")
Back to Journals » Journal of Inflammation Research » Volume 17
How Were the Elderly RA Patients Doing Over the Past Year?—A Post Hoc Analysis for Telephone Based Following Up to RA Patients in Zunyi China
Authors Chen Y , Chen YJ, Luo JF, He M , Zhao SJ , Tian SD, Zhang YQ, Chen XL, Yang CJ, Luo YZ, Nandakumar KS , Tian M
Received 19 September 2024
Accepted for publication 14 November 2024
Published 18 November 2024 Volume 2024:17 Pages 8935—8944
DOI https://doi.org/10.2147/JIR.S493145
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Yong Chen,1 Yan-Juan Chen,1 Jian-Feng Luo,2 Mang He,1 Si-Jin Zhao,3 Shi-Dan Tian,1 Yong-Qiao Zhang,3 Xiao-Long Chen,3 Chuan-Jie Yang,3 Yu-Zhuo Luo,3 Kutty Selva Nandakumar,4 Mei Tian1
1Department of Rheumatology and Immunology, Affiliated Hospital of Zunyi Medical University, Zunyi, People’s Republic of China; 2Department of Biostatistics, School of Public Health, Fudan University, Shanghai, People’s Republic of China; 3The First School of Clinical Medicine, Zunyi Medical University, Zunyi, People’s Republic of China; 4Department of Medical Biochemistry and Biophysics, Karolinska Institute, Stockholm, Sweden
Correspondence: Mei Tian, Department of Rheumatology and Immunology, Affiliated Hospital of Zunyi Medical University, 149 Dalian Road, Huichuan District, Zunyi City, Guizhou Province, 563000, People’s Republic of China, Email [email protected] Kutty Selva Nandakumar, Department of Medical Biochemistry and Biophysics, Karolinska Institute, Stockholm, 17177, Sweden, Email [email protected]
Purpose: The quality of life (QoL) of elderly patients with rheumatoid arthritis (RA) in Zunyi China based on health parameters has not been previously analyzed. This study compares the 36-Item Short Form Health Survey (SF-36) scores and prevailing health complications between < 60y and ≥ 60y patients with RA. Data from 1166 patients with RA who visited the rheumatology department of Zunyi Medical University Hospital were followed up and retrospectively analyzed.
Patients and Methods: Data from 1166 patients with RA who visited the rheumatology department of Zunyi Medical University Hospital (2021.1– 2022.8) were followed up and retrospectively analyzed.
Results: Twenty cases passed away at 61.55 ± 8.11y, which was 6.75 years less than the local average age of death. Elderly patients with RA reported lower recovery levels, and their levels of inflammatory markers such as Immunoglobulin M-rheumatoid factor (IgM-RF), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) levels were significantly higher than those of younger patients during their past one-year observation period. The SF-36 results indicated that eight items of QoL in the elderly patients were all significantly inferior to < 60y patients, while the complications of interstitial lung disease (ILD), latent tuberculosis infection (LTBI) and, lung and herpes zoster infections were significantly higher.
Conclusion: Elderly patients had a higher disease activity along with poor QoL, more health-related complications, and susceptibility to infections. Our study emphasizes the imperative need for optimization of RA treatment modalities in the elderly to alleviate their sufferings.
Keywords: elderly rheumatoid arthritis, SF-36 scores, clinical characteristics, treatment outcomes
Introduction
The elderly rheumatoid arthritis (RA) population consists of both elderly-onset RA (EORA) that manifests after the age of 60 years and individuals diagnosed with RA early in life who aged naturally to become members of this group.1 Much attention has been paid to the EORA cohort, which is believed to possess more remarkable features of acute onset and higher disease activity.2 Irrespective of the subtypes, elderly RA is a diagnosis criteria that combines RA and aging. Although it may seem strange to many doctors, aging is now considered as a disease that could be diagnosed according to the World Health Organization’s International Classification of Diseases (ICD-10/11).3 The elderly RA population is expanding due to increased life expectancy and EORA incidence. The autoimmune reactions due to RA foster the process of aging, known as inflammaging;4 on the other hand, during aging, organisms tend to develop a characteristic inflammatory state that expresses higher levels of pro-inflammatory markers, leading to the patients having more susceptibility to infections, age-related disease onset, and neoplasms.5
Adding basic principles and characteristic features of geriatrics in their diagnosis may help rheumatologists evaluate the disease development in elderly RA for designing proper treatment strategies. Direct observation of the differences in patients’ age is essential; however, only a small number of research studies were undertaken along these lines.1 As robust treatment-to-target approaches must be balanced against adverse events due to increased comorbidities observed in the elderly RA population, while the clinical characteristics are not fully validated, the management of disease development in these patients can be challenging. There is also a limitation in the treatment approach of elderly RA, as elderly patients are usually not well represented in clinical trials.1
Located in southwest China, Zunyi is a revolutionary old city with a glorious red history as the Communist Party of China (CPC) held the famous “Zunyi Conference” in 1935. At this conference, Chairman Mao Zedong was elected as the leader of the CPC and began to move towards final victory in China’s war of liberation.6 However, the medical resources, especially in the rheumatology department, are inadequate due to economic conditions.7 Even then, our interest is mainly focused on understanding the health parameters of elderly patients with RA, as their treatment outcomes are very unclear. By collecting follow-up data on health parameters in these patients with RA who visited the Affiliated Hospital of Zunyi Medical University Hospital, and conducting this post hoc analysis, we focused on understanding the quality of life (QoL) and complications, especially infections, in the elderly, which could be useful for rheumatologists to design new treatment strategies.
Patients and Methods
Patients
This retrospective research was approved by the Ethics Committee of the Affiliated Hospital of Zunyi Medical University (KLL-2023-545). All procedures performed in this study were followed by the ethical standards of the institutional and/or national research committees and by following the 1964 helsinki Declaration and its later amendments or comparable ethical standards. Of all the 2632 patients who met the ACR/EULAR 2010 classification criteria of RA8 and visited the clinic from January 2021 to August 2022, 1166 patients or their guardians answered the telephone and accepted the follow-up study, and in total 1155 cases fulfilled all the follow-up questionnaire. The details of the patients’ backgrounds are summarized in Supplementary Materials (Supplemental Table 1 and Supplemental Figure 1). The reporting of this study conforms to Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.9
Collection of Disease Activity Parameters
The laboratory results of Immunoglobulin M-rheumatoid factor (IgM-RF), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) levels recorded in the hospital information system were selected to evaluate the disease activity. Successive patient data were recorded with baseline, and within three-month (m) periods, 3–6m, 6–9m, and 9–12m. If a patient visited more than once during one of these defined periods, a lower value was given for the patient in our data for analysis.
Treatment
The investigators recorded all the clinically prescribed drugs given by rheumatologists for one whole year to every patient, including glucocorticoids (GCs), nonsteroidal anti-inflammatory drugs (NSAIDs), conventionally synthesized disease-modifying antirheumatic drugs (csDMARDs), JAK inhibitors (JAKi), TNF inhibitors (TNFi) and Jin-gu-lian capsules (JGL, a Chinese traditional medicine10).
Telephone Call-Based Following Up on QoL
QoL of all the recruited patients was assessed using the 36-Item Short Form Health Survey (SF-36). SF-36 survey was followed up by telephone calls enquiring about the patients’ current health situation. In addition, the attacks of lung infection, herpes zoster infection, upper respiratory tract infections (URTIs), urinary tract infections (UTIs), gastrointestinal (GI) symptoms, and others were followed up. In their last year of treatment, they were also enquired about other health-related parameters. All the investigated patients gave verbal consent to participate in the interview, and the study protocol including verbal informed consent process was approved by the Ethics Committee of the Affiliated Hospital of Zunyi Medical University. For this follow-up by telephone, the written consent was not applicable. However, patients or their guardians were asked if they were willing to answer health-related questions, and their confirmation was documented by smartphone recording. The conversation template and detailed questionnaires for this telephone-based follow-up are given in the Supplementary Materials (Supplemental Figure 2). The enrolled patients who underwent high-resolution chest computed tomography (HRCT) for the chests in Zunyi Medical University Hospital were used for statistical analysis. Complications of latent tuberculosis infection (LTBI) identified by T-SPOT. TB assays were recorded from the hospital information system. A flow diagram of the study is seen in Figure 1.
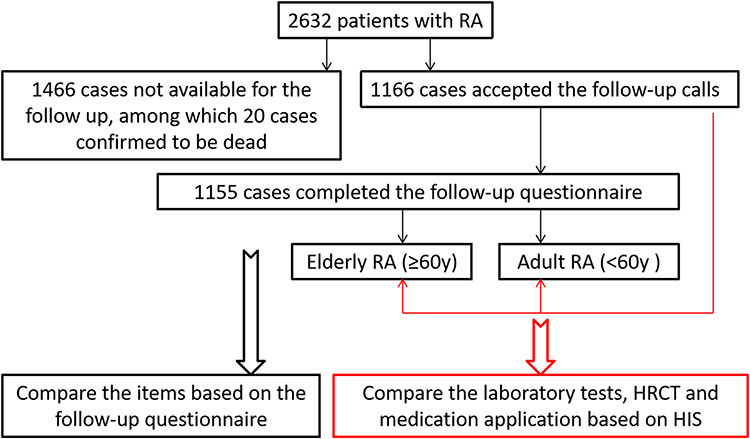 |
Figure 1 Flow diagram of the study. The red coloured arrows/box within the artwork indicated cases with data collected from HIS, although which may lack of results from the follow-up questionnaire. Abbreviations: RA, rheumatoid arthritis; HRCT, high-resolution chest computed tomography; HIS, hospital information system. |
Statistical Analysis
Statistical analysis was performed using the GraphPad Prism 9 software. Patients were divided into two groups based on their age, <60y and ≥60y groups. The measurement data of normal distribution were expressed as mean ± SD and an independent sample t-test was used to compare two groups. Measurement data of non-normal distribution were expressed as median (Q1, Q3) in tables, and median with 95% CI in figures. The Mann–Whitney U-test was used to compare two groups. The categorical data were analyzed using a chi-square (or Fisher’s exact) test based on the sample numbers. Pearson or Spearman correlation analysis was used to find a correlation between the SF-36 score and other quantifiable values such as age, disease course, self-assessed recovery level and inflammatory indexes of ESR and CRP (at time point of 9–12m); SF-36 were set as a dependent variable while age, disease course, recovery level, ESR and CRP levels (at time point of 9–12m) were set as independent variables. Significance was set at p <0.05.
Results
In total, 1166 cases were followed up. Among them, 897 cases <60y (mean, 48.27y; ranged from 13y to 59y) and 269 cases ≥60y (mean, 68.39y; ranged from 60y to 90y) were included in this study (Figure 2A). Elderly RA comprised 23.07% (269/1166) of the enrolled patients. Within the ≥60y patient group, 24.54% were males, a significantly higher percentage than 18.28% of the <60y patients (RR = 1.08, 95% CI: 1.01 to 1.17, P = 0.029; Figure 2B). The average disease duration in ≥60y patients was 10.04 (2.00, 12.50) years, a significantly longer duration than the <60y patients, 6.48 (2.00, 10.00) years (Figure 2C).
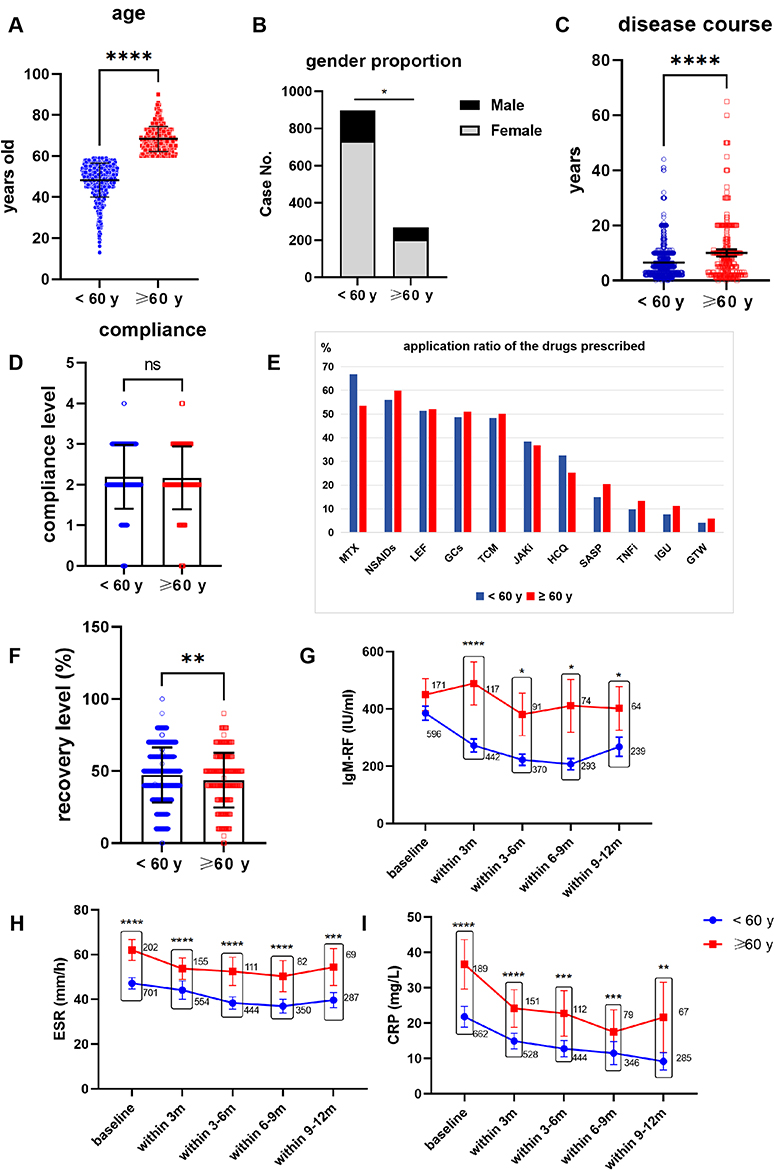 |
Figure 2 Demographic characteristics and treatment effectiveness of the patients with rheumatoid arthritis (RA) <60y and ≥60y patients. (A–C) RA was divided into elderly RA (≥60y) and <60y groups; within the ≥60y group, the male patients’ proportion was significantly higher than the <60y group, and with a significantly longer disease course. (D–E) The compliance levels with the rheumatologists and the application rates of commonly used drugs in both age groups were similar. (F–I) The ≥60y patients reported lower recovery levels, and their inflammatory markers such as IgM-RF, ESR, and CRP were generally higher than the <60y old patients at baseline and hardly declined during the one-year treatment period. *p < 0.05; **p < 0.01; ***p < 0.001; ****p < 0.0001. Abbreviations: ns, not significant; IgM-RF, Immunoglobulin M-rheumatoid factor; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; GCs, glucocorticoids; NSAIDs, nonsteroidal anti-inflammatory drugs; TCM, traditional Chinese medicine; JAKi, JAK inhibitors; TNFi, TNF inhibitors; MTX, methotrexate; LEF, leflunomide; HCQ, hydroxychloroquine; SASP, salazosulfapyridine; IGU, iguratimod; GTW, glucosidorum tripterygll totorum. |
In addition, another 20 cases (11 male and 9 female patients) were reported to have passed away at 61.55 ± 8.11y [6.75 years less than the current average death age of Guizhou province, China (68.30y)], according to the seventh Chinese national population census (t = 3.72, P < 0.001 by one sample t-test). One more female who died at 28y due to a combination of antiphospholipid syndrome and pregnancy with amniotic cavity infection was also excluded.
The compliance levels with rheumatologists in both age groups were also similar (Figure 2C). The application rates of each commonly used anti-rheumatic drug in both age groups also showed no significant difference (Figure 2D). The anti-rheumatic medications applied to the patients in both groups were similar; however, the subjective recovery level in ≥60y patients was lower than the <60y patients (Figure 2E and F). The levels of inflammatory markers used to assess the disease activity such as IgM-RF, ESR and CRP levels were decreasing more steadily in <60y patients but trudged in ≥60y patients. At baseline, IgM-RF levels were without any significant differences between the two age groups of patients but significantly higher in ≥60y patients during their last year observation time period. From baseline to end, the ESR and CRP levels were significantly higher in ≥60y patients than in <60y patients (Figure 2G–I).
A total of 1155 cases completed the SF-36 questionnaires. The results indicated that eight QoL domains and reported health transition in ≥60y patients were significantly inferior to <60y patients (Table 1).
 |
Table 1 Comparison of SF-36 Domains Between the <60y and the ≥60y Patients |
Furthermore, in both female and male patients, overall scores of the SF-36 were negatively correlated with age, disease course, disease activity indexes of ESR and CRP levels, while a positive correlation was observed with the self-assessed recovery level of patients. Except for the correlation between SF-36 score and CRP levels in the males, all the other data showed statistical significance (Figure 3A–J).
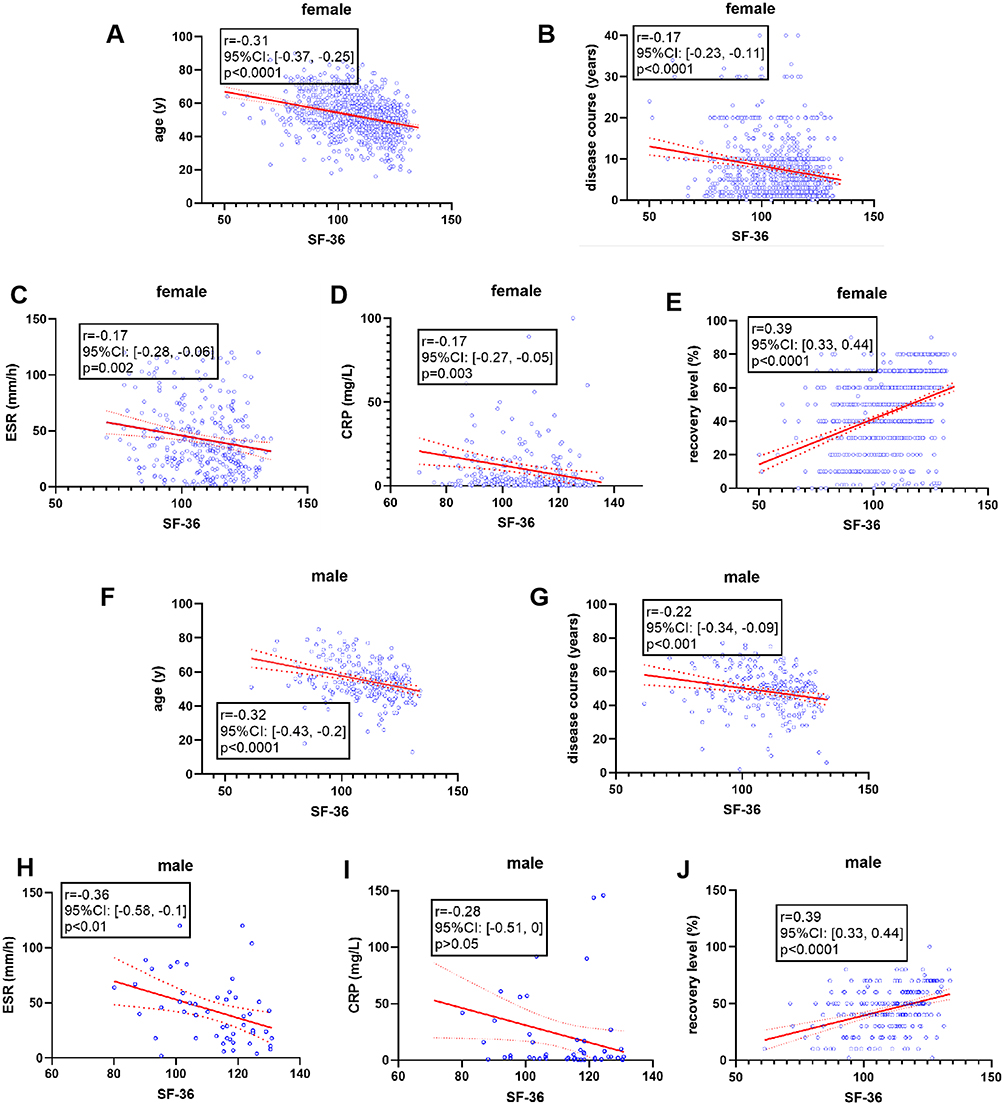 |
Figure 3 Correlation between the overall scores of SF-36 with age, disease course, disease activity indexes of ESR and CRP levels, and self-assessed recovery level of RA patients. The Pearson correlation analysis in the (A–E) female and (F–J) male patients. Abbreviations: ESR, erythrocyte sedimentation rate; CRP, C-reactive protein. |
Based on the HRCT scan results, interstitial lung disease (ILD) was present in 19.73% of patients with RA. Elderly patients (≥60y) had a higher incidence of ILD. The positive incidence of the T-SPOT.TB assay indicating LTBI in 3.86% of the patients, ≥60y patients also showed higher LTBI incidence. Complications of lung and herpes zoster infections, with incidence rates of 17.84% and 8.13% were also present higher in the elderly patients. Gastrointestinal symptoms, URTIs, and UTIs showed higher incidence rates in elderly patients but without any statistical difference (Table 2).
 |
Table 2 Incidence of Complications Between the <60y and ≥60y Patients |
Discussion
RA is a chronic autoimmune disease affecting joints and other organs, which leads to pain, swelling, and deformity, causing considerable morbidity and mortality worldwide.11 Among the 2632 patients who visited the rheumatology department of Zunyi Medical University Hospital, 1155 patients accepted and answered all the follow-up questions, whereas some patients answered only part of the questionnaire. In addition, some other patients or their guardians declined to answer the phone, and we could not reach out to some of the telephone numbers. The situation regarding these patients is unclear, and patients’ death might be one of the possible reasons for failing to answer our calls.
In the current study, due to the retrospective data collection, it was not possible to apply the remission criteria to assess patients’ remission rate. ESR, CRP and RF are the laboratory markers currently most frequently used for assessing RA activity.12 Although patients received treatment with multiple drugs, our data showed both elderly and younger patients had high levels of ESR, CRP, and RF titers during the study period. Also, a substantial portion of patients complained about low level of recovery. A cross-sectional study suggests that the RA remission rate in China was only 4.23%–14.88%, and nearly 80% of patients had moderate-to-severe arthritis.13
Our data indicate a significantly higher proportion of the elderly patients were indeed males compared to <60y patients, similar to the data published in Pakistan.14 Although application ratios of glucocorticoids (GCs), nonsteroidal anti-inflammatory drugs (NSAIDs), and disease-modifying antirheumatic drugs (DMARDs), used to treat both <60y and ≥60y patients were similar, ≥60y patients reported significantly a lower level of recovery by their subjective perception. ≥60y patients had significantly higher levels of disease activity markers (IgM-RF, CRP, and ESR) than <60y patients during the study period. Notably, the average death age of RA patients in Zunyi was 61.55y (6.75 years less than the current average death age of people in Guizhou province (Zunyi is a city within Guizhou province) according to the seventh Chinese national population census.
The comparison of QoL between <60y and ≥60y RA patients based on telephone call follow-up showed elderly patients had significantly lower values in all the nine domains of the SF-36 survey than <60y patients. These results were validated and found to be in concordance with our knowledge of aging and gerontology.15 Gouda et al16 reported age in RA patients was positively correlated with Berlin questionnaire, a tool to assess the risk of obstructive sleep apnea in adults and Health Assessment Questionnaire-Disability Index (HAQ-DI), which confirmed the reliability of our findings. Moreover, geriatric syndromes were more commonly observed in elderly patients screened by various methods such as mini-mental state exam (MMSE), five-item geriatric depression scale-15 (GDS-15), mini nutritional assessment (MNA), and assessment questionnaire disability index (HAQ-DI).17,18 The SF-36 is a frequently used global measure to assess the health-related QoL and hence was applied in this current cross-sectional study for the first time to analyze differences between young and elderly patients. In both female and male patients, overall scores of the SF-36 were negatively correlated with age, disease course, disease activity indexes of ESR and CRP levels, while a positive correlation was observed with the self-assessed recovery level of patients.
ILD had a higher incidence in elderly patients with RA, which is similar to the earlier reported data.19 The overall T-SPOT.TB test positive rate of 3.86% is lower than the reported positive rate in China (ranging between 13.5% and 19.8%).20 This might be due to the fact that T-SPOT.TB screening test was not applied to all the patients because this is an expensive test not financially covered by medical insurance provided by the local government. However, in patients who were screened with T-SPOT.TB test, a positive rate of 7.89% was observed in the elderly, which was significantly higher than the 2.56% observed in the <60y patients. Similarly, the lung and herpes zoster infections in elderly patients were significantly higher than in the younger patients.
Based on the lab and clinical data, patients were prescribed with similar NSAIDs, GCs, and DMARDs including biologic agents to both younger and elderly patients, which is also in compliance with guideline requirements and scientific literature.21,22 However, the outcomes of the real world indicate that elderly patients with RA were suffering from deteriorating disease activity and QoL, which is different from an earlier report in which EORA patients from Western countries had a lower disease activity with reduced drug dosage than younger RA patients.23 It is also generally acknowledged that disease management with different levels of treatment with immunosuppressive drugs or GCs may lead to higher incidence or more severely associated comorbidities in elderly patients with RA.24 A more inadequate treatment to target might result in a higher disease activity in the elderly, as indicated in our study. Hence, the current therapeutic approach for patients with RA needs to be differentiated based on age and subsequently changed to have a higher remission rate.
We would like to document the limitations of our current study. Firstly, Zunyi is a third-tier city in China, with 6.6 million residents having 69,000 RMB (9500 USD) GDP per capita in 2023. This study was conducted at a single hospital center in a third-tier city, hence limiting the generalizability of the findings to other settings or population. Secondly, the analysis relies on patients who were contactable and willing to participate in this follow-up study by telephone, which could introduce a selection bias,25 because the elderly may struggle more with telephone-based communication than younger patients. To circumvent these issues, at present, we are conducting a face-to-face study. Therefore, in the future, we can compare the two follow-up methods, and hopefully to provide more accurate updated data.
Conclusion
In conclusion, our follow-up on a large scale of patients with RA in Zunyi, China, revealed the actual conditions of their recovery and health status. Especially in elderly patients, disease activity was higher than in younger patients as indicated by inflammatory markers, poor QoL as per the SF-36 survey, and higher incidence of ILD, LTBI, and lung, and herpes zoster Infections. Hence, it is imperative to optimize the treatment regimen for elderly patients to control and alleviate their prolonged sufferings.
Acknowledgments
We express our thanks to the patients and their family members who participated in this study, and we are genuinely sorry for the patients who already passed away.
Funding
This work was supported by the Doctoral Research Start-up Fund Project in the affiliated Hospital of Zunyi Medical University (No. YZ-2023-03), and Science and Technology Fund project of Guizhou Provincial Health Commission (gzwkj2024-126).
Disclosure
The authors report no conflicts of interest in this work. This paper has been uploaded to ResearchGate as a preprint: https://www.researchsquare.com/article/rs-4918713/v1.
References
1. Serhal L, Lwin MN, Holroyd C, Edwards CJ. Rheumatoid arthritis in the elderly: characteristics and treatment considerations. Autoimmun Rev. 2020;19(6):102528. doi:10.1016/j.autrev.2020.102528
2. Sugihara T. Treatment strategies for elderly-onset rheumatoid arthritis in the new era. Mod Rheumatol. 2022;32(3):493–499. doi:10.1093/mr/roab087
3. Zhavoronkov A, Bhullar B. Classifying aging as a disease in the context of ICD-11. Front Genet. 2015;6:326. doi:10.3389/fgene.2015.00326
4. Chen Y, Chen Y, Zhao L, et al. Albumin/globulin ratio as Yin-Yang in rheumatoid arthritis and its correlation to inflamm-aging cytokines. J Inflamm Res. 2021;14:5501–5511. doi:10.2147/JIR.S335671
5. Liu Z, Liang Q, Ren Y, et al. Immunosenescence: molecular mechanisms and diseases. Signal Transduct Target Ther. 2023;8(1):200. doi:10.1038/s41392-023-01451-2
6. You-fu W. On the historical status and the times value of zunyi conference and its spirit. J Xihua Univ. 2020;39(4):13–19.
7. Guo X, Chen R, Meadows ME, Li Q, Xia Z, Pan Z. Factors influencing four decades of forest change in Guizhou Province, China. Land. 2023;12(5):1004. doi:10.3390/land12051004
8. Aletaha D, Neogi T, Silman AJ, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010;62(9):2569–2581. doi:10.1002/art.27584
9. von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–349. doi:10.1016/j.jclinepi.2007.11.008
10. Chen Y, He M, Zhao SJ, et al. Jin-Gu-Lian capsule did not significantly improve clinical value in rheumatoid arthritis therapy: a real-world study. J Inflamm Res. 2024;17:5509–5519. doi:10.2147/JIR.S468880
11. Chen Y, Qiu F, Yu B, et al. Metformin, an AMPK activator, inhibits activation of FLSs but promotes HAPLN1 secretion. Mol Ther Methods Clin Dev. 2020;17:1202–1214. doi:10.1016/j.omtm.2020.05.008
12. Da ML, Dos SNL, de Carvalho JF. Autoantibodies and other serological markers in rheumatoid arthritis: predictors of disease activity? Clin Rheumatol. 2009;28(10):1127–1134. doi:10.1007/s10067-009-1223-y
13. Yu C, Li M, Duan X, et al. Chinese registry of rheumatoid arthritis (CREDIT): i. Introduction and prevalence of remission in Chinese patients with rheumatoid arthritis. Clin Exp Rheumatol. 2018;36(5):836–840.
14. Haroon MD, Aamer M. Elderly onset of rheumatoid arthritis is more common in males, and requires maintenance of low-dose corticosteroids along with the combination of disease modifying anti rheumatic agents. Semin Arthritis Rheum. 2021;51(5):e10. doi:10.1016/j.semarthrit.2020.09.017
15. Hill RD, Mansour E, Valentijn S, Jolles J, van Boxtel M. The SF-36 as a precursory measure of adaptive functioning in normal aging: the Maastricht Aging Study. Aging Clin Exp Res. 2010;22(5–6):433–439. doi:10.1007/BF03324943
16. Gouda W, Mokhtar M, Elazab SA, et al. Sleep disorders in patients with rheumatoid arthritis: association with quality of life, fatigue, depression levels, functional disability, disease duration, and activity: a multicentre cross-sectional study. J Int Med Res. 2023;51(10):655701891. doi:10.1177/03000605231204477
17. Niksolat F, Zandieh Z, Roshani F, et al. Geriatric syndromes among patients with rheumatoid arthritis: a comparison between young and elderly patients. Ethiop J Health Sci. 2022;32(4):791–798. doi:10.4314/ejhs.v32i4.16
18. Cleutjens F, Boonen A, van Onna M. Geriatric syndromes in patients with rheumatoid arthritis: a literature overview. Clin Exp Rheumatol. 2019;37(3):496–501.
19. Messina R, Guggino G, Benfante A, Scichilone N. Interstitial lung disease in elderly rheumatoid arthritis patients. Drugs Aging. 2020;37(1):11–18. doi:10.1007/s40266-019-00727-z
20. Cui X, Gao L, Cao B. Management of latent tuberculosis infection in China: exploring solutions suitable for high-burden countries. Int J Infect Dis. 2020;92S:S37–S40. doi:10.1016/j.ijid.2020.02.034
21. Diaz-Borjon A. Guidelines for the use of conventional and newer disease-modifying antirheumatic drugs in elderly patients with rheumatoid arthritis. Drugs Aging. 2009;26(4):273–293. doi:10.2165/00002512-200926040-00001
22. Smolen JS, Landewe R, Bergstra SA, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann Rheum Dis. 2023;82(1):3–18. doi:10.1136/ard-2022-223356
23. Kumagai K, Okumura N, Amano Y, et al. Consideration of differences in drug usage between young-onset and elderly-onset rheumatoid arthritis with target of low disease activity. Mod Rheumatol. 2021;31(6):1094–1099. doi:10.1080/14397595.2021.1883251
24. Cabral VP, Andrade CA, Passos SR, Martins MF, Hokerberg YH. Severe infection in patients with rheumatoid arthritis taking anakinra, rituximab, or Abatacept: a systematic review of observational studies. Rev Bras Reumatol Engl Ed. 2016;56(6):543–550. doi:10.1016/j.rbr.2016.07.008
25. Lu H, Cole SR, Howe CJ, Westreich D. Toward a clearer definition of selection bias when estimating causal effects. Epidemiology. 2022;33(5):699–706. doi:10.1097/EDE.0000000000001516
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.