")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
How Public Service Accessibility Affects Health of Migrants: Evidence from China
Received 30 June 2024
Accepted for publication 30 November 2024
Published 10 December 2024 Volume 2024:17 Pages 3065—3084
DOI https://doi.org/10.2147/RMHP.S475634
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kubra Kaya
Jingqian Li,1 Yu Wang1,2
1School of International and Public Affairs, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 2China Institute for Urban Governance, Shanghai Jiao Tong University, Shanghai, People’s Republic of China
Correspondence: Yu Wang, Email [email protected]
Background: The effects of public service accessibility on migrant health can provide insights for local governments to optimize public service resource allocation. This study aimed to investigate the relationship between public service accessibility and the health of heterogeneous migrant populations in China, as well as the underlying mechanisms of this relationship.
Materials and Methods: Data from the 2017 China Migrants Dynamic Survey were utilized, employing ordinary least squares, instrumental variable estimation, and mediating and moderating effect analyses.
Results: Findings of the regression analysis suggest a positive association between public service accessibility and better health outcomes for migrants, particularly for less educated migrants. Mediating effect analysis revealed that both public service equalization and efficiency significantly mediate the relationship between public service accessibility and migrant health. Enhanced equalization of public services was strongly linked to improved health outcomes among less educated migrants. In contrast, improved public service efficiency significantly benefit highly educated migrants. Moderating effect analysis showed that administrative hierarchy and public service expenditure preference negatively influence the effects of public service accessibility on migrant health. This diminishing effect is more pronounced among less educated migrants in cities with higher administrative hierarchies and among highly educated migrants in cities with a higher proportion of public service expenditure.
Conclusion: This study highlights the relationship between public service accessibility and improved migrant health. Its findings suggest that optimized allocation of public service resources could enhance health equity in China’s migrant population.
Keywords: migrant population, public service accessibility, health vulnerability, health equity, urban governance
Introduction
Differences in regional economic growth and development in China have resulted in significant internal migration in recent years. According to the Seventh National Census, the number of internal migrants in China has reached 376 million, accounting for 26% of the total population.1 Moreover, the transition from a labor-intensive to a technology-intensive industrial structure has contributed to an increasing number of highly educated migrants.2 The features of internal migration in China pose a considerable challenge to health equity for migrants. On the one hand, the restrictive household registration system limits their access to social welfare, making them more vulnerable to physical and mental health risks.3 On the other hand, varying thresholds for household registration create unequal access to public services between highly educated and less educated migrants, thus exacerbating health disparities.4 In this context, improving health equity among migrants with different educational backgrounds is crucial.
Previous studies have shown that direct public services, such as healthcare and health education, and indirect public service policies, such as legal status changes that grant migrants access to public services, affect migrant health.5–7 While the impact of public services on migrant health has been widely examined, little attention has been given to how local government variations in public service provision affect migrant health. In China, local governments could set the policy adjustments based on local conditions in implementing the national policies and adopt flexible coping strategies.8 For example, while the Chinese government has encouraged easing restrictions on migrant access to public services, city-level practices differ. Some cities have broadened the scope of public services that migrants can access, while others have imposed varying restrictions based on the human capital level of migrants.9 Therefore, it is necessary to examine the differences in public service accessibility at the city level and to analyze their impact on the health of highly educated and less educated migrants.
This study investigated the relationship between public service accessibility and the health of diverse migrant groups. First, an ordinary least squares (OLS) model was used to assess the impact of public service accessibility on the health of highly educated and less educated migrants. Second, mediating analysis was used to examine the mediating effect of public service quality for migrants. Third, moderating analysis was also used to assess the moderating effects of urban administrative hierarchy and public service expenditure priorities. The findings contribute to a deeper understanding of the relationship and underlying mechanism between public service accessibility and the health of different migrant groups, offering valuable insights for policymakers and stakeholders aiming to address migrant health inequities through effective resource allocation for public services.
Literature Review
Migrant Health
Extensive research has been conducted on migrant health. Measurement of the health status of migrants mainly includes self-reported health, physical health indicators, and mental health status.10–12 Some studies report that migrants often experience worse physical and mental health outcomes, as well as the prevalence of occupational diseases and injuries.13–15 Infectious diseases, maternal healthcare, and occupational illness are considered the three primary health concerns among China’s migrant population.16 Health risks encountered during migration can significantly heighten migrants’ lifelong vulnerability to disease.17 Compared to non-migrant populations, migrants tend to experience poorer health in later life.
Additionally, migrants often endure stressful experiences that may increase their susceptibility to health problems.18 They may have overcrowded, substandard housing conditions or be employed in labor-intensive industries, which further expose them to health risks.19 Several studies have shown that poor working and living conditions, coupled with inadequate access to public services, are associated with poor health outcomes among migrants.20
Public Service Accessibility and Migrant Health
Most literature on public service accessibility for internal migrants focuses on the difficulties they experience in obtaining these services. Previous studies have found that the overall level of public service provision for migrants in China is currently low, especially among less educated migrants with limited human capital.21–23 Low access to public services has been identified as a key contributor to poor health outcomes among migrants.24 The limitations in public service accessibility lead to low utilization of preventive and treatment services by migrants, often resulting in delayed medical care or health neglect due to economic pressures.25 Furthermore, inadequate social security, such as insufficient basic health insurance coverage and workers’ compensation, worsens migrants’ vulnerability to unforeseen risks.26 Collectively, these factors contribute to the adverse health conditions prevalent among migrants. Enhancing the accessibility of public services has been shown to improve migrant health by facilitating the provision of healthcare resources, social security, and better living conditions.27–30
Overall, previous studies on public service accessibility and migrant health outcomes offer essential insights for the present study. However, most prior studies have focused on the barriers migrants face in accessing public services and the adverse health effects of these barriers. Limited attention has been paid to how improved access to public services provided by local governments could promote migrant health, especially with the household registration reforms occurring in China. Therefore, this study aimed to address this gap in the existing research by investigating the relationship between public service accessibility and migrant health improvement.
Theoretical Analysis and Research Hypotheses
Public Service Accessibility and Migrant Health
The health equity theory posits that equitable access to healthcare is fundamental for achieving equitable health outcomes, emphasizing equal access to healthcare services across diverse demographic groups.31 According to the residence permit system (RPS), local governments provide varying levels of public services to residence permit holders based on their city’s level of development and urbanization, and they may impose different restrictions. Although residence permit implementation varies across cities, the primary objective is the same: the residence permit does not change the household registration status of migrants, but it grants them some registration benefits, ensuring that they can access a relatively comprehensive range of public services.
Improved public service accessibility offers migrants broader access to healthcare resources, thus supporting their health. In particular, less educated migrants generally have fewer means and opportunities to access healthcare compared to highly educated migrants. Consequently, the impact of public service accessibility on the health of less educated migrants may be more substantial than that of highly educated migrants. Thus, this paper proposes the following hypothesis:
H1: Public service accessibility is positively associated with migrant health, with a stronger effect observed among less educated migrants compared to highly educated migrants.
Mediating Effects of Public Service Quality for Migrants
The essence of local governments providing public services to migrants is in public service resource allocation. The public choice theory suggests that, to drive regional economic growth and maximize fiscal revenue, local governments tend to selectively allocate resources to certain migrant groups. This selective provision is intended to mitigate the fiscal externalities of local public service supply stemming from migration.32 However, under the RPS, improving public service accessibility requires local governments to redistribute public resources, which contributes to enhanced quality of provided public services.33
On the one hand, increased public service accessibility allows migrants to access a wider range of public services. It narrows the disparities in service provision between migrants and registered residents. This represents an essential pathway toward equal provision of public services for migrants. On the other hand, enhanced public service accessibility allows local governments to focus on optimized allocation and efficient use of resources. Consequently, they are more proactive in adjusting resource allocations to meet service needs at the lowest possible costs. This optimized resource allocation further enhances the efficiency of providing public services.
The quality of public services provided for migrants directly affects their health. According to the health service utilization model, accessible and efficient public service delivery is crucial for improving health outcomes.34,35 First, equal access to public services allows migrants to access the same services as registered residents, thus reducing disparities due to household registration restrictions. Second, improving the efficiency of public service delivery optimizes resource allocation, enabling migrants to access better healthcare. Therefore, enhancing the quality of public services provided for migrants supports health capital accumulation, strengthens health capacities, and mitigates health risks among migrants.
Education levels also influence the extent to which migrants utilize public services. Highly educated migrants are more likely to access and use public services, so improvements in the efficiency of public service provision can make it easier for them to obtain and benefit from these services for better health outcomes. In contrast, less educated migrants, who may face greater socioeconomic pressures, often rely more on public services to meet their health needs. Improved equalization of public services broadens access for less educated migrants, allowing them to access more health services and improving their overall health.
Thus, this paper proposes the following hypotheses:
H2a: Equalizing public service provision for migrants will positively mediate the relationship between public service accessibility and migrant health, with a stronger effect observed among less educated migrants. H2b: Improving the efficiency of public service provision for migrants will positively mediate the relationship between public service accessibility and migrant health, with a stronger effect observed among highly educated migrants.
Moderating Effects of Administrative Hierarchy and Public Service Expenditure Preference
Census data and special surveys indicate that cities with lower administrative hierarchies are less attractive to migrants due to limited job opportunities and less-developed infrastructure. Consequently, most migrants concentrate in cities with higher administrative hierarchies.36 To manage the influx of migrants, cities with higher administrative hierarchies may set varying entry thresholds for residence permit holders. These thresholds often help to filter out less educated individuals who are perceived as contributing less to local economic development. Such selective approaches may significantly restrict the access of less educated migrants to urban public welfare resources.
Previous studies have shown that the level of public services in a city is pivotal factor in attracting migrants.37 Therefore, stricter household registration thresholds may be set in cities with higher proportions of public service expenditure to mitigate the potential externalities of public services and prevent migrants from over utilizing the welfare intended for registered residents. In addition, education levels influence migrants’ preference for public services in destination cities.38 Highly educated migrants are likely to be more responsive to changes in household registration thresholds and public service accessibility in these cities.
Thus, this paper proposes the following hypotheses:
H3a: Administrative hierarchy negatively moderates the relationship between public service accessibility and migrant health, especially for less educated migrants in cities with higher administrative hierarchies. H3b: Public service expenditure preference negatively moderates the relationship between public service accessibility and migrant health, especially for highly educated migrants in cities with higher proportions of expenditure on public services.
In summary, our theoretical framework is shown in Figure 1.
 |
Figure 1 Theoretical framework. |
Methods
Model Specifications
Baseline Regression Model
This study established a baseline regression model to evaluate the impact of public service accessibility on migrant health. The model is as follows:

Where  represents the migrants,
represents the migrants,  represents the cities,
represents the cities,  represents the dependent variable,
represents the dependent variable,  represents the independent variable,
represents the independent variable,  represents the control variables,
represents the control variables,  represents the error term,
represents the error term,  represents the city-level fixed effects, and
represents the city-level fixed effects, and  represents the interaction term of city-level fixed effects with individual fixed effects.
represents the interaction term of city-level fixed effects with individual fixed effects.
Mediating Effect Model
Given the limitations of the traditional three-step method for testing mediation effects, this study used the mediation model proposed by Aguinis et al39 which involves adding a regression of the mediator variable on the dependent variable.  represents the mediator variable. First,
represents the mediator variable. First,  are used as the dependent variables to examine the impact of public service accessibility on it. Second, the relationship between
are used as the dependent variables to examine the impact of public service accessibility on it. Second, the relationship between  and
and  were examined. Finally,
were examined. Finally,  and
and  were simultaneously included in the model with
were simultaneously included in the model with  as the dependent variable.
as the dependent variable.



Moderating Effect Model
The moderating effect model was constructed by incorporating interaction terms for the moderating variables into the baseline regression model. The moderating effect analysis was conducted as follows:

 represents the moderating variables. The interaction term between
represents the moderating variables. The interaction term between  and
and  was included in the regression between
was included in the regression between  and
and  . If the regression coefficient of the interaction term is significant, it indicates that the moderating variable moderates the relationship between the independent variable and dependent variable.
. If the regression coefficient of the interaction term is significant, it indicates that the moderating variable moderates the relationship between the independent variable and dependent variable.
Variables Selection
Dependent Variables
Since migrants in China are facing the threat of increasing health risks and insufficient health services, this study attempted to employ health vulnerability as a comprehensive measure of migrant health status. The concept of vulnerability originated in the field of ecology and refers to the extent to which a system is susceptible to being affected or unable to withstand harm, disruption, or threats.40 Health vulnerability is defined as the level of sensitivity and adaptive capacity exhibited by a specific population group within a defined geographic area towards external influences.29,41 Based on the definition of health vulnerability and considering the characteristics of migrants, this study posited that the health vulnerability of migrants (HVM) refers to migrant sensitivity and adaptive capacity when exposed to the working and living environments in their destination cities. The higher the HVM, the worse the health status of migrants.
Vulnerability assessments commonly employ indicator systems that highlight multiple dimensions, including risk exposure, sensitivity to stressors, and adaptive capacity.42,43 These three dimensions are widely recognized and utilized as a fundamental analytical framework in vulnerability research. Considering the characteristics of China’s migrant population and integrating the definition of vulnerability, this study measured health vulnerability among migrants through three aspects: health exposure, health sensitivity, and health adaptive capacity. An evaluation index system comprising 16 indicators was devised to evaluate the HVM, following scientific, operable, and goal-oriented principles. Table 1 provides a detailed presentation of the indicators used to measure HVM, along with the corresponding questionnaire items and scoring criteria.
 |
Table 1 Index System for Evaluating the Health Vulnerability of Migrants and the Index Weights |
The health exposure of migrants refers to their proximity to external health disturbances resulting from spatial migration.44 Migrants experience changes in their working and living environments when they move from their hometowns to destination cities, potentially affecting their health. Various aspects of migrants’ experience in their destination cities were measured in the indicator system, including occupational safety, employment status, work intensity, working hours, housing situations, healthcare conditions, and social interactions, based on items from the 2017 China Migrants Dynamic Survey (CMDS) survey. Respondent options for measurement items on occupational safety, work intensity, and working hours were assigned values based on relevant literature,45–47 while options for other measurement items were based on the questionnaire’s design.
The health sensitivity of migrants refers to their ability to withstand pressures and adapt to external disturbances or self-induced changes within their health system.48 This is measured through self-reported health, the prevalence of chronic diseases, acute illnesses, and other health issues, with response options assigned values according to the questionnaire. The health adaptive capacity of migrants refers to their ability to respond to environmental changes and make adjustments to mitigate or offset the harm to their health.49 Measurements in the indicator system were based on medical insurance, social security, health education, health records, and health services, with values assigned based on the questionnaire design.
Finally, the entropy weight method was employed to calculate the weight of each indicator, and the set pair analysis method was used to evaluate HVM. Compared with other evaluation methods, the set pair analysis combined with the entropy weight method proved effective, addressing issues of fuzziness and randomness inherent in the evaluation process and consequently enhancing the precision of evaluation outcomes.50
Initially, adhering to the principles of set pair analysis, HVM assessment transformed into a comparative examination of two sets, where Set A was the evaluation index system, and Set B was the corresponding evaluation standard. Subsequently, through the comparison of each evaluation scheme, the best and the worst schemes were determined respectively. HVM was also measured by calculating proximity to the optimal scheme. The greater the proximity, the greater the vulnerability of migrants. Detailed calculation processes are shown in Appendix A. The sample population was further divided into highly educated and less educated migrants. Following a previous study,51 highly educated migrants were defined as those whose highest education level is tertiary education or above. In contrast, less educated migrants were defined as those whose highest level of education is senior secondary education or below.
Independent Variable
The main disadvantage of migrants in China lies in the household registration system, which has marginalized migrants from accessing household registration welfare benefits as the registered permanent residents, thus hindering their equitable access to public services.52 The Chinese government has promised to accelerate reforms of the household registration system to ease migrant restrictions and improve migrant access to public services.53 The RPS is one of such initiatives to reform the household registration system. According to the RPS, migrants who have lived in their destination city for more than half a year and either have a legal and stable job or have a legal and stable residence may apply for a residence permit.54
Migrants with residence permits are assured of access to some public services.55 However, the range of services offered to residence permit holders varies between cities, typically depending on the city’s level of development and policy priorities.56 Therefore, this study examined the public service accessibility for migrants across different cities under the RPS. Specifically, public service accessibility refers to the extent to which a local government guarantees access to public services for residence permit holders.57 This study quantitatively assessed the level of public service accessibility through manual coding and analysis of policy texts from different cities. The main steps involved in this process are as follows:
First, the National Basic Public Service Standards stipulates fourteen representative public service areas ( 14) related to migrants, including (i) kindergarten education, (ii) primary education, (iii) junior or middle school education, (iv) senior or high school education, (v) secondary vocational education, (vi) occupational guidance, (vii) innovation service, (viii) vocational training, (ix) occupational skill testing, (x) child care and care services for older persons, (xi) minimum subsistence allowances, (xii) living relief, (xiii) public rental housing, and (xiv) medical and health services.58 These public service areas formed the observation system for urban public services.
14) related to migrants, including (i) kindergarten education, (ii) primary education, (iii) junior or middle school education, (iv) senior or high school education, (v) secondary vocational education, (vi) occupational guidance, (vii) innovation service, (viii) vocational training, (ix) occupational skill testing, (x) child care and care services for older persons, (xi) minimum subsistence allowances, (xii) living relief, (xiii) public rental housing, and (xiv) medical and health services.58 These public service areas formed the observation system for urban public services.
Second, the policy texts of the RPS in various cities were examined to determine whether each representative public service area had been guaranteed. If a public service area had been promised to residence permit holders, then  1; otherwise,
1; otherwise,  0.
0.
Third, public service areas that received a larger share of per capita fiscal expenditure indicated relative preferences of local governments.59 This study used the share of fiscal expenditures allocated to the 14 representative public service areas as weights  . These weights reflected the variations in preferences among different city governments for the 14 representative public services.
. These weights reflected the variations in preferences among different city governments for the 14 representative public services.
Finally, the accessibility of public services promised by the RPS in city  was calculated as follows:
was calculated as follows:  .
.
Mediating Variables
(1) Evaluation of the Efficiency of Public Service Provision for Migrants
The efficiency of public service provision for migrants refers to the optimal allocation and utilization of various types of public service resources by local governments, ensuring effective distribution across different groups and service areas to meet people’s basic needs.60 An indicator system encompassing compulsory education, healthcare, and social security for migrants was devised to gauge the efficiency of public services. To address the limitations of the traditional data envelopment analysis (DEA) model in measuring the efficiency of individual decision-making units (DMUs), the super-efficiency of the DEA model using directional distance functions was employed.61 This advanced approach provided a more nuanced measurement by allowing efficiency scores greater than one, which helped in distinguishing the performance of highly efficient units. By incorporating directional distance functions, the model could better account for the direction in which improvements are sought, whether in reducing inputs or increasing outputs.
The input indicators included per capita expenditure on education, healthcare, and social security for the resident population.62,63 In comparison, the output indicators included the number of students and teachers in primary and secondary schools, the number of doctors and hospital beds, and the number of participants in both pension and medical insurance (Appendix B).64,65
The main steps of the efficiency evaluation were as follows: The efficiency evaluation system was assumed to have had  decision-making units (DMUs), where each DMU had input and output vectors,
decision-making units (DMUs), where each DMU had input and output vectors,  and
and  , respectively, with
, respectively, with  and
and  . Based on the input and output data, assuming
. Based on the input and output data, assuming  > 0 and
> 0 and  > 0, the production possibility set represented all combinations of outputs generated by
> 0, the production possibility set represented all combinations of outputs generated by  factor inputs
factor inputs  . If DMU0 was evaluated as slack-based measure efficient, meaning
. If DMU0 was evaluated as slack-based measure efficient, meaning  , its super-efficiency was defined as:
, its super-efficiency was defined as:




Where  and
and  respectively represented the input- and output-slacks of the
respectively represented the input- and output-slacks of the  DMU, while
DMU, while  represented the weighted vector, and the optimal solution of the objective function
represented the weighted vector, and the optimal solution of the objective function  defined the efficiency value of the evaluated DMU0.
defined the efficiency value of the evaluated DMU0.
(2) Evaluation of the Equalization of Public Service Provision for Migrants
This study defined the equalization of public services for migrants as ensuring that migrants have equitable access to public services compared to the registered household population.66 An indicator system including compulsory education, social security, and health care was developed to measure this equalization (Appendix C). The A-F multidimensional analysis method was employed for evaluation.67 First, a matrix of public service access was constructed based on various indicators to ascertain migrants’ access status across different domains. Subsequently, the proportion of public service access for migrants was calculated, and entropy weighting was applied to assign weights to each indicator. Next, migrants’ access status to public services was determined based on the critical value of access share. Following that, the proportion of migrants in the city who have obtained multidimensional public services was calculated to denote the breadth of public service coverage, and the weighted sum of the average share of public service acquisition for each migrant with multidimensional public services was calculated to denote the depth of public service acquisition. Finally, the public service equalization index was calculated as the product of the breadth and depth of public service coverage (Appendix D).
Moderating Variables
This study adopted city administrative hierarchies and the proportion of public service expenditure as moderating variables. First, city samples were classified into three hierarchical levels—prefecture-level cities, provincial capital cities, and direct-controlled municipalities—assigned values from 1 to 3 in ascending order. Second, the proportion of public service expenditure was calculated as the combined spending on education, healthcare, and social security as a percentage of total fiscal expenditure.
Control Variables
Additional control variables were incorporated, drawing from existing research on factors affecting migrant health, to determine the net impact of public service accessibility on migrant health.68 The first aspect involved personal characteristics. Gender was identified as a dummy variable, with “male” coded as 1. Age was the actual age of the respondents. Household registration type was a dummy variable, with “agricultural household registration” coded as 0 and “non-agricultural household registration” as 1. Marital status was also a dummy variable, with “unmarried” coded as 0. Migration time indicated the number of years the respondents had spent in their current destination city. Migration scope was categorized into “Trans-county”, “Trans-city”, and “Trans-province”. The number of migrations referred to the total number of times the respondents had migrated.
The second aspect involved family characteristics. Family income was the respondents’ annual family income from the previous year. The family consumption-to-income ratio measured family consumption relative to income for the last year. The number of family members referred to the size of the respondents’ household. The third aspect focused on city characteristics. The number of resident populations was the log of the number of permanent residents in the destination city. The average wage was the log of the average salary of workers in the destination city, and the unemployment rate was the unemployment level in the destination city. The descriptive statistics of the variables are displayed in Table 2.
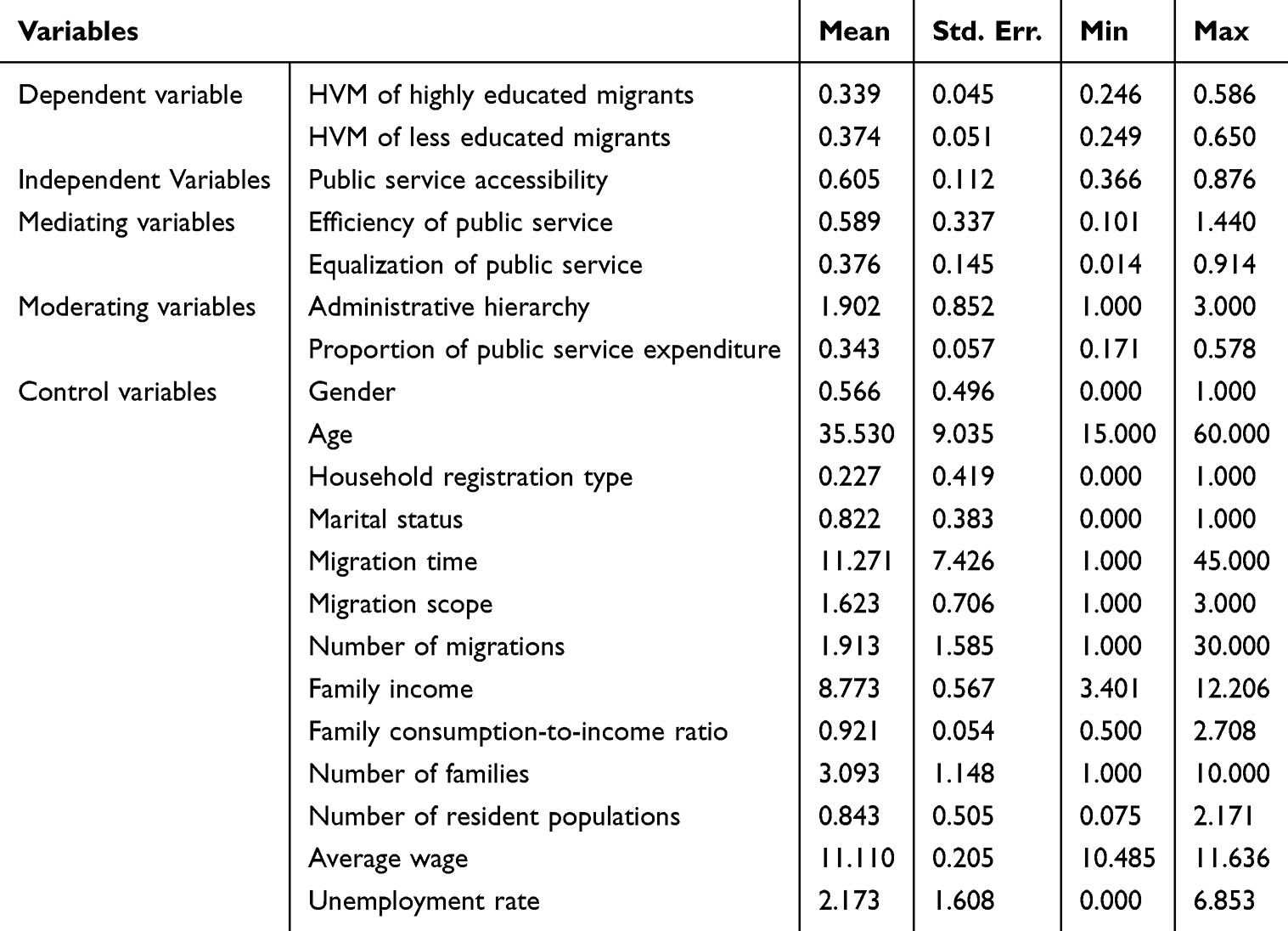 |
Table 2 Descriptive Statistics of Variables (N = 72, 696) |
Data Resources
This study used data from the 2017 CMDS, a nationally representative survey conducted by the National Health and Family Planning Commission Department of China. The CMDS includes 32 provincial units in China and surveys migrants over 15 years of age who have resided in migrant-receiving cities for more than one month. Based on the Probability Proportional to Size sampling method, the survey includes approximately 170,000 samples selected based on the following criteria: (i) lack of local household registration; (ii) current employment status; (iii) possession of a local residence permit; and (iv) no missing values. Macro-level data at city levels were obtained from the China Statistical Yearbook, the China City Statistical Yearbook, and the National Economic and Social Development Statistical Bulletin. The macro-level variables were lagged by one year to reduce endogeneity bias.
Empirical Studies
Baseline Results
Tests were conducted for multicollinearity, heteroscedasticity, and autocorrelation of the variables before baseline regression. The results for all tests met statistical quality control standards. Table 3 illustrates the estimation results of the OLS model, which assesses the impact of public service accessibility on HVM. To control the influence of both urban and individual factors, both city and city-birth fixed effects were applied.
 |
Table 3 The Estimates of Public Service Accessibility and Migrants’ Health |
Table 3 indicate that, after controlling for multiple variables, public service accessibility is significantly and negatively associated with HVM. Specifically, the impact of public service accessibility on less educated migrants was more significant compared to highly educated migrants. This discrepancy may be due to disparities in educational backgrounds, leading to variations in health awareness. Highly educated migrants are more likely to prioritize their health and may be less dependent on public services; instead, they are more likely to promptly address health concerns through regular check-ups, timely medical care, and online consultations. Conversely, less educated migrants tend to have limited health awareness and limited economic and social support, making them more affected by limited access to public services in receiving cities. These findings support Hypothesis 1.
Endogeneity Analysis
The two-stage least squares (2SLS) instrumental variable (IV) method was employed to address potential endogeneity issues. The selected instrumental variable was the 1990 per capita grain output of the migrant cities, selected based on the key criteria of relevance and exogeneity.
First, the 1990 per capita grain output is relevant to the public services accessibility of migrants. In China, during the planned economy era, the Grain and Oil Migration Permit System tied the household registration system to grain supply, making total grain production a crucial factor in determining a city’s population-carrying capacity and migration policies.69 Existing studies confirm that planned migration to Chinese cities between 1952 and 1998 was correlated significantly and positively with prior year’s per capita grain output.70 Although the impact of historical grain output diminishes over time, it still partially shapes current policies on public service accessibility for migrants.
Second, the exogeneity of the 1990 per capita grain output is justified, as it is unlikely to directly affect current migrants. The health status of recent migrants is not significantly correlated with historical grain production in their destination cities. Additionally, the 1990 grain output reflects exogenous factors, such as geography and climate, which do not directly impact the recent health outcomes of migrants, thereby supporting the strong exogeneity of this variable.
Table 4 shows the regression results of the estimation of the 2SLS estimation. In the first-stage regression, the coefficient of the 1990 per capita grain output was significantly negative, suggesting that cities with higher grain output in 1990 currently have lower public service accessibility to public services, which is in line with theoretical expectations. The F-statistic also exceeded 10, ruling out weak instrument concerns.71 In the second stage, results showed that higher public service accessibility was associated with reduced HVM, consistent with the baseline regression findings. Based on the Durbin-Wu-Hausman test results, the null hypothesis is rejected at the 1% significance level, suggesting endogeneity in the explanatory variables and supporting the necessity and appropriateness of employing instrumental variable estimation in this study.
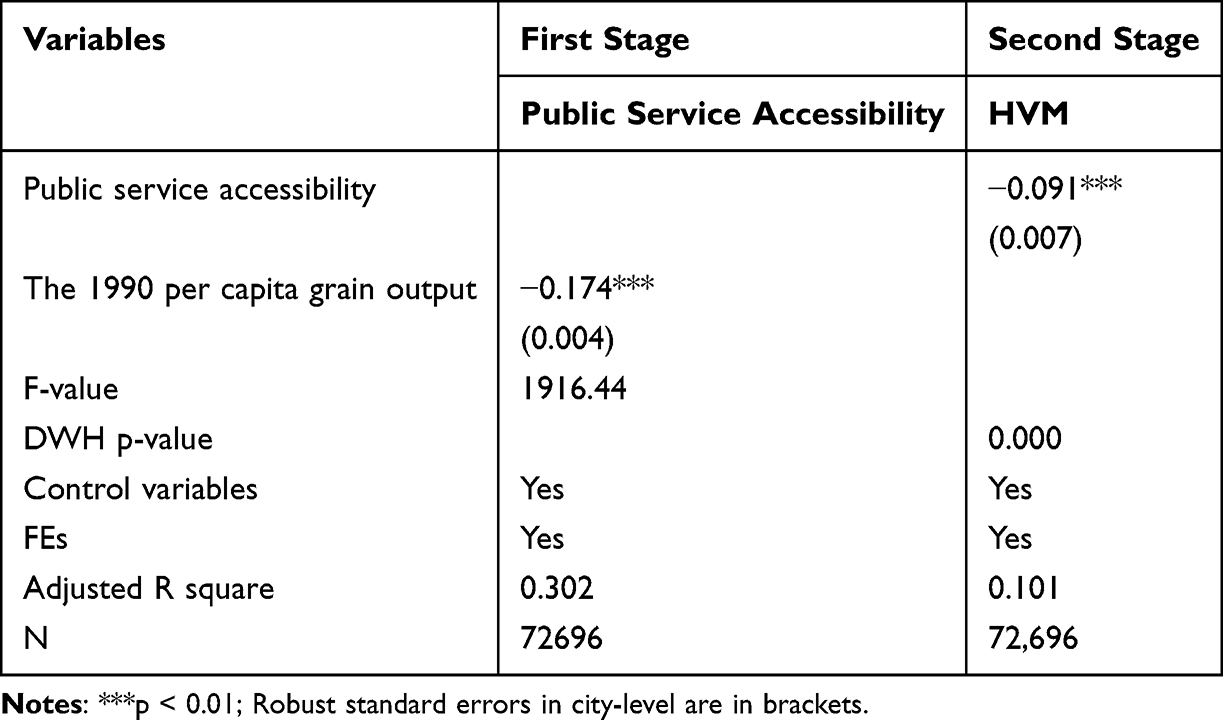 |
Table 4 Endogeneity Analysis |
Robustness Check
Construction of an Alternative Dependent Variable
An alternative measure of migrant health was constructed to further validate the findings. Specifically, respondents in the 2017 CMDS were asked to rate their current health status on a four-point Likert scale, ranging from 1 (very healthy) to 4 (very unhealthy). This self-reported health status served as a comprehensive measure, encompassing aspects of physical health, mental health, illness prevalence, and respondents’ overall satisfaction with their health status.72 Table 5 shows significant negative effects of public service accessibility on migrant health identical to those reported in Table 3, confirming the robustness of the baseline results.
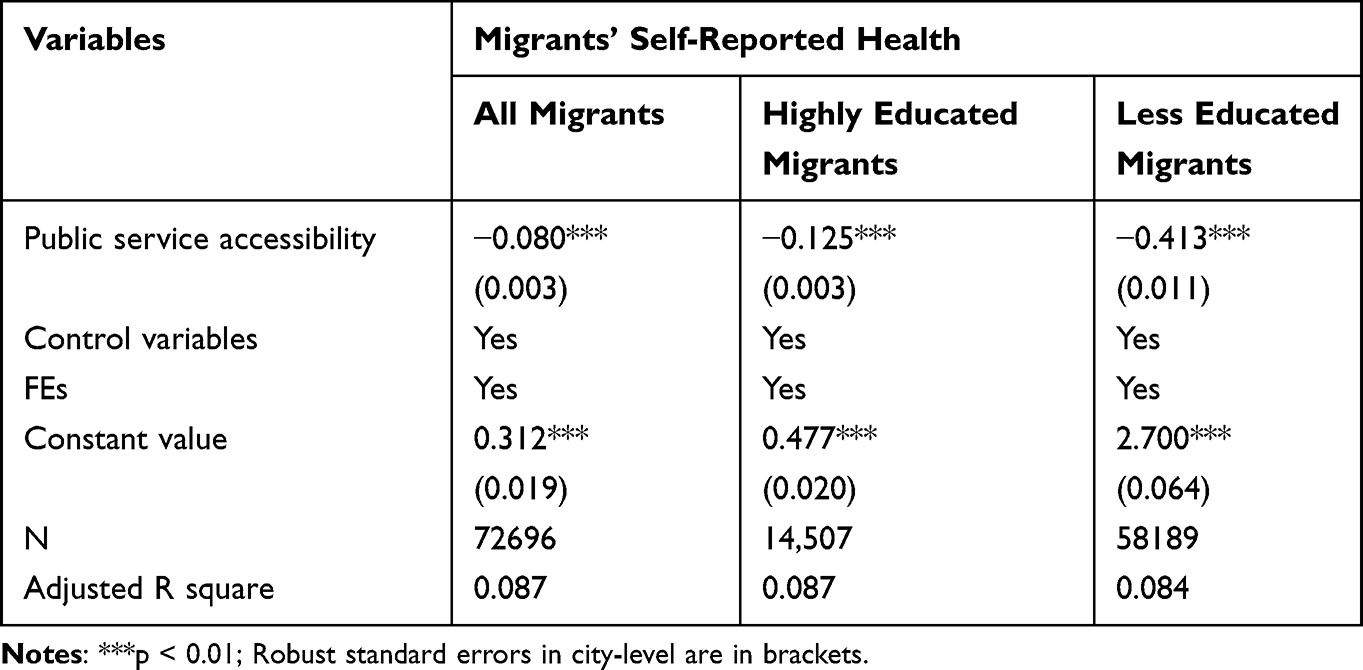 |
Table 5 Robustness Checks: Construction of an Alternative Dependent Variable |
Use of Restricted Samples
To test the robustness of the results further, a narrower sample was analyzed by restricting it to migrants who had lived in the receiving city for over three and five years. Using samples with similar migration durations could mitigate potential omitted variable bias resulting from unobserved heterogeneity.73 Table 6 suggests significant negative effects of public service accessibility on migrant health, confirming the baseline results.
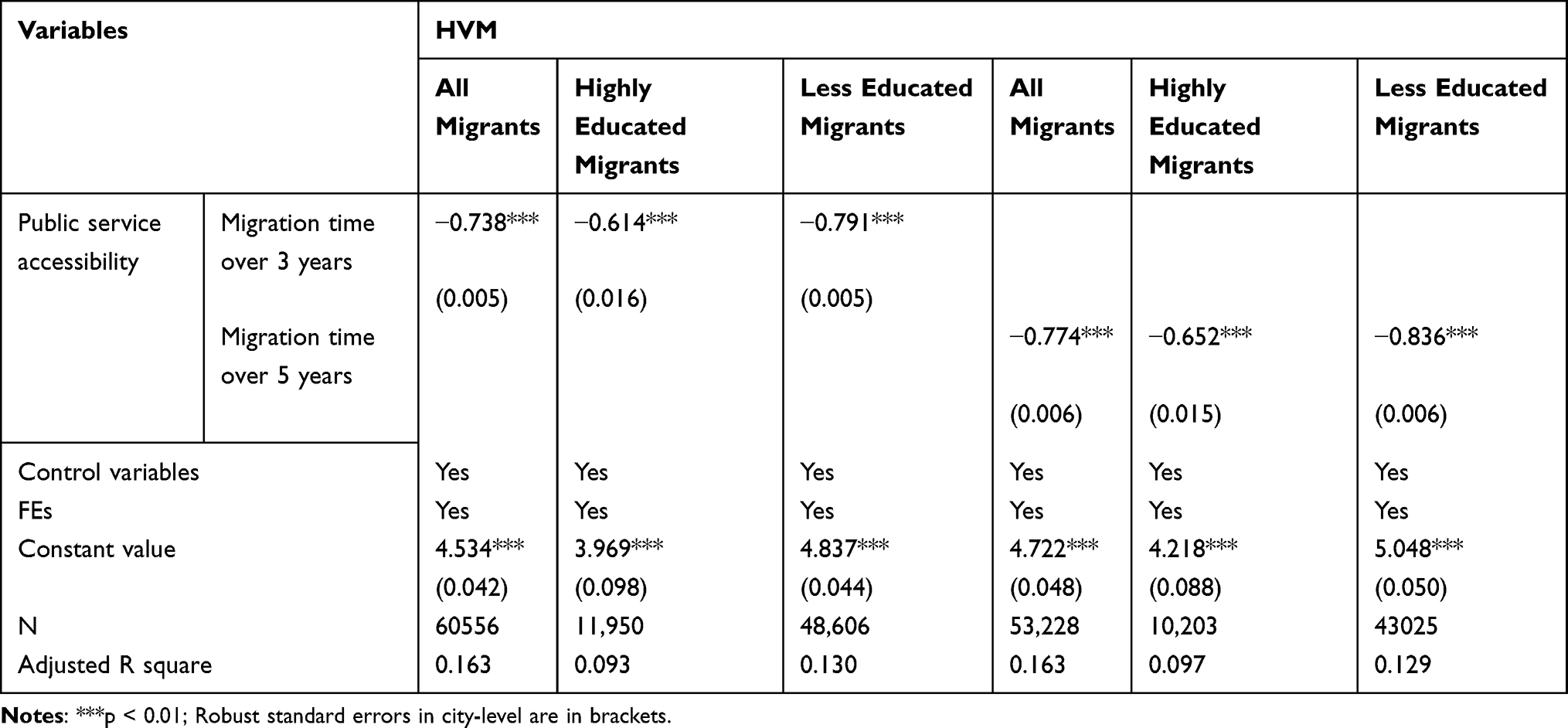 |
Table 6 Robustness Checks: Use of Restricted Samples |
Mediating Effect Analysis
Mediating Effect of the Equalization of Public Service for Migrants
The regression results in column (1) of Table 7 indicate a significant positive correlation between public service accessibility and the public service provision equalization. This suggests that higher levels of public service accessibility are associated with greater inclusion of migrants in urban public service coverage and receiving more public services. The regression results in columns (2), (4), and (6) demonstrate a significant correlation between public service equalization and the reduction in HVM. Greater public service equalization corresponds with more equitable access to health services for migrants, potentially reducing HVM. Notably, the relationship between improved public service equalization and reduced HVM is more pronounced among less educated migrants, implying that enhancing service equalization can lead to higher inclusion of this group in public service coverage and more substantial health improvements.
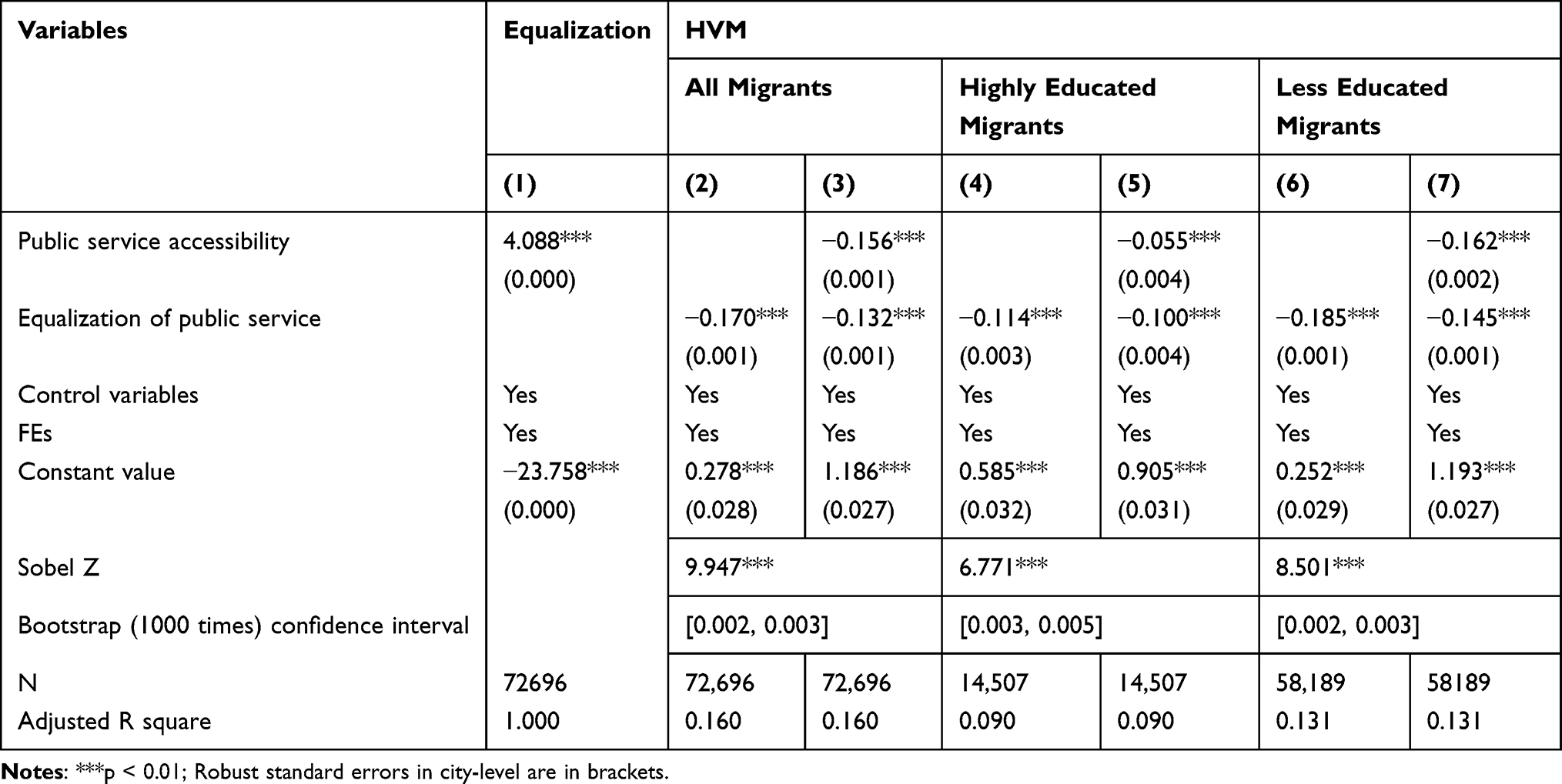 |
Table 7 Mediating Effect Test Results of the Equalization of Public Service |
The regression results in columns (3), (5), and (7) show that, after simultaneously including both public service accessibility and public service equalization variables, the coefficient of the public service accessibility remains significant at the 1% confidence level, and slightly lower compared to the coefficient in the baseline regression. This suggests that public service equalization has partial mediation effects. Both the Sobel and Bootstrap tests further validate this mediation effect. These findings support Hypothesis 2a.
Mediating Effect of the Efficiency of Public Service Provision for Migrants
The regression results in column (1) of Table 8 show a significant positive correlation between public service accessibility and the public service provision efficiency. This suggests that as public service accessibility increases, local governments tend to allocate and utilize public service resources more effectively. The regression results in columns (2), (4), and (6) indicate a significant decrease in the HVM associated with improved efficiency in public service provision. More efficient provision of public services leads to a more effective allocation of health resources for migrants, resulting in greater health capital and reduced health risks, thereby lowering their HVM. Specifically, improvements in public service provision efficiency show a stronger correlation with reduced HVM among highly educated migrants, indicating that they utilize health investments more effectively and make greater use of public service provision to enhance their health.
 |
Table 8 Mediating Effect Test Results of the Efficiency of Public Service |
The regression results in columns (3), (5), and (7) show that, after simultaneously including both the public service accessibility and public service provision efficiency variables, the coefficient of the public service accessibility remains significant at the 1% confidence level, and slightly lower compared to the coefficient in the baseline regression. This suggests that public service equalization has partial mediating effects. Both the Sobel and Bootstrap tests further validate this mediation effect. These findings support Hypothesis 2b.
Moderating Effect Analysis
Moderating Effect of Administrative Hierarchy
The results in columns (1), (2), and (3) of Table 9 indicate a significantly positive coefficient for the interaction term between administrative hierarchy and public service accessibility. Meanwhile, the regression coefficient for administrative hierarchy exhibits a significantly negative effect. These findings suggest a substitution relationship between administrative hierarchy and public service accessibility in reducing the HVM. In other words, the higher the administrative hierarchy of a city, the less impact public service accessibility has on reducing HVM.
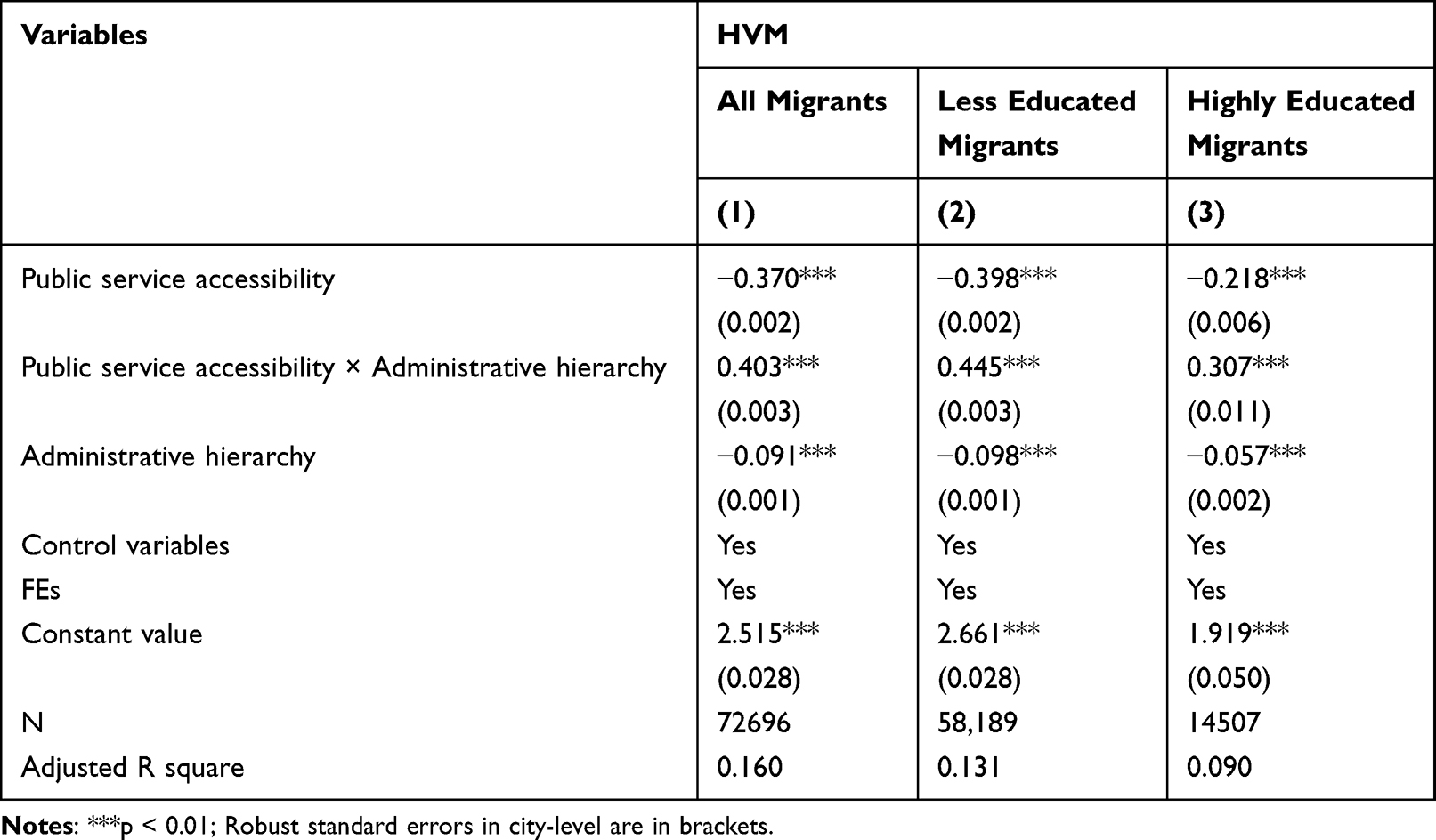 |
Table 9 Moderating Effect Test Results of the Administrative Hierarchy |
By comparing the interaction coefficients of less educated and highly educated migrants, it becomes evident that the impact of public service accessibility on HVM among less educated migrants is more significantly moderated by administrative hierarchy. These findings support Hypothesis 3a. These findings may reflect cities with higher administrative hierarchies tend to create restrictions regulating population influx, thereby preventing excessive migration that could pose challenges to urban management. These restrictions reduce the opportunities for certain migrant groups to benefit from public services, consequently weakening the positive impact of public service accessibility on their health. This effect is particularly pronounced among less educated migrants, who are often perceived as contributing less to the development of the destination city and are therefore subject to greater restrictions.
Moderating Effect of Public Service Expenditure Preference
The results in columns (1), (2), and (3) of Table 10 indicate a significantly positive coefficient for the interaction term between public service expenditure preference and public service accessibility. Meanwhile, the regression coefficient of public service expenditure preference is significantly negative. These findings suggest a substitution relationship between public service expenditure preference and public service accessibility in reducing HVM. In other words, the higher the proportions of expenditure on public services in a city, the less impact public service accessibility has on reducing HVM.
 |
Table 10 Moderating Effect Test Results of the Public Service Expenditure Preference |
By comparing the interaction coefficients of less educated and highly educated migrants, it becomes evident that the impact on HVM among highly educated migrants is more significantly moderated by public service expenditure preference. These findings support Hypothesis 3b. These findings may reflect cities with higher proportions of expenditure on public services, economic strength is often greater, which makes these cities more attractive to migrants. Local governments, aiming to control population size and development costs, tend to limit access to public services for migrants by strengthening the selective function of the household registration system. These policies are designed to prevent an excessive influx of migrants from burdening urban development. Consequently, despite higher public service spending, restrictive access limits migrants’ opportunities to benefit, weakening the positive impact of public service accessibility on their health improvement. This effect is especially noticeable among highly educated migrants who have a stronger preference for public services in their destination cities.
Discussion
Utilizing data from the 2017 CMDS, this study employed various statistical methods, including OLS, IV, and mediating and moderating effect analyses, to investigate the relationship between public service accessibility and HVM. The study has three main findings.
First, a negative correlation was observed between public service accessibility and HVM. This finding aligns with previous studies indicating that improved access to public services positively impacts migrant health.74 Furthermore, the impact of public service accessibility on less educated migrants is more pronounced compared to that on highly educated migrants. This is consistent with a previous report in China, which states that government-led development policies tend to affect less educated migrants more significantly.75 This may be due to the fact that less educated migrants are often in socioeconomically disadvantaged environments with limited health literacy, making their demand for public services more pressing.
Second, both the efficiency and equalization of public service provision for migrants mediate the relationship between public service accessibility and HVM. Specifically, improvements in public service equalization show a stronger correlation with reducing HVM among less educated migrants. In contrast, the more efficient public service delivery was strongly associated with reducing HVM among highly educated migrants. The findings of the present study support the insights of Pu, who emphasized that the distribution of public resources by local governments must be guided to achieve fairness and effectiveness, thereby maximizing health benefits across different populations.76
Third, this study’s findings indicate that administrative hierarchy and public service expenditure preference negatively moderate the association between public service accessibility and HVM. Specifically, the administrative hierarchy significantly diminishes the effect of public service accessibility on improving the health of less educated migrants in cities with higher administrative hierarchies. Similarly, the public service expenditure preference significantly diminishes the effect of public service accessibility on improving the health of highly migrants in cities with higher proportions of expenditure on public services. This reflects the tension between exclusivity and equity in resource allocation for migrants. Cities with higher administrative levels and higher public service expenditure often adopt selective policies to balance developmental demands with public welfare. While these policies aim to reduce the strain that migrants place on local resources, they inadvertently result in inequitable distribution of public services. This finding indicates that household registration threshold restrictions contribute to varying degrees of discrimination experienced by migrants in accessing public welfare, regardless of their education levels. As noted by Xu et al, the positive impact of residence permits was limited when compared with the health inequality faced by migrants.55 There are still structural defects in the RPS that need to be addressed and further improved.
Conclusion
Compared with previous studies, the contributions of the present study are significant. Its findings emphasize the importance of considering the specific needs of different migrant groups in public service resource allocation strategies. The diversity among migrants implies variations in their public service needs and health conditions. It is the responsibility of local governments to ensure the effective distribution of public service resources across different projects and groups of people, thereby maximizing the value of public service.
This study also revealed a contradiction between the intended direction of household registration system reforms and the practical orientation of development-oriented local governments. As a selective mechanism for local governments to allocate public resources, the household registration threshold focuses on optimizing population structure and promoting urban development rather than reducing health disparities. This highlights a fundamental tension between social welfare objectives and economic development goals within the migration policy. Considering these findings, improving the current RPS and optimizing public service resource allocation should be key strategies for China to promote health equity in the future.
Finally, this study had certain limitations. Due to data constraints, our analysis relied solely on the 2017 CMDS data, which does not fully capture the dynamic nature of how public service accessibility affects migrant health. In the future, the authors aim to explore additional data and methods to investigate the dynamic attributes and underlying mechanisms concerning the interplay between public service accessibility and migrant health.
Abbreviations
CMDS, China Migrants Dynamic Survey; DEA, Data Envelopment Analysis; DMU, Decision-Making Unit; HVM, Health Vulnerability of Migrants; IV, Instrumental Variable; OLS, Ordinary Least Squares; RPS, Residence Permit System; 2SLS, Two-Stage Least Squares.
Ethics Approval
The data used in this study were sourced from the publicly available China Migrants Dynamic Survey (CMDS), sponsored by the Migrant Population Service Center of the National Health Commission of the People’s Republic of China. All data are fully anonymized, ensuring that no information can directly or indirectly identify individuals. During the data collection process, participants were explicitly informed about the study’s purpose, social value, and the scope of data collection. Potential privacy risks were thoroughly assessed and mitigated, and all participants provided informed consent, ensuring compliance with ethical standards. All procedures adhered to the principles of the 1964 helsinki Declaration, as well as its subsequent amendments or comparable ethical standards.
This study exclusively utilized de-identified secondary data, containing no information that could directly or indirectly identify individuals. It did not involve physical harm, sensitive personal information, or commercial interests. Furthermore, the study posed no ethical risks or challenges related to life and health, the ecological environment, public order, or sustainable development. This research complies with the ethical exemption criteria outlined in the Ethical Review Measures for Life Sciences and Medical Research Involving Humans, promulgated by the relevant authorities in China. Relevant document can be accessed through the website https://www.gov.cn/zhengce/zhengceku/2023-02/28/content_5743658.htm.
Acknowledgment
The authors sincerely acknowledge the financial support from the National Social Science Foundation of China. The authors also acknowledge the datasets support from the China Migrants Dynamic Survey (CMDS), and the current research follows the CMDS data access policies and publication guidelines.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the National Social Science Foundation of China (21BGL254).
Disclosure
The authors report no conflicts of interest in this work.
References
1. National Bureau of Statistics of China. Bulletin of the Seventh National Population Census (No. 7); 2021. Available from: https://www.stats.gov.cn/sj/tjgb/rkpcgb/qgrkpcgb/202302/t20230206_1902007.html.
2. Gu H, Meng X, Shen T, et al. China’s highly educated talents in 2015: patterns, determinants and spatial spillover effects. Appl Spat Anal Policy. 2020;13:631–648. doi:10.1007/s12061-019-09322-6
3. Hou B, Nazroo J, Banks J, et al. Impacts of migration on health and well-being in later life in China: evidence from the China health and retirement longitudinal study (CHARLS). Health Place. 2019;58:102073. doi:10.1016/j.healthplace.2019.01.003
4. Fu M, Liu C, Yang M. Effects of public health policies on the health status and medical service utilization of Chinese internal migrants. China Econ Rev. 2020;62:101464. doi:10.1016/j.chieco.2020.101464
5. Perreira KM, Pedroza JM. Policies of exclusion: implications for the health of immigrants and their children. Annu Rev Public Health. 2019;40:147–166. doi:10.1146/annurev-publhealth-040218-044115
6. Kim M, Gu H. Relationships between health education, health behaviors, and health status among migrants in China: a cross-sectional study based on the China migrant dynamic survey. Healthcare. 2023;11(12):1768. doi:10.3390/healthcare11121768
7. Martinez O, Wu E, Sandfort T, et al. Evaluating the impact of immigration policies on health status among undocumented immigrants: a systematic review. J Immigr Minor Health. 2015;17(3):947–970. doi:10.1007/s10903-013-9968-4
8. Wang Y, Zhao Y. Is collaborative governance effective for air pollution prevention? A case study on the Yangtze river delta region of China. J Environ Manage. 2021;292:112709. doi:10.1016/j.jenvman.2021.112709
9. Peng X. Development-orientated governments and the threshold of household registration: reflection on the household registration system reform. In: Household Registration System Reform in China’s Megacities. Singapore: Springer Nature Singapore; 2023:177–205.
10. Tong Y, Piotrowski M. Migration and health selectivity in the context of internal migration in China, 1997–2009. Popul Res Policy Rev. 2012;31(4):497–543. doi:10.1007/s11113-012-9240-y
11. Wallace SP, Young MEDT, Rodríguez MA, et al. A social determinants framework identifying state-level immigrant policies and their influence on health. SSM Popul Health. 2019;7:100316. doi:10.1016/j.ssmph.2018.10.016
12. Held ML, First JM, Huslage M, et al. Policy stress and social support: mental health impacts for Latinx Adults in the Southeast United States. Soc Sci Med. 2022;307:115172. doi:10.1016/j.socscimed.2022.115172
13. Ruhnke SA, Reynolds MM, Wilson FA, et al. A healthy migrant effect? Estimating health outcomes of the undocumented immigrant population in the United States using machine learning. Soc Sci Med. 2022;307:115177. doi:10.1016/j.socscimed.2022.115177
14. Lecerof SS, Stafström M, Westerling R, et al. Does social capital protect mental health among migrants in Sweden? Health Promot Int. 2016;31:644–652. doi:10.1093/heapro/dav048
15. Xia QH, Jiang Y, Yin N, et al. Injury among migrant workers in Changning district, Shanghai, China. Int J Inj Control Saf Promot. 2012;19:81–85. doi:10.1080/17457300.2011.603151
16. Hu X, Cook S, Salazar MA. Internal migration and health in China. Lancet. 2008;372(9651):1717–1719. doi:10.1016/S0140-6736(08)61360-4
17. Kristiansen M, Razum O, Tezcan-Güntekin H, et al. Aging and health among migrants in a European perspective. Public Health Rev. 2016;37:1–14. doi:10.1186/s40985-016-0036-1
18. Shao C, Meng X, Cui S, et al. Income-related health inequality of migrant workers in China and its decomposition: an analysis based on the 2012 China labor-force dynamics survey data. J Chin Med Assoc. 2016;79:531–537. doi:10.1016/j.jcma.2016.02.009
19. Wang Y, Hu J, Lin W, et al. Health risk assessment of migrant workers’ exposure to polychlorinated biphenyls in air and dust in an e-waste recycling area in China: indication for a new wealth gap in environmental rights. Environ Int. 2016;87:33–41. doi:10.1016/j.envint.2015.11.009
20. Song Y, Sun W. Health consequences of rural‐to‐urban migration: evidence from panel data in China. Health Econ. 2016;25(10):1252–1267. doi:10.1002/hec.3212
21. Meng X. Does a different household registration affect migrants’ access to basic public health services in China? Int J Environ Res Public Health. 2019;16(23):4615. doi:10.3390/ijerph16234615
22. Hou HL. The difference of urban public service supply and its influence on population movement. Chin J Popul Sci. 2016;01:118–125. Chinese.
23. Liu S, Cai Q, Wang M, et al. Urban public services and fertility intentions of internal migrants in China. PLoS One. 2024;19(3):e0300345. doi:10.1371/journal.pone.0300345
24. Long C, Tang S, Wang R, et al. The migrating mediators and the interaction associated with the use of essential public health services: a cross-sectional study in Chinese older migrants. BMC Geriatr. 2020;20:1–10. doi:10.1186/s12877-020-01878-0
25. Li D, Yamada M, Gao D, et al. Spatial variations in health service utilization among migrant population: a perspective on health equity. Front Public Health. 2024;12:1447723. doi:10.3389/fpubh.2024.1447723
26. Avato J, Koettl J, Sabates-Wheeler R. Social security regimes, global estimates, and good practices: the status of social protection for international migrants. World Dev. 2010;38(4):455–466. doi:10.1016/j.worlddev.2009.10.003
27. Zhao Q, Song M, Wang H. Voting with your feet: the impact of urban public health service accessibility on the permanent migration intentions of rural migrants in China. Int J Environ Res Public Health. 2022;19(22):14624. doi:10.3390/ijerph192214624
28. Nielsen SS, Hempler NF, Waldorff FB, et al. Is there equity in use of healthcare services among immigrants, their descendents, and ethnic Danes? Scand J Public Health. 2012;40(3):260–270. doi:10.1177/1403494812443602
29. Fang H, Jin Y, Zhao M, et al. Does migration limit the effect of health insurance on hypertension management in China? Int J Environ Res Public Health. 2017;14(10):1256. doi:10.3390/ijerph14101256
30. EuroHealthNet. Migrant inequalities in urban settings and changing public health practice. Eur J Public Health. 2019;29(Suppl 4):ckz183–004.
31. Rosa Dias P, Jones AM. Giving equality of opportunity a fair innings. Health Econ. 2007;16(2):109–112. doi:10.1002/hec.1207
32. Mueller DC. Public Choice. Cambridge University Press; 2003.
33. Ahlers AL, Heberer T, Schubert G. Whither local governance in contemporary China? Reconfiguration for more effective policy implementation. J Chin Governance. 2016;1(1):55–77. doi:10.1080/23812346.2016.1138700
34. Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? J Health Soc Behav. 1995;36:1–10. doi:10.2307/2137284
35. Bell E, Christensen J, Herd P, et al. Health in citizen-state interactions: how physical and mental health problems shape experiences of administrative burden and reduce take-up. Public Adm Rev. 2023;83(2):385–400. doi:10.1111/puar.13568
36. Wei H. The administrative hierarchy and growth of urban scale in China. Chin J Urban Environ Stud. 2015;3(01):1550001. doi:10.1142/S2345748115500013
37. Dahlberg M, Eklöf M, Fredriksson P, et al. Estimating preferences for local public services using migration data. Urban Stud. 2012;49(2):319–336. doi:10.1177/0042098011400769
38. He W. Educational Differences, Public service provision and labor settlement intention. Econ Sci. 2020;4:84–96. Chinese.
39. Aguinis H, Edwards JR, Bradley KJ. Improving our understanding of moderation and mediation in strategic management research. Organ Res Methods. 2017;20(4):665–685. doi:10.1177/1094428115627498
40. Janssen MA, Schoon ML, Ke W, et al. Scholarly networks on resilience, vulnerability and adaptation within the human dimensions of global environmental change. Glob Environ Change. 2006;16(3):240–252. doi:10.1016/j.gloenvcha.2006.04.001
41. Eriksson M, Ng N. Changes in access to structural social capital and its influence on self-rated health over time for middle-aged men and women: a longitudinal study from northern Sweden. Soc Sci Med. 2015;130:250–258. doi:10.1016/j.socscimed.2015.02.029
42. Adger WN. Vulnerability. Glob Environ Change. 2006;16(3):268–281. doi:10.1016/j.gloenvcha.2006.02.006
43. Polsky C, Neff R, Yarnal B. Building comparable global change vulnerability assessments: the vulnerability scoping diagram. Glob Environ Change. 2007;17(3–4):472–485. doi:10.1016/j.gloenvcha.2007.01.005
44. McCarthy JJ, Canziani OF, Leary NA. Climate Change 2001: Impacts, Adaptation and Vulnerability. Cambridge: Cambridge University Press; 2001.
45. Viscusi WK. The value of life: estimates with risks by occupation and industry. Econ Inq. 2004;42(1):29–48. doi:10.1093/ei/cbh042
46. Huang Z, Cheng X. Environmental regulation and rural migrant workers’ job quality: evidence from China migrants dynamic surveys. Econ Anal Policy. 2023;8:845–858. doi:10.1016/j.eap.2023.04.034
47. Nie P, Otterbach S, Sousa-Poza A. Long work hours and health in China. China Econ Rev. 2015;33:212–229. doi:10.1016/j.chieco.2015.02.004
48. Füssel HM. Vulnerability: a generally applicable conceptual framework for climate change research. Global Environ Change. 2007;17(2):155–167. doi:10.1016/j.gloenvcha.2006.05.002
49. Turner B, Kasperson RE, Matson PA, et al. A framework for vulnerability analysis in sustainability science. Proc Natl Acad Sci. 2003;100(14):8074–8079. doi:10.1073/pnas.1231335100
50. Zhao KQ. The application of SPA-based identical-discrepancy-contrary system theory in artificial intelligence research. CAAI Trans Intell Syst. 2007;2(5):21–35.
51. Gu H, Shen T. Modelling skilled and less‐skilled internal migrations in China, 2010–2015: application of an eigenvector spatial filtering hurdle gravity approach. Popul Space Place. 2021;27(6):e2439. doi:10.1002/psp.2439
52. Wu J, Yu Z, Wei YD, et al. Changing distribution of migrants and its influencing factors in urban China: economic transition, public policy, and amenities. Habitat Int. 2019;94:102063. doi:10.1016/j.habitatint.2019.102063
53. Sun M, Fan CC. China’s permanent and temporary migrants: differentials and changes, 1990–2000. Prof Geogr. 2011;63(1):92–112. doi:10.1080/00330124.2010.533562
54. China State Council. Provisional Regulation on Residential Permit; 2015. Available from: https://www.gov.cn/zhengce/2015-12/14/content_5023611.htm.
55. Xu H, Yang H, Wang H, et al. The association of residence permits on utilization of health care services by migrants in China. Int J Environ Res Public Health. 2021;18(18):9623. doi:10.3390/ijerph18189623
56. Dong Y, Goodburn C. Residence permits and points systems: new forms of educational and social stratification in urban China. J Contemp China. 2020;29(125):647–666. doi:10.1080/10670564.2019.1704997
57. Qian XY, Song WJ. Study on the accessibility measurement of urban basic public services to migrants. Stat Res. 2020;37(03):33–47. Chinese.
58. China State Council. Notice on promoting the national basic public service standards. Available from: https://www.gov.cn/zhengce/zhengceku/2021-04/20/content_5600894.htm.
59. Grisorio MJ, Prota F. The impact of fiscal decentralization on the composition of public expenditure: panel data evidence from Italy. Reg Stud. 2015;49(12):1941–1956. doi:10.1080/00343404.2013.859665
60. Smith PC, Street A. Measuring the efficiency of public services: the limits of analysis. J R Stat Soc Ser a Stat Soc. 2005;168(2):401–417. doi:10.1111/j.1467-985X.2005.00355.x
61. Stone M. How not to measure the efficiency of public services (and how one might). J R Stat Soc Ser a Stat Soc. 2002;165(3):405–434.
62. Afonso A, Fernandes S. Assessing and explaining the relative efficiency of local government. J Soc Econ. 2008;37(5):1946–1979. doi:10.1016/j.socec.2007.03.007
63. Chen S, Zhang J. Efficiency of local government financial expenditure in China: 1978-2005. Soc Sci China. 2008;4:65–78. Chinese.
64. Shi J, Dai X, Duan K, et al. Exploring the performances and determinants of public service provision in 35 major cities in China from the perspectives of efficiency and effectiveness. Socio Econ Plann Sci. 2023;85:101441. doi:10.1016/j.seps.2022.101441
65. Zhao F, Yuan C. The development of urbanization in China: a study based on spatial equilibrium model. China Econ Q. 2017;16:1643–1668.
66. Li Z, He S, Su S, et al. Public services equalization in urbanizing China: indicators, spatiotemporal dynamics and implications on regional economic disparities. Soc Indic Res. 2020;152:1–65. doi:10.1007/s11205-020-02405-9
67. Alkire S, Foster J. Counting and multidimensional poverty measurement. J Public Econ. 2011;95(7–8):476–487. doi:10.1016/j.jpubeco.2010.11.006
68. Nguyen LT, White MJ. Health status of temporary migrants in urban areas in Vietnam. Int Migr. 2007;45(4):101–134. doi:10.1111/j.1468-2435.2007.00421.x
69. Zhang JP, Hang J, Wang JH, Hang M. Return migration and the hukou registration reform in Chinese Cities. Econ Res J. 2020;55(07):175–190. Chinese.
70. Cai F, Du Y, Wang MY. Household registration system and labor market protection. Econ Res J. 2001;12:41–49+91. Chinese.
71. Stock JH, Yogo WM, Yogo M. A survey of weak instruments and weak identification in generalized method of moments. J Bus Econ Stat. 2002;20(4):518–529. doi:10.1198/073500102288618658
72. Xie S, Mo T. The impact of education on health in China. China Econ Rev. 2014;29:1–18. doi:10.1016/j.chieco.2013.12.003
73. Chen Y, Wang H, Cheng Z, et al. Education and migrant health in China. Econ Model. 2023;121:106223. doi:10.1016/j.econmod.2023.106223
74. Ginsburg C, Collinson MA, Gómez-Olivé FX, et al. Internal migration and health in South Africa: determinants of healthcare utilisation in a young adult cohort. BMC Public Health. 2021;21:1–15. doi:10.1186/s12889-021-10590-6
75. Gu H. Understanding the migration of highly and less-educated labourers in post-reform China. Appl Geogr. 2021;137:102605. doi:10.1016/j.apgeog.2021.102605
76. Pu L. Fairness of the distribution of public medical and health resources. Front Public Health. 2021;9:768728. doi:10.3389/fpubh.2021.768728
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.