")
Back to Journals » Clinical Ophthalmology » Volume 19
Human Factors Studies to Assess the Usability of the Faricimab Prefilled Syringe
Authors Barakat MR , Kwong Jr HM, Marcon G, O'Leary OE, Paris LP, Schneider P, Tang Y , Graff JM
Received 28 October 2024
Accepted for publication 10 January 2025
Published 6 February 2025 Volume 2025:19 Pages 395—406
DOI https://doi.org/10.2147/OPTH.S503060
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mark R Barakat,1,2 Henry M Kwong Jr,2,3 Gelson Marcon,4 Olivia E O’Leary,4 Liliana P Paris,5 Petrick Schneider,4 Yannan Tang,5 Jordan M Graff2,6,7
1Retina Macula Institute of Arizona, Scottsdale, AZ, USA; 2Department of Ophthalmology, University of Arizona College of Medicine – Phoenix, Phoenix, AZ, USA; 3Associated Retina Consultants, Phoenix, AZ, USA; 4F. Hoffmann-La Roche AG, Basel, Switzerland; 5Genentech, Inc., San Francisco, CA, USA; 6Barnet Dulaney Perkins Eye Center, Phoenix, AZ, USA; 7Ophthalmology Division, Creighton University School of Medicine, Phoenix, Arizona, USA
Correspondence: Jordan M Graff, Barnet Dulaney Perkins Eye Center, Phoenix, AZ, USA, Tel +1 480 843 1868, Email [email protected]
Purpose: Faricimab, the first bispecific antibody designed for intraocular use, is approved for the treatment of neovascular age-related macular degeneration (nAMD), diabetic macular edema (DME), and retinal vein occlusion (RVO). Here, we report the usability of a novel faricimab 6 mg pre-filled syringe (PFS) configuration that has been designed specifically for intravitreal use.
Patients and Methods: A simulated-use human factors validation study enrolling 15 retina specialists and 15 ophthalmic assistants was conducted in a market research facility configured to represent an ophthalmology clinic. Participants’ ability to complete tasks related to package handling, dose preparation, and injection of a faricimab 6 mg dose into a polymer eye using the PFS was assessed. In a second Phase 3b, single-arm, actual-use study, the ability of seven retina specialists and six ophthalmic assistants to prepare and administer the PFS in accordance with the instructions for use was assessed. Injections were performed into single eyes of 35 patients with nAMD or DME in three US clinics and patients were followed for 7 days for safety reporting (ClinicalTrials.gov identifier: NCT05569148).
Results: In the simulated-use study, most retina specialists and ophthalmic assistants completed all tasks deemed essential for PFS preparation and administration correctly and without error. Of the 22 tasks, the pass rate was 86.7– 100%; 16 tasks had a pass rate of 100%. No use errors were observed during the actual-use study. One patient experienced one mild adverse event of eye irritation that resolved the same day and was deemed unrelated to the study drug.
Conclusion: Participants were able to safely and correctly prepare and administer a faricimab 6 mg dose using the PFS in accordance with the instructions for use, under realistic conditions representing the real world. The faricimab 6 mg PFS may therefore offer a more convenient, safe-handling alternative to vial administration.
Keywords: intravitreal injection, medical device, retina specialist, human factors validation study, anti-vascular endothelial growth factor therapy
Introduction
Intravitreal injections with anti-vascular endothelial growth factor (anti-VEGF) agents are recommended first-line treatment for patients with retinal vascular diseases, providing improvements in visual outcomes in patients at risk of irreversible blindness within the first year of treatment.1–6 Faricimab (Vabysmo™, Genentech, San Francisco, CA, USA), the first bispecific antibody developed for intraocular use, targets both angiopoietin-2 and VEGF-A to promote vascular stability by reducing vascular leakage, neovascularization, and inflammation.7–11 The efficacy and safety profile of faricimab has been well characterized across six global, multicenter, phase 3 studies, resulting in marketing approvals in nearly 100 countries worldwide, including for the treatment of patients with neovascular age-related macular degeneration (nAMD) and diabetic macular edema (DME) in the USA, Japan, and Europe in 2022, and retinal vein occlusion (RVO) in the USA in 2023 and in Japan and Europe in 2024.12–23
Since the first faricimab approval in 2022, more than 6 million doses of faricimab have been distributed in over 100 countries.24 Most intravitreal therapies, when first approved, are administered by preparing syringes from vials of drug solution; however, this is a time-consuming, multistep process that requires care to ensure dose accuracy and aseptic preparation. To minimize the burden of intravitreal administration on busy eye clinics and to reduce the risk of contamination, prefilled syringe (PFS) configurations are often preferred to vials, offering greater convenience as well as the potential to enhance efficiency and improve patient safety.25 PFS configurations require fewer steps and less time for dose preparation than vial configurations for intravitreal injection, which may contribute to safer handling by reducing the potential for iatrogenic contamination and needlestick injuries to the user.26–30
The number of intravitreal injections administered each year is predicted to reach 10 million by 2025,31 yet most syringes and needles used for intravitreal administration have not been developed specifically for ophthalmic use.26,32 The design of the syringe and needle used for intravitreal injection is critical to ensure that treatments can be administered smoothly and safely. Typically, PFS configurations for anti-VEGF therapies are provided without an injection needle, meaning that, in accordance with prescribing information, any 30-gauge × ½ inch sterile injection needle can be used.33–36 In 2024, the US Food and Drug Administration (FDA) approved a novel faricimab 6 mg PFS for use in patients with nAMD, DME, and RVO.37 The faricimab 6 mg PFS is designed specifically for ophthalmic use, and includes a co-packaged 30-gauge × ½ inch Luer-lock injection filter needle. The syringe has a baked-on silicone coating, which is associated with much lower particulate formation over time compared with syringes with the sprayed-on silicone that is typically used in the vial configuration.38 This feature aims to mitigate the risk of silicone contamination of the drug product and facilitate a smooth injection procedure.39,40 The faricimab 6 mg PFS has a capacity of 0.5 mL and has a distinct 0.05 mL dose mark to facilitate a tight control of dosing volume, with a view to reducing the risk of dosing inaccuracies that have been reported with larger volume syringes with wide dose marks.26,41–43 Finally, unlike standard 30-gauge needles used for intravitreal injections, the co-packaged injection filter needle has an extra-thin walled design to optimize both user and patient experience. With the extra thin-walled design, the outer diameter of the needle (ie the gauge) is left unchanged, but the inner lumen diameter is increased by more than 30%44 (Figure 1). The resultant increased cross-sectional area translates to an improvement in flow characteristics, which generally translates to a lower required injection force and less time to inject, increasing both user and patient comfort.26,44
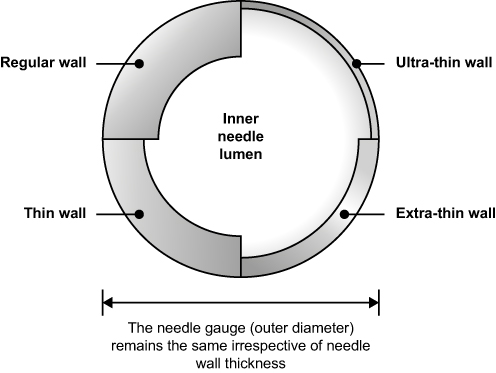 |
Figure 1 The impact of needle wall thickness on inner needle lumen diameter. Notes: Diagram showing the cross-sectional area of a needle and the impact of varying types of needle design (regular, thin-wall, extra-thin wall, and ultra-thin wall) on inner lumen diameter. |
As with all medical devices, the clinical development of PFS configurations is subject to stringent regulation by healthcare regulators. It is recommended that human factors engineering processes are followed during medical device development, meaning that an understanding of human behavior, abilities, and limitations should be applied in designing the device, as well as any other components (eg the instructions for use) that the users will interact with.45,46 An iterative approach to development is recommended, with evaluations conducted throughout the development process to assess how the intended users (eg healthcare professionals) interact with the device, and how the design of the device (including packaging, label, and instructions) or the use environment influences these interactions. Once these components have been optimized, a simulated-use human factors validation study is conducted to demonstrate that the device can be used safely and correctly by the intended users under conditions that represent real-world use.46
Herein, we describe results from two studies evaluating the usability of the faricimab 6 mg PFS that were conducted as part of a comprehensive human factors engineering program. First, we describe the simulated-use human factors validation study that was conducted under conditions representative of real-world use. Second, we describe an actual-use clinical study that was conducted to evaluate the ability of retina specialists and ophthalmic assistants to prepare and successfully administer a faricimab 6 mg dose to patients using the PFS in real-life ophthalmology clinic settings.
Materials and Methods
Faricimab 6 mg PFS User Interface
The faricimab 6 mg PFS is a single use, siliconized 0.5 mL glass syringe with a rubber stopper, plunger rod, and finger grip (Figure 2). Each PFS contains 21 mg faricimab in 0.175 mL solution. This provides a usable amount to deliver a single dose of 0.05 mL solution containing 6 mg of faricimab. The sterile PFS is contained in a sealed thermoformed tray. The sterile injection filter needle is contained in a sealed blister pack. Both components are packaged in a carton that is secured with tamper-evident seals. To prepare the dose, the user opens the syringe packaging and removes the syringe cap. The extra-thin-walled 30-gauge × ½ inch injection filter needle must then be aseptically removed from its packaging and attached securely to the syringe Luer lock before removal of the needle cap. The transparent glass syringe allows inspection of the drug product and removal of air bubbles. To set the dose, the lower edge of the rubber stopper dome is aligned with the 0.05 mL dose mark and the injection is then delivered by pushing the plunger to the bottom of the syringe.
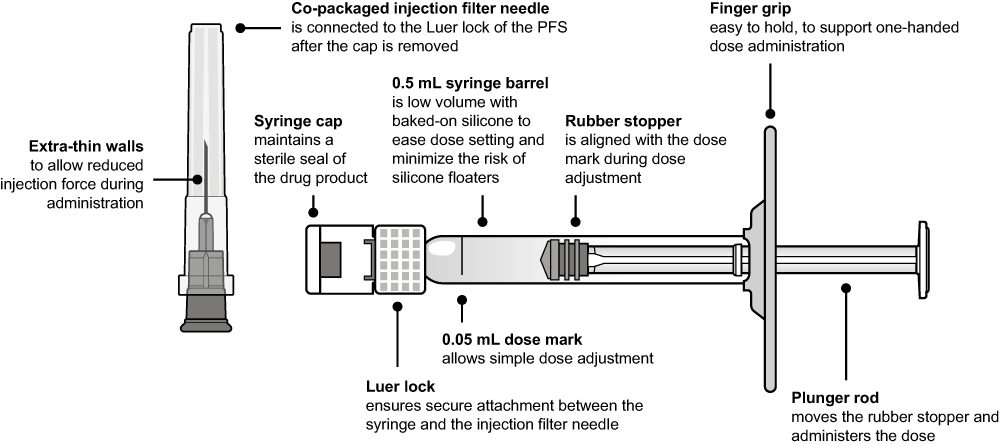 |
Figure 2 Components of the faricimab PFS. Abbreviation: PFS, prefilled syringe. |
In accordance with International Electrotechnical Commission 62366–1 usability standard and FDA recommendations for human factors engineering of medical devices, the tested user interface comprises all components that users interact with when preparing and using the device,46,47 including the packaged and labeled PFS, the co-packaged injection filter needle, and the package insert containing the faricimab prescribing information and the instructions for use.
Simulated-Use Validation Study
The objective of the simulated-use human factors validation study was to assess the usability of the faricimab 6 mg PFS in a representative, simulated-use environment by evaluating the performance of retina specialists and ophthalmic assistants on ‘critical tasks’, which are tasks deemed essential for PFS administration and tasks in which use errors could cause harm to the patient or user.
The study was conducted at three sites in the USA in June 2022. All assessments took place in a market research facility room configured and equipped to represent an ophthalmology clinic. Simulated injections were performed into a transparent polymer eye set into a dummy head. The polymer eyes were filled with a viscous liquid that simulates the human eye’s vitreous humor. Participants were able to move around the dummy head, and the placement of the dummy head also allowed participants to stand or be seated during dose preparation and administration. All supplies typically required to perform an intravitreal injection were provided.
Enrolled participants included practicing licensed US retina specialists who routinely perform intravitreal injections and ophthalmic assistants routinely involved in intravitreal therapy preparation in US clinics. Retina specialists previously involved in testing the faricimab 6 mg PFS were excluded.
Participants were observed in two simulated-use scenarios by two human factors engineers, one assuming the role of observer and one assuming the role of moderator. In scenario one, participants were asked to imagine that they needed to administer an intravitreal injection of a new drug product (faricimab) to a patient, without receiving training or a demonstration on device use from a company representative. All retina specialists and ophthalmic assistants performed tasks related to the handling of the packaging and device preparation. In addition, all retina specialists also performed tasks related to dose setting and injection of faricimab 6 mg using the PFS. In scenario two, all participants were presented with two packaged PFSs, one intact and one with a broken tamper-evident seal and partially opened tray. Participants were told to inspect the packaging to assess if the product was safe to be used.
Performance on critical tasks during the preparation and administration of faricimab 6 mg using the PFS was recorded, including the documentation of any outcome that deviated from the intended use of the device. Based on an established acceptance criterion, the outcomes of tasks were marked as “success”, “difficulty”, “close call”, or “use error” by both the moderator and the observer. The moderator conducted interviews with the study participants after the completion of both scenarios to determine the root cause of any use errors or difficulties during each critical task. Photographs of the PFS were taken during dose setting and after dose delivery, for evaluation. Video cameras also captured a wide-angle view of the room and a close-up view of the dose administration.
After completion of the simulated-use scenarios, participants completed a series of knowledge tasks (tasks that could not be assessed through observation or were not verbalized during simulated use) to evaluate their ability to locate and understand information in the instructions for use or on the PFS packaging. Knowledge tasks were classified as “success”, “difficulty”, or “unsuccessful” and responses to questions were classed as “correct”, “partially correct”, or “incorrect”.
Actual-Use Study
The actual-use study was a phase 3b, single-arm, open-label, multicenter study carried out at three sites in the USA between October 2022 and November 2022 (ClinicalTrials.gov identifier: NCT05569148). The primary objective was to observe whether retina specialists and ophthalmic assistants could correctly prepare and administer a faricimab 6 mg intravitreal injection to patients with nAMD or DME using the PFS in accordance with the instructions for use, in a real-life clinical environment.
All assessments were conducted in outpatient ophthalmology clinics. Study participants included licensed, practicing US retina specialists with previous experience of performing intravitreal injections of faricimab using the vial configuration. Ophthalmic assistants only participated in dose preparation if they were normally involved in the preparation of intravitreal injections at the clinic. Adult patients with a diagnosis of nAMD or DME in one or both eyes who were deemed eligible for intravitreal treatment with faricimab therapy were included. Only one eye was selected as the study eye, as determined by the investigator.
Eligible patients were screened in the 30 days before study day 1. Retina specialists and ophthalmic assistants were asked to familiarize themselves with the faricimab 6 mg PFS instructions for use in the 3 days prior to study day 1; no other demonstration or training was provided. On study day 1, study participants were asked to prepare and administer faricimab 6 mg by PFS to patients under the observation of two human factors observers. The observers documented performance on critical tasks using an assessment checklist without interrupting or interfering with the procedure. All administration procedures were also captured on video for further analysis. To assess the accuracy of dose setting, retina specialists were asked to pause and show the syringe to the observers and allow for video recording. Follow-up interviews were conducted with study participants after the completion of each intravitreal injection. Patients were followed for safety reporting for 7 days and safety telephone calls were conducted on day 3 and day 7 to elicit and record information related to all adverse events occurring during the study period. All data were analyzed using descriptive statistics.
Ethical Conduct of Studies
The studies were conducted in accordance with the principles of good clinical practice and consensus ethical principles derived from the Declaration of Helsinki and Council for International Organizations of Medical Sciences international ethical guidelines. Institutional review board/ethics committee (IRB/EC) approval was obtained for both studies before the studies began (Advarra IRB, Columbia, MD, USA). Written informed consent was obtained from all retina specialists, ophthalmic assistants, and patients participating in the studies.
Results
Simulated-Use Validation Study
A total of 15 retina specialists and 15 ophthalmic assistants participated in the simulated-use validation study. The majority of participants (retina specialists, n = 13; ophthalmic assistants, n = 9) had more than 5 years of experience with the preparation or administration of intravitreal injections. Most retina specialists had previous experience of administering similar marketed ocular PFSs.
Almost all retina specialists and ophthalmic assistants completed all of their respective critical tasks correctly and without any use problems. Of the 22 tasks, 16 had a pass rate of 100% (Table 1). In the remaining six tasks, the pass rate ranged from 86.7% to 96.7%, with only one task (setting the dose) having a pass rate of below 90% (Table 1). During observation, of the 15 ophthalmic assistants, all completed all critical tasks for PFS preparation; however, one ophthalmic assistant made a use error while aseptically attaching the supplied injection filter needle to the syringe Luer lock (Table 1). All 15 retina specialists completed all critical tasks for PFS preparation and medication administration; 3/15 (20%) made a total of four use errors: one error related to removing the filter needle cap, one error related to removing air bubbles, and two errors related to setting the dose (Table 1). During knowledge testing, 2/30 participants (7%) were unsuccessful in locating information; two participants did not locate the information regarding refrigerated storage and one participant did not locate the information related to inspection of the appearance of the drug product (Table 1). One participant provided a partially correct response for the refrigerated storage task.
 |
Table 1 Task Performance in the Simulated-Use Validation Study |
Across all tasks, there were three close calls in which users almost made an error, but self-corrected and completed the task successfully (aseptic removal of the syringe from the tray [n = 1] and removal of the syringe tip cap [n = 2]). Four participants encountered difficulties but were able to successfully complete the tasks: one participant had difficulty removing the syringe tip cap, two participants had difficulty locating information related to refrigerated storage, and one participant had difficulty locating the expiry date.
Actual-Use Study
Of the 35 patients enrolled in the actual-use study, 19 (54.3%) were men and the mean age was 74.7 years (Table 2). Most patients were White (n = 33, 94.3%) and not Hispanic or Latino (n = 32, 91.4%). Twenty-two patients (62.9%) had nAMD in the study eye, 12 (34.3%) had DME, and one patient (2.9%) had both DME and nAMD.
 |
Table 2 Patient Demographics in the Actual-Use Validation Study |
Seven retina specialists and six ophthalmic assistants participated in the actual-use study. In total, 35 injections were performed, of which, five were performed by the retina specialist without help from an ophthalmic assistant. All injections were completed with no use errors (Table 3). There were no aseptic procedural breaches, accidental damage events, or injuries to retina specialists, ophthalmic assistants, or patients. One non-serious adverse event of eye irritation was reported in one patient. The adverse event was reported as mild in intensity and resolved on the same day; the investigator deemed the event to be related to concomitant medication and unrelated to the study drug.
 |
Table 3 Task Performance in the Actual-Use Validation Study |
Discussion
Collectively, these simulated- and actual-use studies demonstrate that retina specialists and ophthalmic assistants are able to successfully prepare and/or administer an intravitreal injection of faricimab 6 mg using the PFS and co-packaged injection filter needle in accordance with the instructions for use. No use errors were observed in the actual-use study, and the majority of participants completed the tasks with no use errors in the simulated-use validation study. Importantly, on assessment of dose-setting accuracy, an issue that has been reported during use of other large volume PFS,25,42,43 we observed a pass rate of 86.7% for the simulated-use study and 100% for the actual-use study.
PFS configurations deliver efficiency benefits and offer a safer handling alternative to vial configurations. The reduced number of steps required for dose preparation decreases the time spent by approximately 50%,25,48,49 which may help to alleviate the burden of intravitreal therapy administration on busy eye clinics. The need for fewer steps that require aseptic handling compared with the preparation of vial configurations may also decrease the risk of infection caused by poor aseptic technique. Indeed, PFS use is associated with reduced risk of endophthalmitis versus vial configurations.29,30
The faricimab 6 mg PFS has several design features that aim to support a more convenient injection procedure than with vial configurations, as well as providing additional benefits. Unlike other available PFS for intravitreal injection,33,34,36 the faricimab 6 mg PFS is co-packaged with an injection filter needle that is designed specifically for ophthalmic use to offer greater convenience. The extra-thin walls of the injection filter needle and resulting wide internal bore diameter mean that low injection forces are required for the procedure. Silicone is baked on to the inner syringe surface to reduce friction between the container wall and the piston to allow smooth plunger movement, while mitigating the risks associated with free silicone previously reported with syringes not designed for ophthalmic use. Dosing inaccuracies reported with other PFSs have been attributed to larger diameter syringes with wider dose marks.26,41–43 The 0.5 mL low-volume syringe and slim dose mark of the faricimab 6 mg PFS aim to mitigate this risk and allow for a tighter control of dosing volume.
Faricimab is the first approved intravitreal therapy that targets both angiopoietin-2 and VEGF-A signaling. Thanks to its dual mechanism of action, faricimab may provide more sustained and durable treatment responses than other available treatments targeting VEGF only.9 Indeed, in clinical trials of faricimab, 45–80% of patients with nAMD, DME, or RVO achieved extended dosing intervals of at least 12 weeks.13,14,50 The combination of procedural efficiency with the PFS configuration and the potential for extended dosing intervals with faricimab may ultimately reduce the burden on eye clinics and, therefore, increase capacity for patients to receive timely treatment.
These study results should be interpreted with the following limitations in mind. First, participants may behave differently when under observation compared with how they would prepare for and perform an intravitreal injection in routine practice. For instance, under simulated conditions with no patient present, retina specialists may put less emphasis on critical tasks, for example dose setting, in the knowledge that patient safety is not at risk in a simulated environment. Second, in order to evaluate the interpretability of the instructions for use, study participants were not trained in the faricimab 6 mg PFS procedure before participating in the studies, whereas some form of practical demonstration may be offered before first use in routine clinical practice. The requirement to pause the procedure to enable data collection, for instance during filming of the dose-setting task, may also have affected how the user performed the task. Finally, the participants of these studies had previous experience with preparing and/or delivering intravitreal injections; the usability of the PFS may therefore differ among users with less clinical experience. However, retina specialists and other healthcare professionals have expressed preferences for PFS configurations, perceiving them to be easier, faster, and safer to use than vial configurations; therefore, those with less clinical experience may appreciate the simplicity of PFS administration.25
Conclusion
These simulated- and actual-use human factors studies demonstrate that the faricimab 6 mg PFS and co-packaged injection filter needle can be used safely and effectively in the real-world clinical environment. The faricimab 6 mg PFS configuration was developed following a comprehensive human factors engineering program that included multiple evaluations and updates to the device and user interface. The innovative injection filter needle and small-volume syringe were designed and optimized specifically for ophthalmic use to offer a more efficient and safe-handling alternative to the vial for intravitreal faricimab administration.
Data Sharing Statement
For eligible studies, qualified researchers may request access to individual patient-level clinical data through a data request platform. At the time of writing, this request platform is Vivli (https://vivli.org/ourmember/roche/). For up-to-date details on Roche’s Global Policy on the Sharing of Clinical Information and how to request access to related clinical study documents, see: https://go.roche.com/data_sharing. Anonymized records for individual patients across more than 1 data source external to Roche cannot, and should not, be linked due to a potential increase in risk of patient re-identification.
Acknowledgments
The authors gratefully acknowledge Aachal Kotecha of F. Hoffmann-La Roche AG for their intellectual contribution and also thank Katy Sutcliffe PhD and Kayleigh Dodd PhD of PharmaGenesis Cardiff, Cardiff, UK for providing medical writing support, which has been funded by F. Hoffmann-La Roche AG., Basel, Switzerland, in accordance with Good Publication Practice (GPP 2022) guidelines (http://www.ismpp.org/gpp-2022).
Funding
Funding for the article was provided by F. Hoffmann-La Roche AG, Basel, Switzerland.
Disclosure
MRB has received personal fees from AbbVie Inc., Alcon, Allegro, Allergan, Alimera, Apellis, Arctic Vision, Astellas, Bausch & Lomb, Biocryst, Biogen, Boehringer Ingelheim, Coherus BioSciences, CalciMedica, Celltrion, Cencora, EyeBio, Harrow, Janssen, Kanghong/Vanotech, Neurotech, Ocular Therapeutix, Outlook Therapeutics, Oxurion, Perfuse, RegenxBio, RevOpsis Therapeutics, Stealth Biotherapeutics, Palatin Technologies, Regeneron, Roche; grants and personal fees from Adverum Biotechnologies, Clearside Biomedical, EyePoint Pharmaceuticals, Graybug, Genentech, Kodiak Sciences, Opthea, Novartis, and RegenxBio; other from NeuBase and RevOpsis Therapeutics; grants and other from Oxurion; and grants from Annexon Biosciences, Gemini Therapeutics, Gyroscope Therapeutics, Oculis, Oxular, ReNeuron, Ribomic, Stealth Biotherapeutics, and Unity Biotechnology. HMKJr has received consulting/speaking fees from Dutch Ophthalmic Research Centre International and Ocular Therapeutix; and research grants/support from Acelyrin, Adverum, Alexion, Alimera, Alkeus, Amydis, Apellis, Aviceda, Boehringer Ingelheim Pharmaceuticals, Clearside, Eyepoint, F. Hoffmann-La Roche AG, Gemini, Genentech, Inc., Henlius, Ionis, Janssen, Nanoscope, Ocugen, Ocular Therapeutix, Ocuterra, Opthea, Rezolute, Smilebiotek Zhuhai, Stealth BioTherapeutics, and Xolaris. GM is an employee of F. Hoffmann-La Roche AG and reports patents (015065385, 29/950674 and 29/950679) pending to F. Hoffmann-La Roche AG. LPP and YT are employees of Genentech, Inc. PS and OEO are employees of F. Hoffmann-La Roche AG and hold stock/stock options. PS reports a patent (P39400-US) pending to F. Hoffmann-La Roche AG. JMG has received personal fees from Alimera, Apellis, Hi-Health, IvericBio, Ocular Therapeutix, Regeneron, RegenxBio, and Roche; grants and research support from Kyowa Kirin, Ocular Therapeutix, Regeneron, RegenxBio, and Roche. The authors report no other conflicts of interest in this work.
References
1. Nikkhah H, Karimi S, Ahmadieh H. et al. Intravitreal injection of anti-vascular endothelial growth factor agents for ocular vascular diseases: clinical practice guideline. J Ophthalmic Vis Res. 2018;13(2):158–169. doi:10.4103/jovr.jovr_50_18
2. Finger RP, Daien V, Eldem BM, et al. Anti-vascular endothelial growth factor in neovascular age-related macular degeneration–a systematic review of the impact of anti-VEGF on patient outcomes and healthcare systems. BMC Ophthalmol. 2020;20(1):294. doi:10.1186/s12886-020-01554-2
3. Rao P, Lum F, Wood K, et al. Real-world vision in age-related macular degeneration patients treated with single anti-VEGF drug type for 1 year in the IRIS registry. Ophthalmology. 2018;125(4):522–528. doi:10.1016/j.ophtha.2017.10.010
4. Ciulla TA, Pollack JS, Williams DF. Visual acuity outcomes and anti-VEGF therapy intensity in diabetic macular oedema: a real-world analysis of 28 658 patient eyes. Br J Ophthalmol. 2021;105(2):216–221. doi:10.1136/bjophthalmol-2020-315933
5. Lanzetta P, Loewenstein A, Vision Academy Steering Committee. Fundamental principles of an anti-VEGF treatment regimen: optimal application of intravitreal anti–vascular endothelial growth factor therapy of macular diseases. Graefes Arch Clin Exp Ophthalmol. 2017;255(7):1259–1273. doi:10.1007/s00417-017-3647-4
6. Fleckenstein M, Schmitz-Valckenberg S, Chakravarthy U. Age-related macular degeneration: a review. JAMA. 2024;331(2):147–157. doi:10.1001/jama.2023.26074
7. Regula JT, Lundh von Leithner P, Foxton R, et al. Targeting key angiogenic pathways with a bispecific CrossMAb optimized for neovascular eye diseases. EMBO Mol Med. 2016;8(11):1265–1288. doi:10.15252/emmm.201505889
8. Canonica J, Foxton R, Garrido MG, et al. Delineating effects of angiopoietin-2 inhibition on vascular permeability and inflammation in models of retinal neovascularization and ischemia/reperfusion. Front Cell Neurosci. 2023;17:1192464. doi:10.3389/fncel.2023.1192464
9. Panos GD, Lakshmanan A, Dadoukis P, Ripa M, Motta L, Amoaku WM. Faricimab: transforming the future of macular diseases treatment - a comprehensive review of clinical studies. Drug Des Devel Ther. 2023;17:2861–2873. doi:10.2147/DDDT.S427416
10. Shirley M. Faricimab: first approval. Drugs. 2022;82(7):825–830. doi:10.1007/s40265-022-01713-3
11. Sahni J, Patel SS, Dugel PU, et al. Simultaneous inhibition of angiopoietin-2 and vascular endothelial growth factor-A with faricimab in diabetic macular edema: BOULEVARD Phase 2 randomized trial. Ophthalmology. 2019;126(8):1155–1170. doi:10.1016/j.ophtha.2019.03.023
12. VABYSMO™ (faricimab-svoa). [US Food & Drug Administration prescribing information]. Genentech, Inc. San Francisco, CA, USA, 2022. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/761235s000lbl.pdf.
13. Heier JS, Khanani AM, Quezada Ruiz C, et al. Efficacy, durability, and safety of intravitreal faricimab up to every 16 weeks for neovascular age-related macular degeneration (TENAYA and LUCERNE): two randomised, double-masked, phase 3, non-inferiority trials. Lancet. 2022;399(10326):729–740. doi:10.1016/S0140-6736(22)00010-1
14. Wykoff CC, Abreu F, Adamis AP, et al. Efficacy, durability, and safety of intravitreal faricimab with extended dosing up to every 16 weeks in patients with diabetic macular oedema (YOSEMITE and RHINE): two randomised, double-masked, phase 3 trials. Lancet. 2022;399(10326):741–755. doi:10.1016/S0140-6736(22)00018-6
15. Khanani AM, Heier J, Ruiz CQ, et al. Faricimab in neovascular age-related macular degeneration: 1-year efficacy, safety, and durability in the phase 3 TENAYA and LUCERNE trials. Invest Ophthalmol Vis Sci. 2021;62(8):428.
16. Wong TY, Haskova Z, Asik K, et al. Faricimab treat-and-extend for diabetic macular edema: two-year results from the randomized phase 3 YOSEMITE and RHINE trials. Ophthalmology. 2024;131(6):708–723. doi:10.1016/j.ophtha.2023.12.026
17. Tadayoni R, Paris LP, Danzig CJ, et al. Efficacy and safety of faricimab for macular edema due to retinal vein occlusion: 24-Week results from the BALATON and COMINO trials. Ophthalmology. 2024;131(8):950–960 doi:10.1016/j.ophtha.2024.01.029.
18. Khanani AM, Kotecha A, Chang A, et al. TENAYA and LUCERNE: two-year results from the phase 3 neovascular age-related macular degeneration trials of faricimab with treat-and-extend dosing in year 2. Ophthalmology. 2024;131(8):914–926 doi:10.1016/j.ophtha.2024.02.014.
19. Vabysmo™ (faricimab). [European Medicines Agency Summary of Product Characteristics]. F. Hoffmann-La Roche AG. Basel, Switzerland, 2022. Available from: https://www.ema.europa.eu/en/documents/product-information/vabysmo-epar-product-information_en.pdf.
20. Chugai Pharmaceuticals [homepage on the Internet]. Chugai obtains regulatory approval for Vabysmo, the first bispecific antibody in ophthalmology, for neovascular age-related macular degeneration and diabetic macular edema; 2022. Available from: https://www.chugai-pharm.co.jp/english/news/detail/20220328160002_909.html.
21. Chugai Pharmaceuticals [homepage on the Internet]. Chugai obtains regulatory approval for Vabysmo, the only bispecific antibody in the ophthalmology field, for additional indication of macular edema associated with retinal vein occlusion; 2024. Available from: https://www.chugai-pharm.co.jp/english/news/detail/20240326160000_1054.html.
22. European Medicines Agency [homepage on the Internet]. European Commission approves Roche’s Vabysmo for treatment of retinal vein occlusion (RVO); 2024. Available from: https://www.roche.com/media/releases/med-cor-2024-07-30.
23. Genentech [homepage on the Internet]. FDA approves Genentech’s Vabysmo for the treatment of retinal vein occlusion (RVO); 2023. Available from: https://www.gene.com/media/press-releases/15009/2023-10-26/fda-approves-genentechs-vabysmo-for-the-.
24. Ali F, Tabano D, Garmo V, et al. Two-year real-world clinical outcomes update with faricimab in patients with neovascular age-related macular degeneration in the USA: the FARETINA-AMD study.
25. Uzzan J, Mapani A, Cox O, Bagijn M, Saffar I. Clinical outcomes and experiences with prefilled syringes versus vials for intravitreal administration of anti-VEGF treatments: a systematic review. Ophthalmol Ther. 2024;13(9):2445–2465. doi:10.1007/s40123-024-01002-0
26. Parenky AC, Wadhwa S, Chen HH, Bhalla AS, Graham KS, Shameem M. Container closure and delivery considerations for intravitreal drug administration. AAPS Pharm Sci Tech. 2021;22(3):100. doi:10.1208/s12249-021-01949-4
27. Sassalos TM, Paulus YM. Prefilled syringes for intravitreal drug delivery. Clin Ophthalmol. 2019;13:701–706. doi:10.2147/OPTH.S169044
28. Benhamou D, Weiss M, Borms M, et al. Assessing the clinical, economic, and health resource utilization impacts of prefilled syringes versus conventional medication administration methods: results from a systematic literature review. Ann Pharmacother. 2023;10600280231212890.
29. Louis AM, Ali AM, Patel SB, et al. Impact of prefilled syringes and masking on postintravitreal injection endophthalmitis. J Vitreoretin Dis. 2023;7(5):382–388. doi:10.1177/24741264231191339
30. Storey PP, Tauqeer Z, Yonekawa Y, et al. The impact of prefilled syringes on endophthalmitis following intravitreal injection of ranibizumab. Am J Ophthalmol. 2019;199:200–208. doi:10.1016/j.ajo.2018.11.023
31. Healio, Occular Surgery News [homepage on the Internet]. Significant investments will continue to advance retinal disease field; 2023. Available from: https://www.healio.com/news/ophthalmology/20230915/significant-investments-will-continue-to-advance-retinal-disease-field.
32. Melo GB, Cruz N, Emerson GG, et al. Critical analysis of techniques and materials used in devices, syringes, and needles used for intravitreal injections. Prog Retin Eye Res. 2021;80:100862. doi:10.1016/j.preteyeres.2020.100862
33. BEOVU® (brolucizumab-dbll). [US Food and Drug Administration Prescribing Information]. Novartis Pharmaceuticals Corporation, East Hanover, New Jersey, USA, 2023. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/761125s021lbl.pdf.
34. EYLEA® (aflibercept). [US Food and Drug Administration Prescribing Information]. Regeneron Pharmaceuticals, Inc. Tarrytown, New York, USA, 2024. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/125387s084lbl.pdf.
35. Antoszyk AN, Baker C, Calzada J, et al. Usability of the ranibizumab 0.5 mg prefilled syringe: human factors studies to evaluate critical task completion by healthcare professionals. PDA J Pharm Sci Technol. 2018;72(4):411–419. doi:10.5731/pdajpst.2017.008342
36. LUCENTIS® (ranibizumab injection). [US Food & Drug Administration prescribing information]. Genentech, Inc. San Francisco, CA, USA, 2024, Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/125156s128lbl.pdf.
37. Roche [homepage on the Internet]. FDA approves Roche’s Vabysmo prefilled syringe (PFS) for three leading causes of vision loss; 2024. Available from: https://www.roche.com/media/releases/med-cor-2024-07-05.
38. Badkar A, Wolf A, Bohack L, Kolhe P. Development of biotechnology products in pre-filled syringes: technical considerations and approaches. AAPS Pharm Sci Tech. 2011;12(2):564–572. doi:10.1208/s12249-011-9617-y
39. Khurana RN, Chang LK, Porco TC. Incidence of presumed silicone oil droplets in the vitreous cavity after intravitreal bevacizumab injection with insulin syringes. JAMA Ophthalmol. 2017;135(7):800–803. doi:10.1001/jamaophthalmol.2017.1815
40. Melo GB, Emerson GG, Dias CS Jr, et al. Release of silicone oil and the off-label use of syringes in ophthalmology. Br J Ophthalmol. 2020;104(2):291–296. doi:10.1136/bjophthalmol-2019-313823
41. Moisseiev E, Rudell J, Tieu EV, Yiu G. Effect of syringe design on the accuracy and precision of intravitreal injections of anti-VEGF agents. Curr Eye Res. 2017;42(7):1059–1063. doi:10.1080/02713683.2016.1276195
42. Dingerkus VLS, Somfai GM, Kinzl S, Orgul SI, Becker MD, Heussen FM. Incidence of severe rise in intraocular pressure after intravitreous injection of aflibercept with prefilled syringes. Sci Rep. 2022;12(1):18136. doi:10.1038/s41598-022-23039-6
43. Guest JM, Malbin B, Abrams G, et al. Accuracy of intravitreal injection volume for aflibercept pre-filled syringe and BD Luer-Lok one-milliliter syringe. Int J Retina Vitreous. 2022;8(1):27. doi:10.1186/s40942-022-00375-3
44. Aronson R, Gibney MA, Oza K, Bérubé J, Kassler-Taub K, Hirsch L. Insulin pen needles: effects of extra-thin wall needle technology on preference, confidence, and other patient ratings. Clin Ther. 2013;35(7):923–933. doi:10.1016/j.clinthera.2013.05.020
45. European Medicines Agency [homepage on the Internet]. Guideline on the quality requirements for drug-device combinations; 2019. Available from: https://www.ema.europa.eu/en/documents/scientific-guideline/draft-guideline-quality-requirements-drug-device-combinations-first-version_en.pdf.
46. US Food and Drug Administration [homepage on the Internet]. Applying Human Factors and Usability Engineering to Medical Devices. Guidance for Industry and Food and Drug Administration Staff; 2016. Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/applying-human-factors-and-usability-engineering-medical-devices.
47. The International Organization for Standardization [homepage on the Internet]. International Electrotechnical Commission 62366-1:2015(en) Medical devices - Part 1: application of usability engineering to medical devices; 201. Available from: https://www.iso.org/obp/ui/en/#iso:std:iec:62366:-1:ed-1:v1:en.
48. Souied E, Nghiem-Buffet S, Leteneux C, et al. Ranibizumab prefilled syringes: benefits of reduced syringe preparation times and less complex preparation procedures. Eur J Ophthalmol. 2015;25(6):529–534. doi:10.5301/ejo.5000629
49. Subhi Y, Kjer B, Munch IC. Prefilled syringes for intravitreal injection reduce preparation time. Dan Med J. 2016;63(4):A5214.
50. Ghanchi F, Abreu F, Arrisi P, et al. Efficacy, safety, and durability of faricimab in macular edema due to retinal vein occlusion: 72-week results from the BALATON and COMINO trials. Invest Ophthalmol Vis Sci. 2024;65(7):3124.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.