")
Back to Journals » Clinical Ophthalmology » Volume 18
Higher-Order Aberrations Following Ray Trace LASIK and the Impact of Eye Movement on Coma
Authors Thananjeyan AL, Bala C
Received 22 September 2024
Accepted for publication 11 November 2024
Published 22 November 2024 Volume 2024:18 Pages 3389—3398
DOI https://doi.org/10.2147/OPTH.S497131
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Akshaya L Thananjeyan, Chandra Bala
PersonalEyes, Sydney, NSW, Australia
Correspondence: Chandra Bala, Personal-Eyes, 2/33 York St, Sydney, NSW, 2000, Australia, Tel +61 88337111, Email [email protected]
Purpose: To assess ocular higher-order aberrations (HOAs) following ray trace guided laser in situ keratomileusis (LASIK).
Methods: Retrospective review at a single-site ophthalmology practice. Two hundred and fifty eyes of 250 patients with myopia and astigmatism undergoing ray trace LASIK were randomly reviewed (Wavelight Plus, Alcon). The InnovEyes Sightmap (Alcon) diagnostic device was used for whole-eye wavefront aberrometry, tomography, and biometry assessment preoperatively and 3 months post-operatively. Ocular HOA, ablation decentration, intraoperative pupil size, and pupil tracking were assessed. Intraoperative eye tracking of x and y coordinates were separately averaged to calculate mean and standard deviation of movement along the x-axis and y-axis to assess eye movement.
Results: Total HOA RMS (n = 250 eyes) increased marginally from 0.306 ± 0.102 to 0.371 ± 0.135 (p < 0.001) post-operatively. Spherical aberration decreased (0.092 ± 0.112 to 0.056 ± 0.125, p < 0.001). There was no significant difference in preoperative to postoperative vertical coma under − 3D SEQ and horizontal coma under 2D SEQ. In eyes with 4D or more myopia treatment, post-operative vertical and horizontal coma was moderately correlated with the product of ablation depth and vertical and horizontal decentration (R2 0.51, p < 0.001, R2=0.34, p < 0.001, respectively). Multivariate analysis further showed this was correlated to eye movement.
Conclusion: Ray trace LASIK results in a minimal increase in total ocular HOA which is statistically but not clinically significant. Spherical aberration decreases. In larger treatments, there is an increase in coma which correlates with vertical and horizontal decentration of ablation, likely due to eye movement during surgery.
Keywords: laser in situ keratomileusis, ray trace, higher-order aberration, eye movement, decentration, coma
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Ning has been published for this article.
Introduction
Ocular higher-order aberrations (HOAs) are known to be induced following refractive surgery and when combined with existing preoperative HOAs, they can lead to a reduction in contrast sensitivity and visual symptoms including diplopia, glare, and starburst can occur. In the early stages of development, laser refractive surgery induced approximately 0.3 µm of spherical aberration per dioptre (D) treated. Laser ablation was associated with a 1.9-fold increase in total HOA at a 6.5 mm pupil, with the greatest source of increase being a 4-fold increase in spherical aberration.1 Laser technology has evolved to minimize the induced HOA in the form of wavefront optimised treatments, asphericity control, and wavefront guided treatments. However, despite best efforts, the HOA have nearly doubled from 0.38 to 0.6 root mean square (RMS) at a 6 mm pupil.2–22 These techniques treat the eye as a single refractive element from which removal of a ‘thin lens’ leads to a refractive correction. These techniques, reliant on paraxial optics, do not account for the light path being affected by the internal architecture of the eye.
Ray trace guided laser in situ keratomileusis (LASIK) creates a personalized optical eye model (“eyevatar”) using ocular wavefront measurements, corneal tomography, pachymetry, and axial length. The eyevatar is iteratively virtually treated to determine the treatment with the best outcome, and the most appropriate treatment is then applied to the patient’s actual eye. It has been shown to be safe and effective in the correction of myopia and myopic astigmatism.23–26 A marginal increase in total HOA has been reported post-operatively, suggesting a potential benefit of this technique in limiting post-operative HOA.24 No detailed study has assessed the impact of ray-trace based LASIK on ocular HOA and its components in a large cohort. The present study assesses changes in HOA components at 3 months post-operatively at a 6 mm pupil zone. The visual outcomes ie sphere and cylinder of a majority of patients in this cohort have been previously presented.23
Methods
Patients
A retrospective review of sequential eyes with myopia and myopic astigmatism in adult patients undergoing ray trace LASIK over a 20-month interval was conducted. One eye was randomly selected for the study. Inclusion criteria included the following: i) myopic eyes in adults 18 years and older who underwent ray-trace-based LASIK surgery ii) no co-existing ocular conditions and no previous ocular surgery. The postoperative predicted residual stromal thickness had to be 300 microns or greater and greater than or equal to 60% of preoperative total central pachymetry. Patients with ectasia, dry eyes, cataracts, uveitis, and retinal pathology were excluded. Patients were excluded if they had had a previous refractive procedure or cataract surgery. Patients were advised not to wear rigid or toric contact lenses for ≥2 weeks or soft contact lenses for 1 week prior to preoperative screening and surgery. Patients were excluded if they did not have a stable refraction for 12 months preoperatively.
Ethics approval for this study was granted by an external ethics committee (Bellberry Limited), and consent to use de-identified data was obtained from patients after they were fully informed about the study’s purpose. This study followed the tenets of the Declaration of Helsinki and was conducted in accordance with the CPMP/ICH Note of Guidance on Good Clinical Practice and the National Statement on Ethical Conduct in Human Research.
Surgical Procedures and Protocol
Surgical protocol and preoperative procedures have been previously described.23 Patients underwent dilated fundus examination, subjective refraction, and cyclopentolate 1% based cycloplegic refraction. Biometry (partial coherence interferometry), tomography (Scheimpflug principle), wavefront refraction, and whole-eye aberrometry (Hartmann-Shack) data were collected preoperatively and 3 months post-operatively using a single device, the InnovEyes Sitemap (Alcon Laboratories, Inc.). Ocular HOA measurements were measured under scotopic conditions with 3 lux of illumination measured at the patient’s temple using a light meter. Preoperatively, data from the InnovEyes Sitemap was exported to the WaveNet Server (Alcon Laboratories, Inc.) and customized ablation profile was applied to each eye using an excimer laser (EX500, Alcon Laboratories, Inc.).
Hundred and ten micron bilateral sequential LASIK flaps were created using the Wavelight FS200 (Alcon Laboratories, Inc.) with a 9.2 mm diameter. The Wavelight EX500 (Alcon Laboratories, Inc.) was used for excimer treatment with a treatment zone of 6.5 mm. A single surgeon (C.B.) performed all surgeries and inspected the wavefront HOA during treatment planning. Outliers that appeared subjectively different from the average on the screen were removed. The patients’ eyes were tracked every 20 ms by a built-in infrared pupil tracker. Postoperatively, patients were reviewed at day 1, week 1, month 1, and month 3.
Outcome Measurements
Wavefront measurements were recorded 3 months postoperatively, according to the convention of the American National Standards Institute (2022) at a 6 mm pupil. A scan was considered acceptable if more than 80% of the points were acquired and there were no disturbances such as dry patches or vitreous floaters seen on the wavefront image. If there was dryness, then only saline and no other ocular lubricants were used. Readings with inappropriate pupil diameter or ellipticity, outlier values, poor tear film quality, and/or eye movement were eliminated, and HOA data from the best 3 readings (preoperatively and post-operatively) were averaged for each eye. Preoperative and post-operative mean HOAs including 3rd order (Z3−3, Z3−1, Z31, Z33), 4th order (Z4−4, Z4−2, Z4°, Z42, Z44), 5th order (Z5−5, Z5−3, Z5−1, Z51, Z53, Z55), 6th order aberrations (Z6−6, Z6−4, Z6−2, Z6°, Z62, Z64, Z66) and total HOA RMS values at a 6mm optical zone were analysed.
A subset of patients who had more than 4D spherical equivalent (SEQ) of treatment were assessed for decentration and its impact on coma. Pachymetry changes of eyes with lower SEQ power were too difficult to be detected reliably on pachymetry maps. In eyes with more than 4D SEQ, 3-month postoperative corneal tomography measurements (tangential and pachymetry maps) were compared with preoperative maps. Pachymetry difference maps between 3 months post-operative to preoperative were generated and the point of maximal depth change was determined. The treatment was aligned with respect to the corneal vertex. The distance from the pachymetry apex to the point of thinnest pachymetry was measured (x and y coordinates) as marker of decentration. The same observer (A.T.) performed all measurements.
Intraoperatively, the eye tracking system follows the pupil center of the eye and an x and y coordinate of its location and pupil diameter is output every 20 milliseconds. To assess eye movement for each eye, all intraoperative eye tracking x and y coordinates were separately averaged to calculate mean and standard deviation of movement along the x-axis and y-axis for each eye. The treatment centration is adjusted based on pupil center tracking. The pupil size variation (mean and standard deviation) and difference from the baseline registration pupil size were also determined throughout the treatment.
Statistical Analysis
Statistical analysis was done on Microsoft Excel (Microsoft Office Excel; Microsoft, Redmond, WA). A paired Student’s t-test was applied when comparing preoperative and post-operative data. Multiple regression analysis was based on ANOVA. A sample size calculation was undertaken. To detect an increase in the total ocular HOA of 0.015 RMS (type II error 0.05, ß 0.2, standard deviation of 0.15, within subject correlation on 0.875) requires an n = 199.
Results
The 250 randomly selected eyes included in the review included 132 right and 118 left eyes. Preoperative manifest sphere was −2.93 ±1.44D (range −7 to −0.25D) and reduced to 0.09 ±0.33D (range −0.5 to 1D). Astigmatism was −0.81 ±0.76D (range −4.25 to 0D) and reduced to −0.25 ±0.21D (range −1.5 to 0D) postoperatively. The SEQ preoperatively was −3.34 ±1.44D (range −7.62 to −0.5D) improved to −0.01 ± 0.26D (range −0.5 to 0.75D) following treatment.
The preoperative ocular total HOA (o-tHOA) increased from 0.306 ±0.102 RMS to 0.371 ±0.135 (p < 0.001)(Table 1). The greatest increase in o-tHOA appears to arise from an increase in 3rd order aberration. (Figure 1) The mean 3rd order aberration increased by 0.055 RMS from 0.236 ±0.100 to 0.291 ±0.137 (p < 0.001). This increase was greater than the increase seen in other orders (Figure 1).
 |
Table 1 Preoperative and 3 Months Postoperative Higher-Order Aberration |
 |
Figure 1 Mean preoperative and post operative higher order aberrations with standard deviation error bars post ray trace LASIK. |
Measurements of individual aberrations at 6 mm show that spherical aberration (Z4°) significantly decreased from preoperative value of 0.092 ± 0.112 µm to 0.056 ± 0.125 µm (p < 0.001) 3 months postoperatively (Table 1). The absolute value of spherical aberration also decreased from 0.123 ± 0.088 µm preoperatively to 0.109 ± 0.088 µm (p < 0.001). No correlation was observed between postoperative spherical aberration and pre-operative SEQ (correlation coefficient R2=0.006; p = 0.22; Figure 2).
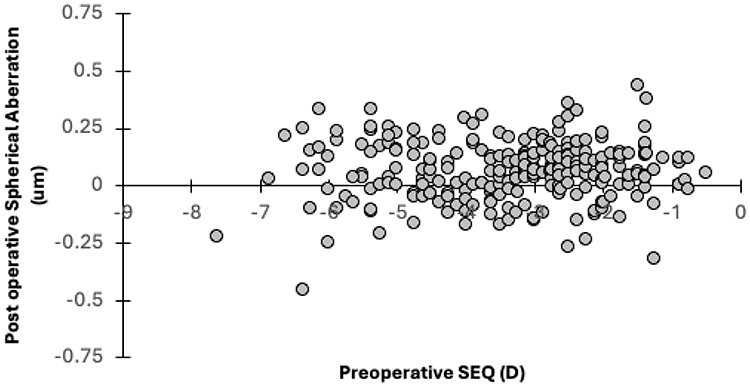 |
Figure 2 Preoperative spherical equivalent (SEQ) vs post operative spherical aberration (Z4°). |
Vertical coma (Z3−1), a component of 3rd order aberrations, increased the most compared to other sources of aberration. Vertical coma increased from −0.041 ± 0.152 µm to −0.098 ± 0.192 µm (p < 0.001) 3 months postoperatively. In comparison, the horizontal coma (Z3 1) did not increase significantly (pre-op −0.007 ± 0.094 µm, post-op −0.031 ± 0.175 µm; p = 0.029). However, both absolute vertical and horizontal coma increased with increase in SEQ treated (Figure 3). In eyes with less than −3D SEQ, there was no significant difference between preoperative and post-operative absolute vertical coma (p > 0.05). In patients with −6 to −5D SEQ, absolute vertical coma increased from 0.125 ± 0.107 µm to 0.280 ± 0.215 µm (p < 0.001). In eyes with greater than −6D SEQ, absolute vertical coma increased from 0.113 ± 0.086 µm to 0.301 ± 0.166 µm (p < 0.001). Similarly, the absolute horizontal coma was not significantly different with low corrections of under −2D SEQ (p > 0.05) but increased with higher corrections. This increase, however, was less than the observed increase in vertical coma. In the eyes with between −6 to −5D SEQ, absolute horizontal coma increased from 0.081 ± 0.054 µm to 0.221 ± 0.123 µm (p < 0.001) and in the eyes with −6D SEQ or more myopia, it increased from 0.077 ± 0.077 µm to 0.168 ± 0.160 µm (p < 0.001).
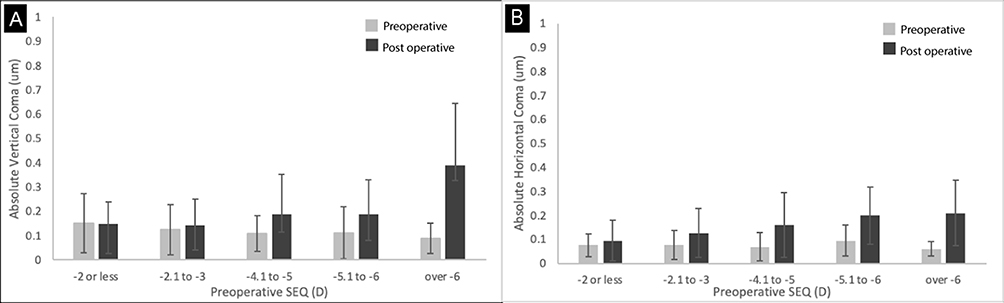 |
Figure 3 Treated spherical equivalent vs post operative coma. (A) Vertical coma (Z3−1) (B) Horizontal Coma (Z31). |
Coma, Decentration, and Intraoperative Eye Movement
Eyes with −4D SEQ or more myopia were assessed to determine the center of ablation with respect to the corneal vertex. The maximum ablation was measured by comparing preoperative and post-operative pachymetry maps. The average ablation depth was 96.1 ± 20.1 µm. The center of ablation was displaced vertically on average by 83 ± 355 µm (range −880 µm to 740 µm) and horizontally by 182 ± 355 µm (range −710 µm to 960 µm) from corneal vertex. Vertical coma (Z3−1) was found to have a moderately positive correlation with the product of the vertical ablation decentration and measured deepest treatment depth (R2 = 0.51, P < 0.001) (Figure 4A). Horizontal coma (Z3−2) was found to have a moderately positive correlation with the product of the horizontal ablation decentration and measured deepest treatment depth (R2 = 0.34, P < 0.001) (Figure 4A).
 |
Figure 4 Intraoperative eye movement during ray trace LASIK and coma in eyes with greater than −4D treated spherical equivalent. (A) Coma vs ablation decentration and treatment depth with least squares line (B) Average intraoperative position and standard deviation of eyes. |
Patients have to maintain fixation during treatment, however, this can be difficult with longer treatments. Figure 4B shows the average position of the eye and standard deviation of eye movement along the horizontal and vertical axis when >-4D SEQ was treated. Most eyes were deviated superiorly, and there was greater variation/standard deviation in eye position along the vertical as compared to horizontal axis.
Multivariate analysis of the product of ablation and decentration showed a significant correlation with eye movement (namely total amount of movement, average movement, standard deviation of movement, and pupil constriction compared to baseline). Both vertical and horizontal movement showed a weak but significant correlation coefficient of 0.19 (p < 0.01) and 0.23 (p < 0.001) respectively. The total amount of horizontal movement (p = 0.01) and the average amount of horizontal movement (p = 0.02) were significantly correlated. There was no correlation with the standard deviation of horizontal movement (p = 0.79) or average amount of pupil movement (p = 0.52). In the vertical direction, only the standard deviation of vertical movement was correlated (p < 0.001). The vertical total movement (p = 0.15), average amount of vertical movement (p = 0.14), and pupil size change (p = 0.27) were not significantly correlated.
Discussion
On review of the literature published in the last 17 years, LASIK causes an increase in o-tHOA.2–22 Baseline o-tHOA at 6mm is on average reported at 0.38 RMS (range 0.23 to 0.55). Postoperatively, it increases to an average value of 0.6 (0.42 to 0.88). There is an average increase of 0.21. The present study had a similar preoperative o-tHOA to previous reports at 0.306 ±0.102. O-tHOA increased at 3 months postoperatively by 0.065 to 0.371 ±0.135 (p < 0.001). This is a statistically significant increase but not clinically significant as it is still below 0.4 at 6 mm. This increase of 0.065 is considerably lower than the average increase of 0.21RMS at 6 mm reported in literature. Ray trace LASIK has been shown to increase o-tHOA by 0.10 in a small cohort and 0.004 in a multicenter trial.24,25 The results of the present study are similar to previously reported results, and the variation in increase may be due to variation in diameter of pupil size used for measurements. To further assess whether the increase in ocular total HoA of 0.065 RMS is clinically significant, studies utilising validated questionnaires will be required to compare these findings with subjective symptoms of glare and halos in patients.
Preoperatively, the most dominant aberration was spherical aberration (0.092 ± 0.112 µm). Spherical aberration decreased following ray trace LASIK. There was a statistically significant decrease in the arithmetic mean (0.092 ± 0.112 µm to 0.056 ± 0.125 µm, p < 0.01) and the absolute mean (0.123 ± 0.088 µm to 0.109 ± 0.088 µm, p < 0.01) value of spherical aberration before and after ray trace LASIK. In comparison, previously published reports show an increase in spherical aberration from 0.08 µm (range −0.16 µm to 0.25 µm) to 0.19 µm (range −0.46 µm to +0.45µm).2–4,7–13,16,19–22,27–29 Previously, the correction/induction of spherical aberration was related to the amount of preoperative myopia treated.1 However, the amount of myopia treated could vary between studies and consequently affect induced spherical aberration. To allow for a better comparison, spherical aberration was assessed as a function of preoperative SEQ treated. There was no significant correlation between the treated myopia and postoperative spherical aberration (R2 = 0.006; p = 0.22). The present study is the first large-scale study reporting a reduction in spherical aberration following ray trace LASIK independent of the degree of preoperative myopia.
The biggest contributor to the increase in o-tHOA following ray trace LASIK is 3rd-order aberration, which increased by 0.055 RMS from 0.236 ± 0.100 to 0.291 ± 0.137 (p < 0.0001). The single largest source of increase was vertical coma. Horizontal coma increased marginally from preoperative values (pre-ray trace LASIK −0.007 ± 0.094 µm, post-ray trace LASIK −0.031 ±0.175 µm, p = 0.029) while vertical coma increased significantly (pre-ray trace LASIK −0.041 ±0.152 µm, post-ray trace LASIK −0.098 ±0.192 µm; p < 0.001). Interestingly, the increase in coma is much less than that of published literature (0.12 µm).28–34
Although the increase in vertical coma was less than that of published literature, it is important to determine its source. Vertical and horizontal coma did not increase significantly following lower power treatments. Vertical coma increased rapidly with longer treatment, while horizontal coma additionally increased by a lesser degree. In the eyes with more than −4D SEQ of treatment, both vertical and horizontal coma correlated with the product of the amount of tissue ablated and decentration. Examining the difference in pachymetry map before and after surgery, a small decentration of treatment from the pachymetry vertex is evident. The average ablation depth was 96.1 ± 20.1 µm (>-4D subgroup). The center of ablation was displaced vertically on average by 83 ± 355 µm (range −880 µm to 740 µm) and horizontally by 182 ± 355 µm (range −710 µm to 960 µm) from corneal vertex. The product of the amount of treatment and its topographical displacement (x-axis and y-axis) are correlated with horizontal (R2 = 0.34, p < 0.001, horizontal coma = −82.3 (displacementxdepth)-12.7) and vertical coma (R2 = 0.51, p < 0.001, vertical coma = −90.6 (displacementxdepth)-13.9). The position of the visual axis horizontally was not accounted for in this assessment, which may explain the lower horizontal coma induced following horizontal decentration as compared to vertical decentration. Figure 4a shows that superior displacement of treatment increases negative coma as seen in keratoconus and an inferior displacement leads to positive coma. The induction of coma is related to the displacement of treatment center as well as the amount of ablation as there is a prismatic induction from small decentration.
Ablation of eyes requiring greater than −4D SEQ treatment was often displaced superiorly and more to the left. The standard deviation of vertical movement for each eye was much higher than horizontal movement in keeping with the Bell’s phenomenon causing a significant amount of eye movement. Multivariate analysis of pupil tracking data at 20 ms interval gives a weak but statistically significant correlation between the product of ablation depth and displacement and vertical or horizontal eye movement (vertical: R2: 0.19, p < 0.01; horizontal: R2: 0.23, p < 0.001, respectively). This highlights the importance of maintaining fixation during prolonged surgery. Eyes tend to deviate during larger treatments (−4D or more myopia) and patient fixation is critical during treatment. This analysis could be improved if the amount of ablation was analysed based on the energy applied to the cornea and correlated with eye movement. Unfortunately, the energy distribution and pulse pattern are not available for analysis. Furthermore, the exact position of the eye at the time of pulse application is not known. The sampling rate of eye position data at 20 ms covers 10 pulses and it does not indicate where the exact treatment was being applied. Therefore, a direct correlation between pulse application and coma could not be determined. It is possible that coma could arise from displacement between the axis of ablation and the line of sight. In the present study, vertical coma behaved differently to horizontal coma. Inferonasal lines of sight should affect horizontal coma as much as vertical coma. This needs to be examined in greater detail in future studies.
It is of interest that the eye movement may have affected vertical coma more than spherical aberration. Vertical coma increased, while spherical aberration stayed the same with higher amounts of spherical equivalent treatment. It is possible that asymmetric aberrations are affected more by eye movement than symmetric aberrations. This would depend on several factors including the pattern of ablation. Further studies would be needed to verify this hypothesis.
A limitation of this study is its retrospective design. Furthermore, the post-operative time frame of this study may not be adequate enough to assess long-term outcomes, stability of results, and long-term complications. Future studies with larger follow-up may guide understanding of long-term changes.
In the past, wavefront guided LASIK was recommended in patients with preoperative o-tHOA of 0.35RMS and above.35 The present study shows that ray trace LASIK may be applied to normal population without a large clinically significant increase in o-tHOA. Furthermore, ray trace LASIK is the only technique reported to reduce spherical aberration and is effective in a large range of eyes. Lastly, there is still room for improvement. While the increase in vertical coma is small and absent in low myopes, in larger treatments, its induction could potentially be limited further by helping patients maintain fixation during ray trace-based LASIK.
Conclusion
Ray trace LASIK leads to statistically but not clinically significant increase in total higher-order aberration and a reduction in spherical aberration. Vertical coma increases slightly and is correlated to vertical micro-decentration which is likely secondary to vertical eye movement during surgery.
Funding
No funding was received.
Disclosure
Bala is a consultant for Alcon and J&J. Eye movement data was provided through a research agreement undertaken with Alcon.
References
1. Moreno-Barriuso E, Lloves J, Marcos S, Navarro R, Llorente L, Barbero S. Ocular aberrations before and after myopic corneal refractive surgery: LASIK-induced changes measured with laser ray tracing. Invest Ophthalmol Visual Sci. 2001;42(6):1396–1403.
2. Wang Y, Zhao K-X, He J-C, Jin Y, Zuo T. Ocular higher-order aberrations features analysis after corneal refractive surgery. Chinese Med J. 2007;120(4):269–273. doi:10.1097/00029330-200702020-00002
3. Villarrubia A, Palacín E, Bains R, Gersol J. Comparison of custom ablation and conventional laser in situ keratomileusis for myopia and myopic astigmatism using the alcon excimer laser. Cornea. 2009;28(9):971–975. doi:10.1097/ICO.0b013e31819ce213
4. Padmanabhan P, Basuthkar SS, Joseph R. Ocular aberrations after wavefront optimized LASIK for myopia. Indian J Ophthalmol. 2010;58(4):307–312. doi:10.4103/0301-4738.64139
5. Yang X, Wang Y, Zhao K, Fang L. Comparison of higher-order aberration and optical quality after Epi-LASIK and LASIK for myopia. Graefe’s Arch Clin Exp Ophthalmol. 2011;249(2):281–288. doi:10.1007/s00417-010-1394-x
6. Wallau AD, Campos M. One-year outcomes of a bilateral randomised prospective clinical trial comparing PRK with mitomycin C and LASIK. Br J Ophthalmol. 2009;93(12):1634–1638. doi:10.1136/bjo.2008.152579
7. Taneri S, Oehler S, MacRae SM. Aspheric wavefront-guided versus wavefront-guided LASIK for myopic astigmatism with the Technolas 217z100 excimer laser. Graefe’s Arch Clin Exp Ophthalmol. 2013;251(2):609–616. doi:10.1007/s00417-012-2143-0
8. Kamiya K, Shimizu K, Igarashi A, Kobashi H, Komatsu M. Comparison of visual acuity, higher-order aberrations and corneal asphericity after refractive lenticule extraction and wavefront-guided laser-assisted in situ keratomileusis for myopia. Br J Ophthalmol. 2013;97(8):968–975. doi:10.1136/bjophthalmol-2012-302047
9. Ryan A, O’Keefe M. Wavefront-guided and aspheric ablation for myopia – one-year results of the zyoptix personalized treatment advanced algorithm. Am J Ophthalmol. 2012;153(6):1169–1177.e1162. doi:10.1016/j.ajo.2011.11.018
10. Wu J, Zhong X, Yang B, Wang Z, Yu K. Combined wavefront-guided laser in situ keratomileusis and aspheric ablation profile with iris registration to correct myopia. J Cataract Refract Surg. 2013;39(7):1059–1065. doi:10.1016/j.jcrs.2013.01.043
11. Hood CT, Krueger RR, Wilson SE. The association between femtosecond laser flap parameters and ocular aberrations after uncomplicated custom myopic LASIK. Graefe’s Arch Clin Exp Ophthalmol. 2013;251(9):2155–2162. doi:10.1007/s00417-013-2328-1
12. He L, Liu A, Manche EE. Wavefront-guided versus wavefront-optimized laser in situ keratomileusis for patients with myopia: a prospective randomized contralateral eye study. Am J Ophthalmol. 2014;157(6):1170–1178.e1171. doi:10.1016/j.ajo.2014.02.037
13. Khan MS, Humayun S, Fawad A, Ishaq M, Arzoo S, Mashhadi F. Effect of wavefront optimized LASIK on higher order aberrations in myopic patients. Pakistan J Med Sci. 2015;31(5):1223–1226. doi:10.12669/pjms.315.7683
14. Gobbe M, Reinstein DZ, Archer TJ. LASIK-induced aberrations: comparing corneal and whole-eye measurements. Optometry and Vision Science: Official Publication of the American Academy of Optometry. 2015;92(4):447–455. doi:10.1097/OPX.0000000000000557
15. Arora R, Goel Y, Goyal JL, Goyal G, Garg A, Jain P. Refractive outcome of wavefront guided laser in situ keratomileusis and wavefront guided photorefractive keratectomy in high pre-existing higher order aberration. Contact Lens & Anterior Eye. 2015;38(2):127–133. doi:10.1016/j.clae.2014.12.001
16. Al-Zeraid FM, Osuagwu UL. Induced higher-order aberrations after laser in situ keratomileusis (LASIK) Performed with wavefront-guided IntraLase femtosecond laser in moderate to high astigmatism. BMC Ophthalmol. 2016;16(1):29. doi:10.1186/s12886-016-0205-5
17. Jahadi Hosseini SH, Abtahi SM, Khalili MR. Comparison of higher order aberrations after wavefront-guided LASIK and PRK: one year follow-up results. J Ophthalmic Vis Res. 2016;11(4):350–357. doi:10.4103/2008-322X.194069
18. Ghoreishi M, Beni ZN, Beni AN, Kianersi F. Effect of iris registration on outcomes of FEMTOLASIK for myopia and myopic astigmatism. Intl Ophthalmol. 2018;38(5):2077–2087. doi:10.1007/s10792-017-0703-3
19. Xia LK, Ma J, Liu HN, Shi C, Huang Q. Three-year results of small incision lenticule extraction and wavefront-guided femtosecond laser-assisted laser in situ keratomileusis for correction of high myopia and myopic astigmatism. Int J Ophthalmol. 2018;11(3):470–477. doi:10.18240/ijo.2018.03.18
20. Zhao PF, Hu YB, Wang Y, Fu CY, Zhang J, Zhai CB. Comparison of correcting myopia and astigmatism with SMILE or FS-LASIK and postoperative higher-order aberrations. Int J Ophthalmol. 2021;14(4):523–528. doi:10.18240/ijo.2021.04.07
21. Humayun S, Tahir A, Ishaq M, Arzoo S. Comparison of higher order aberrations between wavefront optimized photorefractive keratectomy and laser in situ keratomileusis in myopic patients. J College Phys Surg--Pakistan. 2023;33(8):884–889.
22. Gatinel D, Adam PA, Chaabouni S, et al. Comparison of corneal and total ocular aberrations before and after myopic LASIK. J Refractive Surg. 2010;26(5):333–340. doi:10.3928/1081597X-20090617-01
23. He G, Bala C. Ray tracing guided myopic laser in situ keratomileusis - real world clinical outcomes. J Cataract Refract Surg. 2023;49(11):1140–1146. doi:10.1097/j.jcrs.0000000000001286
24. Kanellopoulos AJ. Initial outcomes with customized myopic LASIK, guided by automated ray tracing optimization: a novel technique. Clin Ophthalmol. 2020;14:3955–3963. doi:10.2147/OPTH.S280560
25. Kanellopoulos AJ, Maus M, Bala C, et al. International multicenter, myopic and myopic astigmatism femto LASIK, customized by automated ray-tracing ablation profile calculation: a postmarket study. Clin Ophthalmol. 2024;18:525–536. doi:10.2147/OPTH.S435581
26. Cummings AB, Kelly K. Optical ray tracing-guided myopic laser in situ keratomileusis: 1-year clinical outcomes. Clin Ophthalmol. 2013;7:1181–1191. doi:10.2147/OPTH.S44720
27. Dougherty PJ, Waring G, Chayet A, Fischer J, Fant B, Bains HS. Topographically guided laser in situ keratomileusis for myopia using a customized aspherical treatment zone. J Cataract Refract Surg. 2008;34(11):1862–1871. doi:10.1016/j.jcrs.2008.07.021
28. Zhang J, Zhou YH, Wang NL, Li R. Comparison of visual performance between conventional LASIK and wavefront-guided LASIK with iris-registration. Chin Med J. 2008;121(2):137–142. doi:10.1097/00029330-200801020-00009
29. Goyal JL, Garg A, Arora R, Jain P, Goel Y. Comparative evaluation of higher-order aberrations and corneal asphericity between wavefront-guided and aspheric LASIK for myopia. J Refractive Surg. 2014;30(11):777–784. doi:10.3928/1081597X-20141021-10
30. Kirwan C, O’Keefe M. Comparative study of higher-order aberrations after conventional laser in situ keratomileusis and laser epithelial keratomileusis for myopia using the technolas 217z laser platform. Am J Ophthalmol. 2009;147(1):77–83. doi:10.1016/j.ajo.2008.07.014
31. Cheng ZY, He JC, Zhou XT, Chu RY. Effect of flap thickness on higher order wavefront aberrations induced by LASIK: a bilateral study. J Refractive Surg. 2008;24(5):524–529. doi:10.3928/1081597X-20080501-11
32. El Awady HE, Ghanem AA, Saleh SM. Wavefront-optimized ablation versus topography-guided customized ablation in myopic LASIK: comparative study of higher order aberrations. Ophthalmic Surg Lasers Imag. 2011;42(4):314–320. doi:10.3928/15428877-20110421-01
33. Chen X, Wang Y, Zhang J, Yang SN, Li X, Zhang L. Comparison of ocular higher-order aberrations after SMILE and wavefront-guided femtosecond LASIK for myopia. BMC Ophthalmol. 2017;17(1):42. doi:10.1186/s12886-017-0431-5
34. Anderle R, Ventruba J, Š S. [Comparison of visual acuity and higher-order aberrations after standard and wavefront-guided myopic femtosecond LASIK]. Ceska a slovenska oftalmologie. 2015;71(1):44–50. Czech
35. Stonecipher KG, Kezirian GM. Wavefront-optimized versus wavefront-guided LASIK for myopic astigmatism with the ALLEGRETTO WAVE: three-month results of a prospective FDA trial. J Refractive Surg. 2008;24(4):S424–430.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.