")
Back to Journals » International Journal of Women's Health » Volume 17
Global Trends in Incidence and Mortality Rates of Endometrial Cancer Among Individuals Aged 55 years and Above From 1990 to 2021: An Analysis of the Global Burden of Disease
Authors Gao S , Wang J, Li Z, Wang T , Wang J
Received 30 October 2024
Accepted for publication 26 February 2025
Published 6 March 2025 Volume 2025:17 Pages 651—662
DOI https://doi.org/10.2147/IJWH.S499435
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Songkun Gao,1 Jinhua Wang,2 Zhongxian Li,3 Tong Wang,1 Jiandong Wang1
1Gynecologic Oncology Department,Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing Maternal and Child Health Care Hospital, Beijing, 100026, People’s Republic of China; 2Department of Obstetrics and Gynecology, Beijing Youan Hospital, Capital Medical University, Beijing, 100069, People’s Republic of China; 3Key Laboratory of Nanobiological Effects and Safety, CAS Center for Excellence in Nanoscience, National Center for Nanoscience and Technology, Beijing, 100190, People’s Republic of China
Correspondence: Tong Wang; Jiandong Wang, Gynecologic Oncology Department, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing Maternal and Child Health Care Hospital, Qihelou Street Dongcheng District, Beijing, 100006, People’s Republic of China, Email [email protected]; [email protected]
Purpose: To describe the temporal trend of endometrial burden in postmenopausal women aged 55 years and above worldwide from 1990 to 2021, evaluate the age cohort effect, explore its influencing factors, and predict the disease burden in the next 15 years.
Patients and Methods: Using Joinpoint regression, data from the 2021 Global Burden of Disease Study were assessed for changes in endometrial cancer incidence rate, morbidity, and mortality in postmenopausal women aged 55 years and above. Age period cohort analysis helped estimate age, period, and cohort effects. The Das Gupta method helped analyze effects of different factors on endometrial cancer incidence and mortality among postmenopausal patients. ARIMA helped predict the endometrial cancer disease burden in postmenopausal women from 2022 to 2036.
Results: In 2021, globally, there were 360253 (326,176– 388545) cases and 84630 (75,523– 93215) deaths among postmenopausal patients with endometrial cancer. During 1990– 2021, the global endometrial cancer incidence in postmenopausal women gradually increased, while the mortality rate gradually decreased. Changes in disease incidence and mortality rates are mainly due to population growth and epidemiological changes, with little influence of age. The risk of endometrial cancer in postmenopausal women gradually increased with age, using age, period, and cohort average as the reference groups. The mortality rate decreased gradually decreased in 2019 and continued to rise thereafter. It is expected that by 2036, the incidence of endometrial cancer in postmenopausal women aged 55 years and above will increase by 6.5%, and the mortality rate will decrease by 8.0%.
Conclusion: The number of patients with postmenopausal endometrial cancer aged 55 years and above is still increasing, and it is necessary to establish a comprehensive screening and treatment mechanism to ensure prolongation of patient lifespan.
Keywords: postmenopausal, endometrial cancer, morbidity, mortality, GBD
Introduction
Endometrial cancer is a common gynecological cancer in women, causing over 2% of cancer-related deaths worldwide.1 Studies suggest that genetic factors, obesity, lifestyle, and some diseases are related to the incidence of endometrial cancer.2,3 The structure of the endometrium changes with fluctuations in estrogen and progesterone levels. Multiple pregnancies, early onset menarche, and menopause may lead to individual differences in estrogen exposure, resulting in different directions of endometrial cancer occurrence.4 Endometrial cancer is more common in perimenopausal and postmenopausal women.4 The median age at diagnosis of most patients with endometrial cancer is 67 years.5 The clinical manifestations and characteristics of endometrial cancer in the vast majority of pre-and postmenopausal women differ, with different pathological stages and subtypes.6 In postmenopausal patients, abnormal vaginal bleeding and imaging findings indicating endometrial thickening can aid in earlier diagnosis and treatment compared to younger individuals. However, the incidence rate of non-estrogen-related endometrial cancer in young patients is higher than that in postmenopausal patients, which leads to better prognosis in postmenopausal patients after standard treatment. It is undeniable that aging can lead to a decline in physiological functions and an increase in the incidence of age-related diseases. Due to advanced age at diagnosis and more aggressive tumor features, doctors may adopt fewer or less aggressive treatment methods, whether surgical or systemic.7
 |
Figure 1 Shows the incidence (rate), prevalence (rate), mortality (rate), and Disability Adjusted Life Years (DALYs) of endometrial cancer patients aged 55+years and above in 2021, categorized by age.(A) Incidence number in different age group (B) Prevalence number in different age group (C) Mortality number in different age group (D) DALYs in different age groups (E) Incidence rate in different age group (F) Prevalence rate in different age group (G) Mortality rate in different age group (H) DALYs in different age groups. |
With the advancement of medical technology, there have been significant changes in the screening and treatment of endometrial cancer, which have led to earlier detection and treatment, resulting in better patient prognosis. In a study of all age groups, the incidence and prevalence rate of endometrial cancer gradually increased from 1990 to 2017, and the mortality rate and disability life adjustment years decreased by more than 1% per year.8 However, research is lacking on endometrial cancer in postmenopausal women. The GBD database is commonly used for analyzing the incidence and mortality of different diseases.9
This study used the latest GBD data to describe the global incidence rate and mortality of postmenopausal patients with endometrial cancer from 1980 to 2021, summarized the changes in endometrial cancer screening and treatment, and predicted the disease burden over the next 15 years.
Patients and Methods
Data Source and Screening
The GBD study is currently the largest database available for estimating the prevalence and health burden of diseases, injuries, or risk factors. This is a comprehensive database that records the incidence and prevalence rates of > 300 diseases and injuries in 204 countries and regions. The conclusions obtained can be used for policy formulation, service planning, and further research. GBD quantifies the years of healthy life lost due to disease or injury through disability-adjusted life years (DALYs). The DALYs is a composite of years lived with disability and does not represent the sum of non-lethal burden and years of life with death.10
We obtained data from GBD 2021 (https://vizhub.healthdata.org/gbd-results/). The disease was designated as Uterine cancer. Generally the age at menopause in women is between 42 and 52 years.11 As the GBD database does not include relevant data on menopause, we included women over 55 years old in our study population, with age options including “55+years” and the age range of 55 years and above to achieve our research objectives.
We obtained the annual incidence rate, age-standardized incidence rate, prevalence of cases, age-standardized prevalence rate, DALYs, age-standardized DALYs rate, corresponding percentage changes, and corresponding 95% uncertainty intervals (UIs) by region and country from 1990 to 2019.
Statistical Analysis
We compared the incidence, prevalence, mortality, and DALYs of postmenopausal women with endometrial cancer between 1990 and 2021. The incidence rate, change rule, and trend turning point of morbidity and mortality were estimated using joinpoint regression.12
Using the Das Gupta method for decomposition analysis, we analyzed the impact of population age structure, population growth, and epidemiological trends on the disease burden of endometrial cancer in individuals aged 55 and above.13 An age-period-cohort model was used to test the impact of age, period, and cohort on health outcomes.14 When assessing the trend of the incidence rate by age, period, and cohort, this study used common classification criteria, and the age group and observation period were all 5 years apart. To include as many observation periods as possible to determine the long-term trend in the incidence rate, six time periods from 1990 to 2019 were selected. The study began in 1992 and data were analyzed using statistical software developed by the NIH (https://analysistools. cancer. gov/apc/). Autoregressive integrated moving average model (ARIMA) was employed for practical sequence analysis. Auto. arima() function was used to select the best optimization model based on Akaike information criteria, and the Ljung Box test was used to check whether the residual sequence was white noise. A Q-Q plot, autocorrelation function, and partial autocorrelation function was used to check the normality of the residual distribution. In this study, we used the R4.4.1 as the statistical software, ggplot2/reshape2/dplyr package for line and graph analysis and the forecast/gpubr/ggplot2/stats package for ARIMA model establishment and validation. Statistical significance was set at P < 0.05.
Results
We used data from 1990 to 2021 for our analysis. In the past 30 years, the number of cases of endometrial cancer in patients aged 55 years and above worldwide has increased from 141173 (95% CI: 131743–148151) to 360253 (95% CI: 326176–388,545), more than doubling. The incidence rate per 100000 has increased from 39.22 (95% CI: 36.6–41.16) in 1990 to 45.81 (95% CI: 41.47–49.4) in 2021. However, the number of deaths per 100000 postmenopausal patients due to endometrial cancer decreased by 1.82, and DALYs and Years of Life Loss also gradually decreased (Table 1).
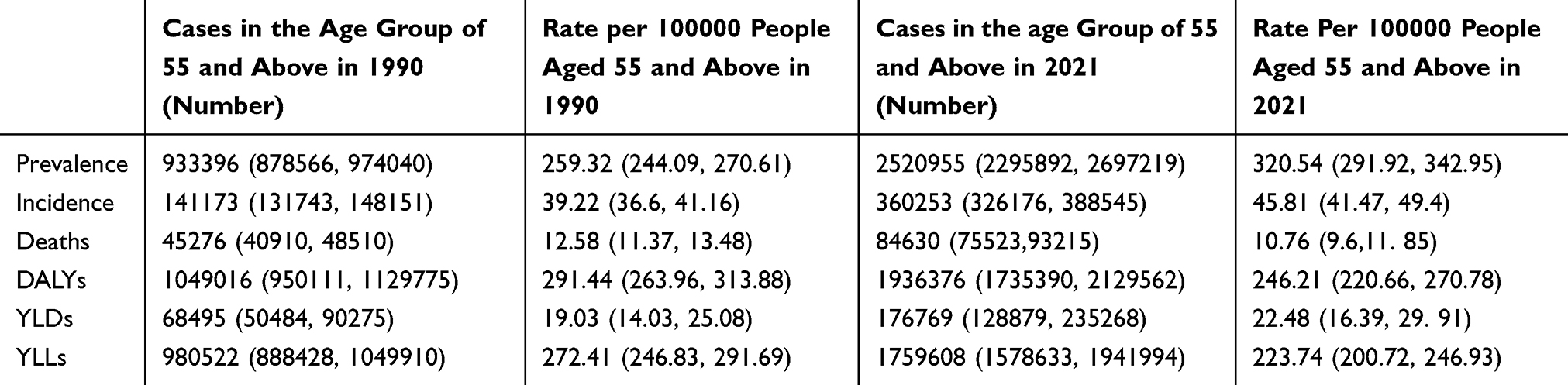 |
Table 1 Worldwide Prevalence, Incidence Rate, Mortality, YLLs, YLDs, and DALY of Endometrial Cancer Among Women Over 55 years of Age in 1990 and 2021 |
Figures 1 and 2 show the incidence rate, morbidity, mortality and DALYs of patients aged 55+ in grade 1990 and 2021. From the incidence results, the peak incidence of endometrial cancer in postmenopausal women in 1990 and 2021 was between 60–64 years, and the number of cases decreased with age thereafter. According to the death data for 1990 and 2021, patients aged 65–69 had the highest number of deaths. In 2021, the number of deaths among patients aged 60–65 was lower than that among patients aged 70–75, while in 1990, the number of deaths among patients aged 60–65 was higher. The DALYs were similar for patients aged 60–65 and 65–69 in 2021, whereas in 1990, the DALYs of patients aged 60–65 were higher than those of patients aged 65–69.
 |
Figure 2 Shows the incidence (rate), prevalence (rate), mortality (rate), and Disability Adjusted Life Years (DALYs) of endometrial cancer patients aged 55+years and above in 1990, categorized by age.(A) Incidence number in different age group (B) Prevalence number in different age group (C) Mortality number in different age group (D) DALYs in different age groups (E) Incidence rate in different age group F Prevalence rate in different age group (G) Mortality rate in different age group (H) DALYs in different age groups. |
In terms of incidence rate, the incidence rate of patients aged 75–79 years was the highest in 1990, followed by patients aged 65–69 years, and the incidence rate of patients aged 70–74 years was the highest in 2021. The incidence rate in the two groups of patients gradually increased after 55 years of age, with the highest incidence in patients aged 60–64, and then gradually decreased. The mortality rate had gradually increased. The DALYs were extended to 70–74 years in 2021 compared to 65–69 years in 1990.
We analyzed the global incidence, morbidity, and mortality rates of postmenopausal endometrial cancer between 1990 and 2021, as shown in Figure 3. From 1990 to 2021, the global incidence rate and prevalence rate of endometrial cancer among patients over 55 years of age increased. The incidence rate increased significantly in 1990–1994 (APC=0.78, P<0.05) and 2004–2015 (APC=0.51, P<0.05), and the prevalence rate increased significantly between 1990–1994 (APC=0.68, P<0.05), 2001–2005 (APC=1.50, P<0.05), and 2009–2018 (APC=1.37, P<0.05). The mortality rate showed a decreasing trend from 1990 to 2014 (P<0.05), with a slight increase in 2014 and 2018 (APC=0.82, P<0.05), and has continued to decline in recent years (APC=−0.71).
 |
Figure 3 The APC of incidence rate, morbidity and mortality of 55+years Endometrial cancer patients in Global from 1990 to 2019 (* means p-values<0.05 and significant results) (A) Incidence rate; (B) Disease incidence rate; (C) Mortality rate. |
As shown in Figure 4, over the past 30 years, the global incidence of diseases among patients aged 55 years and above has significantly increased, with population growth accounting for 72.74% for the increase in deaths, changes in epidemiological characteristics accounting for 27.13%, and population aging accounting for only 1.3%. In terms of mortality rate, epidemiological changes accelerated patient deaths, accounting for 42.71% of deaths. Population growth had a positive impact on mortality rate reduction, accounting for 140.54%, whereas population aging had little impact on mortality rate, accounting for only 1.17%.
 |
Figure 4 The role of three factors (aging, population and epidemiology) driving the change of incidence rate and mortality between 1990 and 2021 (A) incidence rate (B) mortality. |
Figures 5 and 6 show the effects of age cohort on the incidence and mortality rates of endometrial cancer in individuals aged 55 years and older. The results indicated that the incidence rate in patients over 55 years old gradually increased with age (P=0.00), reaching its highest point between 75–80 years old (Rate=2162.36492141.625–2183.303), and then gradually decreased (Figure 5A). From 2000 to 2005, a significant difference was noted in the incidence rate (P=0.00), showing a clear upward trend over time (Figure 5B).
 |
Figure 5 (A) Age effect of longitudinal age curve incidence rate (B) Period relative rate incidence rate (C) Queue relative rate incidence rate (D) Change in incidence rate compared with the previous year. |
 |
Figure 6 (A) Longitudinal age curve: Age effect of mortality rate; (B) Period relative rate: Period effect of mortality rate; (C) Cohort relative rate: Cohort effect of mortality rate; (D) Changes in mortality rate compared to the previous year. |
Figure 5C shows the relationship between the incidence rate and birth cohort, using the 1927 birth cohort as 1, we calculated the relative incidence rate of other birth years (P=0.00). The results indicated that the incidence rate significantly increased with birth age. The change in the incidence rate in the same age group compared to the previous year is shown in Figure 5D. The overall growth rate of patients in all age groups was 0.437, and the incidence rate in all age groups was > 0. This suggests that as the annual incidence rate of each age group increases, the growth of the incidence rate slows down before the age of 80 (the lowest is 0.167,0.098–0.236), and then gradually increases.
The mortality rate gradually increased with age (P=0.00, Figure 6A). The mortality rate of endometrial cancer patients over 55 years of age gradually decreased after 1992, with the lowest rate in 2014 (0.943, 0.932–0.955). Conversely, the mortality rate began to rise again in 2019 (0.967, 0.955–0.98) (Figure 6B). Similarly, using the 2027 birth cohort as 1, the results indicated a significant decrease in the mortality rate with age at birth (P=0.00, Figure 6C). Compared with the mortality rate of the previous year, the mortality rate of each age group has been decreasing annually, but the decline rate gradually decreased with increasing age. The mortality rate of patients aged > 95 years showed almost no change (P=0.017, Figure 6D).
The ARIMA model was used to quantitatively describe the trends in the incidence and mortality rates of postmenopausal endometrial cancer over the next 15 years (Figure 7). The disease rate optimization model was selected as (0,1,0), and after filtering with the Auto ARIMA() function, the AIC value was 25.21, and the residual distribution followed a normal distribution (P=0.438, Figure Supporting files SP1). The Q-Q and PACF plots are presented in Figure Supporting files SP2 and SP3, respectively. Ljung Box test confirmed that the residual error of the model was white noise (χ 2=6.8779, P=0.7369), and the incidence rate would rise to 48.99 per 100000 people in 2036, an increase of 6.5% compared with 2021. The optimization model for mortality rate was selected as (1,1,0), and after filtering with the Auto ARIMA() function, the AIC value was −64.79, and the residual distribution followed a normal distribution (P=0.343, Figure Supporting files SP4). The Q-Q and PACF plots are presented in Figure Supporting files SP5 and SP6. The Ljung Box test confirmed that the residual of the model is white noise (χ 2=4.4679, P=0.9238), and the mortality rate will decrease to 9.96/100000 in 2036, a 8.0% decrease compared to 2021.
 |
Figure 7 Predicted trends in the incidence and mortality rates of endometrial cancer in patients aged 55 and above over the next 15 years (2021–2036). The red line represents the true trend of incidence and mortality rates, while the dashed line represents the predicted trend. (A) Incidence (B) Mortality. |
Discussion
In this study, we analyzed the trend of endometrial cancer in postmenopausal women worldwide from 1990 to 2021. Over the past 30 years, the incidence of endometrial cancer in postmenopausal women has increased 2.55 times from 141173 cases in 1990 to 360253 cases in 2021, but remains consistent with the 2019 data (n=361970). The number of deaths increased from 45276 in 1990 to 84630, but the overall mortality rate showed a downward trend. This is consistent with research results for all patients with endometrial cancer.8 Zhang et al showed that in 195 countries/territories, more than two-thirds of the countries/territories had an upward trend in the incidence and prevalence rates, while more than half of these countries/territories had a downward trend in mortality and DALY.
According to our statistics, the rate of increase in endometrial cancer in postmenopausal individuals in the 20th century was significantly lower than that in the 21st century. Since 2010, the incidence rate of endometrial cancer in postmenopausal individuals has gradually increased. The screening method for endometrial cancer is closely related to the number of patients diagnosed. Initially, transvaginal ultrasound was considered the preferred imaging technique for first-line examination of abnormal uterine bleeding caused by endometrial abnormalities.15 Many studies have evaluated its role in postmenopausal endometrial cancer screening,16,17 but it is not as reliable as a single screening method. Some studies have shown that the ability to diagnose endometrial lesions solely based on cervical dilation and endometrial scraping is limited.18 In 1965, Marleschki introduced the earliest hysteroscopy.19 In the 1990s, hysteroscopy was promoted as a method for evaluating uterine lesions and its diagnostic role in postmenopausal individuals with abnormal uterine bleeding becoming well-recognized. Traditional cervical dilation and endometrial scraping were gradually replaced,20 and hysteroscopic-guided curettage was considered the gold standard for the diagnosis of abnormal uterine bleeding. Other methods, such as endometrial biopsy after saline infusion with contrast agents, have been gradually applied for the diagnosis of endometrial cancer.21,22 In our age group cohort analysis, a later birth cohort among the postmenopausal individuals with endometrial cancer corresponded to a higher incidence rate, which may be attributed to the popularity of these medical detection methods.
The decrease in the mortality rate of patients with endometrial cancer is mainly related to improvements in endometrial cancer treatment, including the development of radiotherapy, changes in surgical scope, and the development of chemotherapy drugs. The initial treatment for endometrial cancer mainly involves surgery and radiation therapy. Although radiation therapy reduces the vaginal recurrence rate of endometrial cancer, it does not lower the overall recurrence rate or improve patient survival. Since 1980, researchers have attempted to use adjuvant chemotherapy as an adjunct or alternative to radiation therapy. Randomized trials conducted by O’Brien et al23 and Morrow et al24 showed no difference in survival rates between patients who received pelvic radiotherapy and those who received chemotherapy combined with radiotherapy. Research on the use of a combination of chemotherapy and cytotoxic drugs as an alternative to radiotherapy and radiochemotherapy has begun. However, chemotherapy remains ineffective for recurrent and late-stage endometrial cancer.25 Experiments are also being conducted using different chemotherapeutic drugs and combinations of radiotherapy and chemotherapy. Paclitaxel, carboplatin, cisplatin, and doxorubicin have been shown to be effective in extending the survival time of patients with advanced endometrial cancer.26 Since 2010, chemotherapy has gradually become the first-line treatment for advanced endometrial cancer. Doxorubicin, platinum drugs, and paclitaxel have been widely used to treat stage III–IV endometrial cancer, and Phase II trials have been successful.27 Scholars have proposed the concept of “sandwich” treatment after surgery, which includes initial chemotherapy as soon as possible, followed by radiotherapy, and finally consolidation radiotherapy.28 Geller et al enrolled 23 IIA-IVB stage patients who received “sandwich” radiotherapy and chemotherapy after surgical treatment. Among all patients, five died or relapsed within 5 years. The estimated 3-year and 5-year progression-free survival rates were 80.4% and 73.7%, respectively. The overall survival rates at 3 and 5 years were 88.2% and 79.3%, respectively. This study demonstrated the feasibility of the sandwich method.28 Compared with patients receiving chemotherapy+radiotherapy or radiotherapy+chemotherapy, the “sandwich” regimen improved their 3-year survival rate and disease-free survival rate.29 The development of tissue gene sequencing is also ongoing, and research suggests that there are a large number of immunophenotypic mutations in POLE mutants and MSI-unstable endometrial cancer, which enhance antitumor immune infiltration.30 This suggests that drugs targeting the immune checkpoints can be applied to specific gene types of endometrial cancer. In clinical trials, PD-1/PD-L1 inhibitors have been used in patients with advanced endometrial cancer, showing good safety and antitumor effects.31 In 2014, according to The Cancer Genome Atlas for endometrioid and serous cancers, molecular subtyping features of endometrial cancer were proposed and included in the FIGO staging guidelines in 2022, which will affect disease staging and subsequent treatment.
The surgical treatment plan was continuously optimized. In 1980, the Mayo Clinic advocated vaginal endometrial resection because less than 20% of patients had larger metastases, while other scholars mentioned the importance of comprehensive exploration. Peritoneal cytology examinations, pelvic and para-aortic lymph node examinations, and other suspicious site biopsies were added to the standard surgical procedure; however, these results were not linked to subsequent treatment options.32 In 1987, owing to the recognition of endometrial risk factors (tumor grade, depth of muscle infiltration, involvement of lymphatic/vascular spaces, involvement of cervix/adnexa, peritoneal cytology testing, and lymph node status), preoperative staging evaluation of patients using magnetic resonance imaging and ultrasound was considered the standard procedure.33,34 Standard staging surgery for early endometrial cancer has also been established, and standard treatment methods for different surgical stages have been developed.35–38 Postoperative supplementary radiotherapy is considered the primary supplementary treatment method, and lymph node metastasis is considered a criterion for expanding the scope of radiotherapy. However, there is no established method or scope of standard radiotherapy.29,39 Radiotherapy is also used to treat local recurrences, especially vaginal fornix recurrences.40 In the first postoperative radiotherapy (PORTEC) experiment for endometrial cancer, 89% of patients with isolated recurrence who received pelvic radiotherapy and vaginal brachytherapy achieved complete remission, with 3-year and 5-year survival rates of 73% and 65%, respectively. However, patients with pelvic or distant metastases had poor prognosis.41 More randomized controlled studies comparing radiotherapy and chemotherapy have also been conducted, mainly comparing the disease-free survival rate and survival period between patients undergoing radiotherapy/radiochemotherapy/chemotherapy at different stages.42–44
The issue of lymph node dissection is still ongoing in 21st century. According to data from the SEER database, lymph node dissection can improve the 5-year survival rate of all patients with endometrial cancer.45,46 The FIGO recommends systematic pelvic lymph node dissection and para-aortic lymph node dissection for patients to clarify patient staging, but there is still controversy over whether lymph node dissection can benefit stage I patients, based on randomized controlled studies. Compared to type I endometrial cancer, new surgical procedures are available for type II endometrial cancer. Due to the high incidence of long-term complications, such as lymphedema after lymph node dissection, which can reach 6–23%, the NCCN included sentinel lymph node biopsy in the treatment guidelines for endometrial cancer in 2014.30 In approximately 85% of patients, the extent of disease metastasis can be identified through sentinel lymph node dissection, thereby avoiding excessive damage to the nonmetastatic lymph nodes.
The detection of disease prevalence and trend prediction are important for disease prevention and control. According to the ARIMA model, it is estimated that by 2036, the incidence rate of postmenopausal endometrial cancer will rise to 48.99 per 100000 people. In recent 5 years, endometrial cancer has become the fifth most common disease among women.47 As the incidence rates of obesity,48 diabetes,49 and hypertension50 increase, the number of patients with endometrial cancer will also increase. It is necessary to establish a screening strategy that covers a wide range of people, screens the elderly and high-risk groups, and further reduces the mortality rate of endometrial cancer.
Conclusion
From 1990 to 2021, the incidence rate and prevalence rate of endometrial cancer in postmenopausal individuals have shown an overall upward trend in the past 30 years, but the mortality rate has declined. The main reason for this result is an increase in the population, rather than changes in epidemiological factors or aging. The development of detection and treatment methods has significantly impacted the discovery and prognosis of endometrial cancer. Moreover, the incidence rate and mortality of postmenopausal endometrial cancer will continue the previous trend in the future.
Abbreviation
ARIMA, Auto regressive Integrated Moving Average Model; ASDR, Age Standardized Death Rate; ASIR, Age-Standardized Incidence Rate; ASPR, age standardized prevalence rate; DALYs, Disability Adjusted Life Years; GBD, Global Burden of Disease; NCCN, National Comprehensive Cancer Network; UI, uncertainty interval; YLL, Years of Life Lost; YLDS, Years Lived with Disability.
Ethical Approval
Given that data in the GBD database have been de-identified and are publicly available after permission, written informed consent for participation was not required for this study. The requirement of ethical approval for this was waived by the Institutional Review Board of Beijing Obstetrics and Gynecology Hospital. We confirm that this study was performed in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Beijing Municipal Science &Technology Commission (Research and Translational Application of Clinical Diagnostic and Treatment Technologies in the Capital, No. Z211100002921014).
Disclosure
All authors have no conflicts of interests to declare for this work.
References
1. Clarke MA, Long BJ, Del Mar Morillo A, Arbyn M, Bakkum-Gamez JN, Wentzensen N. Association of endometrial cancer risk with postmenopausal bleeding in women: a systematic review and meta-analysis. JAMA Intern Med. 2018;178(9):1210–1222. doi:10.1001/jamainternmed.2018.2820
2. Wu Y, Sun W, Liu H, Zhang D. Age at menopause and risk of developing endometrial cancer: a meta-analysis. Biomed Res Int. 2019;2019:8584130. doi:10.1155/2019/8584130
3. Raglan O, Kalliala I, Markozannes G, et al. Risk factors for endometrial cancer: an umbrella review of the literature. Int, J, Cancer. 2019;145:1719–1730. doi:10.1002/ijc.31961
4. Katagiri R, Iwasaki M, Abe SK, et al. Reproductive factors and endometrial cancer risk among women. JAMA Network Open. 2023;6(9):e2332296. doi:10.1001/jamanetworkopen.2023.32296
5. Zentrum für Krebsregisterdaten (ZfKD) beim Robert Koch-Institut. Epidemiologischer Datensatz des ZfKD auf Basis der Landeskrebsregisterdaten, verfügbare Diagnosejahre bis 2021. Version: Epi2022_2; 2024. doi:10.18444/5.03.01.0005.0018.0002
6. Lyu YL, Geng L, Wang FX, et al. Comparative analysis of pre- and postmenopausal endometrial cancer in 216 patients. Transl Cancer Res. 2023;12(3):595–604. doi:10.21037/tcr-22-1616
7. Forte M, Cecere SC, Di Napoli M, et al. Endometrial cancer in the elderly: characteristics, prognostic and risk factors, and treatment options. Crit Rev Oncol Hematol. 2024;204:104533. Epub 2024 Oct 22. PMID: 39442900. doi:10.1016/j.critrevonc.2024.104533
8. Zhang S, Gong TT, Liu FH, et al. Global, regional, and national burden of endometrial cancer, 1990-2017: results from the global burden of disease study, 2017. Front Oncol. 2019;9:1440. doi:10.3389/fonc.2019.01440
9. Gu B, Shang X, Yan M, et al. Variations in incidence and mortality rates of endometrial cancer at the global, regional, and national levels, 1990-2019. Gynecol Oncol. 2021;161(2):573–580.Epub 2021 Feb 5. PMID: 33551200. doi:10.1016/j.ygyno.2021.01.036
10. Santomauro DF, Purcell C, Whiteford HA, Ferrari AJ, Vos T. Grading disorder severity and averted burden by access to treatment within the GBD framework: a case study with anxiety disorders. Lancet Psychiatry. 2023;10(4):272–281.PMID: 36931778; PMCID: PMC10017349. doi:10.1016/S2215-0366(23)00037-8
11. Herson M, Kulkarni J. Hormonal agents for the treatment of depression associated with the menopause. Drugs Aging. 2022;39(8):607–618. doi:10.1007/s40266-022-00962-x
12. Kim HJ, Fay MP, Feuer EJ, et al. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. 2000;19:335–351. doi:10.1002/(SICI)1097-0258(20000215)19:3<335::AID-SIM336>3.0.CO;2-Z
13. Pan H, Zhao Z, Deng Y, et al. The global, regional, and national early-onset colorectal cancer burden and trends from 1990 to 2019: results from the global burden of disease study 2019. BMC Public Health. 2022;22(1):1896. doi:10.1186/s12889-022-14274-7
14. Luo L. Assessing validity and application scope of the intrinsic estimator approach to the age-period-cohort problem. Demography. 2013;50:1945–1967. doi:10.1007/s13524-013-0243-z
15. Karlsson B, Granberg S, Wikland M, et al. Transvaginal ultrasonography of the endometrium in women with postmenopausal bleeding—a Nordic multicenter study. Am J Obstet Gynecol. 1995;172:1488–1494. doi:10.1016/0002-9378(95)90483-2
16. Szabó I, Szánthó A, Német J, Csapó Z, Szirmai K, Papp Z. A myometrium inváziójának meghatározása endometriumcarcinomában transvaginalis ultrahangvizsgálattal assessment of myometrial invasion in endometrial cancer by transvaginal ultrasonography. Orv Hetil. 1997;138(21):1323–1327.
17. Kurjak A, Shalan H, Sosic A, et al. Endometrial carcinoma in postmenopausal women: evaluation by transvaginal color Doppler ultrasonography. Am J Obstet Gynecol. 1993;169(6):1597–1603.PMID: 8267069. doi:10.1016/0002-9378(93)90443-m
18. Schmidt T, Breidenbach M, Nawroth F, et al. Hysteroscopy for asymptomatic postmenopausal women with sonographically thickened endometrium. Maturitas. 2009;62(2):176–178.Epub 2009 Jan 3. PMID: 19121901. doi:10.1016/j.maturitas.2008.11.018
19. Russell JB. History and development of hysteroscopy. Obstet Gynecol Clin North Am. 1988;15(1):1–11. doi:10.1016/S0889-8545(21)00098-X
20. Clark TJ, Voit D, Gupta JK, Hyde C, Song F, Khan KS. Accuracy of hysteroscopy in the diagnosis of endometrial cancer and hyperplasia: a systematic quantitative review. JAMA. 2002;288(13):1610–1621. doi:10.1001/jama.288.13.1610
21. Dijkhuizen FP, Mol BW, Bongers MY, Brolmann HA, Heintz AP. Cost-effectiveness of transvaginal sonography and saline infused sonography in the evaluation of menorrhagia. Int J Gynaecol Obstet. 2003;83:45–52. doi:10.1016/S0020-7292(03)00080-8
22. Leone FP, Carsana L, Lanzani C, Vago G, Ferrazzi E. Sonohysterographic endometrial sampling and hysteroscopic endometrial biopsy: a comparative study. Ultrasound Obstet Gynecol. 2007;29(4):443–448. doi:10.1002/uog.3981.
23. O’brien ME, Killackey M. Adjuvan t th er apy in high-risk endometrial adenocarcinoma Proc. ASCO. 1994;1(3):249.
24. Morrow CP, Bundy BN, Homesley HD. Doxorubicin as an adjuvan t follow in g sur ger y an d r adiation th er ap y in p atien ts w ith h igh -r isk en dom etr ial carcinoma, stage 1 and occult stage II: a gynecologic on co lo gy gr o up study. Gyn Ecol on Col. 1990;36:166–171.
25. Elit L, Hirte H. Novel strategies for systemic treatment of endometrial cancer. Expert Opin Investig Drugs. 2000;9(12):2831–2853. doi:10.1517/13543784.9.12.2831
26. Burke WM, Orr J, Leitao M, et al. SGO Clinical Practice Endometrial Cancer Working Group. Society of gynecologic oncology clinical practice committee. endometrial cancer: a review and current management strategies: part II. Gynecol Oncol. 2014;134(2):393–402. doi:10.1016/j.ygyno.2014.06.003
27. Moxley KM, McMeekin DS. Endometrial carcinoma: a review of chemotherapy, drug resistance, and the search for new agents. Oncologist. 2010;15(10):1026–1033. doi:10.1634/theoncologist.2010-0087
28. Shah PH, Kudrimoti M, Feddock J, Randall M. Adjuvant treatment for stage IIIC endometrial cancer: options and controversies. Gynecol Oncol. 2011;122(3):675–683. doi:10.1016/j.ygyno.2011.05.018
29. Secord AA, Havrilesky LJ, Dm O, et al. A multicenter evaluation of sequential multimodality therapy and clinical outcome for the treatment of advanced endometrial cancer. Gynecol Oncol. 2009;114(3):442–447. doi:10.1016/j.ygyno.2009.06.005
30. Rooney MS, Shukla SA, Wu CJ, Getz G, Hacohen N. Molecular and genetic properties of tumors associated with local immune cytolytic activity. Cell. 2015;160:48–61. doi:10.1016/j.cell.2014.12.033
31. Makker V, Rasco D, Vogelzang NJ, et al. Lenvatinib plus pembrolizumab in patients with advanced endometrial cancer: an interim analysis of a multicentre, open-label, single-arm, Phase 2 trial. Lancet Oncol. 2019;20(5):711–718.Epub 2019 Mar 25. PMID: 30922731. doi:10.1016/S1470-2045(19)30020-8
32. Stallworthy JA. Surgery of endometrial cancer in the Bonney tradition. Ann R Coll Surg Engl. 1971;48(5):293–305.
33. Cagnazzo G, D’Addario V, Martinelli G, Lastilla G. Depth of myometrial invasion in endometrial cancer: preoperative assessment by transvaginal ultrasonography and magnetic resonance imaging. Ultrasound Obstet Gynecol. 1992;2(1):40–43. doi:10.1046/j.1469-0705.1992.02010040.x
34. Innocenti P, Agostini S, Erroi C, Ambrogetti D, Cellerini A, Nori J.Ruolo della risonanza magnetica nella stadiazione del carcinoma endometriale role of magnetic resonance in the staging of endometrial carcinoma. Radiol Med. 1991;81(5):678–683.
35. Lanciano RM, Corn BW, Schultz DJ, Kramer CA, Rosenblum N, Hogan WM. The justification for a surgical staging system in endometrial carcinoma. Radiother Oncol. 1993;28(3):189–196. doi:10.1016/0167-8140(93)90057-f
36. Trimble EL, Jones HW. Management of stage II endometrial adenocarcinoma. Obstet Gynecol. 1988;71:323–326.
37. Lambrou NC, Gómez-Marín O, Mirhashemi R, et al. Optimal surgical cytoreduction in patients with stage III and stage IV endometrial carcinoma: a study of morbidity and survival. Gynecol Oncol. 2004;93(3):653–658. doi:10.1016/j.ygyno.2004.03.015
38. Candiani GB, Belloni C, Maggi R, Colombo G, Frigoli A, Carinelli SG. Evaluation of different surgical approaches in the treatment of endometrial cancer at FIGO stage I. Gynecol Oncol. 1990;37(1):6–8. doi:10.1016/0090-8258(90)90297-x
39. Network NCC. NCCN clinical practice guidelines in oncology: uterine neoplasms (version 1.2018) vol. 2018; 2017.
40. van den Heerik ASVM, Horeweg N, de Boer SM, et al. Adjuvant therapy for endometrial cancer in the era of molecular classification: radiotherapy, chemoradiation and novel targets for therapy. Int J Gynecol Cancer. 2021;31(4):594–604.Epub 2020 Oct 20. PMID: 33082238; PMCID: PMC8020082. doi:10.1136/ijgc-2020-001822
41. Creutzberg CL, Nout RA, Lybeert MLM, et al. Fifteen-year radiotherapy outcomes of the randomized PORTEC-1 trial for endometrial carcinoma. Int J Radiat Oncol Biol Phys. 2011;81:e631–8. doi:10.1016/j.ijrobp.2011.04.013
42. Randall ME, Filiaci V, McMeekin DS, et al. Phase III trial: adjuvant pelvic radiation therapy versus vaginal brachytherapy plus paclitaxel/carboplatin in high-Intermediate and high-risk early stage endometrial cancer. J Clin Oncol. 2019;37:1810–1818. doi:10.1200/JCO.18.01575
43. de Boer SM, Powell ME, Mileshkin L, et al. Adjuvant chemoradiotherapy versus radiotherapy alone in women with high-risk endometrial cancer (PORTEC-3): patterns of recurrence and post-hoc survival analysis of a randomised Phase 3 trial. Lancet Oncol. 2019;20:1273–1285. doi:10.1016/S1470-2045(19)30395-X
44. Matei D, Filiaci V, Randall ME, et al. Adjuvant chemotherapy plus radiation for locally advanced endometrial cancer. N Engl J Med. 2019;380:2317–2326. doi:10.1056/NEJMoa1813181
45. Chan JK, Wu H, Cheung MK, et al. The outcomes of 27,063 women with unstaged endometrioid uterine cancer. Gynecol Oncol. 2007;106:282–288. doi:10.1016/j.ygyno.2007.05.033
46. Smith DC, Macdonald OK, Lee CM, Gaffney DK. Survival impact of lymph node dissection in endometrial adenocarcinoma: a surveillance, epidemiology, and end results analysis. Int J Gynecol Cancer. 2007;18:255–261. doi:10.1111/j.1525-1438.2007.01020.x
47. Contreras NA, Sabadell J, Verdaguer P, Julià C, Fernández-Montolí ME. Fertility-sparing approaches in atypical endometrial hyperplasia and endometrial cancer patients: current evidence and future directions. Int J mol Sci. 2022;23(5):2531.PMID: 35269674; PMCID: PMC8910633. doi:10.3390/ijms23052531
48. World Health Organization. World Obesity Day 2022—Accelerating Action to Stop Obesity. Geneva, Switzerland: World Health Organization; 2022.
49. Peng Y, Liu F, Wang P, et al. Association between diabetes at different diagnostic ages and risk of cancer incidence and mortality: a cohort study. Front Endocrinol. 2023;14:1277935. PMID: 37900125; PMCID: PMC10600378. doi:10.3389/fendo.2023.1277935
50. Angel-Korman A, Rapoport V, Leiba A. The relationship between hypertension and cancer. Isr Med Assoc J. 2022;24(3):165–169. PMID: 35347929.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predictors of Cardiovascular Morbidity Among Adult Hypertensive Patients: A Cross-Sectional Study from the Kingdom of Saudi Arabia
Al-Ghamdi S, Aldosari KH, Hussain ABO
Patient Preference and Adherence 2023, 17:1361-1369
Published Date: 6 June 2023
Uneven Between-Hospital Distribution of Patient-Related Risk Factors for Adverse Outcomes of Colorectal Cancer Treatment: A Population-Based Register Study
Rattenborg S, Möller S, Frostberg E, Rahr HB
Clinical Epidemiology 2023, 15:867-880
Published Date: 22 July 2023
High Preoperative Systemic Immune-Inflammation Index Values Significantly Predicted Poor Outcomes After on-Pump Coronary Artery Bypass Surgery
Parmana IMA, Boom CE, Poernomo H, Gani C, Nugroho B, Cintyandy R, Sanjaya L, Hadinata Y, Parna DR, Yulia M, Hanafy DA
Journal of Inflammation Research 2024, 17:755-764
Published Date: 7 February 2024
Health Hazard Among Shrimp Cultivators in India: A Quantitative Burden of Disease Study
Swain CK, Rout HS, Jakovljevic M
International Journal of General Medicine 2024, 17:1101-1116
Published Date: 21 March 2024
Early Postoperative Complications in Colorectal Cancer Patients Following Colorectal Surgery Among Yemeni Patients: A Prospective Study
Al-Amry AL, Obadiel YA, Al-Shehari MM, Gailan WM, Bajubair MH, Jowah HM
Open Access Surgery 2024, 17:81-90
Published Date: 26 June 2024