")
Back to Journals » Patient Preference and Adherence » Volume 19
Higher Compliance with Treatment Administration Instructions for Injectable Dulaglutide versus Oral Semaglutide Reported by People with Type 2 Diabetes in Clinical Practice Settings in Spain: The TRU-Experience Study
Authors Díaz-Cerezo S, Artime E , Redondo-Antón J , Duque N , Spaepen E, Mangas Cruz MÁ, Arnas-Leon C, Olveira G , Rodríguez IR, Julián Alagarda MT, Valdés N , Merchante AÁ , Masmiquel L, Rubio-de Santos M
Received 30 November 2024
Accepted for publication 31 March 2025
Published 1 May 2025 Volume 2025:19 Pages 1231—1244
DOI https://doi.org/10.2147/PPA.S509483
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Silvia Díaz-Cerezo,1 Esther Artime,1 Jennifer Redondo-Antón,1 Natalia Duque,1 Erik Spaepen,2 Miguel Ángel Mangas Cruz,3 Claudia Arnas-Leon,4 Gabriel Olveira,5– 8 Irene Rodríguez Rodríguez,9 María Teresa Julián Alagarda,10 Nuria Valdés,11,12 Agustín Ángel Merchante,13 Lluís Masmiquel,9 Miriam Rubio-de Santos1
1Medical Department. Eli Lilly and Company, Alcobendas, Madrid, Spain; 2HaaPACS GmbH, Schriesheim, Germany; 3Department of Endocrinology and Nutrition, Hospital Universitario Virgen del Rocío, Seville, Spain; 4Department of Endocrinology and Nutrition, Hospital Universitario de Gran Canaria Doctor Negrín, Las Palmas, Spain; 5Department of Endocrinology and Nutrition, Hospital Regional Universitario de Málaga, Málaga, Spain; 6Institute of Biomedical Research in Malaga (IBIMA)-Bionand Platform, University of Malaga, Málaga, Spain; 7Department of Medicine and Dermatology, Faculty of Medicine, University of Malaga, Málaga, Spain; 8CIBER of Diabetes and Associated Metabolic Diseases, Carlos III Health Institute, Madrid, Spain; 9Department of Endocrinology and Nutrition, Hospital Son Llàtzer, Palma, Spain; 10Department of Endocrinology and Nutrition, Hospital Universitario Germans Trias i Pujol, Badalona, Spain; 11Department of Endocrinology and Nutrition, Hospital Universitario Cruces Biobizkaia, Barakaldo, Spain; 12Endocrinology and Nutrition Department, Universidad del País Vasco/EHU, CIBERDEM, CIBERER, Endo-ERN, Bizkaia, Spain; 13Department of Endocrinology and Nutrition, Hospital General de Castellón, Castellón, Spain
Correspondence: Silvia Díaz-Cerezo, Eli Lilly and Company, Av. de la Industria 30, Madrid, Alcobendas, 28108, Spain, Email [email protected]
Purpose: This study compared patient-reported compliance with package leaflet administration instructions of two glucagon-like peptide 1 receptor agonists (GLP-1 RAs) for the treatment of type 2 diabetes (T2D): weekly injectable dulaglutide and daily oral semaglutide.
Patients and Methods: This was an observational cross-sectional study conducted in Endocrinology Units in Spain. Patients with T2D receiving weekly injectable dulaglutide or daily oral semaglutide at study enrolment who had initiated treatment 3– 12 months before were consecutively recruited during routine visits. Clinical data were extracted from the participants´ medical records. An ad-hoc questionnaire asked how often all and each of the administration instructions specific to each treatment were being followed (eg, timing, steps of intake). Compliance in both groups was calculated using relative and absolute frequencies and matching using the FMA model. The relationship between compliance and sociodemographic/clinical variables was assessed using bivariate analyses. Logistic regression analyses were performed to identify predictors of compliance.
Results: A total of 95 participants treated with weekly injectable dulaglutide and 135 participants treated with daily oral semaglutide were evaluated. More participants treated with weekly injectable dulaglutide (96.8%) than participants treated with daily oral semaglutide (90.4%) were compliant with all package leaflet administration instructions. After adjusting for potential between-group imbalances, higher compliance in the weekly injectable dulaglutide group compared with the daily oral semaglutide group was observed (odds ratio=3.2, 95% confidence interval 1.4– 21.3).
Conclusion: Compliance with package leaflet administration instructions was significantly higher in patients with T2D receiving weekly injectable dulaglutide compared to those receiving daily oral semaglutide. This type of real-world compliance data can inform strategies to improve patient education and adherence, and physician prescribing practices, with the goal of ultimately leading to better clinical outcomes and quality of life.
Keywords: glucagon-like peptide 1 receptor agonists, injectable administration, oral administration, treatment adherence, real world evidence, endocrinology
Introduction
Type 2 diabetes (T2D) is a chronic, progressive, metabolic disease characterized by the presence of high levels of glucose in the blood.1 Current guidelines indicate that the main goal of T2D treatment is to prevent or delay diabetes-related complications, which are mainly cardiovascular, and to maintain quality of life.1,2 Among the multiple therapeutic options available for the treatment of T2D, some glucagon-like peptide-1 receptor agonists (GLP-1 RAs) are drugs that, in addition to their strong anti-hyperglycemic and weight-lowering properties, can provide cardiovascular and renal benefits.1 Most GLP-1 RAs currently commercially available in Spain (dulaglutide, liraglutide, and semaglutide) are administered by subcutaneous injections; in addition, oral semaglutide has also been available in Spain since November 2021. Differences in the profile and administration methods of GLP-1 RAs may play an essential role in treatment adherence, persistence, and eventually real-world effectiveness of these drugs. Prior studies indicate that higher adherence to treatment can contribute to improved glycemic control in people with T2D, which, in turn, can help reduce the risk of cardiovascular disease, one of the main goals of treatment in T2D.2,3
Generally, evidence suggests that less complex treatment administration schedules promote adherence, partly due to the ease of administration and patient compliance with the instructions for use.4,5 Dulaglutide is a once-weekly injectable GLP-1 RA, which is provided in a prefilled pen and can be administered at any time of the day, independent of meals, and should be injected in the abdomen, thigh, or upper arm.6,7 In contrast, oral semaglutide is administered once a day, on an empty stomach, at any time of the day. The tablet should be taken whole, without splitting or chewing, with a glass (approximately 120 mL) of water. In addition, once the tablet has been swallowed, it is necessary to wait 30 minutes before eating, drinking, or taking any other oral medication.8 The REVISE study evaluated the preferences among people with T2D regarding weekly injectable dulaglutide and daily oral semaglutide.9 People with T2D preferred oral treatments versus once-weekly injectable drugs with a ratio of 3:1 before patients were aware of the product-specific instructions for administration. This preference ratio changed to 1:1 when details of the product-specific administration profile (weekly injectable dulaglutide and daily oral semaglutide) were provided.9 Timing and steps of intake were the main reasons for switching from an initial preference for a daily oral to the weekly injectable dulaglutide profile. The REVISE study also showed that administration instructions play an important role in the choice of medication. Preferences depend on several factors, such as the flexibility and complexity of the treatment regimen, the route, the frequency of administration, and the patient’s lifestyle.9
Understanding differences in compliance between medications can provide valuable insights for developing strategies to improve patient education, optimize prescriptions, and enhance therapeutic adherence, ultimately leading to better clinical outcomes and quality of life. No study to date has compared if there are differences in compliance with administration instructions between weekly injectable dulaglutide versus daily oral semaglutide among users in the real world. To address this issue, the TRU-Experience study compared patient-reported compliance with treatment administration instructions of these two drugs in people with T2D in clinical practice in Spain. Additionally, the study aimed to describe the socio-demographic and clinical characteristics of people treated with weekly injectable dulaglutide and those treated with daily oral semaglutide, identify key drivers (socio-demographic, treatment-related, and clinical) of patient-reported compliance with package leaflet recommendations regarding the method of administration, and identify aspects of the method of treatment administration where patients are less/more compliant.
Materials and Methods
Study Design
This was an observational, multicenter comparative study with cross-sectional data collection and retrospective extraction of patient medical records, conducted in seven endocrinology units in Spain, in people with T2D treated with weekly injectable dulaglutide or daily oral semaglutide. Data collection took place from November 2022 to July 2023 (Figure S1). At the time the study started, participants were already on treatment with weekly injectable dulaglutide or daily oral semaglutide, so there was no attempt to influence prescribing patterns, and treatment decisions were solely at the discretion of the investigator and the participant, and completely independent of participation in the study. All participants in the study provided signed informed consent, and the study was approved by the Ethics Committee for Drugs Research of the Hospital Universitario Fundación Alcorcón (Reg. 22/55). This study was conducted in accordance with the protocol and ethical principles that have their origin in the Declaration of Helsinki and that are consistent with applicable Good Pharmacoepidemiology Practices and applicable laws and regulations of Spain.
Site and Participant Selection
A feasibility assessment was conducted to guide site selection and to ensure that enough participants on treatment with weekly injectable dulaglutide or daily oral semaglutide and with data were available to meet study objectives. The sites had to be endocrinology units using GLP-1 RAs in their routine practice, with enough patients meeting the selection criteria within the planned data collection period, geographically spread across Spain, and with accessible medical records. The staff of the site had to be available and willing to participate in the study, with a record of experience in observational studies, and with no participation in other studies that could interfere with recruitment.
Only adults (≥18 years of age) receiving weekly injectable dulaglutide or daily oral semaglutide with a diagnosis of T2D who had started treatment at least 3 months and no more than 12 months prior to inclusion in the study were eligible to participate. Also, participants had to be able to understand and answer study questionnaires correctly (according to the investigator’s opinion), and sign the Informed Consent to participate in the study voluntarily. People with T2D who were participating in any clinical trial or patient support programs or who were unable to self-administer treatment were excluded.
Data Collection
The study collected data reported by the patient via ad hoc electronic questionnaires (e-questionnaires) during a routine care visit to the site, as well as secondary data extracted from the participant’s medical records by the site investigator (Figure S1). Two distinct e-questionnaires were developed in Spanish using the same language as in the Spanish package leaflet for each treatment of interest. No additional testing was required for the purpose of the study. The e-questionnaires (Table 1) recorded self-reported compliance with instructions in the drug package leaflet regarding the method of administration.10,11 The weekly injectable dulaglutide e-questionnaire contained four close-ended questions and the daily oral semaglutide questionnaire contained six close-ended questions. The first question in each of the e-questionnaires evaluated all treatment administration instructions together, and the other questions evaluated the different instructions separately (Table 1). Each participant responded to the questions from one questionnaire (weekly injectable dulaglutide or daily oral semaglutide) according to the specific treatment they were receiving. After confirming that the person with T2D met the study selection criteria and agreed to participate in the study, the participants completed the e-questionnaire on their own (web-based platform), without the assistance of site personnel, during or at the end of the medical consultation in the same consultation room. The e-questionnaire was designed so that it would not take more than 5 minutes to complete. Participants were reminded that this study was not intended to judge anyone, that the doctor/site personnel would not have access to the patient’s answers, that it would not change the care they received regardless of what they answered, and that their data would be coded and disassociated so that it was not linked to their personal data. Participants were not remunerated for participating in the study.
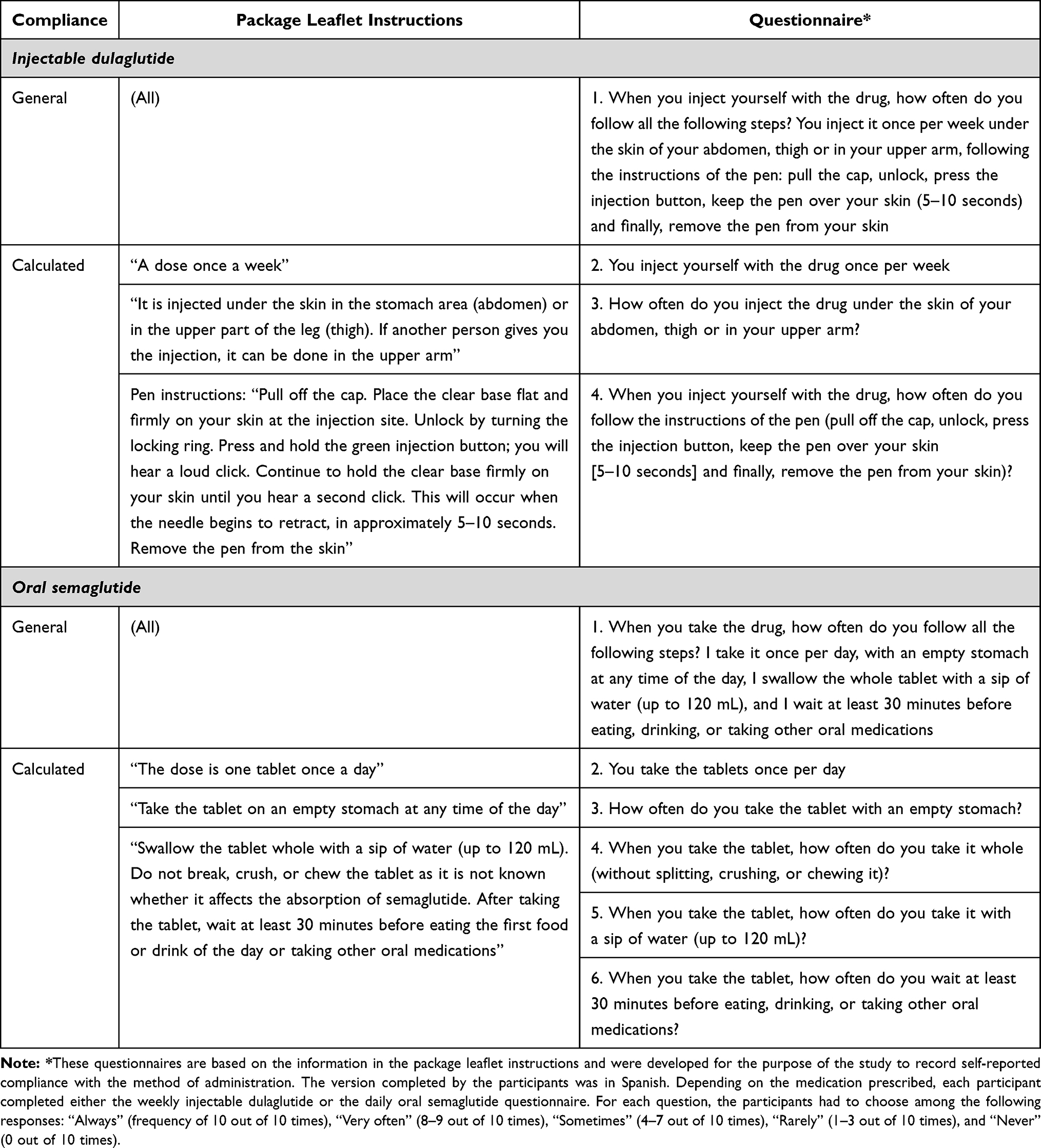 |
Table 1 Type of Compliance (See Methods for Details), Package Leaflet Instructions, and Drug-Specific Questionnaires |
In addition, once participants had completed the e-questionnaire, socio-demographic (age, gender, educational level) and clinical data (T2D diagnosis date, comorbidities, glycated hemoglobin [HbA1c], body mass index [BMI], treatment data on prior GLP-1 RA use and concomitant treatments) were extracted from the participant’s medical records by the site investigator (Figure S1). The investigator selected those comorbidities present in each patient from a predefined list. The investigator could complete the clinical and treatment-related variables after the visit.
Endpoints and Assessments
The primary endpoint was to compare patient-reported compliance with all recommendations provided in the package leaflet regarding the method of administration with weekly injectable dulaglutide versus daily oral semaglutide. Compliance was evaluated by considering the answers to questions in the e-questionnaire on how often treatment administration instructions were being followed, using a five-point Likert Scale: 0–4 (0 = always; 1 = very often; 2 = sometimes; 3 = rarely; 4 = never), where “always” represents a frequency of 10 out of 10 times, “very often”: 8–9 out of 10 times, “sometimes”: 4–7 out of 10 times, “rarely”: 1–3 out of 10 times, and “never”: 0 out of 10 times. “General compliance” was evaluated using responses to question 1 in both questionnaires, and “calculated compliance” was determined based on the answers to questions 2–4 for weekly injectable dulaglutide and 2–6 for daily oral semaglutide questionnaires. Participants were classified as “general” compliant if they responded “always” or “very often” to question 1 of the questionnaires. Participants were classified as non-compliant if they gave a different answer. Participants were classified as “calculated” compliant if they responded “always” or “very often” to questions 2–4 for weekly injectable dulaglutide participants, or 2–6 for daily oral semaglutide participants, evaluating each instruction independently. They could also answer “sometimes” or “rarely” to one of the questions, but not with “never” and still be considered compliant. Participants were classified as “non-compliant” in the remaining cases.
Further, an ad-hoc analysis of general compliance was conducted, considering as compliant only those participants that “always” followed all the instructions (item 1 of the questionnaires).
The secondary endpoints included describing the socio-demographic and clinical characteristics of the study participants, identifying key drivers of patient-reported compliance with package leaflet recommendations, and identifying features of treatment administration where patients were less/more compliant. Sociodemographic (sex, age), treatment-related (GLP-1 RAs prescribed, GLP-1 RA dosage, concomitant treatments, additional diabetes treatment, administration route of previous treatment), and clinical variables (weight, BMI, comorbidities, time between HbA1c tests, HbA1c difference before starting treatment with weekly injectable dulaglutide or daily oral semaglutide and last available value, time from diagnosis to treatment onset, time from treatment onset to patient inclusion) were explored as drivers of participant-reported compliance.
Statistical Analysis
Sample Size Calculation
In the absence of data on compliance with package leaflet recommendations from previous studies, treatment adherence was used as a proxy to estimate sample size. Approximately 60% of people on weekly injectable dulaglutide or daily oral semaglutide have been found to be adherent to treatment.12 With a unilateral confidence level of 95%, a power of 85%, a non-inferiority margin of 15%,13 and applying the formula:14

a minimum sample size of 306 people with T2D treated with weekly injectable dulaglutide or daily oral semaglutide for 3–12 months (153 people per group) was estimated. Assuming a 10% drop-out rate (mainly due to withdrawal or missing data), the study aimed to recruit 340 participants (170 per group). Due to operational and feasibility challenges encountered during recruitment, the final sample included 95 subjects receiving weekly injectable dulaglutide and 135 receiving daily oral semaglutide, corresponding to a statistical power of 75.1%, which was considered adequate to perform the statistical analysis.
Other Analyses
Descriptive statistics (mean, standard deviation [SD], or relative and absolute frequencies) were used to describe demographic and clinical characteristics.
To analyze differences in treatment compliance between weekly injectable dulaglutide and daily oral semaglutide, an un-adjusted analysis was conducted in which proportions of subjects who were considered compliant with treatment instructions from the package leaflet for each group were calculated. Patients were classified as meeting general or calculated compliance criteria as indicated in the previous section.
After the un-adjusted analysis, a frequentist model averaging (FMA) approach was applied to minimize the potential between-group variation at baseline due to non-randomization. The variables used in balancing scores included age, BMI, prior GLP-1 RA, comorbidities, time since diagnosis, HbA1c before current GLP-1 RA, current GLP-1 RA, sex, and education (Supplementary Table S1). The FMA approach runs several matching methods (propensity scores matching or weighting, regression, etc)., giving more weight to the methods which fit the data better and downweighing methods that do not have good predictive ability, and then produces a final estimate that is a weighted average from all the methods (Supplementary Tables S2 and S3).15 Relative frequencies of participants who were considered compliant with treatment instructions in the matched weekly injectable dulaglutide and daily oral semaglutide groups were calculated. The odds ratio (OR) with 95% confidence intervals (CIs) and the respective p-values were derived from the model.
To identify key drivers of participant-reported compliance (binary outcome), bivariate analysis was performed. The relationships between compliance and quantitative variables were measured using Student’s t-test for variables with normal distribution and homogeneous variances and Mann–Whitney U test when the above criteria were not met. The Chi-square test or Fisher’s exact test were used for the quantitative variables. Fisher’s exact test was used when any of the frequencies compared was lower than 5%.
A logistic regression analysis was performed using the stepwise method to assess predictors of compliance. The stepwise methodology used for regression estimation involves a step-by-step iterative construction of a regression model involving the selection of independent variables to be used in a final model. This is done by successively adding or removing possible explanatory variables and testing for statistical significance after each iteration. This iterative process enables the elimination of non-significant variables, thus ensuring that the regression model does not produce results that are not statistically significant. In order to control for confounding variables, a bivariate analysis was performed prior to the regression. The statistically significant variables in one or both groups were then used in the logistic regression. The relationship between compliance and quantitative variables was assessed using the Student’s t-test for variables with normal distribution and homogeneous variances and the Mann–Whitney U test when the above criteria were unmet. For quantitative variables, the Chi-square test or Fisher’s exact test was used, with Fisher’s exact test being used when any of the frequencies compared was less than 5%.
Analyses were conducted using the software STATA v.14 on data from valid participants (defined as those who met the selection criteria and answered all the questions in the questionnaire).
Results
A total of 230 participants were included in the study, 95 receiving weekly injectable dulaglutide and 135 receiving daily oral semaglutide at time of inclusion.
Demographic and Clinical Characteristics
Demographic and clinical characteristics are included in Table 2. Mean (SD) age of the participants was 59.9 (11.5) years and 58.3% were male. The mean HbA1c at GLP-1 RA initiation was 8.1% (1.7), and this occurred 10.6 (8.3) years after diagnosis. At the time of inclusion, mean HbA1c (based on the latest recorded value) was 7.0% (1.1) and mean BMI was 34.5 (5.5) kg/m2. People receiving daily oral semaglutide had a higher BMI than those on weekly injectable dulaglutide. Additionally, the percentages of people presenting with obesity class II and III were also higher in the daily oral semaglutide group than in the weekly injectable dulaglutide group (Table 2). Both groups showed a high comorbidity burden, with 94.3% presenting with at least one comorbidity and mean (SD) number of comorbidities per patient being 3.3 (1.6). Most frequent comorbidities were hypertension and dyslipidemia. People in the weekly injectable dulaglutide group had a slightly higher comorbidity burden than those in the daily oral semaglutide group (Table 2).
 |
Table 2 Patient Demographic and Clinical Characteristics |
Treatment-Related Characteristics
Treatment-related characteristics are included in Table 3. Overall, people had a median time on treatment with weekly injectable dulaglutide or daily oral semaglutide of 189 days at time of inclusion. Weekly injectable dulaglutide participants had been on treatment longer than the daily oral semaglutide group (Table 3). Most participants (91.6%) were receiving the highest dose of weekly injectable dulaglutide commercialized in Spain (1.5 mg). For those taking daily oral semaglutide, the majority were taking the 7 and 14 mg doses (Figure 1). In the weekly injectable dulaglutide group, 87.4% of people were naïve to GLP-1 RAs, while only 60.0% of people using daily oral semaglutide had not been previously treated with GLP-1 RAs. Those who had been previously treated with a GLP-1 RA in the weekly injectable dulaglutide group had received liraglutide or subcutaneous semaglutide, while those who had been previously treated with a GLP-1 RA in the daily oral semaglutide group had received mainly subcutaneous semaglutide (Table 3). Up to 94.3% of all participants were receiving concomitant antidiabetic treatments and 95.2% treatments for other diseases. The most common concomitant antidiabetic treatments were biguanides, sodium-glucose cotransporter 2 inhibitors, and insulin (Table 3).
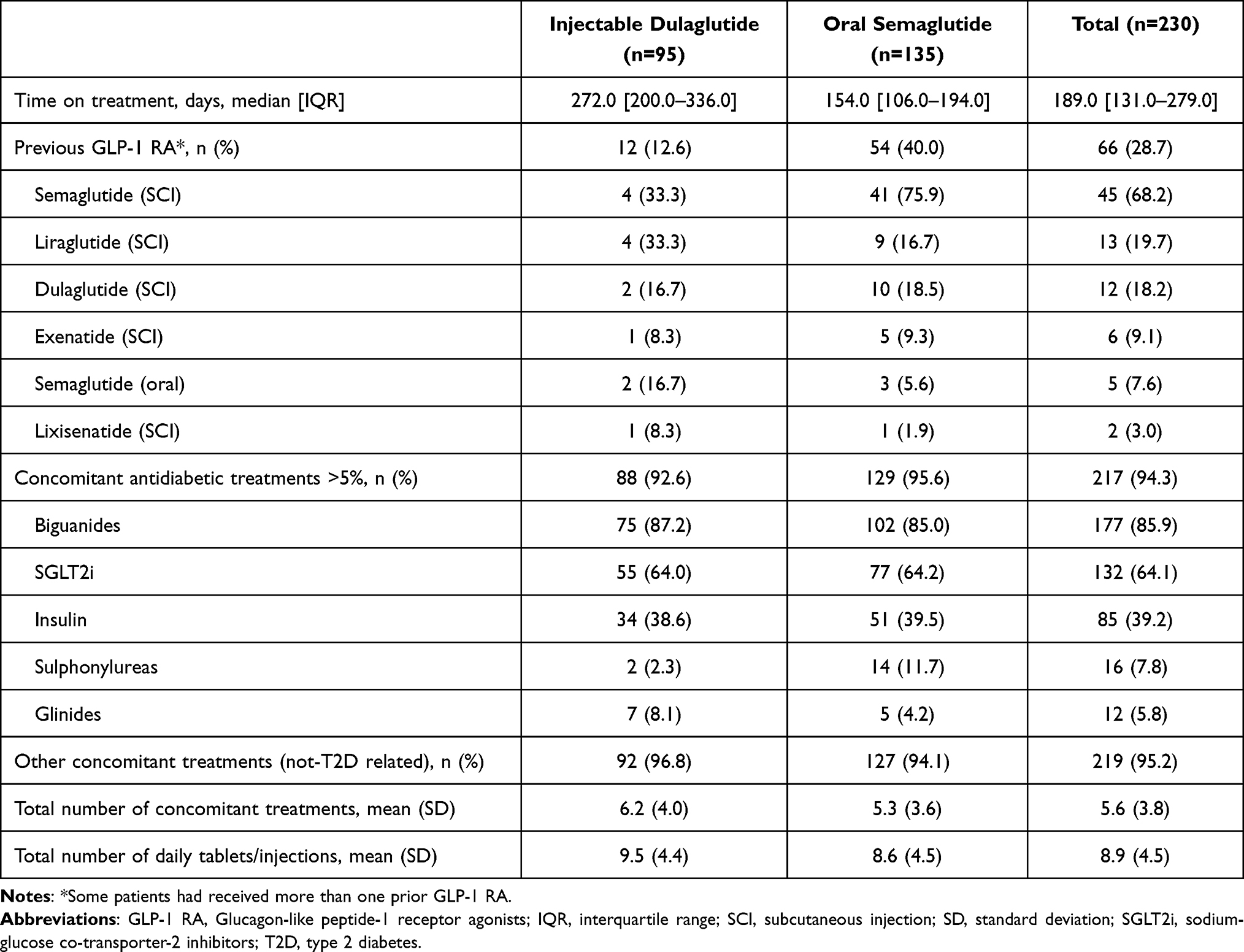 |
Table 3 Treatment-Related Characteristics |
 |
Figure 1 Current GLP-1 RA treatment. Percentage of participants taking the two doses of injectable dulaglutide (0.75 or 1.5 mg; higher doses of dulaglutide are not commercialized in Spain), or three doses of oral semaglutide (3, 7, and 14 mg). Weekly injectable dulaglutide, N=95; daily oral semaglutide, N=135. |
Compliance with Treatment Administration Instructions
General compliance was observed in 96.8% of participants taking weekly injectable dulaglutide and 90.4% of participants taking daily oral semaglutide, who reported being compliant with all instructions “very often” or “often” in their answers to item 1 of the questionnaire (Figure 2). Only 1.1% of participants in the weekly injectable dulaglutide group reported “rarely” or “never” following all instructions, versus 8.1% in the daily oral semaglutide group.
 |
Figure 2 Results indicating the proportion of participants taking weekly injectable dulaglutide or daily oral semaglutide who follow treatment administration instructions Table 2. |
General compliance was also calculated after adjusting for potential between-group imbalances at baseline. The FMA analysis revealed 3.2 times higher odds for general compliance in participants in the weekly injectable dulaglutide group versus the daily oral semaglutide group (OR = 3.2; 95% CI 1.4–21.3), which was statistically significant.
An additional ad-hoc analysis was conducted only for general compliance considering only the participants that “always” followed all the instructions. For these, the comparative adjusted analysis showed a higher general compliance for the weekly injectable dulaglutide group versus the daily oral semaglutide group (OR = 4.1; 95% CI 2.3–7.7), which was statistically significant.
Calculated compliance revealed that 96.8% of the people taking weekly injectable dulaglutide were compliant, versus 85.9% of the people taking daily oral semaglutide. Only 1% of participants in the weekly injectable dulaglutide group reported never following all the steps, 1% rarely injected the drug once per week, and 1% never followed the instructions of the pen (Figure 2). The instructions which participants had the most difficulty following for those taking daily oral semaglutide were following all steps (Question 1), the use of water (Question 5), and the need to have an empty stomach (Question 3) [Figure 2].
Key Drivers of General Compliance
In the bivariate analysis aiming to identify clinical or sociodemographic variables as key drivers of general compliance, no statistically significant association was found between sex and compliance (p>0.05). While participants who were non-compliant with weekly injectable dulaglutide treatment were older than the compliant participants (p=0.031), no relationship between compliance and age was observed in people receiving daily oral semaglutide. Non-compliant participants had more comorbidities than the compliant participants in the total study population (p=0.019), and in the daily oral semaglutide group (p=0.015), but no association was found for participants in the weekly injectable dulaglutide group or with any of the remaining clinical characteristics.
Regarding treatment-related characteristics, the bivariate analysis found a statistically significant difference in general compliance between participants currently treated with daily oral semaglutide versus those receiving weekly injectable dulaglutide (p=0.047), with the former participants being less compliant. No statistically significant association was found with the other analysed treatment-related characteristics (mean time between diagnosis and current GLP-1 RA prescription, mean time on current GLP-1 RA or mean number of tablets or daily injections for concomitant treatments). General compliance of subjects treated with weekly injectable dulaglutide was slightly negatively affected by concomitant treatment with insulin (not significant, p=0.055).
Variables significant in the bivariate analysis (current GLP-1 RA treatment [weekly injectable dulaglutide or daily oral semaglutide], age, and number of comorbidities) were not key drivers of compliance in the multivariable logistic regression analysis (p>0.05).
Discussion
This study compared patient-reported compliance with treatment administration instructions in the package leaflet between two GLP-1 RA treatments for T2D in the real world: weekly injectable dulaglutide and daily oral semaglutide. Overall, the results showed a statistically significant better compliance of participants in the weekly injectable dulaglutide group versus the daily oral semaglutide group. After adjusting for baseline variables, the OR for general compliance in participants receiving weekly injectable dulaglutide, compared to those treated with daily oral semaglutide, was 3.2 (95% CI 1.4–21.3), meaning that participants taking weekly injectable dulaglutide had 3.2 times higher odds of following treatment administration instructions than patients taking daily oral semaglutide.
Overall, participants in this study had similar demographic and clinical characteristics to those seen in other studies of the use of GLP-1 RAs in Spain.16,17 For example, in a real-world study of 1402 people with T2D taking GLP-1 RAs in Spain the mean age and mean BMI were 62.0 years and 35.5 kg/m2, comparable to 59.9 years and 34.5 kg/m2, respectively, in the present study. Although in this study the groups treated with weekly injectable dulaglutide and daily oral semaglutide were generally similar, most participants (87.4%) in the injectable dulaglutide group were naïve to GLP-1 RA treatment, while a large proportion (40.0%) of those in the oral semaglutide group had previously received subcutaneous semaglutide.
Differences in the profile and administration methods of GLP-1 RAs may play an essential role in treatment adherence, persistence, and eventually effectiveness in usual clinical practice of these drugs. One of the causes for non-compliance with the treatment may be poor understanding of medical explanations related to treatment administration. Hence, a possible strategy to increase compliance is simplifying the prescription regimen.18 The REVISE study of patients’ preferences for the product-specific administration of two GLP-1 RAs showed that route, frequency of injection, and complexity of treatment are key factors in patient preferences for treatment.9 This study showed that preferences can switch when participants have clear descriptions of how drugs are administered. Also, another study showed that a large proportion of patients prefer weekly versus daily injection,19 therefore once-weekly administration of injectable dulaglutide may improve compliance compared to more frequently administered regimens.7
The study showed that 94.3% of participants were taking concomitant antidiabetic treatments and 95.2% were taking non-T2D-related concomitant treatments. Further, the number of daily tablets and/or injections was 8.9 (SD=4.5). This level of polypharmacy is in line with results from other observational studies.4 A recent report showed that, paradoxically, more complex regimens are associated with worse HbA1c levels.20,21 In this study, 94.1% of participants taking daily oral semaglutide had comorbidities, with the number of comorbidities being higher in the non-compliant participants than in the compliant participants in the population (p=0.015). A high burden of comorbid conditions associated with polypharmacy has been shown to be perceived as a barrier for treatment compliance in people with T2D,4,22,23 and this effect has also been observed with oral antidiabetic medication.2,24 However, although 76.3% of daily oral semaglutide participants were taking “5 or more” different medications per day (criterion for polypharmacy), no statistically significant differences were found between compliance and the number of daily pills/injections taken. Therefore, other factors could be influencing the worse compliance in individuals with multiple comorbidities. Weekly injectable dulaglutide participants also showed a high burden of comorbidities (94.7%) and polypharmacy (82.1%) but no statistically significant effect on compliance was found.
When analyzing instructions independently, 96.8% and 90.4% of participants with weekly injectable dulaglutide and daily oral semaglutide, respectively, reported “always” or “very often” following each of the package leaflet instructions. However, compliance with package leaflet instructions was lower for those instructions that presented higher difficulties. The use of water, the need to have an empty stomach, and the time necessary to wait before eating after taking medication were the instructions that had the highest number of participants selecting rarely/never in terms of compliance with package leaflet instructions within the oral semaglutide group. In the dulaglutide group, only 1.1% of participants indicated rarely/never following pen instructions. This could be due to the simplicity of the semi-automatic administration device and the fact that the person does not see the needle, requiring minimal manipulation. Generally, for people with T2D with comorbidities and multiple medications, less complex treatments allow easier administration schedules, facilitating following recommendations and adherence with the treatment.25 Therefore, the differences in compliance between treatments observed in the present study could be due to the less complex treatment schedule for injectable dulaglutide, which is administered weekly, compared with the treatment schedule for oral semaglutide, which is administered daily on an empty stomach, and requires a wait of at least 30 minutes before eating, drinking, or taking other oral medications, which might be less adaptable to participants’ daily routines.
A recent study showed that socioeconomic factors can impact on the initiation of a new medication and adherence with treatment in T2D, and that these factors should be taken into account during treatment.26 In this study, the educational level of the participants was well balanced between the groups. However, the bivariate analysis showed that age negatively influenced compliance in participants taking weekly injectable dulaglutide, and a higher number of comorbidities negatively influenced compliance of participants receiving daily oral semaglutide. Although the differences were small, both age and comorbidities have been previously shown to influence adherence to treatment.18,27
The long-term consequences of better adherence can be significant. Better adherence and persistence in people with T2D have been reported in association with lower rates of microvascular and/or macrovascular outcomes and inpatient hospitalization and lower or budget-neutral total healthcare expenditure.28 Lack of adherence can increase healthcare costs, and in the long term, cost savings from better adherence could be substantial.29 Studies such as this one, that provide information on the differences in compliance with administration instructions between medications, can provide valuable insights to inform new patient education strategies and enhance medication adherence, as well as to provide physicians with information on patient preferences to optimize prescribing practices, with the goal of ultimately leading to better clinical outcomes and quality of life.
This study has several limitations that must be considered. As in any retrospective analysis, there could be inconsistencies in the clinical variables collected due to errors in the medical records. This cross-sectional study included a persistent population and, although affecting both treatment groups, this may have had an impact on the generalizability of the results. To minimize this potential bias, a wide entry window of 3–12 months on treatment was allowed. In addition, the projected sample size could not be reached due to operational and feasibility challenges, and a higher number of participants were included in the daily oral semaglutide group than in the weekly injectable dulaglutide group, which may have caused more variability in terms of compliance; however, the final sample size gave strong statistical significance. In this study, in both treatment groups most patients were compliant. Therefore, differences in compliance or factors that influence it may have been obscured by the difference in group size. Moreover, although patients knew that the investigators did not have access to their answers in the e-questionnaire, they may have been afraid of being judged for not following all the instructions, and so may have given answers suggesting they were more compliant than they really were, which is a limitation inherent to studies using self-reported data.30 As a result, the recorded compliance rates may be higher than the actual values, and the wide confidence interval in the statistically significant difference in compliance between groups should be noted. Furthermore, the questionnaire used in the study has not been validated; however, there was no existing validated questionnaire fit for addressing the research objectives and thus it was newly developed using the same language as in the package leaflet for each drug; for this reason, we believe that it could be fully understood by patients and do not consider the lack of validation to be a significant issue. Also, GLP-1 RA shortages may have had an impact on the characteristics of the included population, as changes in treatment with GLP-1 RAs in non-naïve patients can be associated with shortages rather than treatment failure. Finally, the study was conducted in centres across different autonomous communities and healthcare levels, representing diversity within Spain. However, the findings may not be fully generalizable to other countries with different healthcare models.
Conclusion
In summary, the TRU-Experience study has shown that there were differences in patient-reported compliance with treatment administration instructions in the package leaflet depending on whether the patient receives weekly injectable dulaglutide or daily oral semaglutide. The weekly injectable dulaglutide treatment regimen resulted in statistically better compliance with the drug administration instructions, suggesting that the simpler the treatment instructions, the better the compliance. In addition, these data demonstrate that, overall, there is still room for improvement in patient education on the importance of following administration instructions. For healthcare providers, discussing preferences for medication management with people with T2D is important to ensure the correct choices are made. Considering that non-compliance with the treatment instructions may affect adherence to treatment, effectiveness, and safety, it is important to take the treatment complexity into consideration when prescribing these agents. This type of real-world compliance data can inform strategies to improve patient education and adherence, and physician prescribing practices, ultimately leading to better clinical outcomes and quality of life.
Ethics Approval and Informed Consent
All participants in the study provided signed informed consent and the study was approved by the Ethics Committee for Drugs Research of the Hospital Universitario Fundación Alcorcón (Reg. 22/55). This study was conducted in accordance with the protocol and ethical principles that have their origin in the Declaration of Helsinki and that are consistent with applicable Good Pharmacoepidemiology Practices and applicable laws and regulations of Spain.
Acknowledgments
Francisco Pérez and Elena Viciano (Outcomes10) provided operational and statistical analysis support with this study.
Francisco López de Saro and Sheridan Henness (Rx Communications, Mold, UK) provided medical writing assistance with the preparation of this manuscript, funded by Eli Lilly and Company.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Eli Lilly and Company.
Disclosure
Silvia Díaz-Cerezo, Esther Artime, Jennifer Redondo-Antón, Natalia Duque, and Miriam Rubio-de Santos are employees and minor shareholders of Eli Lilly and Company. Erik Spaepen is a paid consultant for Eli Lilly and Company. Gabriel Olveira reports occasional payment for lectures and attendance at conferences from LILLY, during the conduct of the study. Lluís Masmiquel reports personal fees from Lilly, during the conduct of the study; personal fees from Lilly, outside the submitted work. Authors and/or their institutions have received fees for their participation in the study from Eli Lilly and Company.
References
1. Davies MJ, Aroda VR, Collins BS, et al. Management of hyperglycemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;45(11):2753–2786. doi:10.2337/dci22-0034
2. Piragine E, Petri D, Martelli A, Calderone V, Lucenteforte E. Adherence to oral antidiabetic drugs in patients with type 2 diabetes: systematic review and meta-analysis. J Clin Med. 2023;12(5):1981. doi:10.3390/jcm12051981
3. Hamersky CM, Fridman M, Gamble CL, Iyer NN. Injectable antihyperglycemics: a systematic review and critical analysis of the literature on adherence, persistence, and health outcomes. Diabetes Ther. 2019;10(3):865–890. doi:10.1007/s13300-019-0617-3
4. Boye KS, Mody R, Lage MJ, Douglas S, Patel H. Chronic medication burden and complexity for US patients with type 2 diabetes treated with glucose-lowering agents. Diabetes Ther. 2020;11(7):1513–1525. doi:10.1007/s13300-020-00838-6
5. Sims TJ, Boye KS, Robinson S, Kennedy-Martin T. Treatment-related attributes of diabetes therapies and how people with type 2 diabetes report their impact on indicators of medication-taking behaviors. Patient Prefer Adherence. 2022;16:1919–1939. doi:10.2147/PPA.S367046
6. European Medicines Agency. Trulicity, summary of product characteristics. Available from: https://www.ema.europa.eu/en/documents/product-information/trulicity-epar-product-information_en.pdf.
7. Amblee A. Mode of administration of dulaglutide: implications for treatment adherence. Patient Prefer Adherence. 2016;10:975–982. doi:10.2147/PPA.S82866
8. European Medicines Agency. Rybelsus Summary of Product Characteristics. Available from: https://www.ema.europa.eu/en/documents/product-information/rybelsus-epar-product-information_en.pdf.
9. Boye K, Ross M, Mody R, Konig M, Gelhorn H. Patients’ preferences for once‐daily oral versus once‐weekly injectable diabetes medications: the revise study. Diabetes Obes Metab. 2021;23(2):508–519. doi:10.1111/dom.14244
10. Agencia Española de Medicamentos y Productos Sanitarios. Prospecto: información para el paciente (Rybelsus). Available from: https://cima.aemps.es/cima/dochtml/p/1201430005/P_1201430005.html.
11. Agencia Española de Medicamentos y Productos Sanitarios. Prospecto: información para el paciente (Trulicity). Available from: https://cima.aemps.es/cima/dochtml/p/114956002/P_114956002.html.
12. Mody R, Yu M, Nepal B, Konig M, Grabner M. Adherence and persistence among patients with type 2 diabetes initiating dulaglutide compared with semaglutide and exenatide BCise: 6-month follow-up from US real-world data. Diabetes Obes Metab. 2021;23(1):106–115. doi:10.1111/dom.14195
13. Scott IA. Non-inferiority trials: determining whether alternative treatments are good enough. Med J Aust. 2009;190(6):326–330. doi:10.5694/j.1326-5377.2009.tb02425.x
14. Chung S, Shao J, Wang H. Sample size calculations in clinical research. In: Ed: Chapman and Hall/CRC Biostatistic Series.
15. Zagar A, Kadziola Z, Lipkovich I, Madigan D, Faries D. Advancing comparative effectiveness estimation through model averaging [presentation]. In:
16. Norrbacka K, Sicras-Mainar A, Lebrec J, et al. Glucagon-like peptide 1 receptor agonists in type 2 diabetes mellitus: data from a real-world study in Spain. Diabetes Ther. 2021;12(5):1535–1551. doi:10.1007/s13300-021-01039-5
17. Romera I, Rubio-de Santos M, Artola S, Suárez Fernández C, Conget I. GLP-1 RAs in Spain: a short narrative review of their use in real clinical practice. Adv Ther. doi:10.1007/s12325-023-02442-z
18. Dilla T, Valladares A, Lizán L, Sacristán JA. Treatment adherence and persistence: causes, consequences and improvement strategies. Aten Primaria. 2009;41(6):342–348. doi:10.1016/j.aprim.2008.09.031
19. Hauber AB, Nguyen H, Posner J, Kalsekar I, Ruggles J. A discrete-choice experiment to quantify patient preferences for frequency of glucagon-like peptide-1 receptor agonist injections in the treatment of type 2 diabetes. Curr Med Res Opin. 2016;32(2):251–262. doi:10.1185/03007995.2015.1117433
20. Yeh A, Shah-Manek B, Lor KB. Medication regimen complexity and A1C goal attainment in underserved adults with type 2 diabetes. Ann Pharmacother. 2017;51(2):111–117. doi:10.1177/1060028016673652
21. Russell AM, Opsasnick L, Yoon E, Bailey SC, O’Brien M, Wolf MS. Association between medication regimen complexity and glycemic control among patients with type 2 diabetes. J Am Pharm Assoc. 2023;63(3):769–777. doi:10.1016/j.japh.2022.12.028
22. Dehdari L, Dehdari T. The determinants of anti-diabetic medication adherence based on the experiences of patients with type 2 diabetes. Arch Public Health. 2019;77:21. doi:10.1186/s13690-019-0347-z
23. Ayele AA, Tegegn HG, Ayele TA, Ayalew MB. Medication regimen complexity and its impact on medication adherence and glycemic control among patients with type 2 diabetes mellitus in an Ethiopian general hospital. BMJ Open Diab Res Care. 2019;7(1):e000685. doi:10.1136/bmjdrc-2019-000685
24. Nichols GA, Raebel MA, Dyer W, Schmittdiel JA. The effect of age and comorbidities on the association between the medicare STAR oral antihyperglycemic adherence metric and glycemic control. J Manag Care Spec Pharm. 2018;24(9):856–861. doi:10.18553/jmcp.2018.24.9.856
25. Pantuzza LL, Das GB CM, Silveira MR, Junqueira LMR, Reis AMM. Association between medication regimen complexity and pharmacotherapy adherence: a systematic review. Eur J Clin Pharmacol. 2017;73(11):1475–1489. doi:10.1007/s00228-017-2315-2
26. Ekenberg M, Qvarnström M, Sundström A, Martinell M, Wettermark B. Socioeconomic factors associated with poor medication adherence in patients with type 2 diabetes. Eur J Clin Pharmacol. 2024;80(1):53–63. doi:10.1007/s00228-023-03571-8
27. García-Pérez LE, Alvarez M, Dilla T, Gil-Guillén V, Orozco-Beltrán D. Adherence to therapies in patients with type 2 diabetes. Diabetes Ther. 2013;4(2):175–194. doi:10.1007/s13300-013-0034-y
28. Evans M, Engberg S, Faurby M, Jddr F, Hudson P, Polonsky W. Adherence to and persistence with antidiabetic medications and associations with clinical and economic outcomes in people with type 2 diabetes mellitus: a systematic literature review. Diabetes Obes Metab. 2022;24(3):377–390. doi:10.1111/dom.14603
29. Kennedy-Martin T, Boye KS, Peng X. Cost of medication adherence and persistence in type 2 diabetes mellitus: a literature review. Patient Prefer Adherence. 2017;11:1103–1117. doi:10.2147/PPA.S136639
30. Rosenman R, Tennekoon V, Hill LG. Measuring bias in self-reported data. Int J Behav Healthc Res. 2011;2(4):320–332. doi:10.1504/IJBHR.2011.043414
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.