")
Back to Journals » Journal of Pain Research » Volume 17
Hollow Screw Placement Combined with Percutaneous Vertebroplasty Serves as a Valuable Three-Column Intensive Treatment for Patients with Kummell’s Disease and Pedicle Rupture
Authors Liu Y, Su Y , Luan Z, Hou X, Wu G, Xu Y, Wang S, Gao L, Zheng X
Received 26 June 2024
Accepted for publication 21 August 2024
Published 26 August 2024 Volume 2024:17 Pages 2767—2774
DOI https://doi.org/10.2147/JPR.S469755
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Alaa Abd-Elsayed
Yapu Liu, Yuanyuan Su, Zhonghao Luan, Xiuwei Hou, Guangliang Wu, Yonghui Xu, Songmao Wang, Lifeng Gao, Xiaochen Zheng
Department of Spinal Surgery, Second Affiliated Hospital of Luohe Medical College, Luohe, People’s Republic of China
Correspondence: Yapu Liu, Department of Spinal Surgery, Second Affiliated Hospital of Luohe Medical College, 463 Haihe Avenue, Luohe, 462300, People’s Republic of China, Tel/Fax +86-0395-6162312, Email [email protected]
Purpose: To introduce the surgical methods and clinical results of percutaneous vertebroplasty (PVP) combined with hollow screw placement as a treatment for patients with Kummell’s disease and pedicle rupture.
Methods: From January 2020 to January 2023, a total of 10 patients with Kummell’s disease and pedicle rupture confirmed via imaging underwent three-column intensive therapy using hollow screws combined with PVP. There were two males and eight females with an average age 75.7± 6.11 years old. The time of operation, bone cement injection amount, bone cement leakage during operation were recorded. X-ray and CT were reexamined after operation. The improvement in quality of life was assessed using the Oswestry Disability Index (ODI), and the improvement in low back pain was assessed using the visual analogue scale (VAS).
Results: Hollow screw placement combined with PVP was successfully performed in all patients. The average operation time was 39.2± 5.1 min, and the average volume of bone cement injected was 5.85± 0.83mL. No leakage of bone cement into spinal canal occurred.The mean preoperative ODI score was 75.70± 4.39, but this decreased significantly postoperatively(P< 0.05), being 37.70± 6.95 at 1 day and 26.40± 4.90, 23.70± 4.87, 21.70± 5.46, and 20.50± 4.21 at 1, 3, 6, and 12 months after the operation, respectively. The mean VAS pain score before the operation was 8.35± 0.63, but the symptoms of back pain were significantly relieved after operation(P< 0.05). The mean VAS scores 1 day and 1, 3, 6, and 12 months after the operation were 3.45± 0.47, 2.55± 0.60, 1.89± 0.48, 1.50± 0.27, and 1.12± 0.20, respectively.
Conclusion: Hollow screw placement combined with percutaneous vertebroplasty serves as a valuable three-column intensive treatment for patients with Kummell’s disease and pedicle rupture. This procedure has the advantages of minimal trauma, less pain and quick recovery. The strong anchoring of bone cement and hollow screws provides stable and firm healing conditions for vertebral and pedicle fractures.
Keywords: three-column enhancement, PVP, hollow screw, Kummell’s disease, pedicle rupture
Introduction
Kummell’s disease, also known as posttraumatic delayed osteonecrosis of vertebral body, is a delayed vertebral collapse caused by osteonecrosis of vertebral body after minor spinal trauma. It is characterized by intractable back pain and progressive kyphosis, and the common imaging manifestation is vacuum fissure sign (IVC) in vertebral body, with internal gas or liquid; this is most common in the anterior and middle parts of the vertebral body.1–4 Patients with Kummell’s disease usually show severe back pain, which directly leads to a decline in quality of life. Conservative treatment can not achieve a good clinical prognosis; surgical treatment is essential. Common surgical methods include percutaneous vertebroplasty (PVP), percutaneous kyphoplasty (PKP), and pedicle screw internal fixation with bone fusion.1,3,5–10 However, bone cement leakage, loosening or displacement over time, and significant trauma developing during internal fixation surgery affect spinal mobility.3,5,7,10–14 We previously reported treatment of stage I and II Kummell’s disease via bone cement three-column enhanced PVP.13 This was associated with minimal trauma, less pain, and solid cement fixation.
However, in the clinic, we sometimes encounter patients with stage I or II Kummell’s disease and pedicle fractures. If three-column enhanced PVP is directly applied, such patients are at a greater risk of leakage along the broken pedicle into the spinal canal, resulting in spinal cord compression. In this study, 10 cases of Kummell’s disease with pedicle fracture were treated from January 2020 to January 2023 via three-column intensive therapy using hollow screws combined with PVP. Here, we summarize the clinical efficacy of three-column intensive therapy using hollow screws combined with PVP as a treatment for Kummell’s disease with pedicle fracture, and we discuss the specific surgical procedures, precautions and surgical indications.
Methods
General Information
This was a prospective study of 10 elderly patients with radiographically proven Kummell disease with pedicle rupture were treated with three-column reinforcement technique using hollow screw combined with PVP under local anesthesia from January 2020 to January 2023. The mean age of the patients was 75.73 ± 6.11 years (age range 66 ~ 87 years), including 2 males and 8 females. Bone mineral density (BMD) was measured by dual-energy X-ray absorptiometry before surgery, and T-values ranged from −2.5 to −5.5(mean = −3.55±0.52). The segmental distributions of fractures were T11 1, T12 5, L1 3, and L2 1, respectively. The mean time from injury to surgery was 2.45±0.43 months (time range 1.5~4 months). After preoperative education and communication, all patients signed informed consent forms authorized by the local ethics committee.
Inclusion Criteria and Exclusion Criteria
Inclusion criteria were a history of problematic back pain after low-energy damage and obvious symptoms when changing position; imaging evidence of typical signs of vacuum cracks or fluid accumulation in the vertebrae, accompanied by pedicle rupture; bone mineral density T-value ≤-2.5 and age ≥55 years; no signs of nerve or spinal cord injury.
Exclusion criteria: accompanied by spinal cord or nerve injury; vertebral malignancy, infection, bone metabolic disease, coagulation abnormality; the responsible vertebra is not associated with pedicle rupture; the vertebral body is so compressed that puncture cannot be performed; unable to tolerate or cooperate with surgery.
The Procedure of the Operation
The patient was placed in prone position, with routine disinfection and tissue covering. C-arm fluoroscopy was performed to locate the responsible vertebra, and local anesthesia was infiltrated and anesthetized. A 1cm incision was made on each side. Puncture needles were inserted into the inner edge of the pedicle in the upper quadrant of the projection of the joint on both sides, and lateral fluoroscopy was located at the posterior edge of the vertebra, and continued to be inserted into the middle 1/3 of the anterior vertebra. The position of the anteroposteric puncture needle was good, and the tissue fluid in the vertebral body was extracted with a 10mL syringe for pathology examination. The bone cement was slowly injected into the vertebral body along the puncture guide needle under fluoroscopy during the wire drawing stage, and the whole C-arm fluoroscopy was performed to confirm that the bone cement did not leak into the spinal canal. Implant the guide wire along the puncture needle on both sides, screw in two 4.5mm diameter hollow screws, and confirm the screw position by fore-lateral fluoroscopy. The incision was sutured in the whole layer. After the bone cement solidified, the patients turned over and returned to the ward.
Postoperative Management
X-ray and CT were reviewed the next day to confirm the distribution of bone cement and screws. After confirming that the cement was satisfactorily located, and that patients did not experience any unusual discomfort after getting out of bed while wearing the waist band, they were discharged. Calcium carbonate D3, calcitriol, disumab and other drugs were used to treat osteoporosis.
Observational Indicators
The time of the operation, bone cement injection amount, and bone cement leakage during operation were recorded. All patients underwent CT and X-ray examinations on the first day after surgery, and were followed up at 1, 3, 6, and 12 months after discharge.The improvement in quality of life was assessed using the Oswestry Disability Index (ODI),2,13,15 and the improvement in low back pain was assessed using the visual analogue Scale (VAS).9,13,16
Statistical Analysis
SPSS statistical software (ver. 25.0; IBM Corp., Armonk, NY, USA) was used to analyse the data. Paired sample t test was performed by one-way ANOVA. P < 0.05 indicated that the tests were significant.
Results
Hollow screw combined with percutaneous vertebroplasty was successfully performed in all 10 patients. Follow-up x-rays and CT scans on the first postoperative day confirmed that the cement distribution and the hollow screws were in good position. The average operation time was 39.2 ± 5.1 min (range: 30–45 min), and the average volume of bone cement injected was 5.85 ± 0.83 mL (range: 5–8 mL). There was only a very small amount of bleeding during the procedure. No leakage of bone cement into the vertebral canal occurred, but leakage of bone cement to the upper intervertebral disc occurred in one patient, and leakage of bone cement to the anterior superior margin of the vertebral body occurred in another patient. The average length of hospital stay was 4.80±0.86 days (range: 3–6 days). Typical case is shown in Figures 1–3.
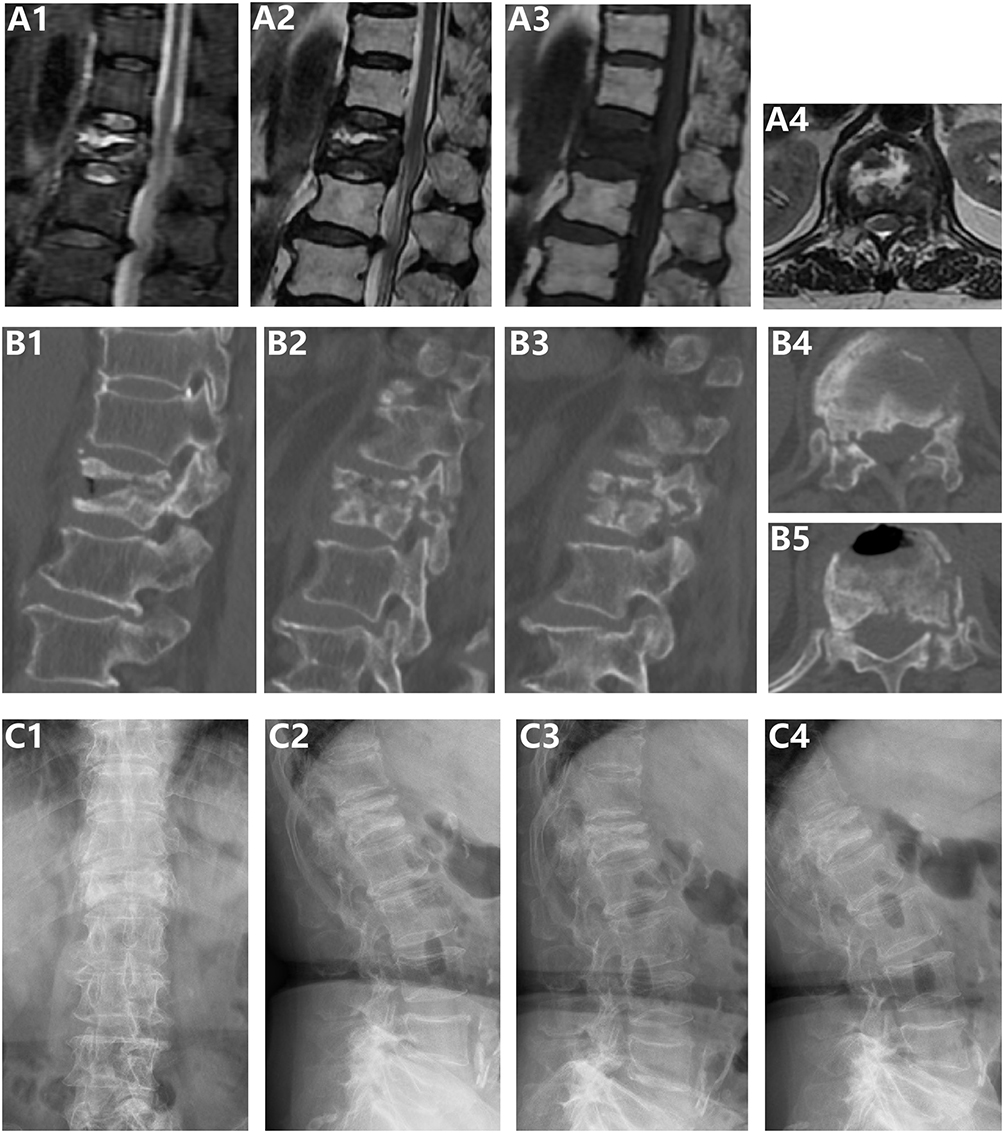 |
Figure 1 Kummell disease with bilateral pedicle rupture. A female 76 years of age complained of “low back pain and discomfort for 3 months”. (A1-A4) MRI examination indicated that the T12 vertebra was a fresh fracture, and the vacuum fissure in the vertebra showed a liquid signal. (B1-B5) Preoperative CT examination showed that the anterior middle part of T12 vertebral body was dehounded and vacuum fissure formed in the vertebral body, accompanied by bilateral pedicle fracture. Preoperative anterograde (C1) and lateral (C2) X-ray examination indicated that T12 vertebral body height decreased and fractures formed in the vertebral body. X-ray examination of the hyperflexion (C3) and hyperextension (C4) positions indicated dynamic instability in the fractures of the T12 vertebrae and the formation of pseudarthrosis. |
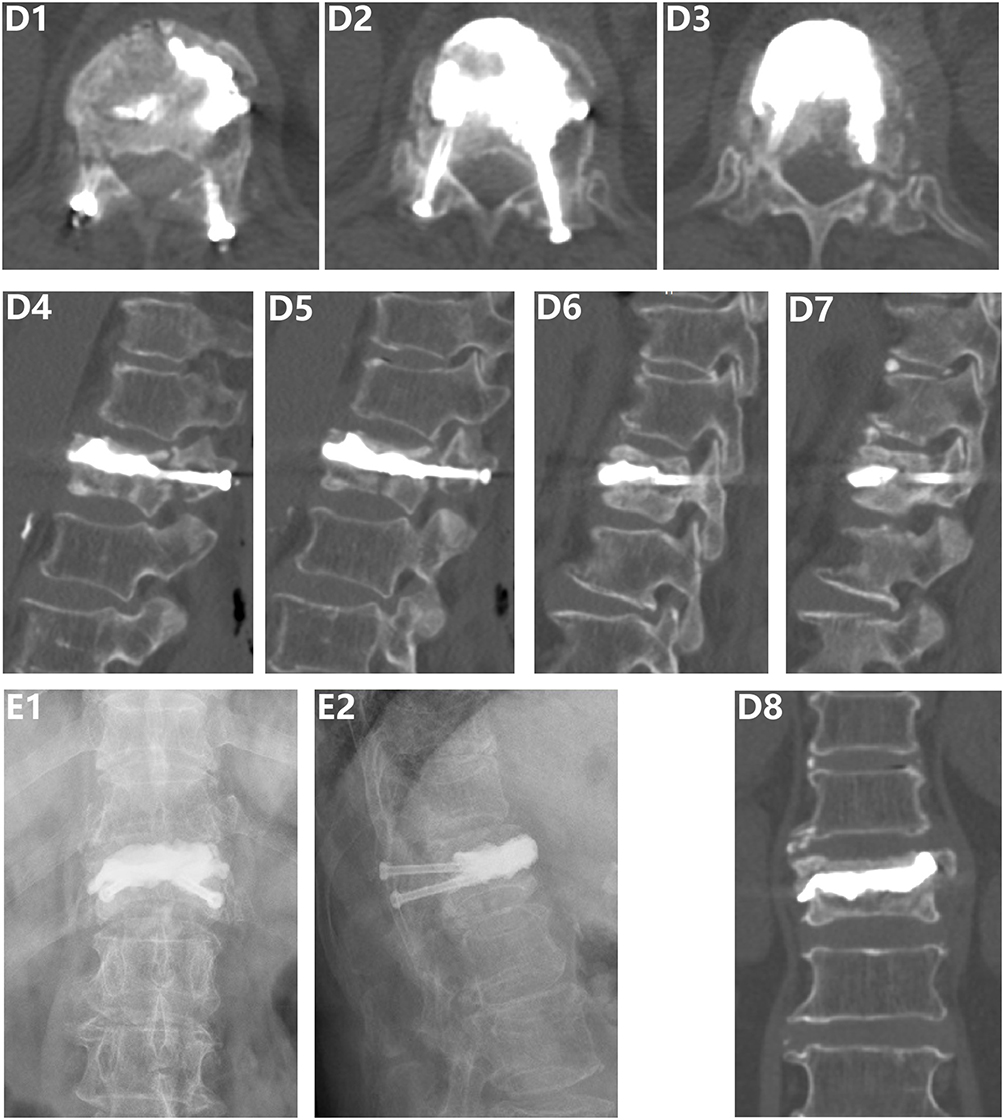 |
Figure 2 Re-examination on the first day after hollow screws combined with percutaneous vertebroplasty for three-column intensive treatment. (D1-D3) Postoperative cross-sectional CT plain scan showed that bone cement was evenly distributed in the vertebral body, no leakage in the spinal canal, and the hollow screw was well anchored to the bone cement, and the position of the hollow screw was good. (D4-D7) Sagittal plain CT scan showed that the vertebral bone cement was well anchored to the hollow screws, and the hollow screws were ideally positioned in the bilateral pedicles. (D8) Coronal CT showed good distribution of bone cement in the vertebral body. Anteroposteric (E1) and lateral (E2) X-rays showed that the bone cement was evenly distributed in the vertebral body, and the hollow screw was well anchored to the bone cement, and the position of the hollow screw was good. |
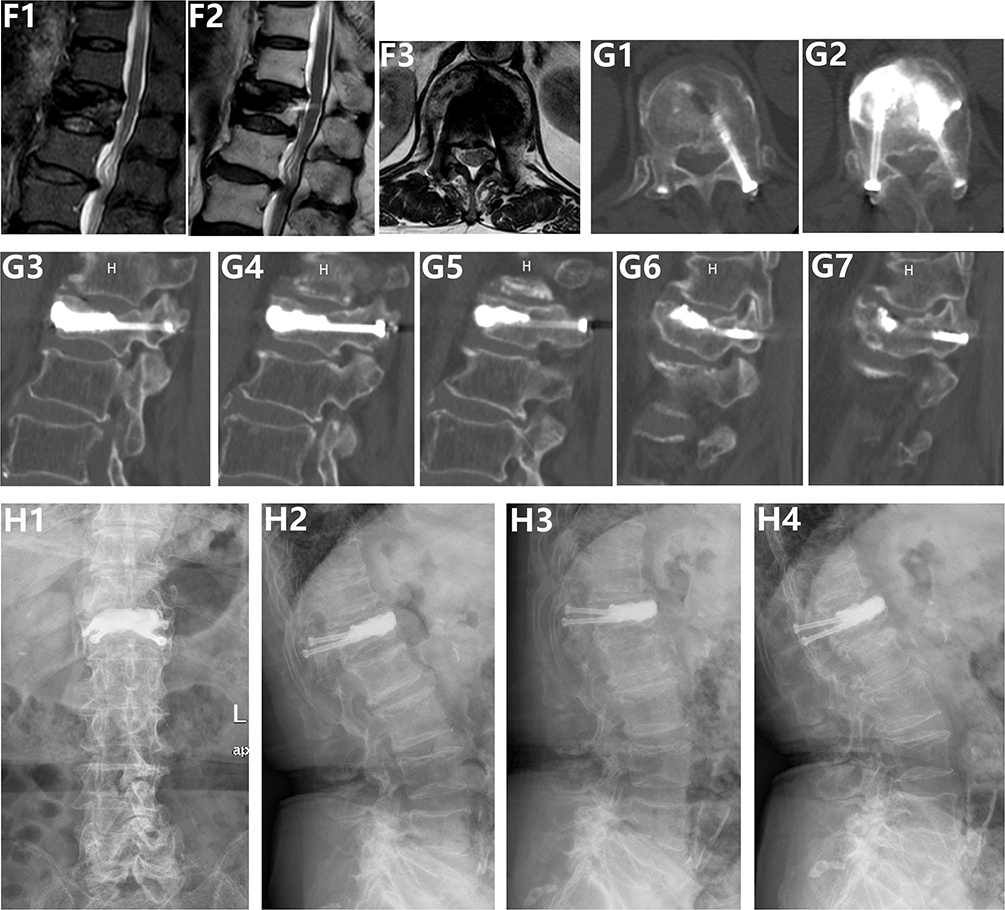 |
Figure 3 Reexamination 2 years after surgery showed that Kummell’s disease of the thoracic 12 vertebrae had been cured and the bilateral ruptured pedicle had healed. (F1-3) MRI examination indicated that the T12 vertebral fracture had healed, and the fluid signal in the vacuum fissure in the vertebral body disappeared. (G1-G2) CT cross-sectional plain scan showed that the hollow screw was well anchored with bone cement, and the broken pedicle was healed. (G3-G7) sagittal plain CT scan showed that the vertebral bone cement was well anchored with hollow screws, the bone cement was not loosened or displaced, and the broken vertebral pedicle was healed. Anteroposteric (H1) and lateral (H2) X-rays showed that the bone cement was evenly distributed in the vertebral body, and the hollow screws were well anchored with the bone cement. X-ray examination of the hyperflexion (H3) and hyperextension (H4) positions showed that the fractures of the T12 vertebrae disappeared and there was no dynamic instability. |
The mean VAS pain score before the operation was 8.35 ± 0.63, but the symptoms of back pain were significantly relieved after operation (P < 0.05). The mean VAS scores 1 day and 1, 3, 6, and 12 months after the operation were 3.45 ± 0.47, 2.55 ± 0.60, 1.89 ± 0.48, 1.50 ± 0.27, and 1.12 ± 0.20, respectively (Figure 4A). The mean preoperative ODI score was 75.70 ± 4.39, but this decreased significantly postoperatively (P < 0.05), being 37.70 ± 6.95 at 1 day and 26.40 ± 4.90, 23.70 ± 4.87, 21.70 ± 5.46, and 20.50 ± 4.21 at 1, 3, 6, and 12 months after the operation, respectively (Figure 4B).
 |
Figure 4 Results of VAS scores and ODI scores. (A) The VAS scores at 1 day and 1, 3, 6 and 12 months after surgery were significantly improved compared with those before surgery. (B) The ODI scores at 1 day and 1, 3, 6 and 12 months after surgery were significantly improved compared with those before surgery. * < 0.05, comparison with pre-operation scores. |
Discussion
We used hollow screws combined with PVP for three-column intensive treatment of Kummell’s disease with pedicle rupture. When the hollow screws were anchored with bone cement, three-column fixation of Kummell’s disease with a pedicle fracture was achieved, and the bone cement was strongly anchored within the injured vertebra, reducing the risks of long-term cement loosening, displacement, and prolapse. This aided healing of the fractured pedicle and avoided the disadvantages of open internal fixation surgery, namely serious trauma and reduced spinal motion.
The advantages of hollow screws combined with percutaneous vertebroplasty as a three-column intensive treatment
Hollow screws combined with PVP provide three-column reinforcement and firm fixation of fractured vertebrae. This not only stabilizes vertebral fractures, but also reduces the incidence rates of bone cement loosening, displacement, and propulsion after traditional PVP and PKP surgeries.11,13,14,17 Back pain was significantly relieved, and the stability of the vertebral pedicle was ensured via fixation of hollow screws, which aided pedicle fracture healing. The operation has the advantages of minimal trauma, a rapid recovery, convenient nursing, and a low surgical cost. There is no need for internal fixation of a bone graft fusion pedicle screw, which is associated with severe trauma, reduced spinal motion, inconvenient nursing, and high medical costs.5,7,14,18–20
Indications for Treatment
Hollow screws combined with three-column intensive percutaneous vertebroplasty can be used to treat stage I or II Kummell’s disease with pedicle rupture. This surgical approach is not recommended for patients with pathologic stage III Kummell’s disease, ie, patients with severe collapse of the posterior vertebral wall with symptoms of spinal cord or nerve root compression. Decompression and internal fixation surgery are required.7,10,14 To treat common osteoporotic vertebral compression fractures, PVP combined with pedicle screw fixation has been used.21 We believe that when the posterior column of the vertebral body is undamaged, it is not necessary to enhance fixation of the posterior column, which increases costs, radiation exposure, and the hospitalization time. In such cases, we do not recommend the use of three-column reinforcement treatment because direct PVP or PKP surgery is superior.22,23 For Kummell’s disease patients without pedicle fractures, percutaneous piercing followed by cement placement combined with three-column enhanced vertebroplasty is recommended.13
Operative Precautions
Bone cement solidifies quickly in vivo, the operation involves multiple steps, and the operative time window is narrow. Thus, the surgeon requires full fluoroscopic guidance when injecting/pushing bone cement and inserting screws, which increases radiation exposure for both the surgeon and patient. During insertion of the fine guide needle and removal of the puncture cannula, the needle should be well-controlled and fluoroscopically visible; it must not slip out.9,11 Preoperative CT should be performed to determine the appropriate screw length. After the guide needle is placed, a sharp surgical blade should be used to enlarge the fascia layer to avoid failed or inadequate fascia incision during screw insertion. Fascial obstruction and stalling during screw insertion increase the operative time. As most patients are severely osteoporotic, the entire screw insertion process should proceed under fluoroscopic guidance to ensure that the insertion depth is neither too deep nor too shallow.
Conclusion
Hollow screw placement combined with PVP as a three-column intensive treatment for Kummell’s disease with pedicle rupture is associated with minimal trauma, a rapid recovery, and firm fixation of bone cement. It not only avoids the disadvantages of traditional open internal fixation, such as major trauma and reduced spinal mobility, but also lessens the risk of bone cement loosening, displacement, and release compared to the risks after traditional PVP and PKP surgeries. The screw stabilizes the pedicle and promotes healing of the pedicle fracture. Our technique is one of the most effective surgical methods for treatment of Kummell’s disease with pedicle fracture.
Shortcomings
Given the low incidence of Kummell’s disease, especially disease with pedicle rupture, only 10 cases were included in this study; more cases are required. Increasing surgical experience will allow the method to be improved and ultimately optimised in future.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the Second Affiliated Hospital of Luohe Medical College. All participants have signed a written informed consent form. All studies were conducted in accordance with relevant guidelines and regulations.
Funding
This work was supported by Joint Co-construction Project of Henan Medical Science and Technology Research Plan (No. LHGJ20230943), Luohe Youth Talents Fund of China (No. 2018QNBJRC01004).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhou C, Huang S, Liao Y, et al. Feasibility Analysis of the Bone Cement-Gelatine Sponge Composite Intravertebral Prefilling Technique for Reducing Bone Cement Leakage in Stage I and II Kümmell’s Disease: a Prospective Randomized Controlled Trial. Orthopaedic Surgery. 2023;15:1763–1771. doi:10.1111/os.13764
2. Li Y, Qian Y, Shen G, Tang C, Zhong X, He S. Percutaneous mesh-container-plasty versus percutaneous kyphoplasty for the treatment of Kümmell’s disease: a retrospective cohort study. J Orthopaedic Surg Res. 2023;18:260. doi:10.1186/s13018-023-03753-1
3. Pan D, Chen D. Comparison of Unipedicular and Bipedicular Percutaneous Kyphoplasty for Kummell’s Disease. Geriatric Orthopaedic Surg Rehabi. 2022;13:21514593221099264. doi:10.1177/21514593221099264
4. Wang W, Liu Q, Liu WJ, Li QB, Cai L, Wang ZK. Different Performance of Intravertebral Vacuum Clefts in Kummell’s Disease and Relevant Treatment Strategies. Orthopaedic Surgery. 2020;12:199–209. doi:10.1111/os.12609
5. Shen H, Tang W, Yin X, et al. Comparison between percutaneous short-segment fixation and percutaneous vertebroplasty in treating Kummell’s disease: a minimum 2-year follow-up retrospective study. J Back Musculoskeletal Rehabi. 2024;37:195–203. doi:10.3233/bmr-230083
6. Kang H, Wei T, Zeng W, Lan S. Treatment of kyphotic deformity in Kümmell’s disease through vertebral body screw fixation and intertransverse process grafting: a case report. Medicine. 2024;103:e37058. doi:10.1097/md.0000000000037058
7. Guo X, Qiu Y, Liu X, Teng H, Hu H. Percutaneous short segmental fixation combined with bone cement augmentation for stage III Kümmell’s disease without nerve deformity. Medicine. 2024;103:37087. doi:10.1097/md.0000000000037087
8. Zou D, Wang H, Zhao Y, Sun X, Du W. Evaluation of the clinical efficacy of the bilateral pedicle cement anchoring technique in percutaneous vertebroplasty for Kümmell disease. Exp Ther Med. 2023;26:391. doi:10.3892/etm.2023.12090
9. Zhan Y, Bao C, Yang H, et al. Biomechanical analysis of a novel bone cement bridging screw system combined with percutaneous vertebroplasty for treating Kummell’s disease. Front Bioeng Biotechnol. 2023;11:1077192. doi:10.3389/fbioe.2023.1077192
10. Liu Y, Zhu Y, Li R, Jiang W, Yang H. Comparison between Percutaneous Kyphoplasty and Posterior Fixation Combined with Vertebroplasty in the Treatment of Stage III Kümmell’s Disease without Neurological Deficit. Biomed Res. Int. 2022;2193895. doi:10.1155/2022/2193895
11. Zhong S, Bao F, Fan Q, Zhao Y, Li W. Prevention of Bone Cement Displacement in Kümmell Disease without Neurological Deficits through Treatment with a Novel Hollow Pedicle Screw Combined with Kyphoplasty. Orthopaedic Surgery. 2023;15:2515–2522. doi:10.1111/os.13815
12. Dai S, Du Y, Chen L, Xu Y, Hu Q. A mid- and long-term follow-up study on the bilateral pedicle anchoring technique with percutaneous vertebroplasty for the treatment of Kümmell’s disease. Front Surg. 2023;10:1061498. doi:10.3389/fsurg.2023.1061498
13. Liu Y, Su Y, Xu Y, et al. The Use of Three-Column Enhanced Percutaneous Vertebroplasty to Treat Kummell’s Disease. J Pain Rese. 2022;15:2919–2926. doi:10.2147/jpr.s370578
14. Kuppan N, Muthu S, Parthasarathy S, Mohanen P. Strategies in the Management of Osteoporotic Kummell’s Disease. J Orthopaedic Case Repo. 2022;12:34–38. doi:10.13107/jocr.2022.v12.i10.3356
15. Wu XF, Ping Y, Zeng XQ, et al. Percutaneous Vertebroplasty with Side-Opening Cannula or Front-Opening Cannula in the Treatment of Kummell Disease? Orthopaedic Surgery. 2020;12:1190–1198. doi:10.1111/os.12730
16. Park JW, Park JH, Jeon HJ, Lee JY, Cho BM, Park SH. Kummell’s Disease Treated with Percutaneous Vertebroplasty: minimum 1 Year Follow-Up. Korean j Neurotrauma. 2017;13:119–123. doi:10.13004/kjnt.2017.13.2.119
17. Kim P, Kim SW. Balloon Kyphoplasty: an Effective Treatment for Kummell Disease? Korean Journal of Spine. 2016;13:102–106. doi:10.14245/kjs.2016.13.3.102
18. Bae J, Ang CY, Syed I, Jeong SK, Shin SH, Lee SH. Minimally Invasive Surgery Transpedicular Intrabody Cage Technique for the Management of Kummell Disease. Int j Spine Surg. 2024;18:73–80. doi:10.14444/8570
19. Park HJ, Kim HB, You KH, Kang MS. Percutaneous transpedicular intracorporeal cage grafting for Kümmell disease. Acta neurochirurgica. 2022;164:1891–1894. doi:10.1007/s00701-022-05211-z
20. Liu F, Chen Z, Lou C, et al. Anterior reconstruction versus posterior osteotomy in treating Kummell’s disease with neurological deficits: a systematic review. Acta orthopaedica et traumatologica turcica. 2018;52:283–288. doi:10.1016/j.aott.2018.05.002
21. Sezer C. Pedicle Screw Fixation with Percutaneous Vertebroplasty for Traumatic Thoracolumbar Vertebral Compression Fracture. Niger J Clin Pract. 24:1360–1365. doi:10.4103/njcp.njcp_47_20
22. Yu W, Chen D, Ding X, et al. A critical appraisal of clinical practice guidelines on surgical treatments for spinal metastasis. Eur Spine J. 2024;33:1868–1898. doi:10.1007/s00586-023-08127-z
23. Liu XY, Feng M, Zhang XL, et al. Are Sandwich Vertebrae Prone to Refracture After Percutaneous Vertebroplasty or Kyphoplasty? A Meta-Analysis. Int j Spine Surg. 2024;27:8577. doi:10.14444/8577
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.