")
Back to Journals » Journal of Inflammation Research » Volume 18
Hs-CRP, Diabetic Status, and Adverse Events Among Patients Receiving Statin Therapy Following PCI—A Prospective Registry-Based Study
Authors Chen X, Wang HY, Sun W, Lin Z, Qiao Z, Bian X, Yin D, Feng L, Zhu C, Song W, Wang H, Jia L, Dong Q, Dou K
Received 19 January 2025
Accepted for publication 27 May 2025
Published 15 July 2025 Volume 2025:18 Pages 9261—9274
DOI https://doi.org/10.2147/JIR.S518383
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Ning Quan
Xinyue Chen,1– 3,* Hao-Yu Wang,1– 4,* Wanqing Sun,1– 3,* Zhangyu Lin,1– 3 Zheng Qiao,1– 3 Xiaohui Bian,1– 3 Dong Yin,1 Lei Feng,1 Chenggang Zhu,1 Weihua Song,1 Hongjian Wang,1 Lei Jia,1 Qiuting Dong,1 Kefei Dou1– 4
1Cardiometabolic Medicine Center, Department of Cardiology, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 2Coronary Heart Disease Center, Department of Cardiology, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 3State Key Laboratory of Cardiovascular Disease, Beijing, People’s Republic of China; 4National Clinical Research Center for Cardiovascular Diseases, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kefei Dou; Hao-Yu Wang, Cardiometabolic Medicine Center, Coronary Heart Disease Center, Department of Cardiology, Fuwai Hospital, State Key Laboratory of Cardiovascular Disease, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, No.167 North Lishi Road, Xicheng District, Beijing, 100037, People’s Republic of China, Tel +86-13801032912, Fax +86-10-6831-3012, Email [email protected]; [email protected]
Purpose: Inflammation represents a key driver of type 2 diabetes (T2DM) and is associated with major adverse cardiovascular and cerebrovascular events (MACCEs). Residual inflammatory risk, defined as persistent inflammation despite lipid-lowering therapy, differs from residual cholesterol risk, which refers to suboptimal lipid levels post-treatment. This study aims to evaluate the impact of T2DM on the relationship between residual inflammatory risk, as assessed by a simple, economical, and easily measurable biomarker—high-sensitivity C-reactive protein (hs-CRP)—and clinical outcomes in statin-treated coronary heart disease (CHD) patients with drug-eluting stent (DES) implantation.
Patients and Methods: 8,628 individuals with CHD treated with statins and DES implantation at Fuwai Hospital were included. Participants were first stratified according to T2DM status, and then baseline hs-CRP levels were further divided into three groups using 1 mg/L and 2 mg/L as the cut-off points. The primary endpoint was MACCEs, defined as the composite of all-cause mortality, myocardial infarction, stroke, and target vessel revascularization.
Results: After 2.4 years of median follow-up duration, 999 patients were defined as MACCEs, whose hs-CRP levels were significantly higher compared to the non-MACCEs group (p = 0.007). The cohort was stratified into T2DM (n = 3,729) and Non-T2DM (n = 4,899) groups. In full adjusted model: for the Non-T2DM group, hs-CRP ≥ 2 mg/L remained significantly associated with MACCEs [HR = 1.39, 95% CI (1.14– 1.85), p = 0.002]. In the T2DM group, no significant association was observed [HR = 1.02, 95% CI (0.73– 1.23), p = 0.453] (p for interaction= 0.040).
Conclusion: Among CHD patients receiving contemporary statin therapy following DES implantation, higher hs-CRP levels appeared to be associated with future MACCEs in those without T2DM, though not in T2DM patients. Hs-CRP, an important diagnostic marker of inflammation, shows different value depending on diabetes status, revealing how diabetes and inflammation jointly influence cardiovascular outcomes and providing clinical insights for optimizing the application of inflammatory biomarkers in personalized cardiovascular risk stratification.
Keywords: high-sensitivity C-reactive protein, risk of residual inflammation, coronary heart disease, statin therapy, diabetes mellitus, major adverse cardiovascular and cerebrovascular events
Introduction
Coronary heart disease (CHD) ranks among the top global causes of mortality.1 Despite the prowess of statins in slashing low-density lipoprotein cholesterol (LDL-C) levels and high-sensitivity C-reactive protein (hs-CRP) levels, and significantly cutting down on cardiovascular incidents, there is still a concerning chunk of patients who linger in the danger zone for heart issues, even after undergoing statin treatment. Residual cardiovascular risk refers to the persistent risk of cardiovascular events that patients with CHD continue to face even after receiving standard treatments.2 In recent years, residual inflammatory risk (often reflected by hs-CRP—a simple, cost-effective, and easily measurable inflammatory biomarker) has gained considerable attention as a significant contributor to the ongoing cardiovascular risks faced by patients with CHD following statin treatment, differs from residual cholesterol risk, which refers to suboptimal lipid levels post-treatment.3 Although statins can reduce hs-CRP levels in many patients, a significant proportion still exhibit persistently elevated hs-CRP concentrations even after achieving guideline-recommended LDL-C targets.4 And study has demonstrated that baseline hs-CRP levels are related to future cardiovascular events in statin-treated CHD patients.5 Therefore, exploring whether hs-CRP can effectively predict major adverse cardiovascular and cerebrovascular events (MACCEs) in the context of statin therapy, especially the prognostic value of different metabolic states (eg, diabetes) remains a key question in current research.
Type 2 diabetes mellitus (T2DM), as an important risk factor for CHD, is strongly associated with a chronic low-grade inflammatory state.6 Individuals with T2DM often exhibit elevated hs-CRP levels and an increased likelihood of experiencing cardiovascular complications.6 Moreover, diabetes-related inflammation involves multiple pathways.7,8 This diabetes-specific chronic low-grade inflammation may alter the effect of statins on hs-CRP. However, it has not been definitively verified whether patients with T2DM and CHD can accurately predict residual cardiovascular risk with hs-CRP after statin therapy. Some studies suggest that the prognostic role of hs-CRP may be weakened due to higher levels of inflammation in patients with T2DM.9 Other studies have suggested that hs-CRP has significant prognostic value despite a strong inflammatory response in patients with T2DM.10 Thus, it remains unclear whether diabetes modifies the prognostic value of hs-CRP. This study focuses on residual inflammatory risk by evaluating the role of hs-CRP in CHD patients undergoing statin therapy and DES implantation. Specifically, it explores how T2DM influences the relationship between hs-CRP and MACCEs.
Patients and Methods
Study Design
This research involved 10,724 CHD patients who received percutaneous coronary intervention (PCI) at Fuwai Hospital, Chinese Academy of Sciences, from January to December 2013.11–13 The following patients were excluded: (1) not on statin therapy; (2) age < 18 years; (3) missing crucial baseline data, including hs-CRP, lipoprotein(a) [Lp(a)], glycated hemoglobin A1c (HbA1c), white blood cell, and left ventricular ejection fraction (LVEF); (4) no drug-eluting stent (DES) implantation; (5) with tumor, infection, impaired liver and kidney. Finally, 8628 patients were included in the study (Figure 1). The research adhered to the principles outlined in the Declaration of Helsinki and received approval from the Institutional Review Board at Fuwai Hospital. Prior to the intervention, all participants gave their informed written consent for ongoing follow-up.
 |
Figure 1 Study flowchart. Abbreviations: HbA1c, hemoglobin A1c; hsCRP, high-sensitivity C-reactive protein; Lp(a), lipoprotein(a); DES, drug eluting stent, LVEF, left ventricular ejection fraction; PCI, percutaneous coronary intervention; T2DM, type 2 diabetes mellitus; WBC, white blood cells. |
Clinical Endpoints and Definitions
Evaluate the clinical condition of patients at 1, 6, and 12 months intervals, and subsequently on an annual basis through either outpatient appointments or telephone consultations. The primary endpoint is MACCEs, defined as the composite of all-cause mortality, myocardial infarction (MI), stroke, and target vessel revascularization (TVR). All-cause mortality is defined as death from any cause, whether cardiac or non-cardiac. MI was determined based on clinical and laboratory parameters, according to the third universal definition of MI (utilizing hs-cTn for the diagnosis of MI).14 TVR is defined as any repeated revascularization of any part of the target vessel. This encompassed both planned and unplanned revascularization procedures. Stroke is characterized as a neurological impairment, which can either be ischemic or hemorrhagic (transient ischemic attacks were excluded from the stroke definition within the primary endpoint of MACCEs),15,16 as assessed by a neurologist through imaging techniques. Each incident was evaluated by two seasoned cardiologists who were not privy to the details of this study. Any discrepancies in their assessments were addressed by seeking the opinion of a third knowledgeable cardiologist. The risk of residual inflammation was based on baseline hs-CRP ≥ 2mg/L.5 Additionally, a recent single-center cohort study from JACC Asia suggested that hs-CRP level ≥1 mg/L may be more suitable for assessing the association with MACCEs after PCI than the traditional residual inflammatory risk threshold of hs-CRP ≥2 mg/L.17 The threshold of 1mg/L has also been supported in exploratory studies of other Asian cohorts.18–20 Based on this, this study categorized hs-CRP into three groups: <1 mg/L, ≥1 mg/L <2 mg/L, and ≥2 mg/L, for further investigation. T2DM was diagnosed based on HbA1c level ≥ 6.5% or a previous diagnosis of T2DM confirmed by the use of antidiabetic medication.21
Statistical Analysis
The Kolmogorov–Smirnov test was employed to assess whether the data followed a normal distribution. To analyze quantitative variables, the Mann–Whitney U-test was applied. Additionally, a chi-square test was conducted to investigate qualitative variables. In analyzing the data, continuous variables were presented as the mean ± standard deviation (SD) or the median along with the interquartile range (IQR) spanning the 25th to the 75th percentile. Statistical comparisons were conducted through the application of the t-test. Categorical variables were summarized as frequency with percentage. The MACCEs risk in each group was represented by Kaplan-Meier survival curves and compared using the Log rank test. Univariate Cox regression, multivariate Cox regression, and Least Absolute Shrinkage and Selection Operator (LASSO) regression were used to select covariates. Collinearity analysis was performed to observe the degree of correlation between covariates. The final covariates included in the model were: age, body mass index (BMI), bifurcation lesions, beta-blockers, calcium channel blockers (CCB), glycoprotein IIb/IIIa antagonists, HbA1c, hypertension, LDL-C, left main (LM)/three-vessel disease, previous coronary artery bypass grafting (CABG), previous PCI, previous stroke, previous MI, sex, smoking status, syntax score, and WBC count. Cox regression analyses were performed to assess the prognostic value of hs-CRP for MACCEs in different populations of CHD with different diabetes statuses from which hazard ratio (HR) and 95% confidence intervals (95% CI) were calculated. The Schoenfeld residual test examines the validity of the proportional hazards assumption. RCS analysis was conducted to more comprehensively assess the association between hs-CRP levels and MACCE risk. Sensitivity analyses included: incorporating patients without DES implantation in the study population for COX analysis; performing COX analysis with hs-CRP using a cutoff of 2 mg/L; conducting COX analysis in combination with LDL-C. Subgroup analysis was performed stratified by HbA1c. Analyses of this study mainly relied on R (version 4.4.2) and SPSS version 26.0 (IBM Corporation, Armonk, NY). All tests were two-sided with a significance level of 0.05.
Results
Baseline Characteristics
The research encompassed 8,628 patients undergoing statin therapy for CHD, with a median age of 59 years [IQR: 51–65]. Among these participants, 77.2% were male. The average follow-up period lasted 2.4 years [IQR: 2.2–2.6]. Figure 1 provides a visual representation of the selection process for the study population. Table S1 presents the initial attributes of subjects categorized based on MACCEs during the observation period. Among the 7,629 patients who did not experience MACCEs and the 999 who did, those in the MACCEs group exhibited markedly higher rates of T2DM (48.1% compared to 42.6%, p < 0.001) and hypertension (67.6% versus 63.7%, p = 0.016) than their non-MACCEs counterparts. Furthermore, both white blood cell counts and hs-CRP levels were significantly elevated in the MACCEs group (p = 0.002 and p = 0.007, respectively). The administration of glycoprotein IIb/IIIa antagonists was also more prevalent among patients experiencing MACCEs (p < 0.001). Notably, there were significant disparities in coronary artery features and treatment-related variables, such as the extent of coronary calcification (p = 0.003), the existence of bifurcation lesions (p = 0.004), and Syntax score (p < 0.001) between the two populations.
A deeper examination categorized the cohort based on the presence of T2DM and levels of hs-CRP (Table S2 and Table 1). Patients without T2DM were notably younger (p < 0.001) and had a greater percentage of males (p < 0.001), along with lower BMI (p < 0.001) and reduced rates of hypertension (p < 0.001) and hyperlipidemia (p < 0.001). In contrast, those in the T2DM group displayed significantly elevated WBC counts (p < 0.001) and hs-CRP levels (p < 0.001), indicating that individuals with diabetes tend to experience both heightened inflammatory reactions and more significant difficulties in managing blood glucose levels. Furthermore, this group showed increased usage of calcium channel blockers (p < 0.001) and beta-blockers (p < 0.001). The severity of coronary artery disease was also exacerbated in the T2DM group, which exhibited a higher occurrence of LM/three-vessel disease, coronary calcification, and elevated Syntax scores (p < 0.001, p = 0.014, and p < 0.001, respectively). Table S3 presents a comparison of baseline characteristics between DES-implanted patients including non-statins-treated people and included patients in the study. The hs-CRP levels in this group ranged from 1.59 [0.81, 3.52] mg/L. In the sample after excluding statin-treated individuals (n=8,624), the hs-CRP levels ranged from 1.58 [0.80, 3.52] mg/L, with no statistically significant difference between the two groups (p=0.657). Table S4 presents a comparison of baseline characteristics between patients excluded due to missing data and patients included in the study. No systematic differences were found between patients with missing data and those included.
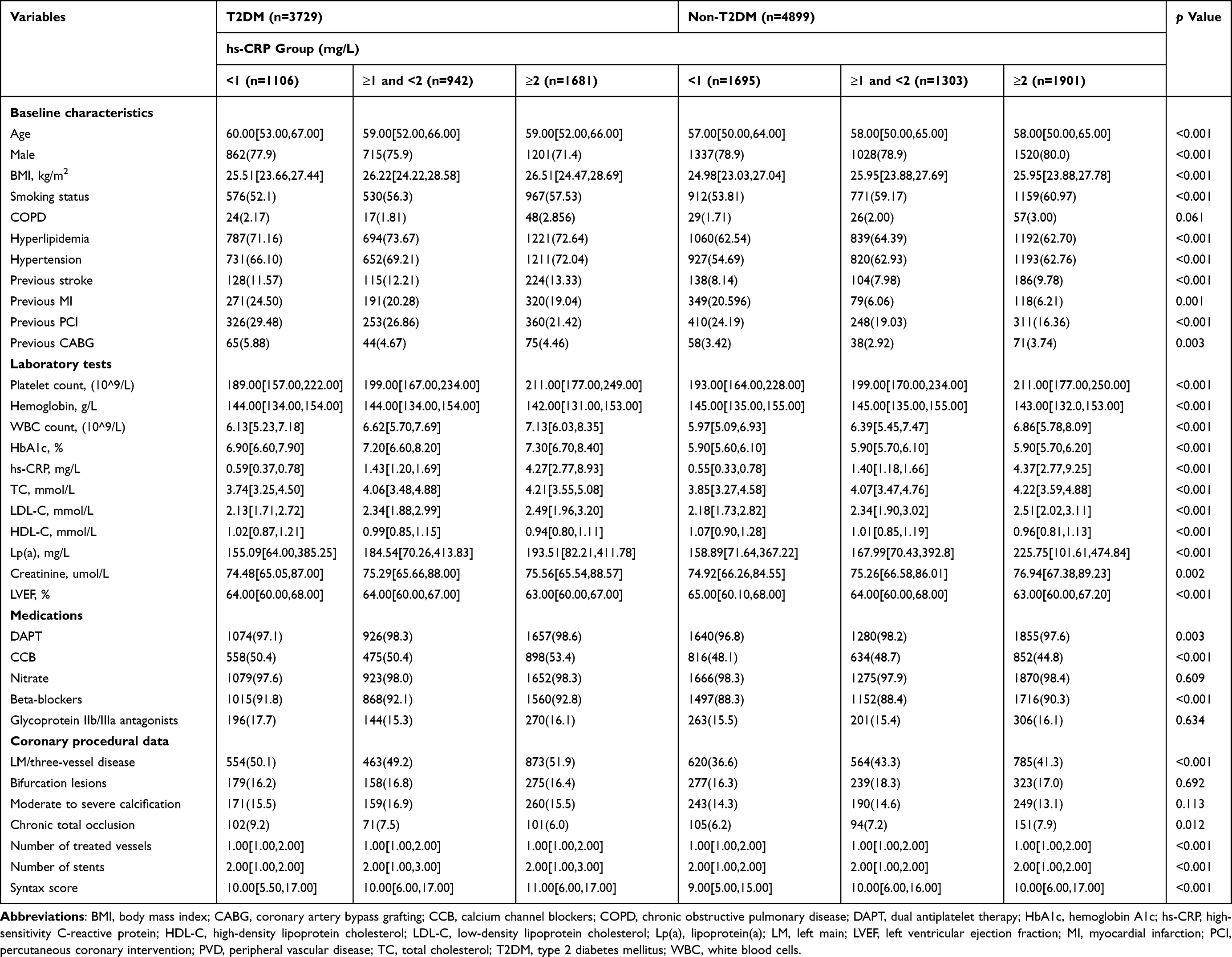 |
Table 1 Baseline Characteristics Stratified by T2DM and hs-CRP |
Prognostic Association of hs-CRP for MACCEs in T2DM and Non-T2DM Groups
Kaplan-Meier survival analysis revealed significant differences in MACCEs incidence across hsCRP categories in the Non-T2DM group (Log-rank p = 0.011) (Figure 2A), but no significant differences were observed in the T2DM group (Log-rank p = 0.310) (Figure 2B). Next, the research delved into the influence of a variety of clinical and lab factors on MACCEs through a univariate Cox regression analysis, as detailed in Table S5. Those variables that did not exceed the significance threshold of p ≤ 0.20 were then subjected to a more rigorous examination via the LASSO regression technique, as depicted in Figure S1. The 20 variables selected by LASSO regression were then incorporated into the multivariate Cox regression, with the results presented in Table S6. Then, based on multivariate Cox regression, clinical relevance, and literature review, the following variables for inclusion in further study were selected: age, BMI, bifurcation lesions, beta-blockers, CCB, glycoprotein IIb/IIIa antagonists, HbA1c, hypertension, LDL-C, LM/three-vessel disease, previous CABG, previous PCI, previous stroke, previous MI, sex, smoking status, Syntax score, and WBC count. Collinearity analysis showed that the variance inflation factor (VIF) for all covariates was below 5 (Figure S2), indicating no significant multicollinearity in the model.
 |
Figure 2 Kaplan–Meier analysis for MACCEs outcomes according to different hs-CRP levels in Non-T2DM and T2DM. (A) Kaplan–Meier analysis for MACCEs outcomes according to different hs-CRP levels in Non-T2DM group; (B) Kaplan–Meier analysis for MACCEs outcomes according to different hs-CRP levels in T2DM group. Abbreviation: hs-CRP, high-sensitivity C-reactive protein; T2DM, type 2 diabetes mellitus; MACCE, major adverse cardiovascular and cerebrovascular event. |
Table 2 presents the findings from the unadjusted Cox regression analysis. In the Non-T2DM cohort, individuals with a hs-CRP level of 2 mg/L or higher faced a notably greater chance of experiencing MACCEs than those with levels below 1 mg/L [HR = 1.36, 95% CI (1.11–1.67), p = 0.003]. However, the T2DM group did not exhibit a significant rise in MACCEs risk at the 2 mg/L threshold [HR = 0.98, 95% CI (0.79–1.21), p = 0.835], as opposed to levels below 1 mg/L. In the three models adjusted for covariates, the results remained consistent (Table 2). Specifically, In Adjusted model 1, in the Non-T2DM group, the risk of MACCEs jumped in the 2 mg/L or higher hs-CRP group versus those under 1 mg/L [HR = 1.30, 95% CI (1.05–1.61), p = 0.017]. For the T2DM group, no significant link was found [HR = 0.92, 95% CI (0.73–1.15), p = 0.459]. The analysis of the interaction between hs-CRP and T2DM status using the Cox model resulted in a p-value of 0.048, implying that the prognostic association between hs-CRP and MACCEs differed significantly in patients with and without T2DM. To further validate this effect, we assessed the heterogeneity of hs-CRP across different diabetic statuses using the Q-test. The results showed Q = 4.80, p = 0.028, I² = 79.6%, indicating a significant difference in the association between hs-CRP and MACCE risk between the two groups. In full adjusted model (Adjusted model 3), for the Non-T2DM group, hs-CRP ≥ 2 mg/L remained significantly associated with MACCEs [HR = 1.39, 95% CI (1.14–1.85), p = 0.002]. In the T2DM group, no significant association was observed [HR = 1.02, 95% CI (0.73–1.23), p = 0.453]. The p-value for interaction between hs-CRP and T2DM status was 0.040. The Schoenfeld residual test confirmed that the proportional hazards assumption of the Cox model holds (all covariates p > 0.05). After adjusting for covariates, the results showed a nonlinear relationship between hs-CRP and MACCE risk in the Non-T2DM group (P for non-linearity = 0.043, P for overall = 0.032) (Figure S3A). In the T2DM group, no significant nonlinear relationship was observed (P for non-linearity = 0.906, P for overall = 0.869) (Figure S3B).
 |
Table 2 Prognostic Association of the hs-CRP for MACCEs with and without T2DM in Cox Regression Analyses for MACCEs |
Several sensitivity analyses were conducted. First, we performed a COX analysis in the population that did not exclude individuals who did not receive DES. The inclusion and exclusion criteria remained the same as before, except for not excluding those who did not receive DES, ultimately including 9,030 patients (Non-T2DM: n=5,050; T2DM: n=3,980). Cox regression results were consistent with our primary findings. In the fully adjusted model (Adjusted model 3), hs-CRP ≥2 mg/L was associated with increased MACCE risk in Non-T2DM patients [HR=1.37, 95% CI (1.14–1.67), p=0.008], but not in T2DM patients [HR=1.02, 95% CI (0.82–1.21), p=0.791]. The analysis of the interaction between hs-CRP and T2DM status using the Cox model resulted in a p-value of 0.037. Full results are presented in the revised manuscript (Table S7). The Schoenfeld residual test confirmed that the proportional hazards assumption of the Cox model holds (all covariates p > 0.05). Second, we conducted a sensitivity analysis using 2 mg/L as the threshold (Table S8). Patients with hs-CRP ≥ 2 mg/L had a significantly higher risk of MACCEs compared to those with hs-CRP < 2 mg/L across all models in Non-T2DM Group. No significant association was observed between hs-CRP ≥2 mg/L and MACCEs in T2DM Group. The interaction between hs-CRP and T2DM status remained statistically significant (p for interaction = 0.014 in Adjusted model 3), consistent with our primary findings using the three-group categorization. Third, we supplemented the COX analysis results based on risk stratification combining LDL-C + hs-CRP. The results showed that the combined classification of LDL-C and hs-CRP did not have a statistically significant effect on MACCEs risk stratification (Table S9). Additionally, we have added subgroup analyses based on HbA1c levels (Table S10): for the HbA1c<6.5% (n=5658) group, hs-CRP ≥ 2 mg/L remained significantly associated with MACCEs [HR = 1.26, 95% CI (1.04–1.54)]. In the 6.5% ≤ HbA1c < 7% (n=958) and HbA1c ≥ 7.0% (n=2012) group, no significant association was observed [HR = 0.74, 95% CI (0.44–1.19); HR =0.90, 95% CI (0.63–1.05)]. The p-value for interaction between hs-CRP and T2DM status was 0.037.
Discussion
This large-scale prospective observational cohort study sought to explore the association between hs-CRP as an indicator of residual inflammation related to MACCEs in individuals with CHD who are undergoing statin treatment and DES implantation, paying special attention to the influence of diabetes status. The study found that hs-CRP ≥ 2 mg/L significantly related with MACCEs in Non-T2DM patients with CHD. In contrast, hs-CRP has a limited association with MACCEs in patients with T2DM, which suggests that hs-CRP alone may be insufficient, and alternative or complementary inflammatory biomarkers for risk stratification in T2DM patients should be explored.
Residual cardiovascular risk refers to the persistent risk of cardiovascular events that patients with CHD continue to face even after receiving standard treatments, such as statin-based lipid-lowering therapy and interventional procedures.2 Such risks typically span multiple dimensions, with the most extensively studied being residual cholesterol risk (ie, failure to achieve target lipid levels, such as LDL-C, despite statin therapy) and residual inflammatory risk (often reflected by hs-CRP).2 Large-scale clinical trials have demonstrated that statins can exert anti-inflammatory effects by reducing hs-CRP levels. For example, the JUPITER trial enrolled 17,802 participants with no history of cardiovascular disease, normal LDL-C levels (<130 mg/dL), but elevated hs-CRP levels (≥2 mg/L).22 It found that the median hs-CRP level in the rosuvastatin (20 mg/d) treatment group significantly decreased from a baseline of 4.2 mg/L to 1.8 mg/L (p<0.001), while the risk of major cardiovascular events was reduced by 44%.22 However, although statins can reduce hs-CRP, studies indicate that residual inflammatory risk persists. A significant proportion of patients still exhibit persistently elevated hs-CRP levels even after achieving the LDL-C targets recommended by guidelines.4 An analysis estimated that nearly 30% of patients receiving statin therapy, despite having LDL-C levels below 70 mg/dL, still had hs-CRP levels of 2 mg/L or higher.23 The LoDoCo2 study,24 which included 5,522 patients with chronic coronary artery disease, all on statin therapy with well-controlled LDL-C (median 1.8 mmol/L) but a median hs-CRP of 1.6 mg/L, found that adding low-dose colchicine (0.5 mg/d) significantly reduced the risk of cardiovascular events (HR=0.69, 95% CI: 0.57–0.83, p<0.001). This result indicates that residual inflammatory risk persists despite statin therapy, and additional benefits can be obtained by targeting other pathways of inflammation. Additionally, a collaborative analysis by Ridker et al included 31,245 statin-treated patients from three trials: PROMINENT, REDUCE-IT, and STRENGTH.5 The results demonstrated that baseline hs-CRP levels were a significant prognostic factor of future major adverse cardiovascular events (MACE), cardiovascular death, and all-cause mortality. The adjusted HR increased significantly with higher hs-CRP quartiles (p-trend < 0.001). This indicates that elevated hs-CRP levels remain associated with a high risk of MACE in statin-treated CHD patients. Therefore, investigating hs-CRP as a residual inflammatory risk during statin therapy will help optimize clinical medication. This study focuses on residual inflammatory risk by evaluating the role of hs-CRP—a simple, cost-effective, and easily measurable inflammatory biomarker—in CHD patients undergoing statin therapy and DES implantation. Specifically, it explores how T2DM influences the relationship between hs-CRP and MACCEs.
What is the biological mechanism behind the lack of association between hs-CRP and MACCEs in T2DM patients found in this study? There are three possible reasons. First, since T2DM patients are already in a state of chronic inflammation, hs-CRP may reach a “plateau phase”, where further increases fail to reflect additional risk signals. This saturation effect could weaken the sensitivity of hs-CRP as a prognostic marker for acute inflammation or cardiovascular events. Moreover, endothelial dysfunction, chronic immune system activation, and metabolic disorders (such as hyperglycemia and insulin resistance) present in T2DM patients may amplify inflammatory responses,8,25 thereby affecting the prognostic value of hs-CRP in this population. Secondly, the anti-inflammatory effects of statins may be partially offset in T2DM. Although there is currently a lack of systematic studies directly comparing the hs-CRP-lowering effects of statins between diabetic and non-diabetic patients, based on biological mechanisms, we hypothesize that diabetes-related inflammation involves multiple pathways,7,8 which extend beyond the scope of statins’ primary anti-inflammatory action via the 3-hydroxy-3-methylglutaryl coenzyme A reductase (HMGCR) pathway. Moreover, the hyperglycemic state in diabetic patients exacerbates oxidative stress,26 while the antioxidant capacity of statins is limited. Additionally, statins can impair insulin sensitivity and increase insulin resistance.2–6 This may counteract some of the beneficial effects of statins, including their anti-inflammatory properties. Thirdly, the dominant role of other pathological mechanisms in T2DM surpasses the contribution of inflammation alone. Studies consistently indicate that T2DM is associated with increased platelet activation and reactivity.27 This heightened platelet activity may be driven by various factors such as hyperglycemia, insulin resistance, and metabolic abnormalities.27 Activated platelets can promote thrombus formation, accelerate the progression of atherosclerosis, and contribute to plaque instability and rupture, thereby leading to acute coronary syndrome (ACS) and MACCEs.27 A study found that in patients with T2DM and CHD receiving dual antiplatelet therapy, high platelet reactivity was associated with an increased risk of long-term adverse cardiovascular events.28 Additionally, patients with T2DM exhibit various abnormalities in the coagulation system, leading to a chronic hypercoagulable state, which also increases the risk of thrombosis.29 Although inflammatory and thrombotic pathways are interconnected, the direct prothrombotic effects of enhanced platelet reactivity and coagulation abnormalities in T2DM represent significant non-inflammatory mechanisms contributing to plaque instability, which may operate independently of hs-CRP levels.30
It is noteworthy that other inflammatory biomarkers, such as interleukin-6 (IL-6), tumor necrosis factor-α (TNF-α), and fibrinogen, may provide additional prognostic advantages in patients with T2DM. Elevated serum IL-6 levels can predict long-term cardiovascular events in various patient populations, including high-risk individuals undergoing coronary angiography and those with stable coronary artery disease.31 Particularly in diabetic patients, elevated IL-6 levels are associated with an increased risk of major cardiovascular events such as MI, stroke, and cardiovascular death.31 It is noteworthy that the study by Shinohara et al32 demonstrated that elevated IL-6 levels independently predict the incidence of cardiovascular events in T2DM patients without comorbid structural heart disease. Furthermore, studies consistently demonstrate that serum TNF-α levels are significantly elevated in patients with T2DM compared to those with prediabetes and healthy control groups.33 Research indicates a positive correlation between TNF-α levels and glycemic markers such as fasting blood glucose and HbA1c in T2DM patients.33 Research by Jabber et al34 also reported that patients with both cardiovascular disease and diabetes had higher TNF-α levels compared to those with diabetes alone and the healthy control group, suggesting an association between this marker and the coexistence of CHD in diabetic patients. Fibrinogen is a key protein in the blood that plays a central role in the coagulation process, and as an acute-phase reactant, it can indicate the presence of inflammation.35 Research indicates that elevated fibrinogen levels are associated with increased complexity of coronary artery anatomy and patients with T2DM show a significantly higher incidence of MACCEs after PCI.35 A large cohort study further confirmed that in CHD patients undergoing PCI, fibrinogen levels are independently associated with long-term all-cause mortality and cardiac mortality, with this association being particularly pronounced in individuals with diabetes and prediabetes.36 Future research should focus on evaluating the potential of these alternative inflammatory markers, either used alone or in combination with hs-CRP and other clinical parameters, to improve the prediction of cardiovascular event risks in patients with T2DM and CHD undergoing statin therapy.
Several studies have specifically investigated how the presence of T2DM influences the prognostic value of hs-CRP in statins-treated patients with CHD. Notably, some findings align with the current study, revealing differential associations based on diabetic status.37 In a study conducted by Luigi M. Biasucci and colleagues, 251 individuals with ACS were enrolled, comprising 193 without diabetes and 58 with diabetes.9 Within the group of ACS patients diagnosed with T2DM, hs-CRP levels did not correlate with cardiovascular events over a one-year follow-up period. However, in Non-T2DM patients, hs-CRP levels were closely associated with 1-year cardiovascular events (p = 0.0012). Meisinger, C. et al, found similar results in an acute MI population (1,124 nondiabetic and 461 diabetic patients with a follow-up period of 28 days).38 Nonetheless, the two investigations were hampered by a limited sample size and a brief follow-up period, which curtailed the capacity to gauge the enduring prognostic value of hs-CRP in T2DM patients. It is noteworthy that our study involved a larger sample size (n=8628) and a longer follow-up period (2.4 years), arriving at conclusions similar to those of these two studies—hs-CRP does not appear to have a sufficiently strong association with the risk of cardiovascular events in diabetic patients. Additionally, Shahnam Sharif et al conducted a study with 1,679 T2DM patients and discovered that hs-CRP levels did not correlate with cardiovascular events in this population.39 Additionally, research on patients with triple-vessel disease (TVD) undergoing PCI with DES found that elevated hs-CRP was an independent predictor of long-term MACCEs in T2DM patients, but no such association was observed in non-diabetic individuals.10 This suggests that in the context of severe CHD requiring revascularization, the prognostic significance of hs-CRP may differ between diabetic and non-diabetic patients, reinforcing the view that diabetes may indeed alter the relationship between hs-CRP and cardiovascular outcomes. Lucci et al found that hs-CRP predicted hospitalization prognosis and two-year mortality in patients with acute MI with or without diabetes.40 However, lower hs-CRP thresholds were more effective in for assessing the association with mortality risk in nondiabetic patients than in diabetic patients.40 Therefore, while patients with T2DM tend to have higher levels of hs-CRP, this biomarker may not be as crucial for assessing the association with cardiovascular disease risk in individuals with diabetes compared to those without.
However, studies have shown that elevated hs-CRP levels are associated with cardiovascular events in patients with T2DM,10,39 which is inconsistent with our findings. This discrepancy may be partly due to differences in the definition of composite endpoint events and partly attributable to variations in the characteristics of the included populations (such as the influence of medication and the effects of diabetes treatment). For example, the population in this study received statin therapy, whereas Lei Guo et al6 did not report the medication status of their patients. Given that statins and other medications can affect hs-CRP levels,41 differences in medication use among different populations may lead to inconsistent results. Additionally, an unexpected finding from one study—that elevated hs-CRP may have a protective effect in non-diabetic ACS patients after PCI42—contradicts the general understanding of hs-CRP as a risk marker and warrants further investigation. The specific inflammatory environment during the acute phase of coronary events may be differentially regulated by diabetes, which could partly explain this observation. The current study focuses on populations receiving modern statin therapy and DES implantation, which may partially account for the discrepancies observed in studies employing different treatment regimens or older-generation stents. The study also confirmed that in T2DM patients, hs-CRP levels are closely related to the degree of blood glucose control. Moreover, diabetic patients with CHD generally have higher hs-CRP levels than non-diabetic CHD patients.43 This indicates that for individuals with diabetes, hs-CRP may primarily reflect the systemic inflammatory burden associated with their metabolic abnormalities.44 The heterogeneity of these findings highlights the complexity of the relationship between inflammation, diabetes, and cardiovascular outcomes in CHD patients undergoing PCI with DES. Factors such as differences in study design, patient characteristics (eg, ACS vs stable angina), duration of follow-up, and specific definitions of clinical endpoints may all contribute to the observed variations in results.
It is worth noting that the therapeutic effects of statins are influenced to some extent by genetic factors.45 For example, HMGCR is the target of statins, and its genetic variations are associated with differences in the response to LDL-C level reduction by statins.45 SLCO1B1 (Solute Carrier Organic Anion Transporter Family Member 1B1): this gene encodes the OATP1B1 transporter protein, which is primarily expressed in the liver and responsible for transporting various statin drugs into hepatocytes.46 Therefore, the SLCO1B1 genotype may be an important factor contributing to the variability in statin tolerance and potential efficacy in this study cohort, and its differential distribution between patients with and without T2DM could influence the study outcomes.47 T2DM is a complex metabolic disorder with its own genetic basis, which may influence the impact of genetic variations on the efficacy and tolerance of statins.48 Genetic factors affecting statin response may have different impacts on lipid-lowering effects or adverse reactions in patients with T2DM compared to those without T2DM.48 Genetic factors contribute to 35–50% of the phenotypic variation in hs-CRP levels.49 Genetic variants in the CRP gene itself (located on chromosome 1q23.2) play a significant role in regulating hs-CRP concentrations.49 Specific single nucleotide polymorphisms have been consistently associated with baseline hs-CRP concentrations.49 Therefore, the lack of association between hs-CRP and MACCEs observed in this study among T2DM patients receiving statin therapy may be related to genetic factors, which both alter the inflammatory response in diabetes and modify the effect of statins on this response.48 Future research should further elucidate the complex interactions among genetics, inflammation, statin therapy, diabetes, and cardiovascular outcomes to gain a more comprehensive understanding of the heterogeneity in statin response among patients with diabetes, as well as to identify novel biomarkers and therapeutic targets. Additionally, given that both residual cholesterol risk and residual inflammatory risk significantly impact the prognosis of CHD, residual cholesterol risk (reflected by LDL-C) and residual inflammatory risk (reflected by hs-CRP) may collectively influence the prognosis of CHD patients.2,5 However, our study did not identify a significant combined effect of these two factors (Table S9), which may be related to the sample size. Future research could further evaluate their interaction under different diabetic statuses and their potential for optimizing risk stratification.
In recent times, anti-inflammatory treatment has taken center stage as a promising avenue for addressing cardiovascular disease, particularly for patients who continue to experience elevated cardiovascular risks even when undergoing statin therapy. Studies have shown that targeting residual inflammation may provide additional benefits for these patients. Colchicine is a traditional alkaloid used to treat gout and other inflammatory diseases. It exerts its anti-inflammatory effects through multiple mechanisms, including disrupting microtubule assembly, inhibiting the NLRP3 inflammasome, reducing hs-CRP levels, suppressing platelet activity, and improving endothelial function.24 The COLCOT trial was the first large-scale study to evaluate the role of colchicine in secondary cardiovascular prevention,50 which showed that compared to the placebo group, patients in the colchicine group experienced a significant 23% reduction in the risk of MACCEs after an average follow-up of 22.6 months. Similarly, the LoDoCo-2 trial found that the colchicine group showed a 31% reduction in the risk of MACCEs among patients with stable coronary artery disease.24 These findings suggest that colchicine represents a promising and cost-effective therapeutic option for targeting inflammation in cardiovascular disease, particularly in secondary prevention. Low-dose colchicine (0.5–1.0 mg/day) is generally considered safe. However, common side effects include gastrointestinal discomfort. Due to its narrow therapeutic window, caution is advised when using colchicine in patients with severe kidney or liver disease. The CANTOS study51 demonstrated that the use of canakinumab (an anti-inflammatory monoclonal antibody targeting IL-1β) significantly reduced inflammation levels and markedly decreased the incidence of cardiovascular events, without affecting LDL-C levels. These findings further suggest that inflammation control may be a crucial component of cardiovascular risk management. In the future, combining lipid-lowering drugs with anti-inflammatory therapy may become a powerful strategy to enhance the prevention of cardiovascular diseases.
The advantages of this research include its extensive sample size, and clearly defined study population. However, some limitations remain. Firstly, it was a single-center study and the external generalizability and replication of the results may be limited. The findings may not be generalizable to western populations or diverse ethnic groups. Further validation in multi-center or international cohorts is needed. Nonetheless, it is worth mentioning that our crew has a track record of delivering solid research using data from a single source, which has significantly boosted insights into how cardiovascular diseases develop and are treated.52–54 Second, hs-CRP was recorded only once at admission, and changes in hs-CRP were not recorded during the follow-up period. However, inflammation levels fluctuate over time. Future studies should track hs-CRP longitudinally. Third, the study focused mainly on hs-CRP and did not consider other inflammatory markers that may have prognostic value (eg, IL-6, TNF-α, etc)., which may have missed more prognostic biomarkers. Fourth, there is a lack of objective methods to assess adherence to drugs therapy (including statin). Adherence was evaluated based on patient self-reports and physician-recorded prescriptions during follow-up, rather than through objective measures such as pill counts, pharmacy refill records, or serum drug levels. This approach may introduce variability or bias, potentially underestimating the impact of non-adherence on the relationship between residual inflammatory risk (hs-CRP) and MACCEs. Although standardized follow-up protocols and a large sample size may have mitigated some of these effects, future studies incorporating quantitative adherence metrics (such as medication possession ratios or biomarker-based validation) could provide a more robust assessment of these associations. Fifth, this study did not include information on the intensity of statin therapy, preventing us from stratifying patients by statin intensity or adjusting for it as a confounding factor. Future research should obtain detailed data on statin intensity to further clarify its role as a potential confounder in the relationship between residual inflammatory risk and cardiovascular outcomes. Sixth, our dataset did not collect information on adjunctive anti-inflammatory treatments such as colchicine or PCSK9 inhibitors. Future studies should prioritize assessing their importance as potential confounding factors. Seventh, the median follow-up period of 2.4 years is relatively short for assessing long-term MACCEs, and future studies will require longer follow-up durations. Eighth, this study could not provide complete data on insulin usage and the course of diabetes. The absence of these factors may have limited our comprehensive assessment of the prognostic value heterogeneity of hs-CRP in T2DM subgroups. Future research needs to incorporate more detailed diabetes-related variables (such as insulin usage and disease duration).55,56
Conclusion
This study suggests that in CHD patients receiving contemporary statin therapy following DES implantation, higher levels of hs-CRP may be associated with future MACCEs in non-T2DM patients, while this association should be cautiously considered in T2DM patients. Alternative inflammatory markers should be explored in T2DM. Hs-CRP, a key inflammatory marker, varies significantly with diabetes status, highlighting the joint impact of hyperglycemia and inflammation on cardiovascular risk and guiding targeted use of inflammatory biomarkers in clinical risk assessment.
Abbreviations
ACS, acute coronary syndrome; BMI, body mass index; CABG, coronary artery bypass grafting; CCB, calcium channel blockers; CHD, coronary heart disease; COPD, chronic obstructive pulmonary disease; CI, confidence intervals; DAPT, dual antiplatelet therapy; HbA1c, hemoglobin A1c; hs-CRP, high-sensitivity C-reactive protein; HDL-C, high-density lipoprotein cholesterol; HR, hazard ratio; IL-6, interleukin-6; LASSO, Least Absolute Shrinkage and Selection Operator; LDL-C, low-density lipoprotein cholesterol; Lp(a), lipoprotein(a); LM, left main; LVEF, left ventricular ejection fraction; MACCEs, major adverse cardiovascular and cerebrovascular events; MI, myocardial infarction; PCI, percutaneous coronary intervention; PVD, peripheral vascular disease; SLCO1B1, Solute Carrier Organic Anion Transporter Family Member 1B1; TNF-α, tumor necrosis factor-α; TC, total cholesterol; T2DM, type 2 diabetes mellitus; WBC, white blood cells.
Ethics Approval and Informed Consent
The study process was in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Fuwai hospital. All subjects provided informed written consent for long-term follow-up before intervention.
Consent for Publication
The manuscript was approved by all authors for publication.
Acknowledgments
Xinyue Chen, Hao-Yu Wang, and Wanqing Sun are co-first authors for this study. Kefei Dou and Hao-Yu Wang are co-correspondence authors for this study.
Funding
This work was supported by Noncommunicable Chronic Diseases-National Science and Technology Major Project (Grant Number: 2023ZD0513900), the Fundamental Research Funds for the Central Universities (Grant Number: 3332024033), CAMS Innovation Fund for Medical Science (Grant Number: 2021-I2M-1-008), the National High Level Hospital Clinical Research Funding (Grant Number: 2023-GSP-RC-05 and 2023-GSP-QN-34).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Safiri S, Karamzad N, Singh K, et al. Burden of ischemic heart disease and its attributable risk factors in 204 countries and territories, 1990-2019. Eur J Prev Cardiol. 2022;29(2):420–431. doi:10.1093/eurjpc/zwab213
2. Hoogeveen RC, Ballantyne CM. Residual Cardiovascular Risk at Low LDL: remnants, Lipoprotein(a), and Inflammation. Clin Chem. 2021;67(1):143–153. doi:10.1093/clinchem/hvaa252
3. Ridker PM, Lei L, Louie MJ, et al. Inflammation and cholesterol as predictors of cardiovascular events among 13 970 contemporary high-risk patients with statin intolerance. Circulation. 2024;149(1):28–35. doi:10.1161/CIRCULATIONAHA.123.066213
4. Xie S, Galimberti F, Olmastroni E, et al. Effect of lipid-lowering therapies on C-reactive protein levels: a comprehensive meta-analysis of randomized controlled trials. Cardiovasc Res. 2024;120(4):333–344. doi:10.1093/cvr/cvae034
5. Ridker PM, Bhatt DL, Pradhan AD, et al. Inflammation and cholesterol as predictors of cardiovascular events among patients receiving statin therapy: a collaborative analysis of three randomised trials. Lancet Lond Engl. 2023;401(10384):1293–1301. doi:10.1016/S0140-6736(23)00215-5
6. Pellegrini V, La Grotta R, Carreras F, et al. Inflammatory trajectory of type 2 diabetes: novel opportunities for early and late treatment. Cells. 2024;13(19):1662. doi:10.3390/cells13191662
7. Henriksbo BD, Schertzer JD. Is immunity a mechanism contributing to statin-induced diabetes? Adipocyte. 2015;4(4):232–238. doi:10.1080/21623945.2015.1024394
8. Mirza S, Hossain M, Mathews C, et al. Type 2-diabetes is associated with elevated levels of TNF-alpha, IL-6 and adiponectin and low levels of leptin in a population of Mexican Americans: a cross-sectional study. Cytokine. 2012;57(1):136–142. doi:10.1016/j.cyto.2011.09.029
9. Biasucci LM, Liuzzo G, Della Bona R, et al. Different apparent prognostic value of hsCRP in type 2 diabetic and nondiabetic patients with acute coronary syndromes. Clin Chem. 2009;55(2):365–368. doi:10.1373/clinchem.2008.119156
10. Guo L, Lv H, Wang J, et al. Predictive value of high sensitivity C-reactive protein in three-vessel disease patients with and without type 2 diabetes. Cardiovasc Diabetol. 2023;22(1):91. doi:10.1186/s12933-023-01830-7
11. Wang HY, Mo R, Guan CD, et al. Establishing the optimal duration of DAPT following PCI in high-risk TWILIGHT-like patients with acute coronary syndrome. Catheter Cardiovasc Interv off J Soc Card Angiogr Interv. 2022;100(4):593–595. doi:10.1002/ccd.30363
12. Wang HY, Yin D, Zhao YY, et al. Prognostic and practical validation of ESC/EACTS high ischemic risk definition on long-term thrombotic and bleeding events in contemporary PCI patients. J Atheroscler Thromb. 2022;29(4):502–526. doi:10.5551/jat.60129
13. Shi B, Wang HY, Liu J, et al. Prognostic Value of Machine-Learning-Based PRAISE Score for Ischemic and Bleeding Events in Patients With Acute Coronary Syndrome Undergoing Percutaneous Coronary Intervention. J Am Heart Assoc. 2023;12(7):e025812. doi:10.1161/JAHA.122.025812
14. Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. Circulation. 2012;126(16):2020–2035. doi:10.1161/CIR.0b013e31826e1058
15. Sacco RL, Kasner SE, Broderick JP, et al. An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013;44(7):2064–2089. doi:10.1161/STR.0b013e318296aeca
16. Hicks KA, Mahaffey KW, Mehran R, et al. 2017 Cardiovascular and Stroke Endpoint Definitions for Clinical Trials. Circulation. 2018;137(9):961–972. doi:10.1161/CIRCULATIONAHA.117.033502
17. Yu M, Yf Y, Yang F, et al. Residual inflammatory risk in outcomes of Chinese patients after percutaneous coronary intervention. JACC Asia. 2024;4(8):636–638. doi:10.1016/j.jacasi.2024.05.004
18. Takahashi N, Dohi T, Endo H, et al. Residual Inflammation Indicated by High-Sensitivity C-Reactive Protein Predicts Worse Long-Term Clinical Outcomes in Japanese Patients after Percutaneous Coronary Intervention. J Clin Med. 2020;9(4):1033. doi:10.3390/jcm9041033
19. Kamath DY, Xavier D, Sigamani A, Pais P. High sensitivity C-reactive protein (hsCRP) & cardiovascular disease: an Indian perspective. Indian J Med Res. 2015;142(3):261–268. doi:10.4103/0971-5916.166582
20. Sabanayagam C, Shankar A, Lee J, Wong TY, Tai ES. Serum C-reactive protein level and prehypertension in two Asian populations. J Hum Hypertens. 2013;27(4):231–236. doi:10.1038/jhh.2011.117
21. American Diabetes Association. and diagnosis of diabetes: standards of medical care in diabetes—2021. Diabetes Care. 2020;44(Supplement_1):S15–33. doi:10.2337/dc21-S002
22. Ridker PM, Danielson E, Fonseca FAH, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med. 2008;359(21):2195–2207. doi:10.1056/NEJMoa0807646
23. Pradhan AD, Aday AW, Rose LM, Ridker PM. Residual Inflammatory Risk on Treatment With PCSK9 Inhibition and Statin Therapy. Circulation. 2018;138(2):141–149. doi:10.1161/CIRCULATIONAHA.118.034645
24. Nidorf SM, Fiolet ATL, Mosterd A, et al. Colchicine in Patients with Chronic Coronary Disease. N Engl J Med. 2020;383(19):1838–1847. doi:10.1056/NEJMoa2021372
25. Sabapathi SP, Selvaraj K, Balasubramaniyan AG. Assessment of Endothelial Dysfunction in T2DM: a Doppler Ultrasound Study Correlated with CRP Levels, Glycemic Control, and BMI. International Journal of the Cardiovascular Academy. 2024;10(3):62–69. doi:10.4274/ijca.2024.85856.
26. Caturano A, Rocco M, Tagliaferri G, et al. Oxidative Stress and Cardiovascular Complications in Type 2 Diabetes: from Pathophysiology to Lifestyle Modifications. Antioxid Basel Switz. 2025;14(1):72. doi:10.3390/antiox14010072
27. Mahmoodian R, Salimian M, Hamidpour M, Khadem-Maboudi AA, Gharehbaghian A. The effect of mild agonist stimulation on the platelet reactivity in patients with type 2 diabetes mellitus. BMC Endocr Disord. 2019;19(1):62. doi:10.1186/s12902-019-0391-2
28. Angiolillo DJ, Bernardo E, Sabaté M, et al. Impact of platelet reactivity on cardiovascular outcomes in patients with type 2 diabetes mellitus and coronary artery disease. J Am Coll Cardiol. 2007;50(16):1541–1547. doi:10.1016/j.jacc.2007.05.049
29. Roberts JD, Oudit GY, Fitchett DH. Acute coronary thrombosis in a patient with diabetes and severe hyperglycemia. Can J Cardiol. 2009;25(6):e217–219. doi:10.1016/S0828-282X(09)70113-8
30. Rodriguez BAT, Johnson AD. Platelet Measurements and Type 2 Diabetes: investigations in Two Population-Based Cohorts. Front Cardiovasc Med. 2020;7:118. doi:10.3389/fcvm.2020.00118
31. Herder C, Schöttker B, Rothenbacher D, et al. Interleukin-6 in the prediction of primary cardiovascular events in diabetes patients: results from the ESTHER study. Atherosclerosis. 2011;216(1):244–247. doi:10.1016/j.atherosclerosis.2011.01.041
32. Shinohara T, Yufu K, Kondo H, et al. Interleukin-6 as an independent predictor of future cardiovascular events in patients with type-2 diabetes without structural heart disease. J Clin Exp Cardiol. 2012;3(09). doi:10.4172/2155-9880.1000209.
33. Ezzat Abd El-Raouf Mohamed M, Khalil Ahmed Y, Mohammed Ghamry E, Abd El-Hamid Khedr M. STUDY OF SERUM TUMOR NECROSIS FACTOR ALPHA LEVEL IN PREDIABETICS AND TYPE 2 DIABETIC EGYPTIAN PATIENTS. Al-Azhar Med J. 2022;51(2):1193–1198. doi:10.21608/amj.2022.230481
34. Jabber HN, Charfeddine B, Abbas HJ. Evaluation of Tumor Necrosis Factor Alpha, Insulin, glucose, HbA1c% and HOMA-IR as Predictors for Cardiovascular Diseases in Patients with Type 2 Diabetes. Pharmacognosy Journal. 2024;16(1):195–201. doi:10.5530/pj.2024.16.27
35. Su H, Cao Y, Chen Q, et al. The association between fibrinogen levels and severity of coronary artery disease and long-term prognosis following percutaneous coronary intervention in patients with type 2 diabetes mellitus. Front Endocrinol. 2023;14:1287855. doi:10.3389/fendo.2023.1287855
36. Yuan D, Jiang P, Zhu P, et al. Prognostic value of fibrinogen in patients with coronary artery disease and prediabetes or diabetes following percutaneous coronary intervention: 5-year findings from a large cohort study. Cardiovasc Diabetol. 2021;20(1):143. doi:10.1186/s12933-021-01335-1
37. Sattar N. High sensitivity C-reactive protein in cardiovascular disease and type 2 diabetes: evidence for a clinical role? Br J Diabetes Vasc Dis. 2006;6(1):5–8. doi:10.1177/14746514060060010101
38. Meisinger C, Heier M, von Scheidt W, Kuch B. The MONICA/KORA Myocardial Infarction Registry. Admission C-reactive protein and short- as well as long-term mortality in diabetic versus non-diabetic patients with incident myocardial infarction. Clin Res Cardiol. 2010;99(12):817–823. doi:10.1007/s00392-010-0193-z
39. Sharif S, Van der Graaf Y, Cramer MJ, et al. Low-grade inflammation as a risk factor for cardiovascular events and all-cause mortality in patients with type 2 diabetes. Cardiovasc Diabetol. 2021;20(1):220. doi:10.1186/s12933-021-01409-0
40. Lucci C, Cosentino N, Genovese S, et al. Prognostic impact of admission high-sensitivity C-reactive protein in acute myocardial infarction patients with and without diabetes mellitus. Cardiovasc Diabetol. 2020;19:183. doi:10.1186/s12933-020-01157-7
41. Kandelouei T, Abbasifard M, Imani D, et al. Effect of Statins on Serum level of hs-CRP and CRP in Patients with Cardiovascular Diseases: a Systematic Review and Meta-Analysis of Randomized Controlled Trials. Mediators Inflamm. 2022;2022:8732360. doi:10.1155/2022/8732360
42. Zhang L, Zhang Y, Deng F, Chu C, Yuan Z, Zhang M. Evaluation of hs-CRP is Associated with lower 2-year MACCEs Following Percutaneous Coronary Intervention in Non-diabetic Patients with Acute Coronary Syndrome. 2022. doi:10.21203/rs.3.rs-2034387/v1
43. Dayoub A, Khayat MI, Zrieki A. Association of high sensitivity c-reactive protein (Hs-CRP) with poor glycaemic control and coronary heart disease in type 2 diabetes mellitus. Res J Pharm Technol. 2023;16(1):193–199. doi:10.52711/0974-360X.2023.00036
44. Anubha Mahajan AM, Rubina Tabassum RT, Sreenivas Chavali SC, et al. High-sensitivity C-reactive protein levels and type 2 diabetes in urban North Indians J. Clin. Endocrinol. Metab. 2009;94(6): 2123–2127. doi:10.1210/jc.2008-2754
45. Postmus I, Verschuren JJW, de Craen AJM, et al. Pharmacogenetics of statins: achievements, whole-genome analyses and future perspectives. Pharmacogenomics. 2012;13(7):831–840. doi:10.2217/pgs.12.25
46. Canestaro WJ, Austin MA, Thummel KE. Genetic factors affecting statin concentrations and subsequent myopathy: a HuGENet systematic review. Genet Med off J Am Coll Med Genet. 2014;16(11):810–819. doi:10.1038/gim.2014.41
47. Kitzmiller JP, Mikulik EB, Dauki AM, Murkherjee C, Luzum JA. Pharmacogenomics of statins: understanding susceptibility to adverse effects. Pharmacogenomics Pers Med. 2016;9:97–106. doi:10.2147/PGPM.S86013
48. Laakso M, Fernandes Silva L. Statins and risk of type 2 diabetes: mechanism and clinical implications. Front Endocrinol. 2023;14:1239335. doi:10.3389/fendo.2023.1239335
49. Mahajan A, Tabassum R, Chavali S, et al. Common variants in CRP and LEPR influence high sensitivity C-reactive protein levels in North Indians. PLoS One. 2011;6(9):e24645. doi:10.1371/journal.pone.0024645
50. Tardif JC, Kouz S, Waters DD, et al. Efficacy and Safety of Low-Dose Colchicine after Myocardial Infarction. N Engl J Med. 2019;381(26):2497–2505. doi:10.1056/NEJMoa1912388
51. Ridker PM, Everett BM, Thuren T, et al. Antiinflammatory therapy with canakinumab for atherosclerotic disease. N Engl J Med. 2017;377(12):1119–1131. doi:10.1056/NEJMoa1707914
52. Wang HY, Dou KF, Guan C, et al. New Insights Into Long- Versus Short-Term Dual Antiplatelet Therapy Duration in Patients After Stenting for Left Main Coronary Artery Disease: findings From a Prospective Observational Study. Circ Cardiovasc Interv. 2022;15(6):e011536. doi:10.1161/CIRCINTERVENTIONS.121.011536
53. Wang HY, Xu B, Dou K, et al. Implications of Periprocedural Myocardial Biomarker Elevations and Commonly Used MI Definitions After Left Main PCI. JACC: Cardiovasc Interv. 2021;14(15):1623–1634. doi:10.1016/j.jcin.2021.05.006
54. Wang HY, Zhang R, Dou K, et al. Left main bifurcation stenting: impact of residual ischaemia on cardiovascular mortality. Eur Heart J. 2023;44(41):4324–4336. doi:10.1093/eurheartj/ehad318
55. Huang Z Sun A. Metabolism, inflammation, and cardiovascular diseases from basic research to clinical practice. Cardiol Plus. 2023;8(1):4–5. doi:10.1097/CP9.0000000000000037
56. Cheng J, Wang HY, Song C, et al. Optimizing long-term cardiovascular risk stratification: integrating biomarkers into the very high-risk ASCVD definition in Asian patients. Am J Prev Cardiol. 2025;16(22). doi:10.1016/j.ajpc.2025.100965):100965.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation of Statin Indication and Dose Intensification Among Type 2 Diabetic Patients at a Tertiary Hospital
Fisseha PY, Baye AM, Beyene MG, Makonnen E
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1157-1169
Published Date: 7 March 2024
Serum FGF23 and DPP4 Levels as Biomarkers for Coronary Artery Disease Severity in Type 2 Diabetic Patients with Coronary Heart Disease
Zhong X, Liang Z, Liao H, Zhan Y, Li G, Wu H, Li J
International Journal of General Medicine 2025, 18:1757-1764
Published Date: 28 March 2025