")
Back to Journals » Journal of Pain Research » Volume 17
Home-Based Shi’s Knee Daoyin Exercise for Knee Osteoarthritis: A Randomized Controlled Pilot Trial
Authors Xu K , Zhang J, Ma W, Wang Y, Chen B, Gao N, Pang J, Zhan H
Received 16 March 2024
Accepted for publication 16 August 2024
Published 29 August 2024 Volume 2024:17 Pages 2811—2822
DOI https://doi.org/10.2147/JPR.S469176
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Houman Danesh
Kun Xu,1,2 Jiefan Zhang,1,2 Wei Ma,1,2 Yongyu Wang,1,2 Bo Chen,1,2 Ningyang Gao,1,2 Jian Pang,1,2 Hongsheng Zhan1,2
1Shi’s Center of Orthopedics and Traumatology, Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 2Institute of Traumatology & Orthopedics, Shanghai Academy of Traditional Chinese Medicine, Shanghai, People’s Republic of China
Correspondence: Hongsheng Zhan; Jian Pang, Email [email protected]; [email protected]
Objective: Shi’s Knee Daoyin (SKD) exercise is a treatment derived from Traditional Chinese exercise (TCE) specifically designed for lower limb health care. This study aimed to assess the feasibility of conducting a randomized controlled trial to explore the effectiveness of SKD exercise in treating knee osteoarthritis (KOA).
Methods: Participants were randomized to receive Health Education (HE) or SKD exercise. The primary outcomes were feasibility and safety outcomes, including participant recruitment rate, retention rate, as well as adherence to intervention. The secondary outcomes included Visual Analogue Scale (VAS) scores for pain, the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score, the 20-Meter Walk Test (20-MWT) and the 5-times Chair-Stand Test (5-CST).
Results: The results indicate that out of 89 individuals invited to participate in the study, 72 were eligible and agreed to participate, resulting in a recruitment rate of 80.9%. All participating patients completed the follow-up and were included in the analysis; no patients dropped out of the study due to adverse events. The secondary outcome measures showed that after twelve weeks of treatment, the VAS score, WOMAC total score, WOMAC pain score, WOMAC stiffness score, and WOMAC function score of patients in the HE group and SKD group all improved, but the improvement was more significant in the SKD group. The 20-MWT of SKD group after treatment was significantly shorter than before treatment (P< 0.001); There was no significant difference in 20-MWT between the HE group and baseline after treatment. The performance of the two groups of patients improved in 5-CST, but there was no statistical difference between the two groups after treatment (P=2.439).
Conclusion: This study evaluated the feasibility and effectiveness of home-based SKD exercise intervention in alleviating symptoms in patients with symptomatic KOA, providing valuable information for designing an appropriate randomized controlled study.
Keywords: knee osteoarthritis, pilot, exercise, randomized controlled trial
Introduction
Knee osteoarthritis (KOA) is a prevalent joint disease among middle-aged and elderly patients, impacting all tissue components within and surrounding the joint.1 KOA is characterized by cartilage degeneration, subchondral bone remodeling,2 meniscal degeneration,3,4 inflammation and fibrosis of both infrapatellar fat pad and synovial membrane that are involved in pain.5 Factors contributing to the development of OA include age, joint trauma, other joint diseases, and overweight/obesity.6 Moreover, KOA causes a low health-related quality of life by negatively affecting psychological and physical wellbeing.7,8 It is the primary cause of disability with a negative impact on the physical and mental health of people across the globe.9 Based on epidemiological statistics, the incidence rate of KOA sharply increases with age.10 The increasing incidence of OA has globally led to substantial health and economic burden;11 specifically in China, where, the number of aging population has been rapidly growing.12 China has the largest global population, besides, its national population is rapidly aging; the rate of aging population (≥60 years) is predicted at 25.3% in 2030, and over 30% in 2050.13 According to a 2014 national population-based survey in China, the prevalence rate of symptomatic KOA was at approximately 8.1% among Chinese residents aged 45 years, and significantly increased with advancing age.14
Nonetheless, to our knowledge, no effective disease-modifying therapy for KOA has been reported. Existing treatments are available to reduce pain, improve joint mobility, and optimize survival and quality of life. Although pharmacological treatment can effectively relieve pain and improve mobility in KOA, accumulating evidence reveals that long-term use of pharmacotherapy and intra-articular injections may lead to severe undesirable side effects, including gastrointestinal reactions and multi-organ failure.15
In recent years, exercise therapy is highly recommended inexpert consensus guidelines for the treatment of osteoarthritis in many regions and countries; most experts recommend exercise therapy as preferred non-pharmacological intervention for KOA patients.13,16,17 Increasing evidence from meta-analyses and randomized controlled trials reported that the practice of Traditional Chinese exercise (TCE), a category of therapeutic exercises, is increasing across the globe.18–21 These exercises include Tai Chi, Qigong and Daoyin, which have substantially benefited human health for over 2000 years in treating KOA.22–26 Notably, TCE is generally accepted by doctors and patients in China. Specifically, Shi’s Knee Daoyin (SKD) exercise is a treatment based on TCE established for lower limb health care. However, unlike the conventional exercises, SKD is more simplified and targeted in exercise protocol.27–29 Therefore, although many older adults already practice SKD, no randomized controlled studies have been performed to validate its therapeutic effect in treating KOA. Future research should conduct a comprehensive powered randomized controlled clinical trial to confirm the efficacy of SKD exercise for KOA. Nonetheless, a feasibility and pilot study should be first conducted to find out its acceptability, safety and potential treatment effect.
As such, this paper seeked to assess the feasibility of the research methods, procedures, and interventions of conducting a two-group parallel randomized controlled clinical study, to provide a research foundation for exploring the effectiveness of home-based SKD exercise on KOA in the future.
Methods
Study Design and Setting
In preparation for a comprehensively powered randomized controlled trial, this pilot and feasibility randomized controlled trial was conducted at the outpatient clinic of Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine in Shanghai, China.
The trial was performed based on the principles outlined in the Declaration of Helsinki (2013 revision World Medical Association Declaration of Helsinki) and Consolidated Standards of Reporting Trials (CONSORT) 2010 extension for randomised pilot and feasibility trials.30 The study protocol was approved by the Chinese Ethics Committee of Registering Clinial Trials (No.ChiECRCT-20170083). The trial protocol was also registered to the Chinese Clinical Trial Registry and chictr.gov.cn (No.ChiCTR-IPR-17013465). All participants signed informed consent forms before participating in the study.
Participants
Inclusion Criteria
The inclusion criteria included: age ≥ 45years (either sex); patients fulfilling the diagnostic criteria of KOA proposed by American Rheumatism Association guidelines;31 patients experiencing chronic knee pain during the past six months; patients not under any clinical study and/or exercise program before enrolling into this study.
Exclusion Criteria
Participants will be excluded if they meet any of the following criteria: pain in the knee caused by floating cartilage, joint effusion, malignant, or autoimmune disease; patients complicated with infection diseases or severe systemic diseases: heart and cardiovascular system dysfunction, liver dysfunction, renal dysfunction, coagulation dysfunction, or serious psychosomatic diseases; patients with injections in knee joints within 6 months before the study; patients with a history of trauma or previous operations on the knee.
Recruitment
Patient diagnosis of KOA was confirmed at the Orthopedic-Traumatological Department, Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine. The patients were consecutively screened for availability between January 2017 and December 2019. Before enrolment, each participant was verbally and in written form informed on the objective and nature of the trial and about the investigator. The investigator also informed the patients that their participation is voluntary and are free to withdraw at any time for any reason. A written formal informed consent form was signed and obtained from all interested and eligible participants. The researcher recorded data from all potential participants including primary reasons for exclusion, declines, or withdrawals for the entire duration of the study (Figure 1).
 |
Figure 1 Flow diagram showing patient enrolment and follow-up. |
Sample Size Calculation
Notably, the primary goal of this pilot trial was to assess the feasibility of the research methods, procedures, and interventions. According to the research guidelines, a pilot feasibility study can accept 20–30 samples.32–34 Thus, based on the consensus opinion of experts including statisticians, public health specialists and clinicians, it was agreed that a sample of 72 would be adequate to inform feasibility for a fully powered randomized controlled trial and gather preliminary outcome data.35
Intervention
Health Education Group (HE Group)
At the first visit, each subject acquired HE lecture on KOA for approximately one hour and a paper version of manual titled “Health Education for KOA” was provided to consolidate their understanding and memory of health knowledge on KOA (Appendix 1). This education involved several chapters including risk factors; examination and diagnosis of KOA; lifestyle modifications including weight reduction and activity modification; nursing care and treatment options for KOA; home environment; benefits of regular physical activity and methods of self-assessment and recording fluctuate of KOA symptoms. The frequency of HE is once a week, and the total times of treatments is 10. The follow-up times is 12 weeks.
SKD Group
The SKD group was subjected to SKD exercise treatment based on the HE group. The exercise protocol comprised three forms (Appendix 2). During the exercise, it was necessary to lay stress on the coordination of limb movements, respiratory movements and mind, whole-body relaxation, and spiritual relaxation. An experienced coach provided guidance to patients on how to perform the exercises. The coach instructed participants on how to perform exercises 3 times in the first two weeks, 30 minutes each time. Then, 3 to 12 weeks was devoted for the SKD exercise, and exercise frequency is once a week, and the total times of treatments is 10. At the end of each exercise period, participants noted down the exercise record using a personal exercise record booklet, which included the duration of the exercise. The follow-up times is 12 weeks.
Randomization and Allocation Concealment
Blocked randomization was used to assign participants to two groups of the HE group and the SKD group at the ratio of 1:1. This was conducted using SPSS software by an independent statistician who was not involved in any other part of the trial. Block size was randomly selected between 2 and 4. The randomization list was kept in a locked cabinet. Serially numbered, identical opaque, and sealed envelopes were used to guarantee randomization concealment. Thereafter, concealment of allocation was also ensured by sealed, opaque, and sequentially numbered envelopes.
Outcomes
Primary Outcomes
The primary outcomes were feasibility and safety outcomes, including participant recruitment rate, retention rate, as well as adherence to intervention. Recruitment rate was computed as the percentage of randomized eligible participants. Retention rate was calculated as the proportion of the number of subjects participating until the end of the study period. Participant treatment adherence to intervention was calculated as the completion percentage of the protocol exercise program. Security was assessed by monitoring the occurrence of harmful events.
Secondary Outcomes
The secondary outcomes of the study included the following preliminary effectiveness outcomes, primarily including patient self-assessment measures; a visual analogue scale (VAS) scores for pain, the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score, the 20-Meter Walk Test (20-MWT) and the 5-times Chair-Stand Test (5-CST).
VAS
The VAS-pain score was used to quantify the subjective pain intensity of knee joint in daily life. The VAS-pain method was performed employing a10-cm horizontal line segments with marked “no pain” on the left (scored as 0), representing the absence of any pain, and “the worst pain” (scored as 10) on the right, representing extreme or intolerable pain.36 Participants were required to mark the VAS drawing a vertical line on the horizontal bar to record the degree of pain they perceived while on walking on a flat way weekly during intervention.
WOMAC
This work used the Chinese Likert-scale version of WOMAC questionnaire.37 The WOMAC questionnaire comprises five questions assessing pain intensity in daily activities (pain subscale, range 0–20), two items for stiffness (stiffness subscale, range 0–8), and 17 items for physical function (physical function subscale, range 0–68). Each of WOMAC questions is answered by selecting one of the five different answers: none (0), mild (1), moderate (2), severe (3) and extreme (4). We calculated the WOMAC total score and subscales score. Notably, the WOMAC score has been extensively validated, and widely recommended and used in studies of KOA.38 The higher the WOMAC score, the greater the pain, stiffness, and dysfunction.
20-MWT
The 20-MWT was used to assess walking ability and endurance;39 participants were instructed to walk three times along a 20-meter walkway at a comfortable walking pace. The researchers recorded the time the participants spent on a 20-meter walk and further calculated the average walking time in seconds.
5-CST
Of note, 5-CST provides a direct assessment of overall physical health, including leg strength and knee function.40 Participants were asked to repeat the sitting test five times, while sitting on a chair. The researchers recorded the duration participants spent on a chair repeating the sitting test five times.
Statistical Analysis
All relevant data obtained in this study were further compiled and analyzed using SPSS 17.0 statistical software.41 Continuous data with a normal distribution are presented as mean ± standard (X±S) deviation and analyzed for differences between groups using Student’s T-test. For data not normally distributed, we present the results as median (Q1,Q3) and analyze intergroup differences using the Wilcoxon rank sum test. Categorical data are expressed as counts and percentages, with differences between study groups determined using either the chi-square test or Fisher’s exact test, depending on which is most appropriate. And p<0.05 was considered indicative of a significant difference in the data. Used the last observation carry over method to compensate for the missing data.
Results
Primary Outcomes
Recruitment and Retention Rate
The flow chart for patient recruitment and retention is shown in Figure 1. A total of 89 participants were invited to participate in this study; out of whom 72 of them (64 women, 8 men, mean age=67.65±6.53 years) were found eligible and participated in the trial. The recruitment rate was 80.9%. Analysis and follow-up were performed in all patients.
Treatment Adherence
Generally, 58/72 (81%) of patients attended at least 80% of their sessions.
Safety
Safety was analyzed in 72 patients participating in the trial. No deaths or other adverse events were reported during the study period; besides, no patients were discontinued due to adverse events.
Baseline Characteristics
HE group comprised 36 cases, including 4 males (11.1%) and 32 females (88.9%); their average age and BMI was 68.08±5.64 years and 23.09±3.51 Kg/m2, respectively. Furthermore, the disease duration distribution was between 3 and 108 months; the average duration was 12 (8, 34) months. SKD group comprised 36 cases, including 4 males (11.1%) and 32 females (88.9%); their average age was 67.22±7.37 years and BMI was 24.05±2.89 Kg/m2, respectively. Furthermore, the disease duration distribution was between 1 and 144 months, and the average duration was 10.6 (8, 36.5) months. The two groups were comparable on their baseline information without any significant differences (P>0.05) (Table 1).
 |
Table 1 Baseline Characteristics of Participants |
Secondary Outcomes
Table 2 provides a summary of VAS pain scores and WOMAC scores at Baseline, 4 weeks, 8 weeks, and 12 weeks, along with 20-MWT and 5-CST times at both Baseline and 12 weeks.
 |
Table 2 WOMAC, VAS, 20-MWT and 5-CST Score Changes |
VAS
In general, the degree of pain in both groups decreased after treatment (Figure 2); specifically, the pain improvement in the SKD group was better than that in the HE group. No significant difference was noted in VAS-pain scores between the two groups in baseline (P=0.465). VAS-pain score of SKD group after treatment was significantly lower than that before treatment (P<0.001). However, no significant difference was found between the VAS-pain scores before and after treatment in the HE group (P=0.638) (Table 2).
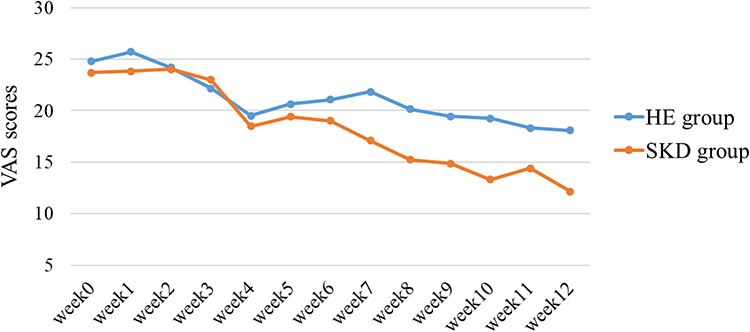 |
Figure 2 The effects of SKD on VAS-Pain scores. The scores were shown as mean. |
WOMAC
One of the secondary outcome measures for both groups was the change in the WOMAC score 12 weeks after treatment (Figure 3–6). The WOMAC scores of both groups were significantly lower than that of the baseline. The mean WOMAC pain, stiffness, physical function, and total score gradually declined over time in both groups. Analysis revealed significant changes in the WOMAC scores and subscales over time (P<0.001), indicating a significant change over group-by-time interactions for WOMAC pain (P=0.03), physical function (P=0.019), and total score (P=0.023). However, the interactions group-by-time were not significant in stiffness (P=0.572). Additionally, analysis of variance with repeated measures over time showed no difference between the groups (P=0.706) (Table 2).
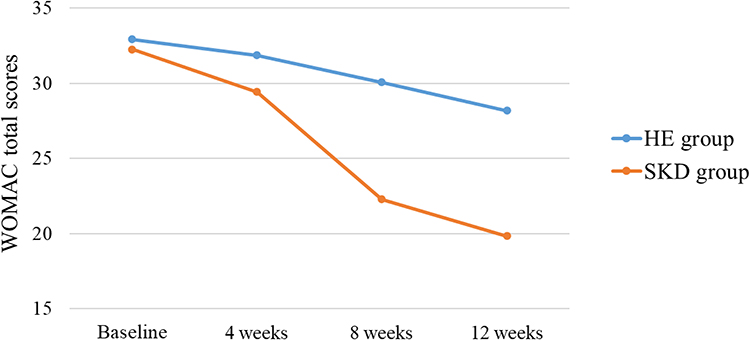 |
Figure 3 The effects of SKD on WOMAC total scores. The scores were shown as mean. |
 |
Figure 4 The effects of SKD on WOMAC pain scores. The scores were shown as mean. |
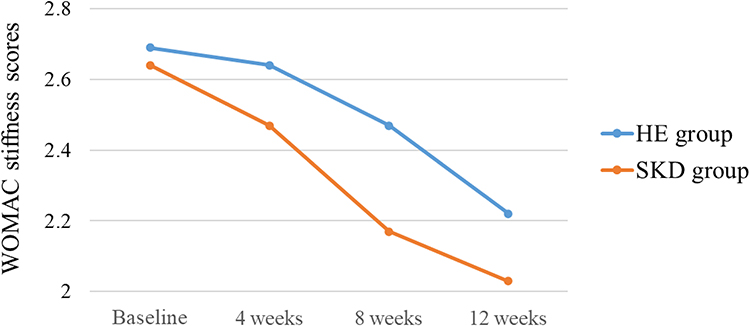 |
Figure 5 The effects of SKD on WOMAC stiffness scores. The scores were shown as mean. |
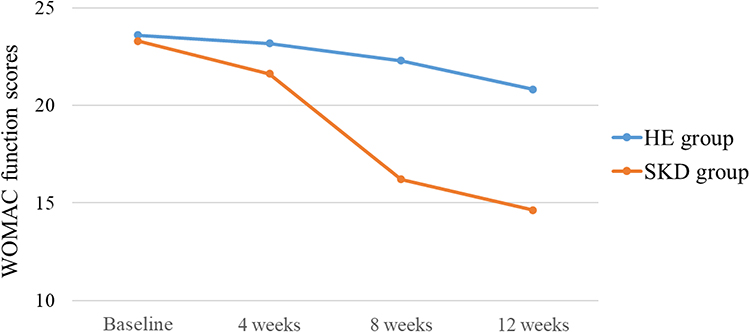 |
Figure 6 The effects of SKD on WOMAC function scores. The scores were shown as mean. |
20-MWT
Participants improved their performance of 20-MWT from baseline to week 12. No significant difference was noted in 20-MWT between the two groups in baseline (P=0.312). The 20-MWT after treatment in the SKD group was significantly shorter than that before treatment (P<0.001); no significant difference was noted between the 20-MWT after treatment and baseline in the HE group (P=1.036) (Table 2).
5-CST
Participants improved their performance of 5-CST from baseline to week 12, but no statistical difference was found between the two groups when compared after treatment (P=2.439) (Table 2).
Discussion
The present pilot study found that unsupervised SKD exercise in a home setting thrice-weekly for 12 consecutive weeks is feasible and acceptable recommendation to patients with KOA. Moreover, we provide preliminary, exploratory information to inform the design of future fully powered trial. To our knowledge, this is the first clinical study to investigate the efficacy and feasibility of SKD exercise as an intervention for individuals diagnosed with KOA.
In this pilot trial, the recruitment rate is 80.9%, retention rate is 100%, and treatment adherence is 81%. The author believes that the high recruitment rate, retention rate, and treatment adherence may be related to the researchers’ sufficient supportive supervision and frequent interaction with participants. Previous studies have also shown that sufficient supportive supervision and frequent interaction with participants can improve retention rate and treatment adherence.42 Nonetheless, attendance and compliance figures in the present study were comparable. Notably, adherence and compliance rates could be increased with simplified exercise protocol. In contrast with the protocol of SKD exercise (Appendix 2), the other TCEs (e. g.Tai Chi) protocols are lengthy and complex, thus regarded as a class of exercises requiring high degree of fixed attention and strong remembrance.43 Aging is often associated with a decline in cognitive function and memory.44 OA is a chronic degenerative disease affecting the aging population. Thus, simpler exercise protocols have advantages compared to other conventional exercises among individuals with KOA. For instance, home-based SKD exercise may be more suitable for older people with frailty or at risk of frailty, this is because they allow practice in a familiar environment. Practitioners may derive long-term benefit from daily SKD exercises, since they are implemented without supervision and requirements of adaptation to environmental conditions. However, lack of supervision is a potential limitation that potentially leads to unsafety, non-adherence, and incorrect quantification.45 Our findings showed that SKD was tolerated without adverse events. Notably, regarding the ongoing 2019 novel coronavirus (2019-nCoV) pandemic, individuals are expected to minimize outdoor movements or even self-isolate at home, thereby resulting in less physical activity and additional novel health problems with KOA. Although other exercises are available, with additional apparatus and equipment, SKD has its unique advantage as an exercise that can be performed at home at any time.
Several pieces of research evidence have been published regarding the benefit of therapeutic exercise for KOA.46–48 Evidence from high-quality studies demonstrates that therapeutic exercise is effective in pain reduction, improvement of articular function and global life quality among individuals with symptomatic KOA.49 As for TCE, a recent meta-analysis suggested that TCE may be effective in relieving pain, alleviating stiffness and improving the functions of the joints in patients with KOA.22 In different meta-analysis, the results supported the evidence that Tai Chi exercise, one type of TCE, has a significant beneficial effect on improving function of walking and posture control among older patients with KOA.50–53
This pilot study provides encouraging results for SKD exercise in KOA, and demonstrates the feasibility of conducting larger comprehensive powered randomized controlled trial with a similar intervention protocol. This study was designed to assess feasibility and estimated effect size, but was not powered to detect between-group. Through data analysis, we noted a decreasing trend of the WOMAC total score in the SKD and control groups; a significant decrease was observed in the SKD group. Meanwhile, the mean score reduction on WOMAC pain subscale of SKD group after 12 weeks of intervention was 3.14 compared to the baseline time value; besides, the decrease of mean VAS-pain score of SKD group was 11.56 compared to the baseline time value. This was remarkably better than that of the control group. Therefore, these preliminary results support the efficacy of SKD in alleviating symptoms in patients diagnosed with KOA. Our findings provide a reference for sample size calculation of comprehensively powered randomized controlled trial with similar interventions. Based on the foregoing data on VAS-pain score (the smallest clinically relevant difference (MCID) of the VAS-pain index of 1.8 units),54 we preliminarily estimated the sample size necessary for the main trial to be 80 (HE group=40, SKD group=40). If we want to detect 6.7 unit MCID of WOMAC total score,55 approximately 260 subjects (HE group=130, SKD group=130) should be recruited. Thus, this study is exploratory by design. The efficacy of SKD exercise treatment on KOA will be assessed in a fully loaded randomized controlled study.
This study has worth-mentioning limitations. First, SKD may improve the lower limb muscle strength of patients, however, the objective indicators including Isometric Muscle Strength and Gait Parameters were not included. Secondly, relatively small sample size led to the lack of statistical significance of the results. In the planned next steps, a larger sample size is necessary to confirm our preliminary findings of reduction in pain intensity and explore other potential undetected benefits. Thirdly, this pilot study did not collect Kellgren Lawrence information from patients, lacking an assessment of the severity of KOA in patients. Additionally, this pilot study only included mild to moderate pain cases, whereas patients with severe pain may hardly tolerate this exercise intervention. As such, our findings may not be precisely extrapolated to KOA patients with severe pain.
Conclusion
In conclusion, the present study provides important and valuable information to design a suitably powered randomized controlled study assessing the efficacy of home-based SKD exercise intervention in relieving symptoms of patients diagnosed with symptomatic KOA.
Data Sharing Statement
The research team will preserve the original paper-version CRFs in a locked cabinet at the Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine for at least 5 years after publication of the study results. The datasets are available from the corresponding author on reasonable request.
Acknowledgments
The authors would like to thank all subjects who volunteered to participate in this study and demonstrated great motivation and commitment.
Funding
This work was supported by the Science and Technology Commission of Shanghai Municipality (no. 21Y11921600), Shanghai Municipal Clinical Research Center for Chronic Musculoskeletal Conditions (no. 20MC1920600), Shanghai Municipal Key Clinical Specialty Project (no. shslczdzk03901), Shanghai Medical Innovation Research Project (no. 21Y11921600) and financially supported by Program for Shanghai High-Level Local University Innovation Team (SZY20220315).
Disclosure
No potential conflict of interest was reported by the authors.
References
1. Zeng L, Zhou G, Yang W, Liu J. Guidelines for the diagnosis and treatment of knee osteoarthritis with integrative medicine based on traditional Chinese medicine. Front Med Lausanne. 2023;10:1260943. doi:10.3389/fmed.2023.1260943
2. Zhu X, Chan YT, Yung P, Tuan RS, Jiang Y. Subchondral Bone Remodeling: a Therapeutic Target for Osteoarthritis. Front Cell Dev Biol. 2020;8:607764. doi:10.3389/fcell.2020.607764
3. Ozeki N, Koga H, Sekiya I. Degenerative Meniscus in Knee Osteoarthritis: from Pathology to Treatment. Life. 2022;12. doi:10.3390/life12040603
4. Battistelli M, Favero M, Burini D, et al. Morphological and ultrastructural analysis of normal, injured and osteoarthritic human knee menisci. Eur j Histochem. 2019;63.
5. Emmi A, Stocco E, Boscolo-Berto R, et al. Infrapatellar Fat Pad-Synovial Membrane Anatomo-Fuctional Unit: microscopic Basis for Piezo1/2 Mechanosensors Involvement in Osteoarthritis Pain. Front Cell Dev Biol. 2022;10:886604. doi:10.3389/fcell.2022.886604
6. Bliddal H. Definition, pathology and pathogenesis of osteoarthritis. Ugeskr Laeger. 2020;182.
7. Vennu V, Alshammary AF, Farzan R, Ali KI. A conceptual model of factors associated with health-related quality of life in men and women with knee osteoarthritis in Riyadh, Saudi Arabia: a multicenter cross-sectional study. Medicine. 2023;102:e34175. doi:10.1097/MD.0000000000034175
8. Aw NM, Yeo SJ, Wylde V, et al. Impact of pain sensitisation on the quality of life of patients with knee osteoarthritis. RMD Open. 2022;8.
9. Vina ER, Kwoh CK. Epidemiology of osteoarthritis: literature update. Current Opinion in Rheum. 2017;30:1.
10. Chen H, Wu J, Wang Z, et al. Trends and Patterns of Knee Osteoarthritis in China: a Longitudinal Study of 17.7 Million Adults from 2008 to 2017. Int J Environ Res Public Health. 2021;18:8864. doi:10.3390/ijerph18168864
11. Weng Q, Chen Q, Jiang T, et al. Global burden of early-onset osteoarthritis, 1990-2019: results from the Global Burden of Disease Study 2019. Ann Rheum Dis. 2024;83:915–925. doi:10.1136/ard-2023-225324
12. China NBOS Communiqué of the Seventh National Population Census (No. 5). 2021.
13. Wu Y, Dang J, Liu F, Ao T, Wang L China report of the development on Siliver industry (2014).Social Sciences Academic Press (China); 2014.
14. Ao KT, Wang S, Zhang Y, Niu J, Ao KT, Lin J. The prevalence of symptomatic knee osteoarthritis in China: results from China Health and Retirement Longitudinal Study. Osteoarthritis Cartil. 2015;23. doi:10.1016/j.joca.2015.03.021
15. Jung SY, Jang EJ, Nam SW, et al. Comparative effectiveness of oral pharmacologic interventions for knee osteoarthritis: a network meta-analysis. Modern Rheumatology. 2018;1–19.
16. Hochberg MC, Altman RD, April KT, Benkhalti M, Tugwell P. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, Hip, and knee. Arthritis Care Rese. 2012;64:465–474. doi:10.1002/acr.21596
17. Maurizio C, Francis B, Marc H, et al. Commentary on recent therapeutic guidelines for osteoarthritis. Semin Arthritis Rheum. 2015.
18. Siu PM, Yu AP, Yu DS, Hui SS, Woo J. Effectiveness of Tai Chi training to alleviate metabolic syndrome in abdominal obese older adults: a randomised controlled trial. Lancet. 2017; 390:S11.
19. Fong SSM, Liu KPY, Luk WS, Leung JCY, Chung JWY. Tai Chi Qigong for survivors of breast cancer: a randomised controlled trial. Lancet. 2017;390:S32. doi:10.1016/S0140-6736(17)33170-7
20. Chow TH, Lee BY, Ang ABF, Cheung VYK, Takemura S, Takemura S. The effect of Chinese martial arts Tai Chi Chuan on prevention of osteoporosis: a systematic review. J Orthopaedic Translation. 2017;12:74–84. doi:10.1016/j.jot.2017.06.001
21. Claudia C, Wang K, Arkopal L, et al. Trends in Yoga, Tai Chi, and Qigong Use Among US Adults, 2002-2017. Am J Public Health. 2019.
22. Ruojin L, Hongwei C, Jiahao F, et al. Effectiveness of Traditional Chinese Exercise for Symptoms of Knee Osteoarthritis: a Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int J Environ Res Public Health. 2020;18:17. doi:10.3390/ijerph18010017
23. Miao Z, Hailong Z, Fenglei L, et al. Pulmonary Daoyin as a traditional Chinese medicine rehabilitation programme for patients with IPF: a randomized controlled trial. Respirology. 2020.
24. Chan J, Ho R, Ka-Fai C, et al. Qigong Exercise Alleviates Fatigue, Anxiety, and Depressive Symptoms, Improves Sleep Quality, and Shortens Sleep Latency in Persons with Chronic Fatigue Syndrome-Like Illness. Evid Based Compl Alternat Med. 2014;2014:106048. doi:10.1155/2014/106048
25. Zhang Y, Huang L, Su Y, et al. The Effects of Traditional Chinese Exercise in Treating Knee Osteoarthritis: a Systematic Review and Meta-Analysis. PLoS One. 2017; 12:e0170237.
26. Li F. Transforming traditional Tai Ji Quan techniques into integrative movement therapy— tai Ji Quan: moving for Better Balance. J Sport Health Sci. 2014;3:9–15. doi:10.1016/j.jshs.2013.11.002
27. Zhu S, Shi K, Yan J, et al. A modified 6-form Tai Chi for patients with COPD. Comp Ther Med. 2018;S0443034201.
28. Chen MC, Liu HE, Huang HY, Chiou AF. The effect of a simple traditional exercise programme (Baduanjin exercise) on sleep quality of older adults: a randomized controlled trial. Int J Nursing Stud. 2012;49:265–273. doi:10.1016/j.ijnurstu.2011.09.009
29. Liang S, Wu WC, Liang S. Tai chi chuan.YMAA. Publication Center Roslindale, Mass; 1996.
30. Eldridge SM, Chan CL, Campbell MJ, Bond CM, Lancaster GA. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ. 2016;355:i5239.
31. Anne-Kathrin RO, Karin N, Jürgen B, et al. EULAR recommendations for physical activity in people with inflammatory arthritis and osteoarthritis. Ann Rheumatic Dis. 2018;2018–213585.
32. George A, Johanson G, Brooks P. Initial Scale Development: sample Size for Pilot Studies. Educ Psychol Meas. 2009;70:394–400.
33. Totton N, Lin J, Julious MBA A review of sample sizes for UK pilot and feasibility studies on the ISRCTN registry from 2013 to 2020. pilot and feasibility studies 2023;9.
34. Teresi J, Yu X, Stewart A, Hays R. Guidelines for Designing and Evaluating Feasibility Pilot Studies. Med Care. 2022;60:95–103. doi:10.1097/MLR.0000000000001664
35. Billingham SA, Whitehead AL, Julious SA. An audit of sample sizes for pilot and feasibility trials being undertaken in the United Kingdom registered in the United Kingdom Clinical Research Network database. BMC Med Res Method. 2013;13. doi:10.1186/1471-2288-13-13
36. Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a comparison of six methods. PAIN. 1986;27.
37. Xie F, Li S, Goeree R, et al. Validation of Chinese Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) in patients scheduled for total knee replacement. Qual Life Res. 2008;17.
38. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the Hip or knee. J Rheumatol. 1988;15:1833–1840.
39. Dunlop DD, Jing S, Semanik PA, Sharma L, Chang RW. Physical activity levels and functional performance in the osteoarthritis initiative: a graded relationship. Arthritis Rheum. 2011;63.
40. MD SS, PhD SP MPH, PhD DW, et al. Physical Performance Measures in the Clinical Setting. J Am Geriatr Soc. 2003;51.
41. Norusis M SPSS statistics 17.0. 2008.
42. Picorelli A, Pereira L, Pereira DS, Felício D, Sherrington C. Adherence to exercise programs for older people is influenced by program characteristics and personal factors: a systematic review. J Physiotherapy. 2014;60:60. doi:10.1016/j.jphys.2013.12.014
43. Yang JH, Wang YQ, Ye SQ, Cheng YG, Chen Y, Feng XZ. The Effects of Group-Based versus Individual-Based Tai Chi Training on Nonmotor Symptoms in Patients with Mild to Moderate Parkinson’s Disease: a Randomized Controlled Pilot Trial. Parkinson’s Dise. 2017;2017:8562867.
44. Kauffman AL, Ashraf JM, Corces-Zimmerman MR, Landis JN, Murphy CT. Insulin Signaling and Dietary Restriction Differentially Influence the Decline of Learning and Memory with Age. PLoS biol. 2010; 8:e1000372.
45. Thiebaud RS, Funk MD, Abe T. Home-based resistance training for older adults: a systematic review. Geriatrics Gerontol Int. 2014;14:750–757. doi:10.1111/ggi.12326
46. Liu J, Chen L, Tu Y, et al. Different exercise modalities relieve pain syndrome in patients with knee osteoarthritis and modulate the dorsolateral prefrontal cortex: a multiple mode MRI study. Brain Behav Immun. 2019;82:253–263. doi:10.1016/j.bbi.2019.08.193
47. Allen KD, Woolson S, Hoenig HM, et al. Stepped Exercise Program for Patients With Knee Osteoarthritis: a Randomized Controlled Trial. Ann Intern Med. 2021;174:298–307. doi:10.7326/M20-4447
48. Song J, Wei L, Cheng K, et al. The Effect of Modified Tai Chi Exercises on the Physical Function and Quality of Life in Elderly Women With Knee Osteoarthritis. Front Aging Neurosci. 2022;14:860762. doi:10.3389/fnagi.2022.860762
49. Marlene F, Sara M, Alison R, et al. Exercise for osteoarthritis of the knee: a Cochrane systematic review. Br J Sports Med. 2015. doi:10.1136/bjsports-2015-095424
50. Kelley GA, Kelley KS, Callahan LF. Clinical Relevance Of Tai Chi On Pain, Stiffness, And Function In Knee Osteoarthritis: a Meta-analysis: 1285. Med Sci Sports Exercise. 2022;54.
51. Kong X, Chen J, Ma C, Jiang Y, Cai Y, Gao X. Effects Of Tai Chi Exercise For Symptoms Of Knee Osteoarthritis: a Systematic Review And Meta-analysis. Med Sci Sports Exercise. 2022;467. doi:10.1249/01.mss.0000880920.13424.67
52. Bannuru RR, Abariga S, Wang C. How effective is tai chi mind-body therapy for knee osteoarthritis (KOA)? A systematic review and meta-analysis. Osteoarthritis Cartil. 2012; 20:S281–82.
53. Chen YW, Hunt MA, Campbell KL, Peill K, Reid WD. The effect of Tai Chi on four chronic conditions-cancer, osteoarthritis, heart failure and chronic obstructive pulmonary disease: a systematic review and meta-analyses. Br J Sports Med. 2016;50:397–407. doi:10.1136/bjsports-2014-094388
54. Tubach F. Evaluation of clinically relevant changes in patient reported outcomes in knee and Hip osteoarthritis: the minimal clinically important improvement. Ann Rheumatic Dis. 2005;64:29–33. doi:10.1136/ard.2004.022905
55. Bellamy N, Hochberg M, Tubach F, et al. Development of Multinational Definitions of Minimal Clinically Important Improvement and Patient Acceptable Symptomatic State in Osteoarthritis. Arthritis Care & Rese. 2015;67:972–980. doi:10.1002/acr.22538
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.