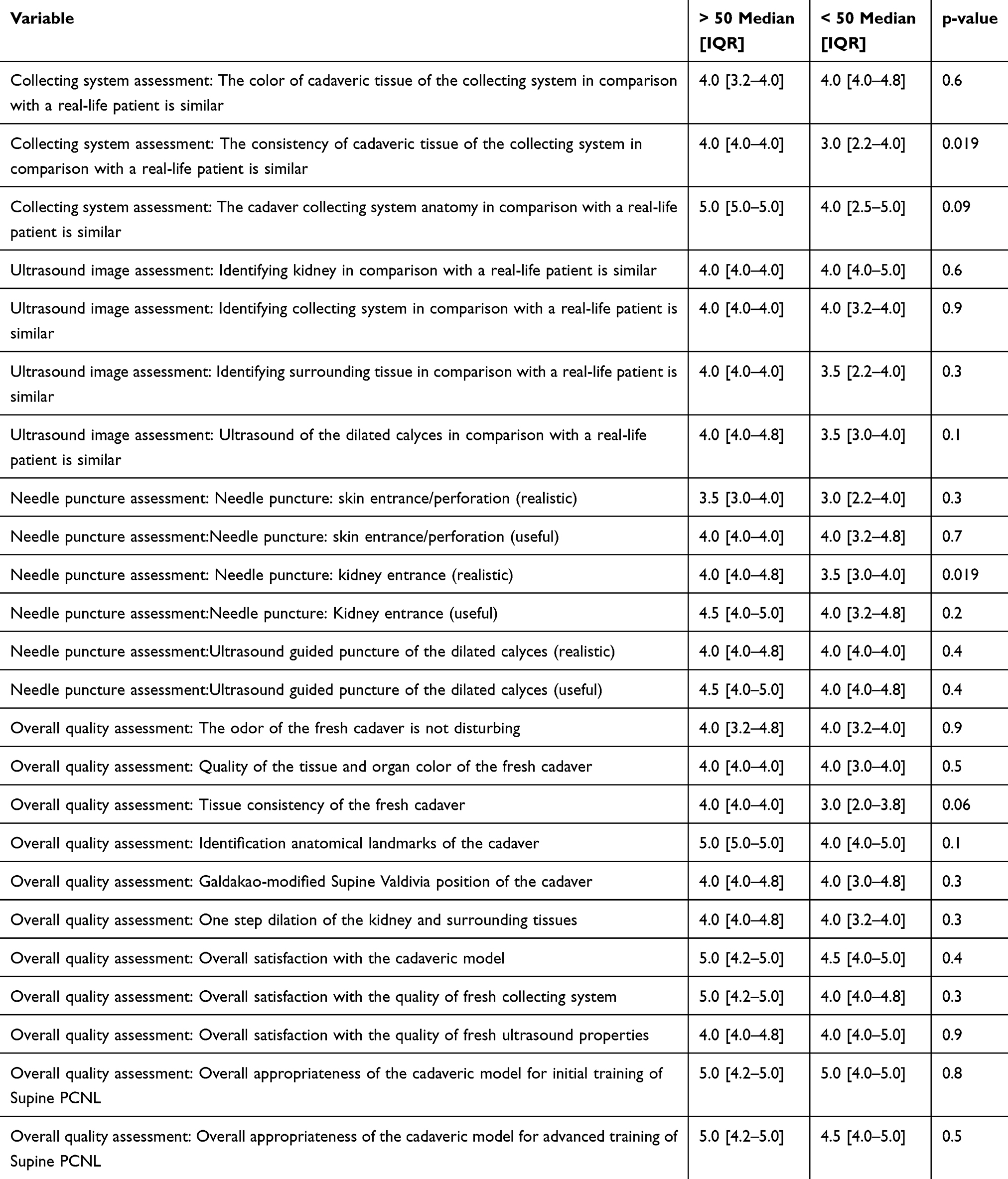 |
Table 1 Descriptive Comparative Table Based on PCNL Experience (>50 Vs <50) |
Advancements in PCNL include the miniaturization of percutaneous instruments and combined approaches with URS, such as endoscopic combined intrarenal surgery (ECIRS), thereby expanding its indications and improving patient outcomes.5 Central to the success of PCNL is the ability to achieve safe and precise percutaneous renal access. The techniques for renal access vary, utilizing ultrasound (US), fluoroscopy, or other needle guidance methods, with the goal of facilitating comprehensive access to the collecting system.6
Despite its widespread use, PCNL remains a technically demanding procedure with a steep learning curve, complication rates as high as 21.3%, and notable re-treatment rates.6,7 Novice surgeons often face challenges, including longer operative and fluoroscopy times, reduced stone-free rates, and higher retreatment rates than experienced practitioners.8,9 Therefore, structured training is critical for residents and novice endourologists as it can help minimize patient risk and accelerate surgical proficiency.10
Various models have been introduced to address the need for high-level PCNL training, including inanimate benchtop models, virtual reality (VR) simulators, animal models, and human cadavers.11–15 Among these, Thiel-embalmed cadavers (TEC) have gained attention in urology training because of their realistic tissue consistency, color, and flexibility without the odors typically associated with cadaveric models.10,16–21 TEC have already shown promise in training for laparoscopy and endoscopic procedures involving the upper and lower urinary tract. TEC has already been evaluated in the context of ECIRS training by Veys et al, who showed that the TEC model was rated as good to excellent, comparable to real-life procedures, and deemed excellent for both initial and advanced supine PCNL training. TEC provided good US visualization of the distended calyces during puncture, although the skin penetration was less realistic. Kidney puncture, dilatation, and anatomy were highly realistic despite the pale mucosa. US needle guidance was excellent, and needle puncture assessment was realistic and effective for training.22 Despite the several advantages, TEC are not easy to be prepared and available for training purposes in different settings.
In contrast, fresh-frozen cadavers (FFC) preserve the natural properties of living tissues, including resistance and bleeding. They provide a closer simulation of live surgical scenarios, particularly for advanced procedures such as percutaneous nephrolithotomy. However, they degrade quickly after thawing and pose a high risk for pathogen transmission.23,24 Freshly frozen cadavers were subjected to urological training.25–29
Therefore, in the context of PCNL and ECIRS training, FFC and TEC complement each other, with TEC excelling in controlled skill-building and FFC realistic procedural challenges. This study aimed to evaluate the FFC as a novel model for PCNL training, focusing specifically on US-guided supine PCNL, using a previously described methodology for assessing TEC.22
Materials And Methods
Sixteen urologists (6 tutors and 10 trainees) participated in a 2-day course at a tertiary center to assess the utility of a fresh frozen cadaver (FFC) model for ultrasound-guided supine percutaneous nephrolithotomy (PCNL). Written informed consent was obtained from all the urologists who participated in the questionnaire survey.
Each urologist performed a percutaneous kidney puncture under ultrasound (US) guidance using an ArietaTM 650 DeepInsight ultrasound machine (Fujifilm, Tokyo, Japan) and 18-G 15-cm locking stylet trocar needle (Cook Medical, Bloomington, Indiana, USA). After successful US- and endoscopy-guided puncture of the targeted calyx, a stiff guidewire (Cook Medical, Bloomington, Indiana, USA) was inserted, enabling tract dilation with either an Ultraxx™ Nephrostomy Balloon (Cook Medical, Bloomington, Indiana, USA), a Amplatz rigid serial dilators (Cook Medical, Bloomington, Indiana, USA) or a one-step dilator (Karl Storz, Tuttlingen, Germany). A 24-F rigid nephroscope (Karl Strotz, Tuttlingen, Germany) was used for nephroscopy, although full inspection of the collecting system was not performed by all participants because the course primarily focused on ultrasound-guided access in supine PCNL.
After the procedure, participants completed a 24-question evaluation of the FFC model using a 5-point Likert scale (1 = strongly disagree/absolutely not realistic or useful; 5 = strongly agree/very realistic or useful), which was similar to the one previously used by Veys et al for the assessment of the TEC model (Supplementary Figure 1). The questionnaire assessed tissue quality, US imaging, procedural steps, overall experience compared to live patient procedures, and suitability of the model for both basic and advanced supine PCNL training.22 Descriptive statistical analysis for this cross-sectional study was conducted on the responses, with median values and interquartile ranges (IQRs) calculated, and the results are displayed using divergent bar graphs. The validity of the FFC model was evaluated using Messick’s contemporary framework, as outlined by Goldenberg and Lee,30 rather than traditional metrics such as face, content, and construct validity, which are now considered outdated. For all statistical analyses, R software environment for statistical computing and graphics (version 3.4.3, R Foundation, Vienna, Austria) was used.
Results
Sixteen questionnaires were collected at the end of the ultrasound-guided supine PCNL these Six urologists (38%) performed > 50 PCNLs (Table 1).
The course was generally well-attended, as most commented that it was useful. However, tactile sensation, skin stiffness, distensibility of the calyces, and US quality varied depending on the thawing of the cadavers. In particular, tactile sensation, skin stiffness, and distensibility of the calyces resembled real-life scenarios as cadavers thawed out. Similarly, US quality was worse in frozen cadavers and improved after irrigation with the collection system. Placing ureteric catheters and access sheaths was considered better than in formalin-embalmed cadavers, even if some resistance was still encountered at the vesicoureteral and ureteropelvic junctions, which sometimes required serial dilation before sheath placement. Finally, Valdivia-Galdakao positioning was considered somewhat more difficult than in real life because of rigor mortis, thawing of the cadaver, and partly due to insufficient equipment.
Despite the general comments, the objective measures showed good-to-excellent validity. The tissue quality of the collecting system in the FFC model was evaluated by assessing its color, consistency, and anatomy. These three aspects were found to be similar to real life (median [IQR]: 4 [3–4], 4 [3–4], and 5 [4–5]). The color of the FFC model was considered undisturbing, with good tissue quality and realistic organ color, even if tissue consistency was neither distinctly unrealistic nor convincingly realistic (median [IQR] Likert scores of 4 [3–4], 4 [3–4], and 3 [2–4], respectively). The anatomical landmarks were identified as excellent (median [IQR] Likert score 5 [4–5]), and the Galdakao-modified supine Valdivia position of the cadaver was considered good (median [IQR] Likert score 4 [3–5]). These results yielded a median [IQR] overall satisfaction with the FFC collection system of 4 [4–5] (Figure 1).
 |
Figure 1 Adjusted stacked distributions of the scores for each component of the assessment questionnaire for the fresh frozen cadaver model. |
US image assessment, identification of the kidney, collecting system, and surrounding tissue, and ultrasound of the dilated calyces were considered lifelike (median [IQR] Likert scores of 4 [4–5], 4 [3–4], 4 [2–4], and 4 [3–4], respectively). US-guided puncture of the dilated calyces was considered a realistic and useful tool (median [IQR] Likert scores 4 [4–4] and 4 [4–5], respectively), even if needle puncture of the skin was deemed not very realistic (median [IQR] Likert score 3 [3–4]) but still useful (median [IQR] Likert score 4 [4–4]). However, needle puncture of the kidney was considered both realistic and useful (median [IQR] Likert scores of 4 [3–4] and 4 [4–5], respectively). Similarly, one-step dilation of the kidney and surrounding tissues was considered good (median [IQR], 4 [4–4]). These results yielded a median [IQR] overall satisfaction with the ultrasound properties of FFC of 4 [4–5] (Figure 1).
No statistically significant differences in the responses were recorded among those who performed fewer than 50 PNCLs and the more experienced ones, except for the accuracy of the FFC model when considering the consistency of the collecting system and kidney entrance with the needle (median Likert score of 4 vs 3 for both, p<0.05).
Overall, responders were very satisfied with the FFC model, with excellent appropriateness for both initial and advanced training of PCNL (median [IQR] Likert scores of 5 [4–5] for all three, Figure 1).
Discussion
Acquiring skills in a safe and controlled environment outside the operating room has become increasingly important, not only for its potential to expedite the learning process but also to reduce surgical complications, thereby enhancing the quality and safety of patient care.31 This is particularly important in endourology, especially for PCNL and ECIRS, which are characterized by a steep learning curve for achieving proficiency in percutaneous renal access and may require up to 60 cases.
Despite the availability of various PCNL training models, a validated simulator capable of reliably transferring acquired skills to a clinical setting remains unavailable, thereby highlighting the need for further development.31 Despite ongoing advancements, most inanimate models fail to replicate the anatomical and tactile nuances of the human body.19
Cadaver-based training continues to be regarded as the cornerstone of surgical education owing to its unparalleled anatomical accuracy.27 However, cadavers used for surgical training are not without limitations. They do not exhibit bleeding or respiratory movements, and are associated with high initial costs. FFC and formalin-embalmed cadavers (FEC) were among the first cadaveric models to be used for surgical training.23,24 FFC, while anatomically realistic, has limited durability and carries a risk of infectious diseases. In contrast, FEC, although longer-lasting, suffers from an unpleasant odor and alterations in tissue properties, including flexibility and discoloration. Another possibility is TEC, which are thought to offer superior preservation of tissue texture, colour, and flexibility, while being low-odour, durable and reusable.18
TEC models were previously assessed in the context of US-guided PCNL training by Veys et al, in which participants rated their suitability for both beginner and advanced PCNL training in the supine position as excellent.22 In this study, we used the same questionnaire used by Veys et al to assess the validity of the FFC models as a training tool for US-guided PCNL and supine ECIRS. The FFC models received high ratings for training suitability, with overall satisfaction scores of five (IQR, 4–5). Tissue quality, particularly color and anatomy, was scored 4 (IQR, 3–4) to 5 (IQR, 4–5), but consistency was less uniform, with a median score of 3 (IQR, 2–4). Ultrasound imaging and needle puncture ratings ranged from 3 to 4 and improved as cadavers thawed. TEC models were also rated highly for overall satisfaction and appropriateness for training, with a median Likert score of 5 (IQR, 5–5). Tissue quality, including color and anatomy, received scores of 4 (IQR 4–5) to 5 (IQR 5–5), although the collecting system appeared paler, and skin penetration was less realistic, scoring 3 (IQR 2–4). Ultrasound image quality was consistently rated as 4–5 across the key parameters. These results suggest that both the FFC and TEC models meet Messick’s framework for content validity,30 with some differences in specific metrics, TEC excelling in procedural consistency, and FFC offering more lifelike surgical resistance.
Although the results of this study highlight the value of FFC as a training model for PCNL, several limitations that are shared with other cadaveric models should be noted. First, the evaluation relied on a non-validated questionnaire, which was, however, previously used by Veys et al.22 Additionally, the tactile sensation, skin stiffness, distensibility of the calyces, and US quality were dependent on the thawing of the cadavers. Despite these limitations and worth noting to better define model preparation in the pre-training setting, the variability might mirror real-life scenarios. Furthermore, unlike living patients, the FFC model lacks critical physiological features such as respiratory movements. Finally, the study is mainly based on the use of ultrasound for PCN. It would be interesting and important to evaluate the usefulness of using fresh frozen cadavers also for fluoroscopic puncture training.
Further studies are needed to determine whether training on FFC models translates to improved surgical performance and shorter learning curves in clinical practice. Comparative studies using other US-guided puncture training models such as TEC could also yield valuable insights.
Conclusions
Despite minor limitations, FFC demonstrated robust content validity as a training model for PCNL. Its application is particularly well-suited for training in US-guided renal access and supine ECIRS. The model provides a realistic and effective training experience, offering a promising tool for developing critical surgical skills, while minimizing radiation exposure and procedural risks.
Ethics
Written informed consent was obtained from all the urologists who participated in the questionnaire survey. No data from cadavers or patients were collected or evaluated in this study. No data were collected or evaluated by the urologists who replied to the survey.
Funding
There is no funding to report.
Disclosure
Dr Thomas Tailly is a consultant for Ambu, Boston Scientific, Cook Medical, Dornier and Storz, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Raheem OA, Khandwala YS, Sur RL, et al. Burden of urolithiasis: trends in prevalence, treatments, and costs. Eur Urol Focus. 2017;3(1):18–26. doi:10.1016/j.euf.2017.04.001
2. Mantica G, Balzarini F, Chierigo F, et al. The fight between PCNL, laparoscopic and robotic pyelolithotomy: do we have a winner? A systematic review and meta-analysis. Minerva Urol Nephrol. 2022;74(2):169–177. doi:10.23736/S2724-6051.21.04587-0
3. Kidney stones: surgical management guideline - American urological association Available from: https://www.auanet.org/guidelines-and-quality/guidelines/kidney-stones-surgical-management-guideline.
4. EAU guidelines on urolithiasis - uroweb [Internet].
5. Ghani KR, Andonian S, Bultitude M, et al. Percutaneous nephrolithotomy: update, trends, and future directions. Eur Urol. 2016;70(2):382–396. doi:10.1016/j.eururo.2016.01.047
6. Hajiha M, Baldwin DD. New technologies to aid in percutaneous access. Urol Clin North Am. 2019;46(2):225–243. doi:10.1016/j.ucl.2019.01.001
7. Quirke K, Aydin A, Brunckhorst O, et al. Learning curves in urolithiasis surgery: a systematic review. J Endourol. 2018;32(11):1008–1020. doi:10.1089/end.2018.0425
8. Schilling D, Gakis G, Walcher U, et al. The learning curve in minimally invasive percutaneous nephrolitholapaxy: a 1-year retrospective evaluation of a novice and an expert. World J Urol. 2011;29(6):749–753. doi:10.1007/s00345-010-0553-3
9. Yanase T, Taguchi K, Sugino T, et al. Defining a learning curve for urology trainees to achieve renal access without complications in endoscopic combined intrarenal surgery. Int J Urol. 2024;31(9):1046–1051. doi:10.1111/iju.15520
10. Bele U, Kelc R. Upper and lower urinary tract endoscopy training on Thiel-embalmed cadavers. Urology. 2016;93:27–32. doi:10.1016/j.urology.2016.01.040
11. Mishra S, Kurien A, Ganpule A, et al. Percutaneous renal access training: content validation comparison between a live porcine and a virtual reality (VR) simulation model. BJU Int. 2010;106(11):1753–1756. doi:10.1111/j.1464-410X.2010.09753.x
12. Häcker A, Wendt-Nordahl G, Honeck P, et al. A biological model to teach percutaneous nephrolithotomy technique with ultrasound- and fluoroscopy-guided access. J Endourol. 2007;21(5):545–550. doi:10.1089/end.2006.0327
13. Turney BW. A new model with an anatomically accurate human renal collecting system for training in fluoroscopy-guided percutaneous nephrolithotomy access. J Endourol. 2014;28(3):360–363. doi:10.1089/end.2013.0616
14. Klein JT, Rassweiler J, Rassweiler-Seyfried MC. Validation of a novel cost effective easy to produce and durable in vitro model for kidney-puncture and percutaneous nephrolitholapaxy-simulation. J Endourol. 2018;32(9):871–876. doi:10.1089/end.2017.0834
15. Abdallah MM, Salem SM, Badreldin MR, et al. The use of a biological model for comparing two techniques of fluoroscopy-guided percutaneous puncture: a randomised cross-over study. Arab J Urol. 2013;11(1):79–84. doi:10.1016/j.aju.2012.12.001
16. Mains E, Tang B, Golabek T, et al. Ureterorenoscopy training on cadavers embalmed by Thiel’s method: simulation or a further step towards reality? Cent Eur J Urol. 2017;70(1):81–87.
17. Healy SE, Rai BP, Biyani CS, et al. Thiel embalming method for cadaver preservation: a review of new training model for urologic skills training. Urology. 2015;85(3):499–504. doi:10.1016/j.urology.2014.11.009
18. Porzionato A, Polese L, Lezoche E, et al. On the suitability of Thiel cadavers for natural orifice transluminal endoscopic surgery (NOTES): surgical training, feasibility studies, and anatomical education. Surg Endosc. 2015;29(3):737–746. doi:10.1007/s00464-014-3734-0
19. Rai BP, Stolzenburg JU, Healy S, et al. Preliminary validation of Thiel embalmed cadavers for laparoscopic radical nephrectomy. J Endourol. 2015;29(5):595–603. doi:10.1089/end.2014.0719
20. Mantica G, Leonardi R, Diaz R, et al. Reporting ChAracteristics of cadaver training and sUrgical studies: the CACTUS guidelines. Int J Surg. 2022;101:106619. doi:10.1016/j.ijsu.2022.106619
21. Mantica G, Pini G, de Marchi D, et al. Intensive simulation training on urological mini-invasive procedures using Thiel-embalmed cadavers: the IAMSurgery experience. Arch Ital Urol Androl. 2020;92(2):93–96. doi:10.4081/aiua.2020.2.93
22. Veys R, Verpoort P, Van Haute C, et al. Thiel-embalmed cadavers as a novel training model for ultrasound-guided supine endoscopic combined intrarenal surgery. BJU Int. 2020;125(4):579–585. doi:10.1111/bju.14954
23. Song YK, Jo DH. Current and potential use of fresh frozen cadaver in surgical training and anatomical education. Anat Sci Educ. 2022;15(5):957–969. doi:10.1002/ase.2138
24. Mantica G, Leonardi R, Pini G, et al. The current use of human cadaveric models in urology: a systematic review. Minerva Urol Nefrol. 2020;72(3):313–320. doi:10.23736/S0393-2249.19.03558-6
25. Tunc L, Bozzini G, Scoffone CM, et al. Determination of face and content validity of cadaveric model for holmium anatomic endoscopic enucleation of the prostate training: an ESUT AEEP group study. Eur Urol Open Sci. 2021;32:28–34. doi:10.1016/j.euros.2021.07.005
26. Aydın A, Ahmed K, Baig U, et al. The SIMULATE ureteroscopy training curriculum: educational value and transfer of skills. World J Urol. 2021;39(9):3615. doi:10.1007/s00345-021-03604-w
27. Ahmed K, Aydin A, Dasgupta P, et al. A novel cadaveric simulation program in urology. J Surg Educ. 2015;72(4):556–565. doi:10.1016/j.jsurg.2015.01.005
28. Al-Jabir A, Aydin A, Abe T, et al. Validation of the advanced scope trainer for flexible ureterorenoscopy training. Urology. 2017;110:45–50. doi:10.1016/j.urology.2017.07.047
29. Al-Jabir A, Aydın A, Ahmed K, et al. The role of dry-lab and cadaveric simulation for cystoscopy and intravesical Botulinum toxin injections. Transl Androl Urol. 2019;8(6):673–677. doi:10.21037/tau.2019.11.11
30. Goldenberg M, Lee JY. Surgical education, simulation, and simulators-updating the concept of validity. Curr Urol Rep. 2018;19(7). doi:10.1007/s11934-018-0799-7
31. Noureldin YA, Andonian S. Simulation for percutaneous renal access: where are we? J Endourol. 2017;31(S1):S10–S19. doi:10.1089/end.2016.0587
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.